
Postpartum Sterilization Procedures
Authors
INTRODUCTION
Sterilization following delivery during a patient's postpartum hospital stay is a convenient, efficient, and cost-effective means of preventing future pregnancy. Procedures for performing tubal sterilization have become more prevalent in recent years. It has been estimated that more than 340,000 sterilization procedures are performed in the postpartum period annually in the United States, which accounts for sterilization after 8−9% of all live births.1 The methods for elective postpartum sterilization include salpingectomy at cesarean delivery, postpartum salpingectomy by minilaparotomy, and postpartum salpingectomy or occlusion by laparoscopy during initial hospital stay. Cesarean hysterectomy or postpartum hysterectomy are other methods for sterilization, but are generally considered for non-elective indications.
PREOPERATIVE CONSIDERATIONS
Patient preparation
As discussed in the chapter on Surgical Procedures for Tubal Sterilization, proper patient counselling and informed consent is of paramount importance prior to a postpartum sterilization procedure. There must be no contraindication to elective surgery. The decision for sterilization should be made on an entirely voluntary basis following appropriate discussion regarding risks, benefits, and alternatives. The plan for postpartum sterilization should have been discussed and decided upon during the prenatal period. Topics covered should include timing, techniques, side-effects, complications, long-term effects, and an emphasis on the irreversible nature of the procedures used for postpartum sterilization. When appropriate, the patient's partner should be included in the discussion. Alternatives to female sterilization should also be discussed, including long-acting reversible contraception and male sterilization. The counselling and decision to proceed with permanent sterilization should be appropriately documented in the prenatal record.2, 3
In the United States, tubal sterilization procedures are among the most frequent sources of litigation. Adequate informed consent with chart documentation of risks—especially failure rate and the most usual complications—is essential.4 Some physicians and hospitals may require the patient and her husband to sign a sterilization permit as well as the usual consent for surgery. If the patient is a recipient of public aid funding for healthcare, it is necessary to satisfy state and federal regulations regarding consent for sterilization and possibly mandated waiting periods that can be up to 30 days. Although these waiting periods were initially used to help ensure informed consent and to protect patients that are disadvantaged, no data show that the 30-day waiting period decreases abuses or regret.5 An estimated 47% of sterilization requests go unfulfilled, half of which are due to policy-related barriers.6 If these barriers were eliminated, an additional 29,000 unintended pregnancies could be avoided, saving $215 million each year.7
Timing of the procedure
After a routine vaginal or cesarean delivery, tubal sterilization can generally be performed easily. Tubal sterilization may be done immediately following the completion of the vaginal delivery or after closure of the uterine incision during cesarean. If not completed at the time of cesarean or in the first few hours after delivery, the procedure is delayed until an appropriate time is available, generally within the first 48 hours after delivery. There are advantages to both immediate and delayed procedures. Factors include patient and physician preference, anesthesia, and hospital routines. The advantage of performing the tubal procedure at the time of cesarean delivery far outweighs the risks of performing a separate operative procedure after the cesarean.
If there are any significant complications or potential problems at or immediately after delivery, the tubal procedure should be delayed, potentially indefinitely. Concurrent medical, psychological, or neonatal conditions may also warrant deferment. Additionally, if any uncertainty regarding permanent sterilization is expressed by the patient during or after labor and delivery, it is best to delay the procedure. Some patients or couples prefer to wait for 12–48 hours to be as certain as possible that the baby is healthy. Others want no future pregnancy under any foreseeable circumstance, and the procedure may be done at any time. A single anesthetic procedure, avoidance of a second operative protocol and procedure, and shorter hospital stay all favor performing tubal surgery on the day of delivery. Postoperative morbidity is similar regardless of the timing of the tubal surgery.3
Though sterilization is considered an elective procedure when not performed in the postpartum period, it should be considered urgent when postpartum. In a study of women desiring postpartum sterilization who were unable to obtain it due to logistical reasons, 50% were pregnant within a year, versus less than 25% of women who did not desire a postpartum sterilization.8 Thus, those women who desire sterilization are at highest risk of unintended pregnancy, which is why their need for sterilization is of both ethical and medical necessity. Often logistics can be an issue, especially on a busy labor and delivery unit. An “elective” sterilization can be less urgent than a cesarean in the moment. However, if the Labor & Delivery team considers a postpartum sterilization to be urgent and necessary, there is the potential of reducing logistical barriers. Given the further costs of unintended pregnancy, as well as the cost to society, it should be regarded as urgent to oblige those who do not desire future fertility. This should frame further discussions on each labor and delivery floor to guide planning for additional anesthesia and nursing support when needed.9
