This chapter should be cited as follows:
Leitao Jr MM, Nchako CM, Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.421973
The Continuous Textbook of Women’s Medicine Series – Gynecology Module
Volume 13
Gynecological cancer
Volume Editors:
Professor Hextan Ngan, Department of Obstetrics and Gynaecology, The University of Hong Kong, Hong Kong
Professor Karen Chan, Department of Obstetrics and Gynaecology, The University of Hong Kong, Hong Kong
Chapter
Endometrial Cancer: Surgical Aspects
First published: June 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Surgery has long been the principal modality in the management of endometrial carcinoma, serving both diagnostic and therapeutic purposes. Historically, the standard approach consisted of total abdominal hysterectomy with bilateral salpingo-oophorectomy and comprehensive surgical staging, including pelvic and para-aortic lymphadenectomy. This approach not only established the extent of disease but also provided critical prognostic information guiding adjuvant therapy. Over time, refinements in knowledge of surgical anatomy, perioperative care, and oncologic principles have shaped a more nuanced understanding of the role and extent of surgery in this disease.
The evolution of surgical management has paralleled broader trends in gynecologic oncology toward individualized, risk-adapted care, while improving perioperative outcomes and patients’ quality of life. Minimally invasive surgery (MIS) has increasingly replaced traditional laparotomy as the preferred approach for most early-stage cases, offering equivalent oncologic outcomes with reduced perioperative morbidity and faster recovery. Similarly, the development of sentinel lymph node (SLN) mapping has challenged the historical practice of systematic lymphadenectomy by allowing accurate nodal assessment while minimizing complications such as lymphedema and nerve injury.
In Stage-II disease, the role of radical hysterectomy remains an area of ongoing debate, as clinicians balance the potential benefits of wider resection against the morbidity associated with radical surgery. For patients with advanced or recurrent disease, cytoreductive surgery continues to play a pivotal role in select cases in which complete resection is achievable, reflecting principles derived from broader oncologic experience.
Overall, surgical management of endometrial cancer has transitioned from a uniform, one-size-fits-all approach to a more tailored strategy that accounts for tumor biology, disease extent, and patient-specific factors. This evolution underscores the continuing importance of surgical judgment, multidisciplinary collaboration, and institutional expertise in optimizing outcomes for women with endometrial carcinoma.
SURGICAL APPROACH: MINIMALLY INVASIVE OR LAPAROTOMY
Endometrial cancer staging was changed from clinical to surgical in 1988 by the International Federation of Gynecology and Obstetrics’ (FIGO) Gynecologic Oncology Committee. Staging includes findings from total (cervix + uterine corpus) hysterectomy, bilateral salpingo-oophorectomy, lymph node assessment, and inspection of intraperitoneal organs and tissue with biopsy of suspicious lesions. Historically, this was performed via laparotomy through a midline vertical incision. Around the same time, laparoscopic approaches to gynecologic and pelvic surgery began to emerge. The first laparoscopic hysterectomy for benign disease was reported by Reich et al.1 in 1989, and 2 years later, Querleu et al.2 reported the successful use of laparoscopy in pelvic lymph node dissection in a patient with cervical cancer. In 1992, Nezhat et al.3 reported on laparoscopic radical hysterectomy with para-aortic and pelvic lymph node dissection in a patient with cervical cancer. In the early 1990s, Childers et al.4 and Spiritos et al.5 published case series with patients who underwent successful laparoscopic surgical staging and lymph node dissection, helping pave the way for the advent of laparoscopic surgery in endometrial cancer.
The development and refinement of the laparoscopic pelvic technique continued into the 2000s with the landmark Laparoscopic Approach to Cancer of the Endometrium (LACE) trial,6 published in 2006, and the Gynecologic Oncology Group (GOG) LAP2 trial, published in 2009.7 LACE was a multinational randomized trial that compared total laparoscopic hysterectomy (TLH) with total abdominal hysterectomy (TAH) in patients with Stage-I endometrial cancer, with the goal of determining if the approaches were equivalent. A total of 760 patients were randomized to TLH or TAH with or without lymphadenectomy and followed for a median of 4.5 years. The disease-free survival (DFS) rate at 4.5 years was 81.6% vs 81.3% (TLH vs TAH), meeting the prespecified equivalence margin. Overall survival (OS) and relative risk (RR) also were not significantly different between the two groups. TLH was associated with fewer serious postoperative adverse events (AEs) and shorter hospital stay.
The LAP2 randomized trial was also designed to assess the effectiveness of laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer. Patients with clinical Stage-I–IIA endometrial cancer were randomized 1 : 2 to open (n = 920) versus laparoscopic (n = 1696) surgery. Laparoscopic staging was completed in 1248 patients (74%; conversion in 26%). There were fewer moderate to severe postoperative AEs with laparoscopy (14% vs 21%; P < 0.001), similar rates of intraoperative complications, longer operating times in the laparoscopic cases (median, 204 vs 130 min; P < 0.0001), a lower number of hospitalizations > 2 days in the laparoscopic cases (52% vs 94%, P < 0.0001), and no difference in overall detection of advanced disease (17% in both arms, P = 0.841). This landmark study showed that laparoscopic staging was safe and feasible based on short-term outcomes. Quality-of-life assessments were also performed at 1, 3 and 6 weeks, then 6 months postoperatively. Within the 6-week postoperative period, patients who underwent laparoscopy reported superior quality of life, less pain, fewer physical symptoms, earlier resumption of their presurgical activities and work, as well as better body image than those who underwent laparotomy.
The long-term follow-up data from the LAP2 trial were published in 2012 with the primary objective of determining whether surgical technique impacts pattern of recurrence or DFS.8 There was a median follow-up of 59 months with an estimated hazard ratio (HR) for death of 1.14 (CI = 0.92–1.46). The estimated 3-year recurrence rates were 11.39% vs 10.24% with laparoscopic versus laparotomy, respectively. This difference of 1.15% met the study design criteria for non-inferiority (i.e. < 5.3% difference). The 5-year OS rate was 89.8% in both arms. In conclusion, the increased risk for recurrence was small between laparoscopic versus open surgery. Notably, the expected event rate was much less than anticipated. Therefore, the trial technically did not meet its primary endpoint of non-inferiority statistically; however, the survival curves were superimposed without separation.
