Death due to a pregnancy-related cause during reproductive life occurs in 1 in 21 women in Africa (compared to the 1 in 15,000 lifetime maternal mortality in the United States).20 Little is known regarding the precise role of infibulation in maternal mortality, but infibulation does contribute to obstetric difficulties.
A British clinic recently performed antepartum deinfibulation to allow pelvic examinations and delivery without anterior episiotomy.33 This is not common practice, and even when offered, most patients refuse and want to wait until delivery for the deinfibulation. This makes pelvic examination difficult, and obstetric dating often must be augmented with ultrasound studies. Deinfibulation is recommended in the first trimester so that digital examinations can be used to monitor cervical dilation during labor, eliminating the need for rectal examinations to monitor cervical dilation.
In a comparison of the obstetric outcomes of infibulated women to noncircumcised women in a Saudi Arabia hospital, infibulation did not appear to affect the first stage of labor because it did not interfere with uterine activity or cervical dilation.36 The second stage of labor was significantly prolonged in infibulated women because the infant's head was not easily visible as a result of the obstructing scar at the introitus, which created delays in the cutting of the necessary anterior episiotomy. Infibulation had no effect on the rate of instrumented delivery.33,36
Infibulated women had a significantly higher rate of hemorrhage secondary to both an anterior episiotomy and the use of the mediolateral episiotomy to prevent fourth-degree extensions.36,37 The unyielding scar tends to cause a greater degree of perineal tearing. A timely anterior episiotomy by trained personnel appears to avoid obstructed labors, and hence tissue necrosis, vesicovaginal and rectovaginal fistulas, uterine rupture, and infant trauma.36,38 In a recent report on female genital mutilation, 46% of multiparas delivered with intact perinea, and more than 90% of primiparas delivered vaginally (Fig. 1).33
|
A word of caution is necessary regarding cesarean section for recent African immigrants. The surgeon may need to hold extensive discussions with the patient and her family about the need for the surgery. For example, the woman may wrongly think that she is being advised to have a cesarean section because the physician is hesitant to perform an episiotomy on the circumcision scar, rather than the multitude of reasons for which cesarean sections are performed in developed countries. The concept of surgical intervention for the infant's well-being is unfamiliar to many of these women. Informed consent may also be a foreign concept. It is often wise for the obstetrician to discuss the many reasons for a cesarean section before labor ensues, as well as the implications of not performing a cesarean section, so that he or she may develop an understanding of the particular wishes of the patient and her family before an emergent need arises for operative consent.
Before cesarean section or forceps delivery, placement of a urinary catheter is required to reduce complications. Catheter insertion can be performed similar to intrauterine pressure catheter introduction, using palpation and blind guidance of the catheter into the urethra. If necessary, early anterior episiotomy can be performed.
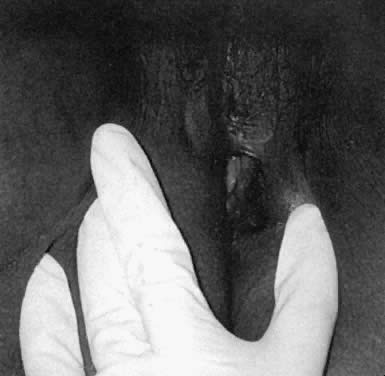
To perform an anterior episiotomy, a finger is introduced into the introitus and the vulvar skin diaphragm is elevated and cut with scissors or a scalpel using the finger to protect the underlying tissue, particularly the urethral meatus.38,39 This widens the introitus and exposes the urethral opening. The cut should be performed only when the head is crowning on the perineum to stretch the tissues. However, the cut should be made before tears begin because the scar has little elasticity, and extensions are common if the head is not well controlled. For additional room, a routine posterior episiotomy can be made. A mediolateral episiotomy also should be considered, since this is often the practice in Africa to avoid rectal tears. Despite counseling about the risks of excess bleeding, pain, and extensions, African women in our clinic tend to insist on a mediolateral cut rather than a posterior midline episiotomy.
After delivery, if the woman chooses to leave the scar tissue open, the two edges of the anterior episiotomy incision can be oversewn with a loose running or interrupted absorbable suture, if needed for hemostasis. The woman is instructed on twice-daily sitz baths and on keeping the scar edges open with mechanical separation with an open gauze during washing. Topical application of estrogen can be applied in lactating women. If the woman chooses to have the edges of her circumcision scar reapproximated, then any bleeding edges can be sutured together with a single subcuticular layer of running absorbable suture. A continuous suture minimizes the development of a fistula in the linear vulvar scar due to the pressure of urination. Even with reapproximation, the introital opening is always larger than it was before delivery because the anterior episiotomy is not cut until after pushing and stretching of the perineum.
Repair of an anterior episiotomy at the time of delivery is illegal in the United Kingdom because it is considered a reinfibulation. Toubia6 described circular stitches over the edges of the cut labia majora scar, but did not discuss or illustrate in the diagrams the point that the scar edges are flaps, rather than flat surfaces. Because no tissue is excised or removed at delivery, oversewing the edges leaves two flaps of scar tissue that are not labia. The rate of spontaneous reformation of the midline scar is high when the woman does not take precautions to avoid reagglutination. The practice of nonobstetric reinfibulation between deliveries or to hide the loss of virginity is not advised, as it will create additional scar tissue and potential complications.10,20,25
Since many women with infibulation FC are Muslim, it is helpful to be familiar with Islamic requirements such as Ramadan. This is a time of daily fasting from sunrise to sunset for the entire ninth month of the Islamic calendar.15,28 Vaginal examinations are forbidden when fasting. Pregnant women are excluded from required fasts, but they will often fast to attain the state of purity. A common request is for all care givers, including physicians, to be female, but it is important to know that this is not an Islamic law; women can be treated by a “trustworthy” male physician when there is no female physician available and the case cannot be delayed.28