<< back to Pathology Atlas menu
Pathology Atlas: Vulva
Condyloma
 Condylomata showing acanthosis, parakeratosis
and koilocytotic changes.
Condylomata showing acanthosis, parakeratosis
and koilocytotic changes.
Back to Top
Vulvar Intraepithelial Neoplasia (VIN)
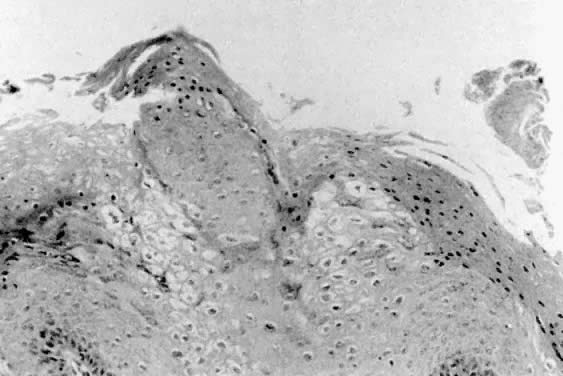
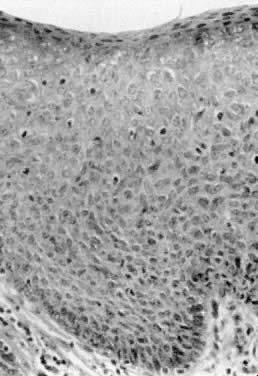
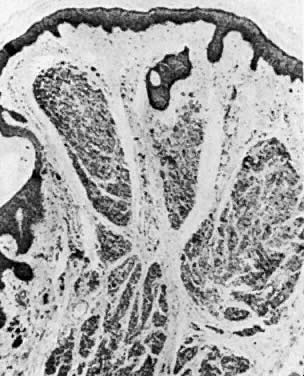
 Flat condyloma acuminatum/vulvar intraepithelial neoplasia (VIN) 1. There
is lack of maturation in the lower one third of the epithelium and
maturation with koilocytosis in the upper epithelium.
Flat condyloma acuminatum/vulvar intraepithelial neoplasia (VIN) 1. There
is lack of maturation in the lower one third of the epithelium and
maturation with koilocytosis in the upper epithelium.
 Vulvar intraepithelial neoplasia (VIN) 3, multifocal. Note raised pale
lesions on outer minora and across fourchette.
Vulvar intraepithelial neoplasia (VIN) 3, multifocal. Note raised pale
lesions on outer minora and across fourchette.
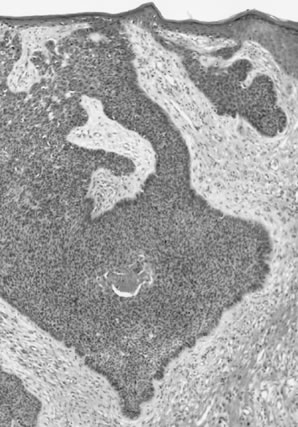
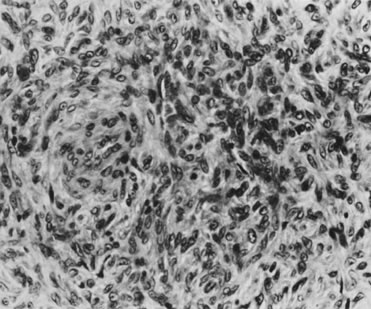
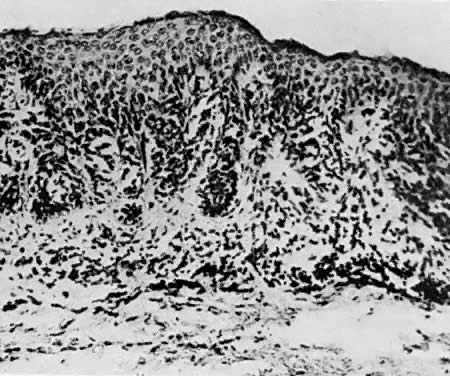
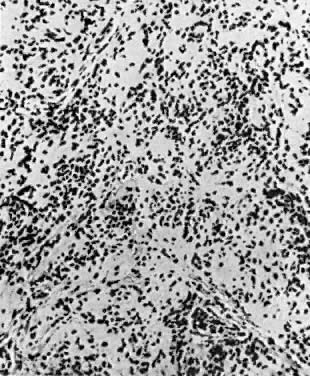
 Vulvar intraepithelial neoplasia (VIN) 3 (severe dysplasia), basaloid type. This
intraepithelial lesion is composed of relatively uniform epithelial
cells with little maturation and nuclear hyperchromasia.
Vulvar intraepithelial neoplasia (VIN) 3 (severe dysplasia), basaloid type. This
intraepithelial lesion is composed of relatively uniform epithelial
cells with little maturation and nuclear hyperchromasia.
