<< back to Pathology Atlas menu
Pathology Atlas: Cervix
Squamocolumnar Junction
 Photomicrograph (low power) of the epithelial
lining at the junction of the cervix and vagina in the human. The glands
of the cervix are definitely evident. There are no glands underlying the
squamous epithelium of the vagina. (After R. Shroder.)
Photomicrograph (low power) of the epithelial
lining at the junction of the cervix and vagina in the human. The glands
of the cervix are definitely evident. There are no glands underlying the
squamous epithelium of the vagina. (After R. Shroder.)
Back to Top
Reserve Cell Hyperplasia
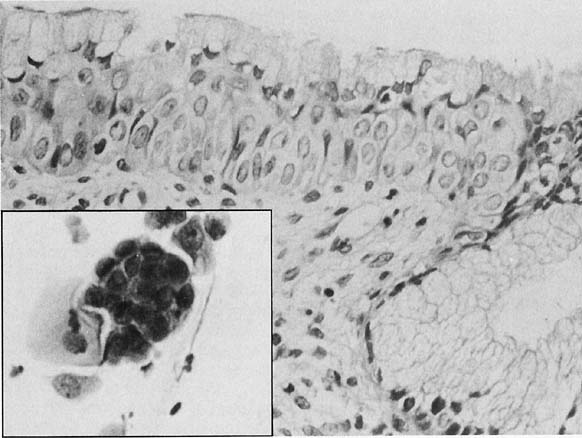 Histologic section showing reserve cell hyperplasia
and squamous metaplasia of the endocervix (Hematoxylin and eosin, ×
260). Inset. Reserve cell hyperplasia and squamous metaplasia of the endocervix.
The cells are small and monomorphic, with finely distributed chromatin.(Papanicolaou,
× 360).
Histologic section showing reserve cell hyperplasia
and squamous metaplasia of the endocervix (Hematoxylin and eosin, ×
260). Inset. Reserve cell hyperplasia and squamous metaplasia of the endocervix.
The cells are small and monomorphic, with finely distributed chromatin.(Papanicolaou,
× 360).
Back to Top
Condyloma
 Condyloma acuminatum. Papillary eqithelial
proliferation with koilocytes and parakeratosis are seen in the periphery
of the epithelium and vascular connective tissue cores in the center.
(Hematoxylin-eosin, ×300.)
Condyloma acuminatum. Papillary eqithelial
proliferation with koilocytes and parakeratosis are seen in the periphery
of the epithelium and vascular connective tissue cores in the center.
(Hematoxylin-eosin, ×300.)
Back to Top
CIN I
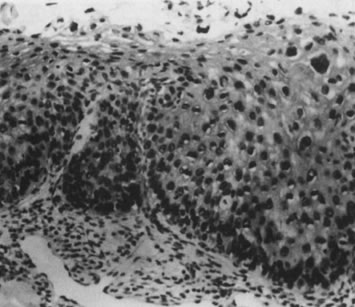 Cervical intraepithelial neoplasia grade 1.
Nuclear atypia, increased mitoses, nuclear crowding, and occasional binucleated
forms are seen on the parabasal cell layers. Koilocytotic changes are
prominent in the upper cell layers. (Hematoxylin-eosin, ×500.)
Cervical intraepithelial neoplasia grade 1.
Nuclear atypia, increased mitoses, nuclear crowding, and occasional binucleated
forms are seen on the parabasal cell layers. Koilocytotic changes are
prominent in the upper cell layers. (Hematoxylin-eosin, ×500.)
