The specific cytomorphologic features of lesions in a variety of body sites
will follow; however, general cytomorphologic criteria of malignancy
for epithelial lesions are presented here. The most useful diagnostic
criterion applied to FNA specimens is cellularity, as nearly all neoplasms (particularly
malignancies) yield cellular specimens on aspiration, whereas
aspirates of nonneoplastic lesions and some benign neoplasms
are hypocellular. Another useful diagnostic criterion is that of
architectural complexity within intact tissue fragments. Although the
practice of cytology is generally thought to rely entirely on evaluation
of subtle cellular and nuclear details, large tissue fragments are
often present in FNA biopsy specimens of epithelial lesions and contain
valuable information. In general, normal parenchyma and benign epithelial
lesions are characterized by architecturally “flat,” two-dimensional
fragments with well-organized and uniformly spaced nuclei (Fig. 2A), whereas malignant epithelial neoplasms generally yield complex, three-dimensional
fragments with significant nuclear overlap and disorganization (Fig. 2B). Obviously, all cases must be evaluated for conventional nuclear criteria
of malignancy, including variation in nuclear size, shape, and chromatin
pattern in adjacent cells. In addition, nuclear membrane abnormalities, altered
chromatin distribution (including both hypochromasia
and hyperchromasia), and elevated nucleus-to-cytoplasm ratios are important
features of malignancy in individual cells (Fig. 3).22 General cytologic features of commonly encountered lesions in the breast, lymph
nodes, gynecologic tract, and pelvis will be presented. |
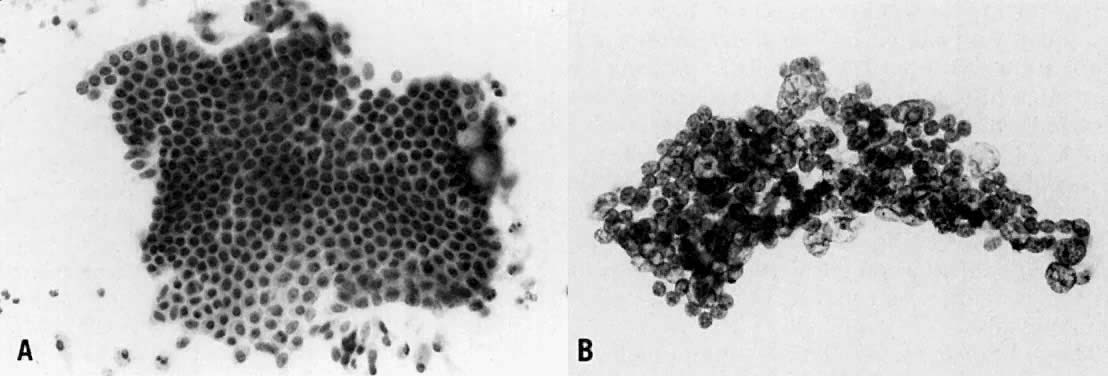 Fig. 2. ( A) Well-organized, 2D tissue fragment typical of benign glandular epithelium (stain, Papanicolaou) in contrast to ( B) architecturally crowded, 3D tissue fragment from case of adenocarcinoma
showing complete loss of cellular polarization and organization (stain, Papanicolaou).
Fig. 2. ( A) Well-organized, 2D tissue fragment typical of benign glandular epithelium (stain, Papanicolaou) in contrast to ( B) architecturally crowded, 3D tissue fragment from case of adenocarcinoma
showing complete loss of cellular polarization and organization (stain, Papanicolaou).
|
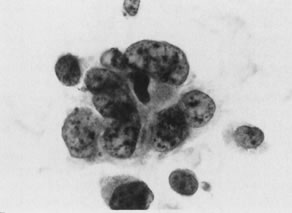 Fig. 3. Cytologic criteria of malignancy are shown in this case of transitional
cell carcinoma. Adjacent cells show significant variation in nuclear
size and shape; individual nuclei display abnormal chromatin distribution
and nuclear membrane irregularities (stain, Papanicolaou). Fig. 3. Cytologic criteria of malignancy are shown in this case of transitional
cell carcinoma. Adjacent cells show significant variation in nuclear
size and shape; individual nuclei display abnormal chromatin distribution
and nuclear membrane irregularities (stain, Papanicolaou).
|
Breast Fine-needle aspiration is a reliable and cost-effective tool in the evaluation
of palpable and nonpalpable breast masses.23–26 The combination of physical examination, imaging findings (mammography
or ultrasound or both), and cytologic examination, known as the triple
test, has a diagnostic accuracy reported to be greater than 95% when
all three elements of the test are concordant.27–32 Current recommendations for patients undergoing the triple test are as
follows: - If all three tests are compatible with a benign process, the patient may
simply be followed clinically, with close observation.
- If all three tests are compatible with malignancy, the patient may undergo
definitive therapy.
- If there is a mixed or inconclusive triple test result (i.e., one or two
of the tests suggest malignancy), excisional biopsy of the index nodule
should be performed.33,34
The breast lesions most commonly encountered in FNA specimens are nonneoplastic
masses, best classified as fibrocystic change. Aspirates from
these lesions generally contain foam cells (histiocytes) and proteinaceous
debris, consistent with cyst contents. In addition, most aspirates
contain relatively few fragments of ductal epithelium, all of which
are tightly cohesive, composed of small, well-organized nuclei and a
distinct second cell population (myoepithelial cells); apocrine metaplasia, characterized
by abundant granular cytoplasm, is also commonly encountered (Fig. 4). Occasional cases of fibrocystic change with ductal hyperplasia may yield
increased numbers of ductal epithelial tissue fragments, often with
some nuclear enlargement and overlap. Such findings, in the absence
of worrisome clinical or mammographic findings, warrant simple observation
rather than surgical intervention. 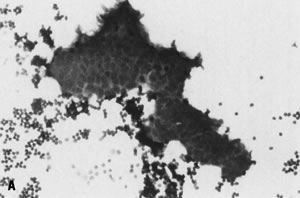 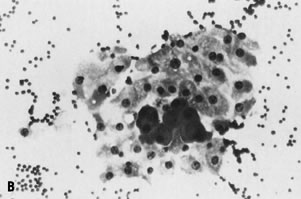 Fig. 4. Fine-needle aspiration of fibrocystic change of breast often yields ( A) few cohesive fragments of benign ductal epithelium (stain, Diff-Quik) and ( B) fragments of apocrine metaplasia (stain, Diff-Quik); proteinaceous debris
may also be seen in cystic lesions. Fig. 4. Fine-needle aspiration of fibrocystic change of breast often yields ( A) few cohesive fragments of benign ductal epithelium (stain, Diff-Quik) and ( B) fragments of apocrine metaplasia (stain, Diff-Quik); proteinaceous debris
may also be seen in cystic lesions.
