Q2:
E.
N. gonorrhoeae, C. trachomatis, and various facultative and obligate anaerobic bacterial species
This is the best answer, because this is the range of microorganisms that you will want to cover with your treatment. Options A, B, or C could be correct, but since any of the organisms can be present in the upper tract, therapy should be broader. This is especially true since this illness appears to be either the second or third episode of PID that this patient has had. First episodes are usually associated with classical STD pathogens such as N. gonorrhoeae or C. trachomatis. However, with repeated damage to the endocervical canal, other bacteria in the vagina may ascend and contribute to a polymicrobial infection in the tube. After several episodes, the presence of a classic STD pathogen may not even be required.
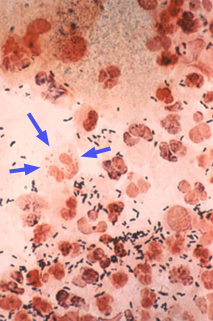
In this case, the Gram stain is positive. Gram stains from women are much more difficult to interpret than those from men with urethritis. This is because the urethra is normal sterile, whereas the vagina and cervix normally have an abundance of other bacteria in residence. It is sometimes difficult to tell whether there are Gram-negative, intracellular diplococci in the smear from a woman. In this case, the smear was positive (see below). C. trachomatis has to be considered a possible co-pathogen for the same reasons as in case #1. In the repeat image showing the Gram stain (below), blue arrows delineate the boundaries of a PMN filled with Grm-negative diplococci. This is N. gonorrhoeae.