This chapter should be cited as follows:
Dhanji S, Jurkovic D, Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.419703
The Continuous Textbook of Women’s Medicine Series – Gynecology Module
Volume 10
Ultrasound in gynecology
Volume Editors:
Professor Antonia Testa, Agostino Gemelli University Hospital, Rome, Italy
Professor Simona Maria Fragomeni, Agostino Gemelli University Hospital, Rome, Italy
Chapter
Fallopian Tube Abnormalities on Ultrasound
First published: May 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Transvaginal ultrasound plays a central role in the assessment of adnexal structures and is often the first-line imaging modality for evaluating Fallopian tube pathology. Although normal Fallopian tubes are not consistently visualized, a wide spectrum of pathological conditions may render them detectable, ranging from inflammatory and infectious processes to benign and malignant neoplasms, as well as pregnancy-related disorders. Accurate recognition of tubal abnormalities is essential, as these conditions are frequently associated with significant morbidity, including infertility, chronic pelvic pain, and life-threatening complications such as ectopic pregnancy and sepsis.
Advances in high-resolution ultrasound technology, combined with the use of Doppler imaging and contrast-enhanced techniques, have significantly improved the ability to characterize tubal morphology and vascularity. In addition, increasing awareness of specific sonographic signs, such as the cogwheel and beads-on-a-string appearances, has enhanced diagnostic confidence in differentiating acute from chronic disease.
This chapter provides a comprehensive overview of the normal sonographic appearance of the Fallopian tubes and the key ultrasound features of common tubal pathologies, with an emphasis on clinically relevant findings that aid diagnosis, guide management and improve patient outcomes.
NORMAL FALLOPIAN TUBES
Assessment of the Fallopian tubes is a routine part of every gynecological ultrasound examination. The interstitial portions of the tube are visible as they leave the endometrial cavity and this remains a key landmark for the identification of congenital uterine anomalies, such as a unicornuate uterus. Identification of the interstitial portion of the Fallopian tube (Figure 1) is also important in excluding interstitial ectopic pregnancy, a rare form that accounts for 3% of all ectopic pregnancies.

1
Transverse section through the uterine fundus showing the right interstitial tube (arrow) which appears as a thin line lateral to the right upper aspect of the endometrial cavity.
The fimbrial ends of the Fallopian tubes are harder to see except in the presence of peritoneal free fluid, which is typically seen after ovulation or in pathological conditions such as ascites. The fimbrial ends of healthy tubes can be seen floating freely in fluid within the pouch of Douglas (Figure 2). The ampullary and isthmic parts of the healthy Fallopian tube are the most difficult to see. However, with modern high-resolution ultrasound machines, they can sometimes be visualized as elongated structures with a hypoechoic outer muscular wall and a central hyperechoic mucosal layer (Figure 3). Nevertheless, contrast-enhanced examinations, such as saline sonohysterography or hysterosalpingo-contrast sonography (HyCoSy), are required to assess reliably the morphology and patency of the Fallopian tube (Figure 4).

2
Fimbrial end of Fallopian tube (F), seen floating freely within the fluid in the pouch of Douglas.

3
A normal Fallopian tube with prominent endosalpinx (E) surrounded by hypoechoic muscularis layer (arrows).

4
Example of normal Fallopian tube filled with contrast (arrows) during hysterosalpingo contrast sonography (HyCoSy). UT, uterus.
PELVIC INFLAMMATORY DISEASE
Pelvic inflammatory disease (PID) is a spectrum of conditions involving inflammation of the female genital tract, including the uterus, Fallopian tubes and adjacent pelvic organs. It typically results from an ascending infection originating in the lower genital tract, leading to cervicitis, endometritis and subsequently salpingitis. This may result in spillage of infected material from the salpinx into the surrounding peritoneum. Adhesion formation may occlude the distal end of the tube, leading to accumulation of pus and formation of pyosalpinx. The adjacent ovaries may also become infected, resulting in an ovarian abscess, which can progress to a tubo-ovarian complex and ultimately to a tubo-ovarian abscess.1
PID may be secondary to sexually transmitted infections such as Chlamydia trachomatis, Neisseria gonorrhoeae and Mycoplasma genitalium, as well as micro-organisms that comprise the normal vaginal flora.2 Although sexually transmitted pathogens often initiate infection, tubo-ovarian abscesses are typically polymicrobial and often involve anaerobic bacteria.
PID is commonly associated with abdominal pain and fever, although fewer than one-third of patients are febrile.3 Other presenting symptoms include abnormal vaginal discharge, abnormal uterine bleeding, nausea, vomiting and lower back pain.
