This chapter should be cited as follows:
Perinpanayagam J, Hartopp R, Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.413983
The Continuous Textbook of Women’s Medicine Series – Obstetrics Module
Volume 11
Labor and delivery
Volume Editor: Dr Edwin Chandraharan, Director Global Academy of Medical Education and Training, London, UK
Chapter
Labor Analgesia
First published: February 2021
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
The International Association for the Study of Pain (IASP)'s definition of pain is 'an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage'.1 The pain associated with labor has been described as one of the most intense forms of pain,2 but the experience of pain during labor is subjective and multifaceted. The complexity arises from many complex interactions including parity, physiological mechanisms, psychosocial factors, education, emotional support, cultural influences and ethnicity. As a result, every woman will have a unique experience during labor pain, thereby necessitating an individualized approach to pain management in labor.
Labor pain is a rare example of pain not being an indicator of potential tissue harm and this may have a bearing on how the pain is perceived by those experiencing it. The severity of pain experienced by women varies widely and labor pains can be alleviated by many factors including simple approaches such as providing continuous support by a caregiver, creating a relaxing setting3 and giving the woman more control during labor. Pain perceptions are influenced by factors such as previous experience, experience of family and friends, level of antenatal education and, ultimately, the expectation of the degree of pain that is acceptable to that individual.
Management of labor pain is not limited purely to clinical interventions due to the complexity of factors influencing pain perception and, therefore, a holistic approach should be followed taking into consideration the patient’s understanding, beliefs and choices. The main professionals with whom laboring women come into contact include midwives, obstetricians and anesthetists, and the woman’s overall experience and satisfaction with labor will be greatly influenced by her interaction with these caregivers and the support and communication they provide.
ANATOMY AND PHYSIOLOGY
The pain of labor is perceived by each woman in a unique manner owing to the complex interactions between physiological, psychological and social factors. Labor is divided into stages: the first stage occurs from the onset of regular painful contractions to full cervical dilatation; the second stage is the time period from full dilatation to expulsion of the fetus; and the third stage is the period from the delivery of the fetus to the expulsion of the placenta.
The pain experienced during labor is intermittent in nature with pain intensity reaching its peak with each uterine contraction and diminishing with relaxation of the uterus. The typical pattern of pain is progressive, with pain intensifying as contractions become more intense, frequent and prolonged, peaking towards the end of the first stage of labor.
The strongest, most frequent and most intense uterine contractions generally occur at the end of the first stage of labor as the cervix reaches full dilatation. The mother then has the urge to push or bear down, which assists the birth of the baby. The severity of the pain varies considerably from woman to woman, and is influenced by mental and emotional factors. For example, continuous support during labor can help women to cope with the pain and help with their overall satisfaction with the childbirth experience.3,4. This can be in the form of a relative, friend or healthcare professional and is thought to enhance the physiological process as well as some degree of empowerment over the woman’s ability to give birth.
Pain during the first stage of labor is transmitted by T10 to L1 spinal nerves due to cervical dilatation and uterine contractions. In the second stage T12 to L1 and S2 to S4 fibers transmit pain signals following stretching and distention of the pelvic floor. Labor pain has two main components: visceral pain which is transmitted by C-fibers during the early first and second stage, and somatic pain which is transmitted by A-delta fibers during the late first and second stage.5
There are a number of physiological changes that take place during pregnancy which impact on pharmacokinetic and pharmacodynamic properties of drugs and need to be considered when administering medication to pregnant women, these are outlined in Table 1.
1
Physiological changes in pregnancy affecting drug handling.
Physiological changes |
Delayed/decreased absorption of oral medication |
Increased sensitivity to inhalational agents (decreased minimum alveolar concentration (MAC)) |
Increased cutaneous blood flow resulting in increased efficacy of transdermal medications |
Altered drug distribution due to increased plasma volume |
Greater storage of lipid soluble drugs and, therefore, reduced free fraction |
Analgesia during labor is important not only for maternal reasons, but also for fetal wellbeing; pain and stress during labor result in increased circulating catecholamines, which cause uterine vasoconstriction and reduced blood flow to the placenta. Hyperventilation due to pain results in respiratory alkalosis and a left shift of the oxygen dissociation curve. Both of these processes consequently reduce oxygen transfer to the fetus and can result in metabolic acidosis thereby making labor analgesia vital for both mother and baby.5
ANALGESIA OPTIONS
There are many options available to laboring women to relieve labor pain depending on healthcare resources, location of childbirth and individual factors. Figure 1 below summarizes the classification of the various analgesic options.
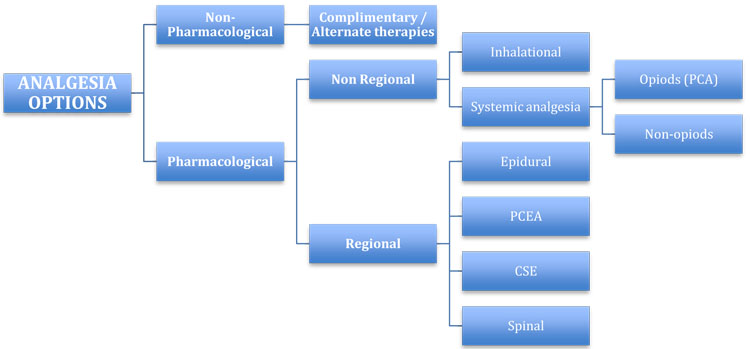
1
Classification of labor analgesia options.
Non–pharmacological analgesia
Non-pharmacological analgesia is available to women opting to have home births, births in midwifery-led units and labor wards, i.e. any setting in which expertise/resources for the specific technique is available. Many women wish to avoid pharmacological methods of pain relief during labor, which is influenced by a variety of cultural and geographical factors as well as individual reasons. Wherever possible and feasible these options should always be offered to women unless there is a specific indication not to do so.
Complementary and alternative medicine (CAM) techniques have become increasingly popular amongst individuals worldwide, especially amongst women of reproductive age6 and, although these practices are often classified as one category, there is a distinction between the two terms. Complementary therapies encompass non-mainstream practices used together with conventional medicine, whereas the use of non-mainstream practices instead of conventional practices is defined as alternative therapies.7
The CAM techniques available for labor analgesia can be classified into psychological, alternative and physical methods and these are summarized in Figure 2. The advantage of such techniques is that they can be taught to women through classes, online media and, subsequently, made widely accessible to a greater number of individuals. They are often (but not always) low cost, low fidelity and easy to implement, but it is important not to dismiss potential side effects and risks that may arise from improper application of some techniques.