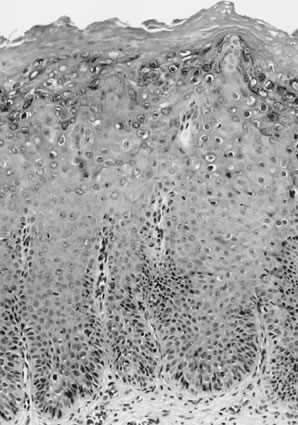
 Vulvar intraepithelial neoplasia (VIN) 3 (severe dysplasia/carcinoma in situ ), warty type. Atypical cells extend throughout the full thickness of
the epithelium. There is nuclear pleomorphism with koilocytes near the
surface.
Vulvar intraepithelial neoplasia (VIN) 3 (severe dysplasia/carcinoma in situ ), warty type. Atypical cells extend throughout the full thickness of
the epithelium. There is nuclear pleomorphism with koilocytes near the
surface.
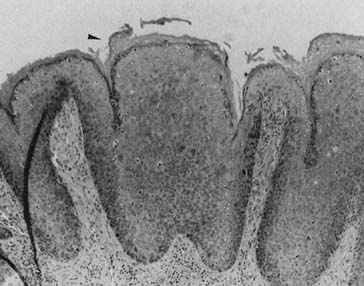 VIN III. Note large irregular nuclei, loss of differentiation, and overlying
hyperkeratosis (black arrow).
VIN III. Note large irregular nuclei, loss of differentiation, and overlying
hyperkeratosis (black arrow).
Back to Top
Paget Disease
 Primary Paget disease (type 1). Note irregular patchy change present on
lateral aspect of labium majus.
Primary Paget disease (type 1). Note irregular patchy change present on
lateral aspect of labium majus.
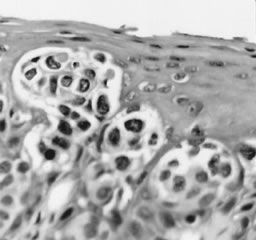
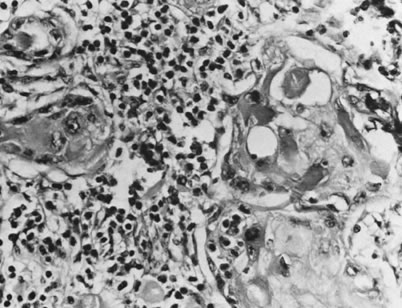
 Primary Paget disease (type 1). Characteristic large, pale Paget cells
are just above basal layer (magnification, ×500).
Primary Paget disease (type 1). Characteristic large, pale Paget cells
are just above basal layer (magnification, ×500).
 Type 3 Paget disease of the vulva (pagetoid urothelial intraepithelial
neoplasia [PUIN]). The vulvar epithelium is infiltrated by clusters
of high-grade urothelial carcinoma. The nuclei are hyperchromatic
with irregular contours.
Type 3 Paget disease of the vulva (pagetoid urothelial intraepithelial
neoplasia [PUIN]). The vulvar epithelium is infiltrated by clusters
of high-grade urothelial carcinoma. The nuclei are hyperchromatic
with irregular contours.
Back to Top
Squamous Cell Carcinoma
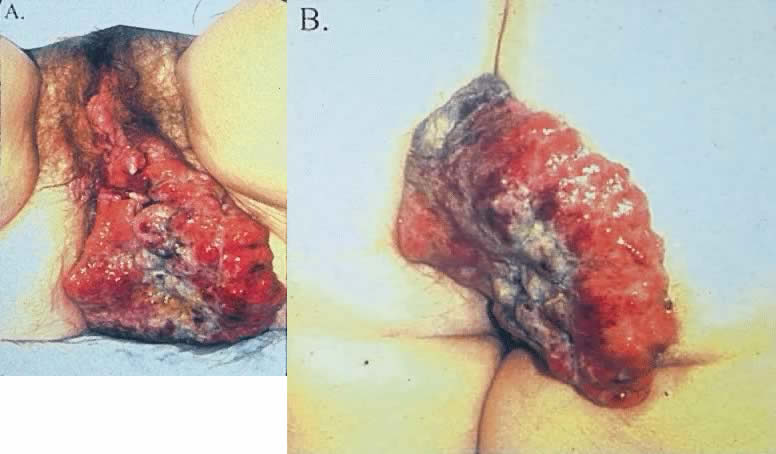 Locally extensive vulvar cancer arising from the posterior lateral vulva ( A) and extending onto the buttocks ( B ). Such cases are commonly associated with profound denial and embarrassment
and are generally not resectable primarily.
Locally extensive vulvar cancer arising from the posterior lateral vulva ( A) and extending onto the buttocks ( B ). Such cases are commonly associated with profound denial and embarrassment
and are generally not resectable primarily.