Back to Top
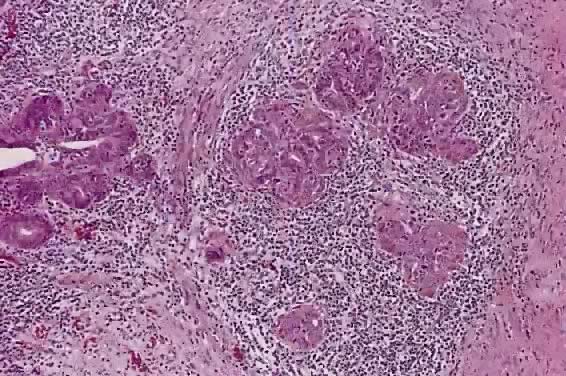
Squamous Cell Carcinoma
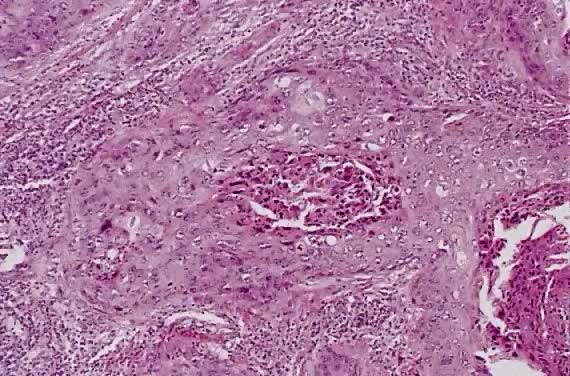 Squamous cell carcinoma, large cell keratinizing
type. Malignant squamous cells form irregular nests invade the stroma.
In the center of the nest, laminated keratin pearl is present. Individual
cells have abundant eosinophilic keratinized cytoplasm.(Hematoxylin-eosin
stain, original magnification
Squamous cell carcinoma, large cell keratinizing
type. Malignant squamous cells form irregular nests invade the stroma.
In the center of the nest, laminated keratin pearl is present. Individual
cells have abundant eosinophilic keratinized cytoplasm.(Hematoxylin-eosin
stain, original magnification  200.) 200.)
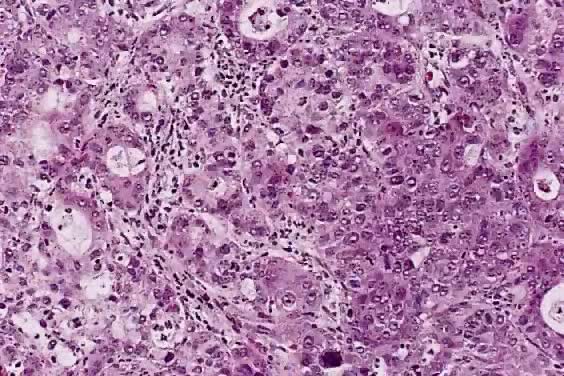
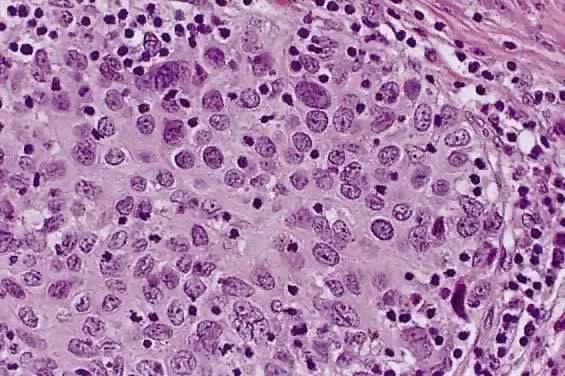 Squamous cell carcinoma, large cell nonkeratinizing
type. Tumor cells have abundant eosinophilic cytoplasm and distinct cell
borders to suggest individual cell keratinization. The irregular, large
nuclei contain multiple nucleoli.(Hematoxylin-eosin stain, original magnification
400.)
Squamous cell carcinoma, large cell nonkeratinizing
type. Tumor cells have abundant eosinophilic cytoplasm and distinct cell
borders to suggest individual cell keratinization. The irregular, large
nuclei contain multiple nucleoli.(Hematoxylin-eosin stain, original magnification
400.)
 Squamous cell carcinoma, small cell nonkeratinizing
type. The tumor cells have small round-to-oval nuclei, finely granular
chromatin, and small nucleoli. Most of the tumor cells contain a small
amount of eosinophilic cytoplasm. Mitotic figures are abundant.(Hematoxylin-eosin
stain, original magnification 400.)
Squamous cell carcinoma, small cell nonkeratinizing
type. The tumor cells have small round-to-oval nuclei, finely granular
chromatin, and small nucleoli. Most of the tumor cells contain a small
amount of eosinophilic cytoplasm. Mitotic figures are abundant.(Hematoxylin-eosin
stain, original magnification 400.)