Music is widely used in a variety of settings to alleviate stress and many maternity units in the UK provide facilities for women to listen to music during labor in low- and high-risk units. Studies have shown that music and music-assisted relaxation techniques significantly reduce arousal resulting from stress;8 however, the latest Cochrane review of relaxation techniques in labor found that, although music was associated with lower pain intensity in the latent phase, there is insufficient high-quality evidence regarding pain reduction in the active phase.4 The use of relaxation techniques during labor has been associated with reduced pain intensity, greater reporting of analgesia satisfaction but no advantages with respect tp the whole childbirth experience, whereas comparing yoga to control interventions found reduced pain intensity, and greater satisfaction with pain relief and the overall childbirth experience.4
Hypnosis is a state of consciousness with focused attention and reduced peripheral awareness in which there is apparent loss of voluntary action and heightened susceptibility to suggestion. Hypnosis has been used during labor to help women focus on calming influences and perceive contractions in a more positive way. High-quality evidence is still lacking for the role of hypnosis in labor pain management and, of the available trials, there are considerable variations in the techniques and timing of hypnosis, for example, practitioner-directed hypnosis vs self-directed. A Cochrane review of nine randomized controlled trials involving 2954 women found that hypnosis may reduce the use of pharmacological analgesia during labor, although this did not extend to epidural use. However, the review found no clear evidence that hypnosis improved satisfaction with pain relief or the ability to cope with labor pain compared to control groups.9

2
Classification of complementary/alternative therapies for labor analgesia.
Homeopathy is an unsupported approach to holistic medicine based on the principle that substances which cause symptoms can be diluted repetitively to a solution no longer containing the initial substance to treat the original symptom. The doses of the active substance in homeopathy are so minute as to avoid any side effects; however, there is no good-quality evidence that homeopathy is effective for any health condition including management of labor pain. Aromatherapy is based on the practice of using essential oils derived from plants to enhance physical and mental wellbeing through direct application to the skin, inhalation techniques or in a bath. The practice is based on the theory that the oils increase sedative and relaxing neurotransmitters; however, a systematic review of the evidence has shown no difference in pain intensity or the use of pharmacological pain relief during labor with aromatherapy.10
Water immersion is a particularly popular practice in midwife-led units and has a long history of being used in labor. It is postulated that increased release of oxytocin and endorphins occurs due to increased perfusion to the uterus during immersion in warm water which subsequently improves maternal satisfaction.11 A systematic review of 15 randomized controlled trials comparing immersion with no immersion found that there may be a reduced use of regional analgesia with water immersion during the first stage of labor, but there is insufficient evidence to show improved pain relief.12
Acupuncture involves the insertion of fine needles into the body at trigger points by trained experts with a view to restoring energy imbalances, whereas acupressure, although based on the same principles, uses the therapist’s hands to apply pressure. The method is thought to work by stimulation of the nervous system to modify pain perception either through transmission of signals to the spinal cord on needle insertion or stimulation of endorphin production.13 When analyzing data from 13 randomized controlled trials there was no difference in pain intensity when comparing acupuncture to placebo control or standard care (including varying uses of pharmacological and neuraxial techniques), but there was reduced pain intensity reporting when compared to no intervention; however, acupuncture did increase satisfaction with pain relief when compared to placebo.13
Transcutaneous electrical nerve stimulation (TENS) is a method of pain relief, which emits low voltage currents via pads applied to the skin on patient demand and has been available since the 1970s. During labor these pads are applied to the lower lumbar region and the patient controls when currents are emitted. Different theories have been proposed about how TENS provides analgesia, including Melzack’s gate control theory in which stimulation of afferent nerves by a low-voltage current inhibits painful stimuli being transmitted via the spinal cord. Another proposed mechanism is that TENS complements the release of endorphins, which subsequently modulate the pain experience.14 There is insufficient evidence to make a judgment on the effectiveness of the analgesic effect of TENS in labor;15 however, the low risks of this method mean that, when it is available, it should be offered as an option to laboring women.
A Cochrane review in 2006 found that acupuncture and hypnosis can relieve labor pain, but that more evidence is needed to support the use of massage, music therapy, acupressure and aromatherapy techniques.6 A recent Cochrane review analyzing data from over 15,000 women across 17 countries found that continuous support during labor decreased the use of analgesia including regional analgesia3 and the support of a designated midwife has also been shown to improve satisfaction reporting with childbirth.16
In summary, CAM techniques in labor can be implemented in low-risk settings, with minimal additional resources and are often inexpensive making them attractive to many laboring women. However, there is very minimal evidence available to support their effectiveness in reducing labor pain which often prevents them being offered in tertiary settings. Nevertheless, as discussed earlier, a woman’s experience of labor pain is so unique that despite the lack of evidence, the impact factor of a particular CAM technique for an individual should always be considered where possible.
Pharmacological analgesia
There are various pharmacological methods of analgesia available to laboring women; however, their use is dependent on many factors. The woman’s medical history, stage of labor and/or obstetric factors may contraindicate the use of some drugs, whereas the location of childbirth and expertise of staff will determine which methods are available to be administered safely. Obstetric units with 24-hour anesthetist cover can provide the greatest range of analgesic options; however, despite this, women cannot be guaranteed advanced techniques if there is excessive demand or staffing limitations.
Non-regional techniques
Inhalational
Inhalational analgesia has been used in labor since the early 18th century with the administration of ether to a woman with a deformed pelvis by James Young Simpson. The inhalational technique enables self administration of analgesia by the laboring woman and can be used on demand, continuously or intermittently and is simple to master following initial supervision to ensure correct procedure; therefore enabling widespread use of the method.
