In the past gestational age was established by a combination of the historical information and the physical examination. Reliance was placed on the menstrual history and the maternal sensation of fetal movement (“quickening”). Other factors include assessment of uterine size by bimanual examination in the first trimester, initial detection of fetal heart tones by Doppler (10–12 weeks) or auscultation (19–21 weeks), and uterine fundal height measurement. However, both the history and the findings on physical examination are fraught with error, even in the best of circumstances (Table 1).6,7,8 It has been estimated that 20% to 40% of women cannot relate the LMP with certainty.6,7 Some of the reasons for this uncertainty include oligomenorrhea, metrorrhagia, bleeding in the first trimester of pregnancy, pregnancy following use of oral contraceptives or intrauterine devices, and becoming pregnant in the postpartum period. Hertz and co-workers9 reported that menstrual history was considered reliable in only 18% of women. In another report, even among women with known LMP, neonatal age assessment differed markedly from that assigned by certain menstrual dates in 15%.8 Physical examination also tends to be inaccurate, especially with advancing gestational age.10 Bimanual examination in the first trimester may be accurate within ±2 weeks; however, fundal height measurement, which is more commonly used to assess gestational age, is only accurate within ±4 to 6 weeks. Clearly, the inaccuracies of history and physical examination may limit their usefulness in assessment of gestational age. Methods that assess the time of ovulation or conception can accurately establish gestational age.11,12,13,14 Timed ovulation, either by basal body temperature recording or semiquantitative assessment of luteinizing hormone surge, predicts gestational age within ±4 to 6 days. Ovulation induction with agents such as clomiphene citrate and Pergonal, also accurately predicts gestational age. In vitro fertilization, with known date of conception, is likely the most accurate means of predicting gestational age (±1 day). However, in most pregnancies, the date of ovulation or conception cannot be as accurately predicted as outlined above and gestational age must be established by other methods.
TABLE 1.Clinical Predictors of Gestational Age
| Estimated Range for |
Parameter | 95% of Cases |
In vitro fertilization | ±1 day |
Ovulation induction | ±4–6 days |
Luteinizing hormone surge indicator | ±4–6 days |
Basal body temperature | ±4–6 days |
Certain menstrual history | ±2 weeks |
Bimanual examination (first trimester) | ±2 weeks |
First fetal heart tones by Doppler | ±2 weeks |
“Quickening” | ±2–4 weeks |
First fetal heart tones by auscultation | ±2–4 weeks |
Fundal height measurement between | ±4 weeks |
18 and 32 weeks' gestation |
|
Fundal height measurement after 32 | ±4–6 weeks |
weeks' gestation |
|
The advent of ultrasound has allowed a more direct means of assessing fetal structures and development. Measurements of a wide variety of parameters have been devised to establish gestational age. Ultrasound assessment of gestational age is feasible in a majority of pregnancies and may be used to establish gestational age with greater accuracy than physical examination. In the first trimester, gestational sac mean diameter and crown-rump length measurements have become the primary means of evaluating gestational age.15,16,17,18,19 In the second and third trimesters, fetal head, body, and extremity measurements have been commonly used to assess gestational age. Those parameters most commonly measured include biparietal diameter,20,21,22,23,24,25,26,27,28 head circumference,29,30 abdominal circumference,31,32,33,34,35 and femur length.36,37,38,39 Although numerous other parameters have been measured and related to gestational age, few offer any improvement in the accuracy of gestational age assessment.40,41,42,43,44,45,46 In this chapter, the most widely used and accepted ultrasound-derived fetal growth parameters are discussed and a review of their accuracies and potential errors is presented.
First-Trimester Assessment
In the first trimester, the gestational sac mean diameter and crown-rump length are used to establish fetal age. Both parameters are useful because each measures a different aspect of the first-trimester pregnancy and may be used at different times during the first trimester.
GESTATIONAL SAC MEAN DIAMETER.