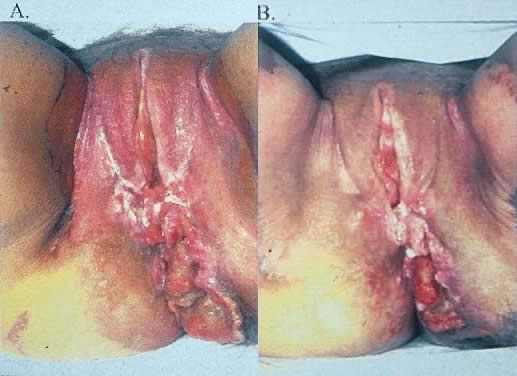 Patient with vulvar cancer after 4 weeks ( A) and 6 weeks ( B) of chemoradiation. Extensive tumor resolution is observed and extensive
skin reaction demonstrated. Further therapy by posterior exenteration
offered local control.
Patient with vulvar cancer after 4 weeks ( A) and 6 weeks ( B) of chemoradiation. Extensive tumor resolution is observed and extensive
skin reaction demonstrated. Further therapy by posterior exenteration
offered local control.
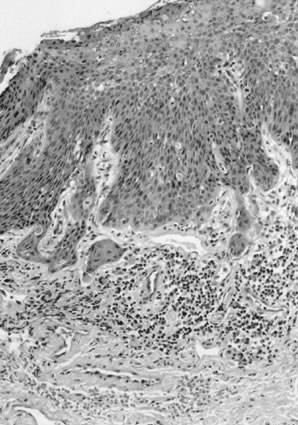 Superficially invasive squamous cell carcinoma with vulvar intraepithelial
neoplasia (VIN) 3. There is a marked inflammatory response.
Superficially invasive squamous cell carcinoma with vulvar intraepithelial
neoplasia (VIN) 3. There is a marked inflammatory response.
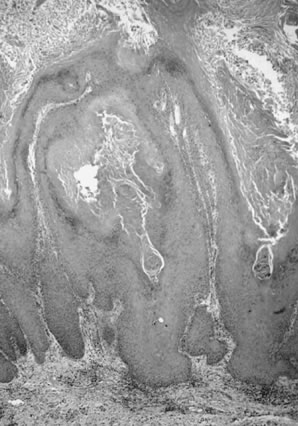
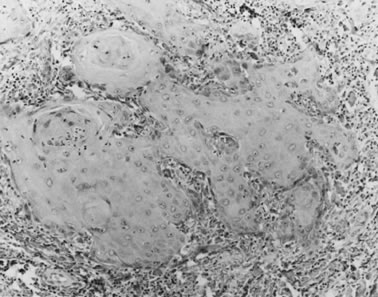 Well-differentiated squamous carcinoma. Large cells with abundant cytoplasm
form keratin pearls (magnification, ×80).
Well-differentiated squamous carcinoma. Large cells with abundant cytoplasm
form keratin pearls (magnification, ×80).
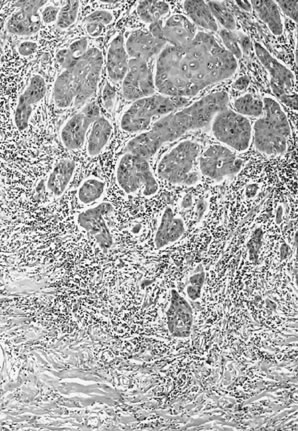 Poorly differentiated squamous cell carcinoma of the vulva. The tumor cells
are nonkeratinized, without prominent intercellular bridges. The
tumor has a “finger-like” pattern of invasion.
Poorly differentiated squamous cell carcinoma of the vulva. The tumor cells
are nonkeratinized, without prominent intercellular bridges. The
tumor has a “finger-like” pattern of invasion.
 Adenoid-squamous pattern with pseudoglandular spaces lined by squamous
cells (magnification, ×500).
Adenoid-squamous pattern with pseudoglandular spaces lined by squamous
cells (magnification, ×500).
 Squamous cell carcinoma, warty or condylomatous type. The epithelium shows
little cellular atypia and the tumor-dermal interface is infiltrative
rather than pushing in appearance.
Squamous cell carcinoma, warty or condylomatous type. The epithelium shows
little cellular atypia and the tumor-dermal interface is infiltrative
rather than pushing in appearance.
Back to Top
Basal Cell Carcinoma
 Basal cell carcinoma. The tumor is composed of small, uniform hyperchromatic
cells with peripheral palisading of the nuclei. Central necrosis
is present focally.
Basal cell carcinoma. The tumor is composed of small, uniform hyperchromatic
cells with peripheral palisading of the nuclei. Central necrosis
is present focally.
Back to Top
Melanoma
 Malignant melanoma. Large nevoid cells with prominent nucleoli extend down
from dermoepidermal junction. Some contain pigment (magnification, ×400).