Early diagnosis and appropriate antibiotic therapy are essential to prevent long-term complications resulting from tubal inflammation and scarring. Common sequelae include infertility due to tubal occlusion by scar tissue, increased risk of ectopic pregnancy and chronic pelvic pain.
Transvaginal ultrasound can be used to aid the diagnosis of PID, monitor response to treatment and guide intervention, where appropriate.
Acute pelvic infection
Pyosalpinx
Pyosalpinx refers to the acute inflammation of the Fallopian tube that contains pus, secondary to PID. Timor-Tritsch et al. described the ultrasound features of a pyosalpinx as an elongated cystic adnexal structure containing echogenic fluid (suggesting purulent material and blood), with a thick wall (> 3 mm) and incomplete septations.4 In cross section, the distended tube may demonstrate the ‘cogwheel’ sign due to thickened endosalpingeal folds (Figure 5).

5
Example of acutely inflamed Fallopian tube (arrow) which is distended with fluid. Note the presence of thick and edematous mucosal folds.
Tubo-ovarian complex
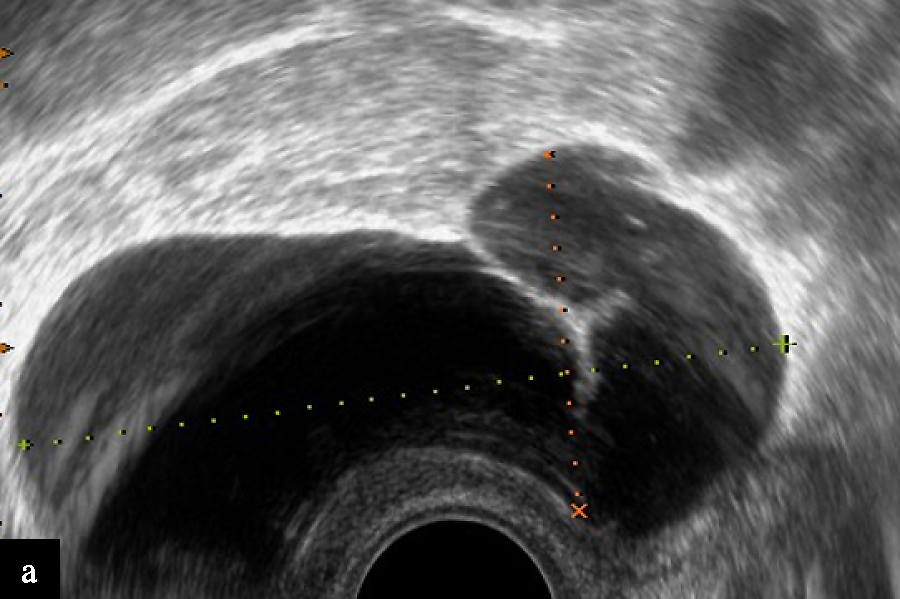
As PID progresses, the inflammatory process may extend beyond the Fallopian tubes to involve the ovary, resulting in the formation of a tubo-ovarian complex. This entity is characterized by inflammation and adhesion of the ovary to the pyosalpinx, though each structure remains at least partially distinguishable. On transvaginal ultrasound, the ovary typically has ill-defined borders and although it may appear as a separate structure from the adjacent pyosalpinx, it cannot be separated from it with gentle pressure from the probe, suggestive of adhesion (Figure 6, Video 1).

6
Example of acute tubo-ovarian complex. The ovary is enlarged with an abscess (O) and the Fallopian tube (FT) is distended with pus. Although the tube is firmly adhered to the ovary, the organs are clearly discernible.
1
Case of tubo-ovarian complex. Note the large ovarian abscess and dilated tube fixed to the ovary.
A tubo-ovarian complex represents an intermediate stage between early PID and a fully formed tubo-ovarian abscess. Clinically, patients typically present with acute symptoms of PID. Prompt diagnosis and treatment are essential to prevent progression and avoid long-term sequelae such as infertility, chronic pelvic pain and ectopic pregnancy.
