Fertility Awareness Methods of Family Planning for Achieving or Avoiding Pregnancy
Authors
INTRODUCTION
The term fertility awareness is used to describe an individual's understanding of male and female reproductive anatomy and physiology as it relates to fertility. For a woman it includes being able to identify the fertile time during her menstrual cycle. For a man it includes understanding his own reproductive potential. For a couple it includes developing a shared understanding about their fertility potential at different stages of their lives and their ability to communicate about fertility issues with each other and with health professionals. Knowledge about fertility awareness is fundamental to making informed decisions about reproductive and sexual health.1 There are key opportunities for health and educational professionals to offer information about fertility awareness and encourage individuals to become more aware about the changes that occur in their own bodies at different times of their life, for example: during puberty; when considering choice of appropriate family planning methods; when making sexual and reproductive health decisions; during pre-conception; during breastfeeding; and during the peri-menopause.2
Information about fertility awareness helps young people understand the normal variations in the age individuals reach puberty, normal variations in the genitals and breast development, and the normal variation of menstrual cycles. Information about fertility awareness is also useful in clarifying the difference between a normal physiological discharge caused by cervical secretions and an abnormal discharge caused by a sexually transmitted infection, as well as increasing awareness that if sexually transmitted infections are not treated then the fallopian tubes or vas deferens may be infected, potentially resulting in infertility. During family planning consultations, fertility awareness improves people's understanding about how each method of family planning prevents fertilization taking place and how if the method is not used correctly, then the risk of pregnancy will increase. For example, how the combined oral contraceptive pill prevents ovulation and makes the cervical secretions thick and impenetrable to sperm as well as understanding how fertility can quickly return if pills are not taken as directed.3
This chapter focuses on how fertility awareness can be used as a method of family planning, either to achieve or to avoid pregnancy. It offers an overview of the scientific understanding of fertility awareness methods (FAMs) and describes the practical application of the knowledge to manage and counsel couples wishing to use each method. It also describes how fertility awareness knowledge can be used alongside other methods of family planning such as barrier methods and the withdrawal method. It describes how fertility returns after discontinuing hormonal contraception or breastfeeding and how fertility decline can be monitored during the peri-menopause. Finally it describes how couples can utilize technology at home to monitor their potential fertility and cyclic changes in fertility.
FERTILITY AWARENESS METHODS
FAMs include all family planning methods based on the identification of the fertile time.4 This knowledge can be used to plan or avoid pregnancy. FAMs depends on two key variables, the accurate identification of the fertile days of a woman's menstrual cycle (the fertile time) and the modification of sexual behavior, either to target intercourse to plan or to avoid a pregnancy.5
The effectiveness of FAMs to avoid pregnancy depends on the ability of couples to abstain from intercourse during the fertile time (natural family planning) or to use a barrier method consistently during the fertile time (fertility knowledge with barriers).
History of Fertility Awareness Methods
Men and women have been fascinated by reproductive physiology and ways to plan or avoid pregnancy throughout history. The scientific identification of the fertile time originated in the 1930s when Dr. Ogino in Japan and Dr. Knaus in Austria independently observed that ovulation occurred at a fixed interval of approximately 14 days before the next menstruation. This formed the basis of the rhythm or calendar method.6 In the 1950s, new methods of fertility control were developed based on the physiological signs of ovulation. Drs. John and Evelyn Billings in Melbourne, Australia pioneered a method based on the changes in cervical mucus secretions.7 Dr. John Marshall in London developed the temperature method.8 In the 1970s, Edward Keefe first described cyclic changes in the cervix.9 Over time it was realized that combining two or more of the fertility indicators resulted in a more effective method. Combining indicators has been variously described as the sympto-thermal method,10 the muco-thermic method,11 or the double check method.12
In 1972, the World Health Organization (WHO) established a task force on methods for the prediction and detection of ovulation. One of the major objectives was to develop an accurate, easy, and cheap test that could be used in the home to predict the start and end of the fertile time. WHO research13 on numerous markers of fertility found that the most accurate determinants of the start of the fertile time was the increase of oestrone-3-glucoronide (E-3-G) in urine, and the luteinizing hormone (LH) surge provides the most accurate marker of ovulation and predicting the end of the fertile time. In 1996, the first personal hormone monitoring system an immuno-chemical self-test was launched.14 While researching highly sophisticated and technologically advanced natural methods, the challenge still remained to provide reliable, simple, low-cost methods. The Standard Days Method (fixed formula)15 and the TwoDay Method16 are more recent developments in this area. Table 1 summarizes the key concepts in the understanding of the fertile time from the fourth century BC when jumping up and down was a popular contraceptive idea to the technological sophistication of the 21st century pinpointing the fertile time.
Table 1. The history of fertility awareness methods of family planning
| Dates | Key names | Development of physiological methods to avoid pregnancy |
| 4th C B | Hippocrates | Advised women to “jump so that the buttocks are touched by the feet” |
| 3rd C BC | Aristotle | Conception was most likely immediately before or after menstruation |
| 2nd C AD | Soranus | Conception more likely if the woman has an orgasm (dilates uterus); to avoid conception, women were advised to abstain during the fertile time (Aristotle's theory); hold their breath, not move during intercourse, move away before ejaculation; then get up immediately, squat, promote sneezing, wipe the vagina, and have a cold drink |
| 9th C AD | Rhazes | Advised women to rise roughly immediately after ejaculation, sneeze, and blow their nose several times and call out in a loud noise while jumping violently backwards |
| 1600 | Fallopius | Discovered and christened the Fallopian tubes |
| 1662 | Van Horne | The “female testicles” were renamed the ovaries |
| 1869 | Squires | Noted a decrease in a woman's basal body temperature at the onset of menstruation but did not appreciate the significance of the preceding rise |
| 1928 | Van de Velde | Related the higher temperature in the latter part of the cycle to the activity of the corpus luteum |
| 1928 | Ogino (Japan) Knaus (Austria) | Independently established that ovulation occurs 12–16 days before the onset of the next menstrual period |
| 1937 | Rubinstein & Lindsley | Related increase in basal body temperature to evidence of ovulation (vaginal smears), several researchers then correlated basal body temperature increase with other indicators of ovulation |
| 1950s | JGH Holt | A Dutch gynecologist, first presented basal body temperature method to couples in an intelligible manner to regulate births. |
| 1959 | John Marshall | John Marshall introduced Holt's approach into the UK |
| 1968 | John Marshall | First prospective field trial of the basal body temperature method, published in the Lancet |
| 1968 | John & Evelyn Billings | Developed knowledge about the role of cervical secretions into natural family planning methodology—The Billings Ovulation Method |
| 1968 | Dr John Marshall | Questionnaire survey of psychological experiences of couples in the BBT field trial published in Fertility and Sterility |
| 1977 | Edward F Keefe | Developed methodology related to self-palpation of the cervix |
| 1981 | WHO | First prospective trials of the Ovulation Method (cervical secretions only) |
| 1981 | Rice et al US ‘Fairfield Trial’ | The effectiveness of combining the indicators of fertility was increasingly recognized through prospective studies |
| 1988 | Bellagio, Italy | Lactational amenorrhoea method—consensus statement in the Lancet |
| 1995 | Wilcox, US | Hormonal assays and ultrasound determine the fertile time lasts from 5 days before to the estimated day of ovulation |
| 1999 | Unipath UK ‘Persona’ | A hand-held computerized device measures changes in urinary estrone-3-glucoronide (E-3-G) and LH by means of a simple urine dipstick |
| 1999 | Arevalo, US | Introduction of the Standard Days Method (fixed formula: 8–19) rule |
| 2001 | Jennings, V | The TwoDay Method based on the presence or absence of cervical secretions |
(Adapted from: Green S, The curious history of contraception, Ebury Press, London 1971. Mucharski J, History of the Biologic Control of Human Fertility, Oakridge, New Jersey USA 1982; Belfield T, BBC Radio 4—From Crocodile Dung to Electrocution, BBC Radio 4, Jan 2001; and data on file including published papers.)
Physiology: Defining the Fertile Time
FAMs are based on an understanding of reproductive physiology. Fig. 1 summarizes the physiological changes that occur during the menstrual cycle and the observed indicators of fertility.
|
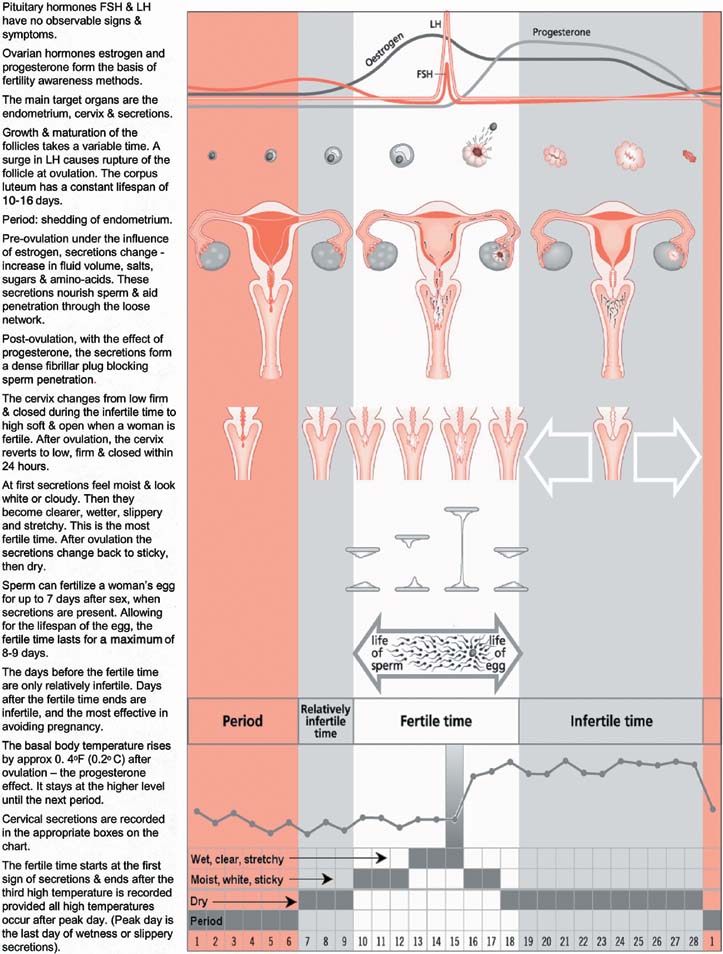
The hypothalamus secretes pulses of gonadotrophin-releasing hormone (GnRH) to regulate the pituitary output of follicle stimulating hormone (FSH) and LH. FSH and LH act on the ovaries to stimulate the production of the ovarian hormones, estrogen, and progesterone. In the first half of the cycle (the follicular phase), FSH controls follicular growth, the growing follicles secrete estrogen, and a surge of LH triggers ovulation. The ruptured follicle develops into the corpus luteum and secretes progesterone. Estrogen and progesterone in turn affect the target organs—the endometrium (lining of the uterus), the cervix and cervical secretions and the breasts. Progesterone also has a thermogenic effect causing an increase in basal body temperature. If the egg is not fertilized, estrogen and progesterone levels decrease and the endometrium is shed at the next menstruation. In addition to its role in controlling the menstrual cycle, the hypothalamus also controls body temperature, sleep, thirst, appetite, and fluid balance. Disturbances to these bodily processes can affect the hypothalamic function and hence cause menstrual disturbances.
