Lifestyle and Behavioral Therapies for Urinary Incontinence
Authors
INTRODUCTION
Behavioral treatments are a group of interventions that improve urinary incontinence and other lower urinary tract symptoms by changing the patient’s daily habits or environment or teaching new skills. One basic approach to behavioral treatment focuses on improving bladder control by modifying voiding habits, such as with scheduled voiding or delayed voiding. Another basic approach focuses on the bladder outlet, strengthening pelvic floor muscles and using them to prevent leakage and control bladder function.
In clinical practice, behavioral interventions are usually comprised of multiple components, tailored to the individual needs of the patient, the characteristics of her symptoms, and her life circumstances. Among the techniques included in behavioral treatment programs are: self-monitoring with a bladder diary, pelvic floor muscle training techniques (including biofeedback or digital teaching), pelvic floor muscle exercise regimens, active use of pelvic floor muscles for urethral occlusion (stress strategies, the knack), urge control and urge suppression strategies, urge avoidance strategies, scheduled voiding regimens (including bladder training), delayed voiding, teaching normal voiding techniques, fluid management, dietary changes to avoid bladder irritants (including caffeine), weight loss, management of constipation, and other lifestyle changes. It is generally accepted that the best behavioral programs are implemented with the supervision of a health care provider to ensure that the patient is guided in the correct skills, and to facilitate adherence in the early phases of treatment.
The behavioral programs with the most evidence are pelvic floor muscle training, behavioral training with urge suppression, and bladder training. Each of these programs has a central defining characteristic, but they are multi-component by nature and have been implemented successfully using a wide variety of specific parameters. Other behavioral interventions, such as fluid management and reducing bladder irritants, have less evidence, but they are used widely because they are safe and without the risks and side effects associated with some other therapies.
Although they are not curative in most patients, it is well established that behavioral interventions are effective for improving symptoms, as described in several systematic reviews.1, 2, 3, 4, 5, Further they are recommended as first-line therapies by several consensus panels and societies, including the International Consultation on Incontinence and the American Urological Association Guideline on Diagnosis and Treatment of Overactive Bladder in Adults.1, 3, 6
PATIENT EDUCATION
Most behavioral programs can be considered self-management programs requiring the active engagement of the patient. Social cognitive theory tells us that patients will adopt new behaviors if they believe they can perform them, and if they believe that doing so will lead to a good outcome. Thus, it is important that any behavioral program begin by providing basic patient education, so that the patient can understand her condition, the treatment process and the therapeutic goals.
Patient education includes an explanation of the anatomy of the bladder and pelvic floor, how they function normally, and the causes and mechanisms of urinary incontinence. Patients also need to understand their role in the treatment process, which begins with discussing the relevant treatment options and informing patients about what each treatment entails. This enables patients to ascertain their ability to change their habits and learn new skills and be prepared to engage in the treatment process. In particular, it is essential for women to understand that their therapeutic outcomes will depend on their active participation and daily practice.
As women consider whether their efforts could lead to a positive outcome, it is important they understand that behavioral treatments yield significant improvements for most patients who comply, but they are not usually curative. Further, understanding that improvement is often gradual facilitates realistic expectations about potential therapeutic outcomes.
ASSESSMENT AND BLADDER DIARIES
Because behavioral treatments are safe and reversible, the assessment consists primarily of the medical history and detailed continence history, including characteristics of symptoms, onset, course, and duration. Most relevant for developing a behavioral program is understanding the patient's daily life and the circumstances that precipitate urine loss. To expand on the patient's verbal description of her symptoms, having her complete a bladder diary for 5–7 days can be extremely informative and revealing.7, 8
In the assessment phase, a diary provides information on the type and frequency of urine loss, frequency of micturition, and other symptoms, which helps the clinician plan appropriate components of behavioral intervention. Usually, patients record the time of each incontinent episode, its size, and the circumstances or reasons for the episode. In addition, it is useful for patients to record the times that they void, which provides a foundation for determining baseline voiding intervals in bladder training programs. Voided volumes are more burdensome to document and are usually recorded for only 24−48 hours, but they provide a practical estimate of the patient’s functional bladder capacity in daily life. To improve the chances of obtaining a useful diary, it is best to look at the diary with the patient in person, review its component, and explain how and when to fill it out. Patients should be encouraged to carry the diary with them at all times and to make entries as soon as it is feasible.
During the course of treatment, the diary can be used to monitor symptoms and to guide the intervention by tracking the efficacy of various treatment components. In addition to informing the provider, the self-monitoring effect of completing the diary enhances the patient’s awareness of voiding habits and helps them recognize how their incontinence may be related to their activities.9 By reviewing the bladder diary with the clinician, patients can identify the times when they are at increased risk of an incontinence episode and activities that trigger incontinence. In particular, learning about the circumstances that precipitate urine leakage prepares the patient to implement the continence skills they are about to learn.
PELVIC FLOOR MUSCLE TRAINING
Pelvic floor muscle training (PFMT) is the cornerstone of any behavioral or physical therapy treatment program for incontinence or overactive bladder. PFMT was first described by Margaret Morris in 193610 who described tensing and relaxing of the pelvic floor muscles as an approach to the prevention and treatment of urinary incontinence. PFMT was later popularized in the 1950s by Arnold Kegel, a gynecologist who proposed that stress incontinence was due to a lack of awareness of function and coordination of pelvic floor muscles, and reported significant reductions of stress incontinence using pelvic floor muscle exercise.11, 12 Over the decades, PFMT has evolved both as a behavioral therapy and as a physical therapy, combining principles from behavioral science, nursing, physical therapy, and muscle physiology into a widely recommended conservative treatment for stress incontinence, as well as urgency incontinence and other lower urinary tract symptoms.
Teaching pelvic floor muscle control
The goal of behavioral treatment for stress incontinence is to teach patients how to improve urethral closure and bladder neck support by voluntarily contracting pelvic floor muscles during whatever physical activities precipitate urine leakage. The first step is to properly identify the pelvic floor muscles and to contract and relax them selectively (without increasing intra-abdominal pressure on the bladder or pelvic floor). Confirming that patients have identified the correct muscles is an essential and often overlooked step. While it is easy for the clinician to give patients a pamphlet or brief verbal instructions to “lift the pelvic floor” or to interrupt the urinary stream during voiding, these approaches do not ensure that she knows which muscles to use before she is sent home to do daily exercises.
Most often, proper muscle contraction can be taught using digital palpation and verbal feedback. It can also be taught using biofeedback or electrical stimulation. Biofeedback is a teaching technique that helps patients learn control by giving them instantaneous feedback of their pelvic floor muscle activity, based on manometric or electromyographic (EMG) measurements. Kegel designed a simple biofeedback device he called the perineometer.11 This device consisted of a pneumatic chamber (placed in the vagina) and a hand-held pressure gauge, which visually displayed the pressure generated by circumvaginal muscle contraction.
Now, most biofeedback instruments are computerized and display feedback visually on a computer monitor. Pelvic floor muscle activity can be measured by manometry or EMG, using vaginal or anal probes or surface electrodes. Signals are enhanced via computer, and feedback is provided visually on a monitor or via speakers for auditory feedback. When patients observe the results of their attempts to control bladder pressure and pelvic floor muscle activity, learning occurs by means of operant conditioning (trial and error learning). Some clinicians use electrical stimulation, resistive devices, or weighted vaginal cones to assist or enhance the teaching of pelvic floor muscle control.