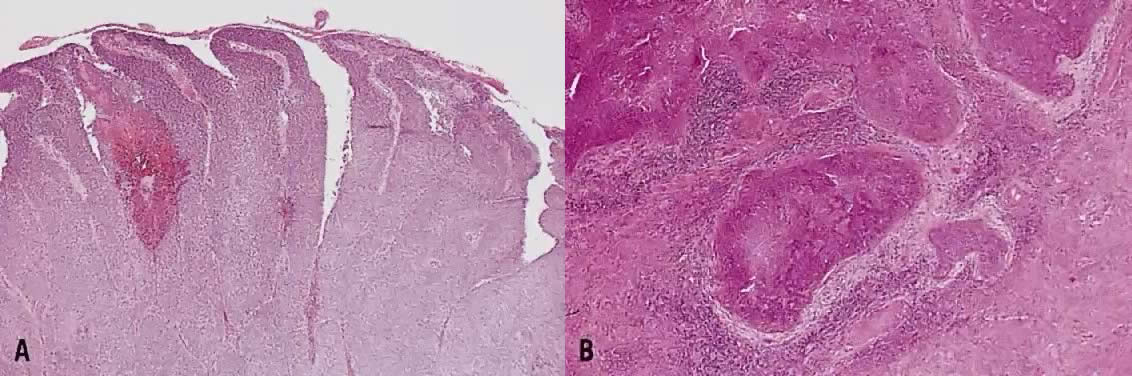 Papillary squamous carcinoma. ( A) Multiple
papillary fronds are supported by delicate fibrovascular cores. ( B) Irregular
nests of invasive squamous cells at the base of papillary structures.
Desmoplastic reaction occurs around the tumor cells.(Hematoxylin-eosin
stain, original magnification A: 40,
B: 40.)
Papillary squamous carcinoma. ( A) Multiple
papillary fronds are supported by delicate fibrovascular cores. ( B) Irregular
nests of invasive squamous cells at the base of papillary structures.
Desmoplastic reaction occurs around the tumor cells.(Hematoxylin-eosin
stain, original magnification A: 40,
B: 40.)
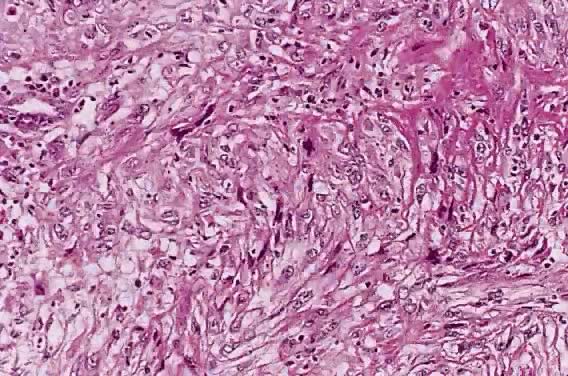 Squamous carcinoma, spindle cell type. Elongated
tumor cells are arranged in bundles simulating spindle cell sarcoma. Immunohistochemical
stain for cytokeratin is positive to confirm carcinoma (not shown).(Hematoxylin-eosin
stain, original magnification 200.)
Squamous carcinoma, spindle cell type. Elongated
tumor cells are arranged in bundles simulating spindle cell sarcoma. Immunohistochemical
stain for cytokeratin is positive to confirm carcinoma (not shown).(Hematoxylin-eosin
stain, original magnification 200.)