Baerwald evaluated changes in the ovarian follicle dynamics during the menstrual cycle.17 She found that women ovulate only once per cycle. However, women experience multiple waves of follicular development each cycle, but only one of these waves results in an actual ovulation. In 100% of the women they studied, a wave of follicular development occurred in the first half of the menstrual cycle and culminated in ovulation around the middle of the cycle. This was followed by additional follicular waves that never resulted in an ovulation.
The fertile time (days of potential fertility) is defined by the WHO as the time from the first act of intercourse, which may lead to pregnancy, to the demise of the ovum.13 The fertile time lasts for an average of 6 days. To identify the fertile time during each menstrual cycle, it is essential to know the lifespan of the sperm in the female genital tract before ovulation, the timing of ovulation, and the length of time during which the ovum can be fertilized after ovulation.
The lifespan of the sperm is up to 7 days. In the female genital tract, the survival of the sperm depends on the presence of alkaline cervical secretions (mucus), produced from the secreting cells lining the cervix. In the absence of cervical secretions, the acidic vaginal environment will rapidly destroy sperm.18, 19 In the presence of fertile secretions, sperm will live an average of 3 days, with a 99% probability that the survival time is less than 7 days.20 The average life span of the ovum is approximately 17 hours.21 Fertilization must take place during those few hours after ovulation if pregnancy is to occur.
Detection of Ovulation and Correlation With the Indicators of Fertility
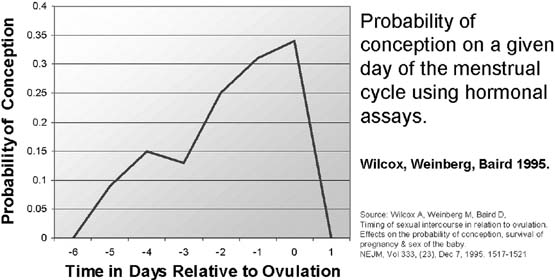
Ultrasound gives the most accurate information on the time of ovulation. Ultrasound studies have shown that the temperature increase and cervical secretion changes are accurate in indicating the time of ovulation.22 Ovulation can also be detected by hormone assays in plasma or urine.23 In the North Carolina Early Pregnancy Study, Wilcox researched the chances of conception on each day of the menstrual cycle.24 The estimated day of ovulation was determined by ratios of urinary metabolites of estrogen and progesterone. They identified the limits of the fertile window from 6 days before to 1 day after ovulation (Fig. 2).
|
Dunson25 compared the North Carolina data with the Barrett and Marshall data26 that used the basal body temperature (BBT) increase as a marker of ovulation. They used a new statistical model to correct for errors in estimating the day of ovulation. They suggested that BBT-based estimates of the day of ovulation are not perfect but have a high probability of being ± 1 day of the true ovulation day. They estimated the same 6-day fertile window in both studies after controlling for error.
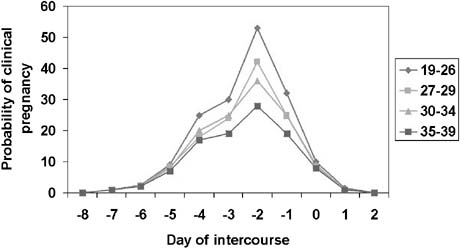
The probability of conception on a given day of the cycle was also analyzed using data from a large prospective European study of 782 women aged 18–40 who kept daily records of waking temperature, cervical secretions, menstruation, and intercourse. Nearly all pregnancies occurred within a 6-day fertile window. This analysis included a review of the effects of age on conception rate. There was no evidence for a shorter fertile window in older men or women. The team concluded that women's fertility begins to decrease in the late 20s, with substantial decreases by the late 30s. Fertility for men is less affected by age but shows significant decline by the late 30s27 (Fig. 3).
|
Further research on the probability of conception on each day of the cycle is required to more clearly define the outer limits of the fertile time. This will require larger studies that use more precise markers of ovulation and more detailed data on intercourse frequency.
Cycle Length Variability
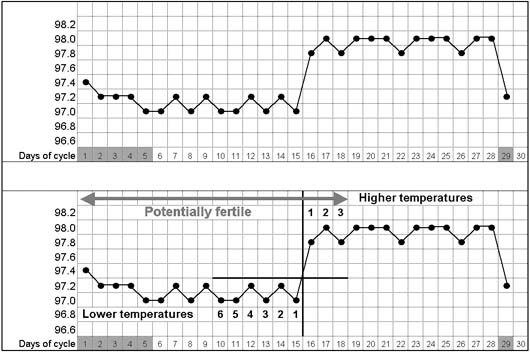
The length of a menstrual cycle is measured from the first day of menstruation, (the first day of fresh red bleeding) up to, but not including, the first day of the next menstruation. The position of the fertile time will vary according to the length of the cycle. The time from ovulation to the next menstruation is likely to be constant (approximately 10–16 days), whereas the time before ovulation is more variable (Fig. 4).
|
It is important that women understand that there is a wide variation in normal cycle length that is compatible with good health so that they do not become overly concerned by the 28-day ideal.28 In 1977 Vollman29 evaluated the variability in cycle length. The 28-day cycle was the commonest length cycle recorded but only in 12.4% of cycles. Cycle length is most variable in the first few years after the menarche and in the years preceding the menopause. A woman's age minus her age at menarche (her gynecological age) is also an important factor when considering cycle length and regularity. Cycle length changes with age, forming a U-shape curve from the menarche to menopause. The mean cycle length decreases from 35 days at age 12 to a minimum of 27 days at age 43, increasing to 52 days at age 55 years, with an enormous range of cycle length.
A large Danish study (n = 3743) investigated the epidemiology of menstrual patterns among women of fertile age (15–44) and confirmed the normally used definitions of polymenorrhea (cycle length less than 21 days) and oligomenorrhea (cycle length between 36 and 90 days). The high frequency in a normal population of large menstrual cycle length variation challenges the view that an intraindividual variation of more than 5 days should be regarded as a sign of disease in women.30
Methods Used to Identify the Fertile Time
The fertile time can be identified by using three different approaches—observing physiological indicators; using a calculation based on cycle length, or by using fertility monitoring devices. The first approach—observing the physiological indicators of fertility (the observed indicators)—may include recording the basal body temperature (BBT); monitoring cervical secretions either by observing the changing characteristics or by the more simplified TwoDay Method and possibly by recording the changes in the cervix. The second way to identify the fertile time is by using calculations based on cycle length—either personalized information based on a woman's previous cycle lengths or a more simplified Standard Days Method. Finally the fertile time can be identified by using fertility monitoring devices such as personal hormone monitoring systems, and saliva testing devices. The methodology, effectiveness and evidence-base of these approaches will be discussed. The knowledge gained about the fertile time through these methods can then be used to either plan or avoid a pregnancy.
The Observed Indicators
Women are taught to observe, record, and interpret the changes in one or more of the following indicators of fertility to identify the fertile time: the BBT, the cervical secretions, and the cervix. Each of these indicators of fertility will change in response to the increasing and decreasing levels of estrogen and progesterone during the menstrual cycle. These indicators may be used alone to identify the fertile time but are more commonly combined to improve the effectiveness to avoid a pregnancy.
MONITORING BASAL BODY TEMPERATURE
This section describes the monitoring of basal body temperature as a single indicator to identify the fertile time. Progesterone causes an increase in BBT (waking temperature), defined as the temperature before getting out of bed and after resting for at least 3 hours. After menstruation the temperature stays at the lower level. Immediately after ovulation progesterone increases the temperature by at least 0.4°F (0.2°C). The higher temperature is maintained until the progesterone decreases at menstruation. Digital thermometers or mercury fertility thermometers can be prescribed. These help to ensure accurate recordings. Simplified charts (Fig. 5) can be downloaded from www.fertilityuk.org. Couples using the temperature as a single indicator method have to abstain from intercourse from the beginning of menstruation until they have recorded three temperatures at least 0.4°F (0.2°C) higher than the preceding six31(Fig. 6).
|

|
Body temperature is influenced by the circadian rhythm or internal body clock, with the temperature being at its lowest in the early hours of the morning, then rising by approximately 0.2°F (0.1°C) for every hour spent in bed. If the reading is not taken within 1 hour of the target time then the actual time should be recorded and a note made that this reading is less reliable when interpreting the chart. Other factors or events that may disturb temperature readings include poor equipment or recording technique, alcohol, late night or disturbed night, oversleeping, illness causing low-grade pyrexia (fever), or medication such as antipyretics. It is therefore important to record any disturbed readings. Using temperature as a single indicator requires an average of 16 days of abstinence each cycle, because the couple have to abstain from intercourse until the temperature has remained at the higher level for 3 days. For couples planning a pregnancy, temperature recording is of no value in predicting ovulation. In summary, using temperature as a single indicator, there is no indication of the start of the fertile time. The fertile time ends after three high temperatures are recorded (at least 0.4°F (0.2°C) above the preceding six.
Barrett and Marshall researched the chances of conception on each day of the menstrual cycle.26 They used the rise of basal body temperature to estimate the time of ovulation. All the conceptions occurred during the fertile window extending from 5 days before to 1 day after the temperature rise. The chances of conception approximated to zero, 6 days before the day of the temperature rise, and 2 days after the temperature rise (Fig. 7).
|

The Effectiveness of Using BBT as a Single Indicator
In a study of 351 participants, using temperature as a single indicator of fertility, the overall failure rate was 5.4% compared with a method failure rate of 1%. This finding illustrates that the temperature method is only effective if used by highly motivated couples who are able to tolerate at least two weeks abstinence, because they have to abstain from the start of the cycle until after the temperature increase.31
MONITORING CERVICAL SECRETIONS
This section describes the monitoring of cervical secretions as a single indicator to identify the fertile time. Slight variations in the guidelines are used by the Billings Ovulation Method and the Creighton Model.
