Vaginal Rejuvenation and Cosmetic Vaginal Surgery
Authors
INTRODUCTION
Vaginal rejuvenation and cosmetic genital vaginal surgery have been performed and popularized increasingly in gynecology, urogynecology and plastic surgery. However, controversy and debate over the subject remain the most discussed issue in this area, not the in-depth surgical techniques. The line between cosmetic and medically indicated surgical procedures is a gray-area, and procedures are performed for both purposes. In the current chapter we review the background and history of these procedures, the available data to support them as well as review techniques and complications of the procedures. In addition, we discuss some of the controversy surrounding these topics. Finally, we also attempt to shed light on what is myth and what is science in this relatively new field of elective genital vaginal surgery for sexual function and cosmesis of the female vagina and vulva.
The current chapter is divided into two sections, the first covering vaginal rejuvenation procedures and the second covering external vaginal/vulvar cosmetic surgery. Many use the term “Vaginal Rejuvenation” to encompass all elective vaginal/vulvar surgery; however, we feel that it should be used only to refer to functional procedures of the internal vaginal canal and introitus that are designed to enhance sexual function, which includes ensuring adequate support of the pelvic floor and then internal vaginal canal repairs and repair of the introitus. Similarly, cosmetic vaginal surgery to many just means labiaplasty or labial minora reduction, however, as demonstrated in the second section of the chapter, it is much more comprehensive than this. Therefore, we have defined “cosmetic vaginal/vulvar surgery” as cosmetic or aesthetic procedures of the outside of the vagina and/or vulva, including labiaplasty, labia minora reduction, excess or redundant clitoral prepuce reduction, labia majora reduction or augmentation, labia majora divergence repair, perineal skin reduction and mons pubis reduction. In most instances to achieve the outcome desired by the woman, a combination of these external cosmetic procedures needs to be undertaken, truly bringing in the “art” of aesthetic surgery.
VAGINAL REJUVENATION
Vaginal rejuvenation has also been defined to include perineoplasty and vaginoplasty, which are techniques to “tighten” the vaginal canal and to elevate and strengthen the perineal body.1 The purpose of these procedures is not to correct pelvic floor defects, but they are modifications of traditional colporrhaphy designed to repair the damage from childbirth and are frequently performed concomitantantly with reconstructive procedures for pelvic organ prolapse. These procedures involve vaginal reconstructive techniques to anatomically modify the vaginal caliber by decreasing the diameter of the vaginal canal while reconstructing the perineal body and the vaginal introitus in an attempt to enhance sexual gratification for the woman.2, 3, 4 Utilizing this definition, one realizes that this is not a new field at all, i.e. gynecologists have been dealing with sexual dysfunction related to vaginal pathology resulting mostly from vaginal childbirth for hundreds of years. However, the implication of this definition is to give credence to women’s complaints of altered sexual function secondary to vaginal relaxation/looseness (Figure 1) and possibly to perform vaginal repairs prior to developing signs or symptoms of true prolapse or incontinence. Many women who are candidates for vaginal rejuvenation have symptoms and clinical findings of prolapse. Therefore, a proper repair must involve restoring the foundation of pelvic floor support and encompass some of the newer concepts of vaginal rejuvenation in the repair.