The LACE and LAP2 studies provided pivotal evidence for the current guidelines used by the National Comprehensive Cancer Network (NCCN), Society of Gynecologic Oncology (SGO), European Society of Gynaecological Oncology (ESGO), and FIGO for MIS (laparoscopic or robotic-assisted) as the standard of care for most early-stage (Stages I and II) endometrial cancers, reserving laparotomy for select advanced cases or technically challenging patients with early disease.
The vaginal approach for surgical staging is not routinely used for patients with known or suspected endometrial malignancy, due to limitations such as the inability to evaluate the upper abdomen or pelvis, inability to perform pelvic or para-aortic lymph node assessment, inability to obtain pelvic washings, possible inability to remove adnexal structures, and the possible need for specimen morcellation upon transvaginal extraction. Pure vaginal approaches have decreased in utilization worldwide for all indications, which has been attributed primarily to the rise of laparoscopic and robotic-assisted procedures.
With the US Food and Drug Administration’s (FDA) approval of computer-assisted surgical platforms (i.e. 'robotic surgery') for gynecologic indications in 2005 came further investigation of the cost-effectiveness and safety of laparotomy versus laparoscopic and robotic-assisted approaches. In 2014, Leitao Jr et al.9 from Memorial Sloan Kettering Cancer Center published a study assessing the direct costs of the three surgical approaches in uterine cancer, as well as the cost impact of incorporating robotic-assisted surgery. Direct costs of 436 cases were assessed: 132 involved laparoscopy, 262 involved robotic-assisted surgery, and 42 involved laparotomy. They found that laparoscopy was least expensive when including capital acquisition costs and was comparable to its robotic counterpart if upfront costs were excluded. They also found that there was cost neutralization with robotic-assisted surgery when it helped decrease laparotomy rates, which was primarily driven by the decreased length of hospital stay and complications for an entire cohort of patients with endometrial carcinoma.
Another study by the same group published in 2016 evaluated the use of the robotic surgical approach and costs in the management of morbidly obese patients with newly diagnosed uterine carcinoma.10 The body habitus of morbidly obese patients tends to make minimally invasive approaches more challenging due to complexities related to intraperitoneal entry, respiratory tolerance of Trendelenburg positioning, and increased risk of blood loss and/or postoperative infection. They retrospectively analyzed 426 morbidly obese patient cases across 15 surgeons during a 20-year study period. For MIS cases in the morbidly obese patient cohort, they reported shorter median length of stay, lower complication rates, and lower rates of wound-related complications; all were statistically significant. Open surgical approaches were associated with higher costs. Overall, the robotic MIS approach was shown to provide significant health and cost benefits in a patient population that had historically been considered suitable only for open surgery.
Despite the advances in minimally invasive technology and the evidence supporting its utilization, the selection of surgical approach must be individualized for the patient. We recognize the diversity in regional and global practice settings, resources, surgical training, and level of expertise. The optimal surgical strategy should reflect a balance between evidence-based practice, surgeon capabilities, oncologic safety, surgical center resources, and patient-specific factors.
ROLE OF RADICAL HYSTERECTOMY FOR FIGO 2009 STAGE-II DISEASE
The primary treatment modality for early-stage endometrial carcinoma has predominantly been surgical excision of the uterine corpus and cervix, along with the Fallopian tubes and ovaries. An area of debate in the surgical management of endometrial carcinoma has been regarding the extent of surgery for FIGO 2009 Stage-II disease. This stage is defined by cervical stromal invasion without extension beyond the uterus. Historically, the presence of cervical involvement prompted some surgeons to perform a radical or modified radical hysterectomy – analogous to the surgical practices undertaken in earlier-stage cervical carcinoma. This approach assumed that cervical involvement meant a higher risk of parametrial spread, warranting a wider or more radical resection.
The rationale for a more radical hysterectomy for Stage-II disease originated from small retrospective studies noting an association with improved survival for Stage-II uterine corpus carcinomas treated with radical hysterectomy over simple hysterectomy.11,12 Surgeons thus advocated for removal of the parametrium and upper vagina to achieve negative margins and prevent local recurrence; however, subsequent studies did not find the same association. For example, a retrospective study by Watanabe et al.13 of over 330 patients with endometrial carcinoma who underwent radical hysterectomy over almost a 20-year timespan revealed that only 8.4% of patients had histopathologically confirmed parametrial spread; and on multivariate analysis, parametrial spread was not an independent prognostic factor in patients with endometrial carcinoma. They concluded that parametrial spread cannot be predicted by cervical involvement alone but may be predicted by various lymphovascular space invasion-related histopathologic factors.
Several studies and meta-analyses have compared oncologic outcomes between radical and simple hysterectomy for FIGO 2009 Stage-II disease.14,15,16 Most studies showed no statistically significant difference in OS or DFS between patients who underwent simple versus radical or modified radical hysterectomy, even with adjustment for adjuvant therapies. Conversely, radical hysterectomy was associated with increased operative time, blood loss, and postoperative complications, including urinary dysfunction, fistula formation, and longer recovery.17,18 These morbidity considerations have become increasingly important as MIS has become the standard for early-stage endometrial cancer, as detailed in the previous section.
Current guidelines from NCCN and ESGO state that simple hysterectomy is preferred over its radical counterpart for clinically apparent Stage-II disease, with the radical approach utilized only in the pursuit of negative margins otherwise unattainable (e.g. high pre/intraoperative suspicion of parametrial involvement). Prospective trials remain limited and could help delineate which patients, if any, would derive any meaningful benefit from a radical hysterectomy in this setting. It is unlikely, however, that a randomized controlled trial will ever be feasible as the number of Stage-II cases is quite small. Radical hysterectomy should be avoided unless needed for negative tumor resection, as our focus continues to shift toward risk-adaptive and less invasive surgery that maximizes safety and minimizes harm, which is in line with the evolution of gynecologic oncology surgery toward precision, personalization, and preservation of quality of life without compromising survival outcomes.
SURGICAL NODAL ASSESSMENT
The surgical assessment of lymph nodes is an established and essential part of endometrial carcinoma treatment. It is necessary for accurate staging and prognosis and for guiding adjuvant therapy; however, the approach to lymph node dissection has been debated constantly, with experts advocating for comprehensive bilateral pelvic and para-aortic lymphadenectomy up to the renal vessels, various modifications of this approach, and for utilization of algorithms to guide selective lymphadenectomy. Before the 1970s, endometrial cancer was primarily treated with simple hysterectomy and bilateral salpingo-oophorectomy, often without formal staging. Lymphatic spread was recognized pathologically but not routinely addressed surgically. The prevailing belief was that most cases were confined to the uterus and that adjuvant radiotherapy could manage occult regional disease. Pelvic and para-aortic nodal dissections were performed sporadically, largely for diagnostic rather than therapeutic intent.
