This chapter should be cited as follows:
Jauniaux E, Hussein AM, et al., Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.422193
The Continuous Textbook of Women’s Medicine Series – Obstetrics Module
Volume 20
Surgical Techniques in Obstetrics
Volume Editors:
Professor Michael Stark, New European Surgical Academy (NESA) and Charité University Hospital, Berlin, Germany
Professor Sergej Barinov, Omsk State Medical University, Ministry of Health of Russia
Professor Gian Carlo Di Renzo, PREIS International School, Florence, Italy
Chapter
Complex Cesarean Section
First published: April 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Surgically complex cesarean delivery (CD) is a critical topic in obstetric care, reflecting the intricate challenges faced by healthcare providers in managing high-risk pregnancies. We recently proposed a classification for surgical difficulty in elective CD.1 The resources required, which can be adapted to different healthcare settings, vary according to maternal condition, presence of fetal developmental anomalies, gestational age at delivery, maternal history of previous uterine surgery, and presence of placentation anomalies (Table 1). As the rate of cesarean section continues to rise globally, an increasing number of patients present with anomalies of placentation, such as placenta previa and placenta accreta spectrum (PAS), that necessitate advanced surgical techniques and a multidisciplinary (MDT) approach.2
1
Levels II and III of surgical difficulty at elective cesarean delivery and resources required. (Modified from Jauniaux et al.1)
Classification | Condition | Resource required |
Level II (Expert) |
|
|
Level III (MDT) |
|
|
BMI, body mass index; CD, cesarean delivery; FGR, fetal growth restriction; LUS, lower uterine segment; MDT, multidisciplinary team; MRI, magnetic resonance imaging; PAS, placenta accreta spectrum.
This chapter aims to explore the various factors contributing to surgical complexity in CD, including maternal health conditions, surgical history and fetal conditions. By examining the latest research and clinical practices, we can better understand the implications for maternal and neonatal outcomes, as well as the evolving management strategies that enhance safety and efficacy in these challenging surgical procedures.
RISK FACTORS FOR COMPLEX CESAREAN DELIVERY
Maternal health conditions
The main maternal factors that can complicate a CD are diabetes, hypertension and pre-eclampsia, cardiac or respiratory disorders, coagulation disorders, and acute and chronic infectious diseases such as malaria and HIV. These conditions may lead to excessive intraoperative blood loss and anesthetic complications, and their management is guided by local or national protocols to optimize patient comorbidities and preoperative interventions.3
Maternal obesity (body mass index (BMI) of 35.0–39.9) and particularly morbid obesity (Class III; defined as BMI of ≥ 40) has been rising worldwide. It makes surgical access during CD more difficult, leading to longer operation times and increased risk of hemorrhage.4 While neuraxial anesthesia (epidural/spinal) is the preferred technique for peripartum and CD anesthesia, procedures can be technically challenging in patients with high BMI and may require more time, longer needles, increased experience or ultrasound guidance.5 If neuraxial anesthesia is not available, as in many low-resource settings, and general anesthesia is required, obesity can also complicate airway management, making intubation more challenging, and higher doses of anesthetic drugs may be required, raising the risk of side effects and complications. Obese patients often present with hypertension, diabetes and cardiovascular issues, which can add to the risk of deep vein thrombosis, pulmonary embolism, wound infections and delayed healing due to increased adipose tissue and reduced blood flow.4
Chronic maternal infections are more prevalent in low-resource settings and require adherence to strict surgical safety protocols to reduce the risk of mother-to-child transmission. For patients with HIV or hepatitis C, independently of their viral status, standard cesarean techniques are used, but careful handling of sharps is crucial, and staff must use comprehensive barrier precautions, including double gloving, goggles and masks to protect against blood exposure.6
Fetal health conditions
Several fetal conditions can complicate CD, impacting both the procedure and outcomes.7,8 Macrosomia can make delivery more challenging, requiring the use of forceps and increasing the risk of complications during surgery, such as accidental tearing of the lower uterine segment (LUS) and intraoperative hemorrhage. Fetal malpresentation, such as transverse presentation, may require specific surgical techniques (e.g. a T-shaped incision). Similarly, twins and higher-order multiples are often associated with fetal malpresentation and increased risk of hemorrhage due to uterine atony. Structural fetal abnormalities, such as hydrocephaly or fetal tumors (teratomas), can complicate the delivery process.
CD performed before 32 weeks focuses on reducing fetal trauma and stress through specialized techniques such as ‘en caul’ delivery (retaining the amniotic sac) when feasible, avoidance of excessive fundal pressure and delayed cord clamping to improve neonatal blood volume.9 A small hysterotomy is preferred, and a vertical incision may be required if the LUS is not well formed, to avoid trauma to the fetus.
Uterine fibroids
Traditionally, fibroids are left in situ for CD because the highly vascular, pregnant uterus increases the risks of excessive bleeding, blood transfusion and even hysterectomy. However, fibroids that obstruct delivery or interfere with uterine closure may be removed, and uterine incisions through fibroids should be avoided where possible or managed carefully to minimize bleeding.7,8 If performed, myomectomy usually occurs after delivery of the baby and closure of the main uterine incision to minimize bleeding. A tourniquet (e.g. Penrose drain or latex sterile glove) around the cervix or LUS (Figure 1) and uterine artery ligation may be used to minimize blood loss, depending on the topography of the fibroid.

1
Fibroid removal during cesarean section. (A) Following bladder dissection and mobilization, a large fibroid located in the anterior uterine segment was identified. Fetal extraction was performed through a transverse hysterotomy immediately cephalad to the fibroid. (B) A uterine tourniquet made from a sterile latex glove was placed beneath the fibroid. (C) The right uterine artery was ligated prior to fibroid resection. (D) The tourniquet allowed complete control of bleeding after fibroid resection, followed by uterine reconstruction with a two-layer hysterorrhaphy. (E,F) Bladder mobilization is essential for this procedure. The reconstructed uterus with the bladder in its original position (E) and after mobilization (F) shows a normal contour following the procedure, free of abnormal bleeding due to effective hemorrhage control with the tourniquet.