Back to Top
Adenocarcinoma
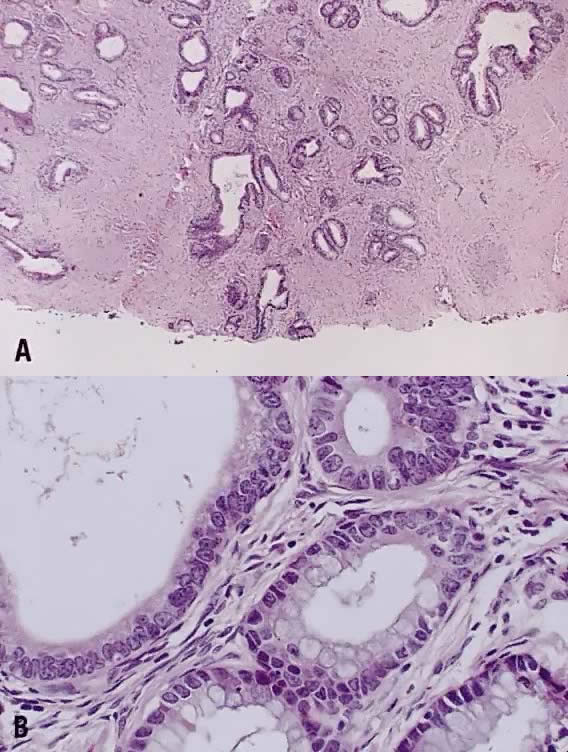
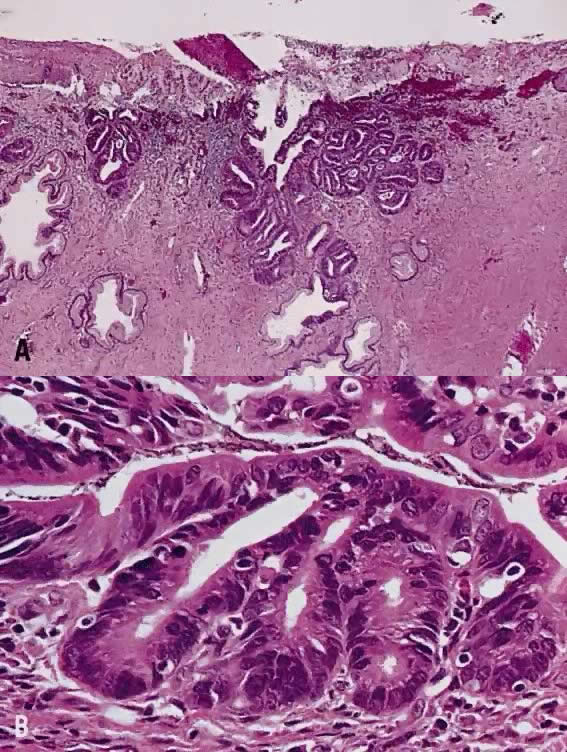 Adenocarcinoma in situ, endocervical type.
( A) The neoplastic glands retains the branching and budding pattern of
normal endocervical glands. These glands have smooth borders and are surrounded
by normal fibromuscular stroma without desmoplastic reaction. At the base
of tumor, malignant cells replace normal endocervical cells. ( B) Higher
magnification to reveal tall columnar neoplastic cells with nuclear stratification,
hyperchromasia, elongation, and irregularity.(Hematoxylin-eosin stain,
original magnification A: 40,
B: 100.)
Adenocarcinoma in situ, endocervical type.
( A) The neoplastic glands retains the branching and budding pattern of
normal endocervical glands. These glands have smooth borders and are surrounded
by normal fibromuscular stroma without desmoplastic reaction. At the base
of tumor, malignant cells replace normal endocervical cells. ( B) Higher
magnification to reveal tall columnar neoplastic cells with nuclear stratification,
hyperchromasia, elongation, and irregularity.(Hematoxylin-eosin stain,
original magnification A: 40,
B: 100.)
 Microinvasive adenocarcinoma forms multiple,
irregular tongue-like protrusions from the periphery of endocervical glands
involved by adenocarcinoma in situ. These protrusions are associated with
fibrotic stroma and chronic inflammation ( right two thirds ). In contrast,
adenocarcinoma in situ retains smooth borders ( left one third ).(Hematoxylin-eosin
stain, original magnification 200.)
Microinvasive adenocarcinoma forms multiple,
irregular tongue-like protrusions from the periphery of endocervical glands
involved by adenocarcinoma in situ. These protrusions are associated with
fibrotic stroma and chronic inflammation ( right two thirds ). In contrast,
adenocarcinoma in situ retains smooth borders ( left one third ).(Hematoxylin-eosin
stain, original magnification 200.)