In the late 1980s, GOG 3319 was published, which was a landmark single-arm, clinicopathologic prospective study defining the patterns of spread in clinical Stage-I endometrial cancer. All patients with endometrial carcinoma underwent hysterectomy along with comprehensive bilateral pelvic and para-aortic nodal dissection to the level of the renal vessels. Lymph node metastasis was noted in 11% of patients with clinical Stage-I disease. This study demonstrated a relationship between tumor grade, depth of invasion, and nodal disease. FIGO officially transitioned to surgical staging in 1988, incorporating lymphadenectomy as part of comprehensive staging for accurate prognostication, based on this single-arm, clinicopathologic study as opposed to Level-I evidence from a randomized controlled trial. An unintentional consequence of this decision was the drive toward aggressive lymph node dissections for these patients. While the study objective was ‘to correlate the uterine and adnexal pathology with extrauterine spread and recurrence’, the result was a major adoption of routine lymphadenectomy in all patients with endometrial carcinoma.
Through the 1990s, comprehensive pelvic and para-aortic lymphadenectomy became standard in many centers, particularly in the USA where surgeons viewed lymph node dissection as both diagnostic and potentially therapeutic, believing that removing microscopic nodal disease might improve survival and allow tailored adjuvant therapy. In the early 2000s, there was also an increasing recognition of the morbidity of extensive lymph node dissections, particularly lymphedema, lymphocyst formation, vascular injury, increased blood loss, and prolonged operative times.
Then in 2008 and 2009, two multicenter randomized controlled trials were published that helped shed light on the routine practice of lymphadenectomy. Benedetti Panici et al. randomized patients to standard hysterectomy with bilateral salpingo-oophorectomy alone (n = 250) or to this and pelvic systemic lymphadenectomy (n = 264).20 Patients without myoinvasion or with well-differentiated tumors with less than half myoinvasion on intraoperative assessment were excluded. Unsurprisingly, lymphadenectomy improved surgical staging through the discovery of more patients with lymph node metastases. The 5-year DFS (85.9% vs 90%) and OS (81% vs 81.7%) rates in an intention-to-treat analysis were similar between the lymphadenectomy and non-lymphadenectomy arm, respectively. The ASTEC trial published 1 year later randomly allocated 1408 patients with histologically proven endometrial carcinoma to standard surgery (hysterectomy, bilateral salpingo-oophorectomy, peritoneal washings, and palpation of para-aortic nodes; n = 704) or to standard surgery plus pelvic lymphadenectomy (n = 704).21 The primary outcome was OS and an intention-to-treat analysis was planned. With a median follow-up of 37 months, the absolute difference in OS rate was 1% in favor of standard surgery (the study was designed to show improved OS by 10%) and the absolute difference in recurrence-free survival rate was 6% in favor of standard surgery. They concluded there was no evidence of benefit of lymphadenectomy and thus it cannot be recommended as a routine procedure for therapeutic purposes. Both trials have been heavily criticized mainly for inclusion of mostly low-risk cases and lack of para-aortic lymphadenectomy; however, they catalyzed a philosophical shift away from routine full lymphadenectomy in many patients.
Over the past 15 years, the surgical practice of SLN mapping has become the preferred staging method in many international guidelines (e.g. NCCN, ESGO, European Society for Radiotherapy and Oncology [ESTRO]), especially for early-stage, apparent uterine-confined disease. The concept of SLN mapping was originally adapted from melanoma and breast cancer surgery. The SLN is the first to collect lymphatic fluid from the organ or tissue of interest, and thus a representative of possible regional involvement. In theory, if the first lymph node in a connective chain is negative for disease, then lymphatic extension to the remaining lymphatic tissue has not yet occurred, negating the need for a full lymphadenectomy. Cervical injections of tracer are done superficially and deep in the cervical stroma most commonly at the 3 o’clock and 9 o’clock positions (Figure 1). Mapping tracers include isosulfan (blue) dye, indocyanine green (ICG), technetium (Tc)-99m, carbon nanoparticles (CNP), or some combination thereof. Systematic reviews and meta-analyses comparing various tracers have consistently demonstrated that ICG achieves the highest pooled detection rates, ranging from 90% to 94% for overall and bilateral mapping.22,23,24 Owing to its superior optical properties, safety profile, and ease of intraoperative use, SGO and other international bodies now recommend ICG dye with near-infrared fluorescence imaging as the preferred tracer for SLN mapping in endometrial cancer.25 This approach offers excellent reproducibility, shorter learning curves, and improved bilateral detection compared with conventional blue dyes or radiocolloids. Radioactive Tc-99 use has not improved detection rates, especially if using ICG, and add costs and patient inconvenience; therefore, it is not routinely recommended.
|
|
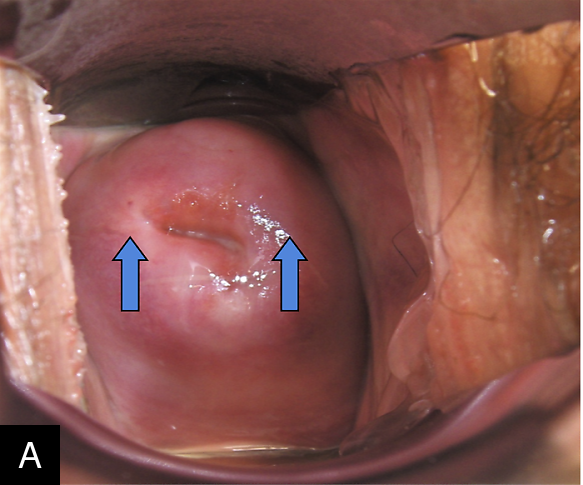

1
Injection of tracer for sentinel lymph node mapping in endometrial cancer. (A) The 3 and 9 o’clock positions (arrows) on the cervical stroma, usually selected for site of injection of tracer. (B) Injection of indocyanine green into the cervix.
