CT Atlas
Cervical Cancer
 Computed tomography with contrast in a 44-year-old woman. This necrotic node deviating the ureter medially at the pelvic brim was not palpable in this patient with a stage IB (1 cm) adenosquamous cell carcinoma
of the cervix.
Computed tomography with contrast in a 44-year-old woman. This necrotic node deviating the ureter medially at the pelvic brim was not palpable in this patient with a stage IB (1 cm) adenosquamous cell carcinoma
of the cervix.
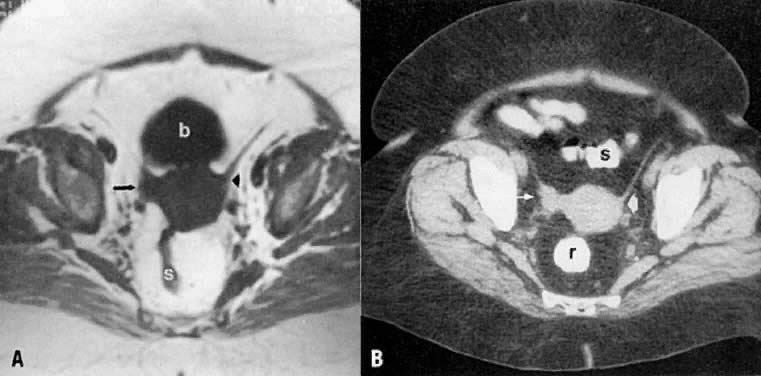 Axial T1-weighted MR (A) and CT (B) images of the pelvis in a patient with cervical cancer show right parametrial extension of tumor (arrow). Note the normal left parametrium (arrowhead). Proven stage IIB. (s, sigmoid; b, bladder; r, rectum.)
Axial T1-weighted MR (A) and CT (B) images of the pelvis in a patient with cervical cancer show right parametrial extension of tumor (arrow). Note the normal left parametrium (arrowhead). Proven stage IIB. (s, sigmoid; b, bladder; r, rectum.)
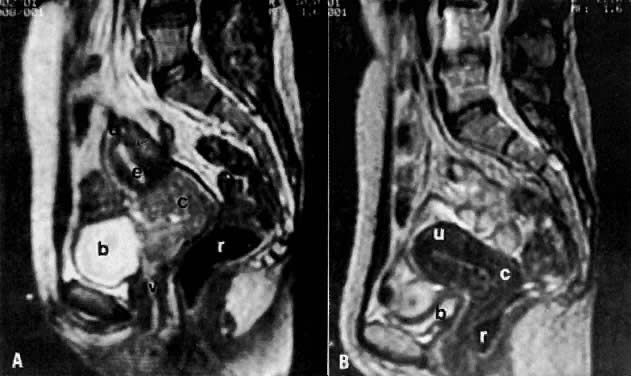 A. Sagittal T2-weighted MRI of the pelvis shows increase in size and signal intensity of the cervix (proven cervical carcinoma). B. Sagittal T2-weighted MRI of the pelvis shows resolution of the tumor after radiation therapy. (u, uterus; c, cervix; v, vagina; b, bladder; r, rectum; e, endometrium; arrow, uterine junctional zone.)
A. Sagittal T2-weighted MRI of the pelvis shows increase in size and signal intensity of the cervix (proven cervical carcinoma). B. Sagittal T2-weighted MRI of the pelvis shows resolution of the tumor after radiation therapy. (u, uterus; c, cervix; v, vagina; b, bladder; r, rectum; e, endometrium; arrow, uterine junctional zone.)
