This chapter should be cited as follows:
Tinelli A, Pecorella G, et al., Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.422213
The Continuous Textbook of Women’s Medicine Series – Obstetrics Module
Volume 20
Surgical Techniques in Obstetrics
Volume Editors:
Professor Michael Stark, New European Surgical Academy (NESA) and Charité University Hospital, Berlin, Germany
Professor Sergej Barinov, Omsk State Medical University, Ministry of Health of Russia
Professor Gian Carlo Di Renzo, PREIS International School, Florence, Italy
Chapter
Myomectomy in Pregnancy
First published: April 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Uterine fibroids, or leiomyomas, are the most common benign tumors of the uterus, arising from the smooth muscle (myometrium). They represent a major global health concern due to their impact on physical health, quality of life and economic wellbeing.1 During a woman's life cycle, uterine fibroids typically occur less frequently before puberty, are more common during the reproductive years and reduce in size after menopause.1
Histological studies indicate that uterine fibroids are characterized by three main features: increased sensitivity to sex steroid hormones, altered extracellular matrix deposition and enhanced proliferation of smooth muscle cells.2
Epidemiological research has identified several risk factors associated with leiomyoma growth, including age, ancestry, family history, reproductive factors, hormonal influences, hypertension and certain infections. Furthermore, specific dietary components may influence hormone-related diseases and the development of fibroids.3,4
Epidemiology of uterine fibroids
The prevalence of fibroids increases with age and appears to vary according to geographic location. In the USA, 70% of white women and over 80% of black women will develop fibroids by the age of 50.1 A similar prevalence is found in Italy, whereas fibroids appear to be less common in Sweden.5 In the 40–49-year age range, the prevalence of uterine fibroids varies from 4.5–9.4% in the UK to 9.8–17.8% in Italy.6 The prevalence of uterine fibroids in pregnancy varies between 1.6% and 10.7%.7
Although younger women are more likely to become pregnant, the average maternal age has increased in recent decades, which is associated with a higher prevalence of uterine fibroids. Some pregnant women require non-obstetric surgical procedures, most commonly cholecystectomy (45%), followed by ovarian surgery for predominantly benign cysts or tumors (34%), appendectomy (15%) and other procedures (6%). These surgeries are most frequently performed in the second trimester (56%), compared to the first (33%) and third (11%) trimesters.8,9
Uterine fibroids in pregnancy are associated with an increased likelihood of cesarean delivery, with reported rates of up to 40%. This is primarily due to complications such as malpresentation and mechanical obstruction, while common symptoms include pain, bleeding, and abdominal tenderness.10
Due to social factors, such as delayed childbearing, and advances in assisted reproductive technologies, including in-vitro fertilization, which makes it possible for even menopausal women to become pregnant through egg donation, the number of pregnant women with uterine fibroids is increasing, and this is especially true in western countries.11
Furthermore, the rate of cesarean delivery has been steadily increasing worldwide, especially among women undergoing treatment for infertility and those who give birth later in life. Because uterine fibroids are more common in these groups, pregnancies complicated by fibroids are also more frequently associated with cesarean delivery.12
Clinical presentation and complications of fibroids during pregnancy
Prenatal ultrasound reveals that 1–10% of expectant mothers have fibroids. While many women already know they have them, this is a novel discovery for some. According to scientific literature, infections and postpartum hemorrhage have been associated with complications related to the presence and/or growth of uterine fibroids during pregnancy and the puerperium. Fibroids are often detected during a woman’s first prenatal visit. Because fibroids may occur in any part of the uterus during pregnancy and do not always obstruct the birth canal, the reported complications are variable.
Generally, uterine fibroids during pregnancy are associated with an increased risk of postpartum hemorrhage, breech presentation and need for cesarean delivery, particularly when large or numerous. Depending on their size, number and position (particularly when close to the placenta), fibroids may also increase the risk of complications such as discomfort, early pregnancy loss, fetal growth restriction, premature labor, placental abruption, fetal malpresentation (such as breech) and placenta previa. Nevertheless, many pregnancies complicated by fibroids proceed normally.13,14
In the past, in certain facilities, surgeons sometimes performed a hysterectomy following delivery by cesarean section, in cases involving very large or multiple fibroids during pregnancy.15 In addition, submucosal fibroids have been associated with reduced clinical pregnancy rates and increased risk of miscarriage.16
Women with uterine fibroids detected during their first pregnancy have been found to have a high risk of hypertensive disorders of pregnancy (HDP), even after adjusting for multiple confounding factors. Given the adverse outcomes associated with HDP, pregnant women with uterine fibroids should have their blood pressure monitored regularly and undergo HDP prevention measures.17
That fibroids inhibit fetal growth and result in lower birth weight and earlier gestational age at delivery is supported clinically only by a drop in birth weight for mothers with many fibroids.18
Although most fibroids remain asymptomatic during pregnancy, pain represents the most frequent clinical manifestation, occurring in up to 8–15% of cases, and is more commonly associated with fibroids larger than 5 cm.18,19 Pain is typically experienced in the late first or early second trimester and may be accompanied by low-grade fever, leukocytosis, nausea and/or vomiting. Red degeneration, resulting from acute ischemia and necrosis of fibroid tissue, is the most common underlying mechanism and is usually managed conservatively.
Management of symptomatic fibroids during pregnancy
During pregnancy, fibroids may undergo dynamic changes in size and vascularity under the influence of hormonal stimulation and increased uterine blood flow. Enlargement is most commonly observed during the first trimester, while stabilization or regression often occurs in the second half of gestation and postpartum period.13 These changes may contribute to the onset of symptoms.
In a study of 113 pregnant women, 9% of fibroids showed cystic changes or a heterogeneous echogenic pattern on ultrasonography, which indicated the development of red degeneration. Among these women, 70% (7 of 10) experienced severe abdominal pain, compared with only 11.7% (12 of 103) of women with fibroids who showed no echogenic changes on ultrasonography.19
The severe pain associated with red degeneration has been explained by three primary mechanisms.20,21,22 First, the tissue outgrows its blood supply due to fast fibroid growth, which causes tissue anoxia, necrosis and infarction. Second, even in the absence of fibroid growth, the expanding uterus causes the blood supply to the fibroid to alter (kink), which causes ischemia and necrosis. Third, the fibroid's cellular damage causes prostaglandins to be released, which causes pain. The finding that ibuprofen and other prostaglandin synthetase inhibitors effectively and quickly manage fibroid pain lends credence to this.
Because surgery is typically avoided during pregnancy due to the risk of bleeding, management of fibroids focuses on conservative therapy. This includes rest, adequate hydration, safe analgesia and close clinical monitoring by an obstetrician. Acetaminophen (paracetamol) is commonly used for pain control, while non-steroidal anti-inflammatory drugs (NSAIDs) should be used cautiously for short periods, particularly before 30 weeks of gestation. Prolonged use, especially during the third trimester, has been associated with adverse fetal and neonatal outcomes, such as premature closure of the fetal ductus arteriosus, pulmonary hypertension, necrotizing enterocolitis, intracranial hemorrhage and oligohydramnios.23 In refractory cases, short-term opioid therapy may be considered.