|
The question of the need for pathologic examination of cyst fluid from
clinically benign breast lesions should be addressed. There are two patient
groups in whom one might argue against routine cytologic evaluation
of all cases: (1) those whose fluid is clear, and (2) those who have
total resolution of the lesion with no residual mass. Patients in whom
this is not the case, however (e.g., those who have opaque or bloody
fluid or in whom a mass remains), should have all aspirated material
sent for pathologic examination as well as additional sampling to rule
out a cystic malignancy.33,35,36 Another benign breast lesion often encountered in FNA specimens, particularly
in the younger patient population, is fibroadenoma. Considered
a true neoplasm, this lesion is composed of both an epithelial and a stromal
component, which should be represented in aspirate smears. The
epithelial component is classically composed of numerous cohesive antler-shaped
tissue fragments, often with some proliferative changes (nuclear
enlargement and overlap). The stromal component is typically represented
by stripped ovoid naked nuclei in the background, often referred
to as bipolar cells. In addition, intact stromal fragments, often with myxoid changes, may
be observed in occasional cases. A combination of these findings, in
the context of the typical clinical findings of a well-circumscribed, movable, rubbery
mass, is diagnostic of fibroadenoma. Papillary lesions in the breast are a frequent source of indeterminate
cytologic diagnoses when aspirated. Both papilloma (a proliferative, benign
lesion) and papillary carcinoma (a malignant lesion) yield hypercellular
aspirate smears, which contain numerous intact tissue fragments
as well as numerous single, intact epithelial cells that are often
columnar in shape.37,38 Because of the cytomorphologic overlap of these entities, such findings
generally result in an FNA diagnosis of “papillary lesion,” with
surgical excision recommended for definitive histologic classification. Although
some reports have attempted to establish criteria
for reliably separating benign from malignant papillary lesions,39 a conservative approach should be adopted in these cases. Carcinoma of the breast may be reliably diagnosed by FNA in the presence
of three criteria: (1) hypercellularity; (2) dyscohesion, defined as
significant numbers of intact single cells; and (3) lack of a second (myoepithelial) cell
population in intact tissue fragments (Fig. 5). Strict adherence to these criteria results in an extremely high specificity
for the diagnosis of breast carcinoma. Aspiration of some tumor
subtypes, such as lobular and tubular carcinoma, may yield material
that may not fulfill all criteria of malignancy, resulting in a “suspicious” diagnosis and a recommendation for surgical biopsy
and histologic confirmation. Nuclear grading may be performed on FNA smears
and correlates well with nuclear grading of the subsequently resected
tumors.40–43 Immunocytochemical stains for the presence of hormone receptors (e.g., estrogen, progesterone) may be performed on cytologic or cell-block material
or both obtained from the FNA of a primary breast tumor or metastatic
lesions.44–47 Assessment of c-erbB2/Her-2/neu overexpression may be analyzed by immunohistochemistry
or fluorescence in situ hybridization on aspirate samples, which may provide important prognostic
information for presurgical treatment planning.48–51 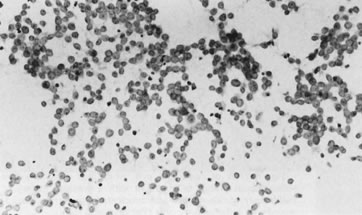 Fig. 5. Fine-needle aspiration of adenocarcinoma of breast typically yields hypercellular
smears containing a single population of dyscohesive epithelial
cells (stain, Papanicolaou). Fig. 5. Fine-needle aspiration of adenocarcinoma of breast typically yields hypercellular
smears containing a single population of dyscohesive epithelial
cells (stain, Papanicolaou).
|
There are some limitations of FNA of the breast that should be recognized. Although
many breast tumor subtypes display classic histologic features, the
accurate subclassification of tumor subtype (i.e., ductal, lobular, or
medullary carcinoma) cannot be performed consistently based
on simple cytomorphologic criteria alone. In addition, the determination
of tumor invasion cannot be made based on cytologic smears and requires
definitive histologic demonstration of stromal invasion; thus, the
FNA diagnosis of “adenocarcinoma” in the breast encompasses in situ and invasive carcinoma.52 In some cases, particularly image-guided FNA of nonpalpable breast lesions, the
addition of core needle biopsy may result in improved diagnostic
accuracy.53–55 Finally, as with FNA in any site, clinical findings must be taken into
account. Thus, a positive FNA diagnosis in the breast in the context
of suspicious clinical or mammographic findings or both is sufficient
for definitive therapy, whereas a negative FNA diagnosis in the presence
of such findings requires further evaluation to rule out an unsampled
or low-grade malignancy. Soft Tissue and Subcutaneous Lesions Fine-needle aspiration represents an extremely useful diagnostic technique
for patients with a soft tissue or subcutaneous nodule, particularly
in the presence of a history of malignancy. Exclusion of metastatic
disease is obviously of paramount importance to the patient and clinician. Positive
cases are easily recognized but require comparison with
previous histologic or cytologic material for confirmation of metastasis (Fig. 6A, B). In contrast, multiple samples by an experienced aspirator without evidence
of malignancy is generally sufficient to exclude metastasis. In
addition to the absence of malignancy, however, an explanation for the
presence of a mass lesion is generally reassuring for both patient and
clinician. Simple keratinous or epidermal inclusion cysts and fat necrosis
are two such entities that are often seen in aspirate specimens
in this clinical setting. Keratinous cysts generally yield benign and
anucleated squamous cells admixed with debris and variable numbers of
acute inflammatory cells (Fig. 7). Aspiration of fat necrosis, which may appear clinically suspicious, yields
only histiocytes and granular debris, sometimes admixed with fragments
of mature adipose tissue. Identification of the diagnostic features
of either of these entities allows conservative management and simple
observation. 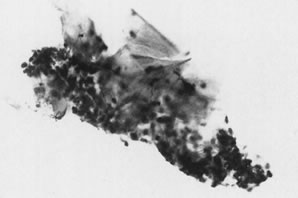 Fig. 7. Fine-needle aspiration of keratinous cyst presenting as firm subcutaneous
nodule in patient with a history of malignancy yields mature and anucleated
squamous cells admixed with inflammatory cells (stain, Papanicolaou). Fig. 7. Fine-needle aspiration of keratinous cyst presenting as firm subcutaneous
nodule in patient with a history of malignancy yields mature and anucleated
squamous cells admixed with inflammatory cells (stain, Papanicolaou).