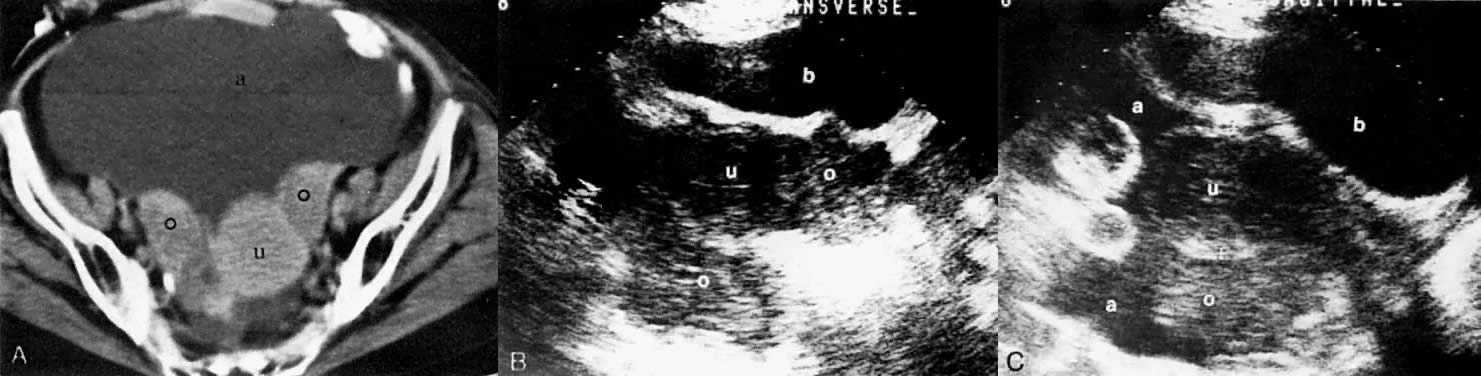
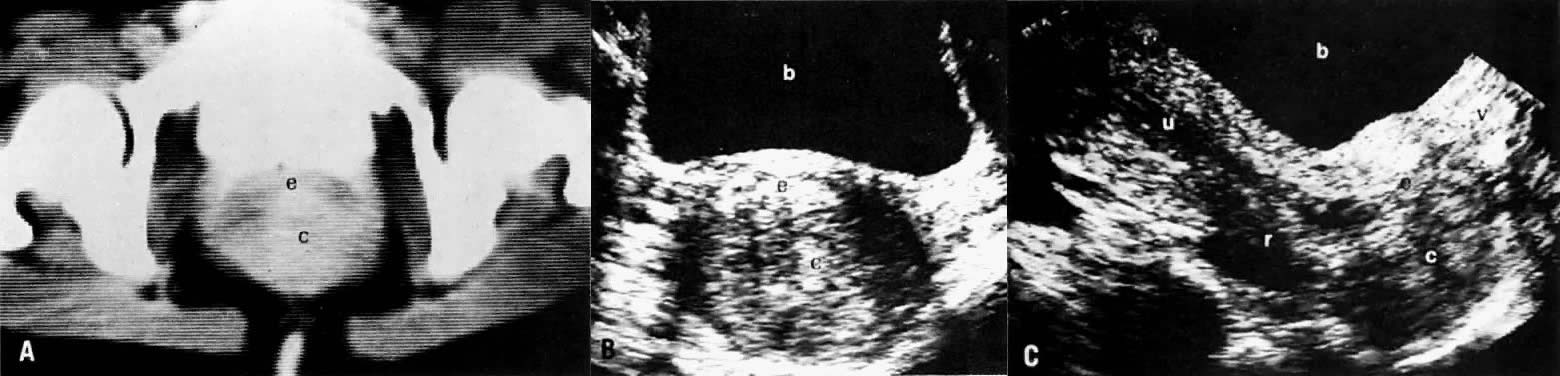 Cervical carcinoma stage IB. CT scan of the pelvis (A) shows a well-marginated posterior cervical mass stretching the cervical canal anteriorly. Transverse (B) and sagittal (C) sonograms of the pelvis show a large, well-defined, inhomogeneous, solid posterior cervical mass stretching the cervical canal anteriorly. It appears confined to the cervix without parametrial spread. The relationship of the mass to the vagina, uterus, rectum, and bladder is best demonstrated on the sagittal view. (c, cervical mass; e, cervical canal; v, vagina; u, uterus; r, rectum; b, bladder.)