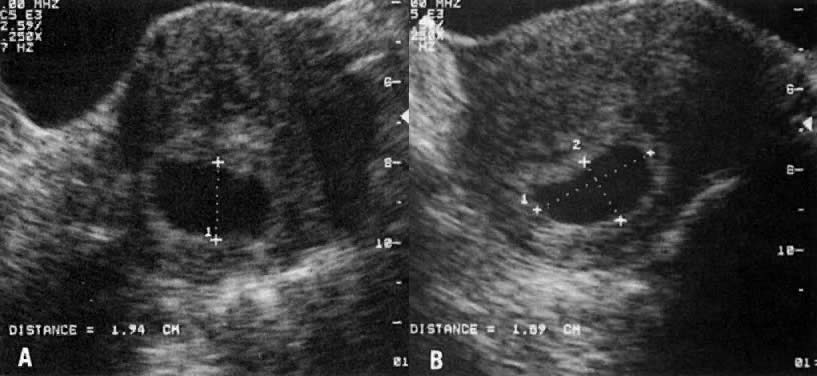
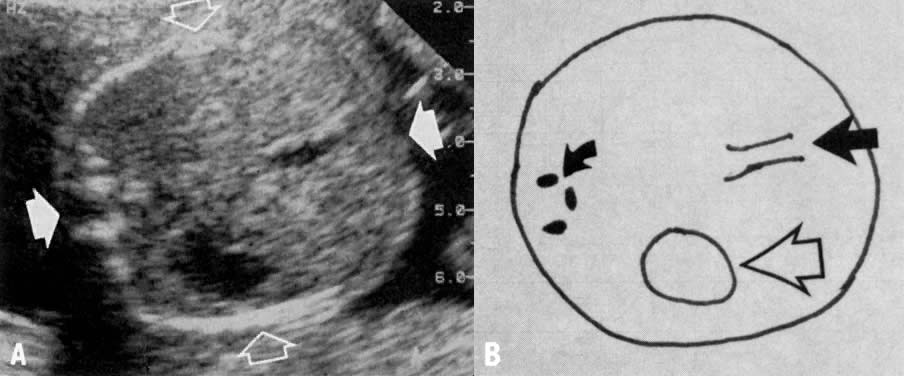
The gestational sac is the first identifiable structure routinely imaged in the first trimester. It is identified by transabdominal ultrasound as early as 5 weeks' gestation and may be seen as early as 4 weeks' gestation by transvaginal ultrasound.15,16,47 The gestational sac is an echo-free space containing the fluid, embryo, and extraembryonic structures. The sac is measured inside the hyperechoic rim, including only the echo-free space (Fig. 1). The gestational sac is imaged first in the longitudinal plane, obtaining long axis and anteroposterior measurements perpendicular to each other. Then, in the transverse plane at the level of the anteroposterior measurement, the width measurement is obtained. The three measurements are averaged to obtain the gestational sac mean diameter. Table 2 compares gestational ages from 5 to 12 weeks with the gestational sac mean diameters.15 The accuracy of gestational sac measurement as a predictor of gestational age has been evaluated in only one report and was found to be approximately ±1 week.16
TABLE 2. Gestational Sac Mean Diameter Measurements Relative to Gestational
Age
Gestational Sac | Gestational Age | Gestational Sac | Gestational Age |
Mean Diameter (mm) | (weeks) | Mean Diameter (mm) | (weeks) |
10 | 5.0 | 30 | 7.9 |
11 | 5.2 | 31 | 8.0 |
12 | 5.3 | 32 | 8.2 |
13 | 5.5 | 33 | 8.3 |
14 | 5.6 | 34 | 8.5 |
15 | 5.8 | 35 | 8.6 |
16 | 5.9 | 36 | 8.8 |
17 | 6.0 | 37 | 8.9 |
18 | 6.2 | 38 | 9.0 |
19 | 6.3 | 39 | 9.2 |
20 | 6.5 | 40 | 9.3 |
21 | 6.6 | 41 | 9.5 |
22 | 6.8 | 42 | 9.6 |
23 | 6.9 | 43 | 9.8 |
24 | 7.0 | 44 | 9.9 |
25 | 7.2 | 45 | 10.0 |
26 | 7.3 | 46 | 10.2 |
27 | 7.5 | 47 | 10.3 |
28 | 7.6 | 48 | 10.5 |
29 | 7.8 | 49 | 10.6 |
|
CROWN-RUMP LENGTH.
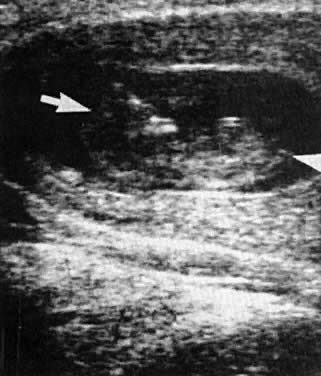
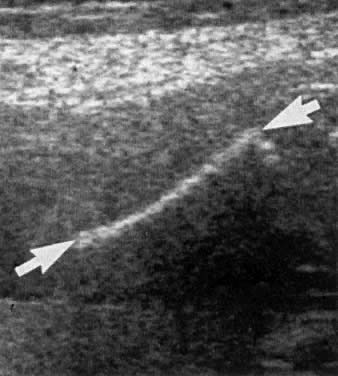
The crown-rump length (CRL) is a measurement of the embryo, usually identified at 6 to 7 weeks' gestation.17,48 The embryo is measured along its longest axis to obtain the CRL measurement (Fig. 2). Crown-rump length may be used to accurately date pregnancy between 7 and 13 weeks' gestation. The technique involves measurement of the fetal length from the tip of the cephalic pole to the tip of the caudal pole. The fetus should be at rest and assuming its natural curvature. At 5 to 6 weeks' gestation, distinct landmarks cannot always be identified but heart motion usually can be detected centrally. As the pregnancy continues, the head can be easily identified from the rest of the body. After 12 weeks' gestation excessive curvature of the fetus may lead to erroneous shortening of CRL measurement; therefore, other measurements, such as the biparietal diameter, should be used to estimate gestational age.