Tubo-ovarian abscess
A tubo-ovarian abscess represents a more advanced stage of infection, in which the normal anatomical planes between the ovary and Fallopian tube are obliterated due to necrotic changes caused by severe inflammation. The resulting inflammatory mass often appears as a thick-walled, complex adnexal tumor with septations and mixed internal echoes suggestive of purulent fluid and debris. On ultrasound, neither the ovary nor the tube can be reliably identified as separate structures (Figure 7, Video 2). The mass is usually tender when palpated with the transvaginal probe. In the most severe cases, the infection may spread contralaterally, resulting in bilateral tubo-ovarian abscesses that occupy the cul-de-sac and both adnexal regions.5 Such extensive disease may necessitate inpatient management with intravenous antibiotics, ultrasound-guided transvaginal or transabdominal drainage of the abscess (Video 3) or surgical management with laparoscopic drainage of the abscess. Image-guided drainage of tubo-ovarian abscesses is associated with a higher success rate, reduced complication rate and reduced hospital stay when compared with laparoscopy.6

7
Tubo-ovarian abscess appearing as a large multilocular lesion filled with echogenic fluid representing pus. Normal ovarian and tubal morphological features are absent.
2
Case of acute tubo-ovarian abscess. The ovary and the tube can be reliably identified as separate structures.
3
Example of transvaginal drainage of pelvic abscess.
Hyperechoic foci with posterior acoustic shadowing within the endometrial cavity may represent gas locules and are suggestive of infection. Echogenic material may also be visible within the pouch of Douglas, suggestive of debris or pus, particularly in advanced infection.7
Chronic pelvic infection
Hydrosalpinx
Hydrosalpinx occurs when fluid accumulates within the lumen of a Fallopian tube due to obstruction of the fimbrial end. Distal tube occlusion is most commonly caused by PID. Other causes include endometriosis, tubal malignancy, tubal ectopic pregnancy and paratubal adhesions.
Ultrasound features that may be useful in distinguishing a hydrosalpinx from other cystic adnexal lesions include the presence of an anechoic, tubular, cystic structure with incomplete septa (Figure 8a, Video 4). The tubal wall is often thin (< 5 mm) with minimal vascularity and, on cross section, displays the ‘beads-on-a-string’ sign (Figure 8b)4
|
|
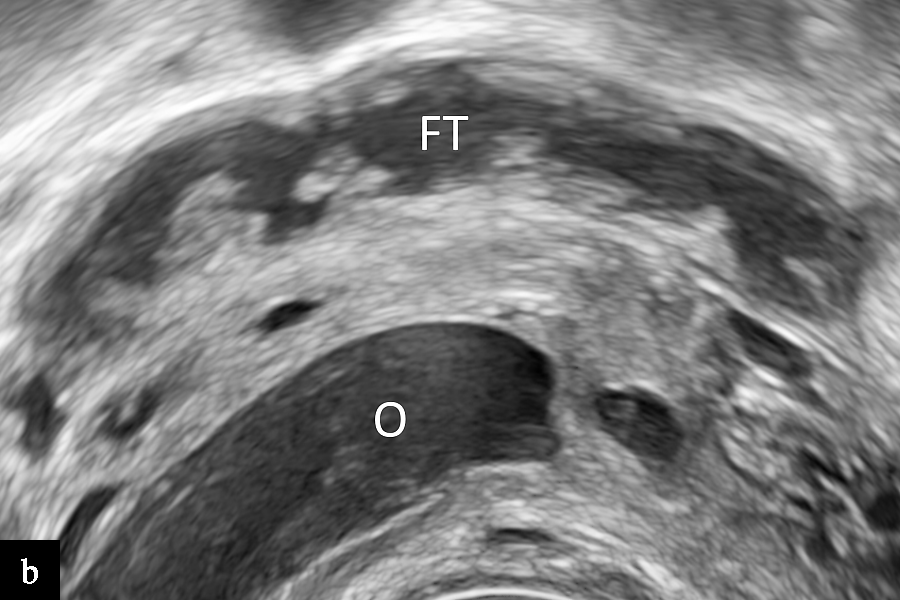
8
Images of hydrosalpinx, showing: (a) a large tubular cyst filled with hypoechoic fluid (note the presence of thin, incomplete septations); and (b) a dilated Fallopian tube (FT) with typical 'beads-on-a-string' sign behind a normal ovary (O).
4
Typical appearance of hydrosalpinx on ultrasound scan.
Chronic tubo-ovarian complex
Chronic tubo-ovarian complex usually appears as a cystic structure which is filled with anechoic or hypoechoic fluid. The inner cyst wall is irregular and is partially formed by the ovarian tissue and partially by a dilated tube. The cyst may also contain complete or partial septations. The complex is typically firmly adhered to the surrounding pelvic structures (Figure 9). The differential diagnosis includes peritoneal pseudocyst which is also a sequela of severe pelvic inflammation or surgical trauma. These represent collections of peritoneal fluid which become trapped within adhesions and often encompass a normal ovary or Fallopian tube.