 Figure 1a Vaginal laxity and damaged perineum
Figure 1a Vaginal laxity and damaged perineum
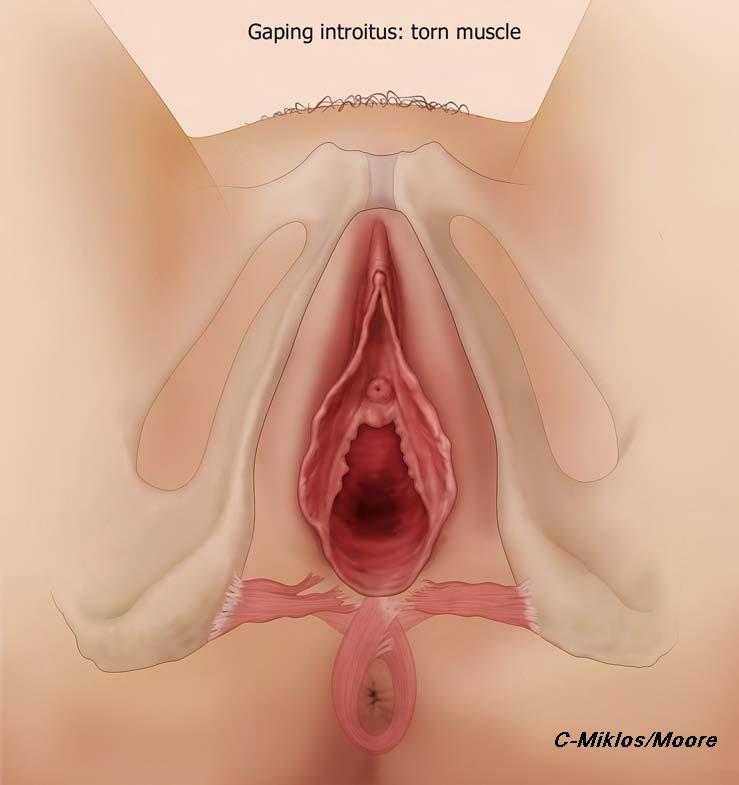 Figure 1b Gaping introitus – torn muscle
Figure 1b Gaping introitus – torn muscle
 Figure 1c Gaping introitus
Figure 1c Gaping introitus
Prolapse and vaginal relaxation occurring after vaginal childbirth is not a new concept. We have clear evidence that vaginal delivery increases the risk of vaginal support problems, vaginal relaxation, prolapse and incontinence. Various pathophysiologic studies have demonstrated marked changes after vaginal delivery to levator muscles,5, 6 nerves,7 and pelvic support.8 It is obvious that parous women are more likely to have pelvic organ prolapse, fecal incontinence, and urinary incontinence than women who have not borne children.9 There is ample epidemiological evidence that vaginal delivery appears to be the strongest risk factor for pelvic floor disorders.10 As evident in the Women’s Health Initiative,11 women who had borne at least one child were twice as likely to have uterine prolapse, rectocele, and cystocele as nulliparas, after adjusting for age, ethnicity, body mass index, and other factors. The amount of damage at the time of vaginal childbirth has also been shown to be strongly correlated with sexual function. At 6 months postpartum, women with an intact perineum or first-degree perineal tear were less likely to experience sexual dysfunction than those with higher degree of perineal tear.12, 13 Interestingly, 80.4% of urogynecologists stated that they would agree to perform elective primary cesarean section on request.14
PROLAPSE AND SEXUAL FUNCTION
Female sexual dysfunction is defined as a disorder of sexual desire, arousal, orgasm and/or sexual pain, contributing to personal distress.15 Sexual dysfunction is a multifactorial disorder; biological, psychosocial, and relational factors can contribute to female sexual dysfunction. Among these factors, the pelvic floor appears to have an important influence. Dysfunction of vaginal support leading to incontinence, prolapse and sexual dysfunction is highly prevalent.16
It is beyond the scope of this chapter to review all of the anatomy, neuroanatomy of pelvic floor support and its relation to sexual function; however, there is good evidence that vaginal childbirth, as well as some other environmental and genetic factors, can lead to issues with pelvic floor support which in turn can affect sexual function. Again, repairs of pelvic floor and vaginal support have been completed for many, many years and one would not argue that one of the goasl of any of these repairs is to “restore sexual function”, therefore we must make the assumption that vaginal relaxation and prolapse affects sexual function in a negative way.
The literature also supports this theory. There have been many studies published in the literature that confirm, with validated sexual function questionnaires, that prolapse affects sexual function and when repaired, function improves (Tables 1 and 2). These studies have confirmed that prolapse, albeit a more severe form of vaginal relaxation, but certainly relaxation, does adversely impact sexual function.
