Complementary and Alternative Medicine and Menopause
Authors
INTRODUCTION
Since the last edition of this text, menopausal medicine has experienced a seismic shift in the standard of practice. The results of the Women’s Health Initiative (WHI), the largest study ever done on menopausal hormone therapy (HT), demonstrated that a number of benefits assigned to hormonal treatment were either of lesser magnitude than had been assumed or in some instances were not evident at all.1 The WHI2 was designed to assess the impact of hormone therapy on cardiovascular events in generally healthy postmenopausal women. The study was planned to run for 8 years but was stopped after 5.2 years when the number of cases of breast cancer reached a pre-set Fleming O’Brien safety threshold for harm. No evidence of cardioprotection was seen and there was perhaps a small increase in cardiovascular risk in women receiving conjugated estrogens and a progestin (EPT). Two years later, the estrogen only arm (ET) was also stopped before the planned end of the trial. In this instance, a small but significant increase in stroke occurred, and interim statistical analysis projected that the primary end point, coronary heart disease (CHD) reduction, would not be realized even if the study continued. These findings were, save for the cardiovascular outcomes, consistent with data from earlier observational and case–control studies of hormone therapy. The rates of pulmonary embolism, breast cancer, colorectal cancer, stroke, and hip fracture tracked closely to earlier estimates. Additional analyses have been done to try to reconcile the disparities between past observational studies and the current findings regarding CHD. It is postulated that the role of HT varies with the timing of initiation of HT and the proximity of use to the onset of menopause. A post hoc follow up study found that women randomized to estrogen have less endothelial thickening than placebo subjects. The current recommendations from regulatory agencies and professional associations advise the use of HT for only moderate to severe hot flashes. If complaints are confined to vaginal atrophy, topical estrogens are advised. Osteoporosis may be treated with estrogens when other treatment modalities have failed or are poorly tolerated.
The risks of HT in younger menopausal women are reassuring. In women aged 50–54, those most likely to benefit from HT, estrogen plus progestin therapy (EPT) carries a small increase in absolute risk, 1.56 events per 1000 woman-years., and for estrogen only therapy the risk is 0.8 events per 1000 woman-years. Estrogen therapy (ET) and EPT are both associated with a 20% increase in stroke. For women aged 50–54, pulmonary embolism, cardiovascular disease, and breast cancer were increased only in the EPT arm of the study (Table 1).3
Table 1. Relative risks of disease outcomes from the Women’s Health Initiative trials and estimates of absolute differences in risk among women aged 50–54 years. From Grady, 20064 with permission
| Estrogen plus Progestin | Estrogen Only | |||
| Outcome | Relative Risk (95% CI) | Absolute Difference in Risk | Relative Risk (95% CI) | Absolute Difference in Risk |
| Coronary heart disease | 1.29 (1.02–1.63) | 0.26 | 0.91 (0.75–1.12) | — |
| Stroke | 1.41 (1.07–1.85) | 0.20 | 1.39 (1.10–1.77) | 0.20 |
| Pulmonary embolism | 2.13 (1.39–3.25) | 0.45 | 1.34 (0.87–2.06) | — |
| Invasive breast cancer | 1.26 (1.00–1.59) | 0.93 | 0.77 (0.59–1.01) | — |
| Colon cancer | 0.63 (0.43–0.92) | −0.18 | 1.08 (0.75–1.55) | — |
| Hip fracture | 0.66 (0.45–0.98) | −0.10 | 0.61 (0.41–0.91) | −0.12 |
| Net outcomes per 1000 women per year | 1.56 | 0.08 | ||
Retrospective and prospective cohort studies during the 1980s demonstrated a 30–70% reduction in the incidence of CHD events in women taking either ET or EPT, a unexpected benefit beyond the conventional positives – decrease in vasomotor symptoms, improved vaginal atrophy, and preservation of bone mineral density. Moreover, the literature also suggested a lower rate of dementia in long-term users.
Two studies were designed and directed to determining if indeed hormone therapy did lower both secondary and primary cardiovascular risks. The Heart and Estrogen/Progestin Replacement Study recruited women with preexistent CHD. All participants were also required to have an intact uterus, and all were then randomized to placebo or EPT. The study demonstrated no decrease in cardiovascular events. Moreover, there was evidence of early harm in women in the EPT arm, with CVD events and deaths occurring earlier than in those randomized to placebo. The study was extended for 2 years beyond the initial 4 years, but again, no benefit was evident.
Since the initial publication in 2002, dozens of papers have reexamined the risks and benefits of HT in greater detail. As might be predicted, the relative risks in younger menopausal women aged 50–54 are considerably lower than those seen in women age 67, the mean age of participants. While this might appear to be reassuring to health care providers and consumers, scepticism continues to cloud the issues.
Each new report from the WHI, particularly about adverse outcomes, receives extensive media coverage, while the more reassuring reports tend to receive less attention. After the first WHI report, EPT use fell by 60%, and has yet to recover. The seeming contradiction between the older cohort and case–control studies of HT and the more recent WHI, Papworth, and Million Women studies has created mass confusion. The medical community continues to try to define the proper role for hormone therapy. The regulatory authorities recommend that HT use be confined to women with moderate to severe vasomotor symptoms, using the lowest dose for the shortest duration of time. Others believe that the WHI is seriously flawed and should be disregarded. Women are caught in the center of this maelstrom. A celebrity talk show hostess summed up how many women feel. In essence she said…first they told us hormones were good for your heart, then they told us they were bad for your heart, and now it is good but only if you are under 55. I don’t know what they are telling us anymore! Distrust of conventional hormones, the medical establishment and the pharmaceutical industry has left women bereft, now searching for something else…something effective, something safe. Women have turned to complementary and alternative medicine, so called bio-identical hormones, and the counsel of celebrity spokespersons.
There was a significant upswing in the use of black cohosh immediately after the WHI, but over the past 6 years, much of that trend has reversed. This is true for many botanicals. The lack of efficacy is most often cited as the reason when women return and ask about new treatment options. The nonhormonal pharmaceutical options like selective serotonin reuptake inhibitors (SSRIs) are often unacceptable because of limited efficacy or unpleasant side effects.
Women ask about “natural” options, and assume that natural products or plant based medicines are safe and effective. This belief stems from “historical” use. It is commonly believed that if a product or technique has been in use for decades or centuries, it must have some merits. But historical use is not proof of efficacy or safety. The first randomized placebo controlled clinical trial was conducted in 1948, and indeed many of the drugs in our current pharmacopoeia have never been proven to work in a clinical trial, but remain in use based solely on historical precedence.
In the past 10 years, a reasonable though not robust body of evidence has accumulated about complementary and alternative treatments for menopause. The adequacy of the studies varies greatly. Many do not meet even minimal criteria for adequate design and execution, and often are underpowered. This review includes the best evidence available at this time.
DEFINING COMPLEMENTARY AND ALTERNATIVE MEDICINE (CAM)
Alternative medicine encompasses several systematic medical practices based on physical assessments that differ from the physiology used in Western medicine (Table 2). Examples include traditional Chinese medicine, a system defining health in terms of the balance of an essential life force called Qi (pronounced Chee). Acupuncture is said to support wellness and to treat disease by regulating the flow of Qi along meridian courses through the body. Mind–body systems of medicine support health by using conscious and unconscious influences of mind over bodily processes. Manipulative and body-based include chiropractice, osteopathy, and massage. Meditation, hypnosis, music, and prayer fall into the area of mind–body practice. Somewhat related to mind–body medicine are so-called energy modulating modalities which supposedly reorder bioelectric fields of the body. Examples include therapeutic touch, Qi Gong treatment, and magnets. The most recognizable and widely employed practices are biologic-based therapies like botanical medicines, dietary supplements, vitamins, minerals, and orthomolecular medicine.
Table 2. Complementary and alternative medicine (CAM) headings in MEDLINE
| Acupuncture |
| Anthroposophy |
| Biofeedback |
| Chiropractice |
| Color therapy |
| Diet fads |
| Eclecticism |
| Electric stimulation |
| Homeopathy |
| Kinesiology |
| Massage |
| Medicine, traditional |
| Mental healing |
| Moxibustion |
| Music therapy |
| Naturopathy |
| Organotherapy |
| Radiesthesia |
| Rejuvenation |
| Relaxation techniques |
| Therapeutic touch |
Virtually every culture offers some sort of folk remedy for menopause symptoms, and the most common offerings are botanical medicine. While the term herbal applies to the herbaceous portions of plants, namely the leaves and stems, botanical is a broader term which includes all parts: leaves, stems, seeds, fruits, flowers, and roots. Estimates are that 30% of our current pharmacopoeia is derived from plants: digitalis, aspirin, quinine, reserpine, and paclitaxel to mention a few. Different plants are used to different therapeutic purposes, and different parts of the same plant may be used for different complaints.