Anesthesia considerations
The American Society of Anesthesiologist's Task Force on Obstetric Anesthesia published Practice Guidelines for Obstetric Anesthesia in 1999 that included discussion of postpartum sterilization.10 Though considered to be a small surgical procedure, tubal ligation can produce significant pain and cause physiologic changes similar to cesarean delivery due to manipulation and peritoneal stimulation.11 In the setting of tubal ligation at the time of cesarean, the patient should have adequate anesthesia. Choice of anesthetic after vaginal delivery is usually to re-dose an existing epidural if the catheter is still in place and functioning.12 The anesthesia team must assess whether the labor epidural catheter is functioning well-enough to provide adequate anesthesia for a postpartum tubal ligation. If the patient did not receive epidural anesthesia during labor or it is not functioning, a spinal anesthetic may be appropriate. Local infiltration into the abdominal wall and then into the mesosalpinx is a less common alternative and may be employed in the setting of inadequate conduction anesthesia in order to avoid a general anesthetic.11
It is extremely important that the patient who desires postpartum sterilization and is undergoing a routine vaginal delivery should not have any solid oral intake at least 8 hours prior to delivery and immediate postpartum sterilization according to Practice Guidelines for Obstetric Anesthesia. The same publication notes that small amounts of clear liquids may be consumed up to 2 hours before surgery. Given the decreased gastric emptying associated with pregnancy and the subsequent slowing of the intestinal tract during labor, patients are at very high risk of aspiration if general anesthesia is required during tubal ligation.10
TUBAL SURGERY
Anatomy and surgical approach
The uterus is still enlarged and raised out of the pelvis for several days to 3 weeks after delivery, making the tubes more accessible to abdominal surgical techniques and less attainable by vaginal routes. Therefore, almost all sterilization procedures in the early postpartum period are performed through abdominal incisions—generally minilaparotomy.1 However, with the ever-increasing use of minimally invasive surgical techniques some surgeons have begun using a laparoscopic approach. Postpartum laparoscopic tubal sterilizations have been reported in the literature since the mid-1980s with a large published series of such procedures described in 2007 by Huber and colleagues.13 Though the authors of this series concluded that postpartum laparoscopic sterilization may be superior to postpartum minilaparotomy, others have drawn attention to the possibility that this may not always be true in settings with less technical or anesthetic resources available.14
In the early postpartum period the fallopian tubes may be larger and more edematous, and the mesosalpinx, as well as the broad ligament often contain enlarged, tortuous blood vessels. These conditions may make surgical procedures on the tubes more difficult and provide a greater opportunity for bleeding problems to occur. It is extremely important to identify the tubes throughout their entire length before any intervention to ensure that the proper structure is being occluded or divided. Both adnexal regions should be thoroughly inspected for any abnormalities. Likewise, the uterus should be evaluated for any significant or unexpected gynecologic disease.
It is important to consider a woman’s past surgical and medical history in the decision to proceed with a postpartum tubal sterilization. An abdominal approach may be extremely difficult in a woman with a history of multiple abdominal surgeries, intra-abdominal adhesive disease, repaired abdominal wall hernias, morbid obesity or history of pelvic inflammatory disease. It may be better to consider a different form of permanent sterilization such as an interval hysteroscopic approach, however, this will require instituting a method of contraception in the immediate postpartum. For further details on the laparoscopic and hysteroscopic procedures as well as postpartum sterilization, refer to the respective chapters. This chapter focuses on immediate postpartum sterilization procedures.
Preoperative laboratory studies should include evaluation of hemoglobin, hematocrit, and white blood cell count with differential. These studies may be obtained during labor in those patients who are to have immediate postpartum sterilization. Hospital regulations may require a recent electrocardiogram and blood chemistry profile, especially in those women with special medical situations or in those taking certain medications (e.g. steroids, diuretics).
A patient's bladder should always be emptied just before the sterilization procedure to minimize the risk of cystotomy.. An indwelling catheter is not necessary unless one is already in place or is advisable for other reasons (e.g., traumatic delivery). Other standard preoperative preparatory conditions must be met if sterilization is being performed as a separate procedure at a time other than immediately after delivery.