Table 1 Pelvic organ prolapse (POP) effects on sexual function
| Author, year | Study design | N | Objective | Population | Sexual function measurement | Results |
| Ellerkmann et al., 200117
| Prospective observational study | 237 | To compare the symptoms that are related to pelvic floor dysfunction with the location and severity of the coexisting prolapse | Patients with symptomatic pelvic organ prolapse came to Johns Hopkins Medicine | The Pelvic Floor Dysfunction Questionnaire | Increasing severity of POP is associated with sexual dysfunction |
| Barber et al., 200218 | Multi-armed clinical trial | 343 | To compare sexual function in women with urinary incontinence and pelvic organ prolapse | 343 community-dwelling women older than 45 years with urinary incontinence or advanced prolapse | The condition-specific sexual function questionnaire | 33.3% POP group felt that prolapsed or urine leakage affected their ability to have sexual relations compared with 10% of urinary incontinence group (p = 0.02) |
| Novi et al., 200519 | Unmatched case-control | 60 | To compare sexual function in women with vs. without POP | 30 women with pelvic organ prolapse and it was compared with 30 unmatched controls without evidence of prolapse | PISQ | Pelvic organ prolapse appears to have a significant negative impact on sexual function compared with control (81.4 ± 7.3 vs. 106.4 ± 15.5, p <0.001) |
| Botros et al., 200620 | Identical twin study | 542 | To assess the impact of childbirth on sexual function | 276 identical, sexually active twins | PISQ-12 | Nulliparous women reported superior sexual satisfaction scores compared with parous women, regardless of age and mode of delivery (102.5 vs. 93.5, p <0.001) |
| Srikrishna et al., 200821 | Prospective observational study | 43 | To evaluate the expectations and goals of women undergoing surgery for POP | Women with symptomatic POP were recruited from the waiting list for pelvic floor reconstructive surgery | The prolapse quality-of-life (pQoL) questionnaire | 20% women were dissatisfied with their sex lives as a result of their prolapse |
Table 2 Pelvic organ prolapse (POP) repair improved sexual function studies
| Author, year | Study design | N | Objective | Population | Sexual function measurement | Results |
| Barber et al., 200222 | Multi-armed clinical trial | 343 | To compare sexual function in women with urinary incontinence and POP | 343 community-dwelling women older than 45 years with urinary incontinence or advanced prolapse | The condition-specific sexual function questionnaire | Fewer patients with POP reported that their prolapse affected their ability to have sexual relations 6 months after vaginal reconstructive surgery than at baseline (0% vs. 33%, p <0.01). |
| Roger et al., 200623 | Prospective observational | 269 | To assess sexual function in women after surgery for stress urinary incontinence and/or pelvic organ prolapse at 3 and 6 months | Women underwent a variety of anti-incontinence and reconstructive surgeries | PISQ | Sexual function scores improved after surgery (89 vs. 95, p <0.001) |
| Stoutjesdijk et al., 200624 | Prospective observational | 67 | To compare sexual function in women with POP before and after vaginal reconstructive surgery | Women who underwent vaginal reconstructive surgery | The urogenital distress inventory and incontinence impact questionnaire revisited | There was a significant improvement of dyspareunia after surgery. The ability to have intercourse, the satisfaction and the frequency of intercourse improved although not significantly |
| Paraiso et al., 200625 | Randomized controlled trial | 106 | To compare outcomes of 3 different rectocele repair techniques (posterior colporrhaphy, site-specific rectocele repair, or site-specific rectocele repair augmented with a porcine small intestinal submucosa graft) | Patients undergoing surgery for stage II or greater posterior vaginal wall prolapse | PISQ-12 | PISQ-12 improved significantly in all groups postoperatively (p <0.001), with no differences between groups |
| Handa et al., 200726 | The CARE trial | 224 | To describe sexual function before and after sacrocolpopexy | Stress-continent women planning abdominal sacrocolpopexy for stage II–IV prolapse | PISQ-12 | Among women who were sexually active before and after surgery, the mean PISQ-12 score improved significantly (34.1 ± 5.2, p <0.001) |
| Komesu et al., 200727 | Multicenter prospective cohort | 73 | To determine the effect of posterior repair (PR) on sexual function in patients who have undergone incontinence and/or pelvic reconstructive surgery | Sexually active patients who had undergone pelvic reconstructive and/or incontinence procedures | PISQ | Significantly improved their PISQ scores in both PR and non-PR groups, without a difference between groups |