Hospitalization may be necessary for severe pain. Surgical intervention is generally avoided and considered only when conservative treatment fails or when complications such as torsion of a pedunculated fibroid, persistent severe pain or compression of adjacent organs occur. Rarely, rapid fibroid growth raising concern for malignancy may also prompt surgical evaluation. In these selected situations, myomectomy during pregnancy may represent the only effective therapeutic option. Nevertheless, approximately 10–30% of women with uterine fibroids develop complications during pregnancy.20
MYOMECTOMY DURING PREGNANCY
Myomectomy during the first half of pregnancy has historically been uncommon. Traditionally, the presence of fibroids during pregnancy was considered a contraindication to any form of surgical intervention, with management limited to conservative measures. Because of concerns about the associated risks, including heavy bleeding, uterine rupture, miscarriage and preterm labor, myomectomy was rarely performed during pregnancy.24,25 As a consequence, myomectomy during pregnancy was regarded as an exceptional procedure, reserved only for life-threatening situations. Over the past two decades, however, accumulating clinical experience and advances in surgical techniques have progressively challenged this paradigm, leading to a more nuanced and individualized approach in selected cases.20
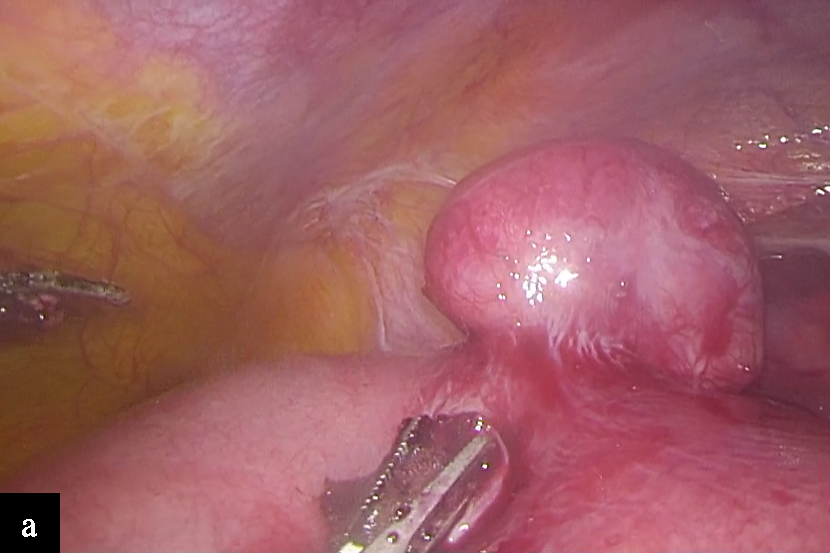
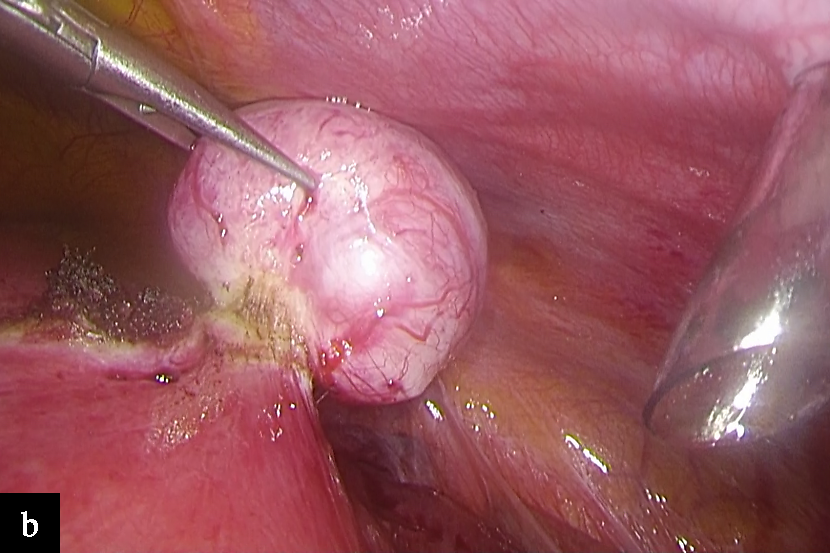
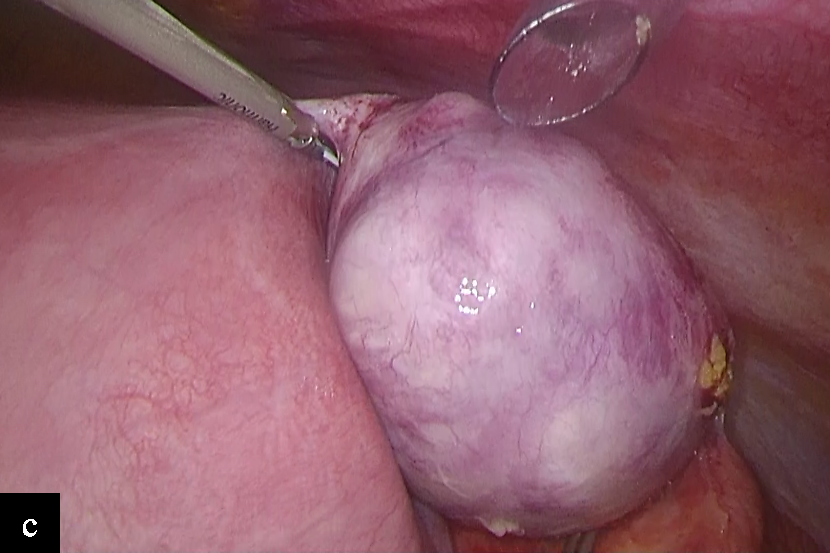
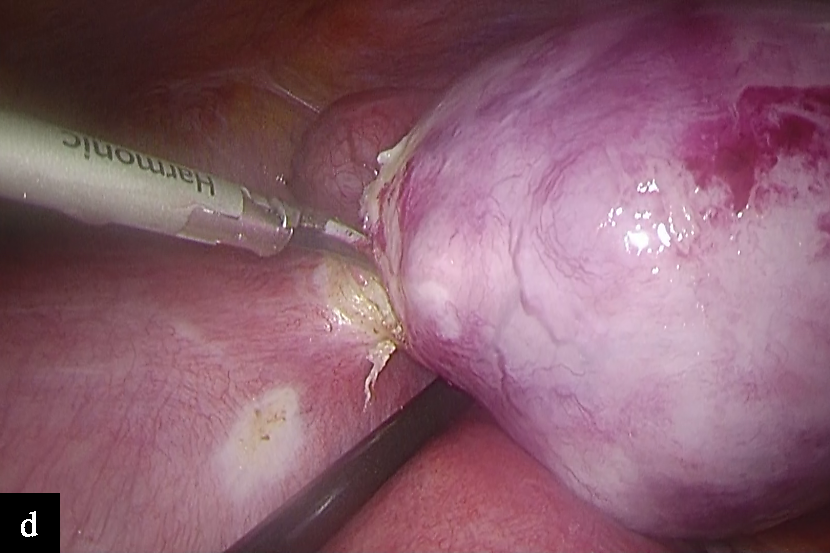
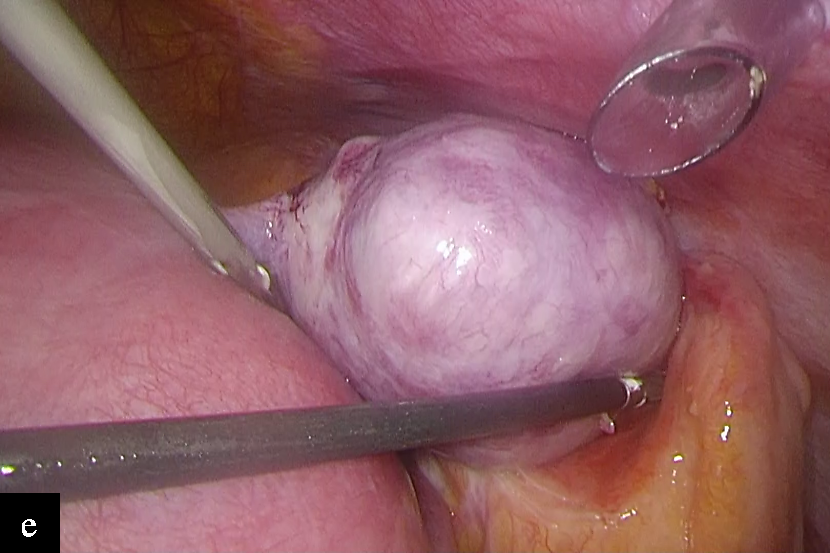
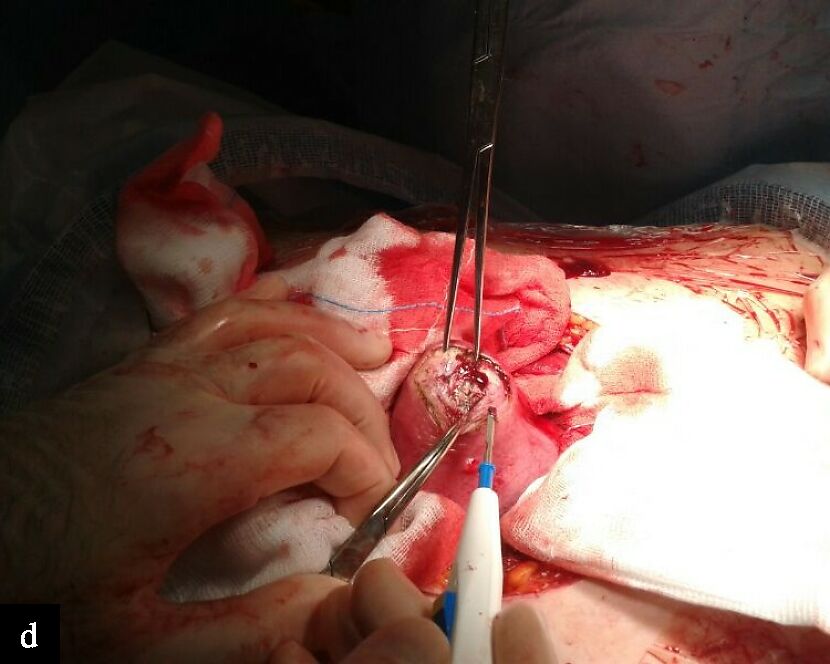
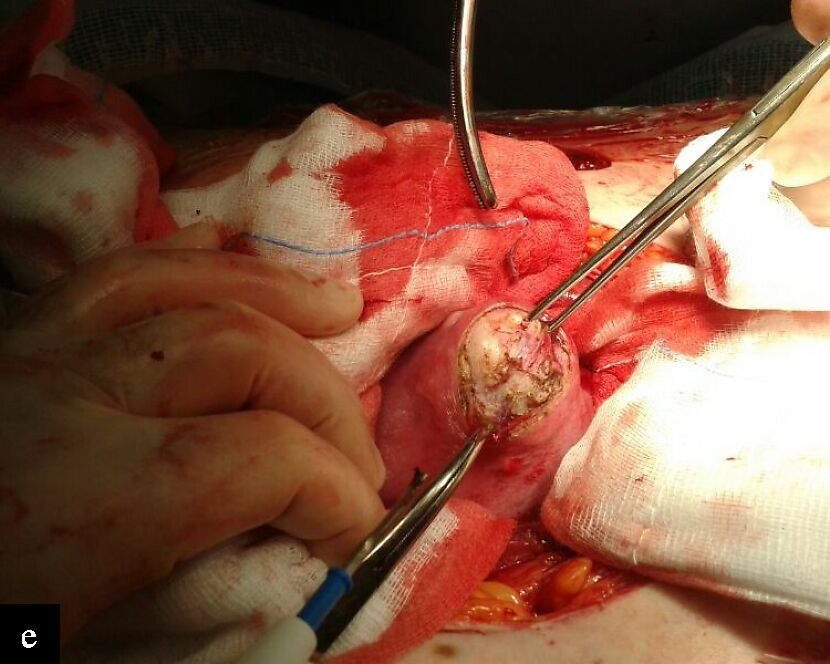
Studies have shown that antepartum myomectomy can be successfully carried out throughout the first and second trimesters if necessary.26,27 Intractable discomfort from a degenerating fibroid, particularly if it is subserosal or pedunculated (Figure 1), a large or rapidly growing fibroid, or any large fibroid (> 5 cm) in the lower uterine segment are acceptable indications.
The most comprehensive synthesis of available evidence on antepartum myomectomy has been provided by the systematic review of Spyropoulou et al., which analyzed 54 studies reporting 97 cases of myomectomy performed during pregnancy.27 The median gestational age at surgery was 16 weeks, with most procedures carried out during the first and second trimesters. Abdominal pain refractory to medical treatment was the most common indication for surgery. The majority of removed fibroids were subserosal or pedunculated and located at the uterine fundus. Laparotomy was the predominant surgical approach, accounting for approximately 