Cervical carcinoma stage IB. CT scan of the pelvis (A) shows a well-marginated posterior cervical mass stretching the cervical canal anteriorly. Transverse (B) and sagittal (C) sonograms of the pelvis show a large, well-defined, inhomogeneous, solid posterior cervical mass stretching the cervical canal anteriorly. It appears confined to the cervix without parametrial spread. The relationship of the mass to the vagina, uterus, rectum, and bladder is best demonstrated on the sagittal view. (c, cervical mass; e, cervical canal; v, vagina; u, uterus; r, rectum; b, bladder.)
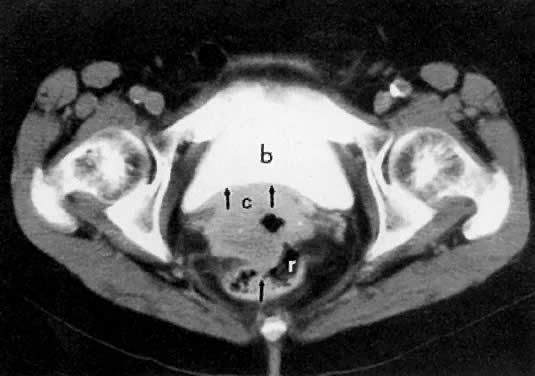
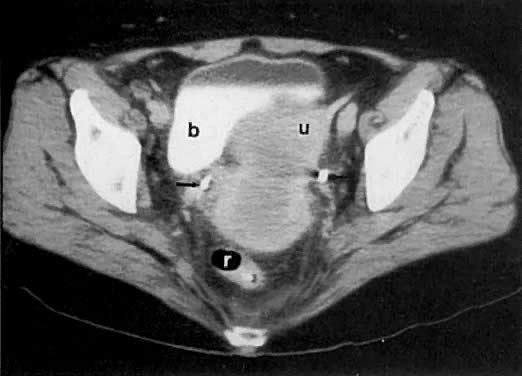 Axial CT scan of the pelvis in a 55-year-old woman with stage IB cervical carcinoma causing obstruction of the uterus (u). (b, bladder; arrows, uterus; r, rectum.)
Axial CT scan of the pelvis in a 55-year-old woman with stage IB cervical carcinoma causing obstruction of the uterus (u). (b, bladder; arrows, uterus; r, rectum.)
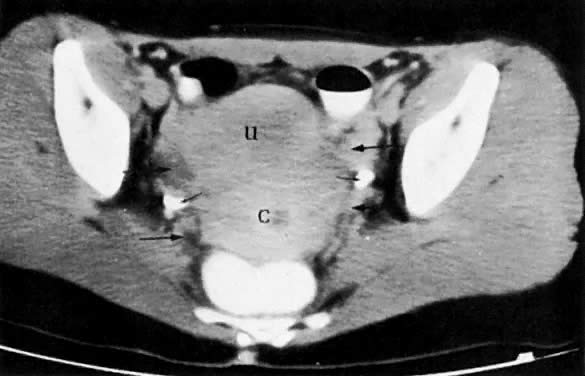 Cervical carcinoma with invasion of the parametria. CT scan of the pelvis shows inhomogeneous and enlarged cervix (c) with irregular soft-tissue densities extending into the parametria (long arrows), without invasion of the pelvic sidewalls. The periureteral fat planes are partially obliterated by tumor (short arrows), but the ureters are not obstructed. (u, uterus.)
Cervical carcinoma with invasion of the parametria. CT scan of the pelvis shows inhomogeneous and enlarged cervix (c) with irregular soft-tissue densities extending into the parametria (long arrows), without invasion of the pelvic sidewalls. The periureteral fat planes are partially obliterated by tumor (short arrows), but the ureters are not obstructed. (u, uterus.)
 Axial CT scan of the pelvis in a patient with stage IIIB cervical carcinoma shows a cervical mass (c) with right pelvic sidewall invasion (arrow).
Axial CT scan of the pelvis in a patient with stage IIIB cervical carcinoma shows a cervical mass (c) with right pelvic sidewall invasion (arrow).
 Axial CT scan of the pelvis in a patient with a stage IVA cervical carcinoma
shows a cervical mass (c) with invasion (arrows) of the bladder (b) and rectum (r).
Axial CT scan of the pelvis in a patient with a stage IVA cervical carcinoma
shows a cervical mass (c) with invasion (arrows) of the bladder (b) and rectum (r).