Methods
Given the size and location of the uterus immediately postpartum, an abdominal approach is the most preferred method for tubal sterilization. A periumbilical transverse incision is often used when the tubal procedure is done soon after delivery and the level of the uterine fundus is near the umbilicus, there is less bleeding, and less postoperative discomfort. The procedure may take slightly longer if this type of incision is used, and the exposure for inspecting the uterus and adnexa is more limited. The other approach is through a vertical midline incision between the umbilicus and the symphysis pubis. The height of the fundus determines the specific location, as well as the possibility of using a preexisting lower abdominal incision.
Most physicians use a small, open laparotomy type of incision rather than laparoscopy unless the procedure has been delayed for more than several days and the uterus has decreased too much in size. If laparoscopy is chosen as the postpartum technique, it should be performed only by physicians who have expertise in the method, because of uterine size and broad ligament vascularity.15, 16 Some physicians who feel that laparoscopic postpartum tubal sterilization is equivalent to or better than the open minilaparotomy approach.13, 14
Several postpartum tubal ligation procedures are popular. (See the detailed descriptions of surgical techniques described in the chapter on Surgical Procedures for Tubal Sterilization). Most often, a portion of the ligated tube is removed so that the cut ends will close over and separate. The Pomeroy method or its modifications remain the most commonly used tubal ligation procedures.17 A small loop in the tube is formed near the mid-portion by picking up the tube with a Babcock clamp. The loop is then ligated at its base using an absorbable suture (Fig. 1); and a portion of the loop is excised. This is the simplest method, and if the cut ends and the surrounding mesosalpinx are hemostatic, complications are unusual. Some surgeons ligate the cut ends individually. However, using more than a single catgut suture at the base of the loop may theoretically increase inflammation and decrease the likelihood of separation of the cut ends.
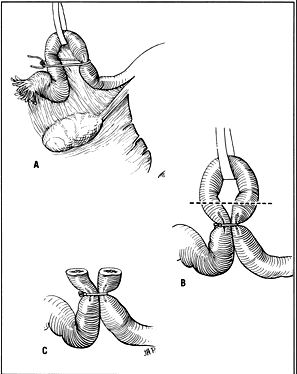
Fig. 1. Pomeroy method for tubal sterilization. (A) Forming loop of tube and ligating base. (B) Site of tube excision. (C) Cut ends before absorption of suture and separation.
Similar to the Pomeroy technique, the Parkland procedure is a method of partial salpingectomy for sterilization. However, rather than ligation of a knuckle of tube followed by creation of a window in the mesosalpinx, the window is created first. The tubal ligation is performed by identifying an avascular section of the mesosalpinx (Fig. 2A) and creating a window in this region (Fig. 2B), below the tube, with Metzenbaum scissors or a hemostat while elevating the tube with Babcock clamps. By opening the hemostat or scissors within the window, it can be stretched in parallel with the tubal lumen. A 2 cm segment of the mid-portion of the tube is then ligated proximally and distally with separate 0-chromic or plain gut sutures (Fig. 2C). The segment between the suture ligatures is then excised (Fig. 2D). The Parkland method provides for immediate anatomic separation of the disconnected tubal segments.18
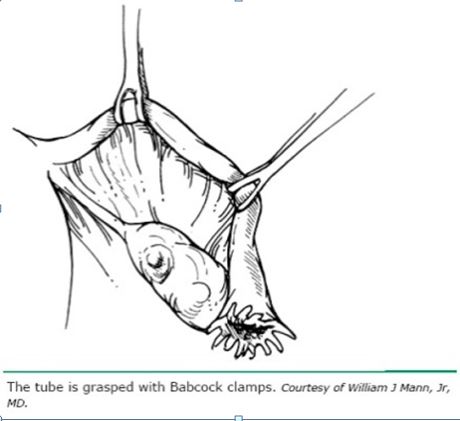 Fig. 2A. Identification of avascular region of mid-portion of tube.
Fig. 2A. Identification of avascular region of mid-portion of tube.

Fig. 2B. Window through mesosalpinx is created below the tube.