78% of cases, while laparoscopic and vaginal approaches were reported in highly selected situations. Despite the heterogeneity of the available data, pregnancy outcomes were favorable in most cases, with low rates of miscarriage, preterm birth and severe maternal morbidity. Importantly, the review highlighted that uterine rupture following antepartum myomectomy was exceedingly rare and generally associated with extensive intramural resections or inadequate myometrial reconstruction. These findings support the concept that, when appropriately selected and performed by experienced surgeons, myomectomy during pregnancy may be safer than traditionally believed.
|
|
|
|
|
1
Subserosal fibroids (a,b) and pedunculated fibroids (c–e), showing torsion (d) and adherence of the fibroid to an intestinal loop (e) in a patient undergoing laparoscopic myomectomy at 17 weeks’ gestation.
Surgical considerations and technical aspects
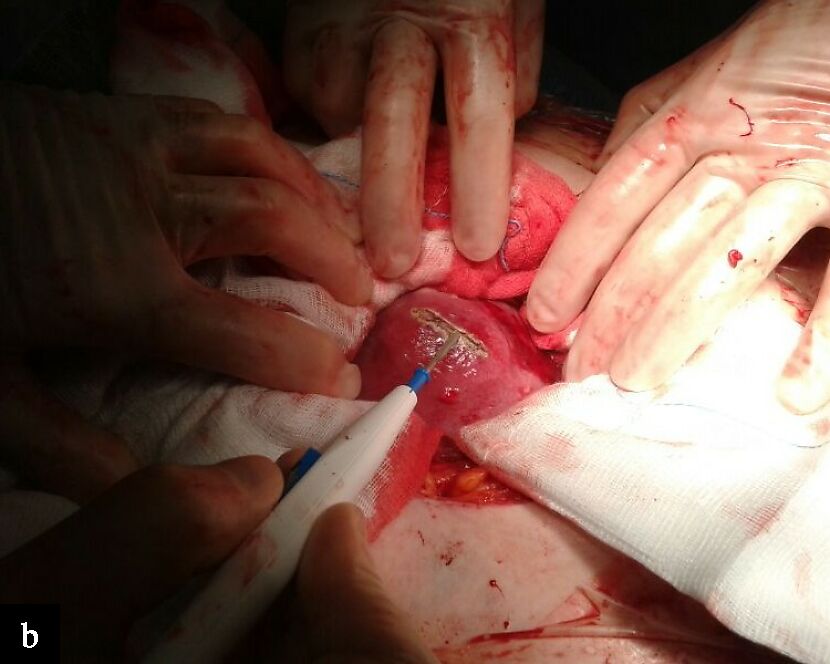
Careful patient selection is crucial from a surgical perspective. Because they allow for a smaller myometrial incision and have lower risk of bleeding, subserosal and pedunculated fibroids are the best candidates for removal during pregnancy (Figure 1). It is usually best to avoid removing deeply intramural or submucosal fibroids, especially those that are in contact with the placenta. The timing of the procedure is also crucial. In order to balance increased uterine vascularity later in pregnancy with decreased miscarriage risk and embryonic viability, the second trimester is sometimes seen as the best window for intervention. To maintain uterine integrity and reduce blood loss, a careful surgical technique is necessary. This includes limited dissection, visualization and preservation of the fibroid pseudocapsule (intracapsular myomectomy), rapid enucleation of the fibroid with minimal blood loss, effective hemostasis (Figure 2), and multilayer (where possible) uterine wall closure. In addition, the edges of the incised myometrium should be carefully approximated to avoid excessive penetration into the myometrial tissue (Figure 3). Although laparotomy is still the most commonly reported procedure in the literature, minimally invasive methods may be considered in certain situations and in facilities with highly skilled laparoscopic specialists. Laparoscopic myomectomy during pregnancy offers potential advantages in terms of postoperative recovery and adhesion formation, but requires strict adherence to safety principles, including low insufflation pressures and careful fetal monitoring.22

2
Laparoscopic myomectomy in a patient at 13 weeks’ gestation, with minimal blood loss and efficient hemostasis.