Back to Top
Endometrial Cancer
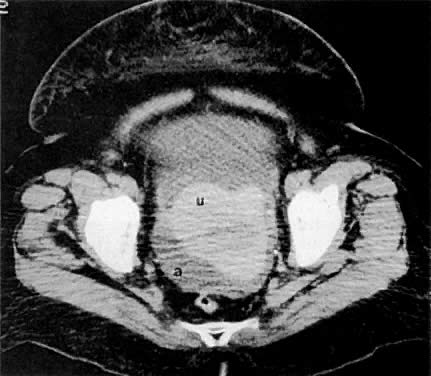 A 61-year-old woman with endometrial cancer. Note enlargement of the uterus (u) with a central area of hypodensity and the surrounding ascites (a).
A 61-year-old woman with endometrial cancer. Note enlargement of the uterus (u) with a central area of hypodensity and the surrounding ascites (a).
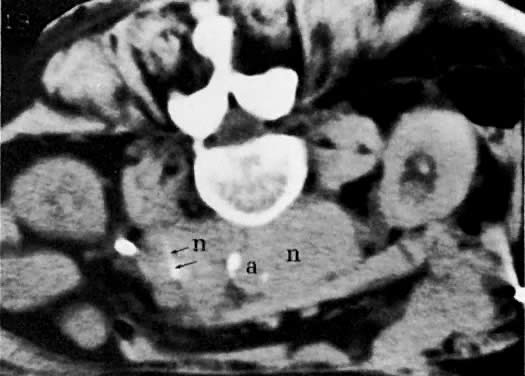
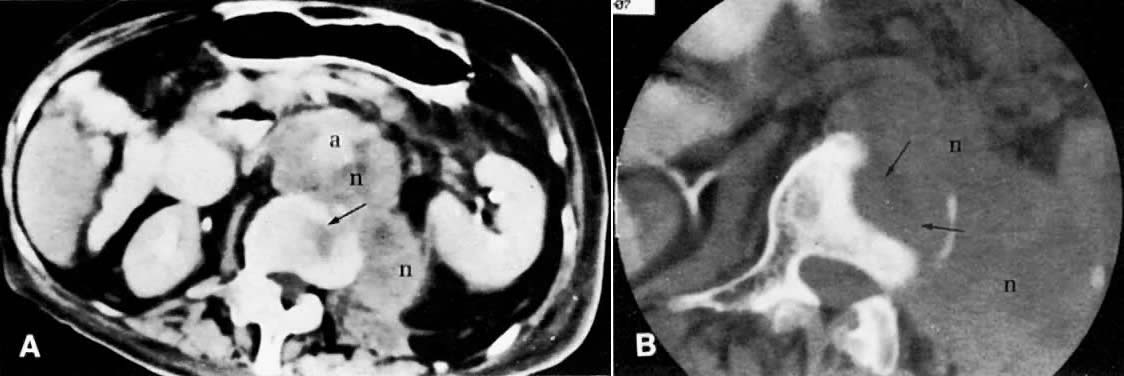 Massive para-aortic metastases from endometrial carcinoma with bony invasion. A. CT scan of the midabdomen shows confluent, massively enlarged para-aortic lymph nodes (n) encircling the aorta (a) and displacing it anteriorly. Note the destructive changes in the vertebral body (arrow). B. Cone-down view of the vertebral body shows massive bony destruction (arrows) caused by para-aortic lymphadenopathy.
Massive para-aortic metastases from endometrial carcinoma with bony invasion. A. CT scan of the midabdomen shows confluent, massively enlarged para-aortic lymph nodes (n) encircling the aorta (a) and displacing it anteriorly. Note the destructive changes in the vertebral body (arrow). B. Cone-down view of the vertebral body shows massive bony destruction (arrows) caused by para-aortic lymphadenopathy.
 CT-guided biopsy. CT scan obtained after introduction of the biopsy needle (arrows) into the matted para-aortic lymph nodes (n). (a, aorta.)
CT-guided biopsy. CT scan obtained after introduction of the biopsy needle (arrows) into the matted para-aortic lymph nodes (n). (a, aorta.)