|
The correlation between sonographic CRL values and dates was first reported by Robinson and Fleming, who obtained CRLs in pregnancies of women with certain menstrual histories.17 Drumm and associates18 performed a similar study; however, their patients fulfilled more stringent dating criteria. These early studies suggested that gestational age assessment by CRL was extremely accurate, approaching ±3 to 4 days. Subsequent studies have suggested that the CRL is somewhat less accurate; however, the accuracy is still within ±5 to 7 days.49,50,51,52 Most recently, MacGregor and co-workers19 evaluated CRL measurements in pregnancies of women with known dates of ovulation and reported data that differed from those of the previous two studies. Table 3 summarizes the results of these three studies evaluating gestational age relative to CRL.
TABLE 3.Crown-Rump Length Measurements Relative to Gestational Age in Three
Studies
| MacGregor et | Robinson and | Drumm et |
Crown-Rump | alGestational Age | FlemingGestational Age | alGestational Age |
Length(cm) | (Weeks + Days) | (Weeks + Days) | (Weeks + Days) |
1.0 | 7 + 5 | 7 + 0 | 6 + 6 |
1.1 | 7 + 6 | 7 + 1 | 7 + 1 |
1.2 | 8 + 0 | 7 + 3 | 7 + 2 |
1.3 | 8 + 1 | 7 + 4 | 7 + 3 |
1.4 | 8 + 1 | 7 + 5 | 7 + 4 |
1.5 | 8 + 2 | 7 + 6 | 7 + 5 |
1.6 | 8 + 3 | 8 + 0 | 7 + 6 |
1.7 | 8 + 4 | 8 + 1 | 8 + 0 |
1.8 | 8 + 5 | 8 + 2 | 8 + 1 |
1.9 | 8 + 5 | 8 + 3 | 8 + 2 |
2.0 | 8 + 6 | 8 + 4 | 8 + 3 |
2.1 | 9 + 0 | 8 + 5 | 8 + 4 |
2.2 | 9 + 1 | 8 + 6 | 8 + 5 |
2.3 | 9 + 1 | 8 + 6 | 8 + 6 |
2.4 | 9 + 2 | 9 + 0 | 9 + 0 |
2.5 | 9 + 3 | 9 + 1 | 9 + 1 |
2.6 | 9 + 4 | 9 + 2 | 9 + 2 |
2.7 | 9 + 4 | 9 + 3 | 9 + 3 |
2.8 | 9 + 5 | 9 + 3 | 9 + 3 |
2.9 | 9 + 6 | 9 + 4 | 9 + 4 |
3.0 | 9 + 6 | 9 + 5 | 9 + 5 |
3.1 | 10 + 0 | 9 + 6 | 9 + 6 |
3.2 | 10 + 1 | 9 + 6 | 10 + 0 |
3.3 | 10 + 2 | 10 + 0 | 10 + 0 |
3.4 | 10 + 2 | 10 + 1 | 10 + 1 |
3.5 | 10 + 3 | 10 + 1 | 10 + 2 |
3.6 | 10 + 4 | 10 + 2 | 10 + 3 |
3.7 | 10 + 4 | 10 + 3 | 10 + 3 |
3.8 | 10 + 5 | 10 + 3 | 10 + 4 |
3.9 | 10 + 6 | 10 + 4 | 10 + 5 |
4.0 | 10 + 6 | 10 + 5 | 10 + 5 |
4.1 | 11 + 0 | 10 + 5 | 10 + 6 |
4.2 | 11 + 1 | 10 + 6 | 11 + 0 |
4.3 | 11 + 1 | 11 + 0 | 11 + 0 |
4.4 | 11 + 2 | 11 + 0 | 11 + 1 |
4.5 | 11 + 3 | 11 + 1 | 11 + 2 |
4.6 | 11 + 3 | 11 + 1 | 11 + 2 |
4.7 | 11 + 4 | 11 + 2 | 11 + 3 |
4.8 | 11 + 5 | 11 + 3 | 11 + 4 |
4.9 | 11 + 5 | 11 + 3 | 11 + 4 |
5.0 | 11 + 6 | 11 + 4 | 11 + 5 |
5.1 | 12 + 0 | 11 + 4 | 11 + 5 |
5.2 | 12 + 0 | 11 + 5 | 11 + 6 |
5.3 | 12 + 1 | 11 + 5 | 12 + 0 |
5.4 | 12 + 1 | 11 + 6 | 12 + 0 |
5.5 | 12 + 2 | 11 + 6 | 12 + 1 |
5.6 | 12 + 3 | 12 + 0 | 12 + 2 |
5.7 | 12 + 3 | 12 + 1 | 12 + 2 |
5.8 | 12 + 4 | 12 + 1 | 12 + 3 |
5.9 | 12 + 4 | 12 + 2 | 12 + 3 |
6.0 | 12 + 5 | 12 + 2 | 12 + 4 |
6.1 | 12 + 6 | 12 + 3 | 12 + 5 |
6.2 | 12 + 6 | 12 + 3 | 12 + 5 |
6.3 | 13 + 0 | 12 + 4 | 12 + 6 |
6.4 | 13 + 0 | 12 + 4 | 12 + 6 |
6.5 | 13 + 1 | 12 + 5 | 13 + 0 |
6.6 | 13 + 2 | 12 + 5 | 13 + 0 |