3
Laparoscopic myomectomy in pregnant patient: the edges of the incised myometrium are brought together by a continuous suture to avoid penetrating too deeply into the muscle.
Obstetric outcomes and mode of delivery
Women undergoing myomectomy during pregnancy are significantly more likely to have a cesarean delivery, largely reflecting a precautionary approach adopted by clinicians rather than absolute obstetric necessity.24,27 In most cases, cesarean delivery is planned to minimize the theoretical risk of uterine rupture during labor. Available evidence suggests that the overall risk of uterine rupture after myomectomy is comparable to that observed after previous cesarean delivery, particularly when the myometrial incision is limited and adequately repaired.28 Nevertheless, individualized delivery planning based on surgical details and obstetric factors remains essential.
Clinical implications and future perspectives
Antepartum myomectomy is a customized surgery that should only be used for a small number of patients who have severe, unresponsive symptoms. Optimal care should include multidisciplinary counseling, a comprehensive risk–benefit analysis and referral to specialized facilities. To further refine indications and enhance patient selection, future research should focus on collection of prospective data and uniform reporting of surgical techniques and results. The role of myomectomy during pregnancy is likely to become clearer as surgical skills and perioperative care continue to advance.
CESAREAN MYOMECTOMY
In 1914, Victor Bonney, a British gynecologist, published his first cesarean myomectomy (CM)29 and became a pioneer in uterine myomectomy. The patient he operated on, a 30-year-old primigravida, had a markedly enlarged uterus at 5 months of pregnancy, but she experienced no discomfort until term, when vaginal delivery proved unfeasible. After delivering the baby and exteriorizing the uterus, Bonney found that it was significantly enlarged by six fibroids: three intramural, two subserosal and the largest (described as ‘the size of a melon’) submucosal with cystic degeneration. Because the patient wished to preserve her fertility, Bonney chose to enucleate the tumors. After removal of the fibroids, the uterine defect was repaired with catgut sutures, which controlled the heavy bleeding. The patient subsequently had three vaginal deliveries.29
It was widely recognized in the first part of the 20th century that fibroids could lead to a variety of health problems both during and after pregnancy. In the years that followed, Bonney's successful CM was not widely accepted by obstetricians. Furthermore, regardless of patients' age or fertility goals, most publications from that era reported cases of hysterectomy as the preferred treatment for myomas detected during pregnancy. During the 1980s and 1990s, obstetricians reported increasing number of CMs and discussed the technical challenges and postoperative outcomes associated with the procedure. Numerous studies published in the final decades of the 20th century suggested that CM is generally a safe procedure, with complication rates comparable to those of cesarean section alone.
Burton et al.,30 were likely the first in contemporary obstetrics to report, in 1989, a series of 13 unplanned CMs carried out in the USA. One patient required uterine artery ligation and a transfusion of one unit of packed red blood cells due to intraoperative bleeding associated with CM. The authors concluded that ‘elective myomectomy at cesarean delivery was both safe and feasible in selected patients’.30 However, myomectomy during CS was strongly discouraged in obstetric textbooks published subsequently.31
Outcomes
Since the early 2010s, several meta-analyses have been conducted to evaluate the feasibility, safety and overall outcomes of CM. In 2013, Song et al.,32 reported the first meta-analysis, including 443 patients who underwent CM out of a total of 1082 patients analyzed. The authors concluded that, when performed ‘by experienced hands’, CM ‘might be a reasonable option for some patients’. They found no significant differences in cesarean section outcomes between patients who underwent CM and those who did not. The authors also noted that the lack of adequate high-quality data limited the generalizability of their findings.
Pergialiotis et al.,33 included in their meta-analysis 19 observational studies published up to March 2017, involving 3900 women of whom 2301 underwent CM. The authors concluded that ‘removal of a single symptomatic leiomyoma that is not located in the parametrium is not associated with significantly increased morbidity and could be considered on a case-by-case basis’, after finding only negligible difference in the blood loss and length of postoperative hospitalization associated with CM.
Goyal et al.,34 analyzed data from 17 studies published up to December 2019, including 6545 patients, of whom 4702 (71.8%) underwent CM and 1843 (28.2%) had CS alone. The authors acknowledged that the quality of the included studies was a limitation, as no randomized controlled trials (RCTs) were available. This may limit the generalizability of the findings because of potential selection bias. Furthermore, these studies considered only short-term morbidity and did not provide information on long-term complications in subsequent pregnancies. They concluded that, while there was no difference in frequency of bleeding, there was a statistically significant rise in the likelihood of receiving a blood transfusion and a 14.7-min increase in the length of the procedure. They highlighted that a CM can be performed safely despite its association with increased blood loss, higher odds of blood transfusion and the need for prolonged hospitalization.
The meta-analysis of Youshanloie et al.,35 included 8521 participants from 33 pertinent trials, of whom 5586 had CM and 2935 had CS alone. According to the authors, the groups differed significantly in mean operative time, hemoglobin drop, transfusion rates and intraoperative hemorrhage. There was no discernible difference in the incidence of postoperative fever. The authors noted that a strength of the study was the inclusion of only cohort studies, case–control studies and RCTs, while cross-sectional studies were excluded. Overall, CM may still be advantageous, especially when performed by experienced surgeons, as it can prevent the need for additional surgery and related costs, despite being associated with a larger drop in hemoglobin and longer recovery and hospital stays.
A meta-analysis published in 2022 by Huang et al.,36 included 8016 participants from 23 studies, comprising 19 retrospective and four prospective studies. Of these, 4061 patients underwent CS alone, while 3955 underwent CM. In terms of hemoglobin decline, hemorrhage incidence, blood loss volume, transfusion rate, length of operation, and length of hospital stay following surgery, the authors found statistically significant differences between the groups. The CM group experienced all these outcomes more frequently. The prevalence of postoperative fever was the sole similarity between the CM and CS-only groups. The authors concluded ‘CM can be performed uneventfully in more complicated cases where patients have myomas that are larger, intramural, multiple, and in other locations (except for the cornual site) as long as care is applied to adequate hemostasis’. Furthermore, consistent with previous reports, it was recommended to avoid operating on myomas located near large blood vessels. Again, due to the lack of such publications in the literature, none of the included studies was an RCT. The authors' inability to do a subgroup analysis pertaining to myoma features is another limitation of this meta-analysis, despite its magnitude.
The findings of these meta-analyses do not allow firm conclusions to be drawn regarding the precise indications and contraindications for CM. They also do not provide a comprehensive understanding of fibroid characteristics and their relationship to the development of complications. The lack of RCTs and significant heterogeneity of the current research data are the primary causes of this.
