Patients clinically suspected of having ectopic pregnancy fall into two
major categories: those who have an acute abdomen and in whom immediate
surgery is indicated, and those who are clinically stable and in whom
adjunctive diagnostic procedures can be performed. Patients with a surgical abdomen are evaluated in the emergency room with
rapid urine pregnancy tests and a culdocentesis. A positive culdocentesis
in a patient with a positive pregnancy test result has been reported
to correspond with ectopic pregnancy in 99.2% of cases.50 The results of a culdocentesis can be classified as negative, positive, or
nondiagnostic. A negative culdocentesis is indicated by the presence
of clear fluid. A positive result refers to the free flow of nonclotting
blood. If no fluid is obtained, the test is considered nondiagnostic. When
bloody fluid is obtained, a hematocrit of the aspirate is helpful. Ectopic
pregnancies are generally associated with hematocrits
of more than 15%. Lower hematocrits frequently indicate the presence of
cystic fluid. Traditionally, culdocentesis was considered useful in
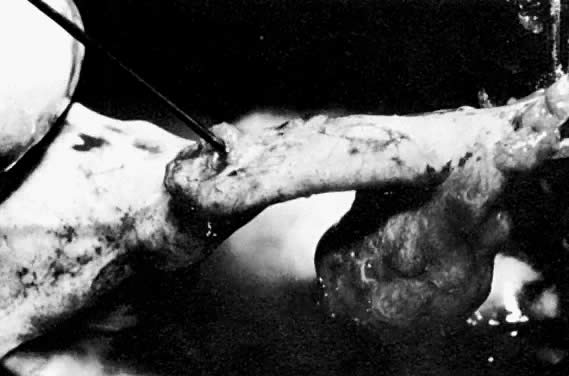
the detection of a hemoperitoneum associated with a ruptured ectopic pregnancy. We
have found that most of the positive culdocenteses in our
institution are associated with an unruptured ectopic pregnancy. In such
cases, bleeding through the distal end of the fallopian tube results
in a hemoperitoneum. In our series, 86% of all positive culdocenteses performed in the emergency
room were associated with an ectopic pregnancy.50 Other causes of positive culdocentesis included ruptured ovarian cysts, retrograde
menstruation, endometriosis, torsion of the fallopian tube, and
bleeding of unknown etiology. It should be emphasized that a nondiagnostic
culdocentesis should not lower the suspicion of an ectopic
pregnancy. In our series, 16% of ectopic pregnancies had nondiagnostic
culdocentesis, and one quarter of these were ruptured at the time of
operation.50 Patients who will benefit most from a culdocentesis are those in whom a
clinical suspicion of ectopic pregnancy exists, and who present at a
time when expeditious diagnosis is desired and when sophisticated diagnostic
modalities, such as ultrasonography and sensitive human chorionic
gonadotropin (hCG) assays, cannot be obtained without significant delay. Under
these circumstances, culdocentesis is an inexpensive, rapid, and
easily performed means of patient evaluation that often provides
the impetus for immediate intervention. In clinically stable patients, a culdocentesis may be indicated when fluid
is visualized in the cul-de-sac at the time of ultrasound examination
of the pelvis. A positive culdocentesis dictates the need for a surgical
diagnosis. The procedure should not be overlooked in patients without
signs of peritoneal irritation. We have found that 45% of our patients
with a positive culdocentesis did not have rebound tenderness.50 The modern approach to the evaluation of clinically stable patients suspected
of having an ectopic pregnancy is based on the combined use of
sensitive pregnancy testing (or hCG testing), ultrasound examination, and
laparoscopy. hCG testing is used to screen for pregnancy, and ultrasonography
is employed to locate it.51 Evaluation of the patients begins with a sensitive and rapid pregnancy
test. Blood and urine pregnancy tests have been used to screen for ectopic
pregnancy. Traditional slide pregnancy tests have been found to have
a 15% to 50% false-negative rate in ectopic pregnancy, and for this
reason they are unsuitable for screening.52 Advances in technologies of enzyme-linked immunoassay and monoclonal antibodies
to the β subunit have promoted the evolution of rapid, inexpensive, and
similar qualitative urinary pregnancy tests. They are
expected to improve the accuracy of the old urine pregnancy tests. Meanwhile, as
the information for these tests becomes available, we prefer
to use the sensitive blood pregnancy testing in the form of a radioimmunoassay
against β-hCG. We recommend an assay with a sensitivity of 2.5 mIU/mL because with this
system the false-negative rate is 0.5%. The radioreceptor assay, with
a sensitivity of 200 mIU/mL, is not suitable for screening because its
false-negative rate ranges between 6% and 12%, which is unacceptably
high for a life-threatening condition.53,54 Other investigators using a urine hCG test with a stated sensitivity of 50 IU/L
support this test's clinical application in detecting ectopic
