Circumcision is commonly performed with the use of either specially designed clamps or disposable plastic stents. Instruments commonly employed include the Gomco (Yellen)114 and Mogen clamps and the Plastibell. All of these devices are designed to isolate the foreskin from underlying structures, protecting the glans from injury. These devices are used most frequently, but many other specialized instruments for circumcision have been described.5
In this section, circumcision with the Gomco clamp is discussed in detail. Much of the illustrated technique is the same, regardless of the type of clamp or stent chosen. As with other operative procedures, surgeons should master one technique fully, develop familiarity with an alternative approach for unusual circumstances and be prepared to manage complications. Regardless of the surgical method chosen, the requirements for initial parental counseling and consent, the appropriate choice of cases, meticulous aseptic technique, and adequate analgesia remain the same.
Pain Perception and Anesthetic Technique
There is good evidence that neonates perceive pain. Neonates respond to the stress of unanesthetized circumcision by increased cortisol levels115,116,117 and various changes in biophysical behavior.118,119,120,121,122 Not surprisingly, neonates who receive adequate anesthesia or analgesia while undergoing circumcision cry less, are less agitated and have less perturbation in other biophysical parameters than those without.115,123,126 How best to achieve safe and adequate pain relief is the issue.
A brief review of the anatomy of the nerves to the penis is helpful in understanding modern techniques for blocking the perception of pain. Anatomically, the nerves serving the penis include the pudendal (S2-S4) nerve and the pelvic anatomic plexus. The principal nerve supply to the prepuce is provided by the dorsal branches of the pudendal nerve. At the penile root, the dorsal nerves, arteries, and veins are located anteriorly at the 2- and 10-o'clock positions, and lie 3 to 5 mm beneath the skin (Fig. 1). Ramifications of the nerve begin approximately 1 cm beyond the penile root. Thus, to be successful, a nerve block needs to be given anteriorly at the penile base, with particular attention to the avoidance of vascular injury. It also is possible to inject an anesthetic for a purely local block, as opposed to a nerve block127 or to apply a local anesthetic as a cream or gel.128,129 The latter technique is discussed in greater detail below.
|
The routine use of an anesthetic for circumcision is strongly encouraged because substantial data now exists documenting safety. The literature includes descriptions of a number of simple techniques employing either local, injectable anesthetics or anesthetic creams or ointments. Several recommendations are discussed below.
For several years we have employed a penile block technique using 0.5 mL or less of 1% or 0.5% lidocaine without epinephrine administered via a tuberculin syringe fitted with a fine-gauge needle (26 to 27 gauge). We usually dilute the standard 1% lidocaine solution with an equal volume of sterile saline and mix by tilting the syringe. The skin around the base of the penile shaft is then cleansed, and a bleb of 0.2 to 0.4 mL of the 0.5% (or 1%. if preferred/lidocaine solution is injected subcutaneously at the 10- and 2-o'clock positions on both sides of the dorsal shaft123,126,130,131 (see Fig. 1). These injections usually result in a dense local block in 80% to 90% of cases; however, it is important to wait for 3 to 5 minutes after the drug is administered until the block is fully developed. As a practical matter, we usually prepare the lidocaine solution and make the injections as the first part of the procedure. Then we prep the operative field, open the surgical kit, and arrange the instruments. Because these preliminaries consume several rainutes, the anesthesia block usually is established by the time the surgeon is prepared to proceed with the operation.
Although injected local anesthetic has been used successfully for nerve block in a large number of cases with minimal evidence of complications, some cautions are in order.115,120,121,122,123,124,126,131,132 The operator must be certain not to inject the drug into either the dorsal vein or artery because this could lead to adverse systemic reactions. Epinephrine containing solutions should never be used because of the possible risk of inducing acute penile ischemia.132 Only lidocaine should be used for injection, and the total volume should not exceed 1 mL of the 1% solution. Substantial data suggest that this dose is safe. Fontaine and co-workers124 have reported on 1022 cases of lidocaine dorsal nerve block. In this series, no instances of lidocaine toxicity, vascular compression, or voiding delays were observed. The complication rate was 1.2%. The problems consisted of 11 instances of minor, local ecchymoses at the injection site, with 1 case involving more significant bleeding. All of these proved to be of trivial clinical consequence.