When learning to control the pelvic floor muscles, patients tend to recruit other muscles, such as the rectus abdominis muscles or gluteal muscles, especially when the pelvic floor muscles are weak. Contracting certain abdominal muscles can be counterproductive, when it increases pressure on the bladder or pelvic floor, and tends to push urine out rather than holding it in. It is important to observe for any bearing down Valsalva response and to help patients to contract pelvic floor muscles selectively while relaxing these abdominal muscles.
Some practitioners recommend coordinated training of transversus abdominis muscles, because it is thought that these muscles facilitate pelvic floor muscle contraction. This approach remains controversial, however, and a review article on this approach noted an absence of evidence for this type of training.13
Daily pelvic floor muscle exercise
Once patients learn to properly contract and relax the pelvic floor muscles selectively, a regimen of daily practice and exercise is prescribed. The purpose of daily practice is twofold: to increase muscle strength and to enhance motor skills through practice. It has also been reported that intensive strength training may increase resting tone and structural support of the pelvis by elevating the levator plate and enhancing the hypertrophy and stiffness of its connective tissues.14
Many different exercise regimens have been used. They vary considerably on all parameters, including frequency and intensity, but evidence is lacking to recommend one over the other, and the ideal program probably depends on the individual patient. However, good results are generally achieved using 45−60 exercises per day.15, 16 To avoid muscle fatigue, it is usually recommended that patients space the exercises across the day, typically in two or more sessions per day as needed. Patients generally find it easiest to practice the exercises in the lying position at first, but it is important to progress them to sitting or standing positions as well, so that they become comfortable and skilled using their muscles to avoid incontinence in any position.
To improve muscle strength, contractions should be sustained for 2–10 seconds,17, 18 depending on the patient’s initial ability. Exercise regimens should be individualized so that patients begin with a comfortable duration and gradually progress to 10 seconds.18 Each exercise consists of muscle contraction followed by a period of relaxation using a 1:1 or 1:2 ratio.18 This allows the muscles to recover between contractions. A template for individualized instructions for daily pelvic floor muscle exercise appears in Figure 1.
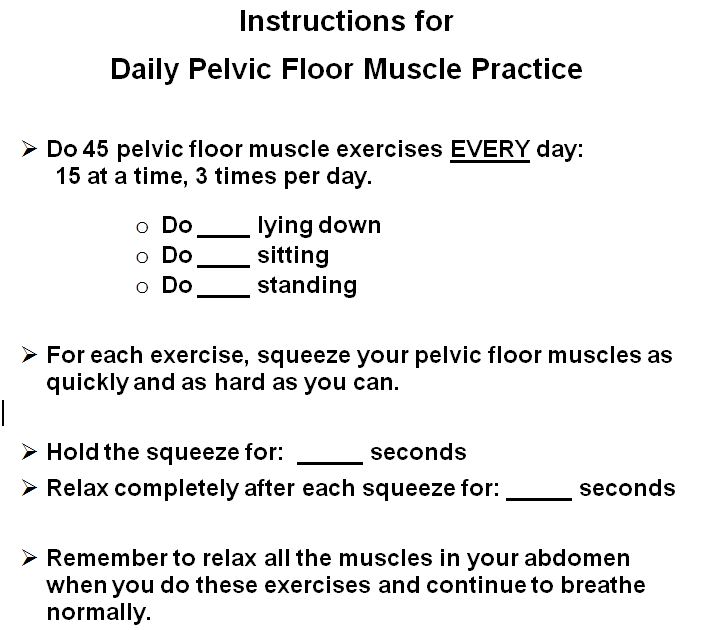 Figure 1 Instructions for daily pelvic floor muscle practice
Figure 1 Instructions for daily pelvic floor muscle practice
It is not uncommon that patients have difficulty adhering to the regimen and sustaining their efforts over time.19, 20 Common barriers include difficulty remembering to do the exercises and difficulty finding time.21, 22 To help patients remember their exercises, a variety of cues can be used, including alarms or notes in prominent places in the home or car. Another approach is to integrate their pelvic floor muscle exercises into their daily activities. Once patients are proficient, they no longer need to set time aside to concentrate on exercises. Rather, they can do a few exercises during certain daily activities, such as taking a shower, standing in line, or sitting at a traffic light. Not only does this save time in their busy schedules, but also the daily activities eventually become cues, reminding them to exercise. This can improve adherence during active treatment, and supports continued exercise during the maintenance phase when motivation tends to wane.
Using muscles to prevent stress incontinence
In PFMT, the focus of treatment is often on the exercise aspect and on increasing muscle strength. Over time, however, more emphasis has been placed on function and coordination, teaching patients to consciously contract the pelvic floor muscles to occlude the urethra during physical activities that cause stress incontinence. Although exercise alone has been known to improve urethral pressure and structural support and reduce incontinence,23 the best results seem to be achieved when patients contract their muscles consciously before and during coughing, sneezing, or any other activities that precipitate urine loss.14 This technique is known as the “stress strategy,”24 “perineal blockage,”25 “perineal co-contraction,” "counterbracing," or “the knack.”26 Initially, this new skill requires a conscious effort, but with consistent practice, patients can develop the habit of automatically contracting their muscles to occlude the urethra in situations of physical exertion.
Even when their muscles are weak, some women will benefit from simply learning how to control their pelvic floor muscles and use them to prevent urine loss. In one trial, women demonstrated reduction in leakage after only 1 week of training to voluntarily contract pelvic floor muscles before or during a cough.26 Pelvic floor muscle pre-contraction has been recommended, not only during coughing, but also during any activity that results in increased intra-abdominal pressure.27 The strength that is needed to occlude the urethra and prevent urine leakage is not known, and likely depends on each woman’s anatomy. But, in addition to learning this skill, some women will still need a more comprehensive program of pelvic floor muscle rehabilitation to increase strength.
The literature on PFMT is extensive, and demonstrates that it is effective for reducing stress, urge, and mixed urinary incontinence in most outpatients who cooperate with training. The majority of studies focus on stress or urgency incontinence in women,1, 2, 4 particularly older women and women in the postpartum period.24, 28, 29, 30, 31, 32, 33, 34, 35, 36 Systematic reviews and the International Consultation on Incontinence (2013) conclude that there is Grade A evidence for pelvic floor muscle training and that it should be offered as first line treatment to women with stress, urgency, or mixed incontinence.1, 2, 4, 37, 38, 39
Studies of PFMT are varied in terms of teaching methods, amount and type of supervision, type of exercise, and exercise intensity (duration, frequency). Studies show that women who receive individual treatment with regular supervision have better outcomes compared to those who receive little or no supervision.40 There is also some evidence that women who receive group supervision in addition to individual PFMT sessions may be more likely to report improvement, but these findings should be interpreted with caution, due to the many other differences between treatment groups. Otherwise, there is inadequate evidence to recommend any particular method or intensity of PFMT. The International Consultation on Incontinence recommends that “clinicians should provide the most intensive health professional led PFMT program possible within service constraints, because professionally taught and supervised programs are better than self-directed programs, and more contact with the provider is better than less”.1
BEHAVIORAL TRAINING WITH URGE SUPPRESSION
Behavioral training is a stand-alone treatment that teaches patients how to use their pelvic floor muscles to inhibit detrusor contraction and how to use this technique as a part of a new strategy for responding to the sensation of urgency. Behavioral training evolved out of biofeedback-assisted behavioral training, in which bladder and anal sphincter biofeedback were used together to teach patients to inhibit detrusor contraction during retrograde bladder filling. Originally, the focus of training was on bladder pressure feedback and learning cortical inhibition of detrusor contraction. During these biofeedback sessions, it was observed that spontaneous sphincter activity appeared to be associated with reduced detrusor pressures. It was subsequently demonstrated that a well-timed, volitional contraction of the anal sphincter (reflecting pelvic floor muscles), guided by visual biofeedback, could suppress fully developed detrusor contractions, deter developing contractions, and suppress urgency.15, 16
Later, it was shown that this skill could be taught without the benefit of biofeedback, using instead verbal feedback based on vaginal palpation. In a randomized controlled trial of behavioral training with and without biofeedback for older women with urgency incontinence, outcomes for women taught using verbal feedback based on vaginal palpation were as good as those achieved using bladder-sphincter biofeedback.41 Thus, behavioral training is now generally conducted without biofeedback, making it more practical and widely available.