Variations in the measurement of CRL can be attributed to differences in fetal growth patterns. Such differences are related to factors similar to those that influence birth weight curves, including maternal age and parity, prepregnancy maternal weight, geographic location, and population characteristics.53,54,55 Indeed, the existence of subpopulations with altered CRL growth patterns has been suggested by previous reports.56,57 Technical factors can also lead to errors in CRL measurements. These include incorporation of the yolk sac or lower limbs in the CRL measurement, excessive curling or extension of the fetus, and tangential section of the trunk.17 Despite these potential sources of error, CRL measurement is an accurate and useful method of assessing gestational age in the first trimester.
Second- and Third-Trimester Assessment
BIPARIETAL DIAMETER.
The biparietal diameter (BPD) is one of the most commonly measured parameters in the fetus. Campbell was the first investigator to link fetal BPD to gestational age20; however, since this original report, numerous publications on this subject have appeared in the literature.20,21,22,23,24,25,26,27,28,58,59,60,61,62,63 The BPD may be rapidly and reproducibly measured by ultrasound examination from 12 weeks' gestation until the end of pregnancy. The BPD is imaged in the transaxial plane of the fetal head at a level depicting thalami in the midline, equidistant from the temporoparietal bones and usually the cavum septum pellucidum anteriorly (Fig. 3).58,59 Although several methods have been used to measure BPD, the most commonly accepted method is measurement from leading edge to leading edge (outer-to-inner) (see Fig. 3).
|
Gestational age assignment is based on the mean BPD; however, a single BPD encompasses a range of ages in which most fetuses of that size are most likely to fall (Table 4).23 The accuracy of fetal age assessment based on BPD is dependent on gestational age.22,23,27,28,51,58 Between 12 and 26 weeks' gestation, the BPD is accurate to within ±10 to 11 days. After 26 weeks' gestation, the accuracy of BPD measurement progressively decreases and is ±3 weeks near term. A number of factors may contribute to variation or inaccuracy in the BPD measurement. Biologic variation, for example, may occur because of differences in maternal age, parity, prepregnancy weight, geographic location, and specific population characteristics. Technical factors including interobserver error, different techniques of measurements, and single versus multiple measurements may likewise influence the accuracy of BPD in assessing gestational age.60,61,62 Although most dating curves show the same general relationship between BPD and gestational age, there are often significant differences in gestational age assignment for any particular BPD measurement. Furthermore, BPD measurement is most accurate in assessing gestational age when the head shape is appropriately ovoid. If the head is unusually rounded (brachycephalic) or unusually elongated (dolicocephalic), BPD measurements would overestimate or underestimate gestational age, respectively. To determine whether head shape is appropriate, Hadlock and co-workers64 compared the BPD and the frontooccipital diameter. The ratio of these diameters is called the cephalic index (CI), with a mean value of 0.78 and a normal range (±2 SD) of 0.70 to 0.86. In the fetus with an abnormal cephalic index (noted in <2% of fetuses prior to 26 weeks' gestation), dates may be estimated more accurately using other fetal parameters, such as head circumference.