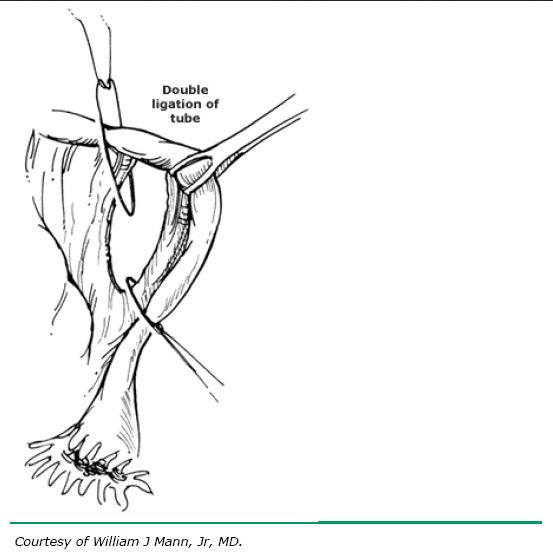 Fig. 2C. Rapidly absorbable (O chromic or plain gut) sutures placed proximally and distally.
Fig. 2C. Rapidly absorbable (O chromic or plain gut) sutures placed proximally and distally.
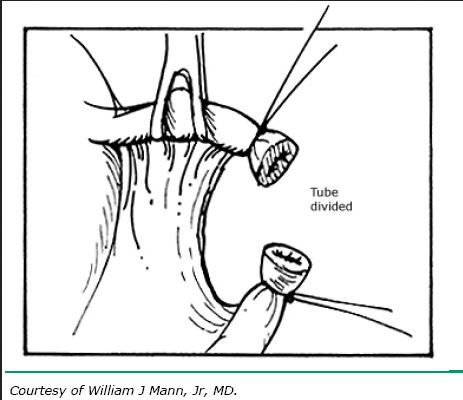 Fig. 2D. Ligated portion of tube excised.
Fig. 2D. Ligated portion of tube excised.
The method of Madlener is similar, but somewhat less effective. The loop of tube is formed, but the portion is not removed. Instead, the tube is crushed at the base of the loop and ligated with a nonabsorbable suture (Fig. 3A). With this method, occlusion, but not division of the lumen is achieved. Care must be taken to not make the ligature so tight as to cut through the tube. Failures are attributed mainly to fistula formation at the ligature site.
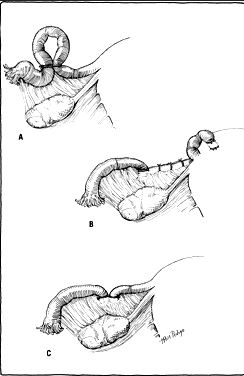 Fig. 3. (A) Madlener method for tubal sterilization. (B) Modified Irving tubal sterilization. (C) Another modified Irving technique. Both cut ends are buried in the broad ligament.
Fig. 3. (A) Madlener method for tubal sterilization. (B) Modified Irving tubal sterilization. (C) Another modified Irving technique. Both cut ends are buried in the broad ligament.
In 1924, Irving described a technique of tubal sterilization at the time of cesarean delivery. After cutting through the tube at the isthmic portion, the proximal end is buried in the posterior wall of the uterus.19 A revision of this procedure was described in 1950 which involves burying the distal end into the leaves of the broad ligament.20 This method takes longer, and there may be greater blood loss; however, the chances of tubal recanalization or pregnancy in the proximal stump are remote.
Other variations of tubal sterilization have been tried but never gained much popularity. The Irving method was modified to bury both cut ends into the broad ligament (Fig. 3C). Additionally, merely burying the fimbriated end of the tube in a pocket in the broad ligament (i.e. Aldridge technique) was thought to be a good temporary means of sterilization (Fig. 4A). Reversal by freeing the ends of the tubes was thought to be easily accomplished. Unfortunately, the rate of pregnancy after restoration was not as anticipated, especially if tubal or peritoneal infection occurred after the initial attempt at sterilization.
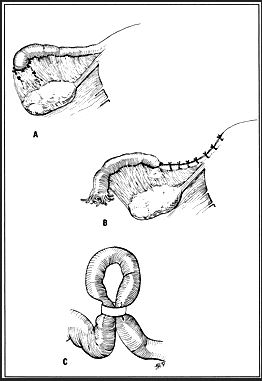 Fig. 4. (A) Aldridge technique of tubal sterilization. (B) Cornual resection of the tube for sterilization. (C) Silastic band for tubal occlusion.
Fig. 4. (A) Aldridge technique of tubal sterilization. (B) Cornual resection of the tube for sterilization. (C) Silastic band for tubal occlusion.
