
Cesarean Hysterectomy
Authors
INTRODUCTION
The concept behind cesarean hysterectomy dates back to descriptions of the procedure on laboratory animals from the mid 1700s. In 1869, Storer performed the first cesarean hysterectomy in the US. Soon thereafter, Porro of Milan described the first cesarean hysterectomy performed to control uterine hemorrhage and prevent peritonitis, in which the infant and mother survived; the procedure is frequently referred to as the Porro operation in his honor.1, 2 At the end of the 19th century, a German gynecologist, Max Sanger, introduced sutural closure of the uterus in cesarean deliveries to try and avoid cesarean hysterectomy. This represented a major turning point in the cesarean technique, and it contributed to a significant reduction in hemorrhage and infection, which in turn resulted in a major decline in maternal mortality. However, despite further advances, Porro’s operation is still required in select circumstances, and this chapter examines the incidence and reasons for cesarean hysterectomy, the technique and possible complications. In updating this chapter (from the previous 2007 version), a review of the literature has been performed and more recent data presented.
INCIDENCE AND INDICATIONS
Cesarean hysterectomy may be classified as emergent, indicated non-emergent, and for elective sterilization. Each of these categories presents different management problems for the obstetric surgeon.3
The classic historical indications for emergency cesarean hysterectomy are life-threatening hemorrhage and infection. The advent of broad-spectrum antibiotics, along with improved pharmaceutical therapy and procedures for controlling hemorrhage (e.g. embolization, B-Lynch suture), has resulted in a decline in the incidence of emergent cesarean hysterectomy. Currently, most cesarean hysterectomies are performed for recalcitrant hemorrhage.
In a previous version of this chapter, the authors presented data from a series of 145 cases from Louisiana State University Hospital, from 1975 through 1985. The most common indications for cesarean hysterectomy in that series were abnormal placentation or abruption. Uterine rupture and placenta accreta, particularly previa with accreta, have been encountered with increasing frequency in recent years as the number of cesarean sections and attempted vaginal deliveries after cesarean section increases.4, 5, 6 Whilst the use of radiologic embolization procedures has become an important tool for the obstetric surgeon and may serve a critical role in the patient with persistent bleeding after surgery,7, 8, 9 cesarean hysterectomy is still frequently required in cases of placenta accreta, increta, and percreta.10
Table 1. Indications for cesarean hysterectomy at Louisiana State University Service – Charity Hospital of New Orleans, 1975–1985 (n = 145)
| Emergency cases (32% of total) | Indicated nonemergencies (31% of total) | Elective sterilization (37% of total) |
|
Placental problems Uterine rupture (7%) Postpartum atony (5%) Extension of cesarean Infection (6%) Chorioamnionitis with
| Leiomyomata uteri (10%) Cervical intraepithelial neoplasia (10%) Adnexal disease (3%)
|
Primary elective sterilization (17%)
|
In comparison, Table 2 shows data from a series of 318 cases of cesarean hysterectomy from 2005 to 2006, covering 229 hospitals throughout the UK.11 This gave an incidence of 4.1 per 10,000 women delivering. There were no cases performed for elective sterilization, and only three cases would have been classified as “nonemergent indicated” (all were for the management of malignancy). The remaining 315 cases were performed for the management of hemorrhage, the causes of which are listed.
Table 2 Indications for cesarean hysterectomy in the United Kingdom (2005–2006). (From Knight et al. Cesarean delivery and peripartum hysterectomy. Obstet Gynecol 2008;111:97-105)
| Emergency (n = 315) | Nonemergent (n = 3) |
| Uterine atony (53%) Morbidly adherent placenta (39%) Uterine rupture (8%) Extension of uterine incision at delivery (6%) Other (5%) | Cervical cancer (66%) Ovarian cancer (33%)
|
Knight et al.11 investigated the number and type of previous deliveries in women subsequently requiring a cesarean hysterectomy. They showed that there was a 1:30,000 chance if undergoing first vaginal delivery, 1:1700 chance if undergoing first cesarean delivery, rising to as much as a 1:220 risk in a woman who had had two or more cesarean deliveries. A further significant risk factor was maternal age over 35, and parity of three or greater. In view of the increasing cesarean delivery rates, and rising maternal age at childbirth (those over 35 have increased from 10 to 20% of all births in the past 10 years), these results may have significant implications for future service planning. It may also influence the counseling that is given to women regarding delivery by cesarean section, particularly those performed for “maternal request”.
