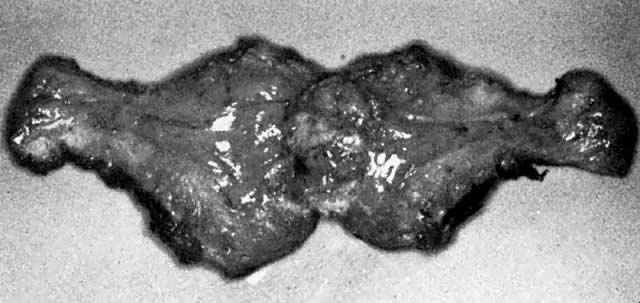
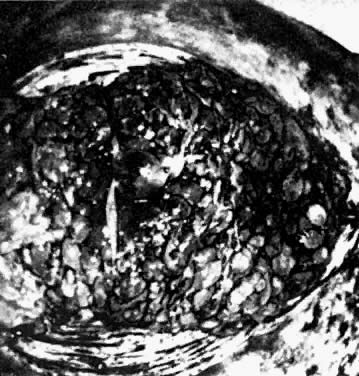
 Fig. 2. In situ hydatidiform mole in hysterectomy specimen. The dilated vesicles
are apparent. The outer membranes surrouding each of these vesicles
are made up of the trophoblastic layer. Volume 4, Chapter 48
Fig. 2. In situ hydatidiform mole in hysterectomy specimen. The dilated vesicles
are apparent. The outer membranes surrouding each of these vesicles
are made up of the trophoblastic layer. Volume 4, Chapter 48
|
Pathology Atlas: Gestational Trophoblastic Disease Michael John Hughey |
|
|
Michael John Hughey, MD |
|
Hydatidiform Mole Invasive Mole |
Partial Mole Choriocardinoma |
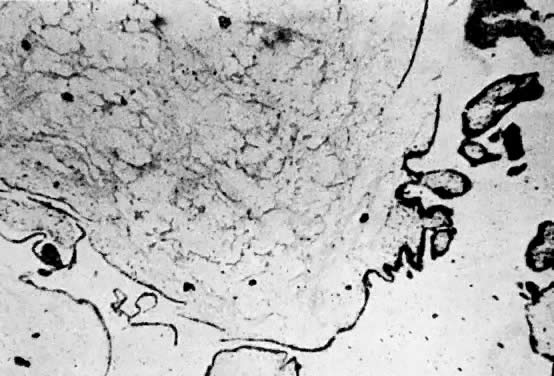
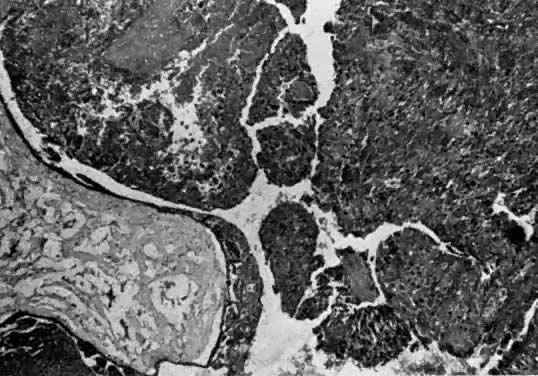
| Hydatidiform Mole |
|
|
|
|
Back to Top
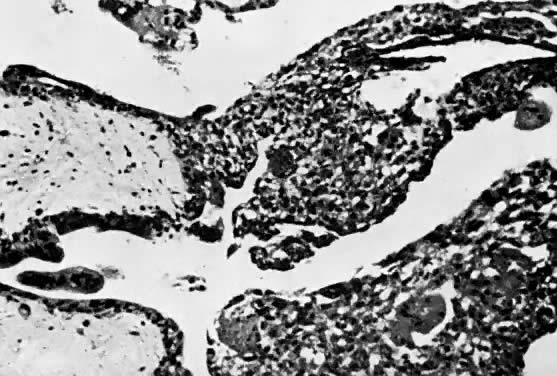
| Invasive Mole |
|
|
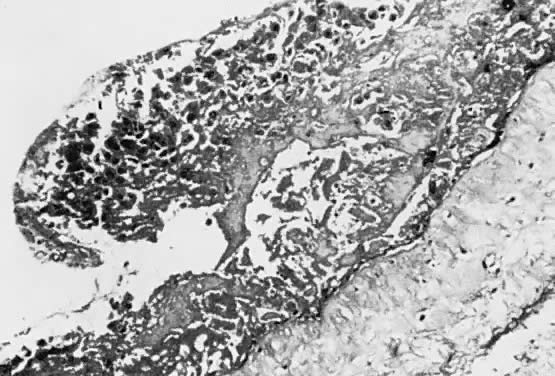
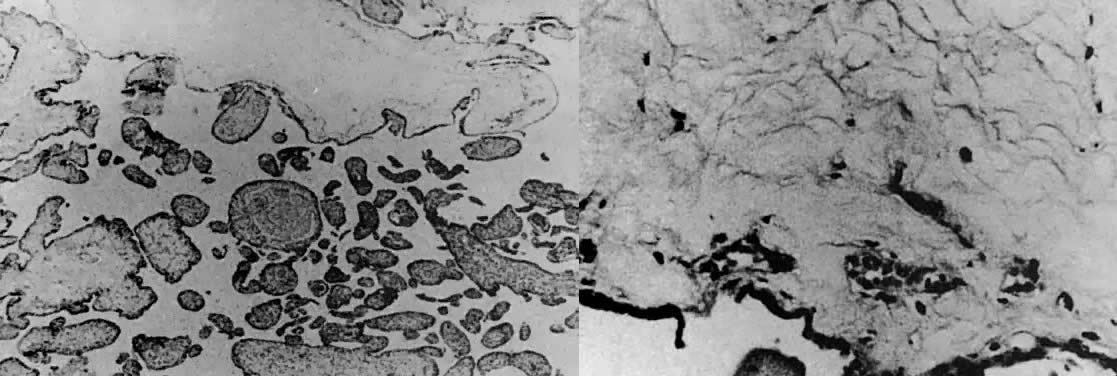
| Partial Mole |
|
|
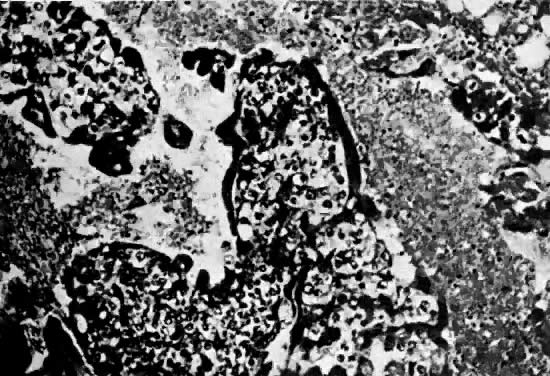
| Choriocarcinoma |
|
|