There have been many agents, especially in recent times which have been tried for labor analgesia including sevoflurane, isoflurane and enflurane, but Entonox (a 50 : 50 mixture of nitrous oxide and oxygen) remains the most widely used agent in obstetric practice. Nitrous oxide has a low blood : gas solubility coefficient which allows rapid onset (within 60 seconds) and short duration and can be used throughout all stages of labor owing to its negligible effects on maternal and fetal physiology.17 At low concentrations nitrous oxide acts as an analgesic and at high concentrations it has an anesthetic effect. The mechanism of analgesic action of nitrous oxide is dependent on the inhibition of supraspinal gamma-aminobutyric acid (GABA)-A receptors in addition to activation of the same receptors in the spinal cord.18 Evidence shows that, although Entonox is not a potent analgesic and side effects of nausea, vomiting, dizziness and drowsiness are common, it is effective in reducing pain intensity and the benefits to parturients are greater when inhalational techniques are properly adhered to.17 A systematic review by Jones et al. in 2012 supports inhalational analgesia as an effective method of analgesia in labor when compared to placebo.15
Systemic analgesia
Systemic analgesic options are available to parturients on low-risk midwifery led units as well as obstetric units and are the most widely used pharmacological agents for labor analgesia worldwide; since in many parts of the world regional analgesic options are not readily available to laboring women. Systemic analgesics include opioids and non-opioids (paracetamol, non-steroidal anti-inflammatory agents and antispasmodic agents).
Opioids
There has been a decreasing trend in parenteral opioid administration in labor in the UK from 33% in 200619 to 25% in 2014.20 In the UK, intramuscular pethidine is the most frequently administered opioid intramuscularly during labor as midwives are licensed to prescribe and administer it.21 Other opioids include dihydrocodeine, morphine, diamorphine, fentanyl and remifentanil. Opioids act on opioid receptors located throughout the central nervous system at a cellular level to reduce excitability of neuronal cells transmitting nociceptive impulses.22 All opioids cross the placenta to a significant degree and the effects can last for over 72 hours after delivery of the neonate; especially meperidine (pethidine) which, together with its metabolite normeperidine, has a prolonged half-life.23 Parenteral opioids have many side effects for both the mother and the fetus; maternal drowsiness, nausea and vomiting, urinary retention and hypoventilation are common maternal side effects. In the fetus opioids can depress breathing and reduce fetal heart rate, variability and accelerations, and can last into the neonatal period causing poor feeding, hypothermia and reduced alertness.15 It is important that fetal monitoring is instigated when opioids have been administered for analgesia in labor and pediatricians informed of any parenteral opioids so they can make accurate assessments of the neonate after delivery.
A large systematic review by Smith et al. in 2018 looked at over 8000 healthy women with low-risk pregnancies between 37 and 42 weeks' gestation and concluded that opioids provided some pain relief in labor and women reporting moderate satisfaction with analgesia, but there were insufficient data to compare different opioids; the review did not find any evidence of neonatal adverse effects.4
Patient-controlled analgesia (PCA) techniques are associated with increased satisfaction of the analgesic effect in itself and this is thought to be due to parturients having a degree of control over their pain management.24 In the labor setting, pethidine, fentanyl and remifentanil have all been used to administer analgesia through this technique. A growing body of evidence has emerged supporting the use of remifentanil for labor analgesia and over a third of obstetric units in the UK now offer remifentanil PCA25 to laboring women. Remifentanil is a synthetic, ultrafast-acting opioid, which has a rapid onset of action and a short half-life of 3 minutes owing to rapid metabolism by plasma esterases to an inactive metabolite. Although remifentanil readily crosses the placenta, it is metabolized extensively by the fetus, this combined with the pharmacokinetic profile of the drug, making it ideal for use in a PCA pump.
Women are more satisfied with analgesia provided by remifentanil compared to other parenteral opioids26 and remifentanil PCA analgesia provides stronger pain relief during early labor.27 The side-effect profile of remifentanil PCA is greater than that of regional techniques and the safety concerns surrounding use of the former remains an issue that needs to be addressed before widespread use of the technique can be implemented. Many units utilize this technique for patients in whom regional techniques are contraindicated or as a bridge to regional anesthesia, where a significant delay is anticipated prior to instigation of regional analgesia.
Non-opioids drugs
Non-opioid drugs which have been used in the management of pain include paracetamol, non-steroidal anti-inflammatory agents (NSAIDS), antispasmodics, sedatives and antihistamines. In some countries these drugs are still offered during early labor, although their use in the UK during labor is not very common. NSAIDs should be avoided to prevent premature closure of the fetal ductus arteriosus and pulmonary hypertension, and paracetamol is the only non-opioid which is commonly offered in labor (although often in combination with a weak opioid such as co-dydramol). The findings of the review conducted by Othman et al. concluded that there is insufficient evidence to support the sole use of non-opioid drugs in labor pains.28
Regional anesthetic techniques
Regional analgesia techniques in the form of central neuraxial blocks are considered the gold standard method of pain relief in obstetrics in the UK. The primary technique is epidural analgesia with variations of the technique and drugs used providing greater versatility and benefits to laboring women at different stages of labor and in the perinatal period. There are some general considerations that apply to all forms of central neuraxial blockade in labor which will be considered first before discussing the specifics of the different techniques.
In addition, provision of analgesia epidurals and variations of the technique can be beneficial in labor for many other reasons. In patients with high BMI, they can be sited early to facilitate urgent operative interventions, this also reduces the need for airway intervention in a high-risk group should an emergency intervention requiring general anesthesia be needed. Epidurals can help blood pressure control in the management of pre-eclampsia and in patients with significant cardiovascular, respiratory and neurological disease. There has been an increase in the number of women with complex cardiac conditions including those with cardiovascular implantable electronic devices (CIEDS) reaching reproductive age and giving birth,29 and the role of an early epidural with ECG monitoring has enabled a greater proportion to be able to deliver vaginally. Similarly, there is an increasing trend to allow women with complex neurological diagnoses, such as arteriovenous malformation (AVM), to deliver vaginally and this is made possible with siting of epidurals early and close monitoring. Other situations which can benefit from epidurals include multiple births, anticipated instrumental delivery, vaginal birth after cesarean section, vaginal breech delivery and urge to push on a non-fully dilated cervix.
There are contraindications to neuraxial block as with any intervention and these can be classified into absolute and relative, as shown in Table 2.
2
Contraindications to neuraxial blockade.
CONTRAINDICATIONS | |
Absolute | Relative |
Patient refusal | Uncooperative patient/inability to communicate |
Local anesthetic allergy | Sepsis |
Lack of sterile equipment | Neurological conditions |
Infection at site of injection | Fixed cardiac output |
Coagulopathy | Anatomical abnormalities of spine |
Severe hypovolemia/uncontrolled hemorrhage | Raised intracranial pressure |
Part of the process of providing epidural analgesia involves informed discussion with the woman about the procedure and the benefits and complications (Table 3). Many women would have received information in the antenatal period; however, it is the duty of the anesthetist to ensure they have discussed and provided all the relevant information regarding regional analgesic techniques to the woman prior to performing the procedure. In most UK centers a standard epidural information card (often available in many languages) created by the Obstetric Anaesthetists' Association (OAA) is available and may be used to supplement the consent process.