Anomalies of placentation
Patients with an anterior placenta previa covering the cervix and a history of multiple CDs and those with a high probability of PAS on ultrasound imaging are considered to be those with the highest level of surgical complexity, particularly those with both conditions combined, and always require multidisciplinary management by an experienced team (Table 1). The main issue in cases of placenta previa accreta is the risk of massive hemorrhage during the surgical procedure, and blood products should be cross-matched (usually 4 units). Key steps include careful bladder dissection downward extensively to expose as much of the LUS as possible, meticulous management of the placental site to control hemorrhage, and swift administration of uterotonics after delivery of the fetus.10,11,12,13,14 Surgical planning (type of skin and uterine incision, need for peripartum hysterectomy for failure to repair the LUS or for hemostasis) in these cases is increasingly based on preoperative imaging, mainly ultrasound, which should be available across different resource settings15,16 and reduce the need for hysterectomy.
PAS has also been reported in the upper uterine segment and is typically referred to in the literature as non-previa accreta. Other surgical traumas to the integrity of the uterine endometrium and/or superficial myometrium, such as those following uterine curettage, postpartum endometritis, hysteroscopic surgery, endometrial ablation, and uterine artery embolization and myomectomy, have been associated with accreta placentation in subsequent pregnancies.11 With the increase in the CD rates worldwide, these cases have become proportionally rarer and have been overdiagnosed over the last two decades by including cases complicated by placental retention and uterine atony.17 The vast majority of patients with non-previa placenta accreta can be managed conservatively with partial myometrial resection, an intrauterine hydrostatic balloon, and/or uterine compressive or endouterine sutures, if required for secondary uterine atony.11
There is consensus that any unprotected vessels within 5 cm of the internal cervical os meet the definition of vasa previa and require CD.18 A LUS transverse uterine incision is appropriate in most cases. The LUS hysterotomy should be performed carefully in the midline, avoiding incising the membranes, and then extending the uterine incision laterally bluntly to expose the amniotic sac and the intact vessels.17
IMPACT OF PREVIOUS CESAREAN DELIVERY ON SURGICAL COMPLEXITY
Patients with a history of multiple CDs will often present with thick pelvic adhesions and an anterior LUS wall largely consisting of fibrotic scar tissue, which often develops into large cesarean scar defects (CSD).1 The risk of developing these complications is directly linked to the number of prior CDs. Even in the absence of PAS, placenta previa over a scarred, thinned or partially disrupted LUS, with dense adhesions between the LUS and posterior wall of the bladder, poses a surgical risk and necessitates careful dissection and surgical expertise (Table 1).
Pelvic adhesions
Adhesions are fibrous, band-like structures that form between two different anatomical surfaces, such as the ovaries, Fallopian tubes and uterus. They usually develop within the first few days to a week after an injury, with the tissue evolving from thin, flimsy structures to dense, thick bands over time.19 Previous abdominal and pelvic surgery, trauma, endometriosis and radiation therapy are the main causes of adhesions. Postsurgical pelvic adhesions, particularly in the vesicouterine pouch, are present in more than a third of patients with a history of one or two prior CDs.20 With each cumulative CD, adhesions increase in frequency, thicken and become denser, and involve larger areas.19 Postoperative wound infection increases the likelihood of adhesions in the anterior pelvic compartment, and there may be an association between skin scar thickness and the severity of pelvic and abdominal adhesions.
Thick and dense adhesions require extensive dissection, which, when combined with LUS dehiscence, bulging and hypervascularization in a patient presenting with an anterior placenta previa, constitute the most complex type of CD with or without part of the placenta being accreta (Table 1).
Post-surgical uterine scarring
Uterine remodeling is a complex process that involves healing, tissue regeneration and hormonal influences.21 Uterine remodeling after surgery, such as cesarean section or myomectomy, involves an initial 3–4 weeks of healing, with full tissue maturation (collagen reorganization) taking months to a year. This process mainly relies on the complex, extensive interactions between growth factors and cytokines, which coordinate the synthesis of various cell types.21 Poor healing of uterine scars after CD is a common complication that can lead to a permanent CSD. A large CSD is also the first step in the development of LUS dehiscence or disruption in subsequent pregnancies, regardless of placental position. Large dehiscences develop progressively as pregnancy advances and the uterus distends, leaving a thin layer of scarred myometrium covered with serosa at the end of the third trimester (Figure 2, Video 1).

2
Placenta previa accreta managed conservatively at 36 weeks of gestation. (A–D) Preoperative ultrasound assessment: (A) Longitudinal abdominal scan showing a placenta (P) previa covering the cervix with lacunae (*) and myometrial thinning of the LUS. (B) Transverse abdominal scan of the placenta showing lacunae (*). (C) Same as previous image but with color Doppler applied, showing the subplacental vascularization. (D) Transvaginal ultrasound showing the placenta (P) containing multiple lacunae covering the cervix (Cx). B, bladder. (E–G) Intraoperative views showing increased vascularization of the LUS before (E) and after (F) dissection and after partial myometrial resection (G) of the accreta dehiscent area and the dehiscent tissue.
1
Transvaginal scan with color Doppler showing the placenta covering the cervix with increased subplacental vascularity around the cervix. Note that the cervix is not involved in lower uterine segment remodeling, thereby facilitating conservative surgical management.
The main issue is the size of the dehiscence at CD in the subsequent pregnancy. Large dehiscences that occupy more than half of the LUS can progress to uterine rupture during labor contractions. Large dehiscences of the LUS after CD or the upper segment after myomectomy often necessitate a planned CD before the onset of labor to avoid the mechanical stress of contractions. During the cesarean section, the dehiscence is assessed and repaired, but if bleeding is uncontrollable or the scar tissue is too necrotic to repair, a hysterectomy is often required for hemostasis.22 The risk of hysterectomy increases in cases of placenta previa due to the associated risk of hemorrhage, particularly in cases of placenta previa accreta, even if the accretic area is small.