|
Lymph Nodes The FNA of lymph nodes, regardless of their location, is generally performed
to determine whether their enlargement is because of (1) a benign, reactive
process that can be treated conservatively; (2) a neoplastic
hematopoietic process (lymphoma) that may require excisional biopsy
for further subclassification and subsequent treatment; or (3) a neoplastic
nonhematopoietic process (e.g., metastatic carcinoma, melanoma, sarcoma)that
may require an extensive workup to identify a potential
primary site. Both palpable and deep-seated lymph nodes may harbor any
of these processes, and FNA represents a cost-effective approach to their
diagnostic evaluation.56–58 Benign, reactive conditions generally yield cellular specimens composed
of a dyscohesive (i.e., single cell) population of lymphoid cells. Lymphocytes
in a number of different states of activation are present, including
small mature lymphocytes, large activated cells, immunoblasts, and
plasma cells, resulting in the classic polymorphous population of
lymphocytes indicative of a reactive condition (Fig. 8A).59 Histiocytes may also be present, often with ingested intracytoplasmic
cellular debris (“tingible body” macrophages) and also suggest
a reactive process. In contrast, aspirates of lymphoma yield a dyscohesive
population of lymphoid cells in an abnormal distribution, with
one subpopulation in dominance, resulting in the classic monotonous
population typical of malignant lymphoma (Fig. 8B). Such a monotonous population of small, intermediate, or large lymphoid
cells without the accompanying cell types just described is highly
suggestive of lymphoma.59 Material from an FNA may be submitted for immunophenotyping by flow cytometry, in
the hopes of objectively showing a monotypic cell population, consistent
with malignancy. Although surgical biopsy may be required
for further subclassification of some types of lymphoma, FNA with flow
cytometry may be used for diagnosing and subclassifying cases of primary
and recurrent non-Hodgkin lymphoma.60–63 Such an approach is particularly appropriate for deep-seated masses in
which open biopsy is technically difficult and perhaps even contraindicated
in debilitated patients. 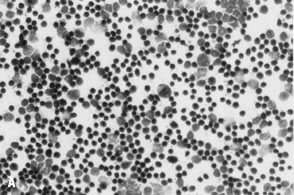 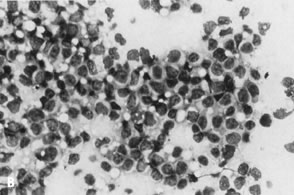 Fig. 8. ( A) Fine-needle aspiration (FNA) of reactive lymph node shows polymorphous
population of small, mature lymphocytes and larger activated lymphoid
cells, consistent with lymphoid hyperplasia (stain, Diff-Quik); compare
with ( B) FNA of malignant lymphoma displaying monotonous population of large lymphoid
cells, consistent with large cell lymphoma (stain, Diff-Quik). Fig. 8. ( A) Fine-needle aspiration (FNA) of reactive lymph node shows polymorphous
population of small, mature lymphocytes and larger activated lymphoid
cells, consistent with lymphoid hyperplasia (stain, Diff-Quik); compare
with ( B) FNA of malignant lymphoma displaying monotonous population of large lymphoid
cells, consistent with large cell lymphoma (stain, Diff-Quik).
|
Metastatic neoplasms are generally easily recognized in aspirates of enlarged
lymph nodes. A foreign population of nonlymphoid cells is usually
obvious, often with an admixture of lymphoid cells in the background. Metastatic
carcinoma is by far the most common entity encountered and
yields both single tumor cells and cohesive tissue fragments of various
sizes. Nuclear and architectural atypia, as described earlier, should
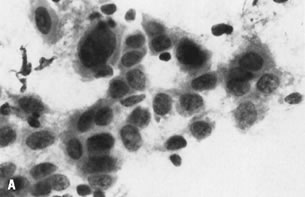
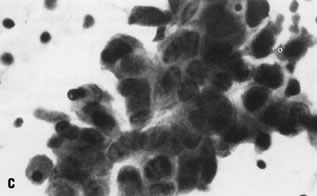
be present and may be profound in poorly differentiated malignancies (Fig. 6C). The distinction between squamous carcinoma and adenocarcinoma can often
be made via cytologic preparations, particularly in well-differentiated
tumors. Cells of squamous carcinoma generally possess homogenous, dense
cytoplasm with distinct cell boundaries and occasional intercellular
bridges. In addition, streaming or spindling of tumor cells is
often seen in squamous lesions. Finally, keratin pearls may also be seen
in some cases and are diagnostic of squamous differentiation. Cells
of adenocarcinoma, in contrast, typically display granular or vacuolated
cytoplasm, sometimes with intracytoplasmic mucin secretions. Cell
boundaries are generally indistinct, resulting in tissue fragments with
a syncytial appearance (Fig. 9A), and glandular structures with distinct lumen formation may be seen in
some tissue fragments. It should be noted, however, that a significant
percentage of cases do not show definitive features of either squamous
or glandular differentiation, resulting in a diagnosis of simply “poorly
differentiated carcinoma.” 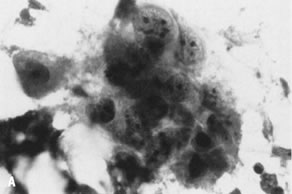 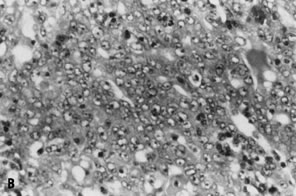 Fig. 9. ( A) Fine-needle aspiration of enlarged inguinal lymph node in patient with
history of endometrial adenocarcinoma shows syncytial fragment of malignant
epithelium with vesicular nuclei and prominent nucleoli, consistent
with metastatic adenocarcinoma (stain,Papanicolaou), morphologically
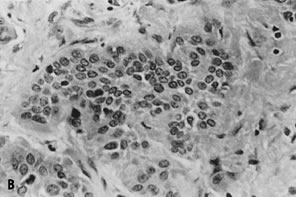
similar to ( B) histologic section of previously resected primary tumor of endometrium (stain, hematoxylin-eosin). Fig. 9. ( A) Fine-needle aspiration of enlarged inguinal lymph node in patient with
history of endometrial adenocarcinoma shows syncytial fragment of malignant
epithelium with vesicular nuclei and prominent nucleoli, consistent
with metastatic adenocarcinoma (stain,Papanicolaou), morphologically
similar to ( B) histologic section of previously resected primary tumor of endometrium (stain, hematoxylin-eosin).