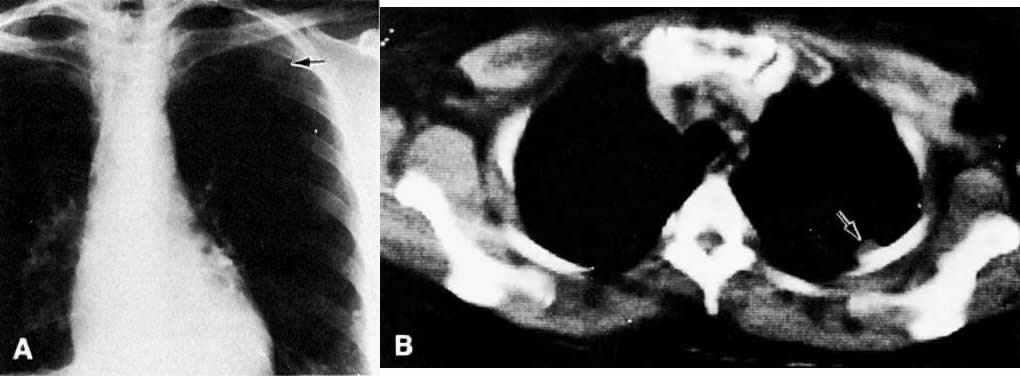 A. Posteroanterior chest film with metastatic lesion in left upper lung field, second
anterior interspace (arrow). B. Axial CT scan shows the lesion (arrow) projecting from the pleura.
A. Posteroanterior chest film with metastatic lesion in left upper lung field, second
anterior interspace (arrow). B. Axial CT scan shows the lesion (arrow) projecting from the pleura.
Back to Top
Leiomyosarcoma
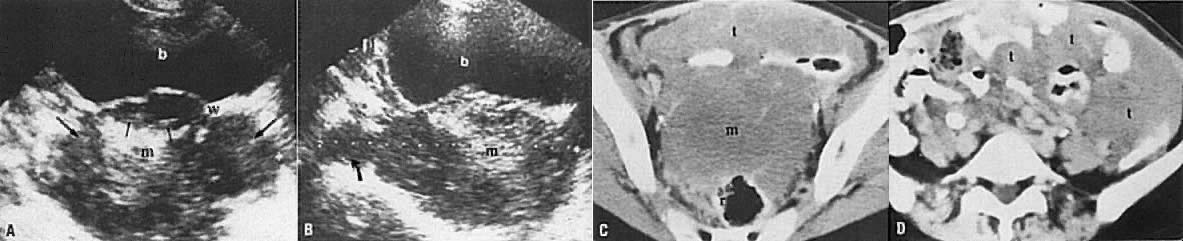 Stage IV leiomyosarcoma of the uterus. Transverse (A) and sagittal (B) sonograms of the uterus show it to be replaced by a large, inhomogeneous solid mass (m) with high- and medium-level echogenicity. There is evidence of extension superiorly (curved arrow) and into the parametria (long arrows) and bladder (short arrows). Serial CT scans of the pelvis (C and D) show a large mass (m) that is seen to spread to the mesentery (t). The perirectal fat plane is also obliterated, which is consistent with rectal invasion. (r, rectum; w, bladder wall; b, bladder.)
Stage IV leiomyosarcoma of the uterus. Transverse (A) and sagittal (B) sonograms of the uterus show it to be replaced by a large, inhomogeneous solid mass (m) with high- and medium-level echogenicity. There is evidence of extension superiorly (curved arrow) and into the parametria (long arrows) and bladder (short arrows). Serial CT scans of the pelvis (C and D) show a large mass (m) that is seen to spread to the mesentery (t). The perirectal fat plane is also obliterated, which is consistent with rectal invasion. (r, rectum; w, bladder wall; b, bladder.)
