This chapter should be cited as follows:
Palacios-Jaraquemada JM, Calvache AJN, et al., Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.422203
The Continuous Textbook of Women’s Medicine Series – Obstetrics Module
Volume 20
Surgical Techniques in Obstetrics
Volume Editors:
Professor Michael Stark, New European Surgical Academy (NESA) and Charité University Hospital, Berlin, Germany
Professor Sergej Barinov, Omsk State Medical University, Ministry of Health of Russia
Professor Gian Carlo Di Renzo, PREIS International School, Florence, Italy
Chapter
Individualized Management of Placenta Accreta Spectrum According to Lesion Topography
First published: July 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Placenta accreta spectrum (PAS) refers to abnormal placental adherence or involvement resulting from defective decidualization at the maternal–fetal interface, most commonly over a uterine scar (Figure 1). Traditionally, the disorder has been classified histologically into placenta accreta, increta and percreta, reflecting increasing depth of villous involvement into or beyond the myometrium.1,2,3,4,5,6,7 Although this classification retains pathological relevance, it has limited practical value for intraoperative decision-making.

1
Surgical view of the anteroinferior aspect of a uterus affected by placenta accreta spectrum. Note the placental protrusion through the uterine defect, with numerous vessels visible on its surface. (Image courtesy of Dr Eduardo García, Hospital General de Zona #18 del IMSS Torreón Coahuila, México.)
PAS should be understood as a spectrum disorder: different areas of the same placenta may show variable degrees of villous attachment or penetration, and these findings do not necessarily define the therapeutic strategy. Management is better guided by the clinical context, topographic anatomy, and expected morbidity than by an attempt to match imaging signs with histological depth. Histological grading is inherently retrospective, and because of the placenta's large size and tissue heterogeneity, sampling may introduce significant variability. For these reasons, histology in PAS should not be treated as a gold-standard guide for clinical management.
The epidemiology of PAS has changed dramatically over the past three decades, driven primarily by rising cesarean delivery rates and other uterine procedures that disrupt the endomyometrial interface.8,9,10,11 More than 90% of clinically significant PAS cases occur in women with a previous cesarean delivery and either a low-lying placenta or placenta previa.7,10,12,13,14
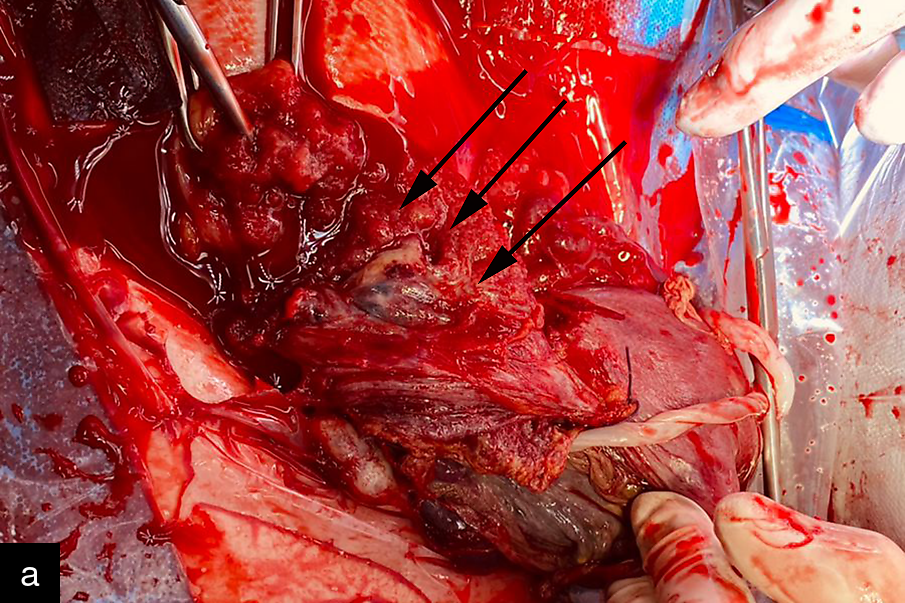
For many years, cesarean hysterectomy with the placenta left in situ was regarded as the safest management option for severe PAS, since attempted placental removal frequently leads to massive hemorrhage.15,16,17,18 Although this approach remains appropriate in many situations, it leads to permanent loss of fertility and is associated with substantial maternal morbidity, including risks for major transfusion, urinary tract injury (Figure 2) and intensive care admission.17,18,19,20

2
Surgical view showing a ureteral injury at the base of the parametrium during dissection for placenta accreta spectrum. The arrow shows the distal portion of the ureter after transection. Although several texts recommend double-J ureteral stents, these stents are soft and may be less easily identified by palpation than a simple, more rigid ureteral catheter.
A more nuanced surgical perspective has emerged over the past two decades. Evidence increasingly shows that histological depth alone does not adequately predict operative difficulty. Instead, the anatomical location of the lesion, its relation to the vesicouterine peritoneal fold, parametrial extension, fibrosis and neovascularization are the variables that most directly determine technical challenge and hemorrhagic risk.21,22,23,24,25,26 This shift has led to individualized management strategies built on lesion topography and intraoperative surgical staging.23,24,25,26,27,28
EPIDEMIOLOGY AND RISK FACTORS
The reported incidence of PAS in the general obstetric population varies with case definition and population risk profile, with estimates commonly ranging from 1 in 500 to 1 in 2000 pregnancies.8,9,29 The risk rises sharply when placenta previa and previous cesarean delivery coexist.29,30 In women with placenta previa and multiple prior cesareans, the probability of PAS may exceed 40%.29
The two strongest risk factors are prior cesarean delivery and placenta previa. Additional contributors include uterine surgery other than cesarean, repeat dilation and curettage, uterine instrumentation, advanced maternal age, multiparity and assisted reproductive technologies.8,29,30,31,32,33 The cumulative effect of repeated uterine injury appears central to disease development.
These observations are clinically important because they allow targeted screening in high-risk populations. A history of cesarean delivery combined with low placental implantation should prompt detailed imaging and referral to a PAS-experienced center.9,10,34
PATHOPHYSIOLOGY
The older concept of PAS as a disease of excessive trophoblastic invasion has been progressively revised. Current evidence supports a primary uterine defect model in which abnormal placental implantation occurs over areas of scarred (Figure 3), poorly decidualized or structurally deficient myometrium.11,35,36,37 In this model, the placenta does not behave as a biologically aggressive lesion; rather, it implants where the normal decidual barrier is absent or incomplete.

3
Resection of a defective hysterotomy after cesarean delivery. In many cases, the defect is located in the retrovesical area and is not evident at first inspection. In this case, the defect was identified by transvaginal ultrasound. (Image courtesy of Dr Miguel Huespe, Hospital Santojanni, Ciudad Autónoma de Buenos Aires, Argentina.)
Histologically, PAS remains classified as accreta, increta or percreta based on the depth of villous involvement.4,6 This classification retains pathological value but correlates imperfectly with the intraoperative situation.22,23,26 The same histological category may carry very different operative risks depending on whether the lesion lies above or below the peritoneal reflection, whether it involves the low retrovesical space, or whether it extends laterally into the parametrium.23,24,25,26,38 Both locations can sometimes coexist, a pattern known as synchronous PAS (Figure 4).