9
Example of a chronic tubo-ovarian complex with complete loss of normal ovarian and tubal structures.
TUBAL TUMORS
Fimbrial cysts
Fimbrial cysts are among the most common adnexal lesions and originate from the mesothelium of the broad ligament.8 They are usually small and asymptomatic but can occasionally cause pelvic pain due to torsion. Fimbrial cysts are sometimes misdiagnosed as ovarian cysts, which may lead to unnecessary surgical intervention. Accurate diagnosis on ultrasound has the potential to reduce such interventions.
Characteristic features of fimbrial cysts on ultrasound include an anechoic, thin-walled, unilocular cyst, adjacent to the ovary. Visualizing the ipsilateral ovary separately from the cyst is helpful in differentiating between fimbrial and ovarian cysts (Figure 10). This can be assessed by applying gentle pressure with the tip of the vaginal probe between the ovary and the fimbrial cyst, known as the ‘sliding organs’ sign.9

10
Small simple cystic lesion adjacent to a normal ovary (O). This is the typical ultrasound appearance of a fimbrial cyst (FC).
Although the incidence of borderline fimbrial tumors is low, cases have been reported in the literature. Key sonographic features of borderline fimbrial tumors include the presence of papillary projections (Figure 11), with or without vascularity on color Doppler.10

11
Small serous borderline tumor arising from a fimbrial cyst. Note prominent papillary projection (P).
Benign tubal tumors
Benign tubal tumors are extremely rare, and their precise incidence is unknown. They can arise from the tubal wall or tubal lumen, or project from the fimbrial end of the tube. Many tumors of the Fallopian tube are histologically identical to those more commonly found within the ovary or endometrium. The histological types that have been reported include papilloma, fibroadenoma, fibroma, leiomyoma, lipoma, hemangioma, teratoma and adenomatoid tumor (Figure 12), lymphangioma, mesothelioma and mesonephroma11 .

12
Benign adenomatoid tumor of the Fallopian tube presenting as a solid swelling (TM) adjacent to a normal ovary (O).
Primary malignant neoplasm
Primary malignant neoplasm of the Fallopian tube accounts for 0.14–1.8% of all gynecological malignancies.12 This is likely an underestimate, as it is now widely accepted that a number of high-grade serous ovarian carcinomas originate from the fimbrial epithelium of the Fallopian tube and subsequently involve the ovary.13 Serous adenocarcinoma accounts for around 80% of Fallopian tube malignancies; other histotypes include endometrioid, clear cell and squamous carcinoma.14
Primary carcinoma of the Fallopian tube typically affects postmenopausal women and has been associated with nulliparity, infertility and history of chronic pelvic infection.15,16 It may present with abnormal vaginal bleeding, watery vaginal discharge (hydrops tubae profluens) and colicky lower abdominal pain. This triad of symptoms was first described by Latzko in 1916, however is reported in less than 15% of cases.17
On ultrasound, tubal carcinoma typically appears as a thin-walled, cystic, sausage-shaped structure which often contains solid, papillary projections; however, it may also appear as a thin-walled cystic structure with large solid components within it, or a completely solid mass (Figure 13). The cystic contents are usually anechoic and the structure is highly vascularized on Doppler assessment.14
|
|
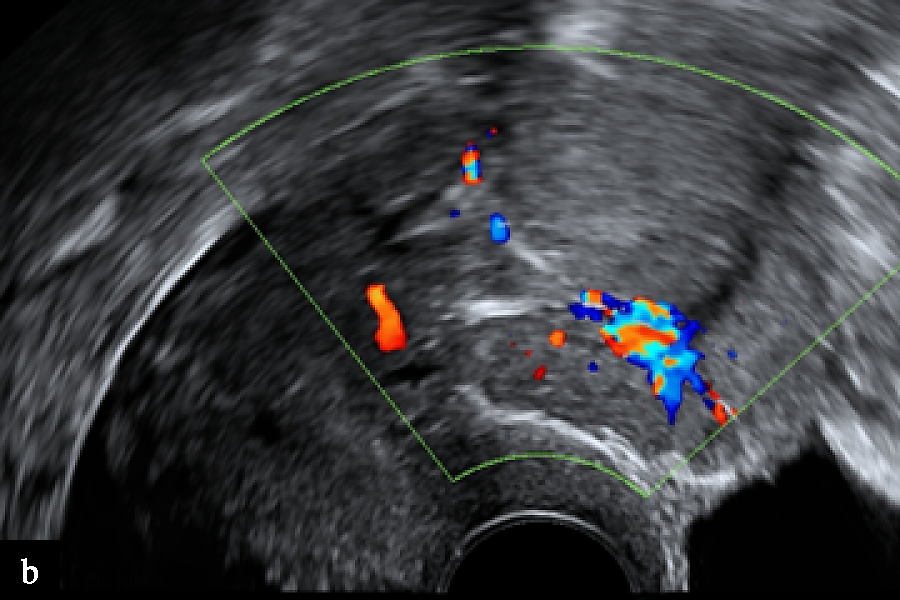
13
(a) Typical ultrasound findings in a case of primary tubal carcinoma, which presented as a tubular solid adnexal tumor. (b) On Doppler examination, the lesion was moderately vascular.