Back to Top
Ovarian Cancer
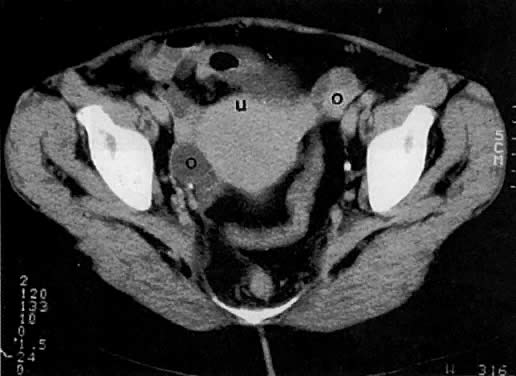 A 44-year-old woman with stage IB ovarian cancer. Axial CT scan of the
pelvis shows bilateral complex cystic/solid ovarian masses (o). Despite contiguity to the uterus (u), there was no evidence of uterine invasion at surgery.
A 44-year-old woman with stage IB ovarian cancer. Axial CT scan of the
pelvis shows bilateral complex cystic/solid ovarian masses (o). Despite contiguity to the uterus (u), there was no evidence of uterine invasion at surgery.
 A 47-year-old woman with stage IB ovarian cancer. Axial CT scan of the
pelvis shows large, bilateral cystic ovarian masses (o). Despite their size, the masses remain confined to the ovaries.
A 47-year-old woman with stage IB ovarian cancer. Axial CT scan of the
pelvis shows large, bilateral cystic ovarian masses (o). Despite their size, the masses remain confined to the ovaries.
 Ovarian adenocarcinoma involving both ovaries (o) and uterus (u) with ascites (a). CT scan of the pelvis (A) shows bilateral ovarian masses with ascites and uterine involvement on the left. Transverse (B) and sagittal (C) sonograms of the pelvis in a different patient show large, bilateral, irregular, and inhomogeneous ovarian masses inseparable from the uterus. Ascites is seen on the sagittal scan. The CT and ultrasound findings are consistent with at least stage II. (b, bladder.)
Ovarian adenocarcinoma involving both ovaries (o) and uterus (u) with ascites (a). CT scan of the pelvis (A) shows bilateral ovarian masses with ascites and uterine involvement on the left. Transverse (B) and sagittal (C) sonograms of the pelvis in a different patient show large, bilateral, irregular, and inhomogeneous ovarian masses inseparable from the uterus. Ascites is seen on the sagittal scan. The CT and ultrasound findings are consistent with at least stage II. (b, bladder.)
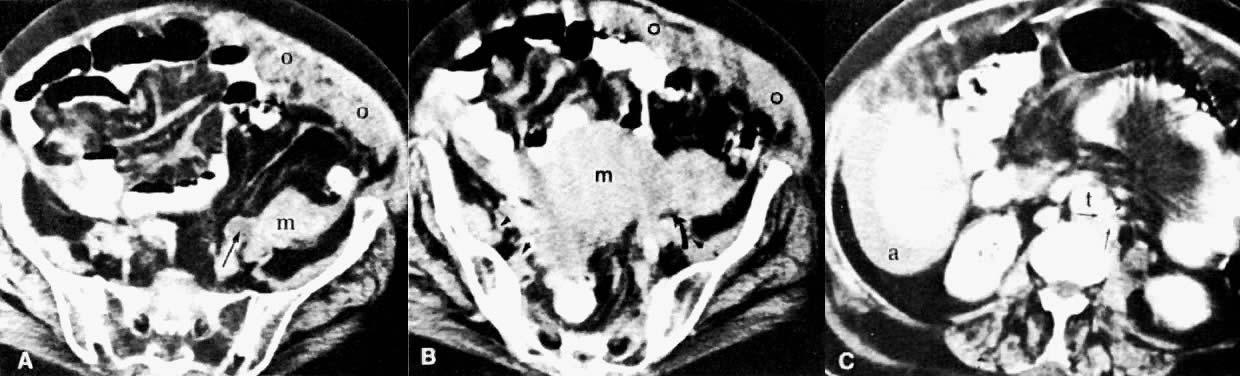 Stage III ovarian adenocarcinoma with ureteral invasion and omental cake. A and B. Serial CT scans of the pelvis 2 cm apart show a large, irregular pelvic mass (m). A thick layer of inhomogeneous soft tissue is seen under the anterior abdominal wall consistent with omental involvement (o). Note the dilated and unopacified left ureter (long arrow) in A and the pinching of the ureter by the pelvic mass (curved arrow) in B. Tumor extension to the pelvic sidewall is seen in B(arrowheads). C. CT scan of the abdomen shows several small, confluent para-aortic lymph nodes consistent with metastases (short arrows). (t, aorta; a, ascites.)