Increased vascularity at the placentation site
Placentation in the LUS is associated with physiological vascular changes that may increase morbidity in patients with a history of CD. During placentation, 30–60 spiral arteries are recruited into the placenta bed.23 The combined effects of conversion of their distal portion and dilatation of the whole uteroplacental circulation increase their visibility on imaging as pregnancy advances.24 In placenta previa, the changes in subplacental vasculature are more pronounced because the LUS is thinner (Figure 2 and Video 1).
ROLE OF PRENATAL IMAGING
Imaging has been an essential part of antenatal care for over 40 years and, in most middle- and high-income settings, pregnant patients have several ultrasound examinations throughout pregnancy. The mid-pregnancy detailed scan is performed routinely to screen for fetal anomalies and record the placental position. With increased awareness of an association between a prior CD and placenta previa accreta, patients at risk should also be screened for PAS.24 Prenatal identification of patients at high risk of PAS at birth reduces maternal hemorrhagic morbidity. Most studies have focused on individual imaging markers or on determining the sensitivity and specificity of antenatal screening for PAS. By contrast, few studies have gone a step further to evaluate the role of ultrasound and magnetic resonance imaging (MRI) in identifying imaging signs of anatomical changes that can impact the risk of intraoperative complications in subsequent CD (Table 2). Overall, imaging has been underused in the preoperative evaluation of surgical risk and can lead to an under- or overestimation of the risk of intraoperative difficulty.
2
Ultrasound signs associated with increased surgical risk in patients with a history of multiple cesarean deliveries. (Modified from Jauniaux et al.1)
| Ultrasound sign | Etiology | Surgical risk | |
(A) | Thin (≤ 2 mm) myometrium involving 3–4 cm of the LUS, with bulging of the fetal presenting part towards the bladder, but myometrial thinning located 2–3 cm from the cervix | LUS dehiscence | Difficult surgical dissection of the LUS. May require focal resection and repair of the LUS. |
(B) | Same as (A) with anterior low-lying placenta or placenta previa reaching or covering cervix. No signs of PAS. | Low-lying or placenta previa with LUS dehiscence | Bladder injury and uterine atony with PPH from the placental bed. May need multiple transfusions and/or placement of a compressive suture. |
(C) | Anterior placenta previa entirely inside the LUS with extended myometrial thinning (< 1 mm) and placental bulge toward the bladder and/or parametrium. No additional signs of PAS. | Placenta previa with extended LUS dehiscence | Bladder injury and intraoperative bleeding. May need emergency hysterectomy for hemostasis and/or inability to effectively reapproximate hysterotomy edge and repair. |
(D) | Same as (C) with increased uteroplacental, cervical, intraplacental (multiple lacunae) and pelvic vascularity. High probability of PAS. | Placenta previa accreta with extended LUS dehiscence and cervical involvement | High risk of bladder injury, massive hemorrhage and peripartum hysterectomy for hemostasis. |
LUS, lower uterine segment; PAS, placenta accreta spectrum; PPH, postpartum hemorrhage.
Anomalies of the uteroplacental interface and uterine contour
Patients with a history of multiple CDs presenting with a placenta previa often show major LUS remodeling and changes in the uteroplacental circulation.24,25 Abnormalities of the uterine contour, including the loss of the clear zone, myometrial thinning, bladder wall interruption and a placental bulge-like appearance on ultrasound, are commonly used in the antenatal evaluation of patients at risk of PAS.24 After multiple CDs, the myometrium of the LUS may appear excessively thin or even undetectable (Figure 2). Physiological thinning of the myometrium occurs with advancing gestation (particularly in the third trimester), independent of PAS, which can lead to false-positive diagnosis, particularly on MRI. Placental budge describes the ‘ballooning’ of the uterus caused by the protrusion of part of the placental tissue towards the pelvis, most commonly the bladder. Although the uterine serosa is always intact, the external contour of the uterus appears distorted. This finding is the consequence of a placental hernia through a dehiscence of the LUS with extended myometrial thinning.22,25 As this sign is often found in patients with a history of multiple CDs, there is also a high risk of thick adhesions between the hernia sac and the pelvic tissue, and bulging near the broad ligament or ureters may prompt preoperative measures such as ureteric stenting to mitigate intraoperative risk.26 This sign is associated with the highest risk of peripartum hysterectomy due to atony of the dehiscent LUS or lack of healthy myometrium needed to repair the dehiscent area after placental delivery or partial myometrial resection.
One could argue that there is no difference in the distribution of these signs between non-PAS previa and PAS previa subgroups because the sonographic findings are secondary to LUS scarring and remodeling rather than to accreta placentation, and therefore may not differentiate between difficult CD due to extended LUS scarring and PAS.22,26 There are currently no standardized ultrasound criteria for diagnosing and assessing the extent of LUS remodeling, and there are no prospective data on the role of MRI in evaluating the surgical complexity of a CD beyond associations with imaging findings associated with PAS.
Uteroplacental and intraplacental vascular changes and surgical complexity
Placentation in the LUS is associated with a marked increase in color Doppler imaging (CDI) signal under the placental bed (subplacental) and between the myometrium and the posterior bladder wall (Figure 2 and Video 1). These changes are more pronounced in PAS, but the definition of what constitutes subplacental or uterovesical ‘hypervascularity’ on imaging in the second half of pregnancy remains elusive.25 By contrast, placental lacunae are defined as numerous, large, irregular hypoechoic (without a hyperechogenic halo) intraplacental spaces that are well defined on imaging (ultrasound and MRI) and give the placenta a ‘moth-eaten’ appearance. These lacunae develop secondary to the distortion of the anatomy of one or more placental cotyledons, including the interlobular septa, due to high-velocity maternal blood coming directly inside the intervillous space from a radial or arcuate artery from the end of the first trimester of pregnancy.27
When combined with changes in the intervillous circulation, i.e. placental lacunae with large feeder vessels, these signs have been found to increase the odds of cesarean hysterectomy and massive transfusion,26 independently of the confirmation of the diagnosis of PAS at delivery. Small accretic areas can also affect the entire LUS circulation, the parametrial circulation, and existing arterial anastomoses with the bladder. The prenatal evaluation of the size and vascular mapping of the suspected accreta area may help the surgical team in planning the procedure, but there are currently no prospective data on this approach.
