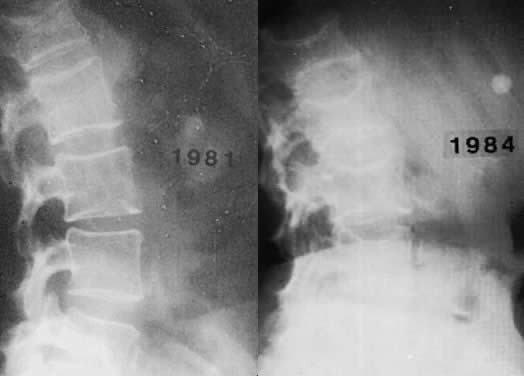
 Fig. 3. Radiograph of the spine of a patient with postmenopausal (involutional) osteoporosis. A. At 51 years of age. B. At 54 years of age. The patient suffered two hip fractures in the intervening 3 years.
Volume 1, Chapter 106
Fig. 3. Radiograph of the spine of a patient with postmenopausal (involutional) osteoporosis. A. At 51 years of age. B. At 54 years of age. The patient suffered two hip fractures in the intervening 3 years.
Volume 1, Chapter 106
|
X-ray Michael John Hughey |
|
|
Michael John Hughey, MD |
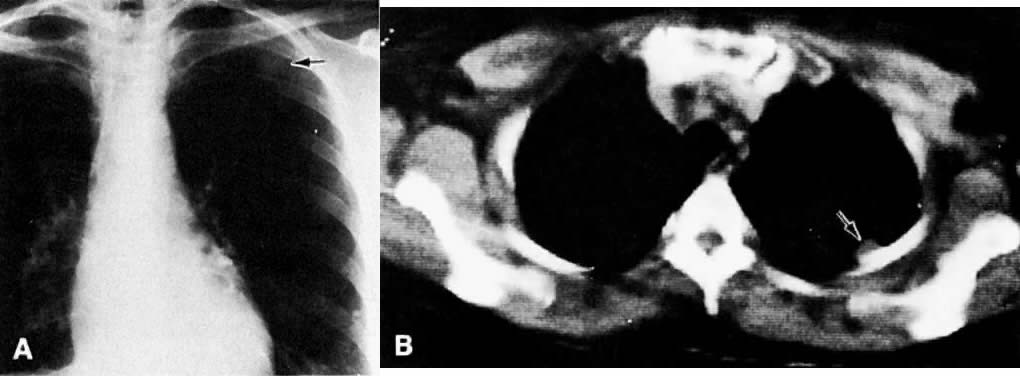
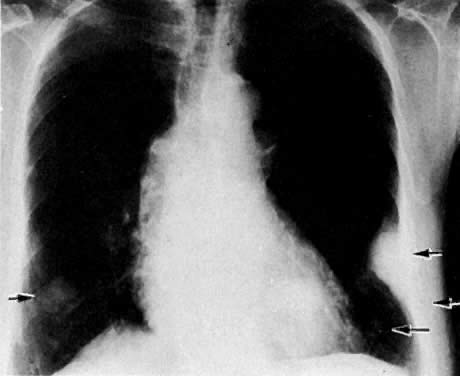
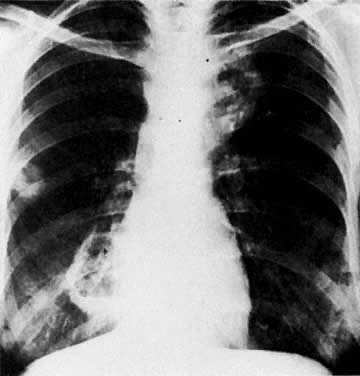
| Chest
X-ray Pneumonia Osteoporosis Ureteral Obstruction |
Bowel Obstruction Fistulas Metastases Hysterosalpingogram |
| Osteoporosis |
|
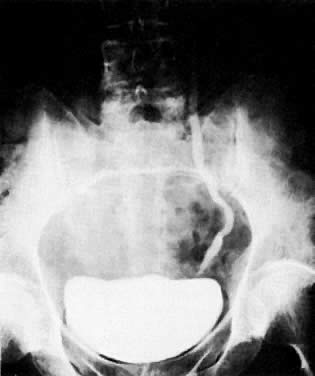
| Ureteral Obstruction |
|
|
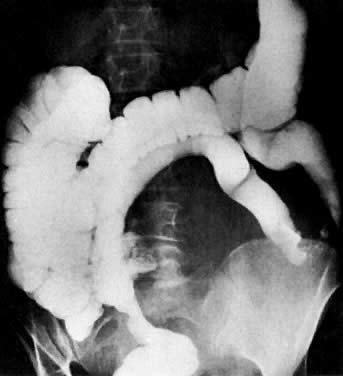
| Bowel Obstruction |
|
|
|
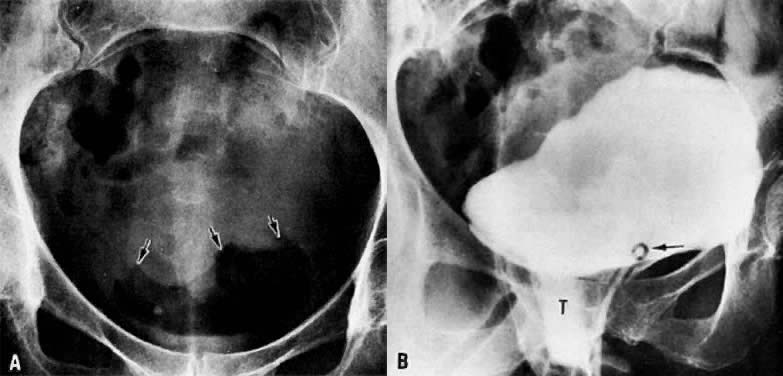
| Fistulas |
|
|
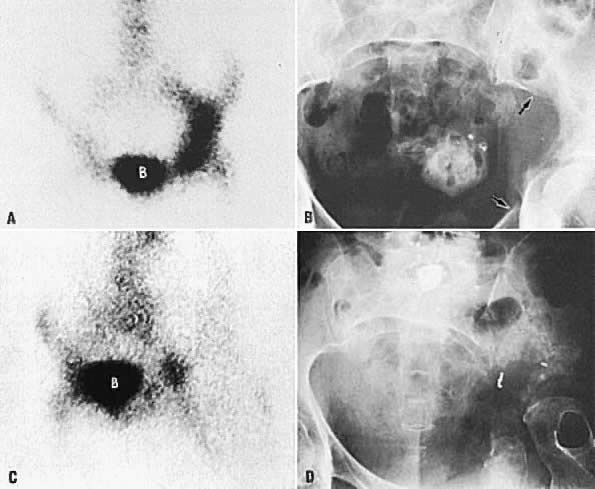
| Metastases |
|
|
|
|
|
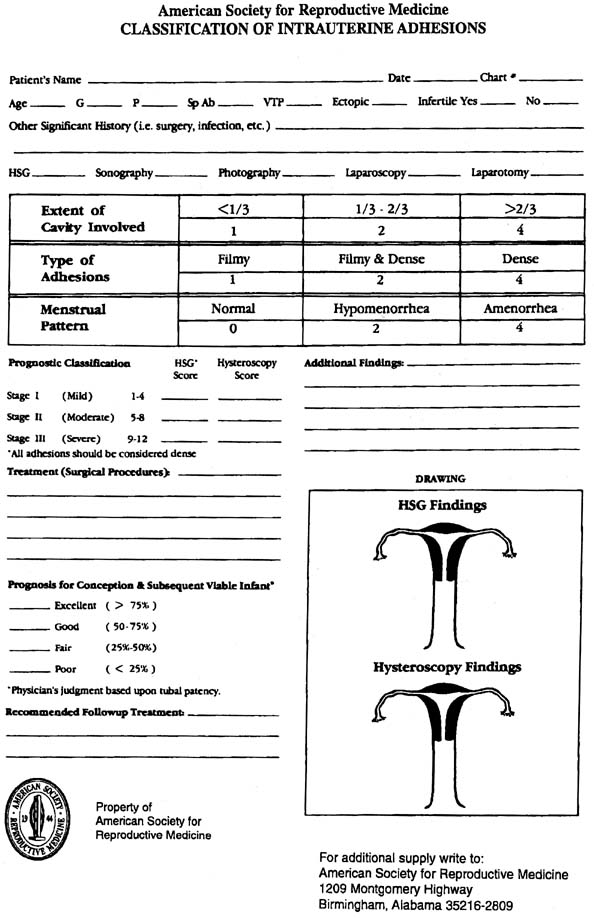
| Hysterosalpingogram |
|