|
Other metastatic neoplasms (e.g., melanoma, sarcoma) are less frequently
encountered in lymph node aspirates. Although special stains (i.e., immunocytochemistry) may
be helpful in this setting, clinical history
is often most useful in these unusual cases. Two sites in which lymphadenopathy must be evaluated in patients with a
history of gynecologic malignancy are the inguinal and supraclavicular
areas. Palpable lymph nodes are present in the inguinal region of most
persons and simply represent chronically stimulated nodes with a variable
degree of fibrosis and fatty replacement. In the presence of a
history of malignancy, however, the possibility of metastatic disease
must be excluded for any mass larger than the typical shotty node; FNA is perfectly suited to such a clinical setting (Fig. 9).64 Enlarged supraclavicular lymph nodes should always be viewed with high
clinical suspicion, particularly in the oncologic patient population. FNA
in this location is easily performed and can reliably establish the
presence of metastatic disease.65–68 Deep-seated lymph nodes aspirated under radiologic guidance in the gynecologic
patient population include those in the pelvis and retroperitoneum. Although
ultrasonography69,70 and lymphangiography71,72 have been used to guide aspirates of these lesions, CT guidance has become
increasingly popular because of a number of advantages.73 These include a high degree of accuracy in detecting pathologic changes
in these nodal groups (often superior to lymphangiography)74 and the ability to detect heterogenous tissue densities in pathologic
nodes; such information allows selective sampling of viable, potentially
malignant tissue rather than necrotic debris. Ovary The volume of gynecologic, cytopathologic, and radiologic literature on
the subject of needle aspiration of the ovary has markedly increased
over the past two decades. Despite the expanding literature and increasing
use of the technique, the role of aspiration of the ovaries is still
controversial, with some authors suggesting that aspiration biopsy
of the ovary (except for the purpose of oocyte retrieval) is potentially
dangerous and should not be regarded as a routinely acceptable clinical
practice.75 The arguments against the use of FNA include the possible spillage of
malignant cells into the abdominal cavity, leading to the potential dissemination
of tumor, as well as misdiagnosis related to sampling errors.76 Having noted this opinion, it is important to quickly point out that the
majority of the current literature indicates that the use of needle
aspiration of the ovary is valuable, safe, and even the standard of care
in certain clinical settings, notably in young women who wish to preserve
their ovarian function.77 The technique of FNA is increasingly being used by gynecologists because
of its valuable diagnostic capabilities, its lack of significant morbidity
for the patient, its simplicity of performance, and its diagnostic
rapidity in comparison with conventional surgical excision and processing
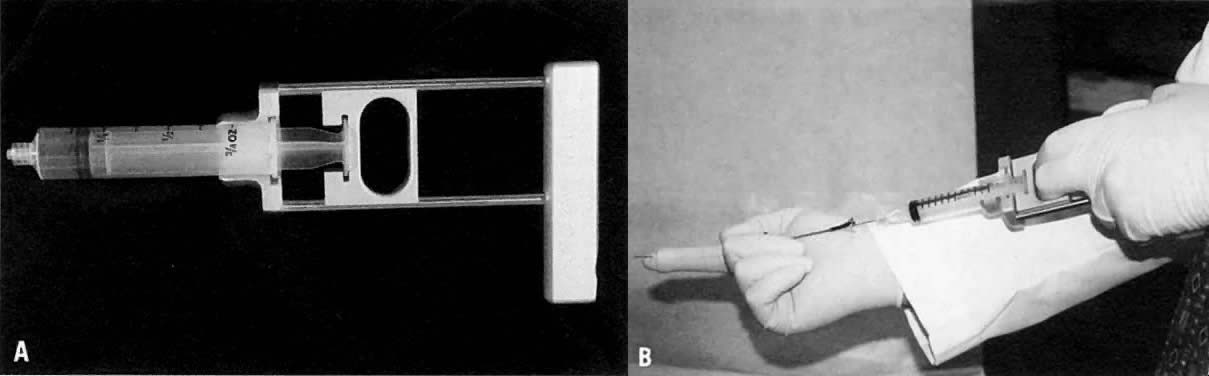
in pathology laboratories.9,78 Aspiration of the ovary can be performed through a transvaginal or transrectal
approach with a sheathed needle guide (e.g., Franzen needle guide; see Fig. 1B). In addition, radiologically (typically ultrasonographically) guided
transabdominal aspiration is possible, as is direct aspiration through
either laparotomy or laparoscopy.9,78 Most ovarian mass lesions in premenopausal women are self-limited functional
cysts.76 Aspiration of such cystic lesions generally yields cytologically accurate
diagnoses and reassurance of the patient while avoiding unnecessary
surgery.79–82 Transvaginal sonographic examination of ovarian masses has led to scoring
systems that are useful for evaluating adnexal lesions before aspiration
or surgical excision. These scoring systems use parameters such
as cystic versus solid nature, smooth-walled versus papillated cyst lining, cyst
wall thickness, presence of septations, and echogenicity. These
systems can be a useful starting point in patient treatment and
reportedly facilitate the distinction between benign lesions (widely accepted
as aspirable) and their malignant ovarian counterparts with a
specificity of 83% and a sensitivity of 100%.83,84 FNA can also be used in young women during laparotomy when only one ovary
is tumor bearing and bilateral oophorectomy is unplanned. Aspiration
of the contralateral ovary may avoid an unnecessary resection and help
reassure both the surgeon and patient.77 Pregnant women constitute a special group of premenopausal patients in
whom cystic ovarian lesions are often noted. As with adnexal lesions in
the general population, ovarian masses in pregnant women are usually
simple (unilocular-to-trilocular) cysts measuring 5 cm or less in diameter. These
cysts are usually functional and resolve spontaneously. The
number of pregnant women reported in the literature who have undergone
aspiration biopsy of the ovary is small; however, most cytologically
studied cases are reported as benign cystic masses.85,86 Pregnant patients should be selected carefully for FNA. Those with a history
of pelvic surgery or pelvic inflammatory disease may be unsuitable
candidates for FNA because of fibrosis, which can produce a hypocellular, nondiagnostic
specimen. Aspiration is suggested when a diagnostic
procedure is indicated and radiologic studies favor a benign process. Ovarian
FNA of a gravid patient should be performed only by an experienced
operator.85 Women presenting for in vitro fertilization (IVF) constitute another subset of young women frequently
noted to have ovarian lesions. Transvaginal ultrasound is routinely
performed in the course of egg retrieval in these patients, and lesions
are generally noted at that time. The recent literature confirms that
the nature of ovarian cysts in IVF patients can be determined in many
cases by the cytologic features of the cysts.87,88 Aspirated material may even help in defining an unsuspected cause of infertility, such
as endometriosis.87 FNA cytology of ovarian cysts in IVF patients can also play a role in
the detection of occult ovarian neoplasms, although detection of malignancies
in this group of patients is rare. Until the exact incidence of
ovarian carcinoma in this subset of patients is known, it would seem
prudent to continue to examine all cyst fluids obtained by needle aspiration.87,88 FNA may be indicated in older patient cohorts as well. For example, the
use of aspiration biopsy is generally accepted (if not indicated) in
that subset of patients with previously documented ovarian malignancy
in whom there is a suspicion of local recurrence.89,90 When a previous diagnosis of malignancy is known, the minimally invasive