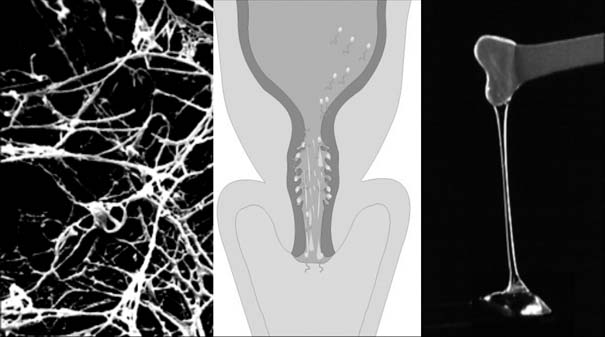
The hormones, estrogen, and progesterone influence the quantity and the quality of cervical secretions (Figs. 8, 9, and 10). The different types of secretions either impede or encourage sperm motility and this determines the state of fertility.7, 32
|

|
|
When the estrogen levels are low, there are minimal white, thick, and sticky secretions present at the cervix. The sperm are rapidly destroyed in the acidic environment of the vagina.
The rising levels of estrogen alter the cervical secretions from being thick and sticky to becoming gradually more transparent, wetter, and stretchier. The secretions become more fluid because of increased water content. The sperm move easily in these fertile secretions, which facilitate their movement upwards through the genital tract (Fig. 9). Chretien has recently confirmed Odeblad's33 earlier research that there is a close relationship between the three-dimensional arrangement of the secretion framework and the ability of sperm to move rapidly in a given direction.34 Some of the sperm rest in small pockets (crypts) in the mucosal lining of the cervix before swimming up through the uterus. The last day of the wet, transparent, slippery, stretchy secretions is known as peak day. This day coincides closely with ovulation.35 Peak day can only be recognized retrospectively on the day following peak when the cervical secretions have become sticky or dry again.
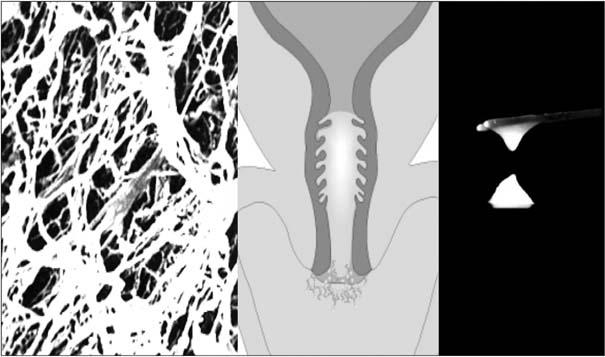
Immediately after ovulation under the influence of progesterone, the cervical secretions become white, thick, and sticky and form a sticky plug in the cervix, which is antagonistic to sperm penetration (Fig. 10). In summary—using the cervical secretions as a single indicator—the fertile time starts when a woman is first aware of any cervical secretions and the fertile time ends on the fourth morning after peak day (the last day showing the most fertile characteristics).
The WHO multicenter study reported that 94% of women could detect changes in cervical secretions indicating the start of the fertile time. Most women need to observe the secretions for approximately three cycles before recognizing the changes with confidence.36 Changes in secretions can be masked by seminal fluid, spermicide, or vaginal infections. The Billings Ovulation Method37 and the Creighton Model, Napro Education Technology, described by Hilgers38 use cervical secretions only.
A recent re-analysis of data from four small published studies (108 cycles) compared the observation of the peak day of cervical secretions with urinary LH. Cycle lengths ranged from 22 to 75 days (mean cycle length 29.4); 93 of the cycles had both an identified peak day and LH surge; 97.8% of the peak days fell within ± 4 days of the LH surge. The analysis concluded that the peak day is very accurate in identifying maximum fertility and fairly accurate in identifying the day of ovulation and the end of the fertile time.39
The Effectiveness of Using the Cervical Secretions as a Single Indicator
A WHO multicenter study40 involving 725 participants showed that if couples are given good natural family planning (NFP) teaching and who follow the instructions correctly, then the cervical secretion indicator has a failure rate of approximately 3%. Such a low rate only occurs with perfect use. However, with typical use, which included cycles in which the method was used correctly and in cycles in which it was not, the study showed an overall failure rate of nearly 20%. In 1990, Trussell critically appraised the overall design of the WHO study.41
The TwoDay Method
The TwoDay Method may provide a simplified method for populations with unmet family planning needs. The TwoDay method16 involves women being taught to monitor whether vaginal secretions are present or absent. The women are taught to monitor their secretions each afternoon and evening, either by a feeling of dampness at the entrance to the vagina or by observing the secretions. Assuming that most couples have intercourse in the late evening or early morning, monitoring at these times avoids confusion between seminal fluid and cervical secretions. The women are taught to ask two simple questions:
- Did I note secretions today?
- Did I note secretions yesterday?
If a woman notices any secretions (today or yesterday), she is probably fertile and needs to abstain from intercourse if she wishes to avoid pregnancy. If a woman does not notice secretions on either day, she is unlikely to be fertile. The estimated mean length of the fertile time (length of abstinence) for couples practicing the TwoDay Method is approximately 10 days. As it is not uncommon for women to notice some secretions in the luteal phase as hormone levels fluctuate, the simple TwoDay Method may be found to require more lengthy times of abstinence.
The TwoDay Method is based on a theoretical model. Secondary analysis42 of the data on cervical secretions from a large multinational European fecundability study assessed the relationship between the days predicted to be potentially fertile by the TwoDay Method and the day-specific probabilities of pregnancy based on 434 conception cycles. The authors concluded that if intercourse occurs on any given day relative to ovulation, the presence of cervical secretions was associated with a two-fold increase in the probability of conception. The Institute for Reproductive Health, Georgetown University has conducted a clinical trial of the TwoDay Method to assess the acceptability and the effectiveness.43 The first-year pregnancy rate was 3.5 (pregnancies per 100 women/years) with correct use of the method (pregnancies and cycles with no intercourse on identified fertile days), 6.3 with use of a backup method on the fertile days, and 13.7 including all cycles and all pregnancies in the analysis.
MONITORING THE CHANGES IN THE CERVIX
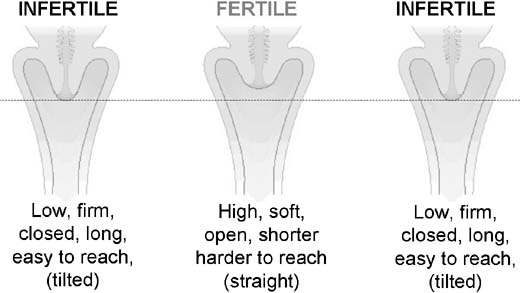
This section describes the monitoring of changes in the cervix. Estrogen and progesterone cause subtle changes (Fig. 11) in the muscle and connective tissue of the cervix.9 Women can learn to recognize these changes by gently palpating the cervix at approximately the same time each day. A woman may notice whether the cervix is low or high in the vagina, firm or soft to touch, and closed or slightly open. It takes several months to be confident in using cervical signs. Palpating the cervix is rarely used alone as a single indicator, but the cervix changes are of particular value to women with long cycles, during breastfeeding when observing returning fertility, and during the perimenopausal years. Using the cervical changes—The fertile time starts at the first sign of the cervix becoming high, soft or open and the fertile time ends after the cervix has been low, firm and closed for three days.
|
The Effectiveness of Using the Cervix as a Single Indicator
There are no effectiveness studies using the cervix indicator alone. A Canadian study44 confirmed that the cervix changes correlate with the cervical secretion and temperature indicators in identifying the fertile time.
Less Precise Indicators of Fertility
Estrogen and progesterone may cause other recognizable changes. These may include abdominal pain, abdominal heaviness, breast changes, intermenstrual bleeding, back pain, skin changes, and changes in libido and mood. Although in individual women the changes may be consistent, they should not be relied on to indicate the fertile time.34 Women must not automatically assume that these changes are physiological when they could be pathological.
A CALCULATION BASED ON CYCLE LENGTH
This section describes ways to identify the fertile time by using calculations either based on personal information about previous cycle lengths or a more simplified Standard Days Method. A calculation to identify the fertile time may be useful to those women who do not wish to observe and interpret their indicators of fertility, to women who have literacy and language difficulties, and to couples who do not have access to other methods of family planning.
Calculation Based on a Woman's Previous Six to Twelve Cycle Lengths
The calculation is based on a woman knowing the length of her previous six to 12 menstrual cycles. The lengths of the shortest and longest cycles are used to identify the likely fertile time. The calculation takes into account the life of the sperm and ovum to estimate the likely fertile time. The fertile time includes the whole of the first and the last fertile days. If a woman's longest or shortest menstrual cycle length changes, she recalculates her fertile time. The shortest cycle minus 20 gives the First Fertile Day and the Longest cycle minus 10 gives the Last Fertile Day.
The Effectiveness of Using the Calculation Based on Knowledge of Past Cycle Lengths
Kambic and Lamprecht reviewed the effectiveness of calendar methods.45 The overall failure rates averaged approximately 20%, ranging from 5% to 47%. Although present research indicates that the calendar method is not sufficiently reliable to be recommended as a single indicator, the information gained by recording cycle lengths is useful when combining indicators.
A Fixed Fertile Time of Days 8 to 19: The Standard Days Method
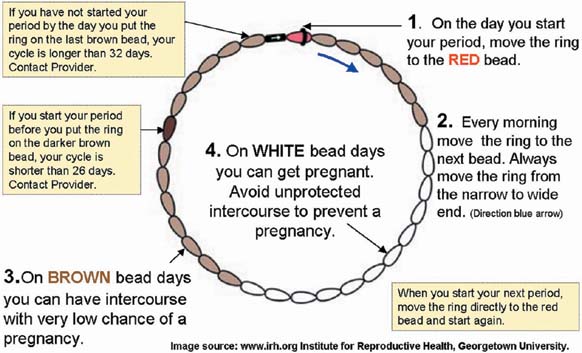
For those women with cycle lengths between 26 and 32 days, the Standard Days Method states that the fertile time is likely to occur within days 8 to 19 of the menstrual cycle. The Standard Days method was derived from analyzing a large data set from a WHO study40 and estimating the theoretical probability of pregnancy on different days of the menstrual cycle. This provides the basis of a simple method.15, 46, 47 The fertile time starts on day 8 and ends on day 19.
The Institute for Reproductive Health at Georgetown University have tested a simple bead method for recording the standard days. To use beads, a woman simply moves a black ring over a series of color-coded beads that represent her fertile and low-fertility days (Fig. 12).
|
In the North Carolina Early Pregnancy Study, Wilcox suggests the identification of a short fixed fertile window (between days 10 and 17) was highly unpredictable.48 However, this analysis included women with cycle lengths varying between 19 and 60 days, which would inevitably result in a far more unpredictable fertile time compared with women with cycle lengths 26 to 32 days, in which the Standard Days Method could be applied.