4
Synchronous placenta accreta spectrum (PAS). Intraoperative view of the lower uterine segment and anterior placenta (AP). Magnetic resonance imaging showed anterior PAS with minimal lateral extension, but the obstetrician dismissed this diagnosis. During placental removal, a massive hemorrhage occurred and was controlled by internal aortic compression. Opening the anterior leaf of the broad ligament is useful for diagnosing this uncommon location, which is strongly associated with maternal death due to hemorrhage.
The distinction is fundamental: pathology defines disease, whereas topography guides surgical management, strategy and technique. Specific areas of involvement have distinct vascular pedicles and anatomical characteristics, including the depth of invasion and proximity to critical structures such as the ureter, which determine the need for selective vascular control and tailored surgical approaches.39
WHY LESION TOPOGRAPHY MATTERS
Topographic assessment has become one of the most useful concepts in contemporary PAS surgery. Lesions differ substantially in bleeding risk and technical complexity depending on their location and relationship to surrounding structures.21,22,23,24,25,26 Upper segment lesions generally involve less complex vascular anatomy and are often more amenable to conservative surgery. By contrast, lesions located in the lower uterine segment, below the vesicouterine peritoneal fold, are more frequently associated with dense fibrosis, aberrant neovascularization, bladder distortion and difficult dissection.23,25,26,39
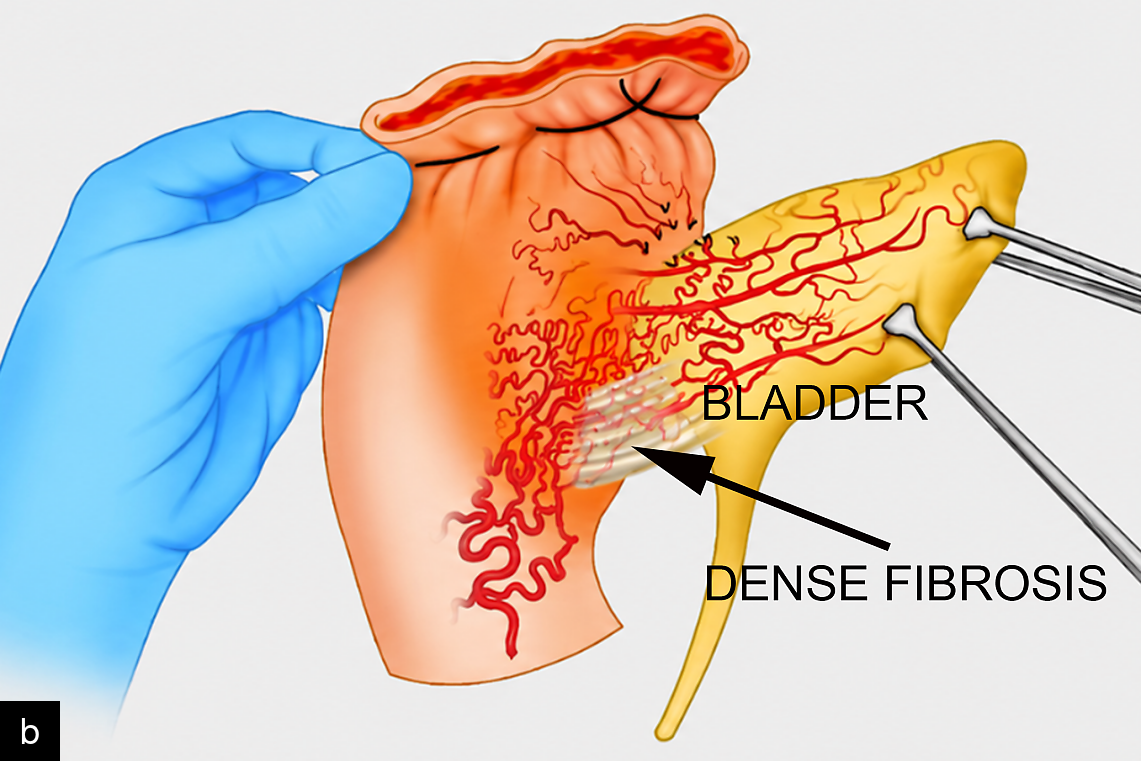
Retrovesical involvement increases the risk of bladder injury. However, lower retrovesical attachment associated with fibrosis also carries a significant risk of massive hemorrhage (Figure 5). In this region, an anastomotic vascular ring connects the vesical, vaginal and uterine arteries. Traumatic disruption of this network during dissection can produce severe and difficult-to-control bleeding, making accurate recognition of this anatomical location essential. Parametrial involvement is particularly challenging because it places major pelvic vessels (Figures 6) and ureters at risk.25,26 Among parametrial lesions, lower lateral extensions are associated with greater morbidity and mortality than upper ones.26 Posterior PAS is less common but may involve the rectum or uterosacral ligaments and can be missed if imaging is incomplete.9,22,25,40,41

5
Surgical view of the vesicouterine interface (arrows). Dense fibrotic adhesion is observed between the bladder trigone and the lower uterine segment. The patient had undergone a previous trachelectomy for cervical cancer and became pregnant 3 months after a failed laparoscopic tubal ligation. The placenta was completely previa, and dissection to complete a conventional hysterectomy was not technically feasible. A modified subtotal hysterectomy was performed, with uterine transection under aortic compression and folding of the posterior uterine wall over the anterior wall as a hemostatic patch.
|
|
6
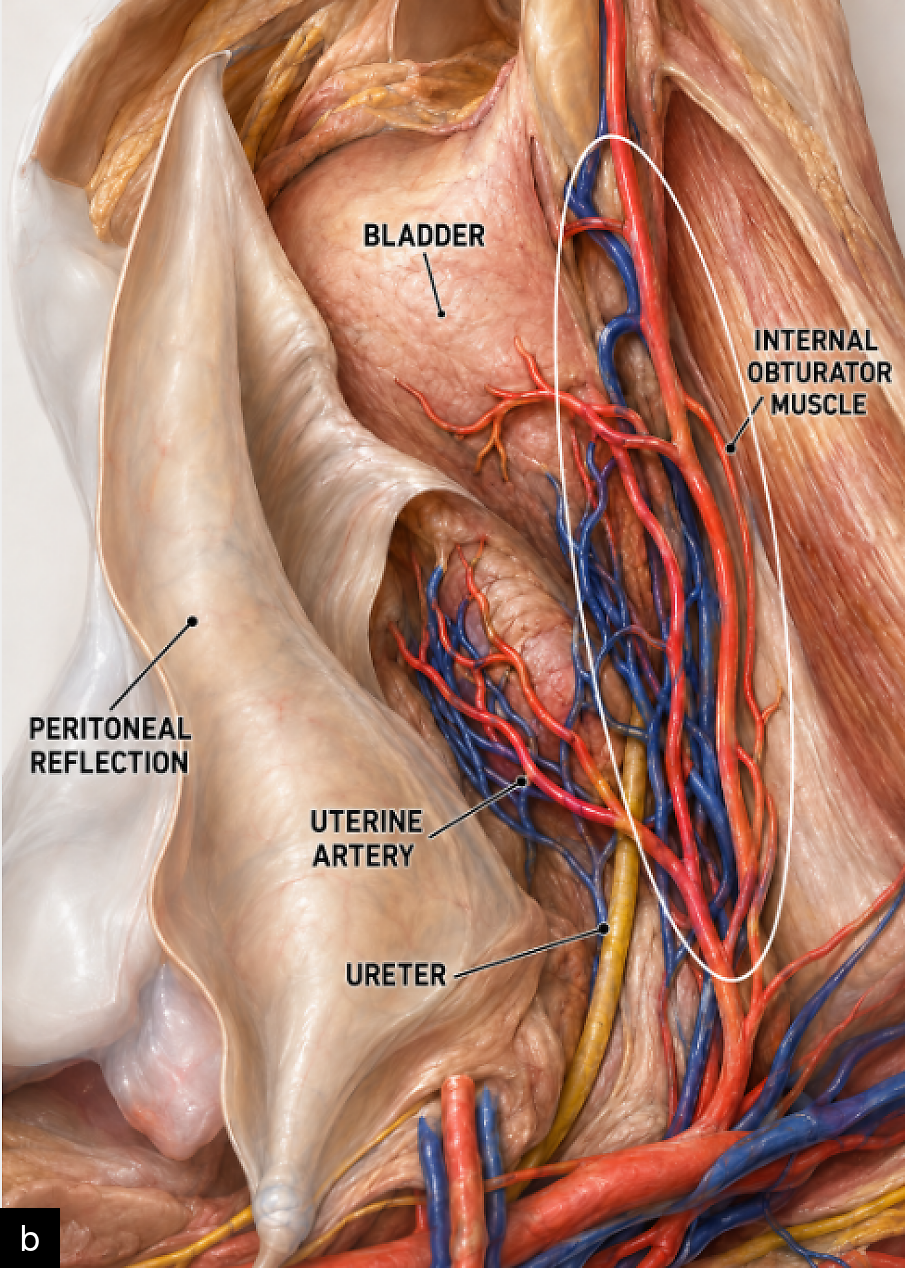
(a) Surgical view of low parametrial placental involvement (arrows) in a 23-week pregnancy. The patient was referred with a diagnosis of anterior placenta accreta spectrum and fetal demise, and cesarean delivery was performed. The left round ligament was markedly adherent; therefore, dissection was started from the lower sector and continued cephalad. A massive hemorrhage occurred during attempted placental release. Internal aortic compression was immediately performed, allowing completion of the dissection and hemostasis. Although the area of placental involvement was no larger than 5 cm, it was firmly and vascularly attached to the anterior branches of the internal iliac artery. (b) Illustration showing a superior view of the right parametrium. The lateral pelvic wall has been resected, exposing the anterior branches of the internal iliac artery, together with the ureter and uterine artery. Under normal conditions, this is a small space, measuring approximately 4–5 cm, but it contains a remarkable number of vascular structures.
Topographic classification explains why disease severity cannot be reduced to histological depth alone. A focal lesion with unfavorable topography may be more dangerous than a deeper lesion located in a surgically accessible and less vascular area.23,24,25,26,28,39
The relationship between the topographic approach and current international recommendations deserves clarification. Major guidelines, including those of ACOG, SMFM and RCOG, still consider planned cesarean hysterectomy with the placenta left in situ as the standard or preferred strategy in many cases of PAS, particularly when uterine preservation is not required or specialized conservative surgical expertise is unavailable.5,42 However, those recommendations were developed before several important advances were made in understanding PAS pathophysiology, pelvic surgical anatomy, uterine remodeling and conservative surgery based on resection and repair.23,39,43,44 Moreover, most international guidelines continue to rely on the FIGO accreta–increta–percreta framework, a classification that does not fully capture the heterogeneous topographic distribution of placental involvement, uterovesical involvement, surgical complexity or the feasibility of uterine preservation.8,23,39,43 The topographic classification should therefore be understood not as a substitute for existing guidelines, but as a complementary surgical stratification system aimed at improving preoperative counseling, intraoperative decision-making, risk prediction and outcome comparison across different strategies. This distinction is clinically relevant: the topographic classification is currently being evaluated in a prospective multicenter study, and preliminary data suggest a consistent relationship between each topographic subtype and maternal morbidity, surgical difficulty, operative time and the probability of successful uterine preservation.43
PRENATAL DIAGNOSIS
Ultrasound
Ultrasound is the cornerstone of prenatal PAS diagnosis.9,34,45,46,47,48 Standardized descriptors include placental lacunae, loss of the retroplacental clear zone, myometrial thinning, abnormal uterovesical hypervascularity (Figure 7), bridging vessels, bladder wall interruption and placental bulging.34,45 These signs must be interpreted in the appropriate clinical context. Although numerous sonographic features have been described, prenatal assessment should be considered suggestive of PAS rather than definitive for selecting the surgical strategy. Because hysterectomy is irreversible, and because severe PAS carries substantial operative risk, the final therapeutic decision should always incorporate intraoperative staging. This approach is consistent with the management of other complex conditions, such as endometrial or ovarian cancer, in which imaging supports preoperative planning, but definitive management depends on intraoperative findings.22,23