Based on these findings, although PFMT and exercise was originally designed for the treatment of stress incontinence, it is now used as a central element in the treatment of urgency incontinence and overactive bladder. In behavioral training, patients are taught pelvic floor muscle control and exercise in the same way as for stress incontinence. What differs is how they use their muscles to respond to urgency and prevent urine loss. In addition to using pelvic floor muscle contraction to occlude the urethra, women learn a new way to respond to urgency.42
Patients with urgency and urgency incontinence often feel the need to rush immediately to the nearest toilet when they feel the desire to void, believing that “when you gotta go, you gotta go” and that emptying their bladder is the only way to relieve the urge. With behavioral training, they learn how this natural response is actually counter-productive, because it increases physical pressure on the bladder, increases the feeling of fullness, exacerbates urgency, and triggers detrusor contraction. Further, as the patient gets closer to the toilet, visual cues can exacerbate urgency and trigger incontinence. To avoid this classically conditioned response, women are taught not to rush to the toilet when they feel the need to void. Instead, they are to stay away from the toilet, so they are not exposed to cues that trigger urgency. They are encouraged to pause, sit down if possible, relax the entire body, and contract the pelvic floor muscles repeatedly, without relaxing in between contractions, to diminish urgency, inhibit detrusor contraction, and prevent urine loss. As they wait for the urge to pass, they focus on inhibiting the urge sensation, giving it time to pass. Once the sensation subsides, they walk at a normal pace to the toilet. (A handout for teaching the urge suppression strategy is in Figure 2.)
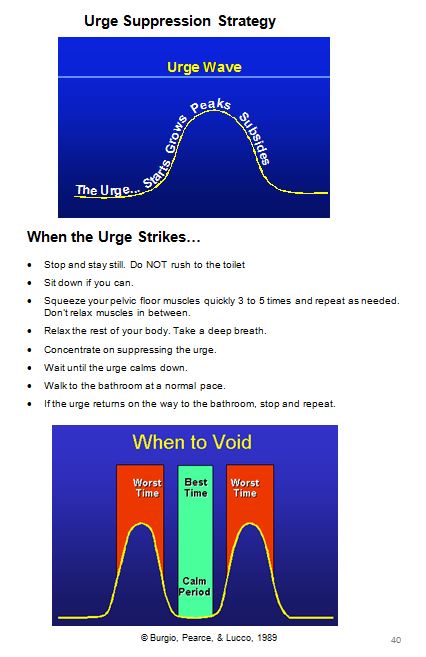 Figure 2 Urge suppression strategy
Figure 2 Urge suppression strategy
Once patients master the urgency suppression strategy, instead of walking to the bathroom immediately after controlling the sensation, they are encouraged to delay voiding for 5 minutes to consolidate their skill. If they are frequent voiders, this delayed voiding interval can be gradually expanded until they achieve a normal voiding frequency.
The effectiveness of behavioral training with urgency suppression as a stand-alone therapy for urgency urinary incontinence has been established in several clinical series studies15, 43, 44 and in randomized controlled trials using intention-to-treat models, in which mean reductions of incontinence range from 60% to 80%.16, 41 In the first randomized controlled trial of behavioral training, older women reduced incontinence episodes significantly more than women who received individually titrated drug treatment, and their perceptions of improvement and satisfaction with their progress were higher as well.16
Behavioral training with urgency suppression has also been shown to reduce nocturia in women.45 Patients are instructed to use urgency suppression techniques when they wake up at night with a need to void. If the urgency passes, they are encouraged to go back to sleep. If the desire to void has not subsided after a minute or two, women are advised to get up and void, so as not to interfere unnecessarily with their sleep. Johnson and colleagues showed that both behavioral training and drug therapy reduced nocturia more than placebo in women, and behavioral training was significantly more effective than drug therapy.45 In addition to being a central element of behavioral training, the urgency suppression strategy has also been adopted as one of several techniques to help patients manage urgency and postpone voiding in bladder training or delayed voiding programs.
BLADDER TRAINING AND OTHER VOIDING SCHEDULES
Scheduled voiding regimens have been used for decades to treat urgency incontinence and functional incontinence by modifying voiding habits. These programs include bladder training, timed voiding, habit training, and prompted voiding. All these approaches are based on a regular toileting schedule, but they differ on whether the patient has an active vs. passive role and how the voiding schedule is determined and adjusted.1 Bladder training is self-administered and requires the patient to resist urgency and delay voiding. Timed voiding, habit training, and prompted voiding, are generally used for patients with cognitive impairment and are implemented by caregivers.
Bladder training
Bladder training was developed originally for the treatment of urgency incontinence. Many patients with urgency incontinence also have excessive frequency of micturition. The premise of bladder training is that habitual frequent voiding can reduce bladder capacity and lead to bladder overactivity, which in turn causes more urgency and urgency incontinence.46, 47 The goal of bladder training is to break this cycle using consistent incremental voiding schedules to reduce voiding frequency, increase bladder capacity, and restore normal bladder function.
Instead of voiding in response to the urgency sensation, bladder training instructs the woman to void at predetermined intervals. In this way, voiding is disassociated from urgency. To determine an appropriate starting voiding interval, the patient completes a voiding diary, which shows the clinician when and how often she voids. After reviewing the diary together with the patient, a voiding interval is selected based on the longest time interval between voids that is comfortable for her. She is then given instructions to void first thing in the morning, every time the interval passes, and before going to bed at night. Over time, the voiding interval is increased at comfortable intervals to a maximum of every 3–4 hours.
The hallmark of bladder training is the expanded voiding interval. But, to follow such a voiding schedule, patients must resist the sensation of urgency and postpone micturition. This requires patients to manage the desire to void while they wait for their voiding interval to pass. The traditional approach to helping patients cope with urgency in bladder training has been to suggest various techniques for relaxation or distraction to another activity.48, 49, 50 Patients are encouraged to get their minds off the bladder by engaging in a task that requires mental but not physical effort. This might include reading, making a telephone call, or making a to-do list. Also affirming self-statements are used, such as “I am in control of my bladder,” or “I can wait.” More recently, traditional bladder training has been enhanced by adopting the urgency suppression strategy from behavioral training (described above). Repeated contractions of the pelvic floor muscles are now often used to control urgency and detrusor contractions while the patient postpones micturition.
Several studies have demonstrated the efficacy of bladder training.5, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59 The first and most definitive study was a randomized clinical trial that showed a mean 57% reduction in frequency of incontinence in older women.48 In this trial, bladder training not only reduced incontinence associated with detrusor overactivity, but also incontinence associated with sphincter insufficiency, possibly because patients developed a greater awareness of bladder function or that having to postpone micturition increased pelvic floor muscle activity. In another trial that compared bladder training to oxybutynin, 73% of women in bladder training were reported to be “clinically cured.”58
Bladder training programs have differed widely in terms of specific voiding schedule parameters, frequency of schedule adjustments, criteria for increasing the voiding interval, strategies for controlling urgency, duration of treatment, intensity of supervision, and use of adjunctive treatments. Because evidence is lacking regarding which parameters are most effective, the International Consultation on Incontinence recommends that clinicians should provide the most intensive bladder training supervision that is possible within service constraints.1
Other scheduled voiding regimens
Voiding schedules are the cornerstone of continence care for cognitively impaired patients and those who require assistance with toileting. Timed voiding, habit training, and prompted voiding are usually “caregiver dependent” and can be beneficial for nursing home residents or women who live at home with a willing caregiver. The choice of program depends upon the cognitive and functional status of the individual, the variability of the patient’s voiding pattern, and the use of positive reinforcement for adherence.