In a prospective observational study, 46% of cesarean hysterectomies occurred in patients at gestations of less than 37 weeks, and nearly 50% of those were carried out for abnormal placentation.12 With this in mind, it is recommended that all women with previous uterine surgery (most commonly cesarean section, but occasionally myomectomy) should undergo ultrasound assessment of placentation in the third trimester.13
It is difficult to ascertain the role of infection in the decision to proceed to hysterectomy from the UK case series.11 In a systematic review of cesarean hysterectomies (including 981 cases from 24 articles in a literature review conducted up to August 2009), infection accounted for only 1% of cases.14
Flood et al.15 performed a retrospective cohort study between 1966 and 2005 from three maternity units in Dublin, Ireland, to identify changing trends in the indication for cesarean hysterectomy. Uterine rupture decreased as an indication from 40.5 to 9.3%, whilst placenta accreta increased significantly from 5.4 to 46.5% during the study period. From 1986 onwards, there were no “elective” cases of cesarean hysterectomy performed (e.g. for sterilization, or dysfunctional uterine bleeding), but 16% of cases were for management of cancer.
Nonemergent indicated cesarean hysterectomies are considered by some to be controversial. It is the current policy to consider cesarean hysterectomy for patients who have a valid obstetric indication for cesarean section and a concurrent valid indication for hysterectomy, e.g. genital tract malignancy. In the US, leiomyomas (fibroids) may be considered to be an indication for nonemergent cesarean hysterectomy.
Small fibroids commonly regress in size after pregnancy and seldom require cesarean hysterectomy for their management. However, some patients have multiple large fibroids that can obstruct the pelvic outlet. Others can experience painful degeneration of fibroids. Such patients may be best served by an operation that accomplishes both delivery and definitive treatment of their symptomatic fibroids. This is not common practice in the UK, and prenatal management of fibroids is a more common scenario, by either myomectomy or embolization. However, there is potentially a small increased risk of cesarean hysterectomy in those with previous myomectomy, due to abnormal placentation.11
Squamous intraepithelial lesions of the cervix have been proposed as an indication for cesarean hysterectomy. During pregnancy, it can be difficult to adequately evaluate the endocervical canal, and the physiologic changes in the cervical epithelium make it difficult for the cytologist to evaluate the condition. Occasionally, dysplastic or malignant changes may progress in the interval between initial diagnosis and delivery; staging of the disease process may then be inaccurate and lead to inappropriate therapy. Of added importance is the sometimes difficult removal of the entire cervix at the time of cesarean hysterectomy. Despite these concerns, there are cases in which cesarean hysterectomy or radical cesarean hysterectomy may be the best management plan, as they can provide definitive, curative therapy for these persistent and potentially evolving lesions.
The most controversial indication for cesarean hysterectomy is elective sterilization. In a multiparous patient who desires permanent sterility and is undergoing a repeat cesarean section, it could be argued that cesarean hysterectomy may be an appropriate option. When surgical sterilization alone is the indication, cesarean section followed by a tubal ligation is a far safer procedure than cesarean hysterectomy. Although a comprehensive review indicates that 17% of women undergoing postpartum sterilization ultimately undergo hysterectomy,16cesarean section and desire for sterilization alone do not warrant cesarean hysterectomy.17, 18, We identified no reported cases in the UK medical literature where cesarean hysterectomy was performed for this indication in the past 20 years.
SURGICAL PITFALLS
The physiologic changes in the maternal pelvis that accompany pregnancy are responsible for many of the surgical challenges of cesarean hysterectomy. The vessels that supply the uterus, ovaries, and bladder are substantially larger and more tortuous in pregnancy than they are in the nonpregnant state. Meticulous care in the manipulation of clamps, cutting of pedicles, and placement of sutures is required to prevent severe bleeding. Edema of the structures surrounding the uterus allows easy dissection of surgical planes but produces large pedicles from which blood vessels may escape. Special attention must be given to the proper size of pedicles and careful hemostatic suturing techniques.
Scarring from previous surgery, particularly previous cesarean sections, is a common complicating feature of cesarean hysterectomy. Great care is necessary to avoid injury to organs that are adherent to the uterus, bladder, adnexa, and abdominal wall. The surgeon must be prepared to recognize and repair injuries of the urinary tract. Cesarean hysterectomy is often performed in the presence of uterine trauma or rupture in which hematomas of the broad ligament and neighboring structures make visualization difficult and distort anatomic relations. Careful exposure, skilled assistants, and attention to hemostasis are of primary importance.17
Guidelines in the UK recommend that the decision for hysterectomy should be made by an experienced and senior physician, and the decision should ideally be discussed with a second experienced physician. Furthermore, the procedure should be undertaken by a surgeon who is experienced in carrying out hysterectomy.19 Hysterectomy should not be delayed until the woman is in extremis or while less definitive procedures with which the surgeon has little experience are attempted.
SURGICAL TECHNIQUE
The following description of the surgical technique of cesarean hysterectomy has been modified from the original version of this chapter.