pregnancy in emergent conditions.55 A negative blood pregnancy test virtually rules out pregnancy and thus
an ectopic gestation. A positive result requires further investigation, requiring
a determination of the hCG titer and an ultrasonographic examination
of the pelvis. A positive diagnosis of ectopic pregnancy can be made if fetal motion is
demonstrated outside the uterus. Unfortunately, this is a rare and late
finding, and awaiting its appearance would delay the diagnosis and
conceivably increase the risk of tubal rupture. In practice, ultrasonography
is used to identify an intrauterine pregnancy, which would render
the simultaneous presence of an ectopic pregnancy extremely unlikely (1:30,000). Confirmation of the presence of an intrauterine pregnancy
can be made by identifying either a gestational sac or a fetal pole
within the endometrial cavity. The traditional ultrasonographic criterion used for the diagnosis of ectopic
pregnancy is failure to visualize a gestational sac in the uterus
of patients with more than 6 weeks of amenorrhea. The problem with this
criterion is that one third of patients with ectopic pregnancy do
not know the date of their last menstrual period, and in others irregular
bleeding makes interpretation of the menstrual history difficult. It has been established that the sac of a normal intrauterine pregnancy
becomes visible with ultrasonography when the hCG titer is greater than 6500 mIU/mL. When
levels are higher than this, the absence of a sac
is associated with an ectopic pregnancy in 86% of cases. This criterion
has a sensitivity of 100%, a specificity of 96%, and a negative predictive
value of 100%. The clinical application of this criterion includes
the fact that approximately 40% of women with an ectopic pregnancy
possess titers in excess of 6500 mIU/mL.50 The absence of a sac at levels less than 6000 mIU/mL is a nondiagnostic
finding and should not lower or raise the suspicion of ectopic pregnancy.56,57 Management of these patients depends on the clinical situation. If a patient
remains clinically stable, serial hCG determinations are used for
the assessment of such a patient and for deciding whether to proceed
to diagnostic laparoscopy. The presence of a sac below an hCG titer
of 6000 mIU/mL can be explained if the pregnancy develops beyond the level
of sac formation (above an hCG level of 6500 mIU/mL) and then stops
secreting hCG. A sac will be detected by ultrasonography when the hCG
titer has dropped below 6000 mIU/mL. Some normal intrauterine pregnancies
produce lower levels of hCG and therefore may show a gestational
sac at lower hCG concentrations. This may account for Nyberg and associates'58 detection of gestational sacs in 13 patients in whom the hCG titer was
less than 6000 mIU/mL. In addition, this discrepancy may be confounded
by the common use of two distinct hCG standards in the evaluation of
ectopic pregnancy. In 1974, the World Health Organization introduced
a new standard that involved the use of a more highly purified preparation
of hCG and subsequently established the International Reference Preparation (IRP). A
decade earlier, the second International Standard
had been introduced, but because of heterogeneity, it was often unsuitable
for use in many immunoassays.59 In comparing the two quantitative standards, clinicians should note that
the serum hCG titers determined by the IRP approximately double the
value calculated by the second International Standard. The hCG values
stated in this review are based on the IRP standard unless otherwise
specifically noted. Finally, ectopic pregnancies can show a single-ring
sac due to the presence of blood within the endometrial cavity in association
with a significant decidual reaction. This appearance has been
shown to occur in 10% to 20% of all cases (Fig. 4).60,61,62,63,64,65,66,67,68 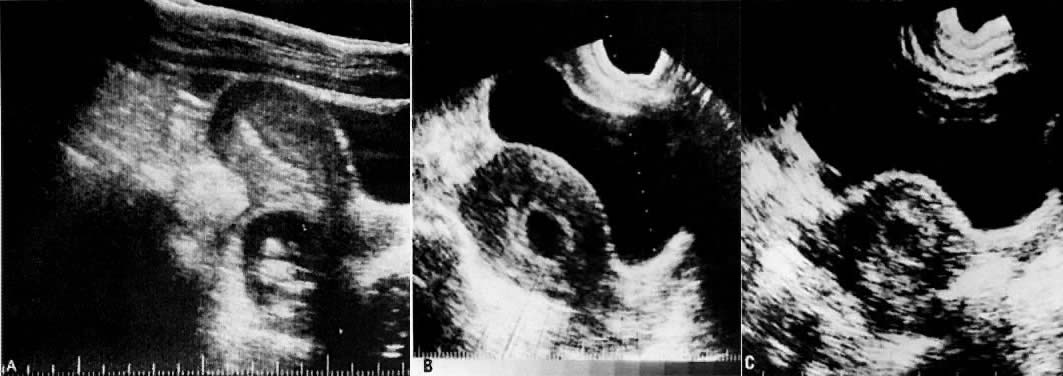 Fig. 4. A. Segmental scan of the pelvis in an ectopic pregnancy. A fetus is visualized
in the cul-de-sac. B. Gestational sac of two normal pregnancies. There is a double ring given
by the separation of the decidual capsularis and the decidual parietalis. C. Pseudogestational sac in an ectopic pregnancy. There is a single ring. Fig. 4. A. Segmental scan of the pelvis in an ectopic pregnancy. A fetus is visualized
in the cul-de-sac. B. Gestational sac of two normal pregnancies. There is a double ring given
by the separation of the decidual capsularis and the decidual parietalis. C. Pseudogestational sac in an ectopic pregnancy. There is a single ring.