Timed voiding has also been called scheduled toileting, routine toileting, and fixed toileting. With this program, the patient is taken to the toilet every 2–4 hours during waking hours, whether or not she has a sensation to void. The goal is to keep the person dry, and no effort is made to motivate her to resist the urge to urinate. The goal is simply to avoid incontinence by providing regular opportunities for assisted bladder emptying before the bladder reaches capacity. Ideally, the toileting schedule is based on some objective measure, such as a bladder diary. Keeping the bladder volume below capacity may decrease leakage associated with a detrusor contraction, as well as stress leakage that might occur with movement. A brief, 2–3 day trial of timed voiding can determine whether it will be successful for an individual patient. Timed voiding has been recommended for patients who cannot toilet independently.60, 61
Habit training is a variant of timed voiding, in which the toileting schedule is matched to the patient’s voiding pattern, rather than being a fixed interval. Using the patient’s bladder diary, a toileting schedule is developed to fit a time interval that is shorter than the patient’s normal voiding pattern and to precede the time period when incontinent episodes are expected. Thus, the voiding interval may vary throughout the day depending on the patient’s voiding pattern.62 Habit retraining is mainly used in institutional settings or with cognitively and physically impaired homebound adults, but it is also useful for unimpaired adults who have a consistent pattern of incontinence occurring at approximately the same time interval each day or is induced by diuretic use.63
Prompted voiding is a toileting program that combines scheduled, prompted voiding with caregiver reinforcement for patients initiating their own toileting by requesting help. It has been used primarily in nursing home settings with cognitively and physically impaired older adults.64, 65, 66 Prompted voiding includes regular monitoring and encouragement to report continence status, prompting the resident to toilet on a scheduled basis, and positive feedback when she is continent and initiates toileting.67, 68 For prompted voiding to be effective, the individual must be aware of when they need to void, able to delay voiding and able to cooperate with toileting. A 3-day trial of prompted voiding can demonstrate whether it is likely to be effective.69 A systematic review of prompted voiding trials concluded that the treatment decreases in incontinent episodes.70
Delayed voiding
Delayed voiding is another approach to helping patients to expand the intervals between voids, but without placing them on a pre-determined voiding schedule. Even a small sensation of urge can trigger a degree of anxiety in patients who have experienced incontinence. They tend to avoid the feeling by going to the bathroom as soon as possible, rather than exercising any control they may have.
As in behavioral training with urge suppression, delayed voiding encourages patients not to run to the bathroom whenever they have an desire to void, but rather to use their urgency suppression techniques and wait for the desire to subside. Instead of going to the bathroom immediately after the sensation passes, they expand their ability to postpone micturition by waiting a short time before voiding. Most women can usually be convinced to try a 5-minute delay initially, and many are surprised to find that the urgency subsides or disappears altogether after a brief wait. This enhances their sense of control, and once confidence has been restored, the delay interval can be gradually increased to achieve a normal 3–4 hour frequency.
BEHAVIORAL LIFESTYLE MODIFICATIONS
Lifestyle modifications are generally used as adjuncts to a primary behavioral intervention such as pelvic floor muscle training or behavioral training with urge suppression strategies. Lifestyle changes include fluid management, reducing caffeine and other bladder irritants, weight control, and managing constipation.
Fluid management
Changes in the volume or timing of fluid intake are recommended by many clinicians to make it easier for patients to control their bladders. Some patients increase their fluid intake purposefully to “flush” their kidneys, lose weight, or avoid dehydration. Many women carry a water bottle wherever they go, taking frequent drinks for unproven health reasons.71 For others, drinking is simply an unconscious habit. For patients who consume an unnecessarily high volume of fluid (e.g. >2100 ml of output per 24 hours), reducing excess fluids can relieve problems with sudden bladder fullness and resulting urgency or incontinence.72
Conversely, many women with incontinence attempt to self-manage by restricting their overall fluid intake or by not drinking at particular times of day.71, 73, 74, 75, 76, 77 In some cases, particularly in older women, this results in inadequate fluid intake and places them at risk of dehydration. Although it may seem counterintuitive, it is usually good for overall health to encourage the patient to consume an adequate amount of fluid each day. Often recommended is at least 6 glasses of fluid each day.78 Some clinicians espouse that increasing fluid intake will also dilute the urine making it less irritating to the bladder. Renal physicians recommend 24 ml/kg body weight total fluid intake in 24 hours in a temperate climate when not exercising.
It should be noted that restricting fluid intake in the evening hours can be helpful for reducing nocturia. Similarly, it can be very helpful for some women to restrict fluids temporarily when they are away from home and may not have access to a toilet. Women using such targeted fluid restriction should be reminded to compensate for these missed fluids earlier or later to ensure that their total daily fluid intake is adequate.
Caffeine reduction
Caffeine, in addition to being a diuretic,79 is also a bladder irritant for many women. Urodynamic studies have shown that caffeine increases detrusor pressure80 and is a risk factor for detrusor instability (overactivity),81, 82 urgency, and incontinence.83, 84, 85, 86 Further, reducing caffeine intake has been shown to reduce episodes of both stress and urgency incontinence.87, 88, 89
Although it can be very difficult for coffee drinkers to completely eliminate it from their daily routine, if they are informed that caffeine may be aggravating their incontinence, many will be willing to reduce their intake or to eliminate it for a few days as a trial. If they experience relief from their symptoms as a result of the trial, they are often more willing to reduce or eliminate caffeinated beverages from their diet altogether. To avoid symptoms of caffeine withdrawal, caffeine can be reduced quite gradually. The process may be facilitated by replacing caffeinated beverages with decaffeinated beverages incrementally. For example, coffees can be mixed to consist of 25% decaffeinated coffee in week 1, 50% in week 2, 75% in week 3, and full decaffeinated coffee in week 4. It is important to explain to women that tea, green tea and even chocolate contain caffeine.
Bladder irritants
There are a number of dietary substances that have been identified as bladder irritants, including sugar substitutes (especially aspartame), citrus fruits, spicy foods, and tomato products. Although there is little scientific evidence for the effects of these substances on the bladder, many clinicians recommend dietary restrictions as first-line therapy. There are innumerable clinical cases in which these substances appear to be aggravating incontinence, and reducing them has led to clinical improvement.
However, this should not be interpreted to mean that all patients need to eliminate these foods from their diets. It is relatively easy for the clinician to provide a list of forbidden foods and beverages, but it may place undue burden on the patient, and dietary habits are among the most difficult behaviors to change. A diary of food and beverage intake is useful for identifying individual patient sensitivities. Then, a trial period of eliminating these substances systematically can be used to confirm the relationship, before long-term dietary restrictions are recommended.