| Azar et al., 200828 | Prospective observational | 60 | To evaluate the effect of surgical repair of POP on female sexual function | Women with POP | FSFI | Sexual function was improved 12–16 weeks postoperatively (15.9±10.7 vs. 21.9±11.1, p <0.05) |
| Kuhn et al., 200929 | Prospective observational | 70 female, 64 male | To determine the male and female sexual function before and 4 months after surgery for POP | Sexually active heterosexual couples with symptomatic cystocele, rectocele or vault descent | FSFI | In women, FSFI scores improved significantly in the domains desire, arousal, lubrication, overall satisfaction, and pain. In men, sexual drive, and overall satisfaction improved significantly |
| Bradner et al., 201130 | Prospective observational | 68 | To evaluate sexual function before and after surgical rectocele fascial repair in sexually active patients who suffer from symptomatic rectoceles | Sexually active female patients who were to undergo rectocele fascial repair for symptomatic rectoceles | FSFI | Significant improvement for desire (p <0.001), satisfaction (p <0.0001), and pain (p <0.0001) |
| Lakeman et al., 201331 | Prospective observational | 29 | To evaluate the effects of vaginal prolapse surgery on vaginal vasocongestion, vaginal wall sensibility, and sexual function | Patients scheduled for vaginal prolapse surgery | FSFI | Improvement of sexual function after prolapse surgery (20.5 vs. 23.3, p = 0.30) |
| Thibult et al., 201332 | Multicenter prospective | 148 | To evaluate the impact of laparoscopic sacrocolpopexy on symptoms, health-related quality of life (HRQL) and sexuality among women with symptomatic urogenital prolapse (UGP) | Patients with symptomatic POP who undergoing laparoscopic sacrocolpopexy | PISQ-12 | Postoperative sexual function had improved significantly (35.42 vs. 32.07, p <0.05) |
| Kim et al., 201433 | Prospective observational | 143 | To evaluate the effect of surgical repair of POP on female sexual function | Patients scheduled to undergo surgery for POP stage II–IV | FSFI, PISQ-12 | Improvement of PISQ score from 25.0±4.95 to 28.33±5.1 postoperatively (p <0.001) No differences of pre- and post-op FSFI (p = 0.08), however, only the satisfaction domain score significantly increased (p = 0.029) |
We feel that the posterior vaginal wall anatomically controls most of the vaginal caliber secondary to its relationship to the levator ani and genital hiatus, and repair of this wall is a major portion of most rejuvenation type procedures. Therefore, studies evaluating rectocele repairs, may have more of a direct correlation to vaginal caliber and sexual function. Bradner et al. reported that posterior repair had a positive impact on sexual function. They examined the FSFI score before and after surgical rectocele repair in sexually active patients who had symptomatic rectoceles. There was significant improvement of FSFI score in domains of sexual desire, satisfaction, and pain.30 Tunuguntia and Gousse found that while posterior repair with levatorplasty leads to sexual dysfunction and pain in many women, posterior colporrhaphy completed alone, with the avoidance of levator ani plication, improves sexual function.34 Komesu et al. investigated the effect of posterior repair on sexual function by using PISQ score. They included a cohort of patients who underwent pelvic floor reconstructive surgery with and without posterior repair and found that both groups significantly improved in sexual function.27 Paraiso et al. compared three different methods of posterior rectocele repair including one that utilized a graft and reported that all three approaches resulted in statistically significant improvements in the PISQ score.25
VAGINAL RELAXATION AND EFFECT ON SEXUAL FUNCTION AND SENSATION
It is clear from the data above that prolapse has a role in causing sexual dysfunction. The difficulty with this is that sexual function is multifactorial and can, because of this, be a very difficult area to study. It is also clear from these studies that vaginal repair improves sexual function and sexual quality of life, but is it because of the prolapse creating discomfort causing the woman to avoid intercourse, or because of self-image issues regarding the prolapse? Or is it because vaginal relaxation and prolapse may cause decreased sensation leading to sexual dysfunction, i.e. feeling less, having more difficulty in achieving orgasm or feeling self-conscious about the fact that she feels her vagina is loose, stretched or relaxed?
