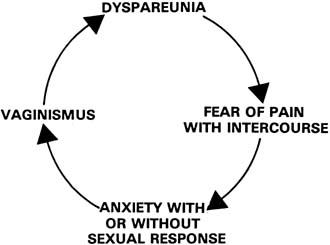
Many patients with symptoms of vaginismus and dyspareunia are seen for
gynecologic consultation. It is important that the consultant recognize
that this is a couple problem. Although much can be accomplished in an office consultation with
the woman alone, the true impact of the symptom or symptoms cannot
be assessed without an assessment of the couple. Similarly, the division
of couple therapy into either relationship or sexual is artificial
and anachronistic.20 The split between viewing this symptom as an individual problem or a couple
problem is anachronistic because it represents our traditional approach
to treating gynecologic symptoms as purely somatic symptoms. Similarly, the
split between relationship therapy and sexual therapy is
anachronistic because it is representative of the alienation that has
existed throughout the Western world between sexuality and personality
in an individual. Proper assessment of these problems begins with a problem-based
approach to history taking and includes a review of the onset and evolution
of the problem to its present state. This review will help determine
the impact of the problem on the patient and her partner, both functioning
as individuals, and as a couple. The problem-solving
approach highlights the couple's intellect, insight, and motivation. A
review of the evolution of the problem will identify the timing
of events and their effect on the patient's sexual response and will
uncover other attempts at therapy. The general principles of assessment include reviews of both individual
and relationship factors, both sexual and nonsexual. For example, it
is important to determine the extent to which a young woman's dyspareunia
is a function of her performance anxiety with her partner or
to what extent it is indicative of a general lack of sexual comfort and
competence. Primary vaginismus, resulting in nonconsummation, may be
the one method of birth control in which this woman has faith, a functional dysfunction as it were. Similarly, a woman with the symptoms of vaginismus may be
locked in a struggle for control with her partner, making treatment of
the presenting symptom pointless unless the relationship problem is resolved. During the assessment, the physician needs to make a distinction between
a sexual or relationship factor and a problem as identified or experienced
by the patient or her partner. For example, during assessment, a
woman with vaginismus may be found to have an inhibition about touching
her own genitals. This is a factor neither she nor her partner perceived
to be related in any way to the presenting problem. During the
assessment, the therapist must help the couple discover connections between
the two. Two final questions in the general assessment include: (1) who
owns the problem and (2) what is the couple's
motivation for treatment? Individual Assessment Individual factors that require some consideration and assessment include
intrapersonal, sexual socialization, gender role socialization, and
biologic factors (Table 1). While all physicians will not have the skills of an experienced
dynamically oriented psychotherapist in assessing intrapersonal factors, it
is important that they have some ability to understand and assess
these factors. Table 1. Individual Factors in the Assessment of Dyspareunia and Vaginismus
| Intrapersonal |
| Autonomy |
| Competence |
| Self-esteem |
| Comfort with affect |
| Mental status |
| Sexual Socialization |
| Knowledge |
| Attitudes toward sexual and sensual pleasure |
| Gender Role Socialization |
| Biologic |
| Organic disease (direct) |
| Organic disease (indirect) |
| Treatment of organic disease | The intrapersonal factors to be assessed are autonomy, competence, self-esteem, comfort
with affect, and mental status. A truly autonomous
adult can function separately both from her partner and from her
parents. A sense of competence refers to the subjective side of one's
actual competence and refers to one's inner sense of mastery. A
patient's self-esteem would include a sense of competence
and a perception of being loved and cherished. Comfort with affect
refers to the ability to discriminate among internal affective states, to
label them appropriately, and to express them in words that lead
to open, honest, interpersonal communication. Assessment of mental status
would include the detection of gross abnormalities in mental functioning, such
as organic brain disease, severe mood disorder, weight loss, abnormally
elated or depressed affect, or psychosis. Sexual socialization requires an assessment of the vertical factors operating
in the family that include “all the family's attitudes, taboos, expectations, labels, and loaded issues with which people
grow up.”20 These institutionalized forces in society work largely through the family
to help shape adult behavior. The two factors requiring assessment
in the area of sexual socialization include: (1) sexual knowledge
and myths and (2) attitudes toward sensual and sexual
pleasure. It is evident that many people live and grow in an environment
of sexual ignorance. In the absence of adequate and systematic sex
education, children invent their own explanations for biologic and sexual
processes, often in the form of mythologies. In addition, in contemporary
society, myths are generated by the authoritarian pronatalist
sex code, sometimes disguised as psychological concepts. Myths of vaginal
orgasm and simultaneous coital orgasm are just two examples of myths
promoted as goals of normal sexual functioning. Attitudes toward sensual
and sexual pleasure emphasize coital performance and de-emphasize
the value of general body pleasure. Gender role socialization refers to a person's learned or cultural