Several meta-analyses and systematic reviews highlight the high detection rate associated with SLN mapping.22,26,27 Subsequently, multiple prospective studies have been performed to validate the accuracy of SLN mapping in detecting nodal disease (Table 1). The multicenter Fluorescence Imaging for Robotic Endometrial SLN biopsy (FIRES) study assessed the accuracy of SLN mapping.28 Eligible patients with clinical Stage-I endometrial carcinoma of any grade or histology who were undergoing robotic-assisted staging surgery were included. ICG was injected intra-cervically; SLN mapping followed by comprehensive pelvic lymph node dissection was performed in 340 patients and para-aortic lymph node dissection was performed in 196. Overall, 86% of patients had successful mapping of one or more SLNs, and 35 (11%) had positive nodes. The sensitivity for SLN mapping in detecting nodal disease was 97.2%, and the negative predictive value (NPV) was 99.6%. The false-negative rate was 2.8% and the NPV was 99.6%. These results, published in 2017, provided evidence that SLN mapping has high diagnostic accuracy and could safely replace lymph node dissection in staging of endometrial carcinoma.
1
Prospective studies evaluating the accuracy of sentinel lymph node mapping in detecting nodal disease.
Study | ||||
Characteristic | FIRES (Rossi et al., 2017)28 | SENTOR (Cusimano et al., 2021)29 | SHREC (Persson et al., 2019)31 | Soliman et al., 201730 |
Study design | Multicenter, prospective cohort | Multicenter, prospective cohort | Two-center, prospective cohort | Single-center prospective |
Patients (n) | 385 (340 per protocol w/ 1+ SLN mapped) | 156 | 257 | 101 (evaluable) |
Disease stage/grade | Clinical stage I, all grades/histologies | Clinical stage I, grade 2 endometrioid and high-grade | Presumed FIGO stage I/II, high-risk EC (high-grade histology, > 50% invasion, or stage II) | High-risk EC (grade 3, serous, clear cell, carcinosarcoma); grade 1 or 2 if deep invasion or cervical invasion |
Proportion high-grade (%) | ~28 | ~81 | 100 high-risk criteria | 100 high-risk histology |
Tracer used | ICG | ICG | ICG | ICG (61%), blue dye (28%), blue dye + Tc-99m (11%) |
Reference standard | PLND ± PALND | PLND (grade 2); PLND + PALND (high-grade, 80%) | PLND + infrarenal PALND | Complete PLND + PALND |
SLND detection rate (per patient) (%) | 86 | 97.4 | Not reported separately | 89 |
Bilateral detection rate (%) | 52 | 77.6 | 95 | 58 |
Node positivity rate (n/N (%)) | 36/340 (10.6) | 27/156 (17) | 54/257 (21) | 23/101 (23) |
Sensitivity (SLN algorithm) (%) | 97.2 (95% CI, 85–100) | 96.3 (95% CI, 81–100) | 98 ICG-SLN; 100 overall SLN algorithm (95% CI, 92–100) | 95 (19/20) |
False negative rate (%) | 2.8 | 3.7 (95% CI, 0–19) | 2 ICG-SLN; 0 overall algorithm | 4.3 (with side-specific LND for failed mapping) |
Negative predictive value (%) | 99.6 (95% CI, 97.9–100) (FNPV 0.4) | 99.2 (95% CI, 96–100) (FNPV 0.8%) | 99.5 ICG-SLN; 100 overall algorithm (95% CI, 98–100) (FNPV 0.5%) | 98.6 (FNPV 1.4) |
EC, endometrial cancer; FIGO, International Federation of Gynecology and Obstetrics; FNPV, false negative predictive value; ICG, indocyanine green; LND, lymph node dissection; PALND, para-aortic lymph node dissection; PLND, pelvic lymph node dissection; SLN, sentinel lymph node; SLND, sentinel lymph node dissection; Tc, technetium.
The SENTOR study also assessed the accuracy of SLN mapping but in intermediate- and high-grade endometrial carcinoma.29 This prospective cohort study of 156 patients identified 126 (81%) with high-grade endometrial cancer. All underwent backup pelvic lymphadenectomy after SLN mapping and biopsy, and 80% also had a para-aortic lymphadenectomy. The overall node-positivity rate was 17%. Sensitivity of SLN mapping to detect nodal positivity was 96.3%, with a false negative rate of 3.7% and a false negative predictive value of 0.8%. To explore this same theme in exclusively high-risk endometrial cancer histologies (serous, clear cell, carcinosarcoma, Grade 3), Soliman and colleagues performed a prospective study of 123 patients with high-risk endometrial carcinomas defined as Grade-3 endometrioid (with any invasion), Grade 1 or 2 with deep invasion or cervical invasion, and any serous, clear cell and carcinosarcoma.30 Again, the sensitivity of SLN mapping was 95% and the NPV was 98.6%. SHREC was another prospective study including all patients with FIGO Grade-3 endometrioid or non-endometrioid histologies with or without myoinvasion, or with any other histology with ≥50% myoinvasion and/or cervical stromal invasion;31 again, a 99.5% NPV was observed.
These studies have helped establish SLN mapping as an accurate method to detect nodal metastasis in apparent uterine-confined disease, though clinical factors such as surgeon expertise and tracer injection technique or site can affect the ability to successfully identify and extract the SLN; however, worldwide debate remains about the oncologic safety in 'high-risk' endometrial carcinomas. There are currently no published randomized controlled trials addressing oncologic outcomes.
Multiple retrospective analyses from our institution, and some in collaboration with other institutions, in high-grade histologies such as serous, clear cell, carcinosarcoma, and advanced-stage disease have noted similar oncologic outcomes for SLN mapping compared to lymph node dissection.32,33,34 National Cancer Database (NCDB) analyses in Stage-I intermediate- and high-intermediate risk endometrioid carcinomas also noted similar oncologic outcomes,35 as have NCDB analyses in patients with nodal metastasis (FIGO Stage IIIC).36 Similar oncologic outcomes have also been reported in ESGO-defined 'high-risk' carcinomas.37
It is important to follow a validated SLN algorithm when instituting this approach. The SLN algorithm for surgical staging of endometrial cancer was developed and published by Barlin et al. at Memorial Sloan Kettering Cancer Center in 2012.38 In comparison to SLN mapping alone, when applied, the algorithm was associated with a drop in false-negative rate from 15% to 2%. It consists of evaluating the peritoneum and serosa, as well as collecting washings. This is followed by retroperitoneal evaluation with excision of all mapped SLNs, and any suspicious nodes regardless of dye or tracer uptake. Importantly, if mapping is unsuccessful in one hemipelvis, a side-specific pelvic lymphadenectomy should be performed. Para-aortic lymph node dissection is at the surgeon's discretion. This algorithm has since been widely accepted, adopted by NCCN, and has become an accepted standard for staging endometrial carcinoma. An important principle is that true SLN mapping requires identification of the lymphatic channels draining from the cervix after development of the pelvic spaces. Only the first draining node should be removed as the SLN. Removal of all colored nodes does not constitute SLN mapping, as nodes beyond the SLN are secondary non-SLNs, and these do not need to be removed.