A recent Cochrane Review37 confirmed these conclusions, reporting very low certainty of evidence for all key outcomes. Consequently, no firm conclusions can be drawn regarding the impact of CM on outcomes such as the need for blood transfusion, risk of bleeding, length of hospital stay, operative time, risk of major surgical complications and postpartum fever. The collected data on the mean change in hemoglobin level were too diverse to be combined. Moreover, fertility outcomes were not available. However, there is mounting evidence from the current meta-analyses that, when carried out by experienced surgeons in facilities with sufficient equipment, CM should be regarded as a reasonably safe treatment.
Pro and cons
For more than a century, obstetric surgeons have been debating CM because it is a surgical procedure that combines two major operations (myomectomy and CS), both associated with a risk of significant bleeding, particularly in the presence of large fibroids. This risk is further increased during pregnancy due to enhanced uterine vascularization, which may lead to intraoperative hemorrhage and subsequent complications. The most common complications of CM include perioperative hemorrhage, which in severe cases may require interventions such as hysterectomy, vascular embolization or ligation, and blood transfusion. Additional risks include disseminated intravascular coagulopathy, postoperative ileus, considerably longer operative time and prolonged hospital stay. Admissions to the obstetric critical care unit following CM have also been reported.38
Regarding placental complications in pregnant women with fibroids, Akkurt et al.,39 reported a 3.1% prevalence of placenta previa after CM, however Adesiyun et al.,40 observed a higher prevalence. Given that postoperative adhesions are a well-known consequence of traditional abdominal myomectomy, Akkurt et al.,39 also investigated adhesion formation as a late complication of CM. Postoperative adhesions were identified in 25% of patients during a repeat cesarean surgery.
Another limitation is the lack of data on fibroid recurrence following CM. Akkurt et al.,39 reported a recurrence rate of 8.4% and found that 4.1% of women who underwent CM required additional major surgery for fibroids (two abdominal hysterectomies and one abdominal myomectomy). The authors identified extended follow-up (mean, 8.2 years), advanced age (> 45 years), history of numerous fibroids, and larger fibroid size (> 70 mm) as risk factors for fibroid recurrence following CM. During the follow-up period, none of the patients with recurrence of fibroids became pregnant.
Additionally, some advantages of CM compared with interval myomectomy or CS without fibroid enucleation have been reported in the literature.10,11,12 During pregnancy, uterine growth typically exceeds fibroid growth, resulting in a lower fibroid-to-uterus size ratio; consequently, the uterine incision required for fibroid removal may be smaller than in a non-pregnant uterus. Due to the increased elasticity and contractility of the uterus during pregnancy, CM is technically easier to perform, and hysterorrhaphy is often simpler in a pregnant uterus than in a non-pregnant one. Furthermore, physiological uterine involution and postpartum contractions help reduce bleeding. By combining the benefits of two procedures into a single operation, CM may reduce the risks and costs associated with a second surgery. In addition, CM may improve quality of life, alleviate fibroid-related symptoms, and reduce the risk of fibroid-related complications during the puerperium and in subsequent pregnancies.41,31
Ultrasound evaluation or intrasurgical visualization during future CS suggests greater scar integrity following CM than that with interval myomectomy, despite the lack of an effective diagnostic tool to evaluate the healing process at the myomectomy site and the quality of the scar.41,31 According to Adesiyun et al.,40 the overall rate of vaginal delivery following CM was 76.5%, indicating that fibroid removal during CM enhanced the likelihood of vaginal delivery in subsequent pregnancies. The same study's findings showed that the rate of spontaneous pregnancy following CM was 79.3%, suggesting that prior CM had no effect on future fertility or the outcome of subsequent pregnancies.
Leaving fibroids in the uterus during cesarean section has also been associated with serious complications. These include a high rate of hysterectomy for postpartum hemorrhage, an increased risk of postpartum sepsis, rapid growth of fibroids following elective CS leading to abdominal pain and hemoglobin drop, necessitating additional surgical management of the patient, malodorous vaginal discharge, urinary retention, pulmonary embolism, prolapse of fibroid into the vagina, and hypovolemic shock due to edema of a pedunculated fibroid that was left in the uterus.38
Techniques
Compared with the early 20th century, when Bonney first introduced CM, CS is now far safer.42 The risk–benefit profile of CM should be re-evaluated in light of the availability of modern antibiotics, advanced surgical instruments and contemporary surgical technologies. Although CM was historically considered controversial, current evidence suggests that it should still be regarded as part of the surgical armamentarium and remain an area of interest in both experimental and clinical research on uterine fibroids.43,44,45 For example, intraoperative blood salvage during CM has recently been recommended as a potential strategy to reduce the risks associated with heterologous blood transfusions in women with anticipated significant intraoperative hemorrhage.
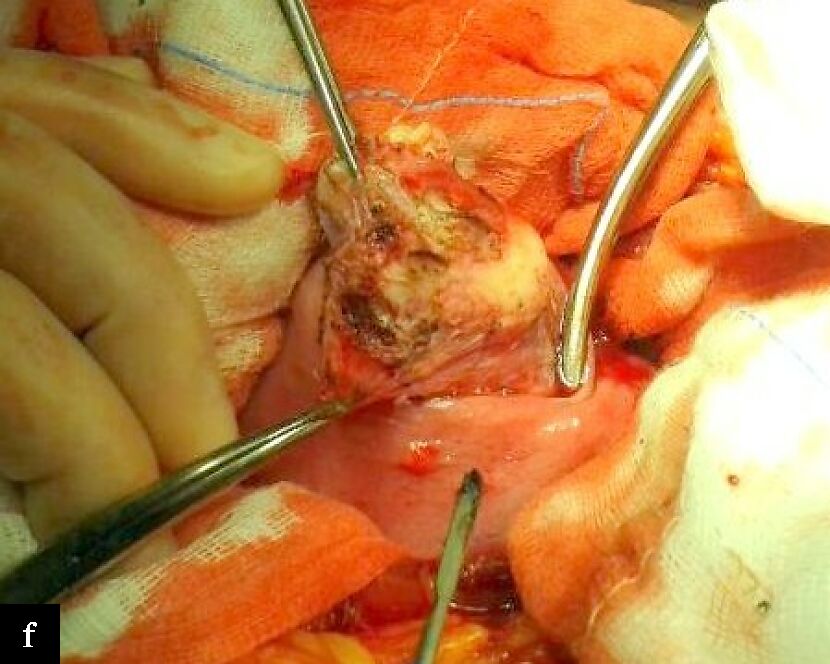
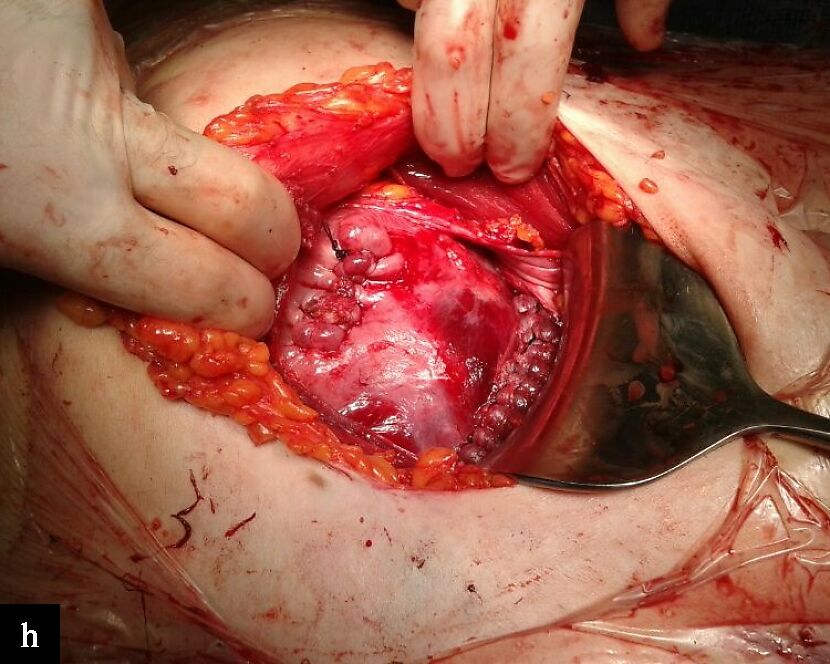