It is important to differentiate tubal cancer from benign pathology such as hydrosalpinx or pyosalpinx, which may have a similar appearance on ultrasound. Although a pyosalpinx often has swollen mucosal folds, which appear as incomplete septa, a tubal cancer is more likely to have only one or two solid protrusions. In addition, the echogenicity in a pyosalpinx is often ground glass rather than anechoic as it contains pus. Furthermore, a pyosalpinx usually has a thick wall, in contrast to a tubal cancer which has a thin wall.
Metastatic tubal tumors
Metastatic involvement of the Fallopian tube is relatively uncommon, except in cases in which there is direct extension from ovarian malignancies. Such metastases are often asymptomatic and are usually identified only on microscopic examination. This is likely because clinical symptoms tend to be driven by the primary malignancy or by more prominent ovarian metastases. Common gynecological primary sources include cancers of the ovary, uterus and cervix. Among non-gynecological primaries, abdominal tumors, particularly colorectal, appendiceal and gastric cancers, are the most frequent.18 Breast cancer has also been reported as a less common origin.19
TUBAL TORSION
Isolated torsion of the Fallopian tube, or torsion of a fimbrial cyst, is extremely rare and the incidence remains unknown. It is challenging to diagnose given the non-specific presenting symptoms such as lower abdominal pain, nausea, vomiting and fever.
Risk factors for tubal torsion include the presence of tubal pathology such as fimbrial cysts, ovarian masses or hydrosalpinx, however, it may also occur in the absence of these findings.
Sonographic features are non-specific; however, an edematous, dilated Fallopian tube and a normal ipsilateral ovary may suggest isolated tubal torsion. A dilated Fallopian tube appears as a distended, tubular structure with a hyperechoic wall and a folded configuration that tapers towards the cornua of the uterus.20 The ‘whirlpool’ sign may be present on power Doppler, as the venous circulation is seen in a circular pattern.21
TUBAL ENDOMETRIOSIS
Endometriosis is characterized by the presence of ectopic endometrial stroma and glands outside of the uterus and is thought to affect around 10% of women of reproductive age.22 Tubal endometriosis refers specifically to the ectopic endometrial tissue on the Fallopian tubes and can further be divided into intraluminal and extraluminal disease. The incidence of tubal endometriosis is uncertain; however, it has been reported to range from 7% to 69%.23 The most common symptoms associated with endometriosis include dysmenorrhea, pelvic pain and infertility.
The ultrasound features of tubal endometriosis are non-specific. A common finding, however, is a slightly distended, fluid-filled tube that is thought to result from significant tubal damage or obstruction, leading to hydrosalpinx and hematosalpinx. Extraluminal endometriosis is more commonly associated with hydrosalpinx due to external adhesions, whereas intraluminal endometriosis may cause cyclical bleeding, resulting in hematosalpinx.24
THE FALLOPIAN TUBE AND EARLY PREGNANCY
Hematosalpinx and ectopic pregnancy
Hematosalpinx refers to blood within the lumen of the Fallopian tube. This can occur as a result of a tubal ectopic pregnancy, retrograde bleeding during miscarriage, endometriosis or the presence of obstructive hematometra.
Ectopic pregnancies account for 2% of all pregnancies. 90% of these are located within the Fallopian tube. Risk factors include a previous ectopic pregnancy, previous PID, tubal surgery or the presence of an intrauterine device. Prompt diagnosis is crucial due to the risk of tubal rupture which may result in hemoperitoneum and hemodynamic instability. Diagnosis of an ectopic pregnancy is made by ultrasound assessment whilst measurements of serum hCG and progesterone are useful for monitoring patients who opt for conservative management.
Ultrasound features of a tubal ectopic pregnancy range from a gestational sac containing a live embryo to a small solid tubal swelling (Figure 14). In modern practice, ultrasound diagnosis is highly accurate regardless of the morphological type of ectopic.25,26

14
Case of live tubal ectopic pregnancy (arrow) adjacent to the uterus (UT).