Molecular classification of endometrial carcinomas is increasingly being performed. Some have suggested that classification of preoperative biopsies may help to decide on surgical approach and need for nodal assessment. A retrospective analysis from our institution, however, noted that there was a risk of nodal metastasis in all four molecular groups (5% in POLE, 8.7% in no specific molecular subtype [NSMP], 22.8% in mismatch repair deficient [MMRd], and 26% in p53 abnormal).39 Very similar findings were reported in the SENECA study, which included 2139 cases from 66 centers.40 The rate of nodal metastasis was 6.3% in POLE, 7.8% in NSMP, 12.4% in MMRd, and 12.5% in p53 abnormal. These authors also noted that the incorporation of molecular grouping to standard histopathologic factors defined by ESGO did not improve the prediction of nodal metastasis. To date, no data support the use of preoperative molecular classification for decision-making about surgical nodal staging.
While lymph node assessment in endometrial cancer is not a one-size-fits-all practice, SLN mapping is emerging as a global standard for surgical staging in most early-stage cases. The gradual evolution from radical uniformity toward risk-adapted, evidence-based, and minimally invasive intervention will continue to decrease the morbidity of surgical intervention and improve survival outcomes.
CYTOREDUCTION IN ADVANCED ENDOMETRIAL CARCINOMA
Surgical cytoreduction or 'debulking' is a consideration in the management of clinically advanced (FIGO Stage III or IV) endometrial carcinoma. Two broad surgical strategies are commonly considered: primary debulking surgery (PDS) i.e. attempting cytoreduction up front followed by adjuvant systemic therapy, and neoadjuvant chemotherapy (NACT) with interval debulking surgery (IDS) i.e. chemotherapy first with cytoreductive surgery performed after a defined number of cycles in patients who demonstrate a response. A core clinical question every surgeon faces is whether initial surgery or a chemotherapy-first approach will yield superior oncologic outcomes for their patient, all while balancing possible perioperative complexity and morbidity.
The role and timing of cytoreductive surgery have been extensively studied in ovarian carcinomas, including in multiple randomized controlled trials; however, there have been no randomized controlled trials in endometrial cancer. Retrospective analyses have demonstrated associations with improved progression-free survival and OS among patients who achieve complete gross resection (CGR) or optimal cytoreduction, while submaximal or suboptimal (≥1 cm) resection has been associated with poorer progression-free survival and OS.41,42 In patients with advanced disease, surgical procedures may also include resections of large and small bowel, diaphragm, splenic or hepatic surfaces, and parenchyma. Patients with good performance status (Eastern Cooperative Oncology Group [ECOG]/Karnofsky Performance Status [KPS]), resectable disease on imaging (limited peritoneal disease, absence of bulky unresectable nodal/metastatic spread), and absence of significant comorbidity are classic candidates for PDS. However, many patients present with disease that is unlikely to be optimally cytoreduced at presentation. Those with widespread peritoneal involvement, massive ascites or bulky extrapelvic disease, poor performance status, or comorbidities precluding major surgery may be better served with NACT and planned IDS.
In an NCDB analysis by Chambers et al. of over 48,000 patients identified with FIGO Stage-III/IV endometrial cancer from 2004 to 2015, PDS followed by chemotherapy (HR, 0.32; 95% CI, 0.30–0.35; P < 0.001) or NACT + IDS (HR, 0.44; 95% CI, 0.40–0.49; P < 0.001) were associated with improved OS compared to chemotherapy alone.43 In the multivariate analysis, PDS + chemotherapy was shown to improve OS in all Stage-III substages in comparison to NACT + IDS, except in patients with Stage IIIB, non-endometrioid endometrial cancer. In Stage-IV disease, PDS + chemotherapy showed an improved OS compared to NACT + IDS.
In another NCDB cohort analysis by Tobias et al. comparing PDS and NACT +/- IDS in patients with Stage-IV endometrial cancer, the findings showed mixed results.44 In the intention-to-treat analysis, OS was superior in the NACT cohort but only for the first 3 months after diagnosis, after which OS was better for those who underwent PDS. Even in the per-protocol analysis, similar survival trends were seen, with the Kaplan–Meier curves crossing after approximately 8 to 9 months. These findings support the notion that surgical treatments must be individualized based upon disease distribution, but treatment plans for advanced endometrial cancer should involve surgical resection whenever feasible.
High-risk histologies frequently present with disseminated disease and have varying responses to first-line platinum-based chemotherapy, adding another layer of complexity to NACT treatment plans. The recent emergence of molecular classification (e.g., p53, MMR, POLE, NSMP) of endometrial cancer has added a lens of investigation, with some data suggesting that molecular subtype may impact chemosensitivity, thus influencing the surgical sequencing decision. There is currently insufficient data to reliably incorporate molecular classifiers into the surgical decision pathways. For example, one retrospective analysis by Caiazzo et al. did not show a statistically significant correlation between the type of surgical approach (PDS vs IDS) and DFS (P = 0.523) or OS (P = 0.797).45 While the cohort had only 51 patients, larger analyses and/or prospective trials will be necessary to draw more definitive conclusions about the impact of molecular classification and surgical treatment of advanced-stage endometrial cancer. It seems that surgical cytoreduction may be of value in patients with clinically advanced disease; however, it remains unclear as to optimal timing of surgery.
Major international guidelines acknowledge both primary and interval debulking strategies. Contemporary NCCN, SGO, and ESGO guidance supports PDS when complete cytoreduction is feasible with acceptable morbidity and the patient can tolerate major surgery; NACT with planned IDS is seen as reasonable for patients with unresectable disease or prohibitive operative risk. Institutional and regional practice patterns vary, with high-volume surgical centers with more surgical expertise often favoring aggressive upfront PDS, while others may adopt selective NACT + IDS strategies to minimize morbidity in the pursuit of CGR. The absence of randomized data means interdisciplinary consensus and institutional experience heavily influence decision-making. Given the significant heterogeneity among institutions worldwide in terms of oncology resources, surgical expertise, and case volume, it is imperative that multidisciplinary treatment planning considers the capabilities of the local practice setting while striving to achieve the best possible outcome for the patient.