3
Complications of neuraxial blockade.
COMPLICATIONS | |
Early | Late |
Local anesthetic toxicity | Postdural puncture headache (1 : 100) |
Failure (1 : 8) | Epidural abscess (1 : 50,000) |
Hypotension (1 : 50) | Epidural hematoma (1 : 170,000) |
High block/total spinal (1 : 100,000) | Temporary neurological injury (1 : 1,000) |
Fetal bradycardia | Permanent neurological injury (1 : 13,000) |
Urinary retention | Severe nerve injury/paralysis (1 : 250,000) |
Once the indications, contraindications and specific patient factors have been considered intravenous access must be secured prior to siting an epidural. In low-risk pregnancies it is not necessary to repeat blood tests; however, in patients with risk of or known pre-eclampsia a full blood count within 6 hours must be available. If the platelet count is less than 100 × 109/L or rapidly dropping, then a coagulation screen must also be completed. All central neuraxial techniques should be performed in a sterile manner and monitoring of fetal heart rate should be commenced at the start of the procedure and continued for a minimum of 30 min. Maternal blood pressure and heart rate should be monitored every 5 minutes for 15 minutes after each intermittent epidural top up and the level of sensory block should be assessed every hour. If a patient controlled epidural technique is being used, the blood pressure and heart rate should be monitored every 5 minutes for 20 minutes and the sensory block assessed every 30 minutes, and with continuous infusions the woman must be assessed every 30 minutes for heart rate, blood pressure, sensory block level, motor power and side effects. After establishment of analgesia, a urinary catheter should be inserted to prevent retention and subsequent bladder damage.
Regional analgesia and anesthesia in labor necessitates the presence of an anesthetist and so availability of these options as a method of pain relief may be limited in under-resourced settings.
Epidural
Epidural analgesia in labor involves insertion of a lumbar epidural catheter by an anesthetist and subsequent injection of an epidural mix to provide pain relief. The mix typically is a combination of local anesthetic and opiate, although there are many variations, which are in use depending on the center, the patient and stage of labor. The local anesthetic is the primary component of the mix and acts reversibly on nerve cells, blocking sodium channels, which results in the inhibition of nerve impulses. Levobupivacaine is most commonly used as the local anesthetic (0.0625–0.1%) with fentanyl (2 μg/ml) during labor, although newer combinations involving ropivacaine, remifentanil and adjuvants such as clonidine are starting to appear.30 The choice of epidural mix depends on the purpose of the top up, for example a top up for instrumental delivery in theater may require a much stronger dose of local anesthetic than that for labor alone. Epidurals in labor are typically sited at L3/L4 or L2/L3, as the spinal cord ends at L1/L2 in adults. The resulting effect is motor and sensory loss below this level providing the needed analgesia for labor. Opioids provide a synergistic effect to local anesthetic solutions and reduce the overall local anesthetic requirement.
Epidurals are effective at reducing labor pain and have no significant impact on the risk of cesarean section, neonatal status and development of back pain.31 Hypotension, pruritus, nausea and failure are common side effects of epidural analgesia, with less common but significant complications including headache, hematoma and nerve injury. The Third National Audit Project conducted in the UK provided high level evidence of the safety of epidural analgesia in labor showing that permanent injury occurred in 1 in 24,000 to 1 in 54,000 and only 20% of the cases were attributable to epidurals sited in labor..32
Effective labor analgesia can prolong the second stage of labor and meta-analyses of randomized control trials show an approximate increase of 15 min in the second stage when comparing regional neuraxial to systemic analgesia.33,34 There is evidence showing an association with increased instrumental delivery in women with epidural analgesia;35 however, this may reflect the increased likelihood of instrumental deliveries being attempted in women who have adequate analgesia as a result of an effective epidural.36 The advent of 'the mobile epidural mix' which is a much more diluted concentration of local anesthetic (typically 0.1% levobupivacaine) has reduced the rate of adverse effects and also improves maternal satisfaction.
Dural puncture epidural is the practice of performing an intentional dural puncture with a spinal needle but no subsequent injection of drugs into the intrathecal space. It is not common practice but the technique is thought to provide better analgesia compared to epidural alone without the more pronounced cardiovascular effects of spinal anesthesia.37
Patient-controlled epidural analgesia
The use of programmed epidural pumps offers an alternative to intermittent midwifery top ups in the form of patient-controlled epidural analgesia (PCEA) or continuous epidural infusion (CEI) with or without PCEA. The benefits and disadvantages of each method are summarized in Table 4.
4
Comparison of the different methods of epidural drug administration.
Advantages | Disadvantages | |
Intermittent bolus | Safe and simple to use No need for specialized equipment | Delays in top up can occur |
Patient controlled epidural analgesia | Local anesthetic dose matches requirement of patient Degree of control held by parturient Lower incidence of motor block | Need for expensive equipment Parturient needs to understand how to use technique effectively |
Continuous epidural infusion | Provides hemodynamic stability | Need for expensive equipment Total dose of local anesthetic much higher compared to other methods |
The method by which epidural analgesia is maintained affects the total dose of local anesthetic administered and, subsequently, the degree of motor block; continuous infusions result in a greater total dose and more dense block compared to intermittent boluses.38 PCEA is a safe and reliable technique in which women have more autonomy over their labor analgesia. The technique permits a lower total dose requirement compared to continuous infusion and subsequently improves mobility during labor which is an added advantage for most women.
Combined spinal and epidural
The combined spinal-epidural (CSE) technique involves an initial injection into the intrathecal space followed by the placement of an epidural catheter through which additional doses (top-ups) can be administered as needed. This method offers the advantage of a more rapid onset of analgesia compared to epidural alone, which can take an average of 20 minutes to take full effect. This is particularly of use in parturients who are experiencing frequent contractions with minimal relief in between, as it offers a period of reprieve to site the epidural which can be more technically challenging. The CSE can be performed as two separate injections or as a needle through needle technique depending on the equipment available and experience of the anesthetist in performing the latter technique. There is no evidence supporting increased maternal satisfaction, ability to mobilize or maternal and neonatal outcome with CSE compared to epidural analgesia alone.5 The added risks of CSE (increased incidence of postdural puncture headache (PDPH), pruritis, meningitis and catheter migration) mean that the technique should be reserved for cases in which the benefits outweigh the risks.39
Single-shot spinal
Single-shot spinal (SSS) anesthesia is not commonly used for labor analgesia, as its limited duration makes it less suitable for the unpredictable length of labor; it is more commonly used for cesarean sections and other operative interventions..