In tubal ectopic pregnancy, the gestational sac is often surrounded by blood, resulting in distension of the Fallopian tube (Figure 15). Rajah et al.27 recommend that, in the presence of hematosalpinx, the size of the Fallopian tube distended with blood should be measured in addition to the size of ectopic pregnancy, as tubal size correlates more strongly with surgical findings than measurement of the ectopic gestation alone.

15
Tubal pregnancy presenting as an empty gestational sac (EP). The pregnancy is surrounded by a blood clot forming a large hematosalpinx (HS).
Residual ectopic pregnancy
A residual ectopic pregnancy refers to a discrete solid adnexal tumor on ultrasound separate from the ovary with a negative pregnancy test.28 This occurs when pregnancy implants within the Fallopian tube, undergoes regression and becomes non-functional. The residual pregnancy is typically composed of trophoblastic tissue, which has undergone degenerative changes, and organized blood clots. They are often asymptomatic but can present with lower abdominal pain, and they have been reported to mimic other pathologies such as fibroids and tubal carcinoma29,30 (Figure 16). In most cases, residual ectopic pregnancy eventually clears spontaneously with expectant management, and surgical excision is rarely necessary.

16
Example of a residual tubal ectopic pregnancy (RE) which presented as a hypoechoic solid lesion adjacent to a normal ovary with a dominant follicle (O).
CONCLUSION
The Fallopian tubes play a vital role in female reproductive health, and their pathology encompasses a broad spectrum of conditions ranging from infection and inflammation to benign and malignant neoplasms. Advances in transvaginal ultrasound imaging have significantly improved our ability to visualize and differentiate normal and abnormal tubal anatomy, allowing for earlier and more accurate diagnosis and management of various tubal abnormalities. Continued refinement of imaging criteria and awareness of the varied presentations of tubal pathology will remain central to optimizing gynecological care.
PRACTICE RECOMMENDATIONS
- Assessment of the Fallopian tubes should be a routine component of transvaginal ultrasound, even when not clearly visualized, as indirect signs of pathology may be present.
- Visualization of the interstitial portion of the tube is an important landmark for identifying congenital uterine anomalies and excluding interstitial ectopic pregnancy.
- Recognition of characteristic ultrasound signs improves diagnostic accuracy, including the ‘cogwheel’ sign in acute salpingitis and the ‘beads-on-a-string’ sign in hydrosalpinx.
- Pelvic inflammatory disease should be suspected in the presence of complex adnexal masses, particularly when associated with pain, fever and echogenic pelvic fluid.
- Differentiation between pyosalpinx, tubo-ovarian complex and tubo-ovarian abscess is essential, as these represent a spectrum of disease with increasing severity and different management strategies.
- Hydrosalpinx should be distinguished from other cystic adnexal lesions by its tubular shape, incomplete septations and typical sonographic signs.
- Demonstrating separation between the ovary and an adnexal cyst is key in distinguishing fimbrial cysts from ovarian cysts (e.g. using the ‘sliding-organs’ sign).
- Suspicion of tubal malignancy should be raised in the presence of solid components, papillary projections and increased vascularity, particularly in postmenopausal women.
- In suspected ectopic pregnancy, careful assessment of the Fallopian tube is critical, and measurement of tubal distension (hematosalpinx) may better correlate with surgical findings than gestational size alone.
- Early and accurate ultrasound diagnosis of tubal pathology is essential to guide timely management and reduce the risk of complications such as infertility, chronic pelvic pain and life-threatening hemorrhage or sepsis.