Research and regulatory issues relating to botanical medicines
The Food and Drug Administration (FDA) restricts the advertising claims that vitamin and supplement manufacturers can make. They are not allowed to make claims about treatment of disease. But advertising copy can push the edge of the envelope. Mood suggests treatment for depression, prostate health becomes a code implying treatment of benign prostatic hypertrophy and urinary problems, claims about improved energy might appeal to sufferers of chronic fatigue, and appetite control products often claim weight loss without diet or exercise.The Dietary Supplement Health and Education Act (DSHEA) exempts botanical medicines from drug regulatory processes by classifying them as dietary supplements. Supplements can be sold without oversight and testing by the FDA, and, in fact, the burden of proof lies with the agency to demonstrate lack of efficacy and lack of safety. This mandate is unfunded.
In 1992, the office of Alternative Medicine was started as a branch of the National Institutes of Health, with minimal funding, $2 million dollars, and even that small amount was thought by many to be a waste of tax money. The National Center for Complementary and Alternative Medicine now has a budget over $120 million dollars.
Evaluating botanical medicines is complex, far beyond the obvious standard. The following need to be assessed:
• Quality
• Efficacy
• Safety
• Standardization
• Adulteration
• Potential drug–herb interactions
• No systematic reporting of adverse events
• Variation in active constituents (batch to batch, season to season, field to field)
• Growing conditions
• Contamination5, 6
Unfortunately adulteration and contamination are rather commonplace. A study of Chinese patent medicines in California found that 30% were adulterated with pharmaceuticals: herbal cold remedies contained pseudoephedrine, aphrodisiacs methyl testosterone, and arthritis remedies ibuprofen.3 Moreover, botanical medicines may vary in potency according to climatic and seasonal growing conditions, processing, shipment, and storage. Different lots from the same manufacturer or the same product from a different manufacturer may vary greatly in the amount of the active ingredient (when it is know and identifiable). Contamination can occur during growing, picking, processing, and packaging.7
Estimates are that only 10% of adverse reactions for drugs and less than 1% for alternative treatments are reported to any regulatory body. Once toxicities are identified, it may take considerable time for regulatory agencies to take action. On February 28, 2004, FDA and the Department of Health and Human Services jointly announced a ban on ephedra.8 The action was prompted by review of some 16,000 adverse event reports. A RAND review of cases enumerated two deaths, four heart attacks, nine strokes, one seizure, and five psychiatric cases involving ephedra with no other contributing factors. The FDA press release cited a study that noted while “ephedra-products make up less than one percent of all dietary supplement sales, these products account for 64 percent of adverse events associated with dietary supplements.” Many medical experts felt that this action should have been implemented years earlier. There are several legislative and regulatory efforts in process to rein in the DSHEA and tighten controls.9
Use of complementary and alternative medicine by menopausal women
Depending on the expansiveness of the definition, CAM use for menopause in the United States ranges from less than 10% to more 60% of women surveyed. The Study of Women’s Health Across the Nation (SWAN) studied the use of complementary and alternative medicine over a 6 year period in 2118 subjects. Excluding diets, exercise, prayer, and vitamins, the SWAN reported that 52.7% of menopausal women reported using complementary and alternative modalities, and 20–30% used more than one modality. The most commonly used dietary and botanical products were soy supplements 16.6%, glucosamine 15.9%, flaxseed/oil 10.6%, ginkgo 6.8%, black cohosh 6.4%, and ginseng 5.8%. Soy and black cohosh were more often used by symptomatic women. The findings are consistent with impressions from earlier smaller surveys.10
BOTANICAL MEDICINES FOR MENOPAUSAL SYMPTOMS
Complementary and alternative treatment of vasomotor symptoms (hot flushes and night sweats)
Many of the botanicals recommended for treatment of vasomotor symptoms (VMS) have been used for generations. The 1899 Merck Manual (Table 3) includes cimifuga (black cohosh) which is still the most commonly botanical remedy for VMS.
Table 3. 1899 Merck Manual remedies for the climacteric
| Aconite |
| Actaea (formerly Cimicifuga) |
| Ammonia/ammonium chloride |
| Amyl nitrite |
| Belladonna |
| Calabar bean |
| Camphor |
| Cannabis indica |
| Change of air or scene |
| Eucalyptol |
| Hot spongings |
| Hydrastinine hydrochlorate |
| Iron |
| Methylene blue |
| Nux vomica |
| Opium |
| Ovaraden |
| Ovariin |
| Physostigmine |
| Potassium bromide |
| Potassium iodide |
| Sodium benoate |
| Stypticin |
| Thymol |
| Warm bath |
| Zinc valerianate |
Some botanicals are said to be estrogenic, and indeed contain phenolic compounds that interact with estrogen receptors (Table 4).
Table 4. Botanical products reputed to be estrogenic
| Alfalfa (Medicago sativa) |
| Apiaceae or Umbelliferae family (aniseed, dill, fennel, wild carrot) |
| Black cohosh (Actaea racemosa formerly Cimicifuga racemosa) |
| Chasteberry (Vitex agnus-castus) |
| Dong quai (Angelica sinensis) |
| Flaxseed (Linum usitatissimum) |
| Ginseng (Panax ginseng and other species) |
| Kudzu (Pueraria lobata) |
| Licorice (Glycyrrhiza glabra) |
| Maca (peruvianum, meyerium) |
| Red clover (Trifolium pratense) |
| Rhubarb (Rheum rhaponticum) |
| Soy (Glycine max) |
| Wild Mexican Yam (Dioscorea villosa, Dioscorea mexicana) |
Before estrogen was linked to breast cancer in the late 1980s, in vitro and in vivo basic science work often used models to try to prove that these botanicals had frankly estrogenic effects. More recently, basic research antecedent to clinical trials centers on providing some sort of selective mechanism of action, usually estrogen receptor beta selective agonist activity, or no estrogenic activity at all.
Phytoestrogens
Phytoestrogens are naturally occurring plant sterols capable of exerting effects similar to estrogen. Phytoestrogens are divided into three groups:
1. Isoflavones are plant sterols found in soy, garbanzo beans, and other legumes. The most commonly consumed are genistein and daidzein.
2. Lignans are components of plant cell wall that become bioavailable through the action of intestinal bacteria on grains. Seeds used to produce oils, particular flaxseed, are rich sources of lignans.
3. Coumestans, although extremely rich in phytoestrogens, are generally not important dietarily in humans. High concentrations are found in red clover, sunflower seeds, and bean sprouts.
Studies of populations in which large amounts of soy-based phytoestrogens are consumed report lower rates of a wide variety of cancers, including breast, endometrium, prostate, intestine, and pancreas. In countries such as China and Japan, where the local diet is high in soy foods, women appear to have few menopausal ailments, and, coincidentally, the incidence of breast, endometrial, and prostate cancers are also markedly reduced when compared with Westernized countries.
Asian diets typically contain 40–80 mg/day isoflavones, whereas American diets average less than 3 mg/day. Nevertheless, American and European diets tend to elevate plasma levels of sex hormones and decrease sex hormone-binding globulin concentrations, thus increasing the exposure of peripheral tissues to the effects of circulating estrogen.
High soy diets act through several mechanisms to lower effective circulating and tissue levels of steroids. High isoflavone intake decreases luteinizing hormone (LH) levels and secondarily decreases estrogen production. Bean products are rich sources of diphenols, which are thought to lower cancer risk by modifying hormone metabolism and production and limiting cancer cell growth. Bean foods also provide large amounts of fiber, and fiber modifies the level of sex hormones by increasing gastrointestinal motility. Fiber alters bile acid metabolism and partially interrupts the enterohepatic circulation causing increased estrogen excretion by decreasing the rate of estrogen reuptake in the enterohepatic system.11
A study by Lu et al. helps to elucidate the magnitude of altered steroid metabolism induced by high isoflavone intake. Women were fed 36 oz of soy milk a day for one menstrual cycle. The calculated intake of isoflavone in this amount of soy milk is approximately 100 mg of daidzein (mostly as daidzin) and 100 mg of genistein (mostly as genistin). Serum 17 beta-estradiol levels dropped by 31–81% at various times in the menstrual cycle during the feeding cycle. Luteal phase progesterone levels fell by 35% and dehydroepiandrosterone sulfate levels by 14–30%. Steroid levels remained lower for an additional two or three menstrual cycles. Menstrual cycle length increased from 28.3 to 31.8 ± 5.1 days during the month of soy milk and did not return to prestudy length until five to six cycles later.12
Effects of soy foods, soy extracts, and red clover extracts on VMS
Plant constituents include ringed phenolic compounds that often have structures with partial homology similar to estrogen (Fig. 1). While isoflavones are commonly called phytoestrogens or plant estrogens, they act as phyto selective estrogen receptor modulators. The isoflavone genistein clearly binds to estrogen receptors, but produces configurational changes in the receptor that differ from those seen with estradiol. The binding affinity is clearly lower than that for true estrogens, and the degree of interaction with the alpha and beta receptors differs as well (Table 5). Effects of isoflavones vary considerably with concentration, cell line, tissue, species, etc., response, ergo in vitro and in vivo studies are inconsistent.13
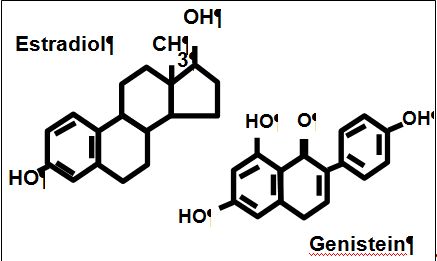 Fig. 1. Structures of estradiol and genistein.