The Effectiveness of Using the Standard Days Method
A multicenter efficacy trial49 was conducted to test the contraceptive efficacy of the Standard Days Method. It included 478 women aged 18–39 years from Bolivia, Peru, and the Philippines with self-cycle lengths 26–32 days desiring to delay a pregnancy for at least 1 year. Unprotected intercourse occurred in only 3% cycles during days 8–19; 43 women out of 478 conceived (n = 4035 cycles). A single decrement multicensoring life table analysis of the data indicated a cumulative probability of pregnancy of 4.75% over 13 cycles of correct use of the method and 11.96% probability of pregnancy under typical use. However, this potentially higher failure rate should be compared with approximately 80–90% probability of pregnancy in 1 year for young couples who use no family planning method.50
FERTILITY-MONITORING DEVICES
Personal Hormone Monitoring
A personal hormone monitoring system (Fig. 13) designed to avoid pregnancy consists of a small hand-held electronic monitor and simple disposable urine test sticks. The sticks collect information about the levels of hormones and the monitor reads and interprets this information. The monitor measures two hormones, E3G, which is a urinary metabolite of estrogen, and LH. The fertile time is indicated by red-light days and the infertile time is indicated by green-light days.
|

This device can be used as a stand-alone method or in conjunction with other fertility indicators. Many women find the device helpful while they are learning to identify their fertility signs. It provides a more objective marker of the start and end of fertility. Well-informed women can use the method more intelligently and recognize which indicators may be affected by illness or stress. An independent European prospective study of 710 women with regular menstrual cycles (23–35 days) using Persona alone showed a method failure rate of 6.2%.14
Other fertility-monitoring devices have been designed to help women achieve pregnancy. Clearblue Easy Fertility Monitor also monitors E3G and LH, but the algorithm is set with a shorter fertile time, aiming to identify the days of high fertility.51 Modified versions of this fertility monitor have been used in a large randomized controlled trial—The Oxford Conception Study—that aims to determine whether or not information about potential fertility from a device that monitors urinary hormones will increase the conception rate in women wishing to conceive. One third of women were randomized to receive information from the fertility monitor about the early fertile time (from the first rise in E3G until the LH surge is detected), one third received information about the late fertile time (the onset of the LH surge and the following 2 days), and a third did not receive any information (control group). All the women were followed up for 6 months or until they were pregnant. A total of 1453 women were recruited into the study. A full description of the study methods has been reported.52
Luteinizing Hormone Sticks
Urinary LH dipsticks are widely marketed toward women wishing to achieve a pregnancy. LH kits only identify a short fertile time from the start of the LH surge to ovulation. Further research is required to investigate the effectiveness and acceptability of these hormone-monitoring devices to achieve a pregnancy.
Computerized Thermometers
Several devices combine an electronic thermometer with a small computer. The computer combines information about the temperature with a calculation based on cycle length. The display indicates the fertile and infertile times. Examples include Bioself,53 Ladycomp/Babycomp,54 and Cyclotest.55 More rigorous research is needed to evaluate the effectiveness of these devices.
Saliva Testing Devices
The ferning effect of estrogenized cervical secretions has been well-documented for many years in laboratory conditions.56 This effect has also been observed in saliva under laboratory conditions. Over the past few years there has been an increasing number of saliva testing devices marketed directly to the public, mainly through the Internet. They have not been subject to rigorous research and cannot be recommended for contraceptive purposes. The devices use a small plastic microscope to detect a possible ferning pattern as an indicator of fertility.
Braat57 studied the reliability of predicting the fertile days by salivary ferning in 30 women with regular menstrual cycles. The day of ovulation was confirmed with ultrasound or BBT. The first group of women (n = 17) used the mini-microscope, which showed a sensitivity of 53%. The second group of women (n = 13) used a normal light microscope, which had a sensitivity of 86%. The researchers repeated the same test for 10 postmenopausal women and 10 men. Eight out of 10 postmenopausal women tested positive and all of the men tested positive for signs of ovulation. The researchers concluded that the saliva ferning test is unreliable for predicting the fertile time and its use should be discouraged.
Fertility monitoring devices differ enormously in price and in effectiveness. Freundl and associates58 have developed a quality index score to be used to evaluate fertility monitors prior to full prospective clinical trials. The days predicted as fertile by the monitors were compared with the fertile time by ultrasound and urinary LH. The researchers concluded that a quality index score of less than 0.5 identifies a monitor whose accuracy in identifying the fertile time is sufficient to warrant prospective clinical trials (this includes Persona and computerized thermometers). Devices with a quality index score of more than 0.5 identifies a monitor whose accuracy in identifying the fertile time is not sufficient to warrant prospective clinical trials (this includes all saliva testing devices). Their findings confirm previous recommendations that saliva testing devices should not be offered to women.
COMBINING THE INDICATORS OF FERTILITY
Many women decide to combine two or more indicators of fertility. The most common combination women use is monitoring the cervical secretions and temperature indicators. This is sometimes called the sympto-thermal method. Cross-checking the indicators, with a calculation based on the shortest length of a woman's previous six cycles, increases the effectiveness of accurately identifying the start of the fertile time. If combining the indicators of fertility, the fertile time starts at the first sign of cervical secretions, the first change from a low firm closed (and tilted) cervix or the first fertile day by shortest cycle calculation, whichever comes earlier. The fertile time ends after the third high temperature past peak day.
Fig. 14 illustrates a completed chart from a woman combining the observed fertility indicators with Persona. Her shortest cycle in the previous year was 28 days. In any given cycle, different indicators may identify the start of the fertile time. To identify the end of the fertile time, at least two indicators must correlate. In this example, day 8 is the start of the fertile time (the calculation is the earliest indicator). Day 19 is the end of the fertile time (third high temperature after peak day). There is no need to wait for the cervix to remain closed for 3 days or to perform a longest cycle calculation provided temperature and secretions are correlated. In addition, this chart shows close correlation between observed indicators and Persona.
|
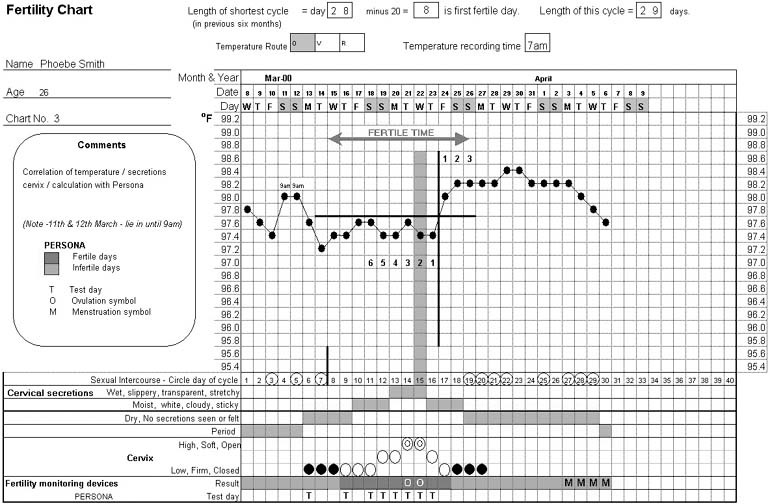
Women are encouraged to record factors or events that may disturb the menstrual cycle or the fertility indicators. These may include alcohol, disturbed nights, holidays, time zone changes, shift work, stress, illness, or medication.59
Effectiveness of Fertility Awareness Methods Using a Combination of Indicators
Table 2 shows six separate studies using a combination of indicators.60, 61, 62, 63, 64 65 The failure rate when combining indicators is less than most of the studies that use a single indicator. If couples are to use FAMs successfully, they require a high degree of motivation. The most recent prospective study using a combination of indicators reported an overall failure of 2.6.
Table 2. Comparison of effectiveness studies using combination of indicators
The study | Description | Participants (n) | Method failure | Overall failure |
| Rice et al. 1981 Multicenter60 | New users | 1022 | 0.9 | 7.5 |
| Canadian Center n=168 | Spacers | 67 | 14.9 | |
| Limiters | 101 | 1.1 | ||
| Marshall UK, 198561 | Experienced users | 118 | 0.3 | 3.9 |
| Barbato, Italy 198862 | New users | 460 | 0.4 | 3.6 |
| Clubb et al. UK 198863 | New users | 72 | 1.3 | 2.7 |
| Freundl, European Multicentre 199964 | New users | 1328 | 0.5 | 2.6 |
| Frank-Herrmann P et al. 2007 65 | New users | 900 | 0.4 | 1.8 |
In the Rice multicenter study, the Canadian Center involving 168 participants clearly demonstrated how family spacers, those who plan more children at a later date (n = 67), are less effective in preventing pregnancy (overall failure of 14.9). They are prepared to take risks whereas family limiters, those who have completed their family (n = 101), are more conscientious users (overall failure of 1.1).
Effectiveness studies and probability of conception studies have confirmed that once correctly identified, the late infertile time is the safest time to have unprotected intercourse and avoid a pregnancy. The most recent effectiveness study shows the methodology is very effective when used correctly. There were 0.4 unintended pregnancies per 100 women years, if there was abstinence during the fertile time. The use-effectiveness of the method, i.e. the overall pregnancy rate was 1.8% after 13 cycles of use and the discontinuation rate due to dissatisfaction with combined indicator use was only 9.2 per 100 women after 13 cycles.65
Advances in teaching techniques and use of combined indicator methods have considerably reduced the unintended pregnancy rate among FAM users. Lamprecht and Trussell performed an evaluation of well-designed effectiveness studies.66 They discuss the many factors influencing the effectiveness of FAMs, propose a framework for evaluating published reports on effectiveness, and provide guidance for the design of future studies.
Table 3. Advantages and disadvantages of fertility awareness methods
| Advantages | Disadvantages |
| No chemical agents or physical devices | Takes time to learn: 3–6 cycles |
| No side effects | Some women find charting difficult |
| Efficient—when well-taught and motivated | Some couples find abstinence difficult |
| Low cost for methods based on observation | Requires commitment of both partners |
| Not dependent on medical personnel after initial instruction | More difficult at times of stress or hormonal change |
| Promotes education/fertility awareness | No protection against STIs |
| Encourages shared responsibility/increased communication | Cannot be used without co-operation of partner |
| Ethically acceptable | Fertility monitoring devices are expensive |
| Can be used to plan or avoid pregnancy |
Comparing the Effectiveness of Different Fertility Awareness Methods
It can be difficult to compare the effectiveness of different FAMs. Some of the variable factors include the indicators of fertility used, the teaching methodology, the characteristics of the study population, new or experienced users, new or experienced teachers, the methods used to calculate the pregnancy rates, methods used to confirm pregnancies, intention to conceive, or avoid indicated at the beginning of the cycle. For example, some efficacy studies have allowed women a three-cycle learning phase before recruitment to the study, whereas other studies, including the more recent Standard Days Method and TwoDay Method, women entered the study as soon as they started using the method. These factors are likely to impact on the effectiveness, because generally more experienced users of a method will use the method more effectively. Lamprecht and Trussel66 suggest that many FAM studies were flawed in design and did not calculate pregnancy rates correctly. They report on the few well-designed studies and provide guidance for the design of future studies. A review of FAM effectiveness studies was performed by Kambic,67 who highlighted that well-designed trials demonstrate the increased efficacy of using two or more indicators compared with a single indicator method.