Cervix
Transvaginal sonography (TVS) is essential for evaluating LUS anatomy, assessing cervical length and accurately determining the position of the lower placental edge in a low-lying placenta and placenta previa. Changes in anatomy and vascularity on TVS have recently been associated with a higher risk of surgical complexity, including the need for hysterectomy for hemostasis, and should therefore be included in the preoperative ultrasound surgical planning evaluation.28,29,30 The need for hysterectomy is associated with myometrial thinning of the distal part of the LUS and increased cervical vascularity on TVS.28,29,30 However, the combination of cervical hypervascularity > 50% and bladder wall remodelling has the highest predictive probability for hysterectomy.28
Abdominopelvic adhesions and the sliding sign
Adhesions do not show up on standard imaging tests (ultrasound, MRI), so they are typically diagnosed during laparoscopy. However, a transabdominal sonographic sign has been described that could detect intra-abdominal adhesions in pregnant patients undergoing repeat CD.31,32 This sign evaluates the sliding of the uterus under the inner part of the rectus fascia during deep breathing, and its absence (sliding-negative) predicts severe intra-abdominal adhesions. This sign was recently validated in a prospective study showing that it provides a reliable, non-invasive method of predicting intra-abdominal adhesions prior to repeat CD and is particularly useful for excluding severe adhesions.33
SURGICAL TIPS FOR COMPLEX CESAREAN SECTION
Although it is impossible to anticipate or describe every situation that may increase the technical difficulty of a cesarean section, certain conditions are consistently associated with greater surgical complexity. Among the most frequent are dense peritoneal adhesions, distortion or remodeling of the LUS secondary to previous uterine surgery, and obstetric conditions associated with a high risk of postpartum hemorrhage. These situations require a structured surgical approach that prioritizes safe entry into the pelvic cavity, careful identification and mobilization of the bladder (which may be abnormally attached to higher planes of the abdominal wall), and appropriate exposure of the anterior surface of the LUS.34,35,36,37 Once adequate exposure is achieved, management of the scarred area should be guided by the vascular anatomy of the uterus. From a practical perspective, uterine blood supply can be divided into two main surgical sectors (Figure 3): Sector 1, corresponding to the uterine body and fundus, which is mainly supplied by the uterine and ovarian arteries; and Sector 2, which includes the LUS and cervix, and is predominantly supplied by the colpouterine arterial system.37 Understanding these vascular territories allows the surgeon to select targeted hemostatic strategies according to the anatomical source of bleeding.

3
Diagram of uterine vascularization sectors. The uterus has two main vascular territories. The uterine body and fundus are supplied by the uterine (uA) and ovarian (oA) arteries, corresponding to Sector 1 (S1). The lower uterine segment and cervix are supplied by the colpouterine arteries (asterisks), which arise from the inferior vaginal arteries (iVA); this region corresponds to Sector 2 (S2). The colpouterine artery located in the midline is also known as the azygos vaginal artery (azA). Sector 2 lies below the vesicouterine peritoneal reflection and is therefore covered by the bladder. Access to this sector requires bladder mobilization. (Modified from Nieto-Calvache AJ, et al. Int J Gynaecol Obstet. 2025;168(3):987–998.37 )
Safe access to the pelvis in patients with bladder adhesions to the abdominal wall
When dense adhesions are suspected between the bladder and the anterior abdominal wall, conventional midline entry may place the urinary tract at significant risk of injury.38 In these cases, a paramedian approach using a preperitoneal plane can provide safer access to the pelvis (Figure 4). After a transverse suprapubic skin incision and exposure of the rectus sheath, the rectus muscles are retracted and a dissection plane is developed behind them, progressing laterally between the muscle and the peritoneum until tissue free of fibrosis is identified. Because postoperative adhesions tend to concentrate in the midline with variable lateral extension, this strategy allows the surgeon to approach the pelvic cavity from a less scarred region. Once a lateral plane is established, the fibrotic block, which may include the bladder or other structures adherent to the abdominal wall, can be progressively separated under direct visualization before opening the peritoneal cavity. This stepwise dissection releases the bladder dome from the abdominal wall and significantly reduces the risk of inadvertent bladder injury during abdominal entry.

4
Paramedian access to the pelvis. In cases of dense adhesions between the bladder and the anterior abdominal wall, preperitoneal dissection (behind the rectus abdominis muscle) toward a lateral (paramedian) area free of adhesions (A) facilitates identification of a thin segment of peritoneum without adhesions, which can be used as an entry point to the peritoneal cavity. This approach then allows the surgeon to guide the required dissection (B) and mobilize the bladder together with the adherent tissue (C), thereby reducing the risk of bladder injury. (Modified from Nieto-Calvache AJ, et al. Int J Gynaecol Obstet. 2025;168(3):987–998.37)
Dissection of the retrovesical space and bladder mobilization
Exposure of the anterior surface of the LUS requires adequate mobilization of the bladder. In complex cesarean sections, adhesions between the bladder and the uterus frequently occur in the midline; therefore, approaching the dissection through lateral avascular spaces is usually safer. Access to the medial paravesical space can be obtained by gentle traction of the round ligament and incision of the anterior leaf of the broad ligament, followed by digital opening of the parametrial plane. From this lateral entry point, the surgeon may advance medially toward the retrovesical space using blunt or sharp dissection.39 Additional maneuvers, such as the retrovesical bypass technique40 or traction of the bladder in an anterocaudal direction, facilitate identification of the vesicouterine plane and allow controlled separation of the bladder from the LUS. Complete bladder mobilization not only decreases the risk of urinary tract injury but also provides the exposure required to perform procedures on the LUS, including vascular ligation, compressive sutures, fibroid removal or resection of abnormal tissue (e.g. dehiscent LUS, focal accreta). However, complete bladder dissection before fetal extraction sometimes is not feasible with major LUS remodeling and dense adhesion, and may lead to massive bleeding; thus, it is advisable, in some cases, to perform fetal extraction and then continue bladder dissection afterwards.