SURGERY FOR RECURRENCE
Approximately 10–15% of patients with early-stage endometrial cancer and up to 50% with high-risk histology experience disease recurrence after primary therapy.46 Recurrence patterns are heterogeneous and may include isolated vaginal or pelvic recurrence, nodal disease, or distant metastases (lung, liver, peritoneum). The decision to pursue surgical intervention depends primarily on site and extent of recurrence, disease-free interval, histology, and prior treatments, as well as patient performance status and institutional expertise. Local or isolated recurrences, particularly within previously unirradiated fields, can often be approached surgically with curative intent, again with the goal of CGR. In contrast, disseminated or multifocal recurrence is typically managed with systemic therapy, though surgery may have a role in select oligometastatic cases for cytoreduction or symptom control.
Patient selection is paramount. Candidates for surgical management typically have isolated or limited disease amenable to complete resection, good performance status (ECOG 0–2), and no contraindications to major surgery. A long disease-free interval, especially exceeding 12 months, also favors consideration for surgery, as it often reflects more indolent tumor biology.47 Conversely, patients with multifocal, unresectable, or rapidly progressive disease are best managed with systemic therapy or radiation. As in primary cytoreductive surgery, achieving CGR is an extremely important determinant of outcome.48
The surgical approach is guided by the site of recurrence. Isolated vaginal cuff recurrence may be managed by local excision or partial vaginectomy, with the addition of adjuvant radiation therapy when appropriate. For patients with central pelvic recurrence after prior radiation, pelvic exenteration can be considered in highly selected cases if a negative margin resection is technically feasible. Despite its substantial morbidity, exenteration offers the possibility of long-term survival, with 5-year OS rates ranging from 20% to over 60%.49,50,51 Nodal recurrence, particularly isolated pelvic or para-aortic nodal disease, can be treated with targeted lymphadenectomy.
Abdominal or peritoneal recurrences pose significant surgical challenges, as they often indicate disseminated disease. Nonetheless, cytoreductive surgery may be appropriate in carefully selected patients with isolated peritoneal implants or limited intra-abdominal spread. Similarly, resection of solitary distant metastases – such as hepatic, splenic, or pulmonary lesions – can provide meaningful survival benefits, particularly when recurrence occurs after a long disease-free interval.
Across studies, CGR consistently correlates with improved outcomes, with median OS exceeding 60 months when achieved, compared to less than 20 months with residual disease.44,52,53,54 Favorable prognostic factors include isolated vaginal recurrence, endometrioid histology, low tumor burden, and the absence of ascites or peritoneal dissemination. Morbidity is largely dependent on the extent of surgery but is reduced in high-volume centers. Minimally invasive approaches may be suitable for select nodal, vaginal, or peritoneal recurrences depending on surgeon expertise, offering lower perioperative morbidity and faster recovery without compromising oncologic results.
International guidelines uniformly emphasize individualized, multidisciplinary decision-making. NCCN recommends considering surgical resection for isolated or oligometastatic recurrences when complete excision is feasible, while ESGO/ESTRO/ESP and European Society for Medical Oncology (ESMO) guidelines similarly endorse surgery for limited, resectable disease within a multimodal framework. SGO further notes that exenterative or secondary cytoreductive procedures can offer curative potential in carefully selected patients treated at experienced centers. Collectively, these guidelines recognize that although evidence is primarily derived from retrospective data, surgery retains a pivotal role in the management of certain recurrent cases.
Overall, surgical intervention for recurrent endometrial cancer offers an opportunity for long-term disease control in appropriately selected patients. The success of this approach depends on achieving CGR, optimizing patient selection, and coordinating care within a multidisciplinary setting. As systemic therapies evolve and molecular profiling refines risk stratification, future strategies will likely integrate surgical cytoreduction with targeted and immunotherapeutic approaches, in the upfront and recurrent settings.
PRACTICE RECOMMENDATIONS
- Minimally invasive surgery, including laparoscopic or robotic-assisted techniques, should be considered the preferred surgical approach for most patients with apparent early-stage endometrial carcinoma because of equivalent oncologic outcomes and reduced perioperative morbidity compared with laparotomy.
- Sentinel lymph node mapping with indocyanine green fluorescence should be utilized as the preferred nodal staging strategy in most uterine-confined endometrial cancers, following an established sentinel lymph node algorithm and including side-specific lymphadenectomy in cases of failed mapping.
- Routine comprehensive pelvic and para-aortic lymphadenectomy should be avoided in endometrial carcinoma because it increases surgical morbidity without demonstrable survival benefit.
- Simple hysterectomy is generally preferred over radical hysterectomy for most patients with FIGO Stage-II endometrial carcinoma unless wider resection is required to obtain negative surgical margins or there is strong suspicion of parametrial involvement.
- Patients with advanced or recurrent endometrial carcinoma should be evaluated in a multidisciplinary setting to determine candidacy for primary cytoreduction, neoadjuvant chemotherapy with interval debulking, or secondary cytoreductive surgery, with the goal of achieving complete gross resection whenever feasible.