 Adenocarcinoma, endocervical type, moderately
differentiated. Tumor cells form small irregular glands and solid nests.
The cytoplasm is vacuolated and mucinous in appearance. Nuclear atypia
is apparent.(Hematoxylin-eosin stain, original magnification 100.)
Adenocarcinoma, endocervical type, moderately
differentiated. Tumor cells form small irregular glands and solid nests.
The cytoplasm is vacuolated and mucinous in appearance. Nuclear atypia
is apparent.(Hematoxylin-eosin stain, original magnification 100.)
 Minimal deviation adenocarcinoma, endocervical
type. ( A) Neoplastic cells form branching, budding glands resembling
normal endocervical glands. Tumor cells extend into the deep margin of
conization specimen. ( B) Individual cells also closely mimic normal endocervical
cells, having tall columnar configuration and abundant mucinous cytoplasm
and basally located, small nuclei. On closer examination, nuclear irregularity
and small nucleoli become evident.(Hematoxylin-eosin stain, original magnification
A: 40,
B: 400.)
Minimal deviation adenocarcinoma, endocervical
type. ( A) Neoplastic cells form branching, budding glands resembling
normal endocervical glands. Tumor cells extend into the deep margin of
conization specimen. ( B) Individual cells also closely mimic normal endocervical
cells, having tall columnar configuration and abundant mucinous cytoplasm
and basally located, small nuclei. On closer examination, nuclear irregularity
and small nucleoli become evident.(Hematoxylin-eosin stain, original magnification
A: 40,
B: 400.)
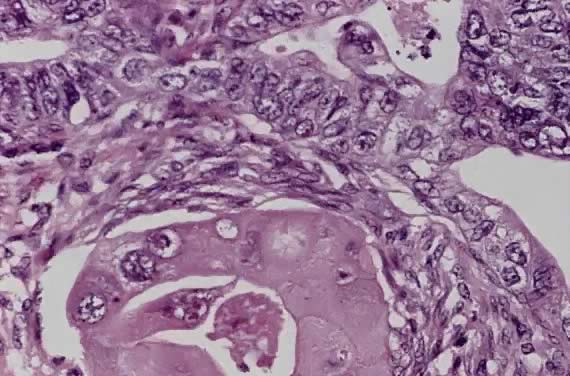
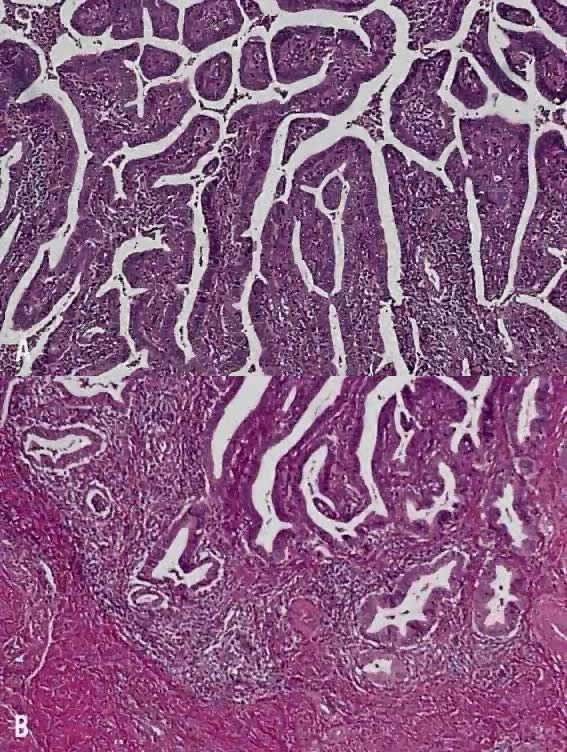 Villoglandular adenocarcinoma, endocervical
type. ( A) On the surface are multiple papillary projections consisting
of columnar cells and fibrovascular cores. ( B) The base of tumor has
smooth borders without infiltrative pattern.(Hematoxylin-eosin stain,
original magnification A: 100,
B: 100.)