7
Transabdominal color Doppler ultrasound showing placenta accreta spectrum (PAS). The image demonstrates a low-lying anterior placenta (PL) in proximity to the posterior bladder wall, with markedly abnormal vascularity at the uterovesical interface. Multiple prominent color Doppler signals corresponding to enlarged, irregular vascular channels are seen between the placental bed and the bladder wall, suggesting numerous bridging vessels. The normal hypoechoic retroplacental clear zone appears interrupted or poorly defined in the anterior lower uterine segment. These findings are consistent with PAS, with suspected abnormal placental adherence and increased vascular remodeling at the vesicouterine interface. The prominent subplacental and uterovesical Doppler flow supports the diagnosis and suggests a potentially high-risk anterior PAS location. (Image courtesy of Dr Jorge Hamer, MAICE, Maternity Integral Center, City of Buenos Aires, Argentina.)
In experienced hands, ultrasound has high diagnostic accuracy.46,47 The most relevant contemporary advance, however, is not simply the binary detection of PAS but the preoperative characterization of surgical risk. A comprehensive evaluation, including transvaginal and color Doppler assessment, can help predict the need for hysterectomy and inform whether uterus-preserving surgery is technically feasible.27,28,49
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is not a replacement for expert ultrasound, but it can be useful as an adjunct in selected cases, particularly when the placenta is posterior (Figure 8), ultrasound windows are limited, or when lateral (parametrial) or posterior extension is suspected.9,36,50,51 MRI may help delineate the relationship between the placenta and adjacent structures, although its value depends heavily on local expertise and the quality of interpretation.52,53

8
Sagittal T2-weighted magnetic resonance image. A focal hypointense area is visible in the posterior placental implantation site (PAS) within an otherwise homogeneous placenta. The patient had a previous vaginal delivery complicated by a retained placenta requiring manual removal. (Image courtesy of Dr Estela Gómez, Sanatorio Otamendi, Ciudad Autónoma de Buenos Aires, Argentina.)
SURGICAL STAGING
Even with high-quality prenatal imaging, the full extent of PAS may only become apparent intraoperatively. Surgical staging involves systematic exploration of pelvic spaces and tissue planes to identify the precise location of placental compromise, the presence of fibrosis or neovascularization, the relationship of the lesion to the vesicouterine peritoneal fold, and the availability of healthy myometrium for reconstruction.23,24
Comprehensive surgical staging converts an uncertain or oversimplified prenatal diagnosis into an anatomically actionable intraoperative assessment.23 It avoids proceeding directly to hysterectomy in all cases and, conversely, helps prevent inappropriate conservative attempts in anatomically unfavorable disease. In practical terms, staging answers four essential questions: where the lesion is, how far it extends, which structures are at risk, and whether reconstruction is feasible. A prospective multicenter evaluation of this staging system is currently underway, representing the first prospective assessment of a surgical classification specifically designed for PAS.23,39
Topographic classification
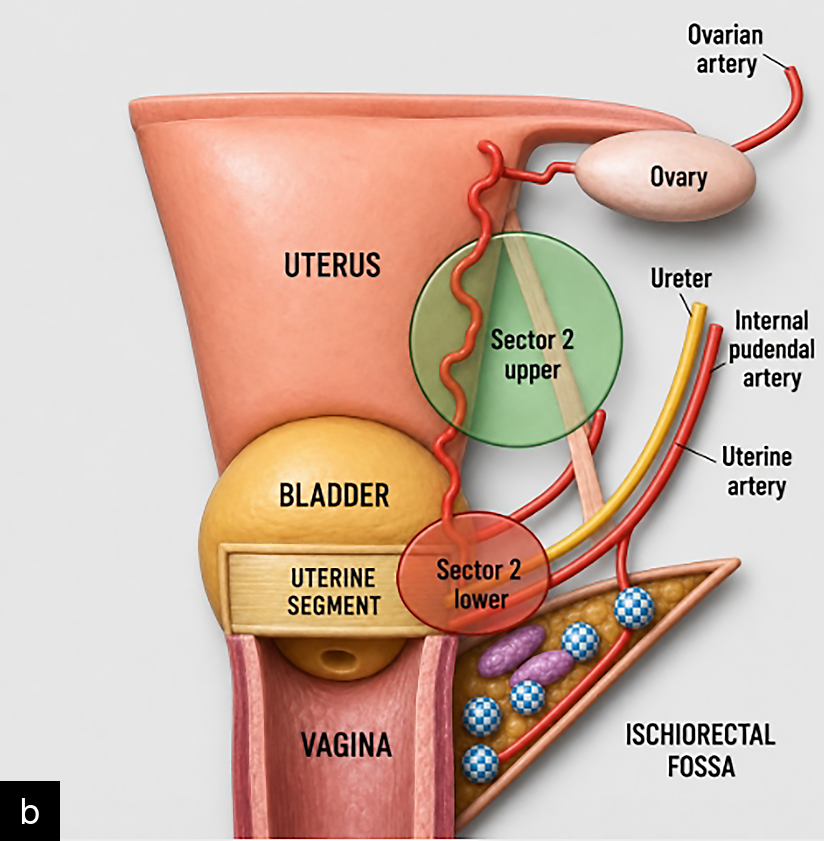
The topographic classification23 defines six anatomical areas: three above and three below the peritoneal reflection, corresponding to anterior, lateral and posterior uterine involvement. Sector 1 accounts for approximately 80% of PAS cases and lies adjacent to the posterosuperior aspect of the bladder. Sector 2 corresponds to lateral involvement and is subdivided into upper and lower forms, the latter extending into the parametrium. Sectors 3 and 4 share the same general location and are related to the posteroinferior aspect of the bladder, or cervicotrigonal area. Sector 4 differs from Sector 3 in that it is associated with intense fibrosis, making safe separation technically impossible. Sector 5 corresponds to posterior involvement and is also subdivided into upper and lower forms (Figure 9a).
|
|
9
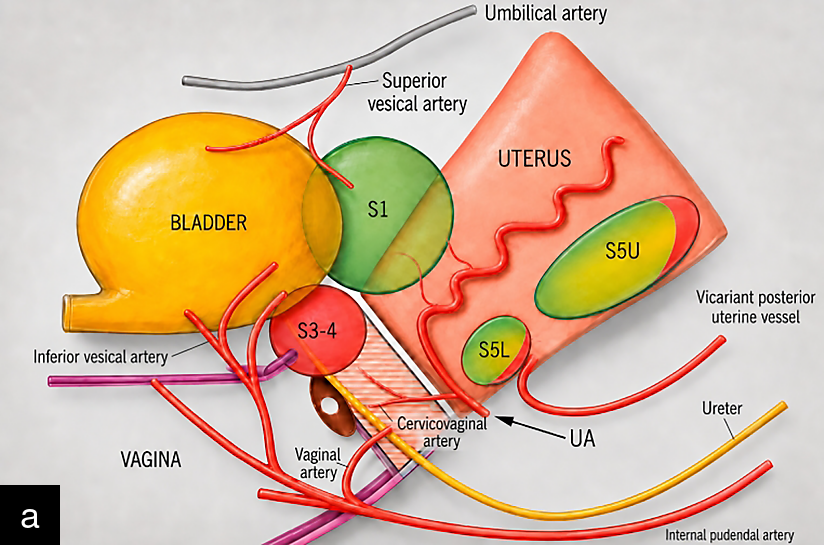
(a) Sagittal diagram of the uterus, vagina and bladder showing Sectors 1, 3, 4 and 5 (S1, S3–4 and upper (U) and lower (L) S5) of the topographic classification, together with their main associated vascular pedicles. The green color indicates a location that is usually easier to resolve surgically and has a high likelihood of preserving the uterus. In contrast, the red color indicates a high risk of massive bleeding. Posterior locations are usually less complex, but they may be associated with varying degrees of surgical difficulty when adjacent organs, such as the colon, rectum or small bowel, are involved. (b) Coronal diagram of the uterus, vagina and bladder showing upper and lower Sector 2 of the topographic classification, together with the main associated vascular pedicles and structures. Color representations are as in part (a)
Intraoperative decision-making is central to individualized management. Staging is not an accessory maneuver; it is the step that determines whether uterus-preserving surgery, local resection, modified subtotal hysterectomy, or total hysterectomy is the safest option.23,24,25,26,27,28,54,43
TREATMENT INDIVIDUALIZATION
Surgical staging examines all uterine surfaces, both above and below the peritoneal reflection, before the placenta is mobilized. After entering the abdominal cavity, the round ligaments are identified, placed under tension with Allis forceps, and the anterior leaf of the broad ligament is opened24 (Figure 10). The index fingers are then introduced downward, separating the tissues in cephalad and caudal directions to open the parametrial space (Video 1). Three situations may be encountered: no intervening tissue is present, and only the uterine vessels are visible; a placenta covered by serosa appears as a lateral bulge; or a placenta with engorged vessels is identified.