When cesarean hysterectomy is planned in advance, the surgeon has the luxury of a complete preoperative evaluation of the patient and her hematologic and coagulation status, and to choose experienced assistants and discuss procedures, necessary instruments, and sutures before the operation. Sadly this is rarely the case as most are emergency procedures.
Cesarean hysterectomy is really two separate operations: cesarean section and hysterectomy.
Cesarean hysterectomy can be accomplished through most abdominal wall incisions. A vertical incision provides best exposure, but often when performed as an emergency a transverse incision has been used and may be adequate. If required, division of rectus muscle with ligation of the inferior epigastric arteries (modified Maylard) is helpful.
The type of uterine incision used is guided by obstetric indications; however, a low vertical incision is less likely to extend and lacerate the uterine vasculature. In all stressful surgical situations, the technique with which the surgeon is most comfortable is appropriate. National guidelines in the UK10 recommend that in the presence of a suspected placenta previa with accreta opening the uterus at a site distant from the placenta, and delivering the baby without disturbing the placenta should be considered. Going straight through the placenta to achieve delivery is associated with more bleeding and a high chance of hysterectomy and should be avoided.
As with many surgical emergencies, the decision to proceed to hysterectomy is often more important than the technique required. The use of B-Lynch suture ligation or embolization of uterine vessels and internal iliac vessels should be considered but are not within the scope of this article. The following is a description of one possible technique for performing a cesarean hysterectomy.
Once the infant is delivered, and if feasible the placenta removed, the uterus should be carefully brought through the incision and placed on the abdominal wall. If the uterine incision is not going to be closed, the uterine angles should still be secured. Often the hysterotomy is closed as the decision for hysterectomy is being considered.
The hysterectomy is performed in the same manner as a routine abdominal hysterectomy. The massively increased vasculature is the main concern. The round ligaments are clamped and divided. The uterovesical fold is opened – often using monopolar diathermy, and the bladder reflected from the lower uterine segment. Posteriorly, the broad ligament is incised laterally and parallel to the infundibulopelvic ligament. The loose areolar tissue encountered in this space, which is more pronounced than usual because of the enlarged uterus, can be carefully dissected parallel to the course of the ureter. This allows visualization of the retroperitoneal space and the ureter throughout its course.
Two straight clamps are placed perpendicular to the uterus incorporating the tube and ovarian ligament, and ligated in the normal way. Often several clamps are required due to the size of the gravid uterus.
Before approaching the uterine arteries, the bladder must be dissected free and displaced below the operative field. Because most patients undergoing cesarean hysterectomy have had previous surgery, significant adhesive disease is frequently encountered; as a result, sharp dissection is the technique of choice. It is extremely important to avoid lateral dissection into the highly vascular bladder pillars. It is also wise not to extend the dissection farther than is necessary to safely ligate the uterine arteries, because excessive dissection can cause additional bleeding and waste time.
Attention is then directed toward the uterine arteries. The uterine vessels are significantly enlarged in pregnancy, and care must be taken in isolating or skeletonizing them. A curved clamp is placed with the distal portion perpendicular to the vessels at the level of the internal cervical os (Fig. 1). Once the same procedure is repeated on the contralateral side, the uterine arteries are secure, and blood loss should rapidly diminish. The use of a second clamp on the specimen side reduces back-bleeding from the uterus, which can obstruct the operative field. Additionally, until the utero-ovarian ligament is ligated, a substantial blood supply to the uterus persists. Care must be taken not to place lateral or downward traction on these clamps, which might tear friable tissues and cause bleeding that cannot be easily controlled. These clamps should be supported and not manipulated.
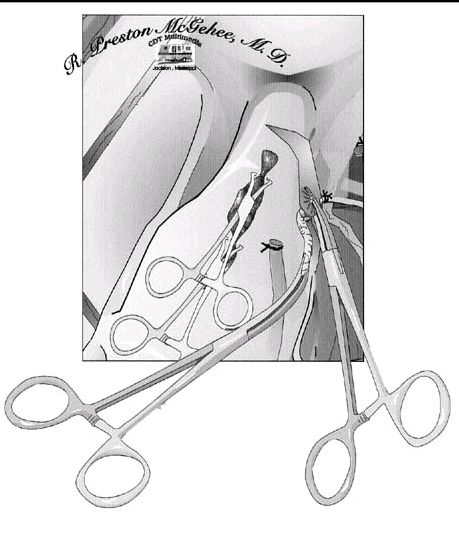 Fig. 1. A Heaney clamp is placed with the distal portion perpendicular to the vessels at the level of the internal cervical os.
Fig. 1. A Heaney clamp is placed with the distal portion perpendicular to the vessels at the level of the internal cervical os.
A second curved clamp is placed medial to the first clamp. Careful placement of clamps medially, moving down the parametrial tissue and hugging the cervix, will allow ligation of any branches of the uterine artery not ligated with the first clamp and ensure the safety of the ureter (Fig. 2). In most cases, conservation of the ovaries should be possible, unless infundibulopelvic ligament hematomas occur.