Ozel and White published one of the first reports evaluating libido, sexual excitement, vaginal sensation and ability to orgasm in a group of women with prolapse compared to women without prolapse. They found that women with prolapse and vaginal relaxation were significantly more likely to report an absence of libido, lack of sexual excitement during intercourse and a much lower frequency of achieving orgasm during intercourse (all statistically significant) compared to women with the same demographics without prolapse (i.e. multiparous, similar age, marital status, etc.).35 This is a landmark study as it is one of the first studies evaluating the sensation of the vagina and the changes following relaxation of the tissues that causes prolapse.
We have shown that vaginal prolapse can affect sexual function and its repair can improve sexual function and ability to orgasm. It therefore seems to make sense that if women present with an enlarged genital hiatus, or widened vaginal canal without symptomatic prolapse that this may also affect sensation and sexual function. Many women do present with these symptoms and, until recently, were told that there was nothing wrong and there were no options to improve her sexual sensation or function.
The theory that vaginal size is related to sexual sensation was first confirmed by Pardo et al.2 in a study of a group of women who presented with symptoms of a wide or relaxed vagina and were interested in vaginal repair for sexual function alone. The women had no symptoms of prolapse or incontinence. Inclusion criteria included a sensation of a wide or loose vagina alone in combination with a decrease or lack of ability to reach orgasm. Exclusion critera included symptomatic prolapse (cystocele, rectocele, or vault/uterine prolapse), dyspareunia, primary anorgasmia or psychologic impairment (all patients had psychological evaluation). Fifty-three patients were included in the study and 96% of the patients experienced decreased vaginal sensation, 73% described difficulty achieving orgasm and 27% could not reach orgasm. All but two patients had previous vaginal deliveries. Following surgical repair of the vaginal caliber and tightening of the vagina itself, 90% of women reported their sexual satisfaction was much or sufficiently improved and 94% of women were able to reach orgasm. This confirmed that vaginal size has a direct impact on sensation and ability to orgasm and when repaired sexual function improves.
DATA SUPPORTING VAGINAL REJUVENATION AND IMPROVED SEXUAL FUNCTION (Table 3)
Table 3 Vaginal rejuvenation studies on female sexual function
Author, year |
Study design |
N |
Population |
Intervention |
Outcomes |
Results |
Follow-up (month) |
Complications |
Pardo et al., 20062 |
Prospective observational |
53 |
Women with wide vagina and decrease or lack of ability to reach orgasm |
Colpoperineoplasty (dissected with a Yag laser) |
Patients’ sexual activity, fulfillment of expectations, and vaginal width using a site-questionnaire |
90% much or sufficiently improved sexual satisfaction 94% tighter vagina, able to achieve orgasm 74% expectation fulfilled completely |
15 |
4% regretted having procedures |
Pardo et al., 200736 |
Prospective observational |
100 |
Women with wide vagina and decrease or lack of ability to reach orgasm |
Colpoperineoplasty |
Patients’ sexual activity, fulfillment of expectations, and vaginal width using a site-questionnaire |
95% tighter vagina during the intercourse 85% achieve vaginal orgasm 79% expectation fulfilled completely |
4 |
4% regretted having the procedures 2 (0.02%) minor surgical complications |
Adamo and Corvi, 200937 |
Prospective observational |
40 |
Women with wide vagina |
Lateral colporrhaphy |
Sexual sensitivity |
95% improvement of vaginal sensation and wide vagina after 6 months 80% partners noticed improvement |
1.5 |
5% local infection 2.5% postoperative vaginal bleeding |
Matlock and Simopolous38 |
Retrospective |
96 |
Women undergoing laser vaginal rejuvenation |
Laser assisted anterior and posterior repair w/perineorrhaphy |
Comparing pre- and post-operative sexual function with PISQ-12 score |
53% reported increased intensity orgasm with intercourse Only 13% had decreased PISQ-12 scores |
6 |
|
Goodman et al., 201039 |
Multicenter cross-sectional |
258 |
Women undergoing female genital plastic surgery |
vaginoplasty/ perineoplasty procedures (n = 81) |
Preoperative sexual functioning per procedure, overall patient satisfaction per procedure, patient's perception of effect on her partner's sexual enjoyment, per procedure, complications |