10
Diagram showing incision of the peritoneum (anterior leaf of the broad ligament) medial to the round ligament as the initial maneuver to access the parametrial space.
1
Surgical video showing opening of the left parametrial space during cesarean delivery. When the round ligament is placed under tension, the anterior leaf of the broad ligament becomes visible. After incision of this leaf, the surgeon introduces the fingers downward, allowing the parametrial space to unfold.
The index finger is then advanced anteriorly toward the medial paravesical space (Figure 11), bounded laterally by the ureter. The ureter and the surrounding pelvisubperitoneal fatty tissue are gently displaced laterally by digital dissection. With both fingers joined in the midline, the surgeon advances upward from the cervix to identify loose or firm adhesions on the posterior bladder wall (Figure 12), after performing the retrovesical bypass maneuver. The retrovesical plane is usually loose, although it may contain adhesions from prior cesarean deliveries. If dissection is not smooth, the surgeon is likely outside the correct plane and should relocate.

11
Diagram illustrating the opening of the parametrial space through fascial dissection of the broad ligament. On the left, the first step of the maneuver shows the fingers separating the tissues cephalad and caudally. On the right, the diagram shows the progression of the dissection toward the medial paravesical and retrovesical spaces.

12
Illustration showing the position of the index fingers from the vesicocervical plane toward the cephalad direction during the retrovesical bypass maneuver.
Bladder mobilization is performed from the posterior bladder wall.23,24 A variable number of vesicouterine (bridging) vessels are typically encountered (Figure 13). These vessels carry blood from the bladder muscular layer toward the placenta and should be ligated individually, since their poorly developed muscular wall may make monopolar electrocautery insufficient.
|
|
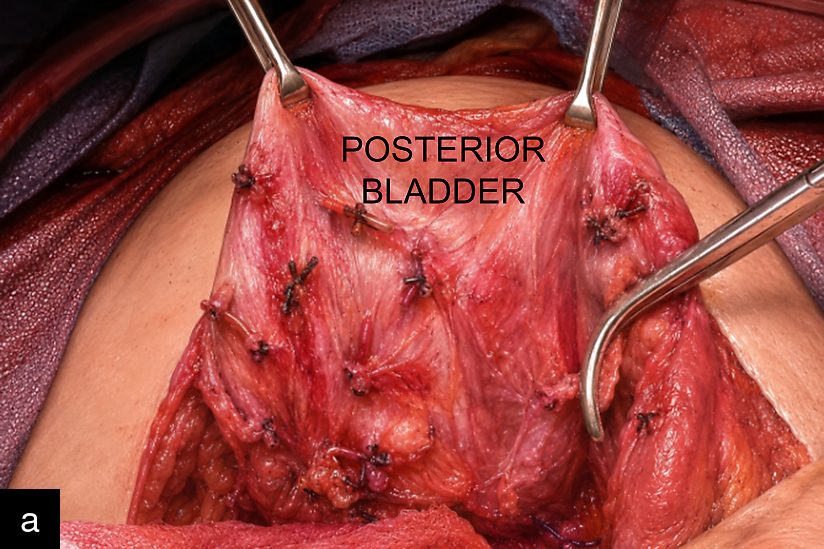
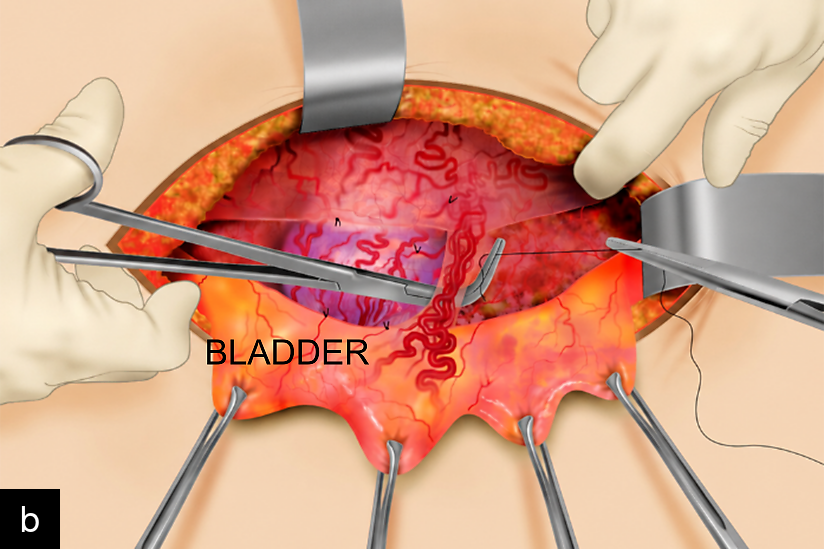
13
(a) Illustration shows multiple vessels arising from the posterior bladder wall and extending toward the placenta (bridging vessels). The use of Allis forceps helps to traction the bladder and create an angle with the uterine wall, thereby facilitating the passage of ligatures. (b) Illustration showing dissection of the vesicouterine space in cases of placenta accreta spectrum. Traction with Allis forceps creates a working space that allows the vesicouterine vessels to be ligated one by one until the posterior bladder wall is fully released. (Reproduced from Nieto-Calvache et al.24, with permission.)
After complete bladder mobilization, three key criteria are evaluated: whether at least 2 cm of healthy myometrium is present below the macroscopically involved area; whether circumferential involvement affects less than 50% of the uterine circumference; and whether the bladder has been completely detached.24,25,26 If all three are met, the patient may be a candidate for conservative treatment, such as one-step conservative surgery. Favorable anatomy meeting these criteria is found in approximately 80% of cases.
A hysterotomy is then performed approximately 1 cm above the upper border of the macroscopically involved area, followed by placental detachment using the Ward maneuver55,56 (Figure 14). At this level, the placenta is normally implanted, so no additional bleeding is expected. After fetal delivery, the uterus is exteriorized, and the final step of staging is completed by examining the posterior uterine wall.