|
Nyberg and colleagues69 and Bradley and associates70 have proposed morphologic criteria to distinguish the pseudogestational
sac of ectopic pregnancy from the gestational sac of a normal intrauterine
pregnancy. They have described the normal intrauterine gestational
sac as having a double contour produced by the decidua capsularis
and the decidua parietalis. The pseudogestational sac of an ectopic pregnancy
has only a single ring. The researchers have reported that 98.3% of
all patients with a double-ring sac had an intrauterine pregnancy
and 64 of 68 patients with a single-ring sac had ectopic pregnancies. Management of patients with an hCG titer less than 6000 mIU/mL is based
mainly on adnexal ultrasonographic findings and clinical suspicion. Romero
and colleagues71 prospectively evaluated 220 patients who were suspected of having ectopic
pregnancy and who had hCG titers less than 6000 mIU/mL and abdominal
ultrasonographic adnexal findings. The demonstration of a noncystic
mass, alone or associated with cul-de-sac fluid, was an indication for
diagnostic laparoscopy. The value of transvaginal ultrasonography in the detection of ectopic pregnancy, especially
in cases of hCG titers less than 6000 mIU/mL, is
now recognized. Proximity of the ultrasound transducer to both the adnexa
and the cul-de-sac allows increased resolution and image quality with
the detection of an intrauterine pregnancy up to 7 days earlier than
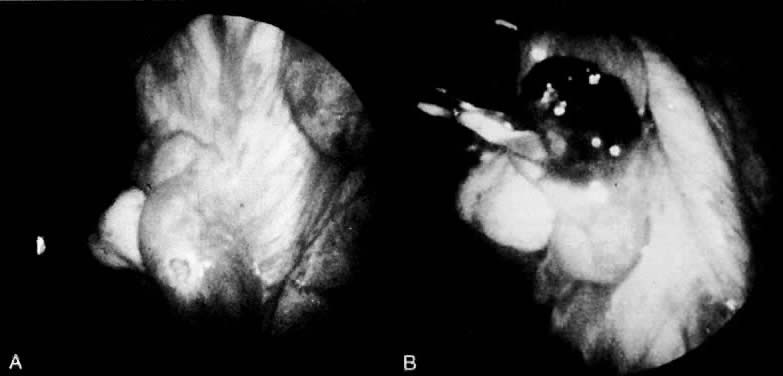
with the classic transabdominal approach (Fig. 5). 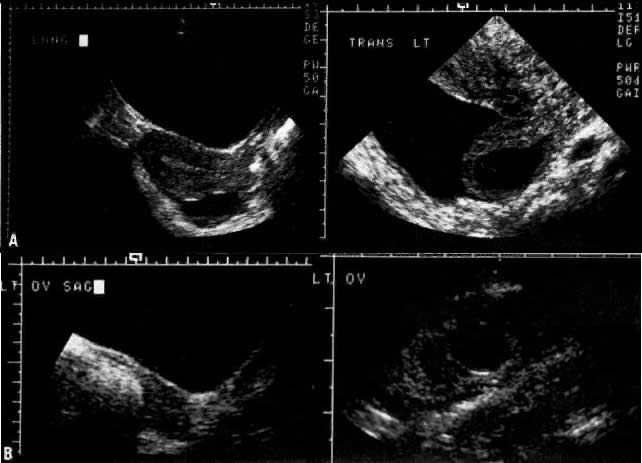 Fig. 5. The increased sensitivity of transvaginal (right) versus transabdominal (left) ultrasonography in detecting an ectopic pregnancy. A. Proximity to the cul-de-sac allowed detection of this ectopic gestation (hCG
titer 880 mIU/mL) by means of transvaginal ultrasonography in this
patient. B. Transvaginal ultrasound permitted verification of a left infundibular
pregnancy missed on abdominal scanning in another woman (hCG titer 4146 mIU/mL) Fig. 5. The increased sensitivity of transvaginal (right) versus transabdominal (left) ultrasonography in detecting an ectopic pregnancy. A. Proximity to the cul-de-sac allowed detection of this ectopic gestation (hCG
titer 880 mIU/mL) by means of transvaginal ultrasonography in this
patient. B. Transvaginal ultrasound permitted verification of a left infundibular
pregnancy missed on abdominal scanning in another woman (hCG titer 4146 mIU/mL)
|
Vaginal scanning has proved to be more accurate than abdominal scanning
in detecting ectopic pregnancies (90% vs 80%) and cul-de-sac fluid (77% vs 46%) and
in discerning whether the tubal pregnancy has ruptured (76% vs 50%).72 In the transvaginal ultrasonographic evaluation of pregnancy, Bernaschek
and associates,73 using a 5-MHz transducer, proposed a “discriminatory zone” of
an hCG titer of 750 mIU/mL (second International Standard) for the
detection of an intrauterine gestational sac. Unfortunately, using this
proposed criterion and similar ultrasonographic equipment, Fossum and
associates74 may have inadvertently surgically investigated several pregnancies that