Published experience with drugs other than lidocaine for neonatal circumcision is minimal.123 Hematomas and gangrene of the skin at the glands have been reported when bupivacalne was used for a dorsal penile block.134 These cases involved older children (13 months and 3 years) undergoing circumcision with general anesthesia. The children subsequently received dorsal local anesthesia blocks for postoperative analgesia. In these cases, it is unclear whether it was the agent used, the technique of administration (i.e., vessel compression by use of excessive volume), or the surgical events that were responsible for the observed complications.134 Local injection of another local anesthetic, prilocalne, has been associated with methemoglobinemia.135,136 The use of this drug as an injectable anesthetic should be avoided.
Topical anesthetics using either 30% lidocaine cream126 or a eutectic mixture (i.e., with a melting point less than room temperature) of 2.5% prilocaine and 2.5% lidocalne prepared as an emulsion (EMLA Cream)137 also have been reported to be effective for circumcision.129 In this technique, approximately 0,1 mL EMLA cream is applied directly to the prepuce with a swab. The area treated is then covered with a lightly occlusive gauze dressing and left for 45 to 60 minutes before the procedure is attempted?9 As noted above, local injections of prilocaine should not be performed because of the risk of methemoglobinemia. It is unclear whether sufficient absorption of EMLA cream might present the same risk in certain patients. So far, such complications have not been reported with the cream, but caution in the use of this preparation is necessary until larger series are reported. This topical technique has yet to be compared directly in adequate patient numbers for both efficacy and safety (specifically systemic absorption of drug) with the technique of lidocaine dorsal nerve blockade (described above). Nonetheless, the initial results are encouraging, and some of these methods may find a place in standard practice.129,138
There are other possible alternatives to the use of an injectable or topical anesthetic. Blass and Hoffmeyer139 described the use of a sucrose-flavored pacifier during circumcision. This technique appears to have some efficacy—at least as reflected in the observation of reduced neonatal crying during the procedure. Whether the positive effect observed was due to the sucrose acting by opioid mediation or to the benefits of nonnutritive sucking is less clear.127 Oral acetaminophen (10 to 15 mg/kg orally or 15 to 20 mg/kg rectally) also can be used to reduce postoperative pain. This compound has the advantage of proven efficacy and safety for treatment of noncircumcision-related pain.140 The one available placebo-controlled study of acetaminophen conducted in neonales undergoing circumcision, however, indicates that the drug is ineffective for operative and immediate postoperative discomfort, whereas it does retain some efficacy in controlling the discomfort that occurs several hours after surgery.143
There are several simple precautions to follow if an injectable local anesthetic is used. Only non-epinephrine-containing solutions are used. The needle must neither enter the dorsal vein of the penis nor penetrate into the shaft itself. When the needle is inserted into the correct subcutaneous plane lateral to the penile shaft, the tip is easily movable, and little, if any, resistance to injection is noted when the plunger of the syringe is depressed. The needle tip should not be advanced beyond 0.5 cm below the skin surface. Care must also be taken to inject only small volumes of fluid, avoiding vessel injury by direct compression. The vessels at the site of injection are in a restricted compartment, and interference with penile circulation, though rare, is a possible complication if too large a volume is vigorously injected.34
Preoperative Management of the Neonate
Once an anesthetic has been chosen and administered, several other steps should be taken. Traditionally, to reduce the possibility of vomiting or aspiration, the child is denied oral intake for at least 1 hour preceding the operation. This is a reasonable precaution that we generally follow, but for which no reliable data exist. Not all experienced clinicians, however, follow this practice. Holding a neonate NPO for an excessive period of time may well be unnecessary, and hunger can contribute to the child's overall distress.21 The easiest way to proceed is to simply perform the operation prior to the next feeding.
Positioning of the infant for the procedure is important. Some of the discomfort the infant experiences during circumcision is due to restriction of his or her movement and exposure to cold. When available, we prefer to use a plastic circumcision board fitted with Velcro restraints. Only the legs are restrained, not the upper extremities. Arm movement does not interfere with the procedure; rather, infants appear to be less distressed when their arms are free. The circumcision board is positioned under a radiant heat source if available, to maintain warmth. If the restraint board is either not available or not desired, an assistant may simply hold the infant in a supine, frog-legged position for the operation. We favor having an assistant present during the procedure. The assistant provides either a finger or a pacifier to help soothe and reassure the infant during the operation and obtains additional equipment or dressings for the surgeon, if required.