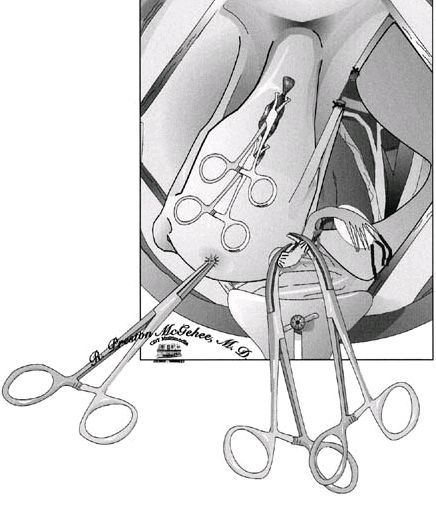 Fig. 2. To ensure that there is no damage to the ovary, Heaney clamps are placed close to the uterus
Fig. 2. To ensure that there is no damage to the ovary, Heaney clamps are placed close to the uterus
|
With the entire blood supply to the uterus now secured, a critical decision must be made in performing an emergent cesarean hysterectomy. If the patient is unstable or if the amount of bleeding has been excessive, the surgeon should consider to a subtotal hysterectomy, which shortens operating time while still accomplishing the primary goal of hemostasis. If subtotal hysterectomy is performed, the uterus is amputated preferably with a scalpel or diathermy; if possible, this is achieved by cutting superiorly to the ligated uterine arteries while angling the scalpel or diathermy blade medially and downward. This technique allows removal of an inverted cone of the cervix, which will facilitate approximation of the edges of the cervical stump regardless of the degree of dilation. Once amputated, the cervical stump can be approximated in an anterior-to-posterior fashion using interrupted figure-of-eight ligatures. Special care should be taken to avoid the bladder. If the patient is stable and the cervix can be removed, the task can prove to be difficult. As the cardinal ligament dissection proceeds downward, dissection of the bladder must also advance. Sharp dissection with Metzenbaum scissors (with tips pointing downward) ensures that no harm comes to the friable posterior bladder wall. Bladder dissection need never progress more than 1 cm distal to the current cardinal ligament dissection.
The next step is the identification of the lowest extent of the dissection: the junction of the cervix and vagina. This junction can usually be felt between the thumb and forefinger by palpating the upper vaginal walls and encountering the thickened cervix. When the cervix is dilated, it can be difficult to discern its lower end. The best approach to this problem is to place each clamp of the cardinal ligament complex medial to the preceding pedicle and roll it off the cervix to lie exactly against the lateral cervical wall. Each pedicle should be no longer than the distal third of the clamp used to grasp it. This allows the surgeon to progress down the cervix while each pedicle falls laterally, and the safety of the ureter is further ensured. In some cases, the uterosacral ligaments are quite prominent and may need to be individually clamped to completely ligate them and ensure hemostasis. Once the cardinal ligament dissection reaches the lower limit of the cervix, the vagina is entered, usually at the last pedicle. Curved scissors are used to amputate the cervix. The inside blade of the scissors is placed just beneath the cervix in the vaginal fornix and circumscribes the upper vagina to complete the dissection under direct vision. Alternatively, clamps may be placed across the vaginal cuff, immediately below the cervix, and the cervix amputated thereafter with a scalpel. When using this method, it is important to ensure adequate bladder dissection, as placement of these clamps (and subsequent sutures to secure the vault) is thought to potentially increase the risk of vesicovaginal fistula formation. Allis or Kocher clamps can be used to maintain traction on the anterior, posterior, and lateral angles of the vaginal wall. The vaginal epithelium is very friable and must be handled gently.
Surgical management of the vaginal cuff begins with supporting angle sutures that incorporate the lateral vaginal angles, the lower cardinal ligament pedicles, and the uterosacral pedicles. We usually hold this suture as a stay suture for subsequent identification of the vaginal angles. The surgeon may now choose to close the vaginal cuff with continuous or interrupted sutures, or to leave the cuff open and to secure hemostasis of the anterior and posterior cuff edges with a continuous nonlocking suture (Fig. 3). This will allow for drainage until spontaneous reperitonealization occurs.
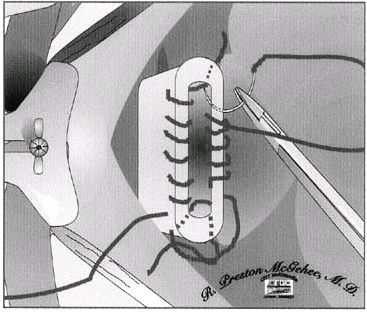 Fig. 3. To allow drainage, the surgeon chooses either to close the vaginal cuff with continuous or interrupted sutures or to leave the cuff open and to secure hemostasis of both the anterior and posterior cuff edges with a continuous nonlocking suture.