Hemostatic strategies for different uterine sectors
Effective control of bleeding during a complex cesarean section depends on recognizing the vascular territory involved (Figure 3). Hemorrhage arising from Sector 1 (the uterine body and fundus) is usually related to uterine atony and can often be controlled through interventions that either reduce blood flow through the uterine arteries or compress the myometrium. Techniques such as uterine artery ligation, uterine compression sutures (Figure 5) or intrauterine tamponade (balloon or suction) are particularly effective in this territory because the principal arterial inflow originates from the uterine arteries with collateral contribution from the ovarian circulation. In contrast, bleeding from Sector 2, which includes the LUS and cervix, presents greater technical challenges.41,42 This region is supplied predominantly by the colpouterine arteries arising from vaginal vessels (branches from the posterior division of internal iliac artery), located in a subperitoneal position. Consequently, adequate bladder mobilization is essential before attempting hemostatic procedures in this area. Once exposure is achieved, targeted techniques such as LUS compression sutures (e.g. Ho-Cho or transverse B-Lynch) or selective vascular control of the lower uterine pedicles can be applied to achieve hemostasis in conditions such as placenta previa, fibroids near the cervix or PAS.34

5
Uterine compression sutures. Multiple techniques have been described to compress the uterus with sutures; however, topographic assessment of bleeding in zones S1 (uterine body and fundus) and S2 (lower uterine segment and cervix) facilitates selection of the most appropriate technique based on the bleeding site. (A) Sutures designed to compress the uterine body and fundus, such as the B-Lynch suture, are useful in cases of uterine atony and other causes of bleeding originating in the S1 sector. (B) Sutures aimed at compressing the lower uterine segment, such as the transverse B-Lynch suture, are effective for controlling bleeding associated with placenta previa. For both types of suture, uterine dissection and mobilization are essential. (Modified from Nieto-Calvache et al. Int J Gynaecol Obstet. 2024 Aug;166(2):902–904.41)
Primary and secondary hemostatic strategies in complex cesarean delivery
During abnormal intracesarean bleeding, the immediate priority is to stop the hemorrhage (primary hemostasis) while preparing and executing a definitive strategy to control blood loss (secondary hemostasis). In many cases, definitive procedures (such as vascular ligation, compression sutures, balloon tamponade or hysterectomy) require time, surgical expertise and specific resources, which may challenge inexperienced obstetricians, and even experienced surgeons, under conditions of severe bleeding. For this reason, we propose an initial approach based on rapid temporary control maneuvers. Techniques such as internal manual compression of the aorta (Figure 6, Video 2) or the application of a uterine tourniquet (Figure 7) can be implemented immediately and without specialized equipment, providing prompt reduction of pelvic blood flow.43,44 Although these interventions do not resolve the underlying cause of hemorrhage, they effectively limit ongoing blood loss and help prevent the physiological consequences of massive bleeding, including coagulopathy and metabolic deterioration.
|
|
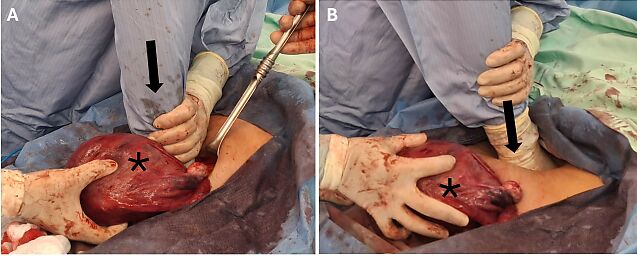

6
Surgical photographs (A,B) and diagrams (C), showing manual compression of the aorta. In cases of profuse pelvic hemorrhage, manual compression of the aorta, either internal (A) or external (B), is effective for temporarily controlling bleeding. The exteriorized uterus (asterisk) rests over the pubis, while one of the surgeons applies downward pressure using body weight, with the arm fully extended (arrow) at a 90° angle to the horizontal plane, compressing the aorta against the vertebral bodies either by inserting the hand into the abdomen (A) or by applying pressure over the umbilicus (B). (Diagrams kindly provided by Sreeharini Murali/ArtiniStudio.)
2
Internal manual aortic compression.

7
Uterine tourniquet. After exteriorization of the uterus, in cases of profuse uterine bleeding, and ideally after mobilization of the bladder, a sterile latex glove may be used as a tourniquet by placing it circumferentially (arrow) around the lower uterine segment (LUS) or cervix, caudal to the bleeding site, while the assistant applies traction upward on the uterus toward the operating room ceiling. UUS, upper uterine segment.
Once temporary control of bleeding has been achieved (primary hemostasis), the obstetrician gains critical time to organize the surgical environment: requesting assistance, preparing additional supplies and selecting the most appropriate definitive intervention. A relatively bloodless surgical field and a less stressful operative context facilitate the safe, controlled execution of more complex procedures aimed at achieving definitive control of bleeding (secondary hemostasis). In this staged approach, temporary vascular control acts as a bridge that stabilizes the patient and transforms an uncontrolled hemorrhagic emergency into a manageable surgical situation.
Hysterectomy vs uterine-sparing surgery in PAS and placenta previa with major uterine remodeling
The choice of surgical plan will depend on multiple factors, including surgical expertise, complexity of the case and availability of resources.45 Numerous surgical techniques have been described, including variations in the type of skin incision, 46,47,48,49 with no clear consensus. These include:
- Primary hysterectomy following delivery of the fetus through a hysterotomy above the placental implantation site, without attempting placental separation.
- Delivery of the fetus through a hysterotomy above the area of abnormal placentation, followed by partial excision of the accreta area (partial myometrial resection) and uterine repair.
- Delivery of the fetus without disturbing the placenta, leaving it in situ, followed by planned hysterectomy 3–7 days later.
- Delivery of the fetus through an incision above the placental implantation site, leaving the placenta in situ, followed by expectant management.