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Crum-Cianflone NF. Pelvic Inflammatory Disease. N Engl J Med. 2015 Aug 13;373(7):686. doi: 10.1056/NEJMc1507793. PMID: 26267641. | |
Soper DE. Pelvic inflammatory disease. Obstet Gynecol. 2010 Aug;116(2 Pt 1):419–428. doi: 10.1097/AOG.0b013e3181e92c54. PMID: 20664404. | |
Eckert LO, Hawes SE, Wölner-Hanssen PK, Kiviat NB, Wasserheit JN, Paavonen JA, Eschenbach DA, Holmes KK. Endometritis: the clinical-pathologic syndrome. Am J Obstet Gynecol. 2002 Apr;186(4):690–695. doi: 10.1067/mob.2002.121728. PMID: 11967492. | |
Timor-Tritsch IE, Lerner JP, Monteagudo A, Murphy KE, Heller DS. Transvaginal sonographic markers of tubal inflammatory disease. Ultrasound Obstet Gynecol. 1998 Jul;12(1):56–66. doi: 10.1046/j.1469-0705.1998.12010056.x. PMID: 9697286. | |
Horrow MM. Ultrasound of pelvic inflammatory disease. Ultrasound Q. 2004 Dec;20(4):171–179. doi: 10.1097/00013644-200412000-00003. PMID: 15602219. | |
Goje O, Markwei M, Kollikonda S, Chavan M, Soper DE. Outcomes of Minimally Invasive Management of Tubo-ovarian Abscess: A Systematic Review. J Minim Invasive Gynecol. 2021 Mar;28(3):556–564. doi: 10.1016/j.jmig.2020.09.014. Epub 2020 Sep 28. PMID: 32992023. | |
Chappell CA, Wiesenfeld HC. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess. Clin Obstet Gynecol. 2012 Dec;55(4):893–903. doi: 10.1097/GRF.0b013e3182714681. PMID: 23090458. | |
Barloon TJ, Brown BP, Abu-Yousef MM, Warnock NG. Paraovarian and paratubal cysts: preoperative diagnosis using transabdominal and transvaginal sonography. J Clin Ultrasound. 1996 Mar–Apr;24(3):117–122. doi: 10.1002/(SICI)1097-0096(199603)24:3<117::AID-JCU2>3.0.CO;2-K. PMID: 8838299. | |
Savelli L, Ghi T, De Iaco P, Ceccaroni M, Venturoli S, Cacciatore B. Paraovarian/paratubal cysts: comparison of transvaginal sonographic and pathological findings to establish diagnostic criteria. Ultrasound Obstet Gynecol. 2006 Sep;28(3):330–334. doi: 10.1002/uog.2829. PMID: 16823765. | |
Zhao F, Zhang H, Ren Y, Kong F. Transvaginal sonographic characteristics of paraovarian borderline tumor. Int J Clin Exp Med. 2015 Feb 15;8(2):2684–2688. PMID: 25932220; PMCID: PMC4402867. | |
Green TH Jr, Scully RE. Tumors of the fallopian tube. Clin Obstet Gynecol. 1962 Sep;5:886–906. doi: 10.1097/00003081-196209000-00022. PMID: 13901452. | |
Kalampokas E, Kalampokas T, Tourountous I. Primary fallopian tube carcinoma. Eur J Obstet Gynecol Reprod Biol. 2013 Jul;169(2):155–161. doi: 10.1016/j.ejogrb.2013.03.023. Epub 2013 Apr 23. PMID: 23622731. | |
Kindelberger DW, Lee Y, Miron A, Hirsch MS, Feltmate C, Medeiros F, Callahan MJ, Garner EO, Gordon RW, Birch C, Berkowitz RS, Muto MG, Crum CP. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol. 2007 Feb;31(2):161–169. doi: 10.1097/01.pas.0000213335.40358.47. PMID: 17255760. | |
Ludovisi M, De Blasis I, Virgilio B, Fischerova D, Franchi D, Pascual MA, Savelli L, Epstein E, Van Holsbeke C, Guerriero S, Czekierdowski A, Zannoni G, Scambia G, Jurkovic D, Rossi A, Timmerman D, Valentin L, Testa AC. Imaging in gynecological disease (9): clinical and ultrasound characteristics of tubal cancer. Ultrasound Obstet Gynecol. 2014 Mar;43(3):328–335. doi: 10.1002/uog.12570. PMID: 23893713. | |
Demopoulos RI, Aronov R, Mesia A. Clues to the pathogenesis of fallopian tube carcinoma: a morphological and immunohistochemical case control study. Int J Gynecol Pathol. 2001 Apr;20(2):128–132. doi: 10.1097/00004347-200104000-00003. PMID: 11293157. | |
Schneider C, Wight E, Perucchini D, Haller U, Fink D. Primary carcinoma of the fallopian tube. A report of 19 cases with literature review. Eur J Gynaecol Oncol. 2000;21(6):578–582. PMID: 11214613. | |