14
Schematic cross-section of the uterus in a patient with placenta previa. The surgeon's hand is introduced through an incision made approximately 2 cm above the upper border of the macroscopically involved area (bulging). The hand is then advanced between the placenta and the myometrium until it reaches the amniotic sac. Note that, at this level, the placenta is normally implanted, therefore, no additional bleeding occurs. PAS, placenta accreta spectrum. (Reproduced from Nieto-Calvache et al.24, with permission.)
SURGICAL MANAGEMENT
Most PAS cases can be managed with one-step conservative surgery; however, certain anatomical locations are more safely handled with an alternative approach (Table 1).
1
Suggested management options for placenta accreta spectrum according to type (mixed, dehiscence, synchronic forms)
OSCS or similar | Hysterectomy | STMH | Delayed |
Type 1 Type 3 Type 2U Type 5 | Type 2L Type 3* | Type 4 | Type 2L Type 4* |
L, lower; OSCS, one-step conservative surgery; STMH, subtotal modified hysterectomy; Type 3*, in some cases, lower hemostasis is not achievable, and hysterectomy becomes mandatory; Type 4*, delayed procedure is possible only if the uterine pedicles are untouched; U, upper.
Cesarean hysterectomy
Cesarean hysterectomy remains the standard treatment for many patients with extensive PAS, particularly those with broad lower segment involvement, severe retrovesical distortion or parametrial extension.15,16,17,18,57 The core principle is to deliver the fetus through an incision placed away from the placenta and then remove the uterus with the placenta left in situ, thereby avoiding placental separation and reducing the risk of uncontrolled hemorrhage. In most cases, this approach prevents massive bleeding; however, when placental involvement is lateral or cervicotrigonal, massive and potentially uncontrollable hemorrhage may still occur. Surgical staging is therefore valuable not only for identifying candidates for conservative treatment, but also for recognizing severe or synchronous disease (Figure 15) that requires a different operative strategy.22

15
Surgical photograph showing lateral placenta accreta spectrum (PAS) adjacent to the round ligament and extending beneath it (**). The anterior uterine surface also showed dehiscence with areas of PAS. Synchronous PAS is uncommon and is usually associated with previous manual placental removal or evacuation curettage. If the lateral uterine surface is not systematically explored, this component may be missed, with a significant risk of unexpected hemorrhage during placental removal.
The main advantages of hysterectomy are procedural familiarity and the definitive treatment it provides. Its disadvantages are equally significant: loss of fertility, increased risk of urinary tract injury, substantial blood loss and prolonged recovery.17,18,19,20,58
The comparison between resective-reconstructive series and hysterectomy cohorts from the meta-analytic literature suggests that the key difference between strategies goes beyond the absolute amount of blood loss. In the resective-reconstructive technique, the placenta and the invaded myometrium are removed en bloc after selective control of the newly formed vesicouterine and colpouterine vessels, and uterine repair is attempted only when sufficient healthy tissue remains.26 In the series of Palacios-Jaraquemada et al., uterine preservation was achieved in 228 of 326 histologically confirmed PAS cases; hysterectomy was required in approximately 30% of patients and was mainly associated with extensive lower uterine damage rather than uncontrolled bleeding.26 Blood loss tracked closely with involvement topography: median estimated blood loss was 1500 mL for Types 1 and 2, and 2000 mL for types 3 and 4. By contrast, hysterectomy arms in the meta-analysis of Pan et al. showed consistently higher blood loss, with mean values ranging from approximately 2000 to 4500 mL, along with greater transfusion requirements, longer operative times, and higher rates of bladder injury, intensive care admission, and coagulopathy compared with conservative strategies.59 Although the meta-analysis primarily defined conservative management as partial or complete placental retention in situ, which is not equivalent to a planned resective-reconstructive procedure, the hysterectomy data remain useful as a reference for the morbidity associated with definitive uterine removal. Taken together, these findings suggest that, once expectant management is excluded, a planned resective-reconstructive strategy may avoid hysterectomy in a substantial proportion of anatomically favorable PAS cases while keeping blood loss within a range largely determined by involvement topography.26,59
Conservative and uterus-preserving surgery
Conservative PAS surgery encompasses a range of procedures designed to remove the compromised uterine segment while preserving the uterus. These include localized resection, segmental myometrial excision with reconstruction, one-step conservative surgery, modified one-step conservative uterine surgery (MOSCUS) and the Triple-P procedure.6,24,26,28,50,54
One-step conservative surgery is one of the best-described uterus-preserving approaches. It combines intraoperative staging, selective hemostatic maneuvers, en bloc resection of the compromised myometrium and placenta, and uterine reconstruction using healthy tissue margins.24,26 Recent prospective and randomized data suggest that, in appropriately selected cases, outcomes may be comparable to those of hysterectomy, with the added benefit of fertility preservation.28
Postoperative outcomes are central to counseling women with PAS, particularly when future fertility is a priority. Available evidence from a feasibility randomized trial, a large resective-reconstructive series, and a cohort of 202 subsequent pregnancies after conservative-reconstructive surgery, supports analyzing estimated blood loss, transfusion requirements, uterine preservation rates, subsequent pregnancy rates, and recurrent PAS risk together rather than in isolation26,28,60 The clinical interpretation of these outcomes varies depending on reproductive goals. For some women, uterine preservation is not limited to the possibility of another pregnancy; it is also tied to body integrity and personal identity. Qualitative evidence shows that hysterectomy can affect perceptions of fertility, womanhood and gender identity, particularly in young women who have not completed childbearing.61 Beyond reproductive considerations, hysterectomy may adversely affect ovarian function even when the ovaries are preserved, likely through interruption of the ovarian branch of the uterine artery and reduction of utero-ovarian blood flow. This mechanism is supported by systematic review data and prospective evidence showing an increased risk of earlier ovarian failure after hysterectomy with ovarian conservation.62,63 Perioperative and reproductive outcomes should therefore be analyzed together, allowing a more balanced assessment of the clinical trade-off between hemorrhagic risk, uterine preservation, future fertility, and long-term reproductive health.
The clearest message from the conservative surgery literature is not that hysterectomy should be abandoned, but that treatment should match topography and objective data after surgical staging. Recent meta-analyses suggest that conservative approaches may be feasible and reduce certain measures of surgical morbidity in selected patients, although outcomes remain strongly influenced by case selection and center expertise.28,49,54
Modified subtotal hysterectomy
Modified subtotal hysterectomy is a salvage procedure reserved for cases with severe placental involvement and dense fibrosis of the anteroinferior uterine sector (PAS type 4), particularly when disease extends toward the bladder trigone.41,64 The cervicotrigonal area is supplied by an anastomotic vascular network connecting the inferior vesical, vaginal and cervical arteries. Dense fibrotic adhesion can prevent safe dissection and carries the risk of disrupting this vascular ring with uncontrollable hemorrhage. From an endovascular perspective, selective hemostasis in this region may also be extremely difficult without producing ischemic injury to the bladder, vagina or adjacent pelvic organs.
In this technique, a standard hysterectomy is performed up to the level of the compromised area. The uterus is then transected under aortic vascular control (Figure 16), the placenta is removed digitally, and the posterior uterine wall is compressed against the thin anterior wall to create a hemostatic patch (Figure 17), even at the risk of including part of the bladder detrusor. Additional sutures close the cervical canal, leaving a cervical stump. After releasing the aortic control, the absence of vaginal bleeding is confirmed; if residual bleeding persists, further hemostatic sutures are placed.
|
|
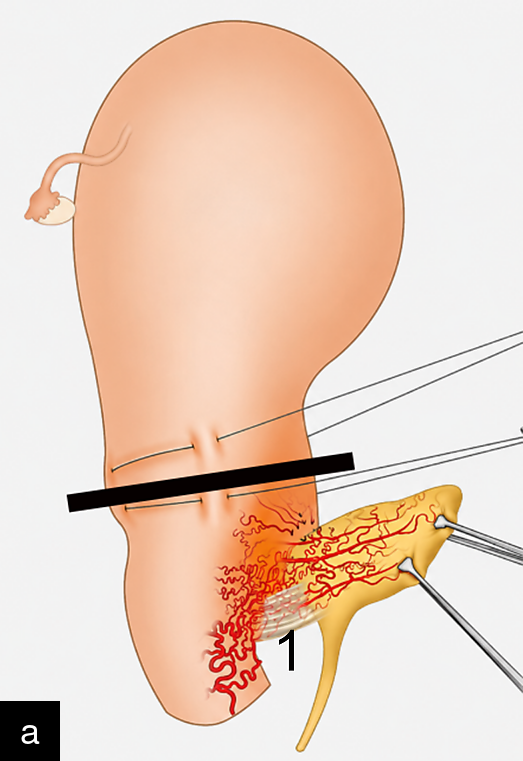
16
(a) Illustration showing Type 4 placenta accreta spectrum, located in the anteroinferior uterine sector (trigone-cervix), with intense fibrosis (1). The bar indicates the transection site and one of the initial steps of the modified subtotal hysterectomy. (b) Illustration showing the third step of modified subtotal hysterectomy. Uterine transection is performed under aortic vascular control, usually by internal aortic compression. The residual placenta is then removed digitally, and a purse-string suture is placed. (Reproduced from Palacios-Jaraquemada et al.41, under the terms of the CC BY licence.)