Spinal catheter techniques are not common practice in the UK, although there is scope for intrathecal catheters following inadvertent dural puncture. Strict guidelines must be adhered to in such circumstances with highly vigilant monitoring and visible labels attached to the intrathecal catheter, and top ups only being administered by anesthetists due to the significant adverse effects of overdose.
Some centers internationally offer continuous spinal analgesia (CSA) with the use of specially designed microcatheters suitable to remain in the intrathecal space; however, the risks of PDPH and cauda equina syndrome are significant and limit its routine use in this setting.40 The benefits of CSA in patients with prior spinal surgery, morbid obesity or severe cardiac disease may outweigh the risks and justify the use of CSA in patients with special circumstances; however, further development of equipment and more research is needed before this technique becomes readily available to laboring women.
SPECIAL CONSIDERATIONS
In the UK the provision of labor analgesia is somewhat standardized according to national guidance issued by the Royal College of Obstetricians and Gynaecologists, the Royal College of Anaesthetists and the Association of Anaesthetists of Great Britain and Ireland; however, each obstetric unit will have developed its own specific guidelines and policies based on the level of care it provides, patient population and resources available. Anesthetists and obstetricians work together with midwives and allied healthcare professionals to provide the high level of care expected in a developed country and it is important that each specialty appreciates and understands the implication of specialty specific conditions on the options available for pain management.
The presence of comorbidities can present numerous challenges to anesthetists when considering provision of labor analgesia as well as the technique for operative intervention. The Confidential Reports into Maternal Morbidity and Mortality have shown a significant impact on anesthetic interventions in reducing these rates.41
There is a continuing increase in the number of obese parturients in the western world and, in the UK, Australia and USA, up to a quarter of women are overweight or obese when they become pregnant.42 Obesity is associated with a wide range of complications in the perinatal period including development of diabetes, pre-eclampsia, hypertension, thromboembolism, higher rates of cesarean section and higher rates of airway complications with general anesthesia. Early epidurals are often advocated with CSEs providing some advantage in this group of patients; however, it is prudent to check whether women have been commenced thromboprophylactic treatment to reduce the risk of developing venous thromboembolism and give appropriate guidance to the timing of neuraxial blocks. Current guidelines recommend a minimum interval of 12 hours between a prophylactic dose of dalteparin and the placement of neuraxial blocks, and 24 hours for patients on therapeutic doses, and variation in these intervals with the use of newer anticoagulants.43 The use of ultrasound to assist neuraxial analgesic techniques has increased in recent years, and this patient group may particularly benefit from such guidance.
Many more women with complex cardiac disease (in developed countries) are becoming pregnant compared to in the past due to advances in treatment improving survival to reproductive age and clinicians taking a more patient-centered approach to advice regarding avoiding pregnancy in cardiovascular disease. These women need to be assessed in a multidisciplinary setting and the specific condition understood, as a drop in vascular resistance due to epidural analgesia can cause catastrophic consequences in certain conditions but be beneficial in others. CSEs allow a small dose of intrathecal opioid to be added and gradual introduction of a low-dose local anesthetic mixture to be introduced to enable a block to be established slowly with careful cardiovascular monitoring.44,45 Epidurals reduce the stress response to pain and help avoid tachycardia, which can exacerbate existing cardiac conditions. The added benefit of epidurals in early labor is the avoidance of a potentially high-risk general anesthetic for emergency cesarean section.
Asthma is one of the most common respiratory conditions. Epidural anesthesia is often recommended during labor for women with asthma, as it reduces oxygen consumption and minute ventilation, lowers the risk of chest infection and atelectasis, and can be extended for emergency surgery, potentially avoiding the complications associated with invasive ventilation under general anesthesia.
The approach to managing women with neurological disease has changed in recent years with an increasing trend towards vaginal delivery and the successful use of regional anesthetic techniques.44 It is important to assess women prior to placement of neuraxial blocks, specifically where a neurological deficit exists and counsel women accordingly about further neurological injury, and to also consider any associated complications such as tethered spinal cord in a patient with spina bifida. These women need to be seen antenatally so that relevant investigations such as MRI of the spine can be conducted in time to offer them the best options for labor analgesia. Where regional techniques must be avoided, the use of remifentanil PCA can offer a suitable alternative.
Diabetes in pregnancy is very common and the control of plasma glucose in the perinatal period can be challenging due to the stress responses faced in all stages of labor. Epidural analgesia helps obtund the stress responses of labor; however, autonomic neuropathy in some patients can make them more prone to hemodynamic instability.45
Table 5 summarizes the specific anesthetic considerations that need to be taken into account, when choosing the most appropriate options regarding labor analgesia for these comorbidities, as well as some other significant medical conditions.
5
Comparison of the different methods of epidural drug administration.
Condition/problem | Consideration | |
High BMI | High BMI | Is patient on thromboprophylaxis? When to stop thromboprophylaxis |
Cardiovascular disease | Cardiac (e.g. cardiomyopathy, valvular lesion, arrhythmia, congenital) | Endocarditis prophylaxis in valve disease Combined spinal-epidurals are preferred to enable slow incremental development of anesthesia Early epidural Left lateral position for siting neuraxial blocks Diluted syntocinon administered slowly and not as a bolus |
Respiratory disease | Respiratory (pulmonary embolism, pulmonary hypertension) | Is patient on thromboprophylaxis? When to stop thromboprophylaxis (is bridging therapy needed) |
Hematological condition | Gestational thrombocytopenia Immune thrombocytopenic purpura Pre-eclamptic toxemia | Trend in platelet count just as important as absolute value Appropriate timing of central neuraxial block after thromboprophylaxis Checking full blood count and clotting within 6 hours of central neuraxial block in severe cases |
Sickle cell | Check clotting Thromboprophylaxis timing | |
Diabetes | Type 1/2 Gestational | Epidurals reduce stress and can help control plasma glucose level |
Musculoskeletal | Scoliosis | Use of ultrasound |
Mental health | Depression Bipolar | Capacity to consent |
Neurological | Epilepsy Arteriovenous malformation Multiple sclerosis Myasthenia gravis (MG) Raised increased intracranial pressure (ICP) | Assessment of impact of disease on pregnancy Optimal seizure control in those with epilepsy Identification of associated complications in those with congenital abnormality Review of relevant investigations Patient-controlled analgesia in those with contraindications for central neuraxial block (raised ICP) Rheumatoid arthritis in patients with MG |
Many obstetric units will see women with complicated pregnancies in a high-risk clinic setting with multidisciplinary input from the relevant specialties. This should be done early, so that appropriate management plans can be developed, relevant investigations conducted and referrals made if necessary to tertiary or quaternary centers where treatment options not available at the booking hospital can be offered.