Weight control
Obesity is a common health problem and an established risk factor for urinary incontinence in women.90, 91, 92, 93 Women with high body mass index are more likely to develop incontinence, and they tend to have more severe incontinence, than women with lower body mass index.94 Research indicates that each five-unit increase in body mass index increases the risk of daily incontinence by approximately 60%.94, 95
Studies of morbidly obese women undergoing bariatric weight loss surgery show significant improvements in incontinence following weight loss of 45–50 kg.96, 97, 98, 99 Non-surgical treatment programs yield less dramatic weight loss, but even 5% reduction in weight has been shown to improve incontinence significantly.100, 101
The most definitive randomized trial of weight loss for incontinence was the Program to Reduce Incontinence with Diet and Exercise (PRIDE) study.102 PRIDE compared an intensive 6-month, group-administered, weight-loss program (including diet, exercise, and behavior modification) to a structured education control program in overweight and obese women with incontinence. Both groups also received a booklet describing a step-by-step self-administered behavioral program to reduce incontinence. After a mean weight loss of 8.0%, the intervention group reported a greater reduction in incontinence episodes compared to the control group (mean = 47% vs. 28%). Because moderate weight loss is an achievable goal for many overweight women, it is reasonable to recommend weight loss as a component in an individualized behavioral program for incontinence in overweight women.
Managing constipation
Fecal impaction and constipation have been cited as factors contributing to urinary incontinence in women, particularly in nursing home populations.103, 104, 105, 106 In severe cases, fecal impaction can obstruct normal voiding, causing incomplete bladder emptying and overflow incontinence. Further, constipation may be an irritating factor in overactive bladder via increased physical pressure on the bladder. Disimpaction usually relieves symptoms, but the effect may be temporary. A bowel management program is often needed to maintain regularity and avoid recurrence. Bowel management may consist of recommendations for normal fluid and fiber intake to maintain normal stool consistency and regular bowel movements. When these usual measures are not fully effective, enemas may be used to stimulate a regular daily bowel movement. Preferably this is done after a regular meal, such as breakfast, to take advantage of postprandial motility.
ADHERENCE AND THE ROLE OF THE PROVIDER
Most behavioral therapies for incontinence are based on self-management models and their success depends on the active participation of a motivated patient. Some patients are self-motivated, but most require assistance from the provider to engage fully in their behavioral program. It can be challenging for women to remember to use their muscles strategically in daily life, as well as to maintain a regular exercise or voiding regimen over time. Self-management is not a concept that every patient understands naturally and they ordinarily need to be empowered to take control of their behavior, including lifestyle and practicing continence skills.
Unlike with some therapies, progress with behavioral treatment is often so gradual as to be imperceptible to the patient. Such gradual change makes it difficult for patients to appreciate even steady improvement over time. According to operant learning principles, positive results reinforce behavior and it is more likely to be repeated. Behaviors that do not produce the desired results tend to be abandoned. Thus, one role of the provider using behavioral interventions is to help the patient sustain her efforts and motivation for long enough to experience a noticeable change in her bladder control.
When initiating behavioral treatment, it is important to make it clear to the patient that her improvement, as with any new skill, will likely be gradual, with good days and bad days, and that it will depend on her consistent practice. The patient who expects this course of treatment will be better prepared to persist over time so that results can be achieved.
In addition to setting expectations, the provider should maintain contact with the patient during the period of time when her benefit is not yet appreciable. Rather than leaving the patient on her own, it is essential that clinicians support the patient’s ongoing efforts by scheduling follow-up appointments to review and reinforce her progress, assess adherence, encourage persistence, identify and address barriers, and make any needed adjustments to her daily regimen.
Even when they achieve noticeable short-term improvements, patients in behavioral treatment tend to have difficulty sustaining a regular regimen long-term, partly because discontinuing the regimen does not result in immediate regression. Little research has examined the durability of behavioral treatments,107, 108, 109, 110 but some studies are promising in that many patients are able to sustain improvements in bladder control up to 5 years after active therapy.107, 108, 109
MODELS OF SERVICE DELIVERY
Historically, behavioral treatments have been implemented in individual sessions by health care professionals, such as a continence nurses, physical therapists, or physicians, in medical settings. Although individually supervised treatment is considered ideal, there is also potential for women to benefit from behavioral interventions using alternate delivery methods, such as internet-based programs111 and group teaching approaches.112, 113, 114, 115, 116, 117, 118 Using alternate delivery methods may expand the availability of behavioral treatment and reduce costs. However, little is known about the feasibility and effectiveness of these methods.
Less intensive delivery methods have the potential to render behavioral interventions less effective. In one study, a low-intensity behavioral therapy program was delivered in weekly 20-min group sessions, and older women showed only a mean 50% reduction in incontinent episodes.116 Similarly, Bo and colleagues studied PFMT taught in a general fitness class for pregnant women and found no difference compared to control groups in the prevalence of urinary incontinence in late pregnancy or in the early postpartum period.117
Conversely, a randomized controlled pilot study of PFMT for stress incontinence in women found that clinical improvements using group sessions were similar to those with individual treatment sessions.118 In another pilot trial, a behavior modification program for incontinence used a single group session followed by individualized reinforcement as needed 2–4 weeks later. Compared to no treatment, the group intervention reduced incontinence and voiding frequency.112 In a later cluster randomized trial, Tennenbaum and colleagues took a community outreach approach to deliver continence education and a self-management intervention for incontinence.113 Group workshops were conducted in not-for-profit community organizations (e.g., interest and charity groups, senior housing groups) resulting in symptom improvements in older women.
Thus, the effectiveness of less intensive or group-administered behavioral interventions may be lower than what is generally reported for individual instruction. But, it may be reasonable to offer treatments using such alternate delivery methods in a range of nonmedical settings, yielding benefit for some participants, and encourage those with insufficient therapeutic response to seek more intensive or individualized approaches. The role and value of several novel instructional methods that capitalize on the efficiencies and dynamics of group delivery have yet to be determined.
SUMMARY
Behavioral interventions are a diverse group of treatments that improve urinary symptoms by altering bladder habits and teaching new skills. They have been used for decades to improve incontinence and other lower urinary tract symptoms in women of all ages. They can be implemented by advanced practice nurses, physical therapists, physicians, or other clinicians in outpatient practice. They do not require special equipment, but they do require the time of a knowledgeable clinician and the active participation of a willing patient.
The collective literature on outpatient behavioral treatments has demonstrated that they are effective for reducing stress, urge, and mixed incontinence, as well as urgency, frequency, and nocturia, in most women who cooperate with treatment. Although most women are not totally cured, the majority will experience meaningful symptom improvements. Behavioral interventions are safe and reversible. They can be combined with any other treatment modality and hold potential for prevention of bladder symptoms. Thus, they are recommended as first-line approaches to the treatment of urinary incontinence and other lower urinary tract symptoms in women.