Fig. 1. Structures of estradiol and genistein.
Table 5. Estrogen receptor (ER) binding affinity for various ligands14
|
| ER alpha | ER beta |
| Estradiol-17b | 100 | 100 |
| Coumestrol | 94 | 165 |
| Genistein | 5 | 36 |
| Tamoxifen | 7 | 6 |
| 4 OH tamoxifen | 178 | 330 |
Effects of soy foods on VMS
TRADITIONAL USAGE
Soy is traditionally used as a human and animal food stuff.
EVIDENCE OF EFFICACY FOR TREATMENT OF VMS
Soy foods and soy based isoflavone extracts or tablets are heavily promoted for vasomotor symptoms. The outcomes of studies have been highly variable, and given that different foods, with different amounts of isoflavones have been tested in different populations, assessment of the results in the aggregate in a meta-analysis has been challenging. Representative studies include Washburn,15 where women were given 20 g soy protein with 34 mg isoflavones or a 20 g carbohydrate complex for 1.5 months. Hot flashes decreased in severity but not frequency in the treatment group. Albertazzi studied more than 100 women with seven or more hot flashes per day, and randomized them to a 60 g soy protein supplement with 76 mg isoflavones or to a casein control. Hot flashes decreased by 45% in the treatment arm, compared to only a 30% decrease in the control group.16 Murkies gave women a soy flour supplement. After 3 months the soy group evidenced a 40% reduction, while the controls fed wheat flour experienced about a 25% decline. The difference was not significant.17
Knight et al. conducted a randomized, double-blind, placebo-controlled, parallel-group trial with 24 postmenopausal women. After 3 months of treatment, women on a dietary beverage with 60 g of soy protein, and 134.4 mg of isoflavones were compared to a control group taking an isoflavone-poor version of the beverage. There were no observed differences in the responses of subjects in hot flushes, Greene Menopause Symptom Scores, vaginal maturation value, levels of follicle stimulating hormone (FSH) or sex hormone-binding globulin (SHBG), or bone turnover markers. The soy group evidenced a 25% drop out rate, bad taste was cited as the main complaint.18 Other studies of soy have reported high rates of discontinuation due to gastrointestinal distress, gas, cramps, and stomach pains.
Burke et al. did a study which included 241 moderately symptomatic women with 2.6–4.2 flashes per day, randomized into one of three groups. All women received 25 g of protein, but the amount of isoflavone was stratified in the soy: (1) isoflavone free soy protein; (2) soy with 42 mg isoflavones; and (3) soy with 58 mg isoflavones. During the 2-year study period, a reduction in the number and severity of vasomotor symptoms was observed in all three treatment groups. No significant differences in the number and severity was seen. The protein only group decreased from 3.5 to 0.8 flashes, while the high and low isoflavone groups decreased from 3.2 to 1.3 and 2.6 to 1.5, respectively. The isoflavones-poor, protein only product in essence is the placebo, and it then appears that isoflavones provide no measurable therapeutic effect.19
CONCLUSION AND RECOMMENDATIONS
The evidence for soy as a treatment for VMS is mixed at best. The most significant review to date, undertaken by Lethaby for the Cochrane Collaboration concluded that “[s]ome trials found a slight reduction in hot flashes and night sweats with phytoestrogens-based treatment but overall there is no indication that phytoestrogens work any better than no treatment”.20 Women should eat soy because they like it, and because plant based proteins are a healthy alternative to meat protein. It is unclear if substituting soy for meat later in life, in contradistinction to those who eat a soy based diet their entire lives, alters the course of cardiovascular disease incidence or progression. The effect of soy on cholesterol is questionable.
The American Heart Association Nutrition Committee issued a summary of a statement for professionals on soy protein, isoflavones, and cardiovascular health. The Committee concluded that “… very large amount[s] of soy protein, comprising more than half of daily protein intake, may lower LDL cholesterol by just a few percent when it replaces dairy protein or a mixture of animal proteins...[and] direct cardiovascular health benefit of soy protein or of isoflavone supplements [are] minimal at best. The contribution of dietary soy to cardiovascular and overall health probably resides in “high content of polyunsaturated fats, fiber, vitamins, and minerals and low content of saturated fat.”83
Soy and red clover based isoflavone supplements
TRADITIONAL USAGE
Soy is traditionally used as a food stuff and red clover as animal fodder. While soy is the most common source of isoflavones in the human diet, red clover, Trifolium pratense, is the richest source of isoflavones of any plant. Red clover is also a rich source of coumestans, another group of phenolic compounds with steroid like activity. Isoflavone isolates claim to provide the same benefits as whole soy foods.
EVIDENCE OF EFFICACY FOR TREATMENT OF VMS
Trials of various isoflavone isolates for hot flashes have been equivocal. A red clover derived commercial preparation containing 40 mg total isoflavones was given to 51 women while 43 women received placebo. Baber found after the 6 month crossover trial that the product was not more effective than placebo. Hot flash frequency decreased in both groups, 18% and 20% in treatment and placebo, respectively. No differences were seen in other symptoms (Greene Scale) or endometrial thickness (ultrasound).21
Knight studied the same product using isoflavone 40 mg, 160 mg or placebo for 12 weeks. Hot flash frequency decreased in all groups – 35%, 29%, and 34%, respectively. There were no differences from baseline in follicle stimulating hormone (FSH) or sex hormone binding globulin (SHBG).22 A small single armed study by Nachtigall showed improvements when patients served as their own controls. This kind of approach obviously does not account for placebo like effects on outcomes.23 A more recent spate of randomized trials of soy and isoflavone isolates have been less supportive of claims for these supplements. A group of 30 women with more than 12 months amenorrhea and experiencing more than five flashes per day were enrolled in a randomized trial which included a 4 week placebo run in, followed by 12 weeks of treatment or placebo.24 The active treatment arm received an 80 mg isoflavone tablet (Promensil). End points included hot flashes per day and changes in Greene Climacteric Scale Score. Hot flashes decreased 16% during the run in phase. During the subsequent double blind phase, a further, statistically significant decrease in VMS of 44% was seen in isoflavones group (p <0.01), whereas no further reduction occurred within the placebo group. Greene Climacteric Scale Score declined by 13% in the treatment arm only and remained unchanged in the placebo group. A much larger study done by Tice et al. included 252 menopausal women, aged 45–60 years, with a higher degree of symptomatology.25 Like FDA registration trials, the participants had to have at least 35 hot flashes per week (7 or more per day), with a mean of 8.1 hot flashes per day. After a 2-week placebo run-in, women were then randomly assigned to Promensil (82 mg of total isoflavones per day), Rimostil (57 mg of total isoflavones per day), or an identical placebo, and followed-up for 12 weeks. In all, 246 (98%) completed the 12-week protocol; an astonishingly high retention rate and 97% of study drug tablets were consumed, again indicating a high level of motivation and compliance. The reductions in mean daily hot flash count at 12 weeks were similar for the Promensil (5.1), Rimostil (5.4), and placebo (5.0) groups, approximately 30–40% over the time period of the study. Quality of life measures and Green Climacteric Scale scores were similar in all groups.
In yet another study by Faure, a standardized soy extract was studied in 75 women with at least seven hot flashes per day who were within 6 months of menopause.26 Women were given Phytosoya (with 70 mg of genistin and daidzin) or placebo. After 16 weeks, the treatment group evidenced a 61.2% reduction in symptoms compared to only a 20.8% reduction in the placebo group. When responders were defined as those with at least a 50% reduction, 65.8% of women in the treatment group were classed as responders, with only 34.2% in the placebo group. Of the women, 15% and 39%,respectively, withdrew during the course of the study.
CONCLUSION AND RECOMMENDATIONS
There is insufficient proof of the safety and efficacy of clover or soy based isoflavone isolates as treatment for VMS. Isoflavones isolates cost around $22–50 per month. The evidence does not support this kind of extravagance. Lethaby et al.20 neatly summarize the available literature on dietary soy, soy extracts, and red clover extracts. Six large databases were searched for randomized trials and of the available literature only 30 studies met the criteria for inclusion in the review. The vast majority of the accessible studies generally suffered from poor study. Of those reviewing dietary soy, only nine studies met criteria for inclusion in the analysis and of those, seven proved negative. Similarly, nine studies of soy extracts were included with five showing some significant outcomes in either frequency or severity of VM, not both and generally the efficacy was limited. Seven studies of red clover extracts were judged to be of quality, and five used one commercial product, Promensil. A meta-analysis of these five found that the extract is not more effective in reducing VMS than placebo.
Black cohosh (Actaea racemosa L. Nutt, family, Ranunculaceae)
Black cohosh goes by many folk names including black snakeroot and bugbane.
TRADITIONAL USAGE
Native Americans use black cohosh for the treatment of snakebites. Other uses included arthritis, kidney, respiratory, and skin disorders. During late colonial times the root was exported to Europe from the continental US, and used in women's health to promote lactation and to induce menstruation or ease menstrual cramps. Lydia Pinkham’s Vegetable Compound contained black cohosh in an 18% ethanol base and the amount of black cohosh is said to approximate to the amount in current commercial preparations.