VARIATIONS IN GLOBAL PRACTICE
Maternal mortality rates are disproportionally higher in low- and middle-income countries (LMIC) compared to high-income countries (HIC). In northern Europe the risk of maternal death during pregnancy is 1 in 30,000, whereas in the poorest parts of the world it is as high as 1 in 6.46 In the majority of these LMIC, major hemorrhage is the main medical cause of death, although local variations exist.
There are many barriers to the delivery of safe obstetric care in LMIC and the focus of care in these settings is primarily safety, which requires skilful management of limited resources and skills and great flexibility on the part of clinical practitioners. LMIC unfortunately face ongoing challenges with supplies of equipment, especially disposable equipment, drugs, blood, staffing levels, training expertise as well as unpredictable political and environmental events which can further impact on the under-resourced setting. Training of anesthetists in LMIC can be limited and not only in relation to performing epidurals, but also with regards to administering intravenous opiates and managing potential complications.
The challenges are not limited to the healthcare setting and begin at home; this can be best explained using the 'three delays' framework.47 This model identifies three key points at which women in LMIC are delayed with regards to obtaining appropriate obstetric care. The first point is the delay in seeking medical health due to poor education/literacy levels, gender inequality, financial burden or prior unfavorable experiences. The second point is the delay in accessing an appropriate facility due to a large number of the population living in remote sites with poor transportation links, and the final point relates to delays once the facility is reached (the barriers discussed earlier).
International human rights law states that all countries are obligated to provide pain treatment as part of an individuals’ right to health (WHO)48 and laboring women should be no exception to this right. Pain during labor may not be life threatening; however, the consequences such as postnatal depression, post-traumatic stress disorder and fetal acidosis are well-recognized complications and need to be avoided. It is perceivable, however, that in LMIC where significant barriers exist to providing the basic healthcare to ensure safe delivery and maternal wellbeing, management of labor pain will not be considered a priority for many clinicians and even patients. For those mothers who attend healthcare settings their priority will be to have access to clinicians to provide safe delivery and resuscitation and this is in part due to the sad fact that many women in LMIC may not be aware that pain relief in labor is even an option. In most LMIC the process of establishing policies and practices for providing gold standard labor analgesia, as in HIC (i.e. an epidural service), is often not possible for all the aforementioned reasons.49
Options in under-resourced countries
In under-resourced countries where anesthesia providers exist and resources permit, there are options for pain relief in labor, but these differ significantly from those available in HIC and this should be recognized by clinicians when evaluating services and pain management in LMIC.
Continuous support by a relative or friend may reduce pain, anxiety and complications,16 which is recognized as an important aspect of managing labor pain in HIC, can be practiced in LMIC with limited resources. The other non-pharmacological methods discussed earlier in the chapter are also feasible where training and expertise permits; for example relaxation therapy, massage and water immersion may be low-fidelity options that can be offered. The availability of nitrous oxide is again variable in LMIC and alternatives such as fixed concentration of inhalational anesthetic agents, such as sevoflurane and isoflurane, are limited due to lack of equipment to provide these forms of analgesia in a safe manner.50
The use of parenteral opioids is a common option in LMIC, with pethidine being the most frequently used opioid for labor analgesia.51 Novel opioids such as tramadol and pentazocine offer similar levels of analgesia in the first stage of labor with the latter offering analgesic effects for a longer duration (up to 4 hours). Although the level of parenteral analgesia is far inferior to epidural analgesia, the option may be offered to women in resource-poor settings.52
Low-dose single-shot spinal technique is a safe method of analgesia during the second stage of labor. A recent study in Ghana looked at the effect of spinal anesthesia with 2.5 mg bupivacaine, 25 μg fentanyl and 0.2 mg morphine in 332 parturients. The results showed 98.8% reported mild or no pain, 87.7% had no limitation with ambulation and only 3.6% experienced fetal bradycardia.53 There was significant pruritus and nausea associated with the spinal technique which was attributed to morphine; however, there were no episodes of hypotension requiring vasopressor support which favors the safety profile of this technique. Although there are some obvious clinical advantages highlighted, more robust clinical trials are needed before this technique can be widely advocated.
There is a risk that practices from HIC may be taken to LMIC in an isolated manner without adequate planning and forethought by certain groups wishing to improve the provision of labor analgesia. While such initiatives may lead to temporary improvements, there is a potential for long-term harm due to lack of ongoing support/training and supervision and absence of standardized protocols for what would be novel practices in these settings. It is the responsibility of clinicians to first do no harm and each setting in LMIC must evaluate its own resources and skills to develop the best technique to improve the provision of labor analgesia for their laboring mothers. The developed world also has a duty of care to ensure that meaningful progress is made towards reducing the gap between standards of global healthcare provision especially for maternal health. The World Health Organization has produced a document, which outlines the basic structure, supply of equipment and human resource needs for facilities.54 However, there is much yet to be done to reduce the existing inequalities in care of the laboring women in LMIC compared to HIC.
PRACTICE RECOMMENDATIONS
- Labor analgesia should not be limited to clinical interventions and all practitioners involved in the care of laboring women should adopt a holistic approach to pain management.
- Ongoing consideration should be given to women’s emotional and psychological needs in addition to the need for analgesia.
- Care providers should support women with their choice.
- A patient-centered approach should be taken to every woman requesting analgesia to ensure special considerations are taken about choice of analgesia based on patient factors, obstetric factors and resource/skill availability.
- Antenatal education regarding all types of labor analgesia should be evidence-based and include the options available, benefits and risks of each technique. These should be made available in the antenatal period.
- A list of service providers in their region and which options they offer should be readily available to women prior to labor.