TABLE 4. Biparietal Diameter Measurements Relative to Gestational Age
| Menstrual |
| Menstrual |
BPD (cm) | Age (weeks) | BPD (cm) | Age (weeks) |
2.6 | 13.6 | 6.4 | 25 |
2.7 | 13.8 | 6.5 | 25.3 |
2.8 | 14 | 6.6 | 25.7 |
2.9 | 14.2 | 6.7 | 26 |
3.0 | 14.4 | 6.8 | 26.3 |
3.1 | 14.7 | 6.9 | 26.7 |
3.2 | 15 | 7.0 | 27 |
3.3 | 15.2 | 7.1 | 27.3 |
3.4 | 15.4 | 7.2 | 27.7 |
3.5 | 15.7 | 7.3 | 28 |
3.6 | 16 | 7.4 | 28.3 |
3.7 | 16.3 | 7.5 | 28.7 |
3.8 | 16.7 | 7.6 | 29 |
3.9 | 17 | 7.7 | 29.4 |
4.0 | 17.3 | 7.8 | 30 |
4.1 | 17.7 | 7.9 | 30.4 |
4.2 | 18 | 8.0 | 31 |
4.3 | 18.3 | 8.1 | 31.4 |
4.4 | 18.7 | 8.2 | 32 |
4.5 | 19 | 8.3 | 32.3 |
4.6 | 19.3 | 8.4 | 32.7 |
4.7 | 19.7 | 8.5 | 33 |
4.8 | 20 | 8.6 | 33.4 |
4.9 | 20.3 | 8.7 | 34 |
5.0 | 20.7 | 8.8 | 34.6 |
5.1 | 21 | 8.9 | 35.3 |
5.2 | 21.3 | 9.0 | 36 |
5.3 | 21.6 | 9.1 | 36.4 |
5.4 | 21.8 | 9.2 | 37.3 |
5.5 | 22 | 9.3 | 37.7 |
5.6 | 22.3 | 9.4 | 39 |
5.7 | 22.7 | 9.5 | 40 |
5.8 | 23 | 9.6 | 40.3 |
5.9 | 23.3 | 9.7 | 40.7 |
6.0 | 23.7 | 9.8 | 41 |
6.1 | 24 | 9.9 | 41.7 |
6.2 | 24.3 | 10.0 | 42.3 |
6.3 | 24.7 |
|
|
HEAD CIRCUMFERENCE.
The head circumference (HC) measurement may be used to estimate gestational age in a similar manner to BPD measurement (Table 5).30 Although tracing of the outer perimeter of the head (by trackball on the ultrasonic equipment or by digitizer) is the most reliable means of measuring HC, the following formula using biparietal and fronto-occipital diameters may be used to calculate HC with a maximum error of 6%:63,65
TABLE 5.Head Circumference Measurements Relative to Gestational Age
Head | Menstrual | Head | Menstrual |
Circumference | Age | Circumference | Age |
(cm) | (weeks) | (cm) | (weeks) |
8.0 | 13.4 | 22.5 | 24.4 |
8.5 | 13.7 | 23.0 | 24.9 |
9.0 | 14.0 | 23.5 | 25.4 |
9.5 | 14.3 | 24.0 | 25.9 |
10.0 | 14.6 | 24.5 | 26.4 |
10.5 | 15.0 | 25.0 | 26.9 |
11.0 | 15.3 | 25.5 | 27.5 |
11.5 | 15.6 | 26.0 | 28.0 |
12.0 | 15.9 | 26.5 | 28.1 |
12.5 | 16.3 | 27.0 | 29.2 |
13.0 | 16.6 | 27.5 | 29.8 |
13.5 | 17.0 | 28.0 | 30.3 |
14.0 | 17.3 | 28.5 | 31.0 |
14.5 | 17.7 | 29.0 | 31.6 |
15.0 | 18.1 | 29.5 | 32.2 |
15.5 | 18.4 | 30.0 | 32.8 |
16.0 | 18.8 | 30.5 | 33.5 |
16.5 | 19.2 | 31.0 | 34.2 |
17.0 | 19.6 | 31.5 | 34.9 |
17.5 | 20.0 | 32.0 | 35.5 |
18.0 | 20.4 | 32.5 | 36.3 |
18.5 | 20.8 | 33.0 | 37.0 |
19.0 | 21.2 | 33.5 | 37.7 |
19.5 | 21.6 | 34.0 | 38.5 |
20.0 | 22.1 | 34.5 | 39.2 |
20.5 | 22.5 | 35.0 | 40.0 |
21.0 | 23.0 | 35.5 | 40.8 |
21.5 | 23.4 | 36.0 | 41.6 |
22.0 | 23.9 |
|
|

The accuracy of gestational age estimation by HC measurement is comparable with that of BPD measurement.30 However, in fetuses with abnormal head shape, either brachycephaly or dolicocephaly, HC may be a more accurate predictor of fetal age than BPD.30,65
ABDOMINAL CIRCUMFERENCE.