Stage III ovarian adenocarcinoma with ureteral invasion and omental cake. A and B. Serial CT scans of the pelvis 2 cm apart show a large, irregular pelvic mass (m). A thick layer of inhomogeneous soft tissue is seen under the anterior abdominal wall consistent with omental involvement (o). Note the dilated and unopacified left ureter (long arrow) in A and the pinching of the ureter by the pelvic mass (curved arrow) in B. Tumor extension to the pelvic sidewall is seen in B(arrowheads). C. CT scan of the abdomen shows several small, confluent para-aortic lymph nodes consistent with metastases (short arrows). (t, aorta; a, ascites.)
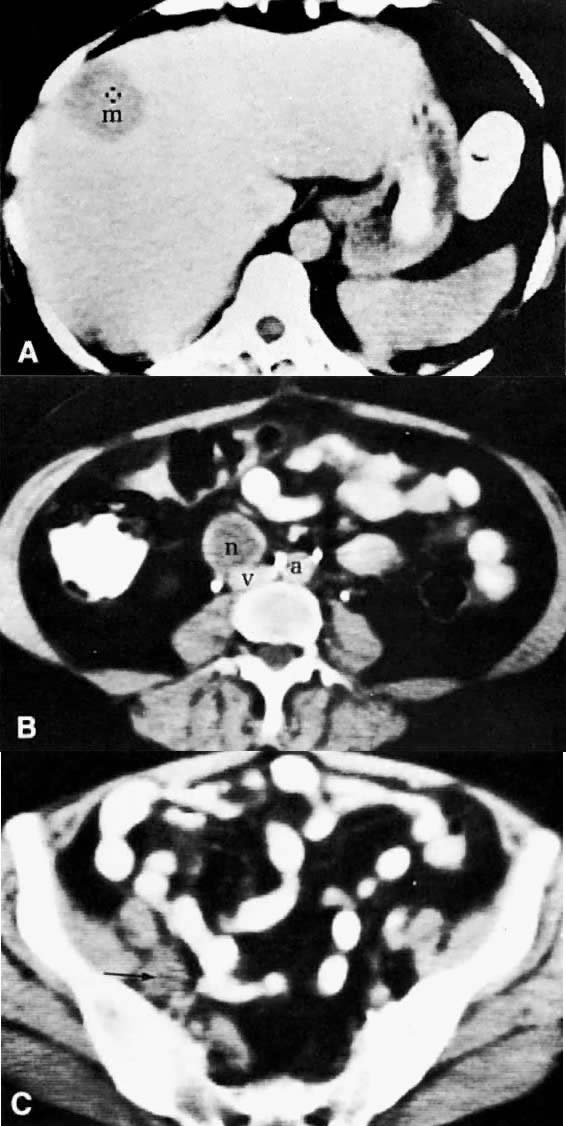 Metastatic granulosa cell tumor. A. CT scan of the upper abdomen shows a low-density, well-marginated mass (m) in the right lobe of the liver. B. Lower abdominal CT scan shows a necrotic paracaval mass (n) consistent with lymphadenopathy. C. CT scan of the pelvis shows an enlarged right external iliac lymph node (arrow) measuring 1.5 cm in diameter with some necrotic changes seen in its center. (a, aorta; v, inferior vena cava.)
Metastatic granulosa cell tumor. A. CT scan of the upper abdomen shows a low-density, well-marginated mass (m) in the right lobe of the liver. B. Lower abdominal CT scan shows a necrotic paracaval mass (n) consistent with lymphadenopathy. C. CT scan of the pelvis shows an enlarged right external iliac lymph node (arrow) measuring 1.5 cm in diameter with some necrotic changes seen in its center. (a, aorta; v, inferior vena cava.)
Back to Top |