technique of aspiration can be of great value in documenting disease
spread and recurrence, with a specificity of up to 100% and a sensitivity
of 96% in one large review.90 Although not generally recommended, the use of aspiration biopsy for the
primary diagnosis and classification of ovarian carcinoma is accurate. For
most nonfollicular cystic lesions, the specificity is reported
at greater than 90%, especially if strict criteria for specimen adequacy
are used and on-site assessment of the specimen is made during aspiration
by a cytopathologist.14,91,92 Because ovarian cancer rarely produces characteristic symptoms or signs
in the early stages, many affected patients present with advanced disease, even
carcinomatosis. In cases of diffuse abdominal involvement, FNA
may be a useful first-line approach to diagnosis, as the potential
for dissemination of disease associated with spillage at the time of
aspiration is of much less clinical import. Early detection of ovarian malignancies markedly improves patient outcomes, with 5-year
survival rates for patients with stage I disease approaching 80% to 85%.93,94 Therefore, early detection of ovarian cancer, especially in young women
with strong family histories, is highly desirable. To benefit this patient
group, protocols designed to screen for ovarian cancer, based on
routine transvaginal sonography complemented by FNA cytology of ovarian
masses, are currently under consideration.77 Only when significant numbers of early cancers are detected will the debate
be resolved regarding efficacy, safety, and risk-to-benefit ratio
of ovarian cyst aspiration.93 Having discussed the indications for FNA of the ovary, let us turn to
the characteristic cytodiagnostic findings and clinicopathologic correlates
associated with the most frequently encountered primary ovarian
lesions. The classification of ovarian tumors is primarily morphologic but is intended
to reflect the current concepts of the embryogenesis of this complex
organ. It is based on the premise that the female gonad is composed
of four major tissue derivatives, all of which are capable of giving
rise to neoplasms: (1) surface, celomic, or germinal epithelium; (2) germ
cells; (3) supporting sex cords; and (4) specialized ovarian stroma.95 Nonneoplastic Ovarian Lesions Appropriate patient treatment requires that all four above-mentioned neoplastic
processes be recognized; however, the majority of ovarian lesions (especially
in the premenopausal population) represent nonneoplastic
changes in the organ. The following is a discussion of a number of
benign (often physiologic or functional) ovarian mass lesions. SIMPLE CYSTIC LESIONS Simple ovarian, paraovarian, serous, epithelial inclusion, paramesonephric, and
paratubal cysts as well as hydrosalpinx are cytologically characterized
by a smear containing only a few epithelial cells in a clear
fluid background.77,96 These entities are often cytologically indistinguishable from one another.29 The cells are generally cuboidal to low columnar and on occasion may possess
cilia.9,77,96,97 The presence of ciliated bodies in the fluids of ovarian cysts indicates
the existence of ciliated columnar epithelial cells on the wall of
the cysts, which excludes the differential diagnosis of cysts of follicular
origin.98 Cilia may also be noted in aspirates from malignant ovarian tumors and
therefore are not pathognomonic of a benign process.98,99 The cellularity may be exceedingly sparse and degenerated with only a
few macrophages, consistent with the cystic nature of these lesions. Hematosalpinx
may present as a simple paraovarian cyst, and aspirated contents
may contain pleomorphic epithelial cells with degenerated erythrocytes
and cellular debris, raising the possibility of a false-positive
diagnosis of malignancy.91 FUNCTIONAL CYSTIC LESIONS (FOLLICULAR AND CORPUS LUTEUM CYSTS) Physiologic (functional) cysts of the ovaries usually appear benign (i.e., thin-walled, unilocular, and not more than 5 cm in diameter) on ultrasound
examination; however, they may mimic malignant tumors.77 Aspirates generally contain follicular cells, typically granulosa cells, arranged
both singly and as tightly cohesive fragments (Fig. 10). These cells house ovoid nuclei with granular chromatin and occasional
nuclear grooves, and they have a small rim of distinct cytoplasm; mitoses
may be present.100 The background of the smear typically shows clear, proteinaceous material
but may be bloody.77 Cyst fluid from functional cysts of folliculogenesis typically have a
high estrogen content. Mulvany and colleagues101 reported a sensitivity of 84% for the detection of follicular cysts by
estrogen assay. As a follicular cyst undergoes luteinization, cytomorphologically
altered granulosa cells appear with prominent nucleoli and
more ample granular cytoplasm.100 Cytoplasmic hyaline droplets may be seen in the corpus luteum of pregnancy.82 On occasion, fluid aspirated from functional cysts may be highly cellular, with
cells featuring high nuclear-to-cytoplasmic ratios and hyperchromasia; papillary
clusters and even small glandular structures may
be noted.102,103 Clinical and radiologic impressions, as well as the presence of well-preserved
granulosa cells in the smears, are helpful for reaching the correct
diagnosis.103 The granulosa cells lining follicular cysts are immunohistochemically
negative for cytokeratins, whereas those epithelial neoplasms considered
in the differential diagnosis would be immunoreactive with antibodies
directed against cytokeratins.102 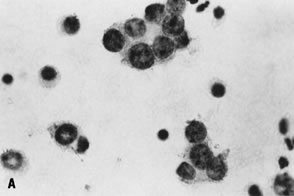 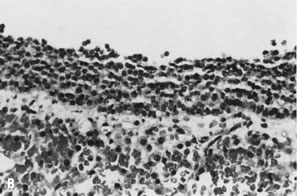 Fig. 10. A. Fluid aspirated from a unilocular ovarian cyst in a young woman shows
small, cohesive aggregates of benign lining cells from the inner granulosa
cell layer of a functional (follicle) cyst; the cells are intermediate
in size with round, vesicular nuclei and scant cytoplasm (stain, Papanicolaou; courtesy
of Bradford Tan, M.D.). B. Corresponding histologic section of a follicular cyst shows orderly layering
of granulosa/theca cells in the cyst wall with bland nuclear features, similar
to that seen in the aspirated fluid (stain, hematoxylin-eosin). Fig. 10. A. Fluid aspirated from a unilocular ovarian cyst in a young woman shows
small, cohesive aggregates of benign lining cells from the inner granulosa
cell layer of a functional (follicle) cyst; the cells are intermediate
in size with round, vesicular nuclei and scant cytoplasm (stain, Papanicolaou; courtesy
of Bradford Tan, M.D.). B. Corresponding histologic section of a follicular cyst shows orderly layering
of granulosa/theca cells in the cyst wall with bland nuclear features, similar
to that seen in the aspirated fluid (stain, hematoxylin-eosin).