Villoglandular adenocarcinoma, endocervical
type. ( A) On the surface are multiple papillary projections consisting
of columnar cells and fibrovascular cores. ( B) The base of tumor has
smooth borders without infiltrative pattern.(Hematoxylin-eosin stain,
original magnification A: 100,
B: 100.)
 Adenosquamous carcinoma, mature, well-differentiated
type. Large malignant squamous cell carcinoma with abundant eosinophilic
cytoplasm ( right ); neoplastic columnar cells form glandular lumens (
left ).(Hematoxylin-eosin stain, original magnification 200.)
Adenosquamous carcinoma, mature, well-differentiated
type. Large malignant squamous cell carcinoma with abundant eosinophilic
cytoplasm ( right ); neoplastic columnar cells form glandular lumens (
left ).(Hematoxylin-eosin stain, original magnification 200.)
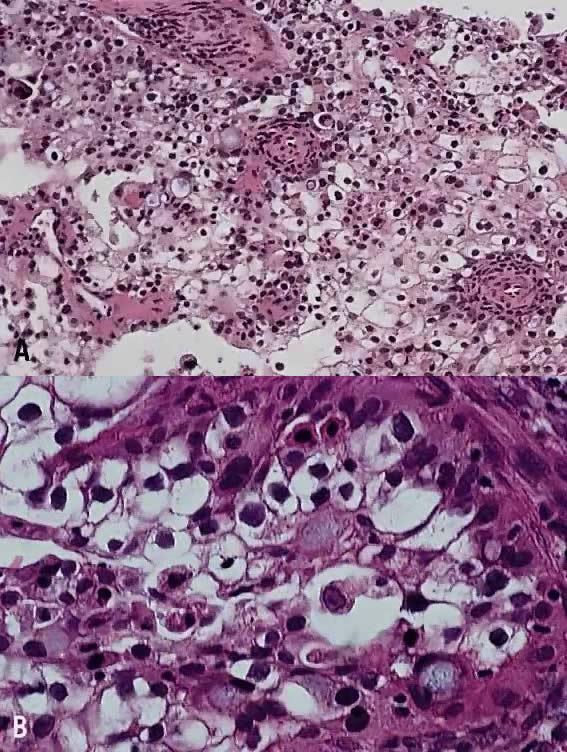 Adenosquamous carcinoma, signet-ring type.
( A) Neoplastic squamous cells have abundant eosinophilic or clear cytoplasm
and distinct cell borders. In addition, there are cells with basophilic
cytoplasm. ( B) Higher magnification reveals signet-ring cells with basophilic
vacuolated cytoplasm.(Hematoxylin-eosin stain, original magnification
A: 100,
B: 400.)
Adenosquamous carcinoma, signet-ring type.
( A) Neoplastic squamous cells have abundant eosinophilic or clear cytoplasm
and distinct cell borders. In addition, there are cells with basophilic
cytoplasm. ( B) Higher magnification reveals signet-ring cells with basophilic
vacuolated cytoplasm.(Hematoxylin-eosin stain, original magnification
A: 100,
B: 400.)