EVIDENCE OF EFFICACY FOR TREATMENT OF VMS
In Europe and the USA, black cohosh has been very popular for treatment of VMS and for other menopause related symptoms in combination with valerian for sleep and with St. John’s wort for mood, and other botanicals. Most commonly used as an ethanolic extract, the most commonly used brand is sold over-the-counter as Remifemin™ and is listed in the Germany Commission E for treatment of the climacteric, premenstrual syndrome, and dysmenorrhea. Prior to the recognition of a potential link between estrogen and breast cancer, the basic science research tried to prove that black cohosh was estrogenic. After 1990, efforts have tried to document other modes of action. The most recent claim is that the effects are mediated via serotonergic pathways. Black cohosh has no effects on endometrial thickness, maturation index of the vaginal epithelium, serum LH, FSH, estradiol, and prolactin,27 confirming that black cohosh does not exhibit peripheral estrogenic effects.
Assessing the clinical utility of black cohosh has been highly problematic since most of studies done before 2001 are replete with methodological problems. Seven of eight published trials did not use placebo controls, and seven of eight are only available in German. Duker et al. compared black cohosh to placebo using 40 mg twice daily (twice the “standard” dose) and found Remifemin suppressed hot flashes about 25% better than placebo in the 2 month trial.28 Stoll29 compared 40 mg twice daily versus conjugated equine estrogen (CEE) 0.625 mg and with placebo. The herbal remedy provided good relief, while estrogen, which is the standard therapy for VMS, performed no better than placebo. The failure of estrogen as a treatment may be explained by the fact that the study included premenopausal, perimenopausal, and postmenopausal women. Another study by Lehmann-Willenbrock30 of women said to be postmenopausal actually included women under the age of 40 who had indeed undergone hysterectomy but who retained one or both ovaries. Women were treated with low dose estrogen, high dose estrogen, high dose estrogen plus a progestin, and with black cohosh; all evidenced equal improvement in climacteric symptoms. No placebo group was included.
A large study conducted by the University of Washington found no evidence of therapeutic efficacy for black cohosh alone, black cohosh in a mix of traditional multiple botanicals used as a supplement, the same supplement coupled with soy dietary counseling, versus placebo. Indeed none of the active treatments demonstrated any efficacy.31
The five randomized trials done since 2001 examining the efficacy of black cohosh have enrolled over 1000 subjects. Only one of the five (Osmers) reported positive results.32, 33, 34, 35, 36
Many conventional and alternative practitioners recommend black cohosh to breast cancer survivors. After an abstract reported enhanced tumor implant growth using a rat experimental model, a pharmaco-epidemiologic observational retrospective cohort study was done in breast cancer survivors. Though the study has some methodological issues, the investigators detected no increased risk of recurrence in women who took black cohosh.37
After the WHI, between 2002 and 2003, sales of black cohosh in the USA increased by 26%. These gains reversed between 2003 and 2005 when reports of hepatotoxicity started to appear. A total of 47 cases have been reported worldwide, ranging from abnormal liver functions to hepatitis, and one case of hepatic failure necessitating transplantation. Australia, the UK, and Sweden have issued warnings or required products to carry warnings on their labels about potential hepatic risks. An estimate is that the risk is <1 in 10 million daily doses.38
Another branded blend of a traditional combination of black cohosh, dong quai, milk thistle, red clover, American ginseng, and chaste tree (Phyto Female Complex) was tested in a randomized controlled trial in 50 healthy pre- and postmenopausal subjects. Over 3 months, the treatment groups had a 73% decrease in hot flashes and a 69% decrease in night sweats, while the score in the placebo group were 47% and 19%, respectively. Many botanical trials include both symptomatic premenopausal women and postmenopausal women, hoping to prove the efficacy of the product across all phases of the menopausal transition.39
CONCLUSION AND RECOMMENDATIONS
Black cohosh is still regarded as safe by most conventional and alternative practitioners save for a minor propensity toward gastrointestinal complaints. While it is not clear if black cohosh, contamination, cross reaction with other medications or herbs, or other concomitant supplements was the source of hepatic damage in reported cases, some caution should be exercised when using this botanical particularly in women with intercurrent illness. Given the lack of convincing proof of efficacy, other therapeutic options should be considered.
Other botanicals commonly recommended for menopause: dong quai, Angelica sinensis also called Dang gui, Tang kuei
Dong quai (Angelica polymorpha Maxim. var sinesis Oliv, aka A. sinensis (Oliv) Diels) is a type of angelica.
TRADITIONAL USAGE
The root is used as the female balancing agent in traditional Chinese medicine (TCM), and is a panacea for almost every gynecologic ailment, including hot flashes, dysmenorrhea, oligomenorrhea, premenstrual syndrome (PMS), amenorrhea, and menopausal syndrome. It is also recommended as a laxative and antispasmodic,and as a treatment for insomnia, anemia, and hypertension. Dong quai is said to be “a warm herb that both circulates and nourishes blood, is also good for strengthening someone who is underweight, frail, anemic ,and chilly.“ Dong quai is supposedly estrogenic, since it has been associated with episodes of uterine bleeding and has uterotropic effects in ovariectomized rats.
EVIDENCE FOR MENOPAUSAL MEDICINE
Hirata studied 71 women with FSH over 30 mIU/mL and randomized them to either 4.5 g dong quai per day or placebo. The outcomes, based on patient diaries and Kupperman index, showed no differences in FSH, LH, estradiol, vaginal maturation index, and endometrial thickness. Critics have noted that the dose of dong quai is low compared to the amounts used in traditional Chinese medicine, and that the product was used alone, rather than with other components of traditional menopausal formulations.40 Nonetheless, in the real world, dong quai is promoted and sold as a single botanical, sometimes in very low doses, far lower than the 7–12 g used by some TCM practitioners. One branded product of dong quai, Rejuvex™ contained bovine ovarian, uterine, mammary, and pituitary tissues, which is considered a potential source of transmission of prions involved in Creutzfeld–Jakob disease (bovine spongiform encephalopathy). I started issuing warnings to patients and other health care providers at the turn of the millennium about the possible risks of this product as well as the instances where women inadvertently violated religious precepts using a product with less than clear disclosure that it contained animal byproducts. Shortly thereafter the FDA as of July 1, 2004, banned all dietary supplements containing brain or spinal cord material from cows over 30 months of age and sometime during 2006 the product effectively disappeared from store shelves and from internet distribution. This probably resulted from FDA restrictions on bovine CNS materials.
CONCLUSION AND RECOMMENDATIONS
Considering the lack of efficacy and its potential for anticoagulation, photosensitization, carcinogenesis, and herb–drug interactions, practitioners should advise women against the use of dong quai.
Evening primrose (evening primrose, evening star, Oenothera biennis L family onagraceae)
The evening primrose is a flowering plant, a volunteer in many gardens, and a rich source of linolenic acid, a type of omega-3 essential fatty acid. Other sources include cold water fish, canola oil, soybean oil, and a few vegetable oils. Gamma linolenic acid (GLA) comes from oils from seed of currant, borage, and evening primrose. These fatty acids are eicosanoid precursors and are part of cell membranes. The pathway for dietary GLA leads to dihomo-gamma-linolenic acid (DGLA), which in turn is converted by inflammatory cells to 15-(S)-hydroxy-8,11,13-eicosatrienoic acid and prostaglandin E1, with potent anti-inflammatory activity. GLA and DGLA appear to affect inflammatory processes by regulating T lymphocytes and GLA inhibits angiogenesis.
TRADITIONAL USAGE
Evening primrose is recommended for a number of inflammatory and autoimmune processes. In reproductive medicine, evening primrose oil (EPO) is used to treat mastalgia and mastadynia, though the claims are poorly substantiated. There are seven studies of EPO for premenstrual syndrome, and in the five of the seven using blinding and randomization, there is no evidence of efficacy.41, 42, 43
EVIDENCE FOR MENOPAUSAL MEDICINE
The one well constructed randomized trial of EPO for VMS was negative.44
CONCLUSION AND RECOMMENDATIONS
EPO is not useful in treatment of menopausal symptoms.
Ginseng (Panax ginseng)
The genus name, panax, derives from the word panacea, meaning cure-all. Many different plants are called ginseng and have many suggested uses.
TRADITIONAL USAGE
Korean or Chinese ginseng is supposedly a stimulant, aphrodisiac, digestive, with anabolic effects, and is promoted as a health tonic for the elderly. American ginseng is said to be an “adaptogen”, helping the body tolerate and acclimate to environmental stress and to defend against illness. Siberian ginseng (Eleutherococcus) not a true ginseng, is promoted to enhance athletic performance and endurance.
EVIDENCE FOR MENOPAUSAL MEDICINE
Wiklund used a research product called G115, said to be equivalent to a marketed product called Ginsana. Postmenopausal women were randomized to the product or placebo. Outcomes included FSH, estradiol levels, endometrial thickness, maturity index, and vaginal pH. After 16 weeks the extract showed slightly better overall symptomatic relief, though the improvements were not statistically significant (p <0.1). Scales for depression, well-being, and health subscales also improved in the ginseng group, but the study was underpowered for proof in these secondary outcomes. Ginseng had no effect on FSH and estradiol levels, endometrial thickness, maturity index, and vaginal pH, and hot flashes were no better in the treatment vs placebo arms.45
Moreover, studies of various ginsengs have found high rates of bacterial and fungal contamination and highly variable amounts of the presumed active ingredient, ginsenosides.46
CONCLUSION AND RECOMMENDATIONS
While Panax ginseng is widely reputed to be estrogenic, the one trial in the accessible literature found no evidence of estrogenic effects and no significant effect on VMS. Other forms of ginseng have not been studied specifically for menopausal symptoms.