REFERENCES
Moore K, Dumoulin C, Bradley C, Burgio K, Chambers T, Hagen S, Hunter K, Imamura M, Thakar R, Williams K. Adult Conservative Management. In Abrams P, Cardozo L, Khoury S, Wein A (eds.) Incontinence, 5th International Consultation on Incontinence, Plymbridge UK: Health Publications Ltd, 1101-1227, 2013. |
|
Shamliyan TA, Kane RL, Wyman J, TJ Wilt. Systematic Review: Randomized, Controlled Trials of Nonsurgical Treatments for Urinary Incontinence in Women. Ann Intern Med 2008;148. |
|
Gormley EA, Lightner DJ, Burgio KL, Chai TC, Clemens JQ, Culkin DJ, Das AK, Foster HE, Scarpero HM, Tessier CD, Vasavada SP, American Urological Association, Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. The Journal of Urology 2012; 188: 2455-63. |
|
Dumoulin C, Hay-Smith EJ, Mac Habée-Séguin G: Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev 2014; May 14;5:CD005654. |
|
Roe B, Ostaszkiewicz J, Milne J, Wallace S: Systematic reviews of bladder training and voiding programmes in adults: a synopsis of findings from data analysis and outcomes using metastudy techniques. J Adv Nurs 2007; 57:15-31. |
|
NIH Consensus Conference: Urinary incontinence in adults. JAMA 1989; 261:2685-2696. |
|
Locher JL, Roth DL, Goode PS, et al. Reliability assessment of the bladder diary for urinary incontinence in older women. J Gerontol: Med Sci 2001;56A:M32-M35. |
|
Sampselle CM: Teaching women to use a voiding diary. Am J Nurs 2003;103(11):62-64. |
|
Vella M, Robinson D, Cardozo L, Mastoroudes H, Vig M. The bladder diary: do women perceive it as a useful investigation? Eur J Obstet Gynecol Reprod Biol 2012;162(2):221-223. |
|
Morris M. Maternity and post-operative exercises. London: William Heinemann; 1936. |
|
Kegel AH. Progressive resistance exercise in the functional restoration of the perineal muscles. Am J Obstet Gynecol 1948; 56:238-48. |
|
Kegel AH. Stress incontinence of urine in women: Physiologic treatment. J Int Col Surg 1956; 25:487-99. |
|
Bo K, Morkved S, Frawley H, Sherburn M. Evidence for benefit of transversus abdominus training alone or in combination with pelvic floor muscle training to treat female urinary incontinence: a systematic review. Neurourol Urodynam 2009; 28: 368-373. |
|
Bø K: Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct 2004; 15:76-84. |
|
Burgio KL, Whitehead WE, and Engel BT. Urinary incontinence in the elderly: Bladder-sphincter biofeedback and toileting skills training. Ann Intern Med 1985; 104: 507-515. |
|
Burgio KL, Locher JL, Goode PS, Hardin JM, McDowell BJ, Dombrowski M, Candib D. Behavioral versus drug treatment for urge incontinence in older women: a randomized clinical trial. JAMA 1998; 23:1995-2000. |
|
American College of Sport’s Medicine: ACSM’s Guidelines for Exercise Testing and Prescription, 2nd ed, Lea & Febiger, Philadelphia, 1993. |
|
Kisner C, Colby LA. Therapeutic Exercise. Foundations and Techniques, 4th ed, F.A. Davis, Philadelphia, 2003. |
|
Fine P, Burgio K, Borello-France D, Richter H, Whitehead W, Weber A, Brown M; Pelvic Floor Disorders Network:. Teaching and practicing of pelvic floor muscle exercises in primiparous women during pregnancy and the postpartum period. Am J Obstet Gynecol: 2007;197: 107.e1–e5. |
|
Bø K, Hilde G: Does it work in the long term?-A systematic review on pelvic floor muscle training for female stress urinary incontinence. Neurourol Urodyn 2013;32(3):215-23. |
|
Borello-France D, Burgio KL, Goode PS, Markland AD, Kimberly K, Balasubramanyam A, Stoddard AM, for the Urinary Incontinence Treatment Network. Adherence to behavioral interventions for urge incontinence when combined with drug therapy: Adherence rates, barriers, and predictors. Physical Therapy, 90: 1493-505, 2010. |
|
Borello-France D, Burgio KL, Goode PS, Ye W, Weidner A, Lukacz E, Jelovsek E, Bradley C, Schaffer J, Hsu Y, Kenton K, Spino C for the Pelvic Floor Disorders Network. Adherence to behavioral interventions for stress incontinence: rates, barriers, and predictors. Physical Therapy, 93:757-73. |
|
Bo K. Pelvic floor muscle exercise for the treatment of stress urinary incontinence: an exercise physiology perspective. Int Urogynecol J 1995;6:282-91. |
|
Goode PS, Burgio KL, Locher JL, Roth DL, Umlauf MG, Richter HE, Varner RE, Lloyd LK. Effect of behavioral training with or without pelvic floor electrical stimulation on stress incontinence in women: A randomized controlled trial. JAMA 2003; 290, 345-352 |
|
Bourcier AP, Juras JC, Jacquetin B. Urinary incontinence in physically active and sportswomen. In: Appell RA, Bourcier AP, La Torre F (eds). Pelvic Floor Dysfunction: Investigations and Conservative Treatment. Rome, C.E.S.I. 1999, p. 9-17. |
|
Miller JM, Ashton-Miller JA, DeLancey J. 1998. A pelvic muscle pre-contraction can reduce cough-related urine loss in selected women with mild SUI. J Am Geriatr Soc 1998;46: 870-874. |
|
Carrière B. The pelvic floor. Stuttgard Georg Thieme Verlag; 2006. |
|
Wells TJ, Brink CA, Diokno AD, Wolfe R and Gillis GL. Pelvic muscle exercise for stress urinary incontinence in elderly women. J Am Geriatr Soc 1991;39:785-91. |
|
Berghmans LCM, Frederiks CMA, de Bie RA. Efficacy of biofeedback when included with pelvic floor muscle exercise treatment for genuine stress incontinence. Neurourol Urodynam 1996; 15:37-52. |
|
Nygaard IE, Kreder KJ, Lepic MM, Fountain KA, Rhomberg AT. Efficacy of pelvic floor muscle exercises in women with stress, urge, and mixed urinary incontinence. Am J Obstet Gynecol 1996; 174:120-5. |
|
Bo K, Talseth T. Single blind randomized controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women. BMJ 1999; 318:487-493. |
|
Wilson PD, Herbison GP. A randomized controlled trial of pelvic floor muscle exercises to treat postnatal urinary incontinence. Int Urogynecol J 1998: 9:257 – 264. |
|
Wilson PD, Herbison GP, Glazener CMA, Lang G, Gee H, MacArthur C. Postnatal incontinence: a multicenter, randomized controlled trial of conservative treatment. Neurourol Urodyn 1997; 16: 349-350. |
|
Burns PA, Pranikoff K, Nochajski TH, Hadley EC, Levy KJ and Ory MG. A comparison of effectiveness of biofeedback and pelvic muscle exercise treatment of stress incontinence in older community-dwelling women. J Gerontol 1993; 48:167-74. |
|
Glazener CM, Herbison GP, Wilson PD, MacArthey C, Lang GD, Gee H, Grant A. Conservative management of persistent postnatal urinary and faecal incontinence: a randomized controlled trial. BMJ 2001; 323: 1– 5. |
|
Morkved S, Bo K. Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow-up. Br J Obstet Gynaecol 2000; 107:1022-1028. |
|
Hay-Smith EJC, Dumoulin C: Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews. CD005654, 2006. |
|
Boyle R, Hay-Smith EJ, Cody JD, Mørkved S: Pelvic floor muscle training for prevention and treatment of urinary and fecal incontinence in antenatal and postnatal women: a short version Cochrane review. Neurourol Urodyn 2014;33(3):269-76. |
|
Boyle R, Hay-Smith EJ, Cody JD, Mørkved S: Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev 2012; Oct 17;10:CD007471. |