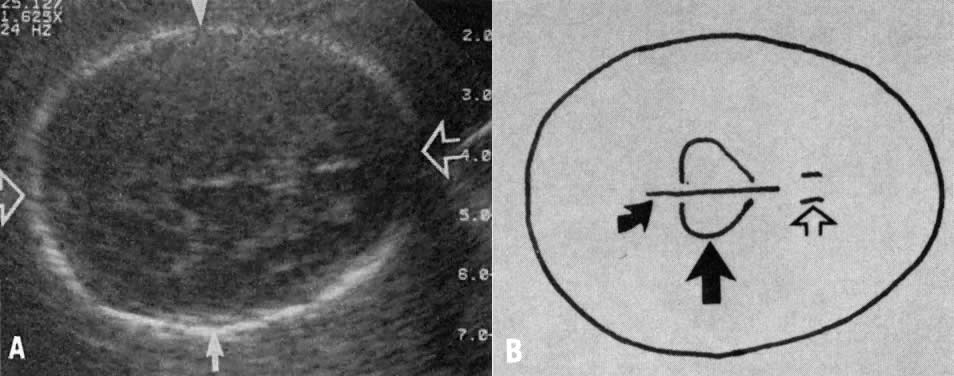
Measurement of the fetal abdominal circumference (AC) is obtained in the transaxial view of the fetal abdomen. The AC is measured at the level of the fetal liver, using the umbilical portion of the left portal vein as a landmark (Fig. 4). The fetal stomach is at the same level, which is slightly caudad to the fetal heart and cephalad to the kidneys. The AC measurement is taken from the outermost aspects of the fetal soft tissues. Measurement of the AC is performed in the same manner as that of the HC, that is, by (1) tracing the outer perimeter of the AC by the trackball on the ultrasonic equipment or by digitizer or (2) the same equation as for HC using transverse and anteroposterior diameters of the fetal abdomen. The AC may be used to estimate gestational age (Table 6) but is less accurate than head measurements (BPD or HC).33 Similar to head measurements, the accuracy of AC in estimating gestational age is greatest in the second trimester, with decreasing accuracy near term. Biologic variation and technical factors may contribute to the inaccuracy of AC measurements in a manner similar to that previously described for bi-parietal diameters. Of particular note, the abdominal circumference is the growth parameter most commonly affected in pregnancies complicated by abnormal fetal growth patterns.33 A macrosomic fetus will have increased AC relative to gestational age, and an asymmetrically growth-retarded fetus will have diminished AC measurements. Variation in AC measurements in macrosomic and growth-retarded fetuses is due to differences in liver size and width of subcutaneous tissue in these two types of abnormal growth patterns. Thus, estimation of gestational age by AC will lead to inaccuracies in fetuses displaying either of these growth patterns. However, the HC/AC ratio may be useful as a predictor of head-to-abdomen symmetry or asymmetry in order to identify the type of abnormal growth (Table 7).66
TABLE 6. Abdominal Circumference Measurements Relative to Gestational Age
Abdominal | Menstrual | Abdominal | Menstrual |
Circumference | Age | Circumference | Age |
(cm) | (weeks) | (cm) | (weeks) |
10.0 | 15.6 | 23.5 | 27.7 |
10.5 | 16.1 | 24.0 | 28.2 |
11.0 | 16.5 | 24.5 | 28.7 |
11.5 | 16.9 | 25.0 | 29.2 |
12.0 | 17.3 | 25.5 | 29.7 |
12.5 | 17.8 | 26.0 | 30.1 |
13.0 | 18.2 | 26.5 | 30.6 |
13.5 | 18.6 | 27.0 | 31.1 |
14.0 | 19.1 | 27.5 | 31.6 |
14.5 | 19.5 | 28.0 | 32.1 |
15.0 | 20.0 | 28.5 | 32.6 |
15.5 | 20.4 | 29.0 | 33.1 |
16.0 | 20.8 | 29.5 | 33.6 |
16.5 | 21.3 | 30.0 | 34.1 |
17.0 | 21.7 | 30.5 | 34.6 |
17.5 | 22.2 | 31.0 | 35.1 |
18.0 | 22.6 | 31.5 | 35.6 |
18.5 | 23.1 | 32.0 | 36.1 |
19.0 | 23.6 | 32.5 | 36.6 |
19.5 | 24.0 | 33.0 | 37.1 |
20.0 | 24.5 | 33.5 | 37.6 |
20.5 | 24.9 | 34.0 | 38.1 |
21.0 | 25.4 | 34.5 | 38.7 |
21.5 | 25.9 | 35.0 | 39.2 |
22.0 | 26.3 | 35.5 | 39.7 |
22.5 | 26.8 | 36.0 | 40.2 |
23.0 | 27.3 | 36.5 | 40.8 |
TABLE 7. Head Circumference to Abdominal Circumference Ratios Relative
to Gestational Age
Gestational Age | HC/AC Ratio | ||
(weeks) | 5th percentile | Mean | 95th percentile |
13–14 | 1.14 | 1.23 | 1.31 |
15–16 | 1.05 | 1.22 | 1.39 |
17–18 | 1.07 | 1.18 | 1.29 |
19–20 | 1.09 | 1.18 | 1.26 |
21–22 | 1.06 | 1.15 | 1.25 |
23–24 | 1.05 | 1.13 | 1.21 |
25–26 | 1.04 | 1.13 | 1.22 |
27–28 | 1.05 | 1.13 | 1.22 |
29–30 | 0.99 | 1.10 | 1.21 |
31–32 | 0.96 | 1.07 | 1.17 |
33–34 | 0.96 | 1.04 | 1.11 |
35–36 | 0.93 | 1.02 | 1.11 |
37–38 | 0.92 | 0.98 | 1.05 |
39–40 | 0.87 | 0.97 | 1.06 |
41–42 | 0.93 | 0.96 | 1.00 |
|
FEMUR LENGTH.