Kudzu (Pueraria lobata)
TRADITIONAL USAGE
Traditional uses include treatment for hangovers, alcoholism, menopause, myalgia, measles, dysentery, gastritis, fever, diarrhea, thirst, allergic rhinitis, colds, and flu.
EVIDENCE FOR MENOPAUSAL MEDICINE
The root, flower, and leaf of kudzu contain isoflavones, such as daidzin, daidzein, puerarin, genistin, and genistein. These are generally well and rapidly absorbed, and converted to aglycones by bacterial activity, as are the isoflavones found in soy foods. It is effective in treating vasomotor symptoms and had similar impact on estradiol, FSH, and LH. Manonai gave postmenopausal women 20, 30, or 50 mg of mirifica vs placebo (51 subjects in treatment modalities, 20 in placebo.) The active arms all reported a decrease in vaginal dryness, and improvements in vaginal maturation index, from pretreatment 46:43:11 (parabasal: intermediate: superficial) to posttreatment 11:65:24 after 24 weeks of therapy.47 Pueraria mirifica (aka Kwao Kruea Khao) 50 mg (and later a study using 50 mg and 100 mg) was compared directly to conjugated estrogens 0.625 mg plus medroxyprogesterone acetate 2.5 mg48 and proved equally effective. These findings contradict earlier work by Woo.49
CONCLUSION AND RECOMMENDATIONS
Kudzu may have estrogen like effects. Further research is need to document efficacy and long term safety.
Maca (Lepidium meyenii, synonym Lepidium peruvianum) Peruvian ginseng, Peruvian maca
TRADITIONAL USAGE
Maca might be regarded as the new world version of ginseng. And like ginseng it is recommended to increase energy and stamina, to enhance athletic performance, and to improve sexual function. Like dong quai, it is said to be a female hormone balancing agent and is offered as a panacea for menstrual disorders and infertility. Interest in maca for menopausal symptoms and osteoporosis appears outside of traditional applications. It is also used as a food stuff.
Dried maca root contains 59% carbohydrates, 10.2% protein, 8.5% fiber, and 2.2% lipids and phyto “estrogens’, it contains a number of phenolic compounds – campesterol, stigmasterol, and beta-sitosterol. Two polyunsaturated fatty acids, macaene and macamide improve sexual and erectile function in animals but this reported evidence does not presage an effect in humans. Like ginseng, maca has been used to treat SSRI induced sexual dysfunction. A small pilot study comparing two doses of maca (but no placebo) found some improvements in scores of sexual function. There was no dose response seen.50
EVIDENCE FOR MENOPAUSAL MEDICINE
Only one study of maca use for menopause is assessable through MEDLINE listings. Fourteen women completed a randomized controlled trial crossover design were they received 3.5 g/day of powered maca for 6 weeks and matching placebo for 6 weeks, in either order, over a total of 12 weeks. Outcomes included estradiol, FSH, LH, SHBG, and Greene Climacteric Scale. The women on maca showed improvement in anxiety, depression, and sexual dysfunction which did not appear to be hormonally mediated.51
Other studies of maca and menopause include abstracts, graduate theses, and articles in nonpeer reviewed journal. A recent review article summarized this body of modest evidence, but robust studies for menopause have yet to be done.52
CONCLUSION AND RECOMMENDATIONS
Maca may indeed have some steroid activity or may act as a steroid receptor modulator. While maca appears to be safe as a food stuff, there is insufficient evidence at this time to support recommending maca for treatment of menopausal symptoms.
Rhubarb (Rheum rhaponticum, Siberian rhubarb)
The roots of rhubarb are used, and the leaves can be toxic. Rhubarb root contains 2–5% anthraquinone derivatives which appear to be responsible for rhubarb’s gastrointestinal effects.
TRADITIONAL USAGE
Traditionally used as a food stuff and for constipation, diarrhea, and other gastrointestinal complaints.
EVIDENCE FOR MENOPAUSAL MEDICINE
A hydrostilbene of derivative resveratrol called rhaponticin, made from an extract of Siberian rhubarb, is being commercially developed (extract ERr 731) as a menopause remedy and branded as Phytoestrol® (Chemisch-Pharmazeutische Fabrik Goeppingen GmbH u Co. KG, Germany) . Virtually all the accessible literature on rhubarb for menopause has been done using this preparation. According to Wober, ERr 731 and its aglyconic metabolites do not activate estrogen receptor alpha, but do demonstrate a dose dependent activation of beta receptors, an action that is inhibited by fulvestrant, an estrogen receptor antagonist. In a 3 day rat study, no uterotropic effects were seen.53 Three clinical reports in the literature are based on study of a single group of patients, a cohort of 110 perimenopausal women aged 45–55 with irregular cycles or with a last menstrual period 3–12 months prior to enrollment. Over 900 women were screened to accrue the 110 who enrolled, with 55 subjects randomized to treatment and 55 to placebo.
An intent to treat analysis found significant improvement in Menopause Rating Scale II, menopause quality of life assessment, and in the number and severity of vasomotor symptoms. Of note is that only seven of the placebo and 39 of the treatment subjects completed the trial. Drop outs from placebo were given the opportunity to enroll in a subsequent open label observation study. Two women in the active treatment arm developed endometrial hyperplasia, though the authors claim that there were no differences in gynecological findings including endometrial biopsies, bleeding, weight, blood pressure, pulse, and laboratory measures.54
Another report based on the same study population found that women randomized to ERr7 reported improvements in Hamilton Anxiety Scale measures and perceptions of health and well being.55 Fifty-one women from the initial study, 23 women continuing out of the ERr731 group, and 28 women crossed over from the placebo group and given ERr731, and all were then enrolled in a long term observational safety protocol. Thus, the 23 women were treated for 336 + 336 days, and 28 were treated for 336 days. At the end of 96 weeks (prior ERr 731) and 48 weeks (prior placebo subjects), respectively, all women had less than 1.4 slight hot flashes per day. There were no significant changes in safety outcomes reported, and no adverse events were observed.56
CONCLUSION AND RECOMMENDATIONS
The total experience on the use of ERr731 rests on a highly selected, small population of women, with 20 followed for 96 weeks and 23 followed for 48 weeks. While the decline in VMS was dramatic in the initial study, the reliability of the data is undermined by a high dropout rate. Additional validation of efficacy and safety should be done.
Ginkgo (Ginkgo biloba)
Ginkgo, also know as maidenhair tree, Asiatic ginseng, Chinese ginseng, and Wonder-of-World, is a very old tree whose leaf extract contains a variety of active flavonoids and terpenes.
TRADITIONAL USAGE
The plant has been used in traditional Chinese medicine for hundreds of years. It is recommended to treat circulatory disorders, tinnitus, premenstrual syndrome, impotence, stroke, shock, headaches, hepatitis, asthma, colitis, and to slow the aging process. Newer suggested uses include treatment of hyperlipemia, enhancement of cerebral blood flow, and treatment of multi-infarct dementia (MID) and Alzheimer’s (AD) and memory loss. It has also been suggested for cochlear deafness. Ginkgo does increase blood flow and tissue perfusion, and stimulates the production of prostaglandins and has some cathecholamine activity.
EVIDENCE FOR MENOPAUSAL MEDICINE
While not specifically recommended for menopausal symptoms, ginkgo is often suggested for cognitive complaints associated with menopause, generalized aging, and for dementias. Clinical trials have demonstrated some improvements in cognitive symptoms in AD and MID. The posited mechanism of action is increased blood flow, and decreased red blood cell aggregation and viscosity. While studies of cognitive function in patients with dementias may show small improvements in function, the literature examining the effects in otherwise healthy individuals has been less encouraging. There are no studies of mid-life or menopausal women. Ginkgo been suggested as an effective therapy in antidepressant induced sexual dysfunction, but the initial reports of success have not been confirmed by subsequent studies.57 Gincosan is a combination of Ginkgo biloba and Panax ginseng was studied in a randomized trial with 30 women in treatment and 20 on placebo for 12 weeks. At 6 and 12 weeks, there were no differences between groups in mood, somatic anxiety, memory or frontal lobe function.58
CONCLUSION AND RECOMMENDATIONS
Since ginkgo causes decreased platelet and red cell aggregation, care should be exercised in recommending it to patients on anti-coagulants, aspirin, and nonsteroidal anti-inflammatory agents. Spontaneous subdural, subarachnoid, retinal, and other bleeds have been reported. It offers no specific verifiable benefits for menopausal women, or other normal aging adults.
Kava (Piper methysticum)
The kava shrub grows in the south Pacific and the roots contain pharmacologically active compounds known as kavapyrones.