17
Illustration showing the next step of modified subtotal hysterectomy. The posterior uterine wall is compressed against the anterior wall, thereby occluding the vessels that supply the placenta in that sector. Note that these steps are performed under aortic vascular control, which is released only after the posterior hemostatic sutures have been completed. (Reproduced from Palacios-Jaraquemada et al.41, under the terms of the CC BY licence.)
PAS lesions in the anteroinferior uterine sector with dense fibrosis represent one of the anatomical patterns most strongly associated with maternal death. Surgeons unfamiliar with this topography may proceed with a conventional hysterectomy while the fibrotic, hypervascular tissue continues to bleed massively. Modified subtotal hysterectomy can be performed with limited additional training and, in selected emergency settings, may allow maternal survival by removing the compromised placenta and controlling hemorrhage without attempting unsafe dissection through the cervicotrigonal fibrotic field.
Expectant management
Expectant management, in which the placenta is left in situ after delivery, has been reported in selected circumstances.6,58 It may avoid immediate hemorrhage in some cases, but exposes the patient to delayed bleeding, infection, sepsis, secondary hysterectomy and prolonged follow-up. It should not be considered equivalent to resective conservative surgery and should be reserved for carefully selected settings with strict surveillance protocols and 24/7 assistance.6
VASCULAR CONSIDERATIONS
Maternal morbidity and mortality in PAS are closely linked to hemorrhage. Analysis of factors associated with maternal death consistently identifies lack of surgical experience as a central determinant, including insufficient understanding of vascular control and pelvic anatomy. PAS surgery is often a low-frequency event in many obstetric units, and in this context, improvisation and conceptual gaps during critical steps increase the risk of major complications.65
The uterus can be divided didactically into two vascular sectors separated by the peritoneal reflection (Figure 18). The upper sector (S1), the uterine body and fundus, receives arterial flow from the uterine and ovarian arteries. The uterine arteries arise from the anterior division of the internal iliac artery; the ovarian arteries arise directly from the abdominal aorta.64
The lower sector (S2) receives its main blood supply from collateral branches of the inferior vaginal artery, a branch of the internal pudendal artery, which itself arises from the posterior division of the internal iliac artery. This inferior vascular system communicates with the uterine system via the colpouterine arteries, which usually form three trunks running along the anterior vaginal wall at the 12, 3 and 9 o'clock positions. The middle trunk, at 12 o'clock, is typically the most prominent and is known as the azygos vaginal artery (Figure 18). These are ascending branches and should not be interpreted as descending branches of the uterine artery, despite how they are often described in the literature. This distinction is clinically important because most PAS lesions involve S2. Accordingly, embolization, ligation or occlusion of the uterine arteries or the anterior division of the internal iliac artery is usually ineffective for controlling hemorrhage from S2.66,67

18
Schematic representation of the main uterine vascular pedicles and the inferior anastomotic system. The black line approximately marks the level of the peritoneal reflection, dividing the uterus into an upper sector (S1), supplied by the uterine and ovarian arteries, and a lower sector (S2), supplied by collateral branches of the internal pudendal artery. The internal pudendal artery gives rise to the inferior vaginal artery, from which three colpouterine branches usually originate. The middle branch is commonly the most prominent and is known as the azygos vaginal artery. (Reproduced from Palacios-Jaraquemada et al.66, with permission.)
For most PAS cases, hemostasis depends on direct control of the colpouterine vessels. In massive bleeding from S2, the first maneuver should be to compress or occlude the infrarenal aorta. This simple step rapidly interrupts most pelvic anastomotic inflow and provides immediate control while definitive hemostatic measures are carried out.68
The concept of ‘descending branches’ of the uterine artery has created significant confusion during hemostatic management, including among interventional radiologists. Many teams, therefore, use ligation or occlusion of the anterior division of the internal iliac artery. However, when the internal pudendal artery remains patent, it continues to supply the inferior vaginal artery, which feeds the colpouterine vessels (Figure 19), leaving S2 bleeding inadequately controlled.64,66,67