All the fetal long bones can be adequately examined and measured by ultrasound; however, the femur is the largest of the long bones, least moveable, and easiest to image. The femur may be adequately visualized from 14 weeks' gestation until delivery.38,39,40,67,68,69,70,71,72,73,74 It is measured along the long axis of the bone; a straight measurement of the osseous portion is taken from one end to the other, disregarding bone curvature (Fig. 5). The femoral neck and both proximal and distal epiphyseal cartilages are excluded from the measurement. Femur length (FL) measurements may be used to accurately predict gestational age between 14 weeks' gestation and term (Table 8).39 Most observers consider the accuracy of the FL and BPD measurements to be similar in the third trimester. Although there is controversy regarding the accuracy of the FL prior to 26 weeks' gestation,38,39 the accuracy of gestational age prediction based on FL is greatest in the second trimester and least near term.
TABLE 8. Femur Length Measurements Relative to Gestational Age
Femur | Menstrual | Femur | Menstrual |
Length | Age | Length | Age |
(cm) | (weeks) | (cm) | (weeks) |
1.0 | 12.8 | 4.5 | 24.5 |
1.1 | 13.1 | 4.6 | 24.9 |
1.2 | 13.4 | 4.7 | 25.3 |
1.3 | 13.6 | 4.8 | 25.7 |
1.4 | 13.9 | 4.9 | 26.1 |
1.5 | 14.2 | 5.0 | 26.5 |
1.6 | 14.5 | 5.1 | 27.0 |
1.7 | 14.8 | 5.2 | 27.4 |
1.8 | 15.1 | 5.3 | 27.8 |
1.9 | 15.4 | 5.4 | 28.2 |
2.0 | 15.7 | 5.5 | 28.7 |
2.1 | 16.0 | 5.6 | 29.1 |
2.2 | 16.3 | 5.7 | 29.6 |
2.3 | 16.6 | 5.8 | 30.0 |
2.4 | 16.9 | 5.9 | 30.5 |
2.5 | 17.2 | 6.0 | 30.9 |
2.6 | 17.6 | 6.1 | 31.4 |
2.7 | 17.9 | 6.2 | 31.9 |
2.8 | 18.2 | 6.3 | 32.3 |
2.9 | 18.6 | 6.4 | 32.8 |
3.0 | 18.9 | 6.5 | 33.3 |
3.1 | 19.2 | 6.6 | 33.8 |
3.2 | 19.6 | 6.7 | 34.2 |
3.3 | 19.9 | 6.8 | 34.7 |
3.4 | 20.3 | 6.9 | 35.2 |
3.5 | 20.7 | 7.0 | 35.7 |
3.6 | 21.0 | 7.1 | 36.2 |
3.7 | 21.4 | 7.2 | 36.7 |
3.8 | 21.8 | 7.3 | 37.2 |
3.9 | 22.1 | 7.4 | 37.7 |
4.0 | 22.5 | 7.5 | 38.3 |
4.1 | 22.9 | 7.6 | 38.8 |
4.2 | 23.3 | 7.7 | 39.3 |
4.3 | 23.7 | 7.8 | 39.8 |
4.4 | 24.1 | 7.9 | 40.4 |
|
Biologic variation may lead to inaccuracies of FL measurements in a manner similar to that of the other fetal growth parameters. In addition, several technical factors are potential sources of error in the measurement of the femur.67,70,72 Sector ultrasound imaging may lead to overestimation of FL, particularly when the femur is in the far field or lateral margins of the image. Linear-array ultrasound imaging provides more accurate measurements of FL. In addition, FL measurements obtained in the axial plane (parallel to the ultrasonic beam) have less mean absolute error than those obtained in the lateral plane, perpendicular to the ultrasonic beam (1.7 mm vs. 3.7 mm, respectively).74 Tangential section of the femur, failing to visualize the entire length of the shaft, leads to underestimation of FL and, therefore, of gestational age. Artifactual bowing of the femur may also occur on ultrasound imaging and lead to a shortened FL measurement. The distal femoral epiphysis becomes echogenic in the third trimester and is separated from the distal end of the diaphysis, the osseous portion of the shaft. Inclusion of the distal epiphysis will falsely overestimate FL.67,68
Gestational age assessment by FL is particularly useful when head measurement is difficult to obtain due to fetal position. The femur length may also be compared with the biparietal diameter (FL/BPD) as an age-independent ratio.73 The FL/BPD ratio (normal values 79 ± 6%) is useful as an internal verification of the measurements obtained, as well as an indicator of pathologic entities, such as microcephaly (FL/BPD abnormally high) and hydrocephalus or short-limb dysplasia (FL/BPD abnormally low). Although the femur length and abdominal circumference (FL/AC) have also been compared in order to diagnose fetal growth abnormalities (macrosomia and fetal growth retardation),34 there is much overlap between normal and abnormal values of this ratio.75,76,77,78