As there are no well-controlled prospective studies stratified by pre- and intraoperative features, the choice of surgical technique is left to the operator's judgment.50
In planned cesarean hysterectomy, fetal extraction should be performed through a vertical or transverse uterine incision away from the placenta (Video 3). The uterine incision is then closed with sutures or towel clips, leaving the placenta in situ. The round ligaments are subsequently clamped, cut and ligated at the junction between the lateral third and medial two-thirds to facilitate access to the pelvic floor, followed by clamping and ligation of the ovarian ligaments bilaterally (Table 3 and Video 4). Dissection of the posterior fold of the broad ligament downward to below the level of the placenta facilitates mobilization of the ureter and reduces the risk of ureteric injury. Bladder dissection is then continued from lateral to medial, if not completed prior to fetal extraction. After identifying the lower edge of the placenta, the vascular pedicles are clamped on both sides of the uterus below this level. The uterus is then removed and the vascular pedicles ligated, followed by stump closure (Figure 8). In more severe cases, total hysterectomy may be required; however, the main aim is to minimize dissection in order to avoid extensive pelvic hemorrhage and reduce maternal morbidity and mortality.
In cases of uterine-sparing surgery, creating a bladder flap to expose the affected LUS and the uterine incision over the lower segment is recommended, as it facilitates hemostasis, enables precise focal resection of the affected area and allows optimal reconstruction (Figure 9).
3
Uterine incision above placenta.
3
Methodological steps involved in the surgical procedures of planned cesarean hysterectomy and partial myometrial resection.
Planned cesarean hysterectomy
|
Partial myometrial resection
|
LUS, lower uterine segment.

8
Cesarean hysterectomy. (A,B) Following a subumbilical midline skin incision and adhesiolysis, the lower uterine segment (LUS) is exposed. (C,D) The round ligaments are clamped, cut and ligated at the junction between the lateral third and medial two-thirds to facilitate access to the whole pelvic floor, then the ovarian ligaments are clamped, cut and ligated bilaterally. (E) Removal of the uterus. (F) Closure of the stump.

9
Partial myometrial resection. (A) A transverse or vertical skin incision is performed, according to preoperative ultrasound mapping, at or slightly below the upper edge of the diseased segment to allow for adequate control of bleeding from the placental bed and facilitate reconstruction. (B) The lower uterine segment (LUS) is exposed with progressive ligation of vessels within the LUS. (C) The placenta and membranes are gently peeled from the uterine wall, starting posteriorly and proceeding towards the most adherent part. (D,E)
Focal myometrial resection is performed to remove the adherent placenta together with the underlying myometrium. (F) Closure of the uterine incision.
4
Preoperative ultrasound imaging, and surgical planning and management of a case of cesarean hysterectomy for placenta accreta spectrum. (Video produced by Medical Aid Films.)
PRACTICE RECOMMENDATIONS
- Surgical complexity in cesarean delivery (CD) is multifactorial, driven by maternal comorbidities, prior uterine surgery, fetal conditions and abnormalities of placentation.
- Placenta previa and placenta accreta spectrum (PAS) represent the highest-risk scenarios, often requiring multidisciplinary team management and advanced surgical planning.
- Maternal obesity significantly increases surgical difficulty, affecting access, anesthesia, operative time and postoperative complications.
- A history of multiple CDs increases the risk of adhesions, lower uterine segment (LUS) remodeling, and cesarean scar defects, all of which contribute to intraoperative complexity.
- Dense pelvic adhesions and bladder involvement increase the risk of urinary tract injury, necessitating careful dissection and alternative surgical entry techniques.
- Prenatal imaging (particularly ultrasound) is essential for risk stratification, surgical planning and reducing hemorrhagic morbidity, especially in suspected PAS.
- Imaging findings, such as myometrial thinning, placental bulge, lacunae and hypervascularity, are associated with increased surgical risk, including hysterectomy and massive transfusion.
- Understanding uterine vascular anatomy (Sectors 1 and 2 ) is critical for targeted hemostatic strategies, particularly in cases of placenta previa and PAS.
- Initial management of intraoperative hemorrhage should focus on rapid temporary control (primary hemostasis), such as aortic compression or uterine tourniquet, before definitive surgical treatment.
- Definitive hemostatic strategies (secondary hemostasis) include vascular ligation, compression sutures, intrauterine tamponade or hysterectomy, depending on the source and severity of bleeding.
- In PAS and major LUS remodeling, minimizing unnecessary dissection is key to reducing blood loss, morbidity and the risk of catastrophic hemorrhage.
- The choice between hysterectomy and uterine-sparing surgery remains individualized, depending on surgical expertise, intraoperative findings and available resources, as no consensus approach exists.