CONFLICTS OF INTEREST
Dr Leitao reports consulting fees from Medtronic; ad-hoc speaker fees from Intuitive Surgical, Inc.; and advisory board participation with JnJ/Ethicon. Dr Nchako reports no potential conflicts.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Reich H, Decaprio J, McGLYNN F. Laparoscopic hysterectomy. J Gynecol Surg. 1989;5(2):213–216. | |
Querleu D, Leblanc E, Castelain B. Laparoscopic pelvic lymphadenectomy in the staging of early carcinoma of the cervix. Am J Obstet Gynecol. 1991;164(2):579–581. | |
Nezhat CR, Burrell MO, Nezhat FR, Benigno BB, Welander CE. Laparoscopic radical hysterectomy with paraaortic and pelvic node dissection. Am J Obstet Gynecol. 1992;166(3):864–865. | |
Childers JM, Brzechffa PR, Hatch KD, Surwit EA. Laparoscopically assisted surgical staging (LASS) of endometrial cancer. Gynecol Oncol. 1993;51(1):33–38. | |
Spirtos NM, Schlaerth JB, Spirtos TW, Schlaerth AC, Indman PD, Kimball RE. Laparoscopic bilateral pelvic and paraaortic lymph node sampling: an evolving technique. Am J Obstet Gynecol. 1995;173(1):105–111. | |
Janda M, Gebski V, Forder P, Jackson D, Williams G, Obermair A. Total laparoscopic versus open surgery for stage 1 endometrial cancer: the LACE randomized controlled trial. Contemp Clin Trials. 2006;27(4):353–363. | |
Walker JL, Piedmonte MR, Spirtos NM, Eisenkop SM, Schlaerth JB, Mannel RS, et al. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J Clin Oncol. 2009;27(32):5331–5336. | |
Walker JL, Piedmonte MR, Spirtos NM, Eisenkop SM, Schlaerth JB, Mannel RS, et al. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J Clin Oncol. 2012;30(7):695–700. | |
Leitao MM, Jr., Bartashnik A, Wagner I, Lee SJ, Caroline A, Hoskins WJ, et al. Cost-effectiveness analysis of robotically assisted laparoscopy for newly diagnosed uterine cancers. Obstet Gynecol. 2014;123(5):1031–1037. | |
Leitao MM, Narain WR, Boccamazzo D, Sioulas V, Cassella D, Ducie JA, et al. Impact of Robotic Platforms on Surgical Approach and Costs in the Management of Morbidly Obese Patients with Newly Diagnosed Uterine Cancer. Ann Surg Oncol. 2016;23(7):2192–2198. | |
Cohn DE, Woeste EM, Cacchio S, Zanagnolo VL, Havrilesky LJ, Mariani A, et al. Clinical and pathologic correlates in surgical stage II endometrial carcinoma. Obstet Gynecol. 2007;109(5):1062–1067. | |
Cornelison TL, Trimble EL, Kosary CL. SEER data, corpus uteri cancer: treatment trends versus survival for FIGO stage II, 1988–1994. Gynecol Oncol. 1999;74(3):350–355. | |
Watanabe Y, Satou T, Nakai H, Etoh T, Dote K, Fujinami N, et al. Evaluation of parametrial spread in endometrial carcinoma. Obstet Gynecol. 2010;116(5):1027–1034. | |
Liu T, Tu H, Li Y, Liu Z, Liu G, Gu H. Impact of Radical Hysterectomy Versus Simple Hysterectomy on Survival of Patients with Stage 2 Endometrial Cancer: A Meta-analysis. Ann Surg Oncol. 2019;26(9):2933–2942. | |
Nasioudis D, Sakamuri S, Ko EM, Haggerty AF, Giuntoli RL, 2nd, Burger RA, et al. Radical hysterectomy is not associated with a survival benefit for patients with stage II endometrial carcinoma. Gynecol Oncol. 2020;157(2):335–339. | |
Phelippeau J, Koskas M. Impact of Radical Hysterectomy on Survival in Patients with Stage 2 Type1 Endometrial Carcinoma: A Matched Cohort Study. Ann Surg Oncol. 2016;23(13):4361–4367. | |
Barquet-Muñoz SA, Cantú-de-León D, Bandala-Jacques A, González-Enciso A, Isla-Ortiz D, Prada D, et al. What is the impact of radical hysterectomy on endometrial cancer with cervical involvement? World J Surg Oncol. 2020;18(1):101. | |
Takano M, Ochi H, Takei Y, Miyamoto M, Hasumi Y, Kaneta Y, et al. Surgery for endometrial cancers with suspected cervical involvement: is radical hysterectomy needed (a GOTIC study)? Br J Cancer. 2013;109(7):1760–1765. | |
Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer. 1987;60(8 Suppl):2035–2041. | |
Benedetti Panici P, Basile S, Maneschi F, Alberto Lissoni A, Signorelli M, Scambia G, et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: randomized clinical trial. J Natl Cancer Inst. 2008;100(23):1707–1716. | |
Kitchener H, Swart AM, Qian Q, Amos C, Parmar MK. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomised study. Lancet. 2009;373(9658):125–136. | |
Bodurtha Smith AJ, Fader AN, Tanner EJ. Sentinel lymph node assessment in endometrial cancer: a systematic review and meta-analysis. Am J Obstet Gynecol. 2017;216(5):459–476.e10. | |
How JA, O'Farrell P, Amajoud Z, Lau S, Salvador S, How E, et al. Sentinel lymph node mapping in endometrial cancer: a systematic review and meta-analysis. Minerva Ginecol. 2018;70(2):194–214. | |
Ji Q, Wang X, Jiang J, Chen L. Sentinel lymph node mapping in high-risk endometrial cancer: a systematic review and meta-analysis. Gland Surg. 2020;9(6):2091–2105. | |
Holloway RW, Abu-Rustum NR, Backes FJ, Boggess JF, Gotlieb WH, Jeffrey Lowery W, et al. Sentinel lymph node mapping and staging in endometrial cancer: A Society of Gynecologic Oncology literature review with consensus recommendations. Gynecol Oncol. 2017;146(2):405–415. | |
Marchocki Z, Cusimano MC, Clarfield L, Kim SR, Fazelzad R, Espin-Garcia O, et al. Sentinel lymph node biopsy in high-grade endometrial cancer: a systematic review and meta-analysis of performance characteristics. Am J Obstet Gynecol. 2021;225(4):367.e1–.e39. | |
Nagar H, Wietek N, Goodall RJ, Hughes W, Schmidt-Hansen M, Morrison J. Sentinel node biopsy for diagnosis of lymph node involvement in endometrial cancer. Cochrane Database Syst Rev. 2021;6(6):Cd013021. | |
Rossi EC, Kowalski LD, Scalici J, Cantrell L, Schuler K, Hanna RK, et al. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): a multicentre, prospective, cohort study. Lancet Oncol. 2017;18(3):384–392. | |
Cusimano MC, Vicus D, Pulman K, Maganti M, Bernardini MQ, Bouchard-Fortier G, et al. Assessment of Sentinel Lymph Node Biopsy vs Lymphadenectomy for Intermediate- and High-Grade Endometrial Cancer Staging. JAMA Surg. 2021;156(2):157–164. | |