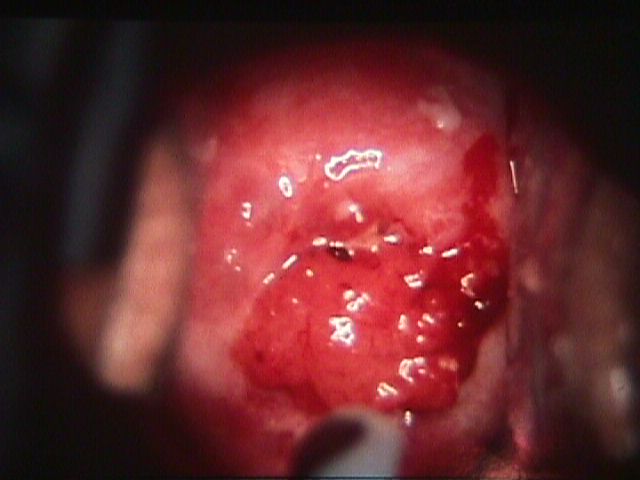 Adenocarcinoma
of the cervix (From Operational Obstetrics & Gynecology
- 2nd Edition, The Health Care of Women in Military Settings, CAPT Michael
John Hughey, MC, USNR, NAVMEDPUB 6300-2C, Bureau of Medicine and Surgery,
Department of the Navy, 2300 E Street NW, Washington, D.C. 20372-5300,
January 1, 2000. Original image courtesy CAPT Richard Stock, MC, USN) Adenocarcinoma
of the cervix (From Operational Obstetrics & Gynecology
- 2nd Edition, The Health Care of Women in Military Settings, CAPT Michael
John Hughey, MC, USNR, NAVMEDPUB 6300-2C, Bureau of Medicine and Surgery,
Department of the Navy, 2300 E Street NW, Washington, D.C. 20372-5300,
January 1, 2000. Original image courtesy CAPT Richard Stock, MC, USN)
Back to Top
Other Cervical Malignancies
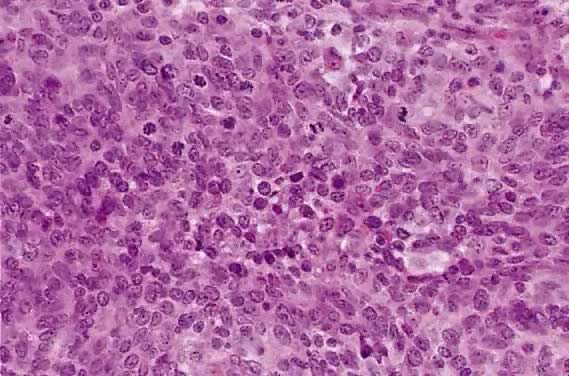
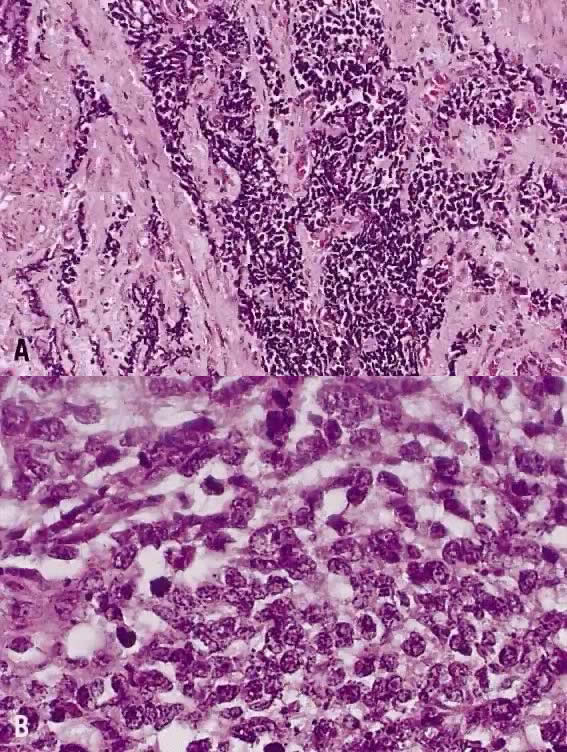 Small cell anaplastic carcinoma. ( A) A diffuse
infiltrative pattern by sheets and cords of malignant cells. The crush
artifact with smudged nuclei is also characteristic of this neoplasm.
( B) The small nuclei are hyperchromatic and have coarsely granular compact
chromatin. The nucleoli are not visible nor inconspicuous. The cytoplasm
is scant, resulting in nuclear molding. Mitotic activity is high.(Hematoxylin-eosin
stain, original magnification A: 100,
B: 400.)
Small cell anaplastic carcinoma. ( A) A diffuse
infiltrative pattern by sheets and cords of malignant cells. The crush
artifact with smudged nuclei is also characteristic of this neoplasm.
( B) The small nuclei are hyperchromatic and have coarsely granular compact
chromatin. The nucleoli are not visible nor inconspicuous. The cytoplasm
is scant, resulting in nuclear molding. Mitotic activity is high.(Hematoxylin-eosin
stain, original magnification A: 100,
B: 400.)