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Jauniaux E, Fox KA, Einerson B, Hussein AM, Hecht JL, Silver RM. Perinatal assessment of complex cesarean delivery: beyond placenta accreta spectrum. Am J Obstet Gynecol. 2023 Aug;229(2):129–139. | |
Jauniaux E, Bartels HC, Nieto-Calvache AJ, Hussein AM. Evolution of modern cesarean delivery: historic perspective and new challenges. Am J Obstet Gynecol. 2026;233(6S):S557–S568. | |
Wilson RD, Monks DT, Sharawi N, Bamber J, Panelli DM, Sauro KM, et al. Guidelines for antenatal and preoperative care in cesarean delivery: Enhanced Recovery After Surgery Society recommendations (part 1)-2025 update. Am J Obstet Gynecol. 2026;233(6S):S153–S169. | |
Gerede A, Danavasi M, Stavros S, Potiris A, Zikopoulos A, Moustakli E, et al. Obesity and pregnancy: Impact on childbirth timing, delivery mode, and maternal recovery: An update. Med Sci (Basel). 2025;13(3):182. | |
Dominguez JE, Taylor CR, Girard T.Morbid obesity: Optimizing neuraxial analgesia and cesarean delivery outcomes. Best Pract Res Clin Anaesthesiol. 2024;38(3):257–266. | |
ACOG Committee Opinion No. 751 Summary: Labor and Delivery Management of Women With Human Immunodeficiency Virus Infection. Obstet Gynecol. 2018 Sep;132(3):803–804. | |
Jauniaux E, Berghella V. The modern caesarean section. Textbook of caesarean section. Eds: Jauniaux E, Grobman W. Oxford University Press. Oxford. 49–68, 2016. | |
Berghella V, Mackeen AD, Jauniaux E. Cesarean Delivery. In: Obstetrics: Normal and Problem Pregnancies 8th Eds: Landon M, Galan H, Jauniaux ERM, Driscoll DA, Berghella V, Grobman WA, Kilpatrick SJ, Cahill AG. Elsevier, Philadelphia. 375–394, 2020. | |
Murakoshi T."En Caul" Cesarean Delivery for Extremely Premature Fetuses: Surgical Technique and Anesthetic Options. Surg J (N Y). 2020;6(Suppl 2):S104–S109. | |
Allen L, Jauniaux E, Hobson S, Papillon-Smith J, Belfort MA; FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Nonconservative surgical management. Int J Gynaecol Obstet. 2018;140(3):281–290. | |
Jauniaux E, Alfirevic Z, Bhide AG, Belfort MA, Burton GJ, Collins SL, et al.; for the Royal College of Obstetricians and Gynaecologists. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. 2019;126(1):e1–e48. | |
Oyelese Y, Shainker SA. Placenta Previa. Clin Obstet Gynecol. 2025;68(1):86–92. | |
Fox KA, Nieto-Calvache AJ, Aryananda RA, Hussein AM, Morel O, Hobson SR. Surgical management of complex cesarean delivery. Am J Obstet Gynecol. 2026 Jan;233(6S):S226–S254. | |
Nieto-Calvache AJ, Ramasauskaite D, Palacios-Jaraquemada JM, Hussein AM, Jauniaux E, Ubom AEB, Rivera-Torres LF, Nunes I, Schlembach D, Beyeza-Kashesya J, Wright A; FIGO Committee on Childbirth and PPH. Complex cesarean section: Surgical approach to reduce the risks of intraoperative complications and postpartum hemorrhage. Int J Gynaecol Obstet. 2025 Mar;168(3):987–998. | |
Nieto-Calvache AJ, Benavides-Calvache JP, Aryananda R, Palacios-Jaraquemada JM, Jauniaux E, Fox KA, et al. Telemedicine ultrasound assessment for placenta accreta spectrum: Utility and interobserver reliability of asynchronous remote imaging review. Int J Gynaecol Obstet. 2025;168(3):1191–1203. | |
Jauniaux E, Nieto-Calvache AJ, Hussein AM. Preoperative ultrasound assessment for surgical risk management in patients with a placenta previa and a history of cesarean delivery. Am J Obstet Gynecol. 2026 ;233(6S):S641–S644. | |
Jauniaux E, Einerson BD, Hussein AM, Silver RM, Burton GJ. What is placenta accreta? Am J Obstet Gynecol. 2026;233(6S):S630–S640. | |
Oyelese Y, Javinani A, Shamshirsaz AA. Vasa Previa. Obstet Gynecol. 2023;142(3):503–518. | |
Lyell DJ. Adhesions and perioperative complications of repeat cesarean Am J Obstet Gynecol. 2011;205S11–8. | |
Moro F, Mavrelos D, Pateman K, Holland T, Hoo WL, Jurkovic D. Prevalence of pelvic adhesions on ultrasound examination in women with a history of Cesarean section. Ultrasound Obstet Gynecol. 2015;45:223–228. | |
Sun Q, Tang L, Zhang. Molecular mechanisms of uterine incision healing and scar formation. Eur J Med Res. 2023 Nov 8;28(1):496. | |
Hussein AM, Elbarmelgy RA, Elbarmelgy RM, Thabet MM, Jauniaux E. Prospective evaluation of impact of post-Cesarean section uterine scarring in perinatal diagnosis of placenta accreta spectrum disorder. Ultrasound Obstet Gynecol. 2022;59:474–482. doi: 10.1002/uog.23732. | |
Burton GJ, Jauniaux E. Placentation in the Human and Higher Primates. Adv Anat Embryol Cell Biol. 2021;234:223–254. | |
Shainker SA, Coleman B, Timor-Tritsch IE, Bhide A, Bromley B, Cahill AG, et al. Special Report of the Society for Maternal-Fetal Medicine Placenta Accreta Spectrum Ultrasound Marker Task Force: Consensus on definition of markers and approach to the ultrasound examination in pregnancies at risk for placenta accreta spectrum. Am J Obstet Gynecol. 2021 Jan;224(1):B2–14. | |
Jauniaux E, D'Antonio F, Bhide A, et al. Modified Delphi study of ultrasound signs associated with placenta accreta spectrum. Ultrasound Obstet Gynecol. 2023;61(4):518–525. | |
Hussein AM, Fox K, Bhide A, et al. The impact of preoperative ultrasound and intraoperative findings on surgical outcomes in patients at high risk of placenta accreta spectrum. BJOG. 2023;130(1):42–50. | |
Jauniaux E, Zosmer N, De Braud LV, Ashoor G, Ross J, Jurkovic D. Development of the utero-placental circulation in cesarean scar pregnancies: a case-control study. Am J Obstet Gynecol. 2022 Mar;226(3):399.e1–399.e10. | |
Jauniaux E, Hussein AM, Thabet MM, Elbarmelgy RM, Elbarmelgy RA, Jurkovic D. The role of transvaginal ultrasound in the third-trimester evaluation of patients at high risk of placenta accreta spectrum at birth. Am J Obstet Gynecol. 2023;229(4):445.e1–445.e11. | |