19
Illustration showing the anterior vaginal wall with three prominent colpouterine vessels: 1, right; 2, middle or azygos; and 3, left. The middle vessel is commonly known as the azygos artery of the vagina. In most cases, these pedicles course within the thickness of the vaginal muscular layer. They constitute the main uterine anastomotic pedicles when the uterine arteries have been embolized or ligated. (Image courtesy of Luis Altamirano, MD, PAS Group, Hospital Bertha Calderón, Nicaragua.)
Another anatomical error reproduced in several textbooks is the description of the internal pudendal artery as a branch of the anterior division of the internal iliac artery. In the largest compiled anatomical analysis encompassing more than 5000 cases of internal iliac artery division, the internal pudendal artery arose from the posterior division in over 60% of cases and from the anterior division in only 13%.69
MULTIDISCIPLINARY CARE AND CENTER EXPERIENCE
Management of PAS requires coordinated care involving experienced obstetric surgeons, anesthesiologists, transfusion specialists, neonatologists, urologists and, when available, interventional radiologists. Specialized PAS teams have consistently been associated with better maternal outcomes and lower morbidity because they combine surgical expertise, standardized protocols, anticipation of blood loss and rapid access to multidisciplinary support.9,15,16,18,19,56,58
Multidisciplinary coordination is particularly important when conservative surgery is considered. Uterus-preserving procedures are not isolated technical maneuvers but part of a broader management strategy that depends on high-quality preoperative imaging, staged intraoperative assessment, careful patient selection and advanced pelvic surgical skills.22,23,24,26,28
For many years, PAS management has been advocated primarily within centers of excellence..70,71 Although this model offers clear advantages, it does not reflect the realities of many healthcare systems worldwide. The more relevant question is whether PAS surgery can be performed safely outside highly specialized referral centers. Increasing evidence suggests that it can, provided that appropriate expertise, multidisciplinary support and structured interinstitutional collaboration are available. Low-cost telemedicine, remote case discussion, shared operative planning and surgical mentorship have made this approach increasingly feasible, particularly in lower-resource settings that often manage a substantial volume of PAS cases.72
The technical skills required for hysterectomy are largely the same as those needed for conservative PAS surgery. The principal difference lies in the addition of specific anatomical knowledge, systematic surgical staging and a structured exploration that defines the extent of disease before treatment decisions are made. In this context, expertise depends not only on operative ability but also on understanding the anatomical principles that underpin individualized management.
Ultimately, the goal should not be to restrict PAS surgery to a small number of referral centers, but to ensure that women have access to teams with appropriate knowledge, experience and multidisciplinary support. Clinicians who continue to rely solely on older concepts without incorporating contemporary anatomical understanding and evolving surgical strategies may inadvertently compromise patient outcomes. Continued education, collaboration and the adoption of evidence-based innovations will be essential to further improving the management of PAS.
PRACTICAL FRAMEWORK FOR CLINICAL DECISION-MAKING
An individualized PAS strategy begins before surgery. The patient's history, placental location, ultrasound findings and likelihood of lower-segment or parametrial involvement should be assessed in advance.9,10,27,34,45 During surgery, the lesion should be staged systematically before definitive action is taken.23,24
A practical framework may be summarized as follows:
- Suspect PAS early in women with placenta previa or a low-lying placenta over a cesarean scar.
- Characterize lesion topography prenatally using expert ultrasound, supplemented by MRI in selected cases.27,28,49,50,51
- Stage the lesion intraoperatively before committing to hysterectomy or reconstruction.23,24
- Choose the operation based on anatomy, not solely on histological terminology.22,23,24,25,26
- Concentrate care in specialized centers with established PAS pathways.9,18,19,58,70
FINAL REMARKS
Progress in PAS management will likely depend on three areas. First, more refined prenatal imaging models may improve the prediction of surgical complexity and the need for hysterectomy.27 Second, multicenter comparative studies and randomized data may better define the role of uterus-preserving surgery in anatomically selected disease.28,49,54 Third, broader adoption of topographic thinking may improve training, communication and surgical planning across centers.22,23,39
PAS is one of the most consequential complications of contemporary obstetrics. Its burden is increasing in parallel with rising cesarean delivery rates, particularly among women with a history of cesarean delivery and placenta previa. Although cesarean hysterectomy remains the standard treatment for extensive PAS with unfavorable anatomy, framing PAS as a single disease with a single surgical solution is no longer adequate.
Current understanding of PAS pathophysiology emphasizes defective decidualization over a scarred uterus rather than intrinsically aggressive trophoblastic invasion. While histological depth remains important for pathological classification, growing evidence demonstrates that lesion topography is a major determinant of operative complexity, hemorrhagic risk and the feasibility of uterine preservation. In particular, retrovesical and parametrial involvement is associated with greater surgical difficulty and blood loss.
Accurate prenatal assessment is therefore essential. Ultrasound remains the first-line imaging modality, with MRI serving as an adjunct in selected cases. The goal of imaging should extend beyond diagnosis to anticipating surgical complexity and facilitating treatment planning. Intraoperative surgical staging further refines assessment and supports individualized management.
An approach based on prenatal imaging, surgical staging, lesion topography and multidisciplinary expertise offers the best opportunity to reduce maternal morbidity while preserving fertility when appropriate. Conservative uterus-preserving surgery may be feasible in carefully selected patients managed by experienced teams, while optimal outcomes overall are most likely to be achieved in specialized PAS centers with coordinated obstetric, anesthetic, urologic, neonatal and transfusion support.
PRACTICE RECOMMENDATIONS
- Screen for PAS in any patient with placenta previa or low-lying placenta over a scar from a previous cesarean section.
- Use expert ultrasound as the first-line diagnostic test; reserve MRI for selected cases in which ultrasound is limited or posterior/lateral extension is suspected.
- Use prenatal imaging to anticipate surgical complexity, to avoid making irreversible operative decisions in isolation.
- Perform systematic surgical staging before placental mobilization whenever anatomy and maternal status allow.
- Base the operative plan on lesion topography, fibrosis, vascular distortion, bladder involvement, parametrial extension and the availability of healthy myometrium for reconstruction.
- Avoid manual placental removal when PAS is suspected unless the surgical plan specifically includes controlled resective reconstruction.
- Consider uterus-preserving surgery only when staging confirms favorable anatomy and the team has the necessary expertise.
- Use modified subtotal hysterectomy or other salvage procedures when cervicotrigonal fibrosis makes conventional dissection unsafe.
- Prioritize direct control of the relevant vascular territory; massive S2 bleeding may require immediate infrarenal aortic compression while definitive hemostasis is achieved.
- Develop institutional pathways, simulation-based training, telemedicine support and interinstitutional collaboration to expand safe PAS care beyond a small number of referral centers.
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Afshar Y, Yin O, Jeong A, Martinez G, Kim J, Ma F, et al. Placenta accreta spectrum disorder at single-cell resolution: a loss of boundary limits in the decidua and endothelium. Am J Obstet Gynecol. 2024;230(4):443.e1–443.e18. | |
Kashani-Ligumsky L, Scott O, Martinez G, et al. Updates and knowledge gaps in placenta accreta spectrum biology. Clin Obstet Gynecol. 2025;68(2):310–316. | |
Afshar Y, Shah S, Brenner ML. Translating placenta accreta biology into surgical principles of uterine conservation: reply. Am J Obstet Gynecol. 2026 Feb 5:S0002–9378(26)00064–5. | |
Hecht JL, Baergen RN, Ernst LM, et al. Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum disorders. Mod Pathol. 2020;33(12):2382–2396. | |
American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 7: Placenta Accreta Spectrum. Obstet Gynecol. 2018;132(6):e259–e275. | |
Sentilhes L, Kayem G, Chandraharan E, Palacios-Jaraquemada J, Jauniaux E. FIGO consensus guidelines on placenta accreta spectrum disorders: conservative management. Int J Gynaecol Obstet. 2018;140(3):291–298. | |
Jauniaux E, Ayres-de-Campos D, Langhoff-Roos J, Fox KA, Collins S; FIGO Panel. FIGO classification for the clinical diagnosis of placenta accreta spectrum disorders. Int J Gynaecol Obstet. 2019;146(1):20–24. | |
Jauniaux E, Chantraine F, Silver RM, Langhoff-Roos J; FIGO Panel. FIGO consensus guidelines on placenta accreta spectrum disorders: epidemiology. Int J Gynaecol Obstet. 2018;140(3):265–273. | |
Kingdom JC, Hobson SR, Murji A. Placenta accreta spectrum. Lancet. 2022;399(10327):2317–2329. | |
Jauniaux E, Einerson BD, Hussein AM, Silver RM, Burton GJ. What is placenta accreta? Am J Obstet Gynecol. 2026;233(6 Suppl):S630–S640. | |
Jauniaux E, Jurkovic D. Placenta accreta: pathogenesis of a 20th century iatrogenic uterine disease. Placenta. 2012;33(4):244–251. | |
Eller AG, Porter TF, Soisson P, Silver RM. Optimal management strategies for placenta accreta. BJOG. 2009;116(5):648–654. | |
Palacios-Jaraquemada JM, D'Antonio F. Possible limitation to use the International Federation of Gynecology and Obstetrics classification of placenta accreta spectrum. Am J Obstet Gynecol. 2020;223(6):944. | |
Dannheim K, Shainker SA, Hecht JL. Hysterectomy for placenta accreta: methods for gross and microscopic pathology examination. Arch Gynecol Obstet. 2016;293(5):951–958. | |
Allen L, Jauniaux E, Hobson S, Papillon-Smith J, Belfort MA. FIGO consensus guidelines on placenta accreta spectrum disorders: nonconservative surgical management. Int J Gynaecol Obstet. 2018;140(3):281–290. | |