 90th percentile); average (10th to 90th percentile); and small (
90th percentile); average (10th to 90th percentile); and small ( 10th percentile). Paired BPD measurements obtained at different gestational
ages allows categorization of the specific cephalic growth pattern. The
first measurement should be obtained between 20 and 26 weeks' gestation, and
the second measurement should be obtained between 30 and 33 weeks' gestation. The
first BPD measurement will not distinguish the
fetus with large, average, or small BPD growth, and, therefore, the
fetus is assigned a mean gestational age based on an assumed average
BPD growth pattern. The second BPD measurement identifies the specific
type of growth pattern. For example, in the fetus with average growth
the second BPD measurement will fall between the 10th and 90th percentiles, confirming
the gestational age assignment from the first BPD measurement. In
contrast, BPD growth in the small-for-gestational age fetus
will follow a slow growth pattern and the second BPD measurement will
be less than or equal to the 10th percentile for the gestational age
assigned by the first BPD. Since the first BPD measurement failed to
recognize the small growth pattern and, therefore, underestimated gestational
age, the second measurement allows the gestational age assessment
to be adjusted based on the BPD growth pattern. Such a fetus with
a slowed growth pattern would have the gestational age advanced by 1 week
at the time of the second BPD measurement. Similarly, dates in the
large-for-gestational age fetus may be adjusted by GASA at the time
of the second BPD measurement, decreasing gestational age assignment
by 1 week if the BPD measurement is greater than or equal to the 90th
percentile (
10th percentile). Paired BPD measurements obtained at different gestational
ages allows categorization of the specific cephalic growth pattern. The
first measurement should be obtained between 20 and 26 weeks' gestation, and
the second measurement should be obtained between 30 and 33 weeks' gestation. The
first BPD measurement will not distinguish the
fetus with large, average, or small BPD growth, and, therefore, the
fetus is assigned a mean gestational age based on an assumed average
BPD growth pattern. The second BPD measurement identifies the specific
type of growth pattern. For example, in the fetus with average growth
the second BPD measurement will fall between the 10th and 90th percentiles, confirming
the gestational age assignment from the first BPD measurement. In
contrast, BPD growth in the small-for-gestational age fetus
will follow a slow growth pattern and the second BPD measurement will
be less than or equal to the 10th percentile for the gestational age
assigned by the first BPD. Since the first BPD measurement failed to
recognize the small growth pattern and, therefore, underestimated gestational
age, the second measurement allows the gestational age assessment
to be adjusted based on the BPD growth pattern. Such a fetus with
a slowed growth pattern would have the gestational age advanced by 1 week
at the time of the second BPD measurement. Similarly, dates in the
large-for-gestational age fetus may be adjusted by GASA at the time
of the second BPD measurement, decreasing gestational age assignment
by 1 week if the BPD measurement is greater than or equal to the 90th
percentile (