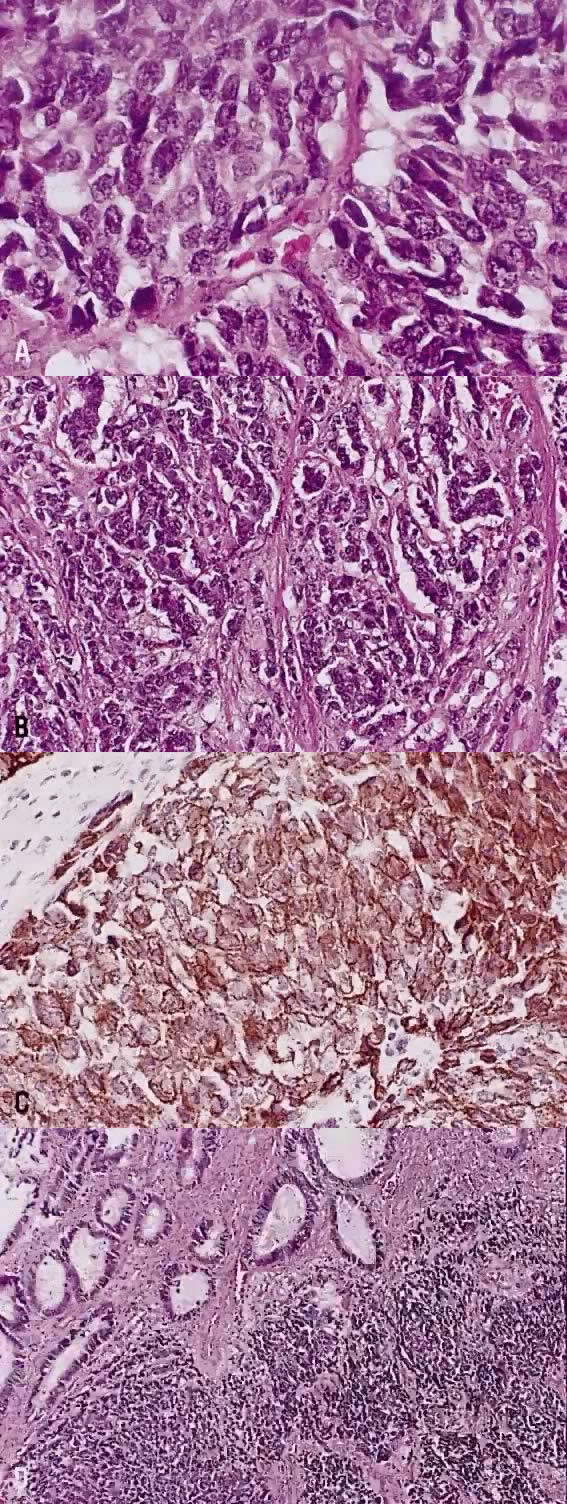 Large cell neuroendocrine carcinoma. ( A) Tumor
cells have large oval of elongated hyperchromatic nuclei which contain
coarsely granular chromatin. The nucleoli are small or absent. There is
a small amount of eosinophilic cytoplasm. ( B) Tumor cells are arranged
in cords and ribbons. ( C) Same tumor as in A. Diffuse cytoplasmic deposit
of chromogranin indicative of neuroendocrine differentiation. ( D) Neuroendocrine
carcinoma ( right lower field) coexists with adenocarcinoma ( left upper
field ).(Hematoxylin-eosin stain, original magnification A: 400,
B: 200,
D: 100;
C: immunohistochemical stain for chromogranin, original magnification
400.)
Large cell neuroendocrine carcinoma. ( A) Tumor
cells have large oval of elongated hyperchromatic nuclei which contain
coarsely granular chromatin. The nucleoli are small or absent. There is
a small amount of eosinophilic cytoplasm. ( B) Tumor cells are arranged
in cords and ribbons. ( C) Same tumor as in A. Diffuse cytoplasmic deposit
of chromogranin indicative of neuroendocrine differentiation. ( D) Neuroendocrine
carcinoma ( right lower field) coexists with adenocarcinoma ( left upper
field ).(Hematoxylin-eosin stain, original magnification A: 400,
B: 200,
D: 100;
C: immunohistochemical stain for chromogranin, original magnification
400.)
Back to Top
|