
Chapter 5
Theater Set Up
(see Video 1: Theater set up)
Video 1 Theater set up
The operating theater is not a playing field where the dimensions are prescribed by written rules. Here, the thought should always be ‘larger is better’, because there must be sufficient space to accommodate the patient’s theater table, the anesthetic machine and its accessories, the electronic cart, the laparoscopic instrument trolley, the vaginal instrument trolley and much more.
Having said this, it is important to remember that the contents of the theater can be structured in such a way that they should not take up an inordinate amount of space or waste it. Simply stated, clutter must be kept to an absolute minimum, and the room must never be used as a storage closet. Apart from the specific equipment accommodation, there should be space for the surgeon, two surgical assistants, anesthetist, anesthetic assistant, scrub nurse, and scriber (to document and print what material was used, how many bags of IV fluid were used, etc.).
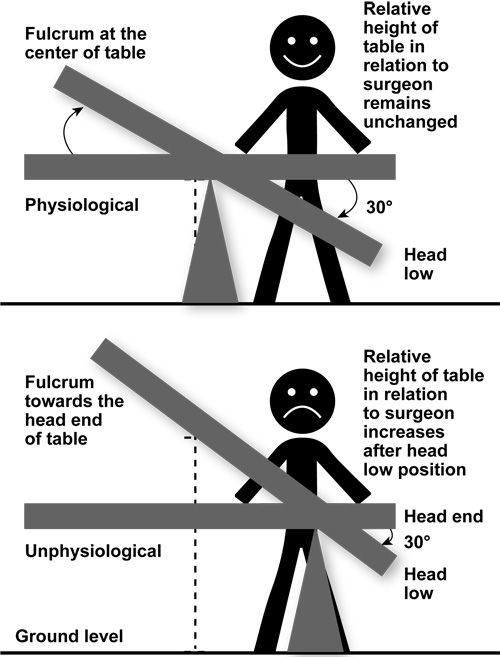
Figure 2 Diagrammatic representation of fulcrum of table: surgeon standing relative to height of table
Video 2 Theater table
A laminated page wherein contact details of all relevant personnel should be present in the theater on the wall where it can be easily seen. Relevant persons include vascular surgeon, general surgeon, gynecological oncologist, ambulance and blood bank services, nearest high dependency unit/intensive care unit, etc.
When the patient arrives in the theater reception area, a formal ‘sign in’ should take place with a checklist. The receiving nurse and the surgeon should confirm this official ‘time out’ which should be conducted in the presence of the operating surgeon and anesthetist before induction or use of any anesthetic agent. According to WHO requirements, the following things should be elicited: name of the patient; confirmation of patient identity; confirmation of the procedure to be performed; introduction of the team members; any specific concerns related to the surgical procedure; estimated probable length of surgery; anesthesia concerns, such as difficult intubation; allergies; and estimated blood loss. If there are any additional informational and/or consenting requirements, this moment represents the final opportunity before the patient goes under anesthesia. All the necessary relevant documents including laboratory investigations and ultrasound report and images should be available.