Cost-Effectiveness of Fertility Awareness Methods
An Oxford study evaluated the cost-effectiveness of teaching FAMs in primary care in the United Kingdom.63 The study confirmed that audio-visual materials reduce teaching time and that group-teaching is feasible for some couples. The time/cost compared favorably with other methods. Although the cost in the first few months was higher (nurses' time), once a couple understood the method they no longer needed to attend the clinic on a regular basis, and the ongoing cost of charts and thermometers was minimal. With increasing numbers of United Kingdom households having access to the Internet, the comprehensive teaching site www.fertilityuk.org can be used as a distance learning resource for clients.
Contraindications to Fertility Awareness Methods
For some couples, a FAM is inappropriate or contraindicated; for example, when the woman is not in a stable relationship or is at risk for sexually transmitted infections, or in situations when the woman has a health condition in which pregnancy is absolutely contraindicated. In other consultations, health professionals may be alerted to the fact that the woman seems excessively anxious or disinterested. In these circumstances, a more in-depth history may elicit other concerns or aspects about the personal or social history that suggest a FAM is inappropriate; for example, in situations in which there is coercion for religious or cultural reasons, the partner does not want to use the method, the woman or her partner has an alcohol or drug-related problem, or there is risk of domestic violence.
Barriers Combined With Fertility Awareness
Many couples choose to combine fertility awareness knowledge with barrier methods during the fertile time. It is important that couples understand the correct use of their chosen barrier method. In practice, the use of barrier methods (particularly if used with additional spermicide) can make the recognition of cervical secretions difficult. Combining the temperature and changes in the cervix can help to avoid this problem.
In a large prospective study68 of 758 new users that analyzed the relation between unintended pregnancy rates and sexual behavior, with special reference to barrier method use during the fertile time; 54% of the participants used NFP only (or predominantly) and 46% combined fertility awareness with barriers (perfect use pregnancy rate: 0.63%; overall pregnancy rate: 2.2%). The study shows that couples who use barrier methods during the fertile time still take risks and have unprotected intercourse during the fertile time. The researchers conclude that FAMs are most unforgiving of imperfect use, but are extremely effective when either abstinence or protected intercourse is used during the fertile time. The most recent effectiveness study showed that when barrier methods were used during the fertile time the rate of unintended pregnancies was not significantly different.65
Withdrawal Combined With Fertility Awareness
Withdrawal method allows vaginal intercourse until ejaculation is impending, at which time the man withdraws his penis from the vagina and away from the woman's genitals. The man relies on his own sensations to determine when he is about to ejaculate.
There has been some concern that the pre-ejaculatory fluid may contain sperm, but this has not been confirmed in research.69, 70 However, if a man has intercourse again within a few hours, there may be some sperm left in the urethra from the earlier ejaculation. It is therefore recommended that a man be advised to pass urine between each ejaculation to flush out any remaining sperm. Couples need to be counseled that they are at risk for sexually transmitted diseases and that although the lubricating fluids that escape from the penis long before ejaculation do not contain sperm, they can transmit infections such as the HIV virus. Withdrawal has no known side effects, although interruption of the sexual response can diminish a couple's sexual pleasure.
The Effectiveness of Withdrawal Method
There has been no effectiveness studies conducted on the withdrawal method. The effectiveness of withdrawal method is estimated to be 96% effective with perfect use and 81% effective with typical use. This means that between four and 19 women out of 100 would conceive in 1 year using withdrawal method.71 This is estimated for couples using withdrawal method alone. There are no effectiveness figures available for couples who combine fertility awareness knowledge with withdrawal method; however, it is likely that couples who only use withdrawal during the fertile time could have an increased failure rate.
ABSTINENCE AND BEHAVIOR MODIFICATION
Exploring the client's views on coping with the relationship during the fertile time is a difficult area to address both for the woman/couple and for the health professional and is easily avoided or addressed very superficially. Effective consultations skills are essential for working with clients requesting any user-dependent method. Ideally, the couple is counseled together. If the woman is seen alone, every effort should be made to discuss the impact of abstinence on the relationship.
FAMs alongside contraceptive pills and barrier methods are user-dependent methods. They all rely on the day-to-day vigilance and motivation of individuals to avoid pregnancy. For individuals who are ambivalent or forgetful, the potential exists to use the method incorrectly or stop using it altogether. Most individuals will get away with the odd forgotten pill or even burst condom over the duration of a cycle; however, FAMs are extremely unforgiving to those who are less-than-perfect users or who are calculated risk takers, because unprotected intercourse occurs at exactly the time when a woman is most likely to be fertile.
Many health professionals believe fertility awareness methods are inappropriate because a woman's libido is highest around ovulation. This belief is not borne out by all research. When exploring ‘mood and well-being’ during the menstrual cycle, Anne Walker72 discusses a review of 32 studies where 17 reported increased sexual activity premenstrually, 18 post-menstrually, 4 during menstruation, and 8 around ovulation. (Thirteen of these studies reported peaks pre and post-menstrually).
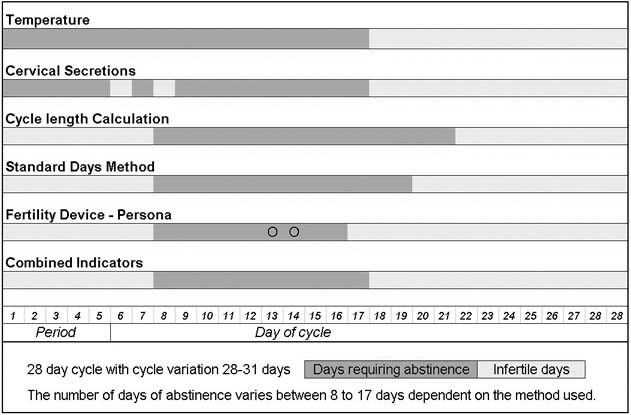
The length of abstinence is a key factor when considering the acceptability and effectiveness of FAMs. Fig. 15 shows the length of abstinence required by the use of different fertility indicators. Although the fertile time is only approximately 8–9 days, the number of days of abstinence required varies from 8 to 17 days, depending on the method used. Difficulties related to the length of abstinence may be directly related to the indicator used. Single-indicator methods generally involve the longest time of abstinence, typically around 16 days. Combined-indicator methods aim to accurately identify the fertile time and reduce the time of abstinence to an average of 10 days. Personal hormone monitoring has the potential for reducing the required time of abstinence still further.
|
“Abstinence from intercourse is the key to success. Yet those who promote NFP are strangely silent about the effect of abstinence on the couple (John Marshall 1996).”73
Marshall and Rowe74 analyzed detailed psychological questionnaires to ascertain the impact on the relationship of 410 couples who used the temperature method as a single indicator. This required an average of 17 days of abstinence each month. The study showed that 41% of the couples were worried about an unplanned pregnancy; this affected their attitude to intercourse in 28% of the men and 38% of the women. The majority of couples both men and women found abstinence difficult.
Couples who choose to abstain from vaginal intercourse during the fertile time have different ways of coping with abstinence. For some couples this involves being physically apart; for others, it involves being more imaginative with their lovemaking. It is important to offer an opportunity to talk openly and discuss strategies to adopt during this time as well as offering additional support/counseling at follow-up visits. Bonnar and Lamprecht75 collected data on alternatives to vaginal intercourse during the fertile time as part of a pilot effectiveness study of Irish women who used a calculation based on the previous six cycles. The required length of abstinence averaged 16 days. The researchers found that approximately one third of couples avoided genital contact, whereas approximately half of the couples reported using various forms of noncoital sexual activity or outercourse: oral sex, frottage (body rubbing), and mutual masturbation.
Although many couples state that they wish only to use abstinence during the fertile time, studies have shown that occasional barrier use is common.68 It is essential that couples who wish to use fertility knowledge with barrier methods are counseled about the fact that if the barrier method fails during this time, then they are at a greatly increased risk of pregnancy. In addition, most women who choose to use FAMs for moral or ethical reasons have concerns related to the use of emergency contraception. Although emergency contraception usually works by preventing fertilization, it is undeniable that the mechanism may prevent implantation.76
CONCERNS ABOUT BIRTH DEFECTS
Concerns have been raised about the risk of birth defects or poor pregnancy outcomes caused by aged ovum or sperm at the time of conception. Unintended pregnancies among couples who use natural methods usually result from having intercourse at the beginning or end of the fertile time. A prospective study showed no significant differences in rates of spontaneous abortion, low birth weight, or preterm birth among women using FAMs who had unintended pregnancies compared with women who had intended pregnancies.77,78,79
The timing of implantation could be related to early pregnancy loss. In a small study, women had a greater chance of having a miscarriage when conception occurred very late in the fertile time.80 It was suggested that pregnancies with late-implanting conceptuses might fail for several reasons. The receptivity of the endometrium decreases during the late luteal phase, and the corpus luteum is less responsive to HCG by 11 or 12 days after ovulation. Factors intrinsic to the zygote could also be at work. Unhealthy zygotes may develop more slowly or implantation may be abnormal, resulting in later and weaker production of chorionic gonadotrophin. To the degree that imperfect embryos develop and are implanted more slowly, a limited window of receptivity may provide a gating mechanism to screen out impaired embryos. Larger studies are required to clarify these findings.
SEX SELECTION
There has long been an interest in predetermining the sex of the child at the time of conception. The ancient Greeks believed that male sperm were produced in the right testicle and boys were formed on the right or warmer side of the uterus and girls on the left. French noblemen were reported to have tied up or even cut off their left testicle in the quest for an heir. Over more recent years, endless theories have been expounded related to diet, intercourse position, and timing of intercourse in relation to ovulation. Despite the passion that this subject can generate, scientifically it seems "to date there is no reliable scientific evidence to support claims made for choosing the sex of the baby, such as timing of intercourse, intercourse positions or diet."81
A WHO study of approximately 1000 births showed no association between timing of conception and the sex ratio at birth.82 Gray and associates commented that reliable sex selection is currently only possible by preimplantation diagnosis and transfer of embryos of a given sex, by prenatal diagnosis, and abortion of undesired sex or perhaps by sperm separation using flow cytometry combined with in vitro fertilization (IVF). In view of the clinical nature and limiting factors of these treatments, many couples still maintain an active interest in any possible way to predetermine the sex of their offspring. Although some studies have shown an excess of male births closer to ovulation, others have shown an excess of female births. One study found a link between a short follicular phase and an excess of male births. However, the current evidence clearly demonstrates that the manipulation of the timing of conception or characteristics of the menstrual cycle cannot be used to preselect the sex of the child.83
USING FERTILITY AWARENESS METHODS
Using Fertility Awareness Methods After Stopping Hormonal Methods of Contraception
Women who are discontinuing hormonal methods of contraception before starting a FAM to achieve or avoid pregnancy require careful management and counseling. Many family planning providers are not as confident to manage women at this time because the return of fertility is unpredictable. For some women discontinuing the combined pill, the return of fertility is immediate; for others, the resumption of fertility may take more than 6 months.