Cornual resection including an adjacent portion of the tube has also been described, but this procedure requires more exposure and results in greater blood loss (Fig. 4B).
The Oxford method of interposing the round ligament between the cut ends of the isthmic portion of the tube has never been prevalent in the United States. Neither has the Uchida method of tubal resection at its ampullary portion been popular because of its complexity, potential for bleeding, and greater length of tubal resection.21 Another method of fimbriectomy following distal ligation with silk sutures attributed to Kroener also carries a high failure rate.
Stainless steel clips and Silastic bands can be used to occlude the tubal lumen (Fig. 4C).22 Laparoscopy and open incisional techniques have both been used for application of these clips and bands in the postpartum period. Complications are minor; mild discomfort has been noticed at the site of occlusion. The effectiveness rate has been found to be very acceptable based on follow-up of patients for several years after application. Green and Laros give a complete description of most traditional and newer techniques.15 With the advent of the titanium tubal occlusive device (Filshie clip), created by British obstetrician–gynecologist, Marcus Filshie, another method was available for use at either interval laparoscopic or postpartum tubal sterilization (Fig. 5). A systemic review compared efficacy of the titanium clip occlusion device in the postpartum setting versus partial salpingectomy. The clip was associated with a failure rate of 1.7% at 24 months, compared to 0.04% at 24 months with partial Pomeroy partial salpingectomy (p = 0.04).23 A Cochrane Review of female sterilization techniques concluded that there is too little evidence to determine which technique is most effective.1 The data do suggest that when partial salpingectomy is possible in the postpartum period, this should be the method of choice.
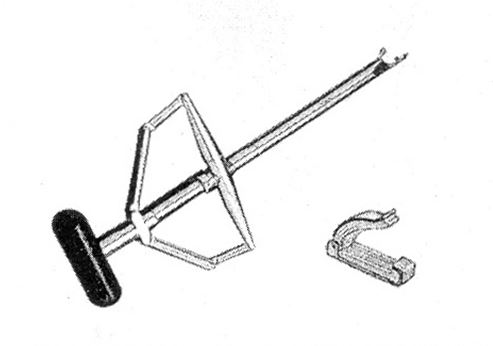
Fig. 5. Minilap applicator and Filshie clip. From Kohaut BA, Musselman BL, Sanchez-Ramos L et al., Contraception, 2004; copyright 1997, with permission from Elsevier
Ancillary procedures
Appendectomy has been routinely performed by some physicians at the time of postpartum tubal sterilization provided there are no medical or surgical contraindications. To add removal of the appendix to the procedure usually requires a larger incision, extra time, and an increase in blood loss. However, at least one study has indicated that there is no difference in postoperative morbidity.24 Removal of ovarian and paratubal cysts, lysis of adhesions, and resection of endometrial implants and small leiomyomas have also been done in conjunction with the tubal procedure. Again, the limitations of anesthesia and exposure might recommend against the additional intervention, but the surgeon must judge the possible benefits against any additional risks. Each patient must be evaluated on an individual basis.
Complications
Tubal sterilization procedures are usually not associated with significant risk or morbidity. Data from 1979–1980 indicate that the risk of death from tubal sterilization is 1–2 per 100,000 procedures. The risk of major morbidity from tubal sterilization after cesarean or vaginal delivery is most likely related to complications of the pregnancy or delivery.25 Bleeding is the most common postoperative problem; it usually occurs as a result of inadequate ligature of the tube or failure to adequately ligate bleeding in the mesosalpinx or broad ligament. The increased blood supply to these areas with varicosities in pregnancy lends itself to the possibility of hemorrhage and hematoma if meticulous hemostasis is not achieved.