Cahill AG, Beigi R, Heine RP, Silver RM, Wax JR. Placenta accreta spectrum. Am J Obstet Gynecol. 2018;219(6):B2–B16. | |
Bailit JL, Grobman WA, Rice MM, et al. Morbidly adherent placenta treatments and outcomes. Obstet Gynecol. 2015;125(3):683–689. | |
Bartels HC, Rogers AC, O'Brien D, et al. Association of implementing a multidisciplinary team approach in the management of morbidly adherent placenta with maternal morbidity and mortality. Obstet Gynecol. 2018;132(5):1167–1176. | |
Wright JD, Herzog TJ, Shah M, et al. Regionalization of care for placenta accreta: effect on maternal morbidity. Obstet Gynecol. 2010;115(1):65–70. | |
Silver RM, Branch DW. Placenta accreta spectrum. N Engl J Med. 2018;378(16):1529–1536. | |
Palacios-Jaraquemada JM. Diagnosis and management of placenta accreta. Best Pract Res Clin Obstet Gynaecol. 2008;22(6):1133–1148. | |
Palacios-Jaraquemada JM, Basanta N, Nieto-Calvache AJ, Aryananda RA. Advantages of individualizing the placenta accreta spectrum management. Front Reprod Health. 2023;4:1096175. | |
Palacios-Jaraquemada JM, Basanta N, Nieto-Calvache A, Aryananda RA. Comprehensive surgical staging for placenta accreta spectrum. J Matern Fetal Neonatal Med. 2022;35(26):10660–10666. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Aryananda R, et al. How to perform the one-step conservative surgery for placenta accreta spectrum move by move. Am J Obstet Gynecol MFM. 2023;5(2):100802. | |
Palacios-Jaraquemada JM, Nieto-Calvache A, Aryananda RA, Basanta N. Placenta accreta spectrum into the parametrium, morbidity differences between upper and lower location. J Matern Fetal Neonatal Med. 2023;36(1):2183764. | |
Palacios-Jaraquemada JM, Fiorillo A, Hamer J, Martinez M, Bruno C. Placenta accreta spectrum: a hysterectomy can be prevented in almost 80% of cases using a resective-reconstructive technique. J Matern Fetal Neonatal Med. 2022;35(2):275–282. | |
Aryananda RA, Adu-Bredu TK, Cininta NI, et al. Diagnostic ultrasound to inform the surgical approach to cesarean delivery in patients at high risk for placenta accreta spectrum disorders. Am J Obstet Gynecol. 2025;233(6):658.e1–658.e16. | |
Nieto-Calvache AJ, Aryananda RA, Palacios-Jaraquemada JM, et al. One-step conservative surgery vs hysterectomy for placenta accreta spectrum: a feasibility randomized controlled trial. Am J Obstet Gynecol MFM. 2024;6(6):101333. | |
Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 1997;177(1):210–214. | |
Thurn L, Lindqvist PG, Jakobsson M, et al. Abnormally invasive placenta: prevalence, risk factors and antenatal suspicion. BJOG. 2016;123(8):1348–1355. | |
Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, Knight M. Incidence and risk factors for placenta accreta/increta/percreta in the UK. PLoS One. 2012;7(12):e52893. | |
Mucio B, Serruya S, Aleman A, Castellano G, Sosa C. Cesarean delivery and other uterine surgery as risk factors for placenta accreta: a systematic review and meta-analysis. Int J Gynaecol Obstet. 2019;147(3):281–291. | |
Garmi G, Salim R. Epidemiology, etiology, diagnosis, and management of placenta accreta. Obstet Gynecol Int. 2012;2012:873929. | |
Collins SL, Ashcroft A, Braun T, et al. Proposal for standardized ultrasound descriptors of abnormally invasive placenta. Ultrasound Obstet Gynecol. 2016;47(3):271–275. | |
Jauniaux E, Collins S, Burton GJ. Placenta accreta spectrum: pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am J Obstet Gynecol. 2018;218(1):75–87. | |
Jauniaux E, Jurkovic D, Hussein AM, Burton GJ. New insights into the etiopathology of placenta accreta spectrum. Am J Obstet Gynecol. 2022;227(3):384–391. | |
Jauniaux E, Hussein AM, Elbarmelgy RM, Elbarmelgy RA, Burton GJ. Failure of placental detachment in accreta placentation is associated with excessive fibrinoid deposition at the utero-placental interface. Am J Obstet Gynecol. 2022;226(2):243.e1–243.e10. | |
D'Antonio F, Iacovella C, Bhide A. Prenatal identification of invasive placentation using ultrasound: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2013;42(5):509–517. | |
Walker SP, Bartels HC, Nieto-Calvache AJ, Palacios-Jaraquemada JM, Collins SL, Aryananda R. Strategies for streamlining uterine topographic classification in placenta accreta spectrum. AJOG Glob Rep. 2026;6(2):100636. | |
Jauniaux E, Bhide A. Prenatal ultrasound diagnosis and outcome of placenta previa accreta after cesarean delivery: a systematic review and meta-analysis. Am J Obstet Gynecol. 2017;217(1):27–36. | |
Palacios-Jaraquemada JM, Nieto-Calvache AJ, Aryananda RA, et al. Placenta accreta spectrum with severe morbidity: fibrosis associated with cervical-trigonal involvement. J Matern Fetal Neonatal Med. 2023;36(1):2183741. | |
Jauniaux E, Alfirevic Z, Bhide AG, et al. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG. 2019;126(1):e1–e48. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Aryananda R, et al. Evaluation of the topographic classification of placenta accreta spectrum: protocol for an ongoing prospective multicenter study. BMC Pregnancy Childbirth. 2025;25(1):1266. Erratum in: BMC Pregnancy Childbirth. 2026;26(1):187. | |
Jauniaux E, Hussein AM, Zosmer N, Elbarmelgy RM, Elbarmelgy RA, Shaikh H, Burton GJ. A new methodologic approach for clinico-pathologic correlations in invasive placenta previa accreta. Am J Obstet Gynecol. 2020;222(4):379.e1–379.e11. | |
Comstock CH. Antenatal diagnosis of placenta accreta: a review. Ultrasound Obstet Gynecol. 2005;26(1):89–96. | |
Bowman ZS, Eller AG, Kennedy AM, et al. Accuracy of ultrasound for the prediction of placenta accreta. Am J Obstet Gynecol. 2014;211(2):177.e1–7. | |
Warshak CR, Eskander R, Hull AD, et al. Accuracy of ultrasonography and magnetic resonance imaging in the diagnosis of placenta accreta. Obstet Gynecol. 2006;108(3 Pt 1):573–581. | |
Meng X, Xie L, Song W. Comparing the diagnostic value of ultrasound and magnetic resonance imaging for placenta accreta spectrum disorders: a systematic review and meta-analysis. Clin Radiol. 2020;75(4):289–297. | |
Hessami K, Kamepalli S, Lombaard HA, et al. Conservative management of placenta accreta spectrum is associated with improved surgical outcomes compared to cesarean hysterectomy: a systematic review and meta-analysis. Am J Obstet Gynecol. 2025;232(5):432–452.e3. | |
Chandraharan E, Rao S, Belli AM, Arulkumaran S. The Triple-P procedure as a conservative surgical alternative to peripartum hysterectomy for placenta percreta. Int J Gynaecol Obstet. 2012;117(2):191–194. | |
Wortman AC, Alexander JM. Placenta accreta, increta, and percreta. Obstet Gynecol Clin North Am. 2013;40(1):137–154. | |
Palacios-Jaraquemada JM, Bruno CH, Martin E. MRI in the diagnosis and surgical management of abnormal placentation. Acta Obstet Gynecol Scand. 2013;92(4):392–397. | |
Palacios Jaraquemada JM, Bruno CH. Magnetic resonance imaging in 300 cases of placenta accreta: surgical correlation of new findings. Acta Obstet Gynecol Scand. 2005;84(8):716–724. | |
Pinto PV, Freitas G, Vieira RJ, et al. Placenta accreta spectrum disorder: a systematic review and meta-analysis on conservative surgery. Int J Gynaecol Obstet. 2026;172(1):115–136. | |
Ward CR. Avoiding an incision through the anterior previa at cesarean delivery. Obstet Gynecol. 2003;102(3):552–554. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Basanta N, et al. How to avoid placental transection during low transverse cesarean delivery for anterior placenta previa. Am J Obstet Gynecol. 2026 Feb 25:S0002–9378(26)00115–8. | |
Einerson BD, Rodriguez CE, Kennedy AM, et al. Magnetic resonance imaging is often misleading when used as an adjunct to ultrasound in the management of placenta accreta spectrum disorders. Am J Obstet Gynecol. 2018;218(6):618.e1–618.e7. | |
Shamshirsaz AA, Fox KA, Erfani H, et al. Multidisciplinary team learning in the management of the morbidly adherent placenta: outcome improvements over time. Am J Obstet Gynecol. 2017;216(6):612.e1–5. | |
Pan S, Han M, Zhai T, Han Y, Lu Y, Huang S, et al. Maternal outcomes of conservative management and cesarean hysterectomy for placenta accreta spectrum disorders: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024;24:463.28 | |
Palacios-Jaraquemada JM, Basanta N, Labrousse C, Martínez M. Pregnancy outcome in women with prior placenta accreta spectrum disorders treated with conservative-reconstructive surgery: analysis of 202 cases. J Matern Fetal Neonatal Med. 2022;35(25):6297–6301. | |
Bottomley D, Bourchier S, Sutherland K, Perz J, Ussher JM. A qualitative analysis of the fertility experience and gender identity in young women following hysterectomy for benign disease. Sex Roles. 2023;89:368–381. | |
Huang Y, Wu M, Wu C, et al. Effect of hysterectomy on ovarian function: a systematic review and meta-analysis. J Ovarian Res. 2023;16(1):35. | |
Moorman PG, Myers ER, Schildkraut JM, Iversen ES, Wang F, Warren N. Effect of hysterectomy with ovarian preservation on ovarian function. Obstet Gynecol. 2011;118(6):1271–1279. | |
Palacios Jaraquemada JM, Garcia Monaco R, Barbosa NE, Ferle L, Iriarte H, Conesa HA. Lower uterine blood supply: extrauterine anastomotic system and its application in surgical devascularization techniques. Acta Obstet Gynecol Scand. 2007;86(2):228–234. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Vergara-Galliadi LM, et al. ; Latin American Group for the Study of Placenta Accreta Spectrum. All maternal deaths related to placenta accreta spectrum are preventable: a difficult-to-tell reality. AJOG Glob Rep. 2021;1(3):100012. | |
Palacios-Jaraquemada JM, Nieto-Calvache AJ, Basanta NA, et al. Essential anatomical knowledge for performing routine and complex cesarean delivery. Am J Obstet Gynecol. 2026;233(6 Suppl):S368–S384. | |
Nieto-Calvache AJ, Palacios Jaraquemada JM, Basanta N, et al. Internal manual compression of the aorta: an effective way to temporarily control pelvic bleeding in obstetrical hemorrhage. Am J Obstet Gynecol. 2022;227(1):96–97. | |
Nieto-Calvache AJ, Palacios-Jaraquemada JM, Aryananda RA, et al. How to identify patients who require aortic vascular control in placenta accreta spectrum disorders? Am J Obstet Gynecol MFM. 2022;4(1):100498. | |
Balcerzak A, Hajdys J, Tubbs RS, et al. Clinical importance of variability in the branching pattern of the internal iliac artery. Ann Anat. 2022;239:151837. | |
Silver RM, Fox KA, Barton JR, et al. Center of excellence for placenta accreta. Am J Obstet Gynecol. 2015;212(5):561–568. | |
Shamshirsaz AA, Fox KA, Erfani H, et al. The role of centers of excellence with multidisciplinary teams in the management of abnormal invasive placenta. Clin Obstet Gynecol. 2018;61(4):841–850. | |
Nieto Calvache AJ. Placenta accreta spectrum in low- and middle-income countries: usefulness of telemedicine [dissertation]. Amsterdam: University of Amsterdam; 2024. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)