Temporary delays in conception are not unusual after stopping oral contraception particularly for nulliparous women older than 30 years.84 The current use of low-estrogen-containing pills cause less concern related to delayed fertility return than the older high-estrogen pills (Bracken 1990 in Farrow).85
A German prospective study86 compared the cycle characteristics of 175 women (3048 cycles) with a control group of 284 women (6251 cycles) who had never used oral contraception. The mean duration of pill use was 3.5 years (ranging from a few months to 13 years). For most women (nearly 60%), the first postpill cycle was a fertile cycle. This is important information for women who wish to avoid pregnancy after stopping pills, because there is a common myth that fertility is suppressed for a while after stopping pills. There were more frequent cycle disturbances in postpill cycles for up to seven cycles after discontinuing the pill. The cycle disturbances included longer cycles more than 35 days, cycles with shortened luteal phases, and cycles that showed no temperature increase indicating absence of ovulation. Cycles that showed no temperature increase occurred in 10% of first cycles after the pill and nearly 2% women had cycle lengths more than 90 days.
Using Fertility Awareness Methods When Breastfeeding
It has long been known that breastfeeding reduces female fertility and overall it is a major factor in reducing population growth. Breastfeeding suppresses ovulation87 because prolactin levels are raised when breastfeeding. During pregnancy, the levels of prolactin rise but the high levels of estrogen and progesterone prevent the prolactin from stimulating milk production in the breasts. Immediately after delivery the prolactin level peaks, estrogen and progesterone levels fall, and the prolactin stimulates the breasts to produce milk. Prolactin acts on the pituitary gland, interfering with the action of FSH and LH, reducing the production of estrogen and suppressing follicular growth, hence suppressing ovulation. Each act of suckling stimulates the production of prolactin, but the level falls again after 3–4 hours. Provided the baby suckles frequently, the level of prolactin remains high and ovulation is suppressed. The natural contraceptive effect of breast-feeding has been recognized throughout history. In 350 BC, Aristotle observed that while women are suckling children, menstruation does not occur according to nature, nor do they conceive.88 Traditionally,89 babies were breastfed from birth and supplements were not introduced until after the milk teeth had erupted at approximately 6–8 months. This temporary reduction in fertility caused by breastfeeding, also known as lactational amenorrhoea, is widely recognized to lengthen intervals between pregnancies in some parts of the world where women often breastfeed for 2 years or longer.
Lactational Amenorrhea Method
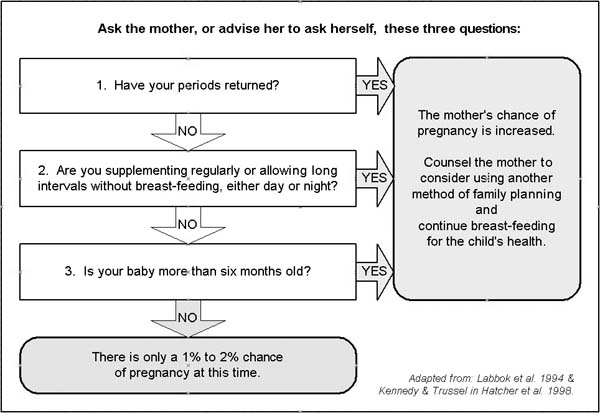
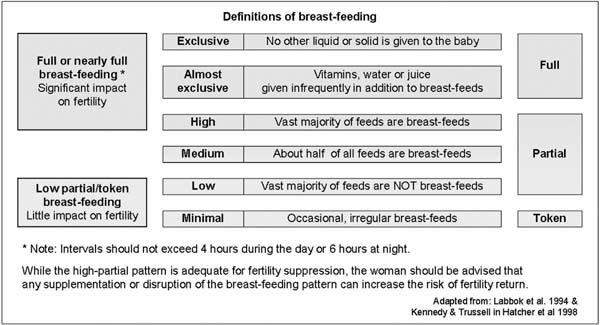
After an international meeting in Italy in 1988, it was formally recognized that breastfeeding was effective to use as a family planning method when certain conditions were met. This method of family planning was called the Lactational Amenorrhea Method (LAM)90 (Fig. 16). It stated that in the first six months following the birth, a woman is 98% protected against pregnancy provided that she is amenorrhoeic and fully breast-feeding her baby. This means she must breastfeed at regular intervals day and night, give no other liquids or solids as a substitute for breastfeeding, and have no periods (no bleeding after the first 8 weeks postpartum). Once any of these conditions is not being met, the chances of pregnancy increase, even if a woman continues to fully breastfeed and remains amenorrheic after 6 months91, 92 (Fig. 17).
|
|
|
A recent WHO multicenter study reported that in the first 6 months after childbirth, the cumulative pregnancy rate ranged from 0.9% to 1.2% during full breastfeeding,93 providing further evidence that fully breastfeeding a baby gives 98% protection against pregnancy. Yet practitioners still lack confidence in reassuring women that breastfeeding can act as an effective contraceptive.94
Breastfeeding has many health benefits for mother and baby. It provides the baby with complete nutrition, a safe food source, and immunological defense against infectious diseases. It also reduces the mother's risk of ovarian and breast cancer. WHO commissioned a systematic review of the published scientific literature on the optimal duration of exclusive breastfeeding, evaluating more than 3000 references. It now recommends exclusive breastfeeding for 6 months, with the introduction of complementary foods and continued breastfeeding thereafter.95 In May 2003, the United Kingdom government publicly endorsed the WHO policy. “Breastfeeding for the first 6 months provides the best start for babies. It establishes a foundation for improving short and long-term health and in so doing can help to reduce health inequalities. We want to support women in their decision to breastfeed and help them continue to do so.” In the United Kingdom in 2000, 69% of women started breastfeeding their babies from birth, but by 1 month, only 44% were continuing. Only 23% of women were breastfeeding their babies by 6 months (compare this with Norway's 97% breastfeeding rate at 1 month decreasing to 80% at 6 months).96
Recommendations for best breastfeeding practice can be found at UNICEF United Kingdom's baby-friendly initiative,97 which promotes strategies for breastfeeding and providing accurate information for parents. The infant feeding survey 200098 confirmed that the most likely groups to breastfeed are older women having received full time education over 18 years and women from higher socio-economic groups. Therefore, the opportunity for using breastfeeding as a fertility suppressant currently tends to be restricted to a select group.
The return of fertility has been compared between breast and bottle feeders.99 In the breastfeeding group, ovulation was delayed for up to 15 months compared with bottle-feeding mothers, who had all resumed ovulation and menstruation by 15 weeks, averaging a return of fertility between 9 and 13 weeks postpartum. Menstruation can return as early as 5 weeks after the birth in bottle feeders. In approximately 50% of women, ovulation occurs before the first menstrual period; therefore, a woman who is bottle-feeding could conceive again within 1 month postnatally. Women who are not protected by LAM will therefore need to have access to another appropriate and effective method of contraception.
THE POSTNATAL FAMILY PLANNING CONSULTATION
Changes in lifestyle and the need to study or work outside the home often interfere with women's breastfeeding patterns.100 Effective communication skills are especially important for the postnatal family planning consultation. Active listening and allowing sufficient time for open-ended questions can provide the necessary space to help women or couples to explore issues related to the recent birth, breastfeeding, the resumption of sexual activity, plans for future children, and counseling about the choice of method suited to the needs of the woman, the couple, and her young family.101 Optimizing the effective use of nature's contraceptive with current breastfeeding practices is a challenge.
The choice of method after childbirth needs to take into account the woman's plans, if any, to have further children. Guillebaud splits the postnatal ages into during breastfeeding; family spacing after breastfeeding, and after the (probable) last child.102 The postnatal contraceptive consultation needs to distinguish carefully between short-term, longer-term, or permanent methods. Women who have experienced a delay in conceiving in the past need particularly careful counseling. Some women who have breastfed for long periods, especially if they are in their late 30s, may experience difficulty in conceiving if they are still breastfeeding even infrequently and despite the resumption of menstruation.
The general advice for resuming sexual activity postnatally is as soon as the woman and her partner feel ready, although almost 50% of women have reduced levels of sexual interest for at least 3 months postnatally.103 Many women will report reduced vaginal lubrication, which is generally more marked for breastfeeding women because of low estrogens.
In the first 6 months postpartum, the majority of women who are fully breastfeeding will be able to rely on LAM (see Figs. 16 and 17). An additional family planning method should be started at a time when the LAM guidelines no longer apply.
Women wishing to delay their next conception may be well-suited to a FAM104 by observing signs of returning fertility such as cervical secretions, temperature, and changes in the cervix (optional). A woman should start observing her fertility signs approximately 2 weeks before it is expected that the LAM criteria will no longer apply.
Barrier methods, condoms or diaphragms, may be appropriate for breastfeeding women who are spacing their births. The diaphragm size should be checked postnatally. Women who experience dyspareunia (pain during intercourse) may find that barrier methods are not comfortable. Any additional lubricants required for vaginal dryness must be water-based if rubber barriers are used. Any progestin-only method is suitable during breastfeeding. Progestin-only pills (POPs), the IUS or an implant, may be suitable for family spacers, but the injection Depo-Provera is appropriate only if a long gap is expected between pregnancies, because of the possible delay in returning fertility. For breastfeeding mothers, the dose of progestin to the baby is believed to be harmless,105 with the quantity being equivalent to one progestin pill in 2 years and considerably less than the progesterone level in dried cows milk. An IUD is generally suited to family spacers and can be used during breastfeeding.
The Personal hormone monitoring system (Persona; Unipath) is not recommended for use while breastfeeding. A woman should wait until she has had at least two normal menstruations with cycle length 23–35 days before using the monitor with the beginning of the third period. Combined oral contraception has long been considered unsuitable for breast-feeding women as the estrogen may affect the quantity and constituents of breast milk. However a recent Cochrane Review106 found no significant differences in infant growth or weight and found the evidence from existing RCTs to be insufficient to establish an effect. They recommended that at least one properly conducted RCT of adequate size is urgently needed to address this question.
Family Spacing or Limiting While Breastfeeding
Women spacing their next pregnancy are ideally suited to using a FAM or barrier method after breastfeeding, provided they have adequate instruction. Estrogen-containing methods (COCs) can be used after breastfeeding when increased effectiveness is required. The IUD, IUS, or implant combines the least long-term health hazards, efficacy, and reversibility. Careful consideration of sexual history is always required for women considering an IUD, particularly in a new relationship or when there may be issues related to exposure to sexually transmitted infections. Injectable hormonal contraceptives may be appropriate if a longer gap is required between pregnancies.