Malignant melanoma. Large nevoid cells with prominent nucleoli extend down
from dermoepidermal junction. Some contain pigment (magnification, ×400).
Back to Top
Leiomyosarcoma
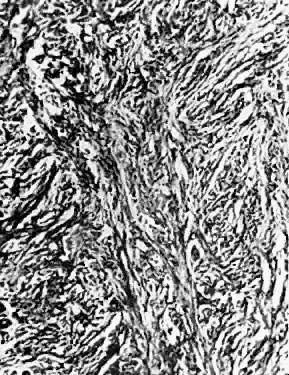
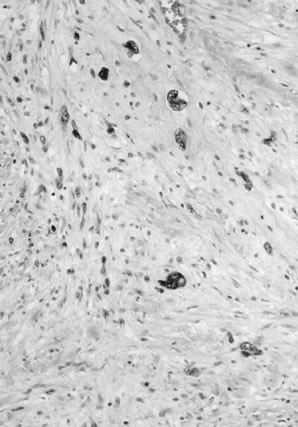 Leiomyosarcoma of the vulva. The tumor is composed of fascicles of smooth
muscle with nuclear atypia, characterized by enlarged, irregular, and
hyperchromatic nuclei.
Leiomyosarcoma of the vulva. The tumor is composed of fascicles of smooth
muscle with nuclear atypia, characterized by enlarged, irregular, and
hyperchromatic nuclei.
Back to Top
Histiocytoma
 Fibrous histiocytoma. Spindle-shaped cells with elongated nuclei form swirling
patterns (magnification, ×400).
Fibrous histiocytoma. Spindle-shaped cells with elongated nuclei form swirling
patterns (magnification, ×400).
Back to Top
Carcinoma in situ
 Carcinoma
in situ showing epithelial atypia throughout the epithelial layer.
Carcinoma
in situ showing epithelial atypia throughout the epithelial layer.
Back to Top
Hidradenoma
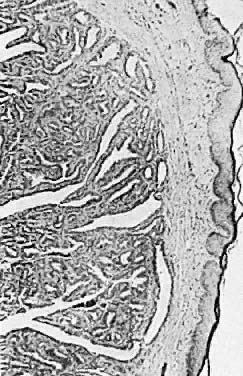 Hidradenoma of the vulva ( × 25)
Hidradenoma of the vulva ( × 25)
Back to Top
Syringoma
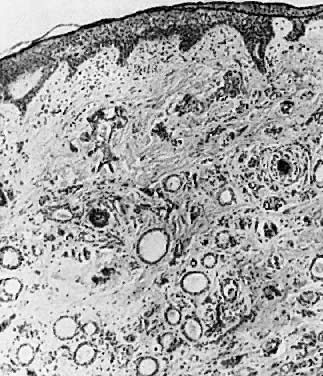 Fig. 8 . Syringoma Numerous dilated sweat gland ducts
are seen ( × 35).
Fig. 8 . Syringoma Numerous dilated sweat gland ducts
are seen ( × 35).
Back to Top
Nevi
 Intradermal nevus. Nevus cells are seen in
the upper dermis ( × 40)
Intradermal nevus. Nevus cells are seen in
the upper dermis ( × 40)
 Junctional nevus. This type may become malignant
( × 50)
Junctional nevus. This type may become malignant
( × 50)
 Compound nevus. Nevus cells are seen at the
junction of the epidermis and dermis and in the upper dermis (× 50)
Compound nevus. Nevus cells are seen at the
junction of the epidermis and dermis and in the upper dermis (× 50)
Back to Top
Fibroma
 Fibroma. Coarse bundles of fibroblasts and fibrocytes are seen ( × 65)
Fibroma. Coarse bundles of fibroblasts and fibrocytes are seen ( × 65)
Back to Top
Neurofibroma
 Neurofibroma. Spindle cells with angulated
nuclei are seen ( × 50)
Neurofibroma. Spindle cells with angulated
nuclei are seen ( × 50)
Back to Top
Granular cell tumor
 Granular cell tumor ( × 70)
Granular cell tumor ( × 70)
Back to Top
Lymphangioma
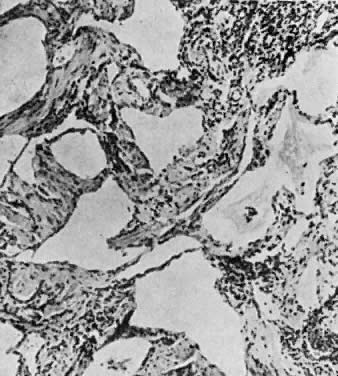 Lymphangioma with many dilated lymphatic channels
( × 90)
Lymphangioma with many dilated lymphatic channels
( × 90)
Back to Top | 