Surgical Technique
An important responsibility of the surgeon is to check the surgical instruments before beginning the procedure. The Gomco clamp includes a number of parts (bell, base, top plate with yoke, nut), and the operator should be confident that all are present and working correctly. Several technical problems may be encountered with the clamp, requiring the surgeon to request a new instrument before the surgery is attempted. The bell may become nicked or grooved by heavy use, the base plate may warp with age, the screw threads may not work easily, or the clamp may have been assembled with an incorrect bell size for the clamp base. Any of these reasons should prompt the surgeon to reject the clamp and request a replacement.
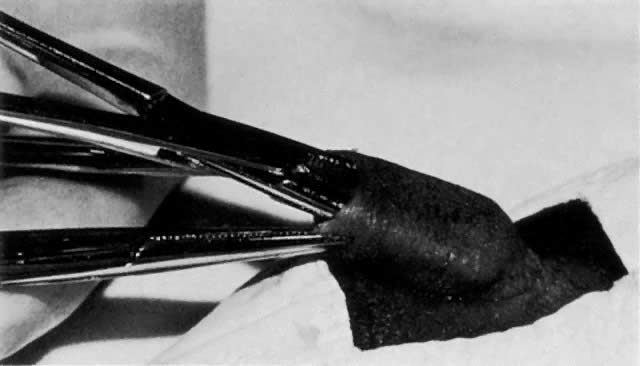
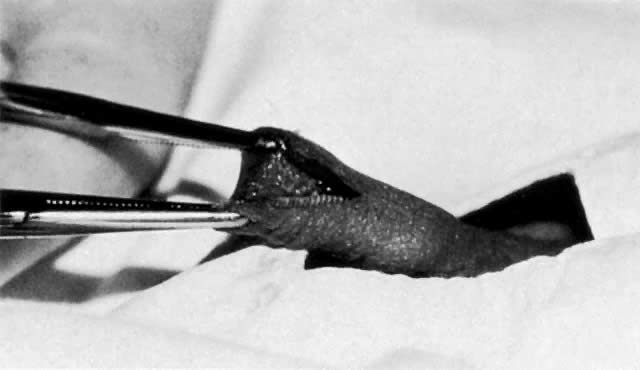
After correct positioning of the child is ensured, the genitalia are cleansed with a povidone-iodine solution. After the anesthetic is administered and the instruments are checked, the surgeon proceeds with the operation. The operative field is draped. We favor a small triangular drape with a circular hole for the phallus. The extreme edges of the foreskin are first grasped with mosquito clamps, carefully avoiding trauma to the glands. Next, the plane between the glands and foreskin is developed by gentle dissection using a blunt probe or hemostat tip (Fig. 2). A dorsal slit is then performed. Using a straight mosquito-type hemostat, the anterior foreskin is crushed longitudinally in the midline. The clamp is removed, and the compressed area is divided with scissors. Because the clamp crushes the tissue, this is usually a bloodless incision (Fig. 3). In making the dorsal slit, close attention is paid to the posterior blade of the scissors to avoid damage to the meatus, which can result in a hypospadias or epispadias or possibly predispose the infant to subsequent fistula formation.21 Care is necessary in applying this initial clamp for another reason: The indentation made by the mosquito clamp for the dorsal slit serves as the marker for the length of skin to be excised from the shaft. The foreskin is quite flaccid and it is easy to mobilize excessive tissue, leading to an overestimate of the extent of skin to be drawn up in the Gomco clamp and removed. Excision of too much tissue results in inadvertent denuding of the shaft, which can necessitate secondary suturing. Kaplan6 described an alternative technique to judge the length of skin to be removed: The location of the coronal sulcus is first marked on the skin of the penis with a pen before beginning the operation.
|
|
Once the dorsal slit is performed, the skin edges are grasped with fine-bladed clamps. The Gomco clamp bell is next inserted under the incised prepuce, entering the potential space between the glands and foreskin (Fig. 4). Usually some twisting and maneuvering is necessary to set the bell correctly. If the usually available bell size (1.3 cm) is too large, the smaller (1.1 cm) size clamp is substituted. The correct bell size for the overwhelming majority of neonates is 1.3 cm. The 1.1 cm bell is uncommonly needed; the 1.6-era clamp size is also available, but is virtually never required for neonatal procedures.