TRADITIONAL USAGE
Kava drinks are used in many ritual settings in the pacific islands for spiritual and amusement purposes. Kava is said to act very much like the benzodiazepines, but does not bind directly to benzodiazepine receptors. Suggested sites of action include the limbic center and GABA receptors. Kava also inhibits norepinephrine uptake, antagonizes dopamine, inhibits MAO-B, and decreases glutamate release, but does not interact with opioid receptors.
EVIDENCE FOR MENOPAUSAL MEDICINE
Kava has not been specifically recommended or studied in menopausal women, but rather has been suggested to treat depression and anxiety associated with the menopausal transition. Seven randomized trials have been done, most often comparing kava to benzodiazepines. The studies are small and have methodological flaws. Side effects include disorientation and intoxication. Alcohol and the use of other sedative hypnotics may potentiate kava’s effects.
CONCLUSION AND RECOMMENDATIONS
Severe hepatic toxicity associated with kava use has been reported. Eleven patients who used kava products developed liver failure severe enough to require liver transplantation. Sales of kava have been halted in several European countries. It should not be recommended.59
St. John’s Wort (Hypericum perforatum)
TRADITIONAL USAGE
Extracts of this flower have been used for hundreds of years to treat mild to moderate depression. St. John's wort (SJW) is currently recommended for dysphoria, depression, seasonal affective disorder, and other depressive problems. The constituents include hypericin, pseudohypericin, and flavonoids.60 Several mechanisms of action for the psychotropic effects of SJW have been proposed but not confirmed. These include inhibition of monoamine oxidase (MAO) and catechol methyl-transferase (COMT); decreased corticotropin releasing hormone and then lowering levels of cortisol or affecting GABA receptors in the brain; and serotonin receptor blockade. St. John’s wort inhibits norepinephrine, serotonin, and dopamine reuptake.
EVIDENCE FOR MENOPAUSAL MEDICINE
Again while SJW is not specifically recommended for menopause, it has been widely used for affective changes during the menopausal transition. While SJW appears to be ineffective for severe depression, it is felt to have a place in the treatment of mild to moderate depression.61 In a double-blind randomized placebo-control study, 301 women experiencing climacteric complaints with psychological symptoms were treated with ethanolic SJW and isopropanolic black cohosh extract or a matched placebo for 16 weeks. The Menopause Rating Scale mean score, and psychological complaints were evaluated using the Hamilton Depression Rating Scale sum score. Menopause Rating Scale score decreased 50% (0.46 +/- 0.13 to 0.23 +/- 0.13) in the treatment group and 19.6% (0.46 +/- 0.14 to 0.37 +/- 0.15) in the placebo group.
The Hamilton Depression Rating Scale total score decreased 41.8% in the treatment group (18.9 +/- 2.2 to 11.0 +/- 3.8 points), and 12.7% in the placebo group (18.9 +/- 2.1 to 16.5 +/- 4.3). The treatment was significantly (p <0.001) superior to placebo in both measures.
CONCLUSION AND RECOMMENDATIONS
Side effects with St John’s wort include dry mouth, dizziness, constipation, gastrointestinal upset, sedation, fatigue, and confusion. St John's wort is potentially photosensitizing, and there is a possible increased risk of cataracts with chronic use. Numerous drug–herb interactions have been reported including potentiation of serotonin-reuptake inhibitors, decreased bioavailability of digoxin, theophylline, cyclosporin, and phenprocoumon, and lowering of serum levels of indinavir, oral contraceptives, calcium antagonists, metoprolol, propranolol, phenytoin, rifampin, midazolam, and other anesthetics, by upregulating cytochrome P450 CYP3A. SJW induces changes in the drug efflux transport P-glycoprotein and subsequently may affect levels of drugs which are metabolized through this pathway.62 Anesthesiologists ask that patients discontinue of all botanicals at least 2 weeks prior to elective surgery.
The fixed combination of black cohosh and SJW is superior to placebo in alleviating climacteric complaints, including the related psychological component. A total of 1000 late perimenopausal and menopausal women were treated with a combination of SJW and Vitex agnus-castus. Outcome measures included Greene Climacteric Scale, Hamilton Depression inventory, and Utian Quality Of Life (UQOL) scale. At weeks 4, 8, and 12 there were no discernable differences between the groups. Both groups improved in Greene and HDI scores, but there was no change in either group in the UQOL.63
Valerian (Valeriana officinalis L valerianaceae)
Common valerian or garden heliotrope, has been used for ages as tranquilizer and soporific. The active component has not been identified, but is thought to be a gamma aminobutyric acid derivative. Note that a similar GABA like compound has been found in chamomile, which also is suggested as a herbal sleep remedy and sedative. Before the advent of benzodiazepines and barbiturates, many psychiatric illnesses were treated with valerian. There is no demonstrable toxicity, and the herbal degrades rapidly. There have been a few reports of dystonic reactions and visual disturbances, perhaps due to interactions with other drugs. When taken as an extract, tea or alcohol tincture it produces mild, limited sedating and calming effects without the lingering metabolites seen after taking benzodiazepams. After L-tryptophan was taken off the market, valerian enjoyed a upsurge in use. Studies on sleep architecture have found that valerian reduces sleep latency, prolongs stage 2 nonrapid eye movement (NREM) sleep, and decreases REM and slow-wave sleep (SWS) duration.64 EEG studies have failed to confirm these findings. While adverse events are rare, a recent case report attributed high output congestive heart failure, tachycardia, and delirium to acute withdrawal after prolonged use of large amounts of valerian.65
CONCLUSION AND RECOMMENDATIONS
Valerian may be useful for anxiety and sleep disorders. Caution should be exercised and alcohol and sedative-hypnotics should not be used with valerian.
BEHAVIORAL APPROACHES TO VASOMOTOR SYMPTOMS
There has also been an increasing interest in behavioral approaches given the negative news in the media about hormone therapy. The unresolved controversies about the breast and cardiovascular impact of HT have fomented a general distrust of any pharmacological approach for many women, driving them toward CAM interventions with mind–body practices having a special appeal. Mind–body methods speak of a holistic approach that encompasses not only disease treatment, but also attention to the pursuit of wellness, with emphasis on prevention and health maintenance. This is especially appealing to women with multiple complaints and co-morbid illnesses. It should be noted here that trials of mind–body therapies for menopause have often demonstrated reductions in psychological symptoms as well. Though mind–body therapies provide smaller incremental improvements in symptoms than pharmacological therapies, they have strategic advantages, particularly in patients with coincident stress, anxiety, or depressive disorders. In addition, risks of drug–drug interactions are not at issue.
One of the most studied complementary and alternative medicine mind–body treatments of VMS is acupuncture. Clinical trial results have been encouraging.66, 67, 68 69, 70 71, 72 Studies cite reductions of as much as 53%, but many have methodological design problems. Studies sometimes do not incorporate placebo treatments and the types of placebo needling sites or sham acupuncture may not be appropriate. Deng et al. more recently reported on acupuncture decreasing the number of VMS in cancer survivors from 8.7 per day to 6.2 (SD 4.2) in the true acupuncture group and from 10.0 to 7.6 in the sham group, therefore true acupuncture evidenced 0.8 fewer hot flashes per day than sham at 6 weeks. This differential, however, was not statistical significant. Patients in sham were crossed over and had further reductions. But clearly consistent proof of concept was not achieved.73 Indeed Lee et al. searched 17 databases, and identified six randomized controlled trials including four with sham acupuncture and concluded that these studies failed to show consistent reductions in hot flushes.74
Conclusion
Mind–body interventions may offer some help for women with VMS and impose almost no risk of adverse events. These techniques may be helpful to some women (Table 6). Acupuncture is the most well studied form of mind–body medicine, but the data are inconsistent. The Cochrane Collaborative announced on 8 October 2008 that they are starting to conduct a systematic review of acupuncture for treatment of VMS and described the project protocol.75
Table 5. Mind body approaches to vasomotor symptoms (VMS)
|
|
| Reduction in VMS | Placebo Effect | Difference |
| Relaxation training76 | Relaxation response | Frequency 22% Intensity 26% | Frequency 9% Intensity 6% | NS 20% |
| Relaxation training77 | Self-relaxation (muscle relaxation) | 55%
| 0
| 55%
|
| Paced respiration78 | Paced respiration | 39% | 0 | 39% |
| Reflexology79 | Foot reflexology | 33% | 22% | NS |
| Magnetic therapy80 | Magnetic therapy | 13% | 36% | NS |
| Mindfulness81 | Mindfulness stress reduction | 40% | No control |
|
THE FUTURE OF BOTANICAL MEDICINE FOR MENOPAUSE
Everyone holds hope for more botanical based medicines like aspirin, based on salicin, a compound obtained from the bark of the willow tree; paclitaxel (Taxol), a cancer treatment derived from the northern yew; and digoxin. Unfortunately the promise of the shaman’s apprentice has been little realized. The future of botanical medicine appears to reside in the identification, isolation, purification, and replication of active constituents of plants, thus transforming them into pharmaceuticals. Research and development costs are not necessarily cheaper than the costs of synthetic drug development, since the process of validation demanded is equally rigorous. There are not “alternative” therapies, there are treatments that work and that don’t work regardless of the cultural origins of the modality. Several companies have formed around botanical development. Recent successes include a botanical based treatment of genital warts, which contains sinecatechins derived from a water extract of green tea (Camellia sinensis). Artemisinin, a sesquiterpene lactone endoperoxide isolated from Artemesia annua, has proved to be a fast acting, safe, and effective drug against some strains multidrug-resistant P. falciparum. A company based in the UK has identified a number of drug candidates in the fields of antivirals, antimicrobials, antiinflammatories, and oncology derived from botanical sources. Menopause is ripe for such developments, since the decline of conventional HT. Furthermore, the pipeline for nonhormonal pharmaceuticals for menopause is extremely limited.