|
ENDOMETRIOTIC LESIONS Symptomatic lesions associated with active endometriosis are composed
of both cystic and solid regions and often yield a thick, chocolate-colored
fluid on aspiration.9 Endometriosis primarily affects women of reproductive age, and if it is
identified by FNA, the need for a diagnostic surgical procedure is eliminated.104 The cellularity in aspirations of endometriosis is typically scant. The
examiner should attempt to find all three components of the classic
diagnostic triad, which includes endometrial glandular cells, endometrial
stromal cells, and hemosiderin-laden macrophages.9 Fresh blood may also be a prominent feature.100 The glandular cells are small, with scanty cytoplasm, round-to-ovoid nuclei, finely
granular chromatin, and occasional chromocenters. When present
in intact tissue fragments, glandular cells are well organized, indicating
their benign nature. Stromal cells may appear as naked, isolated
nuclei.77 Generally, the presence of at least two of the three classic findings
is sufficient for the diagnosis of endometriosis in the appropriate clinical
setting. Finally, it should be noted that endometriotic nodules
may undergo malignant change and should be evaluated for such transformation. Neoplastic Ovarian Lesions Neoplastic ovarian tumors are grouped by the World Health Organization
classification (1995) into surface epithelial-stromal tumors, sex cord-stromal
tumors, germ cell tumors, tumors of uncertain histogenesis, soft
tissue tumors not specific to the ovary, and secondary (metastatic) processes.95 SURFACE EPITHELIAL-STROMAL NEOPLASMS The epithelial group of ovarian neoplasms includes benign, borderline, and
malignant subsets of serous, mucinous, endometrioid, clear cell, and
transitional (Brenner) tumors as well as squamous cell lesions, tumors
of mixed epithelial derivation, and undifferentiated epithelial lesions
that lack the characteristic findings of the more specific categories. Serous fluid aspirated from cystic serous neoplasms generally displays
a granular, eosinophilic background with low cellularity in benign and
well-differentiated lesions.77 The epithelial cells are small and tightly packed, and they have a high
nuclear-to-cytoplasmic ratio (sometimes resembling reactive mesothelial
cells). Spindled stromal cells may be noted if the tumor has a connective
tissue component (e.g., cystadenofibroma).9,77 Histiocytes may also be a prominent component in benign and well-differentiated
tumors. Low-grade carcinomas and borderline tumors are indistinguishable on cytology. FNA
of malignant serous tumors yields thick, turbid fluid with
increased cellularity, including single cells.9 Papillary structures and psammoma bodies may occur.82 Cellular pleomorphism, coarsening of the chromatin pattern, and prominent
nucleoli are all markers of malignancy.82 The differential diagnosis of ovarian serous malignancies includes reactive
mesothelial cells (which may be papillary), endometrioid carcinoma, and
metastatic processes.9 Ancillary studies such as DNA ploidy analysis (highly malignant ovarian
tumors likely to be nondiploid) and CA125 measurement (markedly elevated
in most serous malignancies), may prove helpful.105–107 Epithelial cells from mucinous tumors generally resemble endocervical cells (Fig. 11), particularly in benign and low-grade neoplasms. Benign cases are characterized
by small, regular fragments of uniform columnar cells with
bland, basally located nuclei and vacuolated cytoplasm.82 Desquamated epithelial cells may resemble foamy macrophages.77 Keratin immunohistochemical studies and cytochemical stains for mucin
may be useful in distinguishing epithelial cells from macrophages. 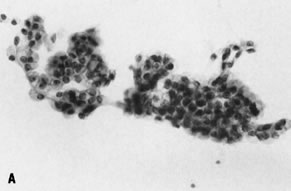 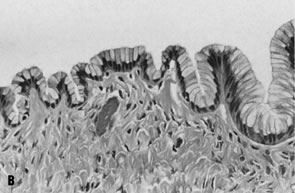 Fig. 11. A. Fluid aspirated from a cystic ovarian mass contains cohesive fragments
of epithelial cells with small, basally located nuclei without atypia
and abundant vacuolated cytoplasm; cytologically, they resemble endocervical
cells and are compatible with a mucinous neoplasm (stain, Papanicolaou). B. Corresponding histologic section shows a single, undulating layer of well-organized, endocervical-type glandular epithelium, consistent with
mucinous cystadenoma (stain, hematoxylin-eosin). Fig. 11. A. Fluid aspirated from a cystic ovarian mass contains cohesive fragments
of epithelial cells with small, basally located nuclei without atypia
and abundant vacuolated cytoplasm; cytologically, they resemble endocervical
cells and are compatible with a mucinous neoplasm (stain, Papanicolaou). B. Corresponding histologic section shows a single, undulating layer of well-organized, endocervical-type glandular epithelium, consistent with
mucinous cystadenoma (stain, hematoxylin-eosin).
|
FNA material from malignant mucinous lesions (borderline lesions as well
as cystadenocarcinomas) is often highly viscous and mucoid. Single cells, irregular
groupings of cells, and syncytial fragments of epithelium
with cellular atypia are noted in malignant mucinous tumors.82 Elevated carcinoembryonic antigen (CEA) and CA125 levels are appreciated
in the cyst fluid aspirated from primary mucinous cystadenomas and
cystadenocarcinomas.106,107 Multinucleated tumor cells may be noted, and the degree of cellular atypia
tends to increase as the lesion becomes more poorly differentiated.82 Benign and borderline endometrioid tumors are uncommon. Most lesions in
this category are carcinomas. Such lesions can be distinguished from
their serous counterparts by their more abundant, granular, eosinophilic
cytoplasm as well as focal areas of squamoid differentiation, which
are not seen in serous lesions.77,82 As with endometriod lesions, most primary clear cell tumors of the ovary
are frankly malignant. Cytologically, they resemble clear cell tumors
arising in the vagina, cervix, or endometrium.77 Generally, the cells of clear cell adenocarcinoma have abundant, pale, vacuolated (glycogenated) cytoplasm with indistinct cell borders and
pleomorphic nuclei.9 The differential diagnosis includes metastatic renal cell carcinoma and
yolk sac tumor.9,77 FNA of benign Brenner tumors shows cohesive fragments and sheets of uniform
cells with oval nuclei and moderate, eosinophilic cytoplasm. Deep
nuclear grooves and small prominent nucleoli may be noted; stromal elements
may also be apparent.9,77,82 Malignant Brenner tumors of the ovary are difficult to categorize cytologically
and may be confused with metastatic transitional cell carcinoma
or nonkeratinizing squamous cell carcinoma. These cells are often arranged
in papillary groups and exhibit dense basophilic cytoplasm and
coarsely granular chromatin.77 Many binucleate and multinucleate forms and mitotic figures may also be
seen.108 SEX CORD-STROMAL NEOPLASMS This broad category of primary ovarian lesions includes thecoma-fibroma, granulosa-stromal
cell tumors, Sertoli-Leydig cell lesions, androblastoma, sex
cord tumors with annular tubules, and gynandroblastomas. Thecoma-fibroma aspirates are extremely hypocellular and may be interpreted
as nondiagnostic.77 Aspirated tumor cells are ovoid with elongated, hyperchromatic nuclei
and scanty, ill-defined cytoplasm.77 Aspirates of granulosa cell tumors are usually highly cellular, with relatively
small tumor cells arranged both singly and in aggregates of a
few to several hundred cells.109 The nuclei are round to ovoid, single, and centrally located, and they
may have marked membrane indentations appearing as longitudinal grooves.109 Rosette-like structures with central, dense, eosinophilic material (Call-Exner
bodies) may be found and are very useful in supporting the diagnosis.77 In the absence of such bodies and in cases with frequent mitoses, the
differential diagnosis of small cell carcinoma (either primary or metastatic) must
be ruled out. Sertoli-Leydig cell tumors yield fragments of uniform, round cells with
moderate amounts of cytoplasm on aspiration.82 These cells may be arranged in cords, acini, or trabeculae, and a few
bare nuclei of stromal origin may be noted.77 Sex cord-stromal tumor with anular tubules is a rare primary lesion, at
times seen in association with Peutz-Jeghers syndrome. Smears from such
lesions have been reported as cellular; both single cells and cohesive
fragments of neoplastic cells arranged in follicular, solid, and trabecular
patterns.110 In classic cases, homogenous, eosinophilic, hyaline bodies surrounded
by palisading nuclei are very helpful at suggesting the appropriate diagnosis.77 GERM CELL NEOPLASMS Mature cystic teratomas are the most common germ cell tumors of the ovary. Other
entities in this category include dysgerminoma, yolk sac tumor, embryonal
carcinoma, choriocarcinoma, and polyembryoma.77,95 It is not uncommon for lesions in the germ cell group to present with
mixed morphologies. Malignant germ cell tumors account for less than 5% of
all ovarian cancers, and such lesions are most often encountered
in young females (younger than 20 years of age).111 In this age group, the tumor may be treated in such a way that reproductive
function is preserved.111 Aspirates of mature cystic teratomas show numerous superficial and anucleated
squamous cells; ciliated and columnar epithelial cells may also
be observed.77 Amorphous material (amphophilic, extracellular sebaceous secretions) is
a frequent finding in the background of smears from benign teratomas, and
it may elicit a foreign body giant cell reaction.77 More important, transvaginal collection of any ovarian aspirate may yield
many contaminating squamous cells. This finding alone should not be
misinterpreted as suggestive of ovarian teratoma. Immature teratomas
are predominantly comprised of neuroglial elements; the presence of a
frankly malignant neuroglial component in a smear favors classification
as a malignant neoplasm.77 Cells normally present in cerebrospinal fluid cytology, such as ependymal
and choroidal cells, may be noted in ovarian aspirates.112,113 When such cells are present in materials obtained from the ovary, malignant
neuroectodermal tumors must be considered. Ovarian carcinoids may
be primary to the ovary, a component of ovarian teratomas, or metastatic.77 Such tumors yield cells with an oval-to-spindled configuration and moderate
cytoplasm. The classic “salt and pepper” chromatin pattern
is most useful in diagnosis. Smears from dysgerminoma are characteristically hypercellular and composed
of large tumor cells with prominent nucleoli admixed with a separate
population of lymphoid cells (Fig. 12).77,114 The background is classically described as “tigroid” and is
best appreciated in air-dried, Diff-Quick-stained smears.114 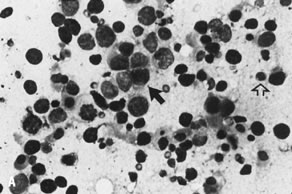 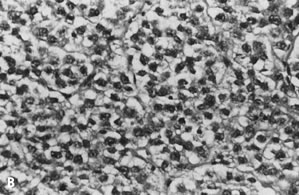 Fig. 12. A. Cytologic preparation of material obtained from a large ovarian mass in
a young woman shows a biphasic cell population comprised of large tumor
cells ( solid arrow) admixed with small lymphocytes ( open arrow) consistent with dysgerminoma (stain, Diff-Quik). Many of the tumor cells
are stripped of their cytoplasm and contain prominent nucleoli on
Papanicolaou stain. B. Corresponding histologic section displays the characteristic “fried-egg” appearance
of dysgerminoma (stain, hematoxylin-eosin). Fig. 12. A. Cytologic preparation of material obtained from a large ovarian mass in
a young woman shows a biphasic cell population comprised of large tumor
cells ( solid arrow) admixed with small lymphocytes ( open arrow) consistent with dysgerminoma (stain, Diff-Quik). Many of the tumor cells
are stripped of their cytoplasm and contain prominent nucleoli on
Papanicolaou stain. B. Corresponding histologic section displays the characteristic “fried-egg” appearance
of dysgerminoma (stain, hematoxylin-eosin).
|
Yolk sac tumors are also characteristically hypercellular on aspiration
and are composed of moderately sized oval cells, dispersed both as single
elements and in fragments. Vacuolated cytoplasm and both intracellular
and extracellular hyaline globules are noted.114 The serum alpha-fetoprotein is typically elevated.77 Embryonal carcinoma of the ovary is very rare, and aspirates of such lesions
are hypercellular, often showing hemorrhage and necrosis. Tumor
cells are bizarre with a high nucleus-to-cytoplasm ratio. The differential
diagnosis is usually poorly differentiated adenocarcinoma. Immunohistochemical
studies may show positivity for chorionic gonadotropin in
syncytiotrophoblastic-like cells.95 Embryonal tumors largely composed of embryoid bodies are referred to as
polyembryomas.95 Most choriocarcinomas of the ovary represent metastases from uterine primaries. Therefore, thorough evaluation of the uterine corpus is indicated
when a diagnosis of ovarian choriocarcinoma is considered.95 Microscopically, an admixture of syncytial and cytotrophoblastic elements
in a necrotic and hemorrhagic background is typical of this lesion. Immunohistochemical
reactivity for human chorionic gonadotropin is the
rule.95 OTHER NEOPLASMS Primary ovarian tumors of uncertain histogenesis include small cell carcinoma
and oncocytoma, among others.95 In two thirds of cases, primary ovarian small cell tumors produce paraendocrine
hypercalcemia.115 In ovarian small cell carcinoma, an intermediate-sized, round-to-oval
cell population with scanty cytoplasm and coarse granular chromatin may
predominate.115 Processes known to secondarily involve the ovary include metastatic carcinomas (from
breast, colon, stomach, pancreas, and gallbladder), malignant
lymphomas, and myeloid leukemias.77,116,117 Cases of metastasis to an ovary that already contains a primary ovarian
neoplasm have been reported in the literature.118 Such cases of “double cancers” are exceedingly rare, but they
show the need for careful review of obviously diagnostic aspirates
to not overlook cellular populations whose recognition may dramatically
alter patient treatment. Thus, despite reported controversial views on the role of ovarian needle
aspiration, the technique has been accepted by many as a relatively
innocuous procedure that can be accomplished with minimal complications
and risks for the patient.77 Without question, the procedure of aspiration with cytodiagnosis can be
used to preserve ovarian hormonal and reproductive function. If definitive
surgical treatment becomes indicated based on information gleaned
from aspirated material, the surgeon and patient may plan appropriately
for expected outcomes. Pelvis Fine-needle aspiration of both palpable and nonpalpable pelvic masses may
be readily performed in the initial evaluation and follow-up of patients
with gynecologic malignancies. Although the issue of the diagnostic
reliability of FNA in primary ovarian masses is the subject of some
debate, as discussed previously, the utility of FNA for the evaluation
of nonovarian primary tumors and potential recurrent gynecologic tumors
is unquestioned. Masses noted during pelvic examination may be aspirated
via either a transvaginal or transrectal approach, often with
the aid of a Franzen needle guide. Lesions located above the pelvic brim
and those deep within the posterior pelvis require radiologic guidance
for accurate placement of the biopsy needle. Ultrasound guidance may
be sufficient for a number of these cases, although CT guidance is
preferred for those lesions deep to bowel or bone.73 Numerous series with histologic or long-term clinical follow-up have confirmed
the extremely high specificity (99%) of the technique for pelvic
lesions.15,17,119–121 As with FNA in other anatomic regions, the sensitivity of the procedure
is slightly lower (85% to 95%) because of occasional false-negative
results.15,17,119,120 Such occurrences are generally ascribed to either technical difficulties (e.g., inexperienced
aspirator) or, more frequently, to intrinsic properties
of the lesion (e.g., significant fibrosis). Thus, a negative
FNA result in the presence of suspicious clinical findings warrants further
evaluation to exclude malignancy. FNA is also valuable in the surveillance of patients with a history of
malignancy after therapy. In a series of patients who underwent FNA biopsy
for evaluation of pelvic masses (parametrial, pelvic sidewall) noted
on pelvic examination or imaging studies after primary therapy (including
radiation therapy and hysterectomy) for cervical carcinoma, 22 of 30 patients
had a positive aspirate.122 The utility of FNA biopsy in patient follow-up after radiation therapy
alone was shown in another study of 58 patients with cervical or endometrial
carcinoma.17 Approximately 40% of the patients were proved to have residual or recurrent
disease on aspiration biopsy, with a 7% false-negative rate. More
important, one third of the patients with a positive FNA had an equivocal
or negative pelvic examination and imaging study results before
the biopsy. Thus, FNA is an extremely useful tool that may be valuable
in the often-difficult distinction between postradiation fibrosis and
recurrent tumor. As with all specimens, proper communication with the interpreting pathologist
is crucial for aspirates from this site. In addition to the mass
in question, a large number of normal structures may be concurrently
sampled depending on the needle approach and direction, including bladder, ureter, and
colon. A history of radiation or chemotherapy or both
must also be relayed to the pathologist, perhaps avoiding a falsely
suspicious or positive diagnosis based on marked therapy changes. Endometrium True fine-needle aspirates of endometrial lesions are rarely performed. Instead, simple
collection of intracavitary fluid or the appearance of
abnormal cells in routine cervical-endocervical smears is sufficient
for a diagnosis of malignancy. |