Aryananda RA, Duvekot H, Dall'Asta A, Lees CC. Transvaginal ultrasound imaging of intracervical hypervascularity grading correlates with maternal outcome in placenta accreta spectrum. Ultrasound Obstet Gynecol. 2024;64(5):705–707. doi: 10.1002/uog.27670. | |
Aryananda RA, Adu-Bredu TK, Cininta NI, Twumasi C, Pranpanus S, Coutinho CM, et al. Diagnostic ultrasound to inform the surgical approach to cesarean delivery in patients at high risk for placenta accreta spectrum disorders. Am J Obstet Gynecol. 2025 Dec;233(6):658.e1–658.e16. | |
Baron J, Tirosh D, Mastrolia SA, et al. Sliding sign in third-trimester sonographic evaluation of intra-abdominal adhesions in women undergoing repeat Cesarean section: a novel technique. Ultrasound Obstet Gynecol. 2018;52:662–665. | |
Drukker L, Sela HY, Reichman O, Rabinowitz R, Samueloff A, Shen O.Sliding Sign for intra-abdominal adhesion prediction before repeat cesarean delivery. Obstet Gynecol. 2018;131:529–533. | |
Vo HL, Le LH, Nguyen MP, Nguyen TTN, Le MT, Nguyen VQH. Transabdominal ultrasound sliding sign for predicting intra-abdominal adhesions in repeat cesarean delivery: a prospective observational study from Vietnam. AJOG Glob Rep. 2025;6(1):100598. | |
Palacios-Jaraquemada JM, Nieto-Calvache Á, Basanta NA. Anatomical basis for the uterine vascular control: implications in training, knowledge, and outcomes. Am J Obstet Gynecol MFM. 2023;5(7):100953. | |
Nieto-Calvache ÁJ, Aryananda RA, Palacios-Jaraquemada JM, Cininta N, Grace A, Benavides-Calvache JP, Campos CI, Messa-Bryon A, Vallecilla L, Sarria D, Galindo JS, Galindo-Velasco V, Rivera-Torres LF, Burgos-Luna JM, Bhide A. One-step conservative surgery vs hysterectomy for placenta accreta spectrum: a feasibility randomized controlled trial. Am J Obstet Gynecol MFM. 2024;6(6):101333. | |
Palacios-Jaraquemada JM, Fiorillo A, Hamer J, Martínez M, Bruno C. Placenta accreta spectrum: a hysterectomy can be prevented in almost 80% of cases using a resective-reconstructive technique. J Matern Fetal Neonatal Med. 2022;35(2):275–282. | |
Nieto-Calvache AJ, Ramasauskaite D, Palacios-Jaraquemada JM, Hussein AM, Jauniaux E, Ubom AEB, Rivera-Torres LF, Nunes I, Schlembach D, Beyeza-Kashesya J, Wright A; FIGO Committee on Childbirth and PPH. Complex cesarean section: Surgical approach to reduce the risks of intraoperative complications and postpartum hemorrhage. Int J Gynaecol Obstet. 2025;168(3):987–998. | |
Nieto-Calvache AJ, Basanta N, Hussein AM, Rivera-Torres LF, Palacios-Jaraquemada JM. Paramedian access to the pelvis as a strategy in patients with bladder adhesions to the abdominal wall. Int J Gynaecol Obstet. 2025;168(1):402–403. | |
Nieto-Calvache AJ, Ramasauskaite D, Palacios-Jaraquemada JM, Hussein AM, Jauniaux E, Ubom AEB, Rivera-Torres LF, Nunes I, Schlembach D, Beyeza-Kashesya J, Wright A; FIGO Committee on Childbirth and PPH. Complex cesarean section: Surgical approach to reduce the risks of intraoperative complications and postpartum hemorrhage. Int J Gynaecol Obstet. 2025;168(3):987–998. | |
Pelosi MA 3rd, Pelosi MA. Modified cesarean hysterectomy for placenta previa percreta with bladder invasion: retrovesical lower uterine segment bypass. Obstet Gynecol. 1999;93(5 Pt 2):830–833. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Sarria-Ortiz D, Galindo-Velasco V, Basanta N. How to choose and apply a uterine compression suture for the management of postpartum hemorrhage? Int J Gynaecol Obstet. 2024 Aug;166(2):902–904. | |
Palacios-Jaraquemada JM. Efficacy of surgical techniques to control obstetric hemorrhage: analysis of 539 cases. Acta Obstet Gynecol Scand. 2011;90(9):1036–1042. | |
Nieto-Calvache AJ, Palacios Jaraquemada JM, Basanta N, Aryananda RA, Sinisterra-Díaz SE, Rodriguez F, Hidalgo Cardona A, Messa Bryon A. Internal manual compression of the aorta-an effective way to temporarily control pelvic bleeding in obstetrical hemorrhage. Am J Obstet Gynecol. 2022;227(1):96–97. | |
Nieto-Calvache AJ, Barona JS, Burgos-Luna JM, Muñoz-Córdoba L, Sarria-Ortiz D, Galindo-Velasco V, Meade Triviño P, Mondragón K, Messa-Byron A. The uterine tourniquet, a simple maneuver that may facilitate surgical management of postpartum hemorrhage. Int J Gynaecol Obstet. 2024;164(1):345–347. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Hussein AM, Jauniaux E, Milani Coutinho C, Rijken M. Management of placenta accreta spectrum in low- and middle-income countries. Best Pract Res Clin Obstet Gynaecol. 2024;94:102475. | |
Hussein AM, Kamel A, Raslan A, Dakhly DMR, Abdelhafeez A, Nabil M, Momtaz M. Modified cesarean hysterectomy technique for management of cases of placenta increta and percreta at a tertiary referral hospital in Egypt. Arch Gynecol Obstet. 2019;299(3):695–702. | |
Jauniaux E, Hussein AM, Fox KA, Collins SL. New evidence-based diagnostic and management strategies for placenta accreta spectrum disorders. Best Pract Res Clin Obstet Gynaecol. 2019;61:75–. | |
Allen L, Jauniaux E, Hobson S, Papillon-Smith J, Belfort MA; FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: Nonconservative surgical management. Int J Gynaecol Obstet. 2018;140:281–290. | |
Khoury-Collado F, Newton JM, Brook OR, Carusi DA, Shrivastava VK, Crosland BA, et al. Pan-American Society for Placenta Accreta Spectrum. Surgical techniques for the management of placenta accreta spectrum. Am J Perinatol. 2023;40:970–. | |
Jauniaux E, Alfirevic Z, Bhide AG, Belfort MA, Burton GJ, Collins SL, Dornan S, Jurkovic D, Kayem G, Kingdom J, Silver R, Sentilhes L; Royal College of Obstetricians and Gynaecologists. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. 2019;126(1):e1–e48. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)