Fig. 3. To allow drainage, the surgeon chooses either to close the vaginal cuff with continuous or interrupted sutures or to leave the cuff open and to secure hemostasis of both the anterior and posterior cuff edges with a continuous nonlocking suture.
|
If the surgeon is suspicious that the integrity of the bladder wall has been breached at any time during the operation, the bladder may be filled with an opaque solution and the operating field inspected for extravasation of the solution. If there has been an inadvertent cystotomy, the area is dissected so that two rows of sutures can be placed without tension. The bladder is closed with two continuous layers of 4.0 polyglycolic sutures, with the second layer imbricating the first. Permanent suture material should never be chosen for bladder closure. The bladder is then refilled to ensure its integrity. When bladder repair is necessary, postoperative antibiotic coverage and Foley catheter drainage of the bladder should be continued for 7–10 days.
All pedicles are individually reinspected for hemostatic security. The pelvis is copiously washed with warm saline and water. Sponges and retractors are removed, and instrument, needle, and sponge counts are checked. The abdominal incision is closed in the routine fashion.
INTRAOPERATIVE COMPLICATIONS
Maternal morbidity associated with cesarean hysterectomy may be as high as 56%.14 The principle problems are bleeding (blood loss requiring transfusion occurs in over 40% of cases) and urinary tract injury (quoted as up to 16%). Intraoperative bleeding difficulties arise from the adnexal pedicles, the uterine vascular pedicles, the cardinal ligaments, or angles of the vagina arise at the time of bladder dissection. When dissecting the bladder inferiorly, the surgeon is cautioned to avoid lateral dissection, which may disrupt dilated veins of the plexus of Santorini.
In a review of cesarean hysterectomies at University of Mississippi Medical Center, bleeding from adnexal pedicles was a common cause of intraoperative bleeding and early postoperative bleeding and an indication for removal of one or both adnexa. These edematous pedicles are under considerable tension, which causes vessels to retract and escape their ligatures.17
The principles of skeletonizing and transfixing the uterine vessels have reduced the incidence of postoperative retroperitoneal bleeding from retracted uterine vessels. Pedicles that are too large and clamp manipulation that tears pedicles away from the uterine wall are the most common continuing problems that result in uterine vascular and cardinal ligament bleeding. Bleeding at the vaginal angles is often caused by injudicious traction and manipulation of stay sutures that open ascending branches of the vaginal arteries. Vigorous use of the suction tip and retractors in the region of the bladder pillars, angles of the vaginal cuff, and beneath the base of the bladder can cause troublesome venous bleeding for which it is often difficult to achieve hemostasis.20
Emergent cesarean hysterectomy presents special bleeding problems. Coagulopathies may be present when the patient is first encountered or may develop as the case progresses. There are often large hematomas in the broad ligament and other retroperitoneal spaces that distort anatomic relations and defy attempts at direct clamping and suturing. It is often possible to find a free dissecting space near the lateral pelvic wall where the uterine vessels can be ligated near their origin from the internal iliac artery or, failing this, the internal iliac (hypogastric) artery itself can be isolated and ligated. In drastic emergencies, the aorta may be compressed for a time to stop copious bleeding while the field is cleared for a more direct attack on the bleeding problem.
The use of surgical packs is a frequently overlooked adjunct in obtaining hemostasis. Temporary packing of a bleeding area can offer time, similar to that of compressing the aorta, and allow blood component replacement to catch up with a possible coagulopathy. Packs can also be used in a more definitive manner. In areas of diffuse venous bleeding, packs can be left in the abdomen after closure. Each pack should be brought out through the skin through a separate incision. They should be tagged and numbered so that they can be removed in the opposite order that they were placed. A Logthatopulos pack or umbrella pack is a bowel bag containing a number of packs with the opening protruding through the vagina. The entire pack can then be placed on traction, compressing the vasculature of the pelvis. Whenever we leave a pack in the abdomen, we administer broad-spectrum antibiotics until the packs are removed, usually within 72 hours.
The use of interventional radiology can be an invaluable tool. Prophylactic hypogastric artery embolization can be performed before cesarean hysterectomy without putting the fetus at risk and can potentially prevent surgical hemorrhage. Radiologic embolization can have an even larger role in cases of postoperative bleeding. Selective embolization can stop bleeding without the need for a second surgical procedure.7, 8, 9 The care of women undergoing massive postpartum hemorrhage, including the use of blood and blood products, has been outlined by the Royal College of Obstetricians and Gynaecologists in the UK, in a clinical guideline.19
Training in cesarean hysterectomy is often a weakness in most obstetrics and gynecology residency and training programs. However, this does not imply that the risks of the procedure are analogous with those of a vaginal delivery and subsequent hysterectomy.17 Seago et al.21 evaluated the role of elective cesarean hysterectomy, emphasizing the low morbidity rates, cost effectiveness of the procedure, and the opportunity for residents to learn the operation with supervision and under controlled circumstances.