The usual sequelae of intra-abdominal surgery (e.g. paralytic ileus, abdominal distention, adhesions, intestinal obstruction) are associated with tubal sterilization procedures. Incisional infections and hematomas are less frequent but occasionally occur, especially in obese patients or in those with a chronic systemic illness. Injury to the bladder is uncommon but may occur if the abdominal incision is too low or if the bladder is distended. As mentioned previously, catheterization to ensure that the bladder is empty should be done immediately before all sterilization procedures. The Pomeroy method and its modifications have the fewest overall operative complications.3
Anesthesia problems are also uncommon, but inadequate anesthesia may occur, especially with regional techniques used for delivery. Supplementation with local or inhalation techniques may be necessary to complete the tubal procedure in the immediate postpartum period. The use of continuous conduction anesthesia may allow for more prolonged and consistent levels when sterilization is combined with delivery. Precautions when using general anesthesia from the immediate postpartum period to several days after delivery are essential to minimize the possibility of aspiration and its sequelae. Residual gastrointestinal changes due to pregnancy make preoperative preparation especially important as described above.10
Side-effects
The short-term puerperal difficulties stem mainly from discomfort at the incision site and at the points where the tubes have actually been ligated or divided. It is unusual for any significant abdominal discomfort to persist beyond 2 weeks. There are usually no long-term alterations in a patient's menstrual or sexual functions. After collection of data from the U.S. Collaborative Review of Sterilization (CREST Study) and a large NIH-funded study there appears to be no clinical or laboratory evidence to support previously held beliefs that tubal sterilization procedures cause menstrual abnormalities.3, 25, 26
A number of studies on patient regret following tubal sterilization emphasize the need for time for adequate, early, and repeated predelivery counseling.3 See the discussion of preoperative considerations above, as well as the chapter on Surgical Procedures for Tubal Sterilization. The CREST Study followed patients for 14 years and found an overall probability of expressing regret was 12.7%, but women age 30 or younger had a 20.3% rate of regret versus only 5.9% among women who were older than 30 at the time of the tubal sterilization. Age less than 30, post-sterilization family events, and discovery that the procedure is not protective against sexually transmitted diseases are the most common causes of later regret.27
Effectiveness
With various tubal methods, the overall failure rate is on the order of 0.5% in the first year when the procedures are performed properly.28 Among the procedures discussed, the Irving and Uchida methods historically were associated with the fewest subsequent pregnancies, and the Madlener and Kroener methods are associated with the highest number. Today the most frequently used postpartum partial salpingectomy method is the Pomeroy procedure or one of its modifications. This is likely due to the fact that it is not only the safest of the methods mentioned but also has a very acceptable level of effectiveness. The effectiveness of all permanent sterilization methods depends on the age of the woman at the time of tubal sterilization. The CREST study followed the experience of 10,685 women from 8 to 14 years after various sterilization techniques were performed and identified 143 sterilization failures.29 An age-stratified analysis of this cohort revealed that the cumulative probability of pregnancy was low for women aged 34–44 years old at the time of sterilization, but as high as 5% for women aged 18–27 years old. Figure 6 demonstrates how the risk of pregnancy accumulates over time after all tubal occlusion methods.25
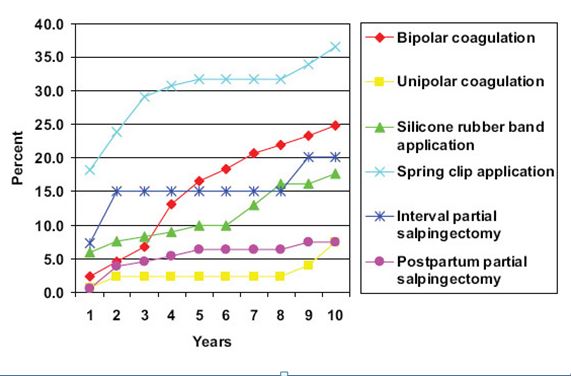
Fig. 6. Life-table cumulative probability of pregnancy among women who had tubal sterilization by method (cumulative probability per 1000 procedures).29