When counseling women about alternative treatments for menopause the discussion should include:
1. Documentation of the severity of symptoms;
2. Evaluation of the supporting evidence for efficacy and safety of alternatives;
3. Adequate informed consent;
4. Follow up care at a reasonable interval of time to assess efficacy and safety outcomes;
5. Referral to a qualified provider of alternative practices when women ask for acupuncture, cognitive behavioral therapy, meditation practice, and other CAM interventions.82
Since botanicals continue to be available without a prescription, responsibility rests with the patient, since access to these products cannot be denied. But due warnings should be issued especially for remedies known to be ineffective or known to hold the potential for harm.
REFERENCES
Vessey MP, Doll R: Investigation of relation between use of oral contraceptives and thromboembolic disease. Br Med J 2: 199, 1968 |
|
Rossouw JE, Anderson GL, Prentice RL et al: Risks and benefits of estrogen plus progestin in healthy postmenopausal women:principal results From the Women's Health Initiative randomized controlled trial. JAMA. 2002 Jul 17;288(3):321-33. |
|
Ko RJ: Adulterants in Asian patent medicines. N Engl J Med. 1998 Sep 17;339(12):847. |
|
Grady D: Clinical practice. Management of menopausal symptoms. N Engl J Med. 2006 Nov 30;355(22):2338-47. |
|
http://www.fda.gov/cder/guidance/4592fnl.htm |
|
http://www.usp.org/USPVerified/ingredients/ |
|
De Smet PAGM. Drug theray: herbal remedies. N Engl J Med 2003; 347:2046-56 |
|
http://www.fda.gov/bbs/topics/NEWS/2003/NEW00875.html |
|
Marcus DM, Grollman AP. Sounding Board: Botanical Medicines — The Need For New Regulations N Engl J Med, 2002; 347: 2073-5 |
|
Gold EB, Bair Y, Zhang G et al Cross-sectional analysis of specific complementary and alternative medicine (CAM) use by racial/ethnic group and menopausal status: The Study of Women’s Health Across the Nation (SWAN) Menopause 2007; 14: 612-23 |
|
Adlercreutz H: Western diet and Western diseases: Some hormonal and biochemical mechanisms and associations. Scand J Clin Lab Invest Suppl 201: 3, 1990 |
|
Lu LJ, Anderson KE, Grady JJ et al: Effects of soya consumption for one month on steroid hormones in premenopausal women: Implications for breast cancer risk reduction. Cancer Epidemiol Biomarkers Prev 5: 63, 1996 |
|
Kuiper GG, Carlsson B, Grandien K, Comparison of the ligand binding specificity and transcript tissue distribution of estrogen receptors alpha and beta. Endocrinology 38:863– 70, 1997 |
|
Washburn S, Burke GL, Morgan T, et al: Effect of soy protein supplementation on serum lipoproteins, blood pressure, and menopausal symptoms in perimenopausal women.. Menopause 1999;6:7—13 |
|
Albertazzi P, Pansini F, Bottazzi M, et al: Dietary soy supplementation and phytoestrogen levels Obstet Gynecol. 1999 Aug;94(2):229-31 |
|
Murkies AL, Lombard C, Strauss BJ, et al: Dietary flour supplementation decreases post-menopausal hot flushes: effect of soy and wheat Maturitas. 1995 Apr;21(3):189-95 |
|
Knight DC, Howes JB, Eden JA, et al: Effects on menopausal symptoms and acceptability of isoflavone-containing soy powder dietary supplementation. Climacteric. 2001 Mar;4(1):13-8 |
|
Burke GL, Legault C, Anthony M, et al: Soy protein and isoflavone effects on vasomotor symptoms in peri- and postmenopausal women: the Soy Estrogen Alternative Study. Menopause. 2003 Mar-Apr;10(2):147-53 |
|
Lethaby AE, Brown J, Marjoribank J et al Phytoestrogens for vasomotor menopausal symptoms. Cochrane Database of Systematic Reviews. 2007; 4: 1-64 |
|
Baber RJ, Templeman C, Morton T et al: Randomized placebo-controlled trial of an isoflavone supplement and menopausal symptoms in women. 1999. Climacteric, 2: 85-92 |
|
Knight DC, Howes JB, Eden JA. The effect of Promensil™, an isoflavone extract, on menopausal symptoms 1999. Climacteric, 2: 79-84 |
|
Nachtigall L, Fenichel F et al: Nonprescriptive alternatives to hormonal replacement therapy for postmenopausal women. Female Patient 24: 59, 1999 |
|
van de Weijer PH, Barentsen R. Isoflavones from red clover (Promensil) significantly reduce menopausal hot flush symptoms compared with placebo. Maturitas. 2002 Jul 25;42(3):187-93 |
|
Tice JA, Ettinger B, Ensrud K et al: Phytoestrogen supplements for the treatment of hot flashes: the Isoflavone Clover Extract (ICE) Study: a randomized controlled trial. JAMA. 2003 Jul 9;290(2):207-14 |
|
Faure ED, Chantre P, Mares P et al: Effects of a standardized soy extract on hot flushes: a multicenter, double-blind, randomized, placebo-controlled study.Menopause. 2002 Sep-Oct;9(5):329-34 |
|
Liske E, Hanggi W, Henneicke-von Zepelin HH et al. Physiological investigation of a unique extract of black cohosh (Cimicifugae racemosae rhizoma): a 6-month clinical study demonstrates no systemic estrogenic effect. J. Womens Health Gend. Based Med.11(2),163–174 (2002) |
|
Duker EM, Kopanski L, Jarry H, Wuttke W. Effects of extracts from Cimicifuga racemosa on gonadotropin release in menopausal women and ovariectomized rats. Planta Med 1991.57(5),420–424 |
|
Stoll W. Phytopharmacon influence atrophic vaginal epithelium: double-blind study of cimicifuga vs. Estrogenic substances. Therapeutikon 1987;1:23. |
|
Lehmann-Willenbrock E, Riedel HH. Clinical and endocrinologic studies of the treatment of ovarian insufficiency manifestations following hysterectomy with intact adnexa. 1988 Zentralbl. Gynakol.110(10),611–618 |
|
Newton KM, Reed SD, LaCroix AZ, Grothaus LC, Ehrlich K, Guiltinan J. Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial. Ann Intern Med 2006;145:869-79 |
|
Jacobson JS, Troxel AB, Evans J, et al. Randomized trial of black cohosh for the treatment of hot flashes among women with a history of breast cancer. J Clin Oncol 2001;19:2739-45 |
|
Osmers R, Friede M, Liske E, Schnitker J, Freudenstein J, Henneicke-von Zepelin HH. Efficacy and safety of isopropanolic black cohosh extract for climacteric symptoms. Obstet Gynecol 2005;105:1074-83 |
|
Frei-Kleiner S, Schaffner W, Rahlfs VW, Bodmer C, Birkhauser M. Cimicifuga racemosa dried ethanolic extract in menopausal disorders: a double-blind placebo-controlled clinical trial. Maturitas 2005;51:397-404 |
|
Pockaj BA, Gallagher JG, Loprinzi CL, et al.Phase III double-blind, randomized, placebo controlled crossover trial of black cohosh in the management of hot flashes: NCCTG Trial N01CC1. J Clin Oncol 2006;24:2836-41 |
|
Newton KM, Reed SD, LaCroix AZ, Grothaus LC, Ehrlich K, Guiltinan J. Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial. Ann Intern Med 2006;145:869-79 |
|
Zepelin HH, Meden H, Kostev K, Schröder-Bernhardi D, Stammwitz U, Becher H. Isopropanolic black cohosh extract and recurrence-free survival after breast cancer. Int J Clin Pharmacol Ther. 2007 Mar;45(3):143-54. |
|
Borrelli F, Ernst E. Black cohosh (Cimicifuga racemosa): a systematic review of adverse events. Am J Obstet Gynecol. 2008 Nov;199(5):455-66 |
|
Rotem C, Kaplan B. Phyto-Female Complex for the relief of hot flushes, night sweats and quality of sleep: randomized, controlled, double-blind pilot study. Gynecol Endocrinol. 2007; 23: 117-22 |
|
Hirata JD, Swiersz LM, Zell B, et al. Does dong quai have estrogenic effects in postmenopausal women? A double-blind, placebo-controlled trial. Fertil Steril. 1997; 68(6):981-6. |
|
Blommers J, de Lange-De Klerk ES, Kuik DJ et al: Evening primrose oil and fish oil for severe chronic astalgia: a randomized, double-blind, controlled trial. Am J Obstet Gynecol. 2002;187(5):1389-94 |
|
Budeiri D , Li Wan Po A , Dornan JC. Is evening primrose oil of value in the treatment of premenstrual syndrome? Control Clin Trials 1996; 17(1):60-8 |