The bladder and ureters are at risk during cesarean hysterectomy, particularly in emergent cases in which trauma and hematomas distort expected anatomic relations. The bladder is at greatest risk during its initial dissection from the anterior cervical wall. We describe techniques that make this dissection safer and allow easy identification of bladder injury (see above).
Some methods of cesarean hysterectomy include the technique of cross-clamping the upper vagina just before excision of the specimen. This technique must be used with caution in the obstetric patient with edematous tissues, because vesicovaginal fistulas have resulted from incorporation of the tented corners of the bladder in these clamps or sutures.20 We recommend the direct visualization technique described in this chapter for ligation of the vaginal cuff. Other causes of bladder fistulas include postoperative abscess formation, which can also contribute to ischemic necrosis at the base of the bladder and may produce a fistula.
There are no convincing data to suggest that subtotal is superior to total hysterectomy. Subtotal hysterectomy appears to be associated with shorter operating time and overall less blood loss. However, it has also been noted that bleeding from the cervical stump can be problematic, therefore sometimes it is essential to proceed to a total hysterectomy. The latter is associated with vaginal cuff bleeding and an increased risk of bladder injury. In current practice, the proportion of women undergoing each procedure appears to be roughly equal.14
The processes of uterine rupture and cesarean section scar dehiscence may directly injure the bladder and/or ureters. The surgeon must look for these, as well as inadvertent surgical injuries. It is usually the unrecognized bladder injury that results in vesicovaginal fistula; the properly repaired bladder usually heals without difficulty. Haynes and Martin22 reported 149 cesarean hysterectomies of which 10 were recognized and repaired cystotomies. No fistulas occurred in this series. Mickal and associates23, reported a series of 383 cesarean hysterectomies from the Louisiana State University service of which 20 cystotomies were recognized and repaired. Only one vesicovaginal fistula developed.
The ureters are most closely approached at three points during the dissection in cesarean hysterectomy: the infundibulopelvic ligament ligation site (when adnexal structures are removed), the uterosacral ligament dissection, and the uterine vascular and cardinal ligament pedicles. The most important principle in approaching the ureter in complicated cesarean hysterectomy cases is direct visualization. Without direct visualization, the ureter, which can inadvertently be lifted into the operative field, can be ligated or transected (Fig. 4). The ureter is avoided at the level of the uterine artery and cardinal ligament pedicles by placing the clamps exactly against the lateral wall of the uterus and cervix. When the uterosacral ligament is divided as a separate pedicle, it must be carefully identified and accurately clamped and ligated without endangering the ureter, which passes just lateral to this dissection. Table 3 summarizes the incidence of major intraoperative and postoperative problems from a review of more than 5000 cases from the cesarean hysterectomy literature of the past 30 years.
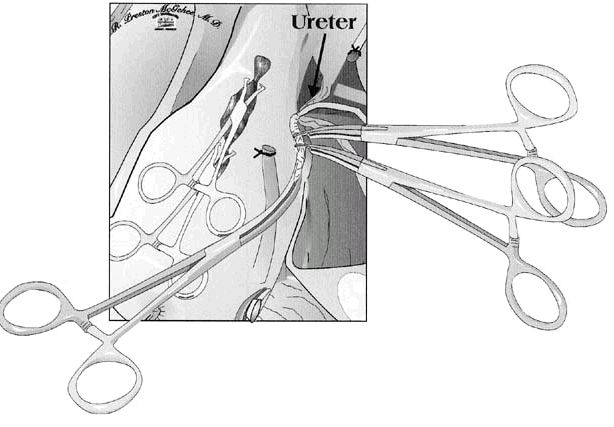 Fig. 4. Without direct visualization, the ureter, which can inadvertently be lifted into the operative field, can be ligated or transected.