Breastfeeding women who decide that they have completed their family may want more protection than lactational amenorrhea can offer. They may prefer not to rely on highly user-dependent methods such as a FAM or barrier methods. After the (probable) last child, there is less concern about protecting fertility or planning the next child, so a longer-term method (IUD, IUS, COC, implant, or injectable) may be more appropriate. Sterilization of either partner should not be considered immediately postnatally because decisions are more likely to be regretted at this time. Requests for sterilization at a young age or at the time of birth require particularly effective counseling.
Fertility Awareness Methods During the Perimenopausal Years
Women who have previously used FAMs value being given information about how the cycle length is likely to vary and their likelihood of getting pregnant at this time. Some women value charting their symptoms, and special charts have been designed that allow for longer cycles. Women who have never used FAMs before find it more difficult to learn to observe the indicators of fertility. Many women experience unusual bleeding patterns during this time. It is very import to advise women that any change from their normal menstrual pattern should be reported and not to assume that unusual bleeding patterns are physiological when they may be pathological. Women should also be aware that they cannot use FAMs if they are using hormone replacement therapy.
Flynn and associates107 prospectively observed 107 cycles in 36 women aged 45–53 years. All the women were experienced FAM users. They measured urinary E3G and pregnanediol glucuronide; 33% had regular cycles consistent with potential fertility, 19% had cycles consistent with infertility, and 47% had a mixture of both types of cycle.
CONCLUSION
If couples are satisfied with their method of family planning, then they are more likely to use it consistently. It is well-recognized that there is no ideal method of family planning. Increasing the range of choice will help to meet the needs of more couples. The most effective FAMs combine two or more indicators to identify the fertile time, but the contraceptive effectiveness of the method relies on the couple's ability either to abstain or to use a barrier method consistently during the fertile time. Research clearly demonstrates that motivated couples can use FAMs successfully, provided they are taught by individuals who have been trained to teach FAMs. Many primary health care or family planning clinics in the United Kingdom now integrate fertility awareness knowledge into comprehensive family planning services. A fertility awareness consultation sheet produced in collaboration with the Family Planning Association UK can help to improve consultations and support health professionals discussing fertility awareness and family planning choice.108
Provided they have been appropriately informed about their full range of choices and the relative effectiveness, advantages, and disadvantages of methods, many couples irrespective of educational level can learn to use FAMs effectively. Some couples choosing FAMs have frequently already exhausted the contraceptive menu and feel dissatisfied with other methods offered. Health professionals need to be alert to the emotional needs of their clients and feel comfortable to address how the client will cope during the fertile time. Couples who find this method suits them report enhanced communication within their sexual relationship. Research clearly demonstrates that motivated couples can use FAMs effectively.
TRAINING AND RESOURCES
Successful use of FAMs depends on adequate teaching and support from a trained practitioner. Many national centers run accredited multidisciplinary courses for health professionals in addition to offering information and referral services.
Useful contact details and web sites are available at:
Fertility UK www.fertilityUK.org
Dr Cecilia Pyper & Jane Knight
Public Health Action Support Team (PHAST)
Department of Primary Care and Social Medicine
Faculty of Medicine
Imperial College London
St Dunstan’s Road
London W6 8RP
c@pyper.net
jknight@fertilityuk.org
The Institute for Reproductive Health
Georgetown University School of Medicine
4301 Connecticut Avenue NW, Suite 310
Washington, DC 20008, USA
www.irh.org
International NFP Directory
3211 4th Street, NE
Washington DC. 20017-1194, USA
http://www.usccb.org/prolife/issues/nfp/international.htm
European Directory of FAM teachers
European Institute for Family Life Education
http://www.eifle.org/index.shtml
Australian Council of NFP
(PO Box 307), 22 Theodore Street
CURTIN ACT 2605
E-mail: nfpp@ozemail.com.au
www.nfpprog.com
Natural Fertility NZ Inc.
PO Box 10-512
Wellington, New Zealand
http://www.naturalfertility.co.nz/
Serena Canada
National Secretariat
151 Holland Avenue, Ottawa, ON K1Y 0Y2
www.serena.ca
ACKNOWLEDGMENTS
The authors thank Dr. Elizabeth Clubb and Dr. Victoria Jennings for their kindness and support in developing this article. Supported by Dr C Pyper's NHS Primary Care Career Scientist Award.
REFERENCES
Pyper CMM: Fertility Awareness & Natural Family Planning. Eur J Contracept Reprod Health Care 2:131-146, 1997 |
|
Pyper CMM, Knight J: Fertility awareness methods: Update Postgraduate Centre Series: Contraception. Excerpta Medica 27-34, 2001 |
|
Pyper C: Reproductive health awareness, an important dimension to be integrated into existing programmes. Adv Contracept 13:331-338, 1997 |
|
World Health Organization: Fertility Awareness Methods–Health for all 2000. Report on a WHO Workshop. Poland, WHO 1986 |
|
Pyper CMM, Knight J: Fertility awareness methods of family planning: The physiological background, methodology and effectiveness of fertility awareness methods, FACT review paper. The Journal of Family Planning & Reproductive Health Care 27(2):103-110, 2001 |
|
Murphy J, Laux J: The Rhythm Way to Family Happiness. London, Staple Press, 1959 |
|
Billings J: The Ovulation Method. Melbourne, The Advocate Press, 1964 |
|
Marshall: The Infertile Period–Principles and Practice. London, Darton, Longman and Todd, 1963 |
|
Keefe E: Cephalad shift of the cervix uteri: Sign of the fertile time in women. Int Rev Nat Fam Plan 1:55-60, 1977 |
|
Clubb E, Knight J: Fertility–Fertility Awareness and Natural Family Planning. 3rd ed. David & Charles, 1996 |
|
Marshall J: Planning for a Family: An Atlas of Mucothermic Charts. London, Boston, Faber and Faber, 1979 |
|
Thyma Paul: The Double Check Method of Family Planning. Marriage Life Information. Sayre, USA, 1977 |
|
World Health Organisation. Temporal relationships between indices of the fertile period. Fertility Sterility; 39(5):647–654 1983 |
|
Bonnar J, Flynn A, Freundl G et al: Personal hormone monitoring for contraception. Br J Fam Plan 24, 128-134, 1999 |
|
Arevalo M, Sinai I, Jennings V: A fixed formula to define the fertile window of the menstrual cycle as the basis of a simple method of NFP. Contraception 60:357-360, 1999 |
|
Sinai I, Jennings V, Arevalo M: The TwoDay Algorithm: A New Algorithm to Identify the Fertile Time of the Menstrual Cycle. Contraception 60:65-70, 1999 |
|
Baerwald AR, Adams GP, Pierson RA: A new model for ovarian follicular development during the human menstrual cycle. Fertil Steril 80:116-122, 2003 |
|
Odeblad E: Cervical mucus and their functions. J Irish Coll Phys Surg 26:(1):1997 |
|
Fordney-Settlage D: A review of cervical mucus and sperm interactions in humans. Int J Fertil 26:161-169, 1981 |
|
Ferreira-Poblete A: The probability of conception on different days of the cycle with respect to ovulation: An overview. Adv Contracep 13:83-95, 1997 |
|
Royston P: Basal body temperature, ovulation and the risk of conception on different days of the menstrual cycle with special reference to the lifetimes of the sperm and egg. Biometrics 38:397-406, 1982 |
|
Flynn A, Docker M, Morris R et al: The reliability of women's subjective assessment of the fertile period, relative to urinary gonadotrophins and follicular ultrasonic measurements during the menstrual cycle. In: Bonnar J, Thompson W, Harrison RF, eds (eds): Research in Family Planning. pp 3-11, Lancaster, England, 1983 |
|
Collins WP: The evolution of reference methods to monitor ovulation prediction. Am J Obstet Gynaecol 165:1994-1996, 1991 |
|
Wilcox A, Weinberg M, Baird D: Timing of Sexual Intercourse in Relation to Ovulation. Effects on the Probability of Conception, Survival of the Pregnancy, and Sex of the Baby N Engl J Med 333:1517-1521, 1995 |
|
Dunson DB, Baird DD, Wilcox AJ et al: Day specific probabilities of clinical pregnancy based on two studies with imperfect measures of ovulation. Hum Reprod 14:1835-1839, 1999 |
|
Barrett JC, Marshall J: The risk of conception on different days of the menstrual cycle. Population Studies 23:455-461, 1969 |
|
Dunson DB, Colombo B, Baird D: Changes with age in the level and duration of fertility in the menstrual cycle. Hum Reprod 17:1399-1403, 2002 |
|
Rees M: The abnormal menstrual cycle. In: McPherson A, Waller D (eds): Women's Health. p 308, 4th ed. OUP. 1997 |
|
Vollman RF: The menstrual cycle. Philadelphia, WB Saunders 1977 |
|
Munster K, Schmidt L, Helm P: Length and variation in menstrual cycle. Br J.Obstet Gynaecol 99:422-429, 1992 |
|
Marshall J: A field trial of the basal body temperature method of regulating births. Lancet ii:8-10, 1968 |
|
Chretien FC, Cohen J: Human cervical mucus during the menstrual cycle and pregnancy in normal and pathological conditions. J Reprod Med 14:193-196, 1975 |
|
Odeblad E: Cervical mucus and their functions. J Irish Coll Phys Surg 26:27-32, 1997 |
|
Chretien FC: Involvement of the glycoprotein meshwork of cervical mucus in the mechanism of sperm orientation. Acta Obstet Gynecol Scand 449-461, 2003 |
|
Depares J, Ryder R, Walker S et al: Ovarian ultrasonography highlights precision of symptoms of ovulation as markers of ovulation. Br Med J 292:1562, 1986 |
|
World Health Organization: A Prospective Multicentre trial of the ovulation method of natural family planning: I The teaching phase. Fertil Steril 36:152-158, 1981 |
|
Billings JJ: Cervical mucus: The biological marker of fertility and infertility. International J Fertil 26:181, 1987 |
|
Hilgers TW, Stanford JB: Creighton Model NaProEducation Technology for Avoiding Pregnancy: Use effectiveness. J Reprod Med 43:495-502, 1998 |
|