The scientific literature also provides a comprehensive analysis of the myoma pseudocapsule and its role in identifying the most physiologically suitable methods for removing fibroids from the uterus. ‘Intracapsular myomectomy’ was first described by Tinelli et al.,10,41,31 (Figure 4). This technique involves removing the myoma while leaving the pseudocapsule intact. This method can be used during CM (Figure 5), as well as during hysteroscopic, vaginal, laparotomic, robotic and laparoscopic myomectomy. The importance of preserving the myoma pseudocapsule during myomectomy has been extensively documented in the literature.46 Preservation of the pseudocapsule is the fundamental principle of this surgical technique, as it helps maintain healthy tissue around the myoma and promotes improved myometrial healing after myomectomy. The myoma pseudocapsule contains neurotransmitters and neuropeptides that are crucial for myometrial physiology. These compounds have a beneficial effect on female reproductive processes by promoting wound healing and muscular functional recovery following myomectomy. Tinelli et al. demonstrated no significant differences in surgical outcomes among 68 patients who underwent intracapsular CM, with the exception of slightly longer hospital stay and operating time.10
|
|

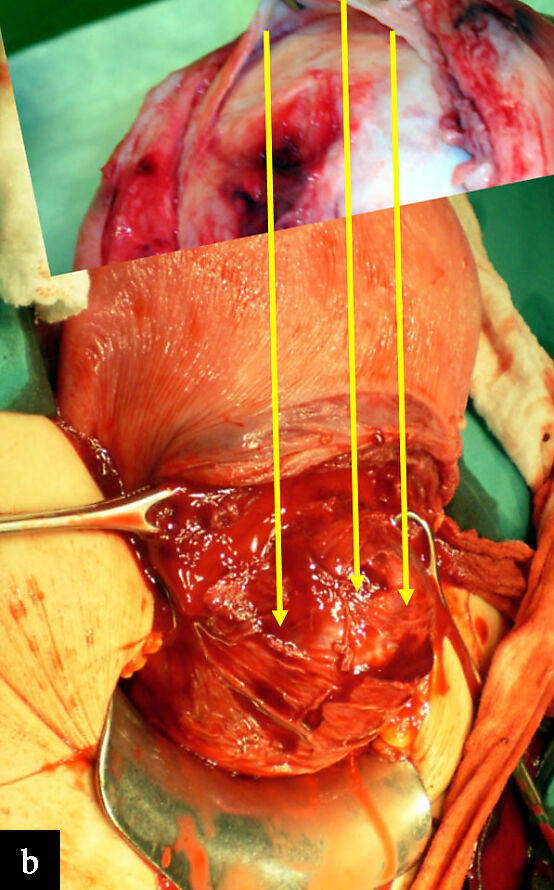
4
Intracapsular myomectomy. (a) Enucleation of a myoma following cesarean section; the pseudocapsule covering the myoma is clearly visible during myomectomy. (b) Lower uterine segment myomectomy, showing the pseudocapsule (arrows) around a large fibroid; in the top inset, the pseudocapsule is clearly seen to be separated from the myoma (Images reproduced from: Cesarean myomectomy. Malvasi A, Stark M, Tinelli A. In: Uterine myoma, myomectomy and minimally invasive treatments. Editors: Andrea Tinelli, Antonio Malvasi. Springer International Publishing Cham, Switzerland 2015, pp. 237–252.31).
|
|
|
|
|
|
|
|



5
Steps involved in intracapsular cesarean myomectomy of anterior fibroid following delivery of the neonate. (a) View of fibroid below uterine surface. (b) Using a monopolar electro-scalpel, a linear incision is made through the uterine serosa into the myoma. (c) Gradual dissection of the myoma from the myometrium until opening the pseudocapsule, enabling entry into the relatively bloodless plane between the pseudocapsule and its myoma. (d) Using the monopolar electro-scalpel, the surface of the myoma is reached and its fiber bridges separated from the tumor. (e) The myoma is gently hooked and carefully extracted from its capsule. (f) Hemostasis is achieved by gentle low voltage (≤ 30 watt) coagulation of pseudocapsule vessels, with minimal bleeding. (g) The fibroid base is grasped by forceps. (h) View following suturing of the uterus after removal of the fibroid (Images reproduced from: Cesarean myomectomy. Malvasi A, Stark M, Tinelli A. In: Uterine myoma, myomectomy and minimally invasive treatments. Editors: Andrea Tinelli, Antonio Malvasi. Springer International Publishing Cham, Switzerland 2015, pp. 237–252.31).
In recent years, CM has emerged as an alternative to conventional serosal myomectomy. Since its first description by two independent research groups,47,48 this technique has been the focus of numerous recent studies. The well-known benefits of hysteroscopic myomectomy, including reduction in intra-abdominal adhesions and blood loss, served as the model for this alternative approach, which begins with an incision on the uterine surface. The general steps of the procedure, as described by Hatirnaz et al.,47,49 and Wang et al.,50 include mobilizing the myoma toward the endometrial surface, suturing the myometrial defect (only if the defect is larger than 30 mm), making a trans-endometrial incision, enucleating the fibroid, and ligating the arteries at the myoma base. Compared with conventional serosal myomectomy, this technique may result in a smaller incision.47,48,49,50 Additionally, uterine involution reduces the size of the surgical site and incision, narrows damaged arteries, and appears to speed up hemostasis. By comparing pre- and postoperative hemoglobin levels, hemoglobin drop and the frequency of blood transfusions, Hatirnaz et al.,47,49 and Wang et al.,50 reported reduced blood loss. Given that the uterus's serosal surface is preserved throughout the treatment, it was assumed that endometrial myomectomy lowers the rate of intra-abdominal adhesion development.51 These results were reported in a study by Yıldırım Karaca et al.,52 who compared the results of various myomectomy techniques and assessed the effects on subsequent pregnancy and CS. They found that women who underwent endometrial myomectomy had significantly reduced intra-abdominal adhesion scores.
In a retrospective multicenter case–control study involving seven hospitals and 226 singleton pregnancies that underwent repeat CS, Güler et al.,53 examined the long-term perinatal, obstetric and surgical outcomes of CM by comparing different CM techniques: endometrial myomectomy and traditional or serosal myomectomy. The enrollment parameters did not significantly differ between the groups. Neonatal weight, Apgar score, fetal growth restriction, preterm premature rupture of membranes, preterm birth, HDP and diabetes mellitus did not differ significantly between the groups in terms of perinatal and obstetric outcomes. The myomectomy scar had a good healing rate of 99.1%, but the fibroid recurrence rate was 28.3%. Preoperative and postoperative hemoglobin levels, perioperative blood transfusion rates, febrile morbidity and length of hospital stay did not differ between groups. Although the serosal myomectomy group's adhesion rate was higher than the endometrial myomectomy group's, there was no statistically significant difference between the two groups in terms of adhesion occurrence.53
CONCLUSION
Myomectomy during pregnancy and CM have long been controversial because of concerns about potential complications and the identification of several risk factors for adverse outcomes.54 However, the decision to avoid myomectomy solely on the basis of these risks may not always be justified. With advances in surgical techniques, including minimally invasive approaches and the use of energy-based instruments such as vessel-sealing devices and harmonic scalpels, operative time and blood loss can be better controlled. Consequently, it is important to identify which fibroids are most likely to lead to complications if left in situ during pregnancy. Future research should therefore focus on refining patient selection and evaluating how emerging surgical techniques55 may influence the decision-making process regarding myomectomy during pregnancy.