Fig. 4. Without direct visualization, the ureter, which can inadvertently be lifted into the operative field, can be ligated or transected.
|
Table 3. Major operative and postoperative complications: review of 5185 cesarean hysterectomy cases, 1951–1984
| Complication | Percentage of cases |
| Postoperative hemorrhage | 3.30 |
| Bladder laceration | 2.80 |
| Ureteral injury | 0.44 |
| Fistula (total) | 0.57 |
| Vesicovaginal | 0.46 |
| Ureterovaginal | 0.10 |
| Rectovaginal | 0.02 |
| Thromboembolism | 0.52 |
| Overall morbidity | 35.3 |
| Maternal mortality | 0.70 |
POSTOPERATIVE MORBIDITY AND MORTALITY
Postoperative complications after cesarean hysterectomy are similar to those after any abdominal hysterectomy performed for gynecologic indications. Other than transfusion (of packed red cells or other blood products), the most common postoperative complication appears to be fever. Shellhaas et al.12 carried out a prospective observational study in 13 American academic medical centers, from January 1999 to December 2000, to determine the frequency of complications following cesarean hysterectomy. The results are presented in Table 4. Postoperative fever was the most common complication, occurring in 11% of patients. The differential diagnosis of postoperative fever must include pulmonary atelectasis and pneumonia; wound seroma, hematoma, and infection; vaginal cuff hematoma and infection; urinary tract infection; deep vein thrombosis; and breast engorgement mastitis. The most frequently occurring complications in patients who are febrile after cesarean hysterectomy are cuff cellulitis and pelvic hematoma or abscess formation.
Table 4. Postoperative complications following cesarean hysterectomy. (From Shellhaas et al. The frequency and complication rates of hysterectomy accompanying cesarean delivery. Obstet Gynecol 2009;114;224-9)
| Complication | n | % |
| Postoperative fever | 21 | 11.3 |
| Ileus | 10 | 5.4 |
| Exploratory laparotomy | 7 | 3.8 |
| Hospital readmission | 7 | 3.8 |
| Urinary tract infection | 6 | 3.2 |
| Cuff abscess | 5 | 2.7 |
| Maternal death | 3 | 1.6 |
| Bowel injury | 2 | 1.1 |
| Wound dehiscence | 2 | 1.1 |
| Septic pelvic thrombophlebitis | 1 | 0.5 |
| Confirmed deep vein thrombosis | 1 | 0.5 |
We encourage a complete work-up and examination of the postoperative patient, including appropriate cultures, whenever significant fever exists. We use antibiotic prophylaxis with one to two doses of a second-generation cephalosporin for all elective procedures. In patients with evidence of chorioamnionitis at the time of cesarean hysterectomy, broad-spectrum antibiotic coverage including ampicillin, gentamicin, and clindamycin is continued postoperatively. All women receive thromboprophylaxis for at least 7 days postoperatively, and use of graduated elastic compression stockings is advised.
Regarding mortality, Table 3 shows the results from a literature review series, and the maternal mortality rate can be seen to be seven per 1000 cases. The Louisiana State University series of 943 cesarean hysterectomies revealed a similar maternal mortality rate of 6.3 per 1000 case (Table 5). Review of these six maternal deaths indicates that half of the cases were very complex management problems in which the cesarean hysterectomy played little role in the death of the patient. The three deaths directly associated with the operation were from unrecognized retroperitoneal postoperative hemorrhage, sepsis with its attendant complications, and advanced pelvic malignancy.
Table 5. Postoperative complications of cesarean hysterectomy at the Louisiana State University Service – Charity Hospital of New Orleans (943 cases)
| Complications | Percentage of cases |
| Urinary tract infection | 17.7 |
| Vaginal cuff hematoma/infection | 14.1 |
| Atelectasis/pneumonia | 4.9 |
| Wound infection/dehiscence | 5.0 |
| Laparotomy for bleeding | 1.8 |
| Fistula | 1.1 |
| Vesicovaginal | 0.9 |
| Ureterovaginal | 0.2 |
| Intestinal obstruction | 0.3 |
| Pulmonary embolism | 0.2 |
| Overall morbidity | 30.1 |
| Mortality* | 0.6 |
*6 cases; 1 death in past 15 years.
I
n contrast, the mortality rate from a review of 69 cesarean hysterectomy cases in Pakistan was reported to be 19%. The review, from 2002 to 2007, attributed these mortalities mainly to the fact that most of the operations were performed on women who presented already in hypovolemic shock and who were coagulopathic, as opposed to the procedure itself. It was also acknowledged that many of these women had been cared for in labor by untrained attendants, which is common place in developing countries, and the most common indication for performing a cesarean hysterectomy was ruptured uterus, followed by uterine atony and morbidly adherent placenta. From the 69 cases, there were 36 stillbirths (45%) and one neonatal death recorded.24
CONCLUSION
Cesarean hysterectomy remains an operation with indications that arise infrequently in obstetric practice. However, the incidence of cesarean section has increased steadily over the past decade, and consequently there has also been a rise in the occurrence of placenta accreta, or placenta previa with accreta. These patients often require cesarean hysterectomy. All physicians who care for pregnant patients must prepare themselves to manage these problems.
When the need for cesarean hysterectomy arises, it often does so under adverse circumstances. Cesarean hysterectomy is one of the most difficult of obstetric operations when it is performed as an emergent procedure. Whilst some experience with uncomplicated, unhurried, preplanned cesarean hysterectomy is valuable in the educational development of obstetrics and gynecology specialists, it is recognized that these opportunities are limited.17, 25 Physicians should consider calling in another senior colleague with superior gynecological surgical skills early in the process.