- Where the resources and expertise to provide complementary and alternative techniques of labor analgesia permit, these methods should be offered to women who request them (with the exception of acupuncture, acupressure and hypnosis).39
- Relaxation techniques, including progressive muscle relaxation, breathing, music, mindfulness and other techniques, are recommended for healthy pregnant women requesting pain relief during labor, depending on women’s preferences.
- Systemic opioid analgesia is recommended for healthy women, but is associated with adverse effects for mother and fetus so attention should be paid to monitor respiratory status.
- Regional analgesia is the gold standard for pain relief and women should not be denied it unless there is a clinical indication.
- On a delivery unit with a dedicated anesthetist, the time from a woman requesting regional analgesia to the anesthetist attending should not exceed 30 minutes except in exceptional circumstances.
- When regional analgesia is being established, continuous cardiotocography should be performed for 30 minutes and again after administration of further boluses of low-dose epidural mix.
- There should be a dedicated consultant anesthetist responsible at all times for the care of women on delivery suite.
- Provision of skills for advanced methods of labor analgesia should be supported by appropriate education and training for the relevant professionals.
- In under-resourced settings with a lack of access to equipment, skills and appropriate settings to monitor patients safely, care must be taken to balance the risks/benefits of each labor analgesia option to ensure safety first for mother and baby.
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
International association for the study of pain (IASP). IASP Terminology 2016 [Online] Available from: https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698#Pain [Accessed 16.02.18]. | |
Melzack R. The Myth of Painless Childbirth (the John J. Bonica lecture) 1984;19(4):321–337. Available from: DOI: 10.1016/0304-3959(84)90079-4. | |
Bohren MA, Hofmeyr GJ, Sakala C, et al. Continuous support for women during childbirth. Cochrane Database of Systematic Reviews 2017. Available from: DOI: 10.1002/14651858.CD003766.pub6. | |
Smith LA, Burns E, Cuthbert A. Parenteral opioids for maternal pain management in labour. Cochrane Database of Systematic Reviews 2018. Available from: DOI: 10.1002/14651858.CD007396.pub3. | |
Labor S, Maguire S. The Pain of Labour. Reviews in Pain 2008;2(2):15–19. Available from DOI: 1177/204946370800200205. | |
Smith CA, Collins CT, Cyna AM, et al. Complementary and alternative therapies for pain management in labour. Cochrane Database of Systematic Reviews 2006. Available from DOI: 1002/14651858.CD003521.pub2. | |
The National Health Service (NHS). Complementary and Alternative Medicine 2016 [Online]. Available from: https://www.nhs.uk/conditions/complementary-and-alternative-medicine/ [Accessed 24.03.2018]. | |
Pelletier CL. The effect of music on decreasing arousal due to stress: a meta-analysis. Journal of Music Therapy 2004;41:192–214. | |
Madden K, Middleton P, Cyna AM, et al. Hypnosis for pain management during labour and childbirth. Cochrane Database of Systematic Reviews 2016. Available from DOI: 10.1002/14651858.CD009356.pub3. | |
Smith CA, Collins CT, Crowther CA. Aromatherapy for pain management in labour. Cochrane Database of Systematic Reviews 2011. Available from DOI: 10.1002/14651858.CD009215. | |
Alleemudder DM, Kuponiyi Y, Kuponiyi C, et al. Analgesia for labour: an evidence-based insight for the obstetrician. The Obstetrician and Gynaecologist 2015;17:147–155. Available from DOI: 1111/tog.12196. | |
Cluett ER, Burns E, Cuthbert A. Immersion in water during labour and birth. Cochrane Database of Systematic Reviews. 2012 Available from DOI: 10.1002/14651858.CD000111.pub. | |
Smith CA, Collins CT, Crowther CA, et al. Acupuncture or acupressure for pain management in labour. Cochrane Database of Systematic Reviews 2020. Available from DOI: 10.1002/14651858.CD009232. | |
Dowswell T, Bedwell C, Lavender T, et al. Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database of Systematic Reviews 2009. Available from DOI: 10.1002/14651858.CD007214.pub2. | |
Jones L, Othman M, Dowswell T, et al. Pain management for women in labour: an overview of systematic reviews. Cochrane Database of Systematic Reviews 2012. Available from: DOI: 10.1002/14651858.CD009234.pub2. | |
Hodnett ED, Gates S, Hofmeyr GJ, et al. Continuous support for women during childbirth. Cochrane Database of Systematic Reviews 2017. Available from DOI: 10.1002/14651858.CD003766.pub6. | |
Klomp T, van Poppel M, Jones L, et al. Inhaled analgesia for pain management in labour. Cochrane Database of Systematic Reviews 2012. Available from DOI: 10.1002/14651858.CD009351.pub2. | |
Sanders RD, Weimann J, Maze M. Biologic effects of nitrous oxide: a mechanistic and toxicologic review. Anesthesiology 2008;109:707–22. Available from DOI: 1097/ALN.0b013e3181870a17. | |
Redshaw M, Rowe R, Hockley C, et al. Recorded Delivery: a National Survey of Women’s Experience of Maternity Care 2006. The National Perinatal Epidemiology Unit, 2007. | |
Redshaw M, Henderson J. Safely Delivered: a National Survey of Women's Experience of Maternity Care 2014. The National Perinatal Epidemiology Unit, 2015. | |
Bricker L, Lavender T. Parenteral opioids for labour pain relief: a systematic review. American Journal of Obstetrics and Gynecology 2002;186(5):94–109. | |
Trivedi M, Shaikh S, Gwinnutt C. Pharmacology of Opioids 2007 [Online] Available from: http://www.frca.co.uk/article.aspx?articleid=100933 [Accessed 22.02.18]. | |
Griffiths SK, Campbell JP. Placental structure, function and drug transfer. Continuing Education in Anaesthesia Critical Care & Pain 2015;15(2):84–89. Available from DOI: 10.1093/bjaceaccp/mku013. | |
Fortescue C, Wee MYK. Analgesia in Labour. Continuing Education in Anaesthesia Critical Care & Pain 2005;5(1):9–13. Available from DOI: 1093/bjaceaccp/mki002. | |