The three most common causes of failure are luteal phase pregnancy if the procedure is delayed beyond 30 days from delivery; occlusion of the wrong structure, most often the round ligament; and most frequently, recanalization of the severed ends of the tube. Although there is an increased incidence of ectopic pregnancy in failures of tubal sterilization, no single technique seems to predispose to this condition (see Table 1). The highest proportion of women who had a sterilization failure resulting in ectopic pregnancy occurred among women who had bipolar coagulation (65%) versus postpartum partial salpingectomy (20%).29, 30
Table 1. Life-table cumulative probability of ectopic pregnancy (EP) among women who had undergone tubal sterilization, according to time since sterilization. US Collaborative Review of Sterilization
| Method |
|
| Years since sterilization |
|
|
| Total EPs | 1 | 5 | 10 | 15 | |
| Unspecified (LS) | 40/22295 | 0.6 (0.3–1.0) | 1.4 (0.9–2.0) | 2.0 (1.5–2.8) | 2.7 (1.8–4.1) |
| Unspecified (ML) | 16/4904 | 0.8 (0.3–2.2) | 2.4 (1.3–4.3) | 3.6 (2.2–6.1) | 3.6 (2.2–6.1) |
| Filshie clip (LS) | 19/11858 | 0.5 (0.2–1.2) | 1.7 (1.1–2.7) | 2.0 (1.2–3.2) | NA |
| Filshie clip (Lap) | <5/2859 | 0.4 (0–2.5) | 0.9 (0.2–3.9) | 2.4 (0.9–6.7) | NA |
| Partial salpingectomy (LS) | <5/108 | 9.7 (1.4–66.6) | 21.5 (5.4–84.0) | 21.5 (5.4–84.0) | NA |
| Partial salpingectomy (ML) | <5/1166 | 0 | 2.3 (0.6–9.6) | 2.3 (0.6–9.6) | 2.3 (0.6–9.6) |
| Coagulation (LS) | 6/789 | 1.3 (0.2–9.1) | 8.4 (3.7–18.6) | 8.4 (3.7–18.6) | NA |
| Coagulation (ML) | 0/19 | 0 | 0 | 0 | NA |
| Salpingectomy (LS) | 0/195 | 0 | 0 | 0 | NA |
| Salpingectomy (ML) | 0/358 | 0 | 0 | 0 | NA |
| Essure hysteroscopy | 0/278 | 0 | 0 | 0 | NA |
| All methods | 89/44829 | 0.6 (0.4–0.9) | 1.7 (1.3–2.1) | 2.4 (1.9–3.0) | 2.9 (2.2–3.9) |
|
|
|
|
|
|
|
LS, laparoscopic; ML, minilaparotomy; Lap, laparotomy
Data are n/1000 procedures (95% confidence interval)
Adapted from Malacova 20142
Noncontraceptive benefits
Epidemiologic studies have shown a reduced risk of ovarian cancer after tubal sterilization.7 The underlying mechanism of reducing ovarian cancer risk has yet to be determined, but population based observational studies note this association. Also, though tubal sterilization does not provide protection from sexually transmitted infections, it does appear to decrease the risk of hospitalization due to pelvic inflammatory disease. This finding is also based on epidemiologic observations, and one theory is that tubal occlusion prevents ascending pelvic infection.7
HYSTERECTOMY
Cesarean hysterectomy has been used for sterilization in the presence of preexisting uterine or adnexal pathology. However, the primary indications for cesarean hysterectomy or immediate post-vaginal delivery hysterectomy are generally due to obstetric and surgical complications at the time of delivery. Hemorrhage, hematomas, uterine injury, and serious infection are among the indications for hysterectomy after cesarean or within the first few days postpartum.
The use of these procedures for sterilization alone without other gynecologic indications has been tempered at most institutions by findings of increased blood loss and postoperative morbidity.31 However, in some studies, no increase in morbidity was found when cesarean hysterectomy and tubal ligations at cesarean section were compared.
If sterilization is planned and major uterine disease is anticipated, the option for cesarean hysterectomy certainly should be discussed before the delivery. However, given the extremely low failure rates of most postpartum tubal sterilization procedures combined with low surgical risk versus the near zero chance of pregnancy after hysterectomy with potentially greater surgical risk, postpartum or cesarean hysterectomy has not been a favored method of sterilization.
Effectiveness
Hysterectomy is the most effective means of preventing pregnancy without depleting ovarian function. Rare failures in which pregnancy occurs in a prolapsed fallopian tube or from sperm passing through a fistulous tract in the vaginal vault have been recognized. However, morbidity and recovery factors rule against hysterectomy as a separate procedure following vaginal delivery unless significant complications or gynecologic pathology indicate removal of the uterus.