|
Hay-Smith JE, Herderschee R, Dumoulin C, Herbison PG. Comparisons of approaches to pelvic floor muscle training for urinary incontinence in women. Cochrane Database of Systematic Reviews 2011;8. |
|
Burgio KL, Goode PS, Locher JL, Umlauf MG, Roth DL, Richter HE, et al. Behavioral training with and without biofeedback in the treatment of urge incontinence in older women: a randomized controlled trial. JAMA 2002; 288:2293-2299. |
|
Burgio KL, Pearce KL, and Lucco AJ. Staying Dry: A Practical Guide to Bladder Control. Baltimore: Johns Hopkins University Press, 1989. |
|
McDowell BJ, Burgio KL, Dombrowski M, Locher JL, Rodriguez E. Interdisciplinary approach to the assessment and behavioral treatment of urinary incontinence in geriatric outpatients. J Am Geriatr Soc 1992; 40:370-4. |
|
Baigis-Smith J, Smith DAJ, Rose M, Newman DK. Managing urinary incontinence in community-residing elderly persons. Gerontologist. 1989; 229:33. |
|
Johnson TM, Burgio KL, Goode PS, et al. Effects of behavioral and drug therapy on nocturia in older incontinent women. J Am Geriatr Soc 2005; 53:846-850. |
|
Frewen WK. Role of bladder training in the treatment of the unstable bladder in the female. Urol Clin of N Am 1979;6:273-7. |
|
Frewen WK. A reassessment of bladder training in detrusor dysfunction in the female. Br J Urol 1982;54:372-373.Gynaecol 1989;96:607-12. |
|
Fantl JA, Wyman JF, McClish DK, et al. Efficacy of bladder training in older women with urinary incontinence. JAMA 1991; 265: 609-613. |
|
Wyman JF, Fantl JA, McClish DK, Bump RC, et al. Comparative efficacy of behavioral interventions in the management of female urinary incontinence. Am J Obstet Gynecol 1998; 179: 999-1007. |
|
Wyman JF, Fantl JA: Bladder training in ambulatory care management of urinary incontinence. Urol Nurs 1991;11(3):11-17. |
|
Elder DD, Stephenson TP. An assessment of the Frewen regime in the treatment of detrusor dysfunction in females. Br J Urol 1980; 52:467-71. |
|
Jarvis GJ and Millar DR. Controlled trial of bladder drill for detrusor instability. Br Med J 1980; 281:1322-3. |
|
Jarvis GJ. A controlled trial of bladder drill and drug therapy in the management of detrusor instability. J Urol 1981;53:565-6. |
|
Jarvis GJ. The management of urinary incontinence due to primary vesical sensory urgency by bladder drill. Br J Urol 1982; 54:374-6. |
|
Pengelly AW, Booth CM. A prospective trial of bladder training as treatment for detrusor instability. Br J Urol 1980; 52:463-466. |
|
Svigos, J.M., and Matthews, C.D. Assessment and treatment of female urinary incontinence by cystometrogram and bladder retraining programs. Obstet Gynecol 1977; 50:9-12. |
|
Jeffcoate TNA, Francis WJ. Urgency incontinence in the female. Am J Obstet Gynecol 1966; 94:604-18. |
|
Colombo M, Zanetta G, Scalambrino S, Milani R. Oxybutynin and bladder training in the management of female urinary urge incontinence: a randomized study. Int Urogynecol J 1995; 6:63-67. |
|
Wallace S A, Roe B, Williams K Palmer, M.H. (2009). Bladder training for urinary incontinence in adults. Cochrane Database of Systematic Reviews Issue 1: Art. No. CD001308 |
|
Ostaszkiewicz J, Roe B, Johnston L: Effects of timed voiding for the management of urinary incontinence in adults: systematic review. J Adv Nurs 2005; 52:420-431. |
|
Ostaszkiewicz J, Johnston L, Roe B: Timed voiding for the management of urinary incontinence in adults. Cochrane Database Syst Rev2004; 1: CD002802 |
|
Ostaszkiewicz J, Johnston L, Roe B: Habit retraining for the management of urinary incontinence in adults. Cochrane Database Syst Rev 2004b; 2:CD002801. |
|
Colling J, Owen TR, McCreedy M, Newman D: The effects of a continence program on frail community dwelling elderly persons. Urol Nurs 2003; 23:117-22, 127-31. |
|
Eustice S, Roe B, Paterson J: Prompted voiding for the management of urinary incontinence in adults. Cochrane Database of Systemic Reviews 2000;:CD002113. |
|
Burgio LD, McCormick KA, Scheve AS, Engel BT, Hawkins A, Leahy E: The effects of changing prompted voiding schedules in the treatment of incontinence in nursing home residents. J Am Geriatr Soc 1994;42(3):315-320. |
|
Schnelle JF, Traughber B, Sowell VA, Newman DR, Petrilli CO, Ory M: Prompted voiding treatment of urinary incontinence in nursing home patients: a behavior management approach for nursing home staff. J Am Geriatr Soc 1989; 37: 1051–1057. |
|
Lekan-Rutledge D: Diffusion of innovation. A model for implementation of prompted voiding in long-term care settings. J Gerontol Nurs 2000; 26:25-33 |
|
Lyons SS, Specht JK: Prompted voiding protocol for individuals with urinary incontinence. J Gerontol Nurs. 2000; 26:5-13. |
|
Ouslander JG, Griffiths PC, McConnell E, Riolo L, Kutner M, Schnelle J: Functional incidental training: a randomized, controlled, crossover trial in veterans affairs nursing homes. J Am Geriatr Soc 2005; 53:1091-1100. |
|
Flanagan L, Roe B, Jack B, Barrett J, Chung A, Shaw C, Williams KS: Systematic review of care intervention studies for the management of incontinence and promotion of continence in older people in care homes with urinary incontinence as the primary focus (1966-2010). Geriatr Gerontol Int 2012; 12:600-611 |
|
Elstad EA, Maserejian NN, McKinlay JB, Tennstedt S: Fluid manipulation among individuals with lower urinary tract symptoms: a mixed methods study. J Clin Nurs 2011;20(1-2):156-65. |
|
Swithinbank L, Hashim H, Abrams P. The effect of fluid intake on urinary symptoms in women. J Urol 2005; 174:187-189. |
|
Diokno AC, Burgio K, Fultz NH, Kinchen KS, Obenchain R, Bump RC: Medical and self-care practices reported by women with urinary incontinence. Am J Manag Care 2004;10:69-78. |
|
Diokno AC, Sand PK, Macdiarmid S, Shah R, Armstrong RB: Perceptions and behaviours of women with bladder control problems. Fam Pract. 2006;23(5):568-577 |
|
Johnson TM, 2nd, Kincade JE, Bernard SL, Busby-Whitehead J, DeFriese GH: Self-care practices used by older men and women to manage urinary incontinence: results from the national follow-up survey on self-care and aging. J Am Geriatr Soc 2000;48:894-902. |
|
Fitzgerald S, Palmer MH, Berry SJ, Hart K: Urinary incontinence: Impact on working women. AAOHN Journal 2000;48:112-118. |
|
Fitzgerald ST. Palmer MH, Kirkland VL, Robinson L: The impact of urinary incontinence in working women: a study in a production facility. Women Health, 2002; 35: 1-16. |
|
Dowd TT, Campbell JM, Jones JA. Fluid intake and urinary incontinence in older community-dwelling women. J Community Health Nurs. 1996; 13:179-186. |
|
Lohsiriwat S, Hirunsai M, Chaiyaprasithi B: Effect of caffeine on bladder function in patients with overactive bladder symptoms. Urol Ann 2011;3:14-18. |
|
Creighton SM, Stanton SL. Caffeine: does it affect your bladder? Br J Urol. 1990; 66:613-614. |
|
Arya LA, Myers DL, Jackson ND. Dietary caffeine intake and the risk for detrusor instability: a case-control study. Obstet Gynecol 2000; 96:85-89. |