85% mild/significant enhanced sexual function 86% satisfaction Subjective improvement in sexual functioning for both women and their sexual partners (p = 0.008) |
6–42 |
4% temporary stricture of vaginal apex 2% wound dehiscence 2% excessive postoperative pain 2% inadequate tightening 2% micro-tear at 1 year follow-up 2% introital tightening 2% bleeding after first sexual intercourse 2% felt sutures inside vagina 2% introital narrowing |
Moore et al., 201440 |
Prospective observational |
78 |
Women presenting for vaginal rejuvenation/ vaginoplasty procedure for a chief complaint of vaginal laxity and decreased vaginal sensation with intercourse |
Vaginal rejuvenation |
Comparing pre- and post-operative sexual function using PISQ-12 score |
Mean PISQ-12 improvement from 30.3 ± 6.6 to 38.2 ± 5.2 (p <0.001) |
>6 |
Pardo et al. published an additional follow-up study in a second group of women confirming their initial findings that vaginal size has a direct impact on sensation and ability to orgasm and when repaired sexual function improves.36
Matlock and Simopoulos also conducted a study to evaluate sexual function in women presenting with subjective symptoms of vaginal relaxation with or without stress urinary incontinence following laser vaginal rejuvenation using PISQ score. Ninety-six patients underwent the procedure and completed PISQ before and 6 months after surgery. All patients presented with chief complaint of relaxed vagina and decreased sensation during intercourse. Of those, 65% had stage II POP-Q. This finding suggests that early pelvic organ prolapse may manifest as vaginal relaxation. The overall sexual function improved after surgery. There were only 13% of women decreased PISQ score postoperatively. In addition, 53% reported increased intensity of orgasm during sexual intercourse.38
Goodman et al. led a recent multicenter US study on women undergoing female genital plastic surgery including vaginoplasty/perineoplasty for vaginal relaxation affecting sexual function. This study gathered data from diverse practices and surgical specialties with surgeons who utilize more than a single technique to achieve their desired outcome.39 Preoperatively 70% of women reported their sexual function was fair/poor. Postoperatively it was found that 86% of 81 women following vaginoplasty/perineoplasty for sexual function reported enhanced sexual function following repair with only 1% reporting a negative effect on sexual function, confirming repair of the vaginal caliber may lead to improved sexual function in women presenting with relaxation. Eighty-three percent of women reported they were “satisfied” with the outcome of vaginal rejuvenation. The predominate reason for surgery from the physicians’ and patients’ perspective was a feeling of looseness and lack of coital friction and sexual pleasure. A literature review by Goodman indicated that female genital plastic surgery procedures including vaginal rejuvenation appear to fulfill the majority of patient's desires for cosmetic and functional improvement, as well as enhancement of the sexual experience. The majority of patients reported improvement of overall satisfaction and subjective enhancement of sexual function and body image.39
Most recently, we evaluated sexual function outcomes in a group of women (n = 78) presenting for vaginal rejuvenation/vaginoplasty procedures for a chief complaint of vaginal laxity and decreased sensation with intercourse. Outcomes were analysed utilizing the validated Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12) before and at least 6 months after repair with vaginal rejuvenation/vaginoplasty procedure (VR). Compared preoperatively and postoperatively, the overall sexual function (Total PISQ-12) statistically improved (30.3 ± 6.6 vs. 38.2 ± 5.2, p <0.001). All individual scores statistically improved except in three categories which had no change (Q1-desire, Q5-pain and Q11- partner premature ejaculation). Overall sexual satisfaction improved as well as subcategories of increased sexual excitement during intercourse and overall increase in intensity of orgasms. Pain with intercourse subscores were found to be no different from preoperatively to postoperatively.40
VAGINAL REJUVENATION − SURGICAL TECHNIQUES
Importance of proper evaluatio and diagnosis
Proper preoperative evaluation is a vital process for a patient who presents with an interest in surgery to repair what she conceives is a loose or relaxed vagina and would like it tightened for sexual enhancement or to correct the feeling of having a “wide-open” vagina, i.e. vaginal rejuvenation surgery. This includes proper medical history, psychosocial evaluation for sexual dysfunction and/or sