Case 3 :
A 26 year old woman complains of a vaginal discharge that has been present intermittently for the past 4 months. The discharge is thin and frothy and has a fishy odor. It is associated with irritation and itching of the vulva and some external burning with urination.
She saw a physician in her hometown on 2 occasions in the recent past and was given a treatment consisting of several pills, which she took all at once and which made her nauseated. She does not know the name of the pills. The treatment seemed to be effective for a short period of time, but the symptoms returned aafter both treatments within a few weeks.
The patient is married and has three young children at home. Her husband works for Ghana Telecom and is required to make monthly trips to Kumasi. She has no other sexual partner apart from her husband.
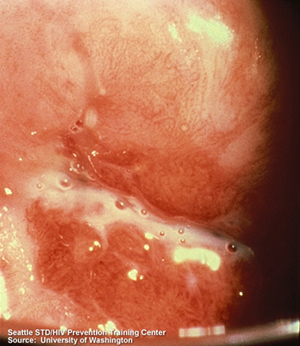
On physical examination, a pelvic examination reveals the watery discharge as shown below. The mucous membranes are erythematous, and there are a few petechiae on the cervix (not seen in this photo). Otherwise, the examination is normal.
A wet preparation of the discharge made with 1:1 normal saline is examined with a light microscope and has the following appearance:
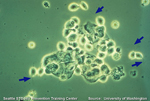
(Click on the image for an enlarged view)
The patient and her husband were both given a 2 gram dose of metronidazole which they were witnessed taking in the clinic. The patient had no further relapses. They were both tested for HIV and were negative.