Ajithkumar TV, Minimole AL, John MM, Ashokkumar OS. Primary fallopian tube carcinoma. Obstet Gynecol Surv. 2005 Apr;60(4):247–252. doi: 10.1097/01.ogx.0000158506.23663.79. PMID: 15795632. | |
Stewart CJ, Leung YC, Whitehouse A. Fallopian tube metastases of non-gynaecological origin: a series of 20 cases emphasizing patterns of involvement including intra-epithelial spread. Histopathology. 2012 May;60(6B):E106–E114. doi: 10.1111/j.1365-2559.2012.04194.x. Epub 2012 Mar 6. PMID: 22394169. | |
Na K, Kim HS. Clinicopathological characteristics of fallopian tube metastases from primary endometrial, cervical, and nongynecological malignancies: a single institutional experience. Virchows Arch. 2017 Sep;471(3):363–373. doi: 10.1007/s00428-017-2186-z. Epub 2017 Jul 13. PMID: 28702779. | |
Tessler FN, Perrella RR, Fleischer AC, Grant EG. Endovaginal sonographic diagnosis of dilated fallopian tubes. AJR Am J Roentgenol. 1989 Sep;153(3):523–525. doi: 10.2214/ajr.153.3.523. PMID: 2669465. | |
Fadıloğlu E, Dur R, Demirdağ E, Öztürk Ç, Fadıloğlu Ş, Kaplan M, Tapısız ÖL. Isolated tubal torsion: Successful preoperative diagnosis of five cases using ultrasound and management with laparoscopy. Turk J Obstet Gynecol. 2017 Sep;14(3):187–190. doi: 10.4274/tjod.57984. Epub 2017 Sep 30. PMID: 29085710; PMCID: PMC5651895. | |
Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021 Feb 27;397(10276):839–852. doi: 10.1016/S0140-6736(21)00389-5. PMID: 33640070. | |
Prodromidou A, Kathopoulis N, Zacharakis D, Grigoriadis T, Chatzipapas I, Protopapas A. Tubal Endometriosis: From Bench to Bedside, A Scoping Review. J Pers Med. 2022 Feb 26;12(3):362. doi: 10.3390/jpm12030362. PMID: 35330363; PMCID: PMC8955934. | |
Stepniewska AK, Clarizia R, De Mitri P, Pesci A, Zorzi C, Albanese M, Trivella G, Guerriero M, Improda FP, Ceccaroni M. Role of ultrasonographic parameters for predicting tubal involvement in infertile patients affected by endometriosis: A retrospective cohort study. J Gynecol Obstet Hum Reprod. 2021 Dec;50(10):102208. doi: 10.1016/j.jogoh.2021.102208. Epub 2021 Aug 18. PMID: 34418594. | |
Dooley WM, Chaggar P, De Braud LV, Bottomley C, Jauniaux E, Jurkovic D. Effect of morphological type of extrauterine ectopic pregnancy on accuracy of preoperative ultrasound diagnosis. Ultrasound Obstet Gynecol. 2019 Oct;54(4):538–544. doi: 10.1002/uog.20274. Epub 2019 Sep 6. PMID: 30937982. | |
Nadim B, Infante F, Lu C, Sathasivam N, Condous G. Morphological ultrasound types known as 'blob' and 'bagel' signs should be reclassified from suggesting probable to indicating definite tubal ectopic pregnancy. Ultrasound Obstet Gynecol. 2018 Apr;51(4):543–549. doi: 10.1002/uog.17435. Epub 2018 Mar 11. PMID: 28195383. | |
Rajah K, Goodhart V, Zamora KP, Amin T, Jauniaux E, Jurkovic D. How to measure size of tubal ectopic pregnancy on ultrasound. Ultrasound Obstet Gynecol. 2018 Jul;52(1):103–109. doi: 10.1002/uog.18958. PMID: 29143993. | |
ESHRE working group on Ectopic Pregnancy; Kirk E, Ankum P, Jakab A, Le Clef N, Ludwin A, Small R, Tellum T, Töyli M, Van den Bosch T, Jurkovic D. Terminology for describing normally sited and ectopic pregnancies on ultrasound: ESHRE recommendations for good practice. Hum Reprod Open. 2020 Dec 16;2020(4):hoaa055. doi: 10.1093/hropen/hoaa055. PMID: 33354626; PMCID: PMC7738750. | |
Sekar H, Divakova O, Alan T, Premetis G. Case of a chronic ectopic pregnancy misdiagnosed as pelvic inflammatory disease. BMJ Case Rep. 2021 Jan 11;14(1):e237053. doi: 10.1136/bcr-2020-237053. PMID: 33431533; PMCID: PMC7802671. | |
Drakopoulos P, Pluchino N, Yaron M, Dällenbach P. Chronic tubal ectopic pregnancy: a rare but challenging diagnosis. BMJ Case Rep. 2014 Jul 31;2014:bcr2014205715. doi: 10.1136/bcr-2014-205715. PMID: 25082870; PMCID: PMC4120042. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)