REFERENCES
Chan LM, Westhoff CL. Tubal sterilization trends in the United States. Fertil Steril 2010;94:1–6. |
|
Female contraceptive sterilization. Int J Gynaecol Obstet 2011;115:88–9. |
|
ACOG Practice bulletin no. 133: benefits and risks of sterilization. Obstet Gynecol 2013;121:392–404. |
|
Soderstrom RM. Case reports. II. Sterilization litigation. Clin Obstet Gynecol 1988;31:174–8. |
|
Borrero S, Zite N, Creinin MD. Federally funded sterilization: time to rethink policy? Am J Public Health 2012;102:1822–5. |
|
Zite N, Wuellner S, Gilliam M. Barriers to obtaining a desired postpartum tubal sterilization. Contraception 2006;73:404–7. |
|
Borrero S, Zite N, Potter JE, Trussell J, Smith K. Potential unintended pregnancies averted and cost savings associated with a revised Medicaid sterilization policy. Contraception 2013;88:691–6. |
|
Thurman AR, Janecek T. One-year follow-up of women with unfulfilled postpartum sterilization requests. Obstet Gynecol 2010;116:1071–7. |
|
Committee opinion no. 530: access to postpartum sterilization. Obstet Gynecol 2012;120:212–5. |
|
Siddik-Sayyid S, Zbeidy R. Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology 2007;106:843–63. |
|
Bucklin BA. Postpartum tubal ligation: timing and other anesthetic considerations. Clin Obstet Gynecol 2003;46:657–66. |
|
Vincent RD, Reid RW. Epidural anesthesia for postpartum tubal ligation using epidural catheters placed during labor. J Clin Anesth n.d.;5:289–91. |
|
Huber AW, Mueller MD, Ghezzi F, Cromi A, Dreher E, Raio L. Tubal sterilization: Complications of laparoscopy and minilaparotomy. Eur J Obstet Gynecol Reprod Biol 2007;134:105–9. |
|
Wang P-H, Lee W-L, Yuan C-C, Chin T-W. Postpartum sterilization: the choice of laparoscopy or minilaparotomy? Eur J Obstet Gynecol Reprod Biol 2008;139:116–7; author reply 117–8. |
|
Green LR, Laros RK. Postpartum sterilization. Clin Obstet Gynecol 1980;23:647–59. |
|
McDonnell CF. Puerperal laparoscopic sterilization. Am J Obstet Gynecol 1980;137:910–3. |
|
Bishop E, Nelms W. Simple method of tubal sterilization. NY State J Med 1930;30:24. |
|
Gentile GP, Kaufman SC, Helbig DW. Is there any evidence for a post-tubal sterilization syndrome? Fertil Steril 1998;69:179–86. |
|
Irving F. A new method of insuring sterility following cesarean section. Am J Obstet Gynecol 1924;8:355. |
|
IRVING FC. Tubal sterilization. Am J Obstet Gynecol 1950;60:1101–11. |
|
Uchida H. Uchida tubal sterilization. Am J Obstet Gynecol 1975;121:153–8. |
|
Pymar, H. C., et al. (2004). "Prospective randomized, controlled study of postoperative pain after titanium silicone rubber clip or Silastic ring tubal occlusion." Contraception 69(2): 145-150. |
|
Rodriguez MI, Seuc a, Sokal DC. Comparative efficacy of postpartum sterilisation with the titanium clip versus partial salpingectomy: a randomised controlled trial. BJOG 2013;120:108–12. |
|
Wilson EA, Dilts P V, Simpson TJ. Appendectomy incidental to postpartum sterilization procedures. Am J Obstet Gynecol 1973;116:76–81. |
|
Peterson HB. Sterilization. Obstet Gynecol 2008;111:189–203. |
|
Shobeiri MJ, Atashkhoii S. The risk of menstrual abnormalities after tubal sterilization: a case control study. BMC Womens Health 2005;5:5. |
|
Hillis SD, Marchbanks PA, Tylor LR, Peterson HB. Poststerilization regret: findings from the United States Collaborative Review of Sterilization. Obstet Gynecol 1999;93:889–95. |
|
Trussell J. Contraceptive failure in the United States. Contraception 2004;70:89–96. |
|
Peterson HB, Xia Z, Hughes JM, Wilcox LS, Tylor LR, Trussell J. The risk of pregnancy after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. Am J Obstet Gynecol 1996;174:1161–8; discussion 1168–70. |
|
Peterson HB, Xia Z, Hughes JM, Wilcox LS, Tylor LR, Trussell J. The risk of ectopic pregnancy after tubal sterilization. U.S. Collaborative Review of Sterilization Working Group. N Engl J Med 1997;336:762–7. |
|
Bey MA, Pastorek JG, Lu PY, Gabert H, Letellier RL, Miller JM. Comparison of morbidity in cesarean section hysterectomy versus cesarean section tubal ligation. Surg Gynecol Obstet 1993;177:357–60. |