proved to be normal intrauterine gestations (Fig. 6). If an hCG titer exceeds 2000 mIU/mL, we now expect to detect an intrauterine
gestational sac using transvaginal ultrasonography.  Fig. 6. Relationship between transvaginal ultrasonographic findings and serum hCG
levels (range and mean ± SEM) using two World Health Organization
standards: the IRP and the second International Standard.(Fossum GT, Davajan V, Kletzky OA: Early detection of pregnancy with transvaginal
ultrasound. Fertil Steril 49:788, 1988. Reprinted with permission
of the publisher, The American Fertility Society) Fig. 6. Relationship between transvaginal ultrasonographic findings and serum hCG
levels (range and mean ± SEM) using two World Health Organization
standards: the IRP and the second International Standard.(Fossum GT, Davajan V, Kletzky OA: Early detection of pregnancy with transvaginal
ultrasound. Fertil Steril 49:788, 1988. Reprinted with permission
of the publisher, The American Fertility Society)
|
Even with the advent of transvaginal ultrasonography, the value of serial
hCG determinations cannot be overemphasized. If hCG titers increase
with time, Table 2 can be used to evaluate the normality of the increase. As a rule of thumb, the
hCG titer should increase by at least 66% of the initial titer
in a 48-hour period of observation.75 On the other hand, in asymptomatic women, declining hCG levels may be
indicative of a nonviable, nondetectable intrauterine gestation. Serum
progesterone values may prove a useful adjunct to hCG titers in distinguishing
a viable intrauterine pregnancy from that of an ectopic or missed
abortion. Accordingly, in two separate reports on 99 women, a progesterone
value less than 15 ng/mL was always predictive either of an
ectopic pregnancy or a nonviable intrauterine gestation.76,77 TABLE 2. Lower Limits of Percentage Increase of Serum hCG
Sampling Interval (Days) | Increase in hCG (%) |
1 | 29 |
2 | 66 |
3 | 114 |
4 | 175 |
5 | 225 | (Kadar N, Caldwell B, Romero R, A method of screening for ectopic pregnancy
and its indications. Obstet Gynecol 58:162, 1980)It should be emphasized that early intrauterine pregnancy failures may
not have enough tissue to be detectable by routine pathologic examination, and
therefore some patients with declining hCG titers will ultimately
prove to have intrauterine pregnancy failures. We recommend laparoscopy for patients with subnormal quantitative increases
of hCG. Normal increments in hCG are monitored until hCG titers exceed
either 2000 mIU/mL or 6500 mIU/mL, at which time either transvaginal
or transabdominal ultrasonography, respectively, may be performed. The
presence or absence of a gestational sac above these hCG levels
should be supportive either of an ectopic or an intrauterine gestation. Finally, if
hCG titers plateau, we perform a diagnostic laparoscopy
because the pattern is often characteristic of an ectopic pregnancy (Fig. 7).  Fig. 7. An algorithm for the management of an ectopic pregnancy. Fig. 7. An algorithm for the management of an ectopic pregnancy.
|
|