Soliman PT, Westin SN, Dioun S, Sun CC, Euscher E, Munsell MF, et al. A prospective validation study of sentinel lymph node mapping for high-risk endometrial cancer. Gynecol Oncol. 2017;146(2):234–239. | |
Persson J, Salehi S, Bollino M, Lönnerfors C, Falconer H, Geppert B. Pelvic Sentinel lymph node detection in High-Risk Endometrial Cancer (SHREC-trial)-the final step towards a paradigm shift in surgical staging. Eur J Cancer. 2019;116:77–85. | |
Basaran D, Leitao MM, Jr. UPDATE ON SENTINEL LYMPH NODE MAPPING IN ENDOMETRIAL CANCER PATIENTS WITH A HIGH RISK FOR NODAL METASTASIS. Indian J Gynecol Oncol. 2020;18(2). | |
Schlappe BA, Weaver AL, McGree ME, Ducie J, Zahl Eriksson AG, Dowdy SC, et al. Multicenter study comparing oncologic outcomes after lymph node assessment via a sentinel lymph node algorithm versus comprehensive pelvic and paraaortic lymphadenectomy in patients with serous and clear cell endometrial carcinoma. Gynecol Oncol. 2020;156(1):62–69. | |
Zammarrelli WA, 3rd, Greenman M, Rios-Doria E, Miller K, Broach V, Mueller JJ, et al. Sentinel lymph node biopsy alone compared to systematic lymphadenectomy in patients with uterine carcinosarcoma. Gynecol Oncol. 2022;165(2):287–292. | |
Nasioudis D, Byrne M, Ko EM, Giuntoli RL, 2nd, Haggerty AF, Cory L, et al. Outcomes of sentinel lymph node mapping for patients with FIGO stage I endometrioid endometrial carcinoma. Gynecol Oncol. 2021;161(3):705–709. | |
Nasioudis D, Byrne M, Ko EM, Giuntoli Ii RL, Haggerty AF, Cory L, et al. The impact of sentinel lymph node sampling versus traditional lymphadenectomy on the survival of patients with stage IIIC endometrial cancer. Int J Gynecol Cancer. 2021;31(6):840–845. | |
Capozzi VA, Rosati A, Maglietta G, Vargiu V, Scarpelli E, Cosentino F, et al. Long-term survival outcomes in high-risk endometrial cancer patients undergoing sentinel lymph node biopsy alone versus lymphadenectomy. Int J Gynecol Cancer. 2023;33(7):1013–1020. | |
Barlin JN, Khoury-Collado F, Kim CH, Leitao MM, Jr., Chi DS, Sonoda Y, et al. The importance of applying a sentinel lymph node mapping algorithm in endometrial cancer staging: beyond removal of blue nodes. Gynecol Oncol. 2012;125(3):531–535. | |
Praiss AM, Dagher C, Zhou Q, Iasonos A, Rios-Doria E, Abu-Rustum NR, et al. Lymph node metastases in endometrial carcinoma: A modern assessment in the era of sentinel lymph node mapping and molecular subtyping. Gynecol Oncol. 2024;191:37–44. | |
Chacon E, Boria F, Lyer RR, Fanfani F, Malzoni M, Bretová P, et al. SENECA study: staging endometrial cancer based on molecular classification. Int J Gynecol Cancer. 2024;34(9):1313–1321. | |
Albright BB, Monuszko KA, Kaplan SJ, Davidson BA, Moss HA, Huang AB, et al. Primary cytoreductive surgery for advanced stage endometrial cancer: a systematic review and meta-analysis. Am J Obstet Gynecol. 2021;225(3):237.e1–.e24. | |
Rajkumar S, Nath R, Lane G, Mehra G, Begum S, Sayasneh A. Advanced stage (IIIC/IV) endometrial cancer: Role of cytoreduction and determinants of survival. Eur J Obstet Gynecol Reprod Biol. 2019;234:26–231. | |
Chambers LM, Jia X, Rose PG, AlHilli M. Impact of treatment modality on overall survival in women with advanced endometrial cancer: A National Cancer Database analysis. Gynecol Oncol. 2021;160(2):405–412. | |
Tobias CJ, Chen L, Melamed A, St Clair C, Khoury-Collado F, Tergas AI, et al. Association of Neoadjuvant Chemotherapy With Overall Survival in Women With Metastatic Endometrial Cancer. JAMA Netw Open. 2020;3(12):e2028612. | |
Caiazzo F, Raspagliesi F, Chiappa V, Bruni S, Ceppi L, Bogani G. Upfront and interval debulking surgery in advanced/metastatic endometrial cancer in the era of molecular classification. Eur J Obstet Gynecol Reprod Biol. 2025;310:113958. | |
Concin N, Matias-Guiu X, Cibula D, Colombo N, Creutzberg CL, Ledermann J, et al. ESGO-ESTRO-ESP guidelines for the management of patients with endometrial carcinoma: update 2025. Lancet Oncol. 2025;26(8):e423–e35. | |
Ueda Y, Matsumura Y, Egawa-Takata T, Miyake T, Miyatake T, Yoshino K, et al. Disease-free interval after primary treatment predicts prognosis of recurrent endometrial carcinoma. Anticancer Res. 2010;30(10):4347–4352. | |
Shikama A, Minaguchi T, Takao W, Hosokawa Y, Nishida K, Tasaka N, et al. Predictors of favorable survival after secondary cytoreductive surgery for recurrent endometrial cancer. Int J Clin Oncol. 2019;24(10):1256–1263. | |
Chiantera V, Rossi M, De Iaco P, Koehler C, Marnitz S, Gallotta V, et al. Pelvic exenteration for recurrent endometrial adenocarcinoma: a retrospective multi-institutional study about 21 patients. Int J Gynecol Cancer. 2014;24(5):880–884. | |
Khoury-Collado F, Einstein MH, Bochner BH, Alektiar KM, Sonoda Y, Abu-Rustum NR, et al. Pelvic exenteration with curative intent for recurrent uterine malignancies. Gynecol Oncol. 2012;124(1):42–47. | |
Seagle BL, Dayno M, Strohl AE, Graves S, Nieves-Neira W, Shahabi S. Survival after pelvic exenteration for uterine malignancy: A National Cancer Data Base study. Gynecol Oncol. 2016;143(3):472–478. | |
Moukarzel LA, Braxton KF, Zhou QC, Pedra Nobre S, Iasonos A, Alektiar KM, et al. Non-exenterative surgical management of recurrent endometrial carcinoma. Gynecol Oncol. 2021;162(2):268–276. | |
Raffone A, Pellecchia G, Pregnolato S, Raimondo D, Travaglino A, Neola D, et al. Impact of optimal secondary cytoreductive surgery on survival outcomes in women with recurrent endometrial carcinoma: A systematic review and meta-analysis. Int J Gynaecol Obstet. 2025;170(1):119–129. | |
Vargiu V, Rosati A, Capozzi VA, Gioè A, Restaino S, Berretta R, et al. Major determinants of survival in recurrent endometrial cancer-the role of secondary cytoreductive surgery: a multicenter study. Int J Gynecol Cancer. 2023;33(10):1572–1579. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)