PRACTICE RECOMMENDATIONS
- Currently, pregnancies complicated by uterine fibroids are relatively common, particularly in women over 35 years. During vaginal or cesarean delivery, large fibroids may lead to serious complications such as significant bleeding.
- Symptoms related to fibroids during pregnancy are usually managed with medical (conservative) treatment. If these measures fail, surgical intervention may be required either during pregnancy (myomectomy during pregnancy) or at the time of cesarean section (cesarean myomectomy, CM). Due to the increased risk of perioperative bleeding and cesarean hysterectomy, obstetricians are generally reluctant to perform a myomectomy during pregnancy or a CM.
- The risks associated with leaving fibroids in the uterus for interval myomectomy may be underestimated, as large fibroids left in situ during cesarean section may result in serious early and late postoperative complications, potentially requiring a repeat laparotomy and/or subsequent hysterectomy. Numerous studies support the feasibility and safety of performing intracapsular myomectomy.
- In certain cases, regardless of the fibroid diameter, myomectomy during pregnancy and CM would be necessary to prevent additional harm or complications.
- Serosal CM, trans-endometrial CM and the intracapsular myomectomy technique are the preferred surgical approaches.
- In addition to minimally invasive surgery that uses energy-based devices to alter surgical times and blood loss, obstetricians should take into account new techniques and their impact on the decision for myomectomy during pregnancy and CM.
- Because of its potential benefits and relatively low risk of complications, CM may also be a useful option in resource-limited settings compared with traditional approaches.
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
REFERENCES
Sparic R, Mirkovic L, Malvasi A, Tinelli A. Epidemiology of Uterine Myomas: A Review. Int J Fertil Steril. 2016;9(4):424–35. | |
Tinelli A, Resta L, Sparic R, Stefanović A, Malvasi A. Pathogenesis, Classification, Histopathology, and Symptomatology of Fibroids. 2018. p. 1–47. | |
Tinelli A, Vinciguerra M, Malvasi A, Andjić M, Babović I, Sparić R. Uterine Fibroids and Diet. Int J Environ Res Public Health. 2021;18(3). | |
Vergara D, Catherino WH, Trojano G, Tinelli A. Vitamin D: Mechanism of Action and Biological Effects in Uterine Fibroids. Nutrients. 2021;13(2). | |
Laughlin SK, Schroeder JC, Baird DD. New directions in the epidemiology of uterine fibroids. Semin Reprod Med. 2010 May;28(3):204-217. | |
Zimmermann A, Bernuit D, Gerlinger C, Schaefers M, Geppert K. Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BMC Womens Health. 2012 Mar 26;12:6. | |
Ramasauskaite D, Purandare N, Diaz I, Kvederaite-Budre G, Beyuo TK, Beyeza-Kashesya J, Jacobsson B. Fibroids and pregnancy. Int J Gynaecol Obstet. 2026 Jan;172(1):51-58 | |
Sparić R, Hatirnaz S, Tinelli A. Editorial: Uterine fibroid surgery in gynecology and obstetrics and reproduction: lights and shadows. Frontiers in Surgery. 2025;12. | |
Pecorella G, Sparic R, Morciano A, Constantin SM, Babovic I, de Rosa F, et al. Mastering nonobstetric surgery in pregnancy: Insights, guidelines evaluation, and point-by-point discussion. Int J Gynaecol Obstet. 2025;168(2):472–483. | |
Tinelli A, Malvasi A, Mynbaev OA, Barbera A, Perrone E, Guido M, et al. The surgical outcome of intracapsular cesarean myomectomy. A match control study. J Matern Fetal Neonatal Med. 2014;27(1):66–71. | |
Sparić R, Kadija S, Stefanović A, Spremović Radjenović S, Likić Ladjević I, Popović J, et al. Cesarean myomectomy in modern obstetrics: More light and fewer shadows. J Obstet Gynaecol Res. 2017;43(5):798–804. | |
Tinelli A, Vinciguerra M, Sparić R, Hatırnaz Ş, Güler O, Kosmas I, et al. Fibroids in Obstetric and Gynecology: Training and Skill in Myomectomy. In: Cinnella G, Beck R, Malvasi A, editors. Practical Guide to Simulation in Delivery Room Emergencies. Cham: Springer International Publishing; 2023. p. 981–1025. | |
Laughlin SK, Baird DD, Savitz DA, Herring AH, Hartmann KE. Prevalence of uterine leiomyomas in the first trimester of pregnancy: an ultrasound-screening study. Obstet Gynecol. 2009;113(3):630–635. | |
Qidwai GI, Caughey AB, Jacoby AF. Obstetric outcomes in women with sonographically identified uterine leiomyomata. Obstet Gynecol. 2006;107(2 Pt 1):376–382. | |
Kwas K, Nowakowska A, Fornalczyk A, Krzycka M, Nowak A, Wilczyński J, et al. Impact of Contraception on Uterine Fibroids. Medicina (Kaunas). 2021;57(7). | |
Chen Y, Lin M, Guo P, Xiao J, Huang X, Xu L, et al. Uterine fibroids increase the risk of hypertensive disorders of pregnancy: a prospective cohort study. J Hypertens. 2021;39(5):1002–1008. | |
Hurst BS, Tinelli A, Malvasi A, Parker WH. Fibroid complications in pregnancy. In: Management and therapy of early pregnancy complications, First and Second Trimesters. Eds: Malvasi A, Tinelli A, Di Renzo GC. Springer International Publishing, Cham, Switzerland 2016, pp. 135–160. | |
Lee HJ, Norwitz ER, Shaw J. Contemporary management of fibroids in pregnancy. Rev Obstet Gynecol. 2010;3(1):20–27. | |
Lev-Toaff AS, Coleman BG, Arger PH, Mintz MC, Arenson RL, Toaff ME. Leiomyomas in pregnancy: sonographic study. Radiology. 1987;164(2):375–380. | |
Katz VL, Dotters DJ, Droegemeuller W. Complications of uterine leiomyomas in pregnancy. Obstet Gynecol. 1989;73(4):593–596. | |
De Carolis S, Fatigante G, Ferrazzani S, Trivellini C, De Santis L, Mancuso S, et al. Uterine myomectomy in pregnant women. Fetal Diagn Ther. 2001;16(2):116–119. | |
Benson CB, Chow JS, Chang-Lee W, Hill JA, 3rd, Doubilet PM. Outcome of pregnancies in women with uterine leiomyomas identified by sonography in the first trimester. J Clin Ultrasound. 2001;29(5):261–264. | |
Norton ME, Merrill J, Cooper BA, Kuller JA, Clyman RI. Neonatal complications after the administration of indomethacin for preterm labor. N Engl J Med. 1993;329(22):1602–1607. | |
Lolis DE, Kalantaridou SN, Makrydimas G, Sotiriadis A, Navrozoglou I, Zikopoulos K, et al. Successful myomectomy during pregnancy. Hum Reprod. 2003;18(8):1699–1702. | |
Parton JR, Arshad I. Antenatal myomectomy of huge pedunculated fibroid. BMJ Case Rep. 2024;17(1). | |
Edney R, Yap C, Childs S, Das S, Fagan P. Second trimester semi-elective abdominal myomectomy to manage severe systemic inflammatory response syndrome secondary to fibroid degeneration. BMJ Case Rep. 2025;18(7). | |
Spyropoulou K, Kosmas I, Tsakiridis I, Mamopoulos A, Kalogiannidis I, Athanasiadis A, et al. Myomectomy during pregnancy: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2020;254:15–24. | |
Tinelli A, Kosmas IP, Carugno JT, Carp H, Malvasi A, Cohen SB, et al. Uterine rupture during pregnancy: The URIDA (uterine rupture international data acquisition) study. Int J Gynaecol Obstet. 2022;157(1):76–84. | |
Bonney V. “Caesarean Myomectomy”; Remarks on the Operation. Proc R Soc Med. 1914; 7:121–123. | |
Burton CA, Grimes DA, March CM. Surgical management of leiomyomata during pregnancy. Obstet Gynecol. 1989;74:707–709. | |
Malvasi A, Stark M, Tinelli A. Cesarean myomectomy. In: Tinelli A, Malvasi A (eds) Uterine myoma, myomectomy and minimally invasive treatments, 1st edn. Berlin: Springer, 2015; 237–252. | |
Song D, Zhang W, Chames MC, Guo J. Myomectomy during cesarean delivery. Int J Gynaecol Obstet. 2013 Jun;121(3):208–213. | |
Pergialiotis V, Sinanidis I, Louloudis IE, Vichos T, Perrea DN, Doumouchtsis SK. Perioperative Complications of Cesarean Delivery Myomectomy: A Meta-analysis. Obstet Gynecol. 2017 Dec;130(6):1295–1303. | |
Goyal M, Dawood AS, Elbohoty SB, Abbas AM, Singh P, Melana N, Singh S. Cesarean myomectomy in the last ten years; A true shift from contraindication to indication: A systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2021 Jan;256:145–157. | |
Youshanloie MM, Vaezi M, Pashazadeh F. Consequences of Concurrent Myomectomy and Caesarean Section versus Caesarean Section Alone in the Last Two Decades: Systematic Review and Meta-Analysis. Current Women`s Health Reviews. 2023;19:133–146. | |
Huang Y, Ming X, Li Z. Feasibility and safety of performing cesarean myomectomy: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2022 Jul;35(13):2619–2627. | |
Dey T, Cole MG, Brown D, Hill RA, Chaplin M, Huffstetler HE, Curtis F. Caesarean myomectomy in pregnant women with uterine fibroids. Cochrane Database Syst Rev. 2025 Jan 27;1(1):CD016119. | |
Tinelli A, Nezhat CH, Likić-Ladjević I, Andjić M, Tomašević D, Papoutsis D, Stefanović R, Sparić R. Myomectomy during cesarean section or non-caesarean myomectomy in reproductive surgery: this is the dilemma. Clin. Exp. Obstet. Gynecol. 2021;48(6):1250–1258. | |
Akkurt MO, Yavuz A, Eris Yalcin S, Akkurt I, Turan OT, Yalcin Y, Sezik M. Can we consider cesarean myomectomy as a safe procedure without long-term outcome? J Matern Fetal Neonatal Med. 2017 Aug;30(15):1855–1860. | |
Adesiyun AG, Ojabo A, Durosinlorun-Mohammed A. Fertility and obstetric outcome after caesarean myomectomy. J Obstet Gynaecol. 2008 Oct;28(7):710–712. | |
Tinelli A, Vinciguerra M, Malvasi A, Stark M. Cesarean section in the setting of fibroid uterus and cesarean myomectomy. In book: Fibroid Uterus: Surgical challenges in minimal access surgery, CRC Press, 2020. p. 120–143. | |
Tinelli A, Vinciguerra M, Sparic R, Hartinaz S, Guler O, Kosmas I, Spyropoulou K, Stark M. Fibroids in obstetrics & gynecology: training and skill in myomectomy. In: Practical guide to simulation in delivery room emergencies. Eds: Cinnella G, Beck R, Malvasi A. Springer, Cham, 2023, pp. 981–1025. | |
Tinelli A, Mynbaev OA, Vergara D, Di Tommaso S, Gerli S, Favilli A, Mazzon I, Sparic R, Eliseeva M, Simakov SS, Danilov AA, Malvasi A. Uterine-preserving operative therapy of uterus myomatosus. In: Hysterectomy – a practical guide. Eds: Alkatout I, Mettler L. Springer International Publishing, Switzerland 2018, pp. 429–466. | |
Tinelli A, Malvasi A. Fibroids and myomectomy in cesarean delivery. In: Cesarean delivery: a comprehensive illustrated practical guide. Eds: Di Renzo GC, Malvasi A. CRC Press, Taylor & Francis Group, Boca Ranton (FL), USA, 2016, pp. 173–188. | |
Stark M, Odent M, Tinelli A, Malvasi A, Jauniaux E. Cesarean section: the evidence-based technique, complications and risks. In Book: Management and therapy of late pregnancy complications, Third Trimester and Puerperium. Eds: Malvasi A, Tinelli A, Di Renzo GC. Springer International Publishing, Cham, Switzerland 2017, pp. 209–231. | |
Cubo-Abert M, Simó-González M, Haimovich S, Melé-Olivé L, Alcázar-Zambrano JL, Gatius S, Muñiz N, Vera-Cartas M, Mestres-Betsebé E, Amés-Trigo C, Calvo-Redol AR, Tinelli A. The importance of the pseudocapsule in the management of uterine myoma: State of the art and expert recommendations. Int J Gynaecol Obstet. 2025 Nov;171(2):639–645. | |
Hatırnaz Ş, Güler O, Başaranoğlu S, Tokgöz C, Kılıç GS. Endometrial myomectomy: a novel surgical method during cesarean section. J Matern Fetal Neonatal Med. 2018;31:433–438. | |
Huang SY, Shaw SW, Su SY, Li WF, Peng HH, Cheng PJ. The impact of a novel transendometrial approach for caesarean myomectomy on obstetric outcomes of subsequent pregnancy: a longitudinal panel study. BJOG. 2018;125:495–500. | |
Hatırnaz Ş, Güler O, Başbuğ A, Çetinkaya MB, Kanat-Pektaş M, Bakay K, Çelik S, Şentürk Ş, Soyer-Çalışkan C, Gürçağlar A, Şahin B, Kalkan Ü, Çelik H, Kalyoncu Ş, Bıyık İ, Yassa M, Erol O, Akarsu S, Turhan U, Ulubaşoğlu H, Sparic R, Tinelli A. A Comparative Multicentric Study on Serosal and Endometrial Myomectomy During Cesarean Section: Surgical Outcomes. J Invest Surg. 2021 Jul;34(7):687–694. | |
Wang Q, Lin J, Dai Y. Outcomes of cesarean myomectomy via trans-endometrial approach in women with single intramural fibroid in the posterior uterine wall. J Matern Fetal Neonatal Med. 2023;36:2232655. | |
Shi C, Chen J, Chen A. Clinical outcome analysis of intramural myoma greater than 8 cm in diameter removed during caesarean section: a retrospective study. BMC Womens Health. 2023;23:60. | |
Yıldırım Karaca S, Kantarcı S, Adıyeke M, Bulut S, Özcan A, Rabia Şenkaya A, İleri A. Comparison of transendometrial myomectomy versus conventional myomectomy in cesarean section. Eur J Obstet Gynecol Reprod Biol. 2021 Dec;267:68–72. | |
Güler O, Hatırnaz Ş, Sparic R, Basbug A, Erol O, Kalkan Ü, Ulubaşoğlu H, Trojano G, Ürkmez SS, Tinelli A. Long-term obstetric, perinatal, and surgical complications in singleton pregnancies following previous cesarean myomectomy: a retrospective multicentric study. Front Surg. 2024 Aug 1;11:1430439. | |
Tabakova N, Sparić R, Tinelli A. Reflections on Postpartum Hysterectomy as a Possible Complication of Cesarean Myomectomy: A Long Debate. Medicina (Kaunas). 2024 Apr 4;60(4):594. | |
Sparić R, Andrić L, Guler O, Malvasi A, Babović I, Hatirnaz S, Dellino M, Tinelli A. Cesarean Myomectomy: Reflections on Clinical and Surgical Controversies between a New Trans-Decidual Technique vs. Traditional Method. Medicina (Kaunas). 2024 Apr 8;60(4):609. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)