Fehring RJ: Accuracy of the peak day of cervical mucus as a biological marker of fertility. Contraception 66:231-235, 2002 |
|
World Health Organization: A Prospective Multi-centre Trial of the Ovulation Method of Natural Family Planning: II The Effectiveness phase. Fertil Steril 36:591-594, 1981 |
|
Trussell J, Gummer-Strawn L: Contraceptive failure of the ovulation method of periodic abstinence. Fam Plan Perspect 22:65-75, 1990 |
|
Dunson DB, Sinai I, Colombo B: The relationship between cervical secretions and the daily probability of pregnancy: Effectiveness of the Two-Day algorithm. Hum Reprod 16:2278-2282, 2001 |
|
Arévalo, M. Jennings, V. Nikula, M. Sinai, I. Efficacy of the new TwoDay Method of family planning, Fertility and Sterility, 2004: Volume 82, Issue 4, 885-892 |
|
Parenteau-Carreau S, Infante-Revard C: Self-palpation to assess cervical changes in relation to mucus and temperature. Int J Fertil 33:(Suppl) 10-16, 1988 |
|
Kambic RT, Lamprecht V: Calendar rhythm efficacy: a review. Adv Contracep 12:123-128, 1996. |
|
Lamprecht V, Grummer-Strawn J: Development of new formulas to identify the fertile time of the menstrual cycle. Contraception 54:339-343, 1996 |
|
Faundes A, Lamprecht V, Osis M et al: Simplifying NFP: preliminary report of a pilot study of the collar method in Brazil. Adv Contracept 13:(2/3):167-171, 1997 |
|
Wilcox AJ, Dunson D, Baird DD: The timing of the "fertile window" in the menstrual cycle: day specific estimates from a prospective study. Br Med J 321:1259-1262, 2000 |
|
Arevalo M, Jennings V, Sinai I: Efficacy of a New Method of Family Planning: The Standard Days Method. Contraception 65:333-338, 2002 |
|
Guillebaud J: Contraception Today. p 6, Dunitz, 1995 |
|
Behre HM et al: Prediction of ovulation by urinary hormone measurements with the home use ClearPlan Fertility Monitor: comparison with transvaginal ultrasound scans and serum hormone measurements. Hum Reprod 15:2478-2482, 2000 |
|
Pyper C, Bromhall L, Altman D, Brownbill P, Murphy M, The Oxford Conception Study design and recruitment experience. Paediatric and Perinatal Epidemiology 2006-1.51–59 |
|
Flynn A, Pulcrano J, Royston P et al: An evaluation of the Bioself 110 electronic fertility indicator as a contraceptive aid. Contraception 44:125-140, 1991 |
|
Freundl G, Frank-Hermann P, Godehardt E et al: Retrospective clinical trial of contraceptive effectiveness of the electronic fertility indicator Ladycomp/Babycomp. Adv Contracept 14:97-108, 1998 |
|
Bremme M, Freundl G, Frank-Hermann P: Analysis of the computer-thermometer cyclotest D to be used for natural family planning. Adv Contracept 8:221, 1992 |
|
Roland M: The Fern Test–A critical analysis. Obstet Gynecol 11:30-34, 1958 |
|
Braat DD: Saliva test as ovulation predictor. The Lancet. Vol. 352. October 17 1998; 1283–4. |
|
Freundl G et al: Estimated maximum failure rates of cycle monitors using daily conception probabilities in the menstrual cycle. Human Reproduction Vol. 18, No. 12:2628-2633, 2003 |
|
Clubb E, Knight J: Fertility. Factors Affecting the Menstrual Cycle. p 52-57, David and Charles, 1996 |
|
Rice FJ, Lanctot CA, & Garcia-Devesa D: Effectiveness of the sympto-thermal method of natural family planning: an international study. International Journal of Fertility 26(3):222-230, 1981 |
|
Marshall J: A prospective trial of the muco-thermal method of natural family planning. International Review of NFP Vol IX NO 2 Summer:p139-143, 1985 |
|
Barbato M, Bartoletti M: Natural methods of fertility control-Prospective study. International Journal of Fertility and Sterility 5 (Suppl):48-51, 1988 |
|
Clubb EM, Pyper CM, Knight J: ‘A pilot study on teaching NFP in general practice’. Natural family planning: Current knowledge and new strategies for the 1990's. Part II Preceedings of a conference, Georgetown University, Washington DC, 130-132, 1990 |
|
Freundl G: European multi-centre study of family planning (1989–1995). Advances in contraception. 15:69-83, 1999 |
|
Frank-Herrmann P, Heil J, Gnoth C, Toledo E, Baur S, Pyper C, Jenetzky E, Strowitzki1 T, Freundl G. The effectiveness of a fertility awareness based method to avoid pregnancy in relation to a couple’s sexual behaviour during the fertile time: a prospective longitudinal study. Human Reproduction 2007 1–10. |
|
Lamprecht V, Trussell J: Natural family planning effectiveness: evaluating published reports. Adv Contracept 13:155-165, 1997 |
|
Kambic R: The effectiveness of natural family planning methods for birth spacing: A comprehensive review. In: Girotto S, Bressan F (eds): Human Fertility Regulation–Demographic and Statistical Aspects. p 63-90, Verona, Edizioni Libreria Cortina, 1999 |
|
Frank-Hermann P, Freundl G, Gnoth CH et al: Natural family planning with and without barrier method use in the fertile phase: efficacy in relation to sexual behaviour: a German prospective long-term study. Adv Contracept 13:179-189, 1997 |
|
Kowal D: Coitus Interruptus (Withdrawal). In: Hatcher RA, Trussell J, Stewart F, et al (eds): Contraceptive Technology. pp 303-307, New York, Ardent Media, 1998 |
|
Zukerman Z, Weiss DB, Orvieto R: Does pre-ejaculatory penile secretion originating from Cowper's gland contain sperm. J Assist Reprod Genet 20:157-159, 2003 |
|
Trussel J, Kost K: Contraceptive failure in the US; a critical review. In: Hatcher RA, Trussell J, Stewart F, et al (eds): Contraceptive Technology. p 216, New York, Ardent Media, 1998 |
|
Walker AE: The Menstrual Cycle. p 134, Routledge, 1997 |
|
Marshall J: Love One Another: Psychological Aspects of Natural Family Planning. p 1, Sheed and Ward, 1996 |
|
Marshall J, Rowe B: Psychological aspects of the basal body temperature of regulating births. Fertil Steril 21:14-19, 1970 |
|
Bonnar J, Lamprecht V, O'Conner E: Alternatives to vaginal intercourse practiced during the fertile time among calendar method users in Ireland. Adv Contracept 13:173-177, 1977 |
|
Guillebaud J: Is It Ethical to Use EC contraception? Contraception–Your Questions Answered. p 428, 3rd ed.. Churchill Livingstone, 1999 |
|
Gray R, Simpson JL et al: Timing of conception and risk of spontaneous abortion among pregnancies occurring during the use of natural family planning. Am J Obstet Gynecol 172:1567-1572, 1995 |
|
Simpson JL et al: Pregnancy outcome in natural family planning users: cohort and case-control studies evaluating safety. Adv Contracept 13:201-214, 1997 |
|
Gray R et al: Sex ratio associated with timing of insemination and length of the follicular phase in planned and unplanned pregnancies during use of natural family planning. Hum Reprod 13:1397-1400, 1998 |
|
Wilcox AJ, Baird DD, Weinberg CR: Time of implantation of the conceptus and loss of pregnancy. N Engl J Med 340:1796-1799, 1999 |
|
FPA UK: Body Works. Feb 2000. |
|
World Health Organization: A prospective multicenter trial of the ovulation method of natural family planning. II. The effectiveness phase Fertil Steril 36:591-598, 1981 |
|
Gray R, Simpson JL, Bitto A et al: Sex ratio associated with timing of insemination and length of the follicular phase in planned and unplanned pregnancies during use of natural family planning. Hum Reprod 13:1397-1400, 1998 |
|
Vessey MP, Smith MA, Yeates D: Oxford FPA study: Return of fertility after discontinuation of oral contraceptives–influence of age and parity. BrJ Fam Plan 11:20-40, 1986 |
|
Farrow A, Hull MGR et al: Prolonged use of oral contraception before a planned pregnancy is associated with a decreased risk of delayed conception [ALSPAC study]. Hum Reprod 17:2754-2761, 2002 |
|
Gnoth C, Frank-Herrmann P, Schmoll A et al: Cycle characteristics after discontinuation of oral contraceptives. Gynecol Endocrinol 16:307-317, 2002 |
|
Glasier A, McNeilly AS: Physiology of lactation. Baillieres Clin Endocrinol Metab 4:379-395, 1990 |
|
Thapa S, Short R, Potts M: Breast-feeding, birth spacing and their effects on child survival. Nature 335:679-682, 1988 |
|
Potts M, Short R: Ever Since Adam And Eve, The Evolution of Human Sexuality. pp 150-154, Cambridge University Press, 1999 |
|
Kennedy KI: Consensus Statement: Breast-feeding as a Family Planning Method. Report by Kathy Kennedy from the Bellagio Study & Conference Centre; Italy Lancet 1204-1205, 1988 |
|
Labbok M, Cooney K, Coly S: Guidelines: Breast-feeding, family planning, and the lactational amenorrhoea method–LAM. Washington DC, Institute for Reproductive Health, Georgetown University. 1994 |
|
Kennedy KI, Trussel J: Postpartum contraception and lactation. In: Hatcher RA, Trussell J, Stewart F (eds): Contraceptive Technology. pp 589-614, New York, Ardent Media, 1998 |
|
WHO Task Force on Methods for the Natural Regulation of Fertility: The World Health Organisation Multinational Study of breast-feeding and lactational amenorrhoea. III Pregnancy during breast-feeding Fertil Steril 72:431-440, 1999 |
|
FPA: Contraceptive Education Bulletin, Winter 2000, Update, FPA.P2 |
|
WHO: 2001 The optimal duration of exclusive breast-feeding–Results of a WHO systematic review. Available at: http://www.who.int/inf-pr-2001/en/note2001-07.html Accessed April 18, 2002 |
|
Boseley S: Guardian. May 12th 2003 |
|
UNICEF: UK Baby friendly initiative. Available at http://www.babyfriendly.org.uk. Accessed April 18 2002 |
|
Department of Health: Infant Feeding Survey 2000. Available at: www.doh.gov.uk Accessed August 2001 |
|
Howie PW: Effect of supplementary food on suckling patterns and ovarian activity during lactation. Br Med J 283, 1981 |
|
IPPF: Family Planning Handbook for Health Professionals. 172, 1997 |
|
Knight J, Pyper C: Postnatal contraception what are the choices? Nurs Pract 5:23-25, 2002 |
|
Guillebaud J: Contraception–Your Questions Answered. 3rd ed. London, Churchill Livingstone, 1999 |
|
Andrews G: Women's Sexual Health. pp 178-184, London, Bailliere Tindall, |
|
Clubb E, Knight J: Fertility–Fertility awareness and natural family planning. p 84, David & Charles, Newton Abbot, 1996 |
|
Guillebaud J: Contraception Today. p 44, London, Martin Dunitz, 1995 |
|
Truitt ST, et al: Combined hormonal versus non-hormonal versus progestin-only contraception in lactation (Cochrane Methodology Review). In: The Cochrane Library, Issue 4, 2003. Chichester UK: John Wiley & Sons, Ltd. |
|
Flynn A: Symptothermal and hormonal markers of potential fertility in climacteric women. Am J Obstet Gynecol 165:1987-1989, 1991 |
|
Knight J, Pyper C: Integrating fertility awareness into family planning consultations. Contraceptive Education Bulletin. p 5, FPA Spring 1999, |