REFERENCES
Park RC, Duff WP: Role of cesarean hysterectomy in modern obstetric practice. Clin Obstet Gynecol 23:(2):601, 1980 |
|
Porro E: Dell'amputazionne utero-ovarica come complemento di taglio cesareo. Ann Univers Med Chir 237:289, 1876 |
|
Plauche Plauché WC, Wycheck JS, Iannessa M et al: Cesarean hysterectomy on LSU Service of Charity Hospital. South Med J 76:1261, 1983 |
|
Clark SL, Yeh ZY, Phelan JP, et al: Emergency hysterectomy for obstetrics hemorrhage. Obstet Gynecol 64:376, 1985 |
|
Chestnut DH, Eden RD, Gall SA et al: Peripartum hysterectomy: A review of cesarean and postpartum hysterectomy. Obstet Gynecol 65:365, 1985 |
|
Raimer KA, O'Sullivan MJ: Cesarean section: History, incidence, and indications. In Plauche Plauché WC, Morrison JC, O'Sullivan MJ (eds): Surgical Obstetrics. p 407, Philadelphia, WB Saunders, 1991 |
|
Mitty HA, Sterling KM, Alvarez M et al: Obstetric hemorrhage: Prophylactic and emergency arterial catheterization and embolotherapy. Radiology 188:183, 1993 |
|
Alvarez M, Lockwood CJ, Ghidini A et al: Prophylactic and emergent arterial catheterization for selective embolization in obstetric hemorrhage. Am J Perinatol 9:(5/6): 441, 1992 |
|
Martin JN, Ridgway LE, Connors JJ et al: Angiographic arterial embolization and computer tomography-directed drainage for the management of hemorrhage and infection with abdominal pregnancy. Obstet Gynecol 76:941, 1990 |
|
RCOG Green-top Guideline Number 27. Placenta praevia, placenta accreta and vasa praevia: diagnosis and management. RCOG London 2011 |
|
Knight et al. Cesarean Delivery and Peripartum Hysterectomy. Obstetrics and Gynaecology 2008; 111:97-105 |
|
Shellhaas et al. The frequency and complication rates of hysterectomy accompanying cesarean delivery. Obstetrics and Gynaecology 2009; 114;224-9 |
|
Confidential Enquiries into Maternal and Child Health. Saving Mothers Lives 2003-05. RCOG Press, RCOG 2007 |
|
Rossi et al, Emergency Postpartum Hysterectomy for Uncontrolled Postpartum Bleeding. A systematic Review; Obstetrics & Gynaecology; VOL.115, No 3, March 2010 |
|
Flood KM, Said S, Geary M, et al. Changing trends in peripartum hysterectomy over the past four decades. Am J Obstet Gynecol 2009;200:632.e1-632.e6 |
|
Hills SD, Marchbanks PA, Tylor LR et al: Tubal sterilization and long-term risk of hysterectomy: Findings from the United States Collaborative Review of Sterilization. Obstet Gynecol 89:609, 1997 |
|
Seago DP, Roberts WE, Johnson VK et al: Can scheduled cesarean hysterectomies be justified. ? Am J Obstet Gynecol 180:1385, 1999 |
|
Bey MA, Pastorek JG II, Lu Py et al: Comparison of morbidity of cesarean section hysterectomy versus cesarean section tubal ligation. Surg Gynecol Obstet 177:357, 1993 |
|
RCOG Green-top guideline 52. Postpartum Haemorrhage, Prevention and Management. 2009 RCOG Press, London |
|
Plauche Plauché WC, Gruich FC, Bourgeois MD: Hysterectomy at the time of cesarean section: Analysis of 108 cases. Obstet Gynecol 58:459, 1981 |
|
Seago DP, Roberts WE, Johnson VK et al. Planned cesarean hysterectomy: a preferred alternative to separate operations. Am J Obstet Gynecol 1999;180:1385-93) |
|
Haynes DM, Martin BJ: Cesarean hysterectomy: A 25 year review. Am J Obstet Gynecol 137:393, 1979 |
|
Mickal A, Begneaud WP, Hawes TP: Pitfalls and complications of cesarean section hysterectomy. Clin Obstet Gynecol 12:660, 1969 |
|
Emergency Obstetric Hysterectomy; Shah N, Khan N; Rawal Medical Journal:Vol. 34. No1, Jan – June 2009) |
|
Gonsoulin W, Kennedy R, Guidry K: Elective versus emergency cesarean hysterectomy cases in a residency program setting: A review of 129 cases from 1984 to 1988. Am J Obstet Gynecol 165:91, 1991 |