|
Budeiri D , Li Wan Po A , Dornan JC. Is evening primrose oil of value in the treatment of premenstrual syndrome? Control Clin Trials 1996; 17(1):60-8 |
|
Chenoy R, Hussain S, Tayob Y, et al: Effect of oral gamolenic acid from evening primrose oil on menopausal flushing. 1994; BMJ 308: 501-503 |
|
Wiklund IK, Mattsson LA, Lindgren R, et al: Effects of a standardized ginseng extract on quality of life and physiological parameters in symptomatic postmenopausal women: a double-blind, placebo-controlled trial. Swedish Alternative Medicine Group. Int J Clin Pharmacol Res. 1999;19(3):89-99 |
|
Krochmal R, Hardy M, Bowerman S Phytochemical Assays of Commercial Botanical Dietary Supplements. Evid Based Complement Alternat Med. 2004;1(3):305-313 |
|
Manonai J, Chittacharoen A, Theppisai U, Theppisai H. Effect of Pueraria mirifica on vaginal health. Menopause. 2007; 14(5):919-24 |
|
Chandeying V, Sangthawan M Efficacy comparison of Pueraria mirifica (PM) against conjugated equine estrogen (CEE) with/without medroxyprogesterone acetate (MPA) in the treatment of climacteric symptoms in perimenopausal women: phase III study. J Med Assoc Thai. 2007; 90(9):1720-6 |
|
Woo J, Lau E, Ho SC, Cheng F, Comparison of Pueraria lobata with hormone replacement therapy in treating the adverse health consequences of menopause. Menopause. 2003 Jul-Aug;10(4):352-61 |
|
Dording CM, Fisher L, Papakostas G, Farabaugh A, Sonawalla S, Fava M, Mischoulon D. A double-blind, randomized, pilot dose-finding study of maca root (L. meyenii) for the management of SSRI-induced sexual dysfunction. CNS Neurosci Ther. 2008 Fall;14(3):182-91 |
|
Brooks NA, Wilcox G, Walker KZ. Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content. Menopause. 2008 Nov-Dec;15(6):1157-62 |
|
Hudson T. Maca: New Insights on an Ancient Plant. Integrative Medicine. Dec 2008/Jan 2009; 6: 55-57 |
|
Wober J, Möller F, Richter T, Activation of estrogen receptor-&b.beta; by a special extract of Rheum rhaponticum (ERr 731®), its aglycones and structurally related compounds 2007; Journal of Steroid Biochemistry and Molecular Biology 107: 191-201 |
|
Heger M, Ventskovskiy BM, Borzenko I, Kneis KC, Rettenberger R, Kaszkin-Bettag M, Heger PW. Efficacy and safety of a special extract of Rheum rhaponticum (ERr 731®) in perimenopausal women with climacteric complaints: A 12-week randomized, double-blind, placebo-controlled trial. Menopause 2006;13(5): 744-759 |
|
Kaszkin-Bettag M, Ventskovskiy BM, Kravchenko A, Rettenberger R, Richardson A, Heger PW, Heger M. The special extract ERr 731® of the roots of Rheum rhaponticum decreases anxiety and improves health state and general well-being in perimenopausal women. Menopause 2007;14:270-283 |
|
Hasper I, Ventskovskiy BM, Rettenberger R, Heger PW, Riley DS, Kaszkin-Bettag M. Long-term efficacy and safety of the special extract ERr 731® of Rheum rhaponticum in perimenopausal women with climacteric complaints. Menopause 2009; 16: 117-131 |
|
Cohen AJ, Bartlik B: Ginkgo biloba for antidepressant-induced sexual dysfunction. J Sex Marital Ther. 1998; 24(2):139-43 |
|
Hartley DE, Elsabagh S, File SE. Gincosan (a combination of Ginkgo biloba and Panax ginseng): the effects on mood and cognition of 6 and 12 weeks’ treatment in post menopausal women. Nutr Neurosci. 2004; 7: 325-33 |
|
Hepatic toxicity possibly associated with kava-containing products--United States, Germany, and Switzerland, 1999-2002. MMWR Morb Mortal Wkly Rep. 2002 Nov 29;51(47):1065-7 |
|
Hypericum Depression Trial Study Group: Effect of Hypericum perforatum (St John's wort) in major depressive disorder: a randomized controlled trial. Hypericum Depression Trial Study Group. JAMA. 2002; 287(14):1807-14 |
|
Uebelhack R, Blohmer JU, Graubaum HJ, Black cohosh and St. John's wort for climacteric complaints: a randomized trial. Obstet Gynecol. 2006 Feb;107(2 Pt 1):247-55 |
|
The Medical Letter, Drug Interactions with St. John’s Wort, Jun 26, 2000 |
|
Van Die MD, Burger HG, Bone KM. Hypericum perforatum with Vitex agnus castus in menopausal symptoms: a randomized, controlled trial. Menopause 2009; 156-163 |
|
Leathwood PD, Chauffard F, Heck E, et al Aqueous extract of valerian root improve sleep quality in man. Pharmacology, Biochem And Behavior. 1982; 17: 65-71 |
|
Garges HP, Varia I, Doraiswamy PM. Cardiac complications and delirium associated with valerian root withdrawal. JAMA 1998;280:1566-67 |
|
Cohen SM, Rousseau ME, Carey BL. Can acupuncture ease the symptoms of menopause? Holist. Nurs. Pract. 2003; 17:295–299 |
|
Wyon Y, Wijma K, Nedstrand E, Hammar M. A comparison of acupuncture and oral estradiol treatment of vasomotorsymptoms in postmenopausal women. Climacteric 2004; 7:153–164 |
|
Nedstrand E,Wijma K,Wyon Y,HammarM. Vasomotor symptoms decrease in women with breast cancer randomized to treatment with applied relaxation or electro-acupuncture: a preliminary study. Climacteric 2005; 8:243–50. |
|
Huang MI, Nir Y, Chen B, Schnyer R, Manber R. A randomized controlled pilot study of acupuncture for postmenopausal hot flashes: effect on nocturnal hot flashes and sleep quality. Fertil Steril 2006;86(3):700–10. |
|
Nir Y, Huang MI, Schnyer R, Chen B, Manber R. Acupuncture for postmenopausal hot flashes. Maturitas 2007;56(4):383–95. |
|
Vincent A, Barton DL, Mandrekar JN, et al .Acupuncture for hot flashes: a randomized, sham controlled clinical study. Menopause 2007;14(1):45–52. |
|
Zaborowska E, Brynhildsen J, Damberg S, et al. .Effects of acupuncture, applied relaxation, estrogens and placebo on hot flushes in postmenopausal women: an analysis of two prospective, parallel, randomized studies. Climacteric 2007;10(1):38–45. |
|
Deng G, Vickers AJ, Yeung KS. Randomized, Controlled Trial of Acupuncture for the Treatment of Hot Flashes in Breast Cancer Patients. J Clin Oncol. 2007; 25:5584-5590. |
|
Lee MS, Shin BC, Ernst E. Acupuncture for treating menopausal hot flushes: a systematic review. Climacteric. 2009 Feb;12(1):16-25 |
|
Dodin S, Asselin G, Blanchet C, Thiebaut C, Gravel K, Marc I, Maunsell E, Ernst E, Wu T. Acupuncture for menopausal hot flushes. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD007410. DOI: 10.1002/14651858.CD007410 |
|
Irvin JH, Domar AD, Clark C, Zuttermeister PC, Friedman R. The effects of relaxation response training on menopausal symptoms. J Psychosom. Obstet.Gynaecol. 1996;. 17:202–207 |
|
Germaine LM, Freedman RR. Behavioral treatment of menopausal hot flashes: evaluation by objective methods. J. Consult. Clin. Psychol. 1984 52: 1072–1079 (1984). |
|
Freedman RR, Woodward S. Behavioral treatment of menopausal hot flushes:evaluation by ambulatory monitoring. Am. J. Obstet. Gynecol.1992; 167: 436– 439(1992). |
|
Williamson J, White A, Hart A, Ernst E. Randomised controlled trial of reflexology for menopausal symptoms. BJOB 2002; 109:1050–1055 . |
|
Carpenter JS, Wells N, Lambert B et al.A pilot study of magnetic therapy for hot flashes after breast cancer. Cancer Nurs. 2002; 25: 104–109 (2002). |
|
Carmody J, Crawford S, Churchill L. A pilot study of mindfulness-based stress reduction for hot flashes. Menopause 2006; 13: 760–769. |
|
Cohen MH, Eisenberg DM: Potential physician malpractice liability associated with complementary and integrative medical therapies. Ann Intern Med. 2002; 136(8):596-603. |
|
Sacks FM, Lichtenstein A., Van Horn L. et al Soy Protein, Isoflavones, and Cardiovascular Health. A Summary of a Statement for Professionals From the American Heart Association Nutrition Committee. Arteriosclerosis, Thrombosis, and Vascular Biology. 2006;26:1689-1692 doi: 10.1161/01.ATV.0000227471.00284.ef |