Howie KM, Millar S. Usage of remifentanil patient controlled analgesia in labour in the UK. International Journal of Obstetric Anesthesia 2011;20:36. | |
Schnabel A, Hahn N, Broscheit J, et al. Remifentanil for labour analgesia: a meta-analysis of randomised controlled trials. European Journal of Anaesthesiology 2012;29:177–185. Available from DOI: 1097/EJA.0b013e32834fc260. | |
Weibel S, Jelting Y, Afshari A, et al. Patient-controlled analgesia with remifentanil versus alternative parenteral methods for pain management in labour. Cochrane Database of Systematic Reviews 2017. Available from DOI: 10.1002/14651858.CD011989.pub2. | |
Othman M, Jones L, Neilson JP. Non-opioid drugs for pain management in labour. Cochrane Database of Systematic Reviews 2012. Available from DOI: 10.1002/14651858.CD009223.pub2. | |
Boulé S, Ovart L, Marquié C, et al. Pregnancy in women with an implantable cardioverter-defibrillator: is it safe? EP Europace 2014;16(11):1587–1594. Available from DOI: 1093/europace/euu036. | |
Rucklidge A. Analgesia for Labour 2006 [Online] Available from: http://www.frca.co.uk/article.aspx?articleid=100551 [Accessed 16.05.2018]. | |
Anim-Somuah M, Smyth RM, Jones L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database of Systematic Reviews 2011. Available at DOI: 10.1002/14651858.CD000331.pub3. | |
Cook T, Counsell D, Wildsmith J. Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. British Journal of Anaesthesia 2009;102:179–190. Available from DOI:1093/bja/aen360. | |
Halpern SH, Leighton BL. Epidural analgesia and the progress of labor. In: Halpern SH, Douglas MJ (eds.) Evidence-based Obstetric Anesthesia. Oxford, UK: Blackwell, 2005;10–22. | |
Sharma SK, McIntire DD, Wiley J, Leveno KJ. Labor analgesia and cesarean delivery: an individual patient meta-analysis of nulliparous women. Anesthesiology. 2004 Jan;100(1):142-8; discussion 6A. doi: 10.1097/00000542-200401000-00023. PMID: 14695735. | |
Anim-Somuah M, Smyth RMD, Cyna AM, et al. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database of Systematic Reviews 2018. Available from DOI: 10.1002/14651858.CD000331.pub4. | |
Bodner-Adler B, Bodner K, Kimberger O, et al. The effect of epidural analgesia on obstetric lacerations and neonatal outcome during spontaneous vaginal delivery. Archives of Gynecology and Obstetrics 2003;267:130–3. | |
Cappiello E, O'Rourke N, Segal S, et al. A randomized trial of dural puncture epidural technique compared with the standard epidural technique for labor analgesia. Anesthesia and Analgesia 2008;107(5):1646–1651. Available from DOI: 10.1213/ane.0b013e318184ec14. | |
Cambic CR, Wong A. Labour analgesia and obstetric outcomes. British Journal of Anaesthesia 105(1):50–60. Available from DOI: 1093/bja/aeq311. | |
National Institute for Health and Care Excellence (NICE). Intrapartum Care: Care of Healthy Women and Their Babies During Childbirth 2014 [Online] Available from: https://www.nice.org.uk/guidance/cg190 [Accessed 25.03.2018]. | |
Veličković I, Pujic B, Baysinger CW, et al. Continuous Spinal Anesthesia for Obstetric Anesthesia and Analgesia. Frontiers in Medicine 2017;4:133. Available from DOI: 3389/fmed.2017.00133. | |
Marchi J, Berg M, Dencker A, et al. Risks associated with obesity in pregnancy, for the mother and baby: a systematic review of reviews. Obesity Reviews 2015;16:621–638. Available from DOI: 1111/obr.12288. | |
Working Party: Association of Anaesthetists of Great Britain & Ireland, Obstetric Anaesthetists' Association, Regional Anaesthesia UK. Regional anaesthesia and patients with abnormalities of coagulation: The association of anaesthetists of Great Britain & Ireland the obstetric anaesthetists' association regional anaesthesia UK. Anaesthesia 2013;68:966 9–72. Available from DOI: 1111/anae.12359. Epub 2013 Aug 1. | |
Francis S, May A. Pregnant women with significant medical conditions: anaesthetic implications. Continuing Education in Anaesthesia, Critical Care and Pain 2004;4(3):95–97. Available from DOI: 1093/bjaceaccp/mkh026. | |
Bajwa SJS, Bajwa SK, Ghuman GS. Pregnancy with co-morbidities: Anesthetic aspects during operative intervention. Anesthesia, Essays and Researches 2013;7(3):294–301. Available from DOI: 4103/0259-1162.123207. | |
Ronsmans C, Graham WJ. Maternal mortality: who, when, where, and why. Lancet 2006;368(9542):1189–1200. Available from DOI: 1016/S0140-6736(06)69380-X. | |
Pelland A, George RD. Safe obstetric anaesthesia in low- and middle-income countries. BJA Education 2017;17(6):194–197. Available from DOI: 10.1093/bjaed/mkw073. | |
Lohman D, Schleifer R, Amon JJ. Access to pain treatment as a human right. BMC Med 8, 8 (2010). https://doi.org/10.1186/1741-7015-8-8. | |
Schnittger T. Regional anaesthesia in developing countries. Anaesthesia 2007;62(1):44–47. Available from DOI: 1111/j.1365-2044.2007.05297.x. | |
Dobson M. Opinion: Labour Analgesia in the Developing World; Why Not. Reviews in Pain 2011;5(3):2–3. Available from DOI: 10.1177/204946371100500302. | |
Bricker L, Lavender T. Parenteral opioids for labor pain relief: a systematic review. American Journal of Obstetrics and Gynecology 2002;186(5):94–109. Available from: https://www.ncbi.nlm.nih.gov/books/NBK69374/ [Accessed 18.05.18]. | |
Shetty J, Vishalakshi A, Pandey D. Labour Analgesia When Epidural Is Not a Choice: Tramadol versus Pentazocine. ISRN Obstetrics and Gynecology 2014; Article ID 930349, 4 pages. Available from DOI: 1155/2014/930349. | |
Anabah T, Olufolabi A, Boyd JC, et al. Low-dose spinal anaesthesia provides effective labor analgesia and does not limit ambulation. South Afr Journal Anesth Analg 2015;21:27–30. Available from DOI: 1080/22201181.2015.1013322. | |
World Health Organization (WHO). Guide to Anaesthetic Infrastructure and Supplies at Various Levels of Health Care Facilities. Geneva, Switzerland, 2012. [Online] Available from: http://www.who.int/surgery/publications/GuideAnaestheticInfrastructureSupplies_revAug2012.pdf [Accessed 24.06.18]. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)