|

When correctly applied, the rim of the Gomco Bell lies below the apex of the original dorsal slit, slightly distending the prepuce. Once the bell is in place, the clamp is assembled. The foreskin is carefully drawn up between the bell and body of the clamp using the mosquito hemostats. Once the Gomco is fully assembled and before compression is applied, the operator checks to be certain that the full length of foreskin marked by the original dorsal slit is drawn into the clamp and that the application is symmetric. If the apex of the original dorsal slit is not included in the skin removed, an unsightly cleft and a site for potential bleeding results. Once the surgeon is satisfied, and after assuring that the foot of the clamp is correctly inserted into the base plate, the finger nut of the clamp is firmly screwed in place. This crushes the foreskin between the bell and body of the clamp. The isolated, avascularized foreskin is then excised with a scalpel (Fig. 5). Electrocautery should never be used for this purpose because of the possibility of extensive injury to the penis. The clamp is left in place for several minutes to ensure hemostasis. Operators vary greatly in recommending how long the clamp should be allowed to remain.20 Yellen recommended waiting for 5 minutes114; however, many surgeons remove the clamp immediately after completing the procedure.
|

After the clamp is disassembled and the bell teased off, the glands and shaft are observed carefully. Slight oozing is common. Persistent oozing from the glans is a common, minor complication due to the disruption of small vascular connections between the glans and the prepuce. Gentle pressure with a saline-moistened sponge for 2 to 5 minutes usually controls the ooze. Direct suturing of the glands is counterproductive and not recommended. Bleeding from the foreskin edge that is not responsive to simple pressure is best controlled by silver nitrate sticks, oxidized cellulose piedgets, or thrombin applications combined with gentle pressure. If bleeding still persists, which is uncommon, the placement of several small sutures of 5–0 or 6–0 chromic or polyglycolic acid may be necessary. Suturing also is indicated if the skin edge has drawn away from the corona, revealing a raw or denuded area on the penile shaft. For many years bleeding that was unresponsive to simple pressure was treated with topical applications of epinephrine (solutions of 1: 10,000 or less), applied to the gauze sponges used for compression. Recently, a controversy has developed about the routine use of such epinephrine-soaked sponges to control bleeding. An uncommon complication of this procedure is absorption, and systemic symptoms or evidence of local ischemia have been observed.142,145 Such untoward reactions from local epinephrine applications are rare; however, we believe that simple, direct pressure and selective suturing remain the best treatments for postcircumcision bleeding, and conclude that epinephrine solutions should be used sparingly, if at all (see section on Complications of Circumcision, below).
Once hemostasis is adequate, a nonocclusive gauze dressing impregnated with petroleum jelly is simply wound loosely around the penile shaft and glands to prevent adherence of the operative field to the diaper (Fig. 6). A constrictive dressing has the potential to obstruct either normal urination or penile blood flow.21,146 The child is then comforted, rediapered, and returned to the mother for holding or feeding. Normally, we intermittently observe the operative site for 1 hour to be certain that hemostasis is adequate.
|

Providing the family with a prepared form Outlining care of the penis during the healing phase is good practice.21 The parents are encouraged to call if questions or problems occur within the next 24 to 48 hours. Circumcisions normally heal within several days. No specific care is required other than simply light washing. The best practice is to leave the original dressing on until it falls off. For several days, petroleum jelly or A and D ointment is applied lightly to the glands every time the diaper is changed. Parents should be instructed that adherent serum or clot are not to be vigorously removed from the penis, but should simply be allowed to spontaneously dissolve. Petroleum jelly or A and D ointment from unit dose foil packets is applied to the glans as a dressing during the healing phase.
Circumcision also can be performed without the use of a crushing clamp. The Plastibell stent can be employed, or a “freehand” technique similar to that illustrated by Howat can be used.39 The latter technique is sometimes necessary if the circumcision is performed on a small child. In occasional cases where the infant's genitals are small, even the 1.1-cm Gomco clamp may prove simply too large. The best technique in such cases is to advance the foreskin beyond the glands and to crossclamp it, with special attention paid to avoiding injury to the unprotected glans. The redundant skin is then excised, and the operative site is examined for bleeding.