|
Holroyd-Leduc JM, Straus SE. Management of urinary incontinence in women: scientific review. JAMA 2004; 291:986-995. |
|
Jura YH TM, Curhan GC, Resnick NM, Grodstein F. Caffeine intake, and the risk of stress, urgency and mixed urinary incontinence. J Urol 2011;185:1775-80. |
|
Townsend MK RN, Grodstein F. Caffeine intake and risk of urinary incontinence progression among women. Obstet Gynecol 2012;119:950-957. |
|
Gleason JL RH, Redden DT, Goode PS, Burgio KL, Markland AD: Caffeine and urinary incontinence in US women. Int Urogynecol J 2013;24:295-302. |
|
Maserejian NN, Wager CG, Giovannucci EL, Curto TM, McVary KT, McKinlay JB: Intake of caffeinated, carbonated, or citrus beverage types and development of lower urinary tract symptoms in men and women. Am J Epidemiol 2013;177(12):13991-410. |
|
Tomlinson BU, Dougherty MC, Pendergast JF, Boyington AR, Coffman MA, Pickens SM. Dietary caffeine, fluid intake and urinary incontinence in older rural women. Int Urogynecol J Pelvic Floor Dysfunct 1999; 10:22-28. |
|
Bryant CM, Dowell CJ, Fairbrother G. Caffeine reduction education to improve urinary symptoms. Br J Nurs 2002; 11:560-565. |
|
Gray M. Caffeine and urinary continence. J Wound Ostomy Continence Nurs 2001; 28:66-69. |
|
Milsom, I., Altman, D., Cartwright, R., Lapitan, M.C., Nelson, R., Sillén, U., Tikinen, K: Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI). In Abrams P, Cardozo L, Khoury S, Wein A (Eds.): Incontinence: Proceedings from the 5th International Consultation on Incontinence. Plymouth UK: Health Publications, 2013,pp.15-1075. |
|
Khullar V, Sexton CC, Thompson CL, Milsom I, Bitoun CE, Coyne KS: The relationship between BMI and urinary incontinence subgroups: Results from EpiLUTS. Neurourol Urodyn 2014;33(4):392-399. |
|
Vaughan CP AA, Cartwright R, Johnson TM 2nd, Tähtinen RM, Ala-Lipasti MA, Tammela TL, Markland AD, Thorlund K, Tikkinen KA. Impact of obesity on urinary storage symptoms: results from the FINNO stud. 2012;189(4):1377-1382. |
|
Subak LL, Richter HE, and Hunskaar S: Obesity and urinary incontinence: epidemiology and clinical research update. J Urol 2009;182:S2-7. |
|
Brown J, Grady D, Ouslander J, Herzog A, Varner RE, Posner S: Prevalence of urinary incontinence and associated risk factors in postmenopausal women. Heart & Estrogen/Progestin Replacement Study (HERS) Research Group. Obstet Gynecol 1999; 94:66. |
|
Brown J, Seeley D, Feng J, et al: Urinary incontinence in older women: who is at risk? Study of Osteoparotic Fractures Research Group. Obstet Gynecol 1996; 87:715. |
|
Bump R, Sugerman H, Fantl J, et al: Obesity and lower urinary tract function in women: effect of surgically induced weight loss. Am J Obstet Gynecol 1992; 166:392. |
|
Deitel M, Stone E, Kassam HA, et al: Gynecologic-obstetric changes after loss of massive excess weight following bariatric surgery. J Am Coll Nutrition 1988; 7:147. |
|
Burgio KL, Richter HE, Clements RH, Redden DT, Goode PS. Changes in urinary and fecal incontinence symptoms with weight loss surgery in morbidly obese women. Obstet Gynecol 2007; 110:1034-40. |
|
Knoepp LR, Semins MJ, Wright EJ, Steele K, Shore AD, Clark JM, Makary MA, Matlaga BR, Chen CC: Does bariatric surgery affect urinary incontinence? Urology 2013;82(3):547-551. |
|
Subak LL, Johnson CEW, Boban D, et al: Does weight loss improve incontinence in moderately obese women? Intl J Urogyn 2002; 13:40. |
|
Wing RR, Creasman JM, West DS, Richter HE, Myers D, Burgio KL, Franklin F, Gorin AA, Vittinghoff E, Macer J, Kusek JW, Subak LL; Program to Reduce Incontinence by Diet and Exercise:. Improving urinary incontinence in overweight and obese women through modest weight loss. Obstet Gynecol 2010;116:284-292. |
|
Subak LL, Wing R, West DS, Franklin F, Vittinghoff E, Creasman JM, Richter HE, Myers D, Burgio KL, Gorin AA, Macer J, Kusek JW, Grady D, for the Program to Reduce Incontinence by Diet and Exercise (PRIDE). Weight loss to treat urinary incontinence in overweight and obese women. New Eng J Med 2009; 360:481-90. |
|
Ouslander JG, Schnelle JF. Incontinence in the nursing home. Ann Intern Med 1995; 122:438-49. |
|
Carter D, Beer-Gabel M: Lower urinary tract symptoms in chronically constipated women. Int Urogynecol J 2012; 23: 1785–1789. |
|
Coyne KS, Cash B, Kopp Z, Gelhorn H, Milsom I, Berriman S, Vats V, Khullar V: The prevalence of chronic constipation and faecal incontinence among men and women with symptoms of overactive bladder. BJU Int 2011; 107: 254–61. |
|
Manning J, Korda A, Benness C, Solomon M: The association of obstructive defecation, lower urinary tract dysfunction and the benign joint hypermobility syndrome: a case-control study. Int Urogynecol J Pelvic Floor Dysfunct 2003; 14: 128–132. |
|
Weinberger MW, Goodman BM, Carnes M. Long-term efficacy of nonsurgical urinary incontinence treatment in elderly women. J Gerontol 1999; 54:M117-21. |
|
Bo K, Talseth T. Long-term effect of pelvic floor muscle exercise 5 years after cessation of organized training. Obstet Gynecol 1996; 87:261-5. |
|
Cammu H, Van Nylen M. Pelvic floor muscle exercises: 5 years later. Urology 1995; 45:113-118. |
|
Bø K, Kvarstein B, Nygaard I: Lower urinary tract symptoms and pelvic floor muscle exercise adherence after 15 years. Obstet Gynecol 2005;105(5 Pt 1):999-1005. |
|
Sjostrom M, Umefjord G, Stenlund H, Carlbring P, Andersson G, Samuelsson E. Internet-based treatment of stress urinary incontiennce: a randomised controlled study with focus on pelvic floor muscle training. BJU Int 2013. |
|
Diokno AC, Ocampo MS, Ibrahim IA, Karl CR, Lajiness MJ, Hass SA. Group session teaching of behavioral modification program (BMP) for urinary incontinence: a randomized controlled trial among incontinence women. Int Urol Nephrol 2010; 42: 375-81. |
|
Tannenbaum C, Agnew R, Benedetti A, Thomas D, van de Heuvel E. Effectiveness of continence promotion for older women via community organisations: a cluster randomised trial. BJM Open 2013; 3:1-10. |
|
Dugan SA, Lavender MD, Hebert-Beirne J, Brubaker L. A pelvic floor fitness program for older women with urinary symptoms: a feasibility study. Physical Medicine and Rehabilitation 2013; 5: 672-6. |
|
McFall SL, Yerkes AM, Cowan LD. Outcomes of a small group educational intervention for urinary incontinence: episodes of incontinence and other urinary symptoms. J Aging Health 2000; 12:250-67. |
|
Subak LL, Quesenberry CP, Posner SF, Cattolica E, Soghikian K. The effect of behavioral therapy on urinary incontinence: a randomized controlled trial. Obstet Gynecol 2002; 100:72-78. |
|
Bo K, Haakstad LA. Is pelvic floor muscle training effective when taught in a general fitness class in pregnancy? A randomized controlled trial. Physiotherapy. 2011; 97:190–5. |
|
Pereira VS, Correia GN, Driusso P. Individual and group pelvic floor muscle training versus no treatment in female stress urinary incontinence: a randomized controlled pilot study. Eur J Obstet Gynecol Reprod Biol. 2011; 159:465–71. |