status or one's sense of self as male or female. It includes the
collective body of attitudes and behaviors that a culture considers appropriate
for males or females. Biologic factors include any organic disorder that directly affects the
endocrine, vascular, and neurologic components of human sexual response. Dermatologic
conditions can affect the epithelium of the vulva, vestibule, and
vagina, causing painful lesions (provoked or unprovoked). These ulcers and erosions of the genital tract can be caused by infections, such
as Candida or herpes, or can be dermatoses such as lichen sclerosus, lichen
planus, Becet's, aphthosis, or contact dermatitis. All
of these erosions and ulcers can cause pain with coital contact (dyspareunia) or
result in pain from anticipatory vaginismus. Secondarily, biologic
factors can affect sexual function indirectly, or
the treatment of an organic problem itself may affect the expression
of sexuality. For example, surgical procedures can directly affect
the nerve supply to the pelvis, or they can indirectly affect sexual function
through an altered body image, with loss of self-esteem
to the point at which a woman no longer sees herself as a sexually attractive
individual. A large number of drugs have shown to affect sexual
appetite, and they function either by central mechanisms or by a direct
effect on the neurologic and vascular components of the genital response. Couple Assessment The interaction among relationship and sexual factors in the production
of problems in a couple is complex (Table 2). Relationship factors include an assessment of the level of communication, the
ability to negotiate, and the degree of mutual support. These
factors can be viewed in terms of interpersonal skills, which can
be taught and learned. Assessment of these factors will identify skill
deficits, and therapy will possibly help couples correct them to ensure
continued symptomatic relief of the dyspareunia or vaginismus. Table 2. Couple Factors in the Assessment of Dyspareunia and Vaginismus
| Relationship Factors |
Sexual Factors |
| Communication |
Function |
| Negotiation |
Range of behaviors |
| Support |
Satisfaction |
| |
Experience with reproduction |
Sexual factors in the assessment include function, range of behaviors, and
satisfaction as well as plans and experiences with reproduction. Although this assessment may appear to be long and complex, an experienced
physician interested in sexual symptoms can assess these factors in
a relatively short time and obtain the necessary information on which
to base a rational approach to therapy. Pelvic Assessment Assessing dyspareunia is not complete until a pelvic examination has been
performed. Relaxation is the key factor in a successful genital examination, both
for the patient and the doctor. It is likely that most
women undergoing pelvic examination feel that this experience is an involuntary
intrusion into their lives and bodies. Although the patient
intellectually consents to her examination to benefit from a complete
assessment, at best, her emotional consent is ambivalent; at worst, her
emotional consent is fearful and revulsive. The physician's ability
to make the patient comfortable and demonstrate a high level of clinical
skill helps to generate a sense of relaxation. A vital factor
in a successful pelvic examination is an acknowledgment of the patient's
vulnerability in the power relationship between the physician
and the patient.21 If the doctor is unaware, insensitive, or unwilling to acknowledge the
patient's vulnerability in this relationship, the examination will
not be an educational opportunity and much clinical data will be lost. A careful pelvic examination allows the physician to assess physiologic
and pathologic factors on the spot. Visual, colposcopic, speculum, bimanual, and
rectovaginal examination provide a detailed assessment of
the genital tract and pelvis and provide an opportunity to confirm the
source of the patient's pain. The cotton swab test of vulva or vagina
allows focused exploration to identify an exact source of discomfort. Through
the use of a hand mirror and diagrams, the physician can
help the patient to be better-informed about her anatomy and physiology
and generate the concept of a three-dimensional view
of her pelvis. A digital examination will clarify the possible role of
vaginismus in dyspareunia and, if present, allow for an assessment of
the degree of vaginismus (Table 3).22 Table 3. Classification of Degrees of Vaginismus
| Classification and Degree |
No. of Patients (80) |
| First degree; perineal and levator spasm—relieved
with reassurance |
27 |
| Second degree: perineal spasm—maintained throughout
pelvis |
21 |
| Third degree: levator spasm and elevation of buttocks |
18 |
| Fourth degree: levator and perineal spasm, elevation;
adduction and retreat |
10 |
| Refused examination |
04 |
If both the individual and the couple assessment strongly suggest a physical
cause of the dyspareunia, the patient may be enlisted in self-examination
to help identify a specific source of pain. A sexologic
examination is useful in patients who have sexual concerns and understand
the goals of this examination. This examination is performed on
a patient, with or without her partner present, to assess the health
of the genital tract and provide an educational opportunity for the patient
regarding the genitals, their function, and the nature of her problem. The
patient's participation in the examination is encouraged
to capitalize on this educational experience to help clarify the location, or
source, of the pain and to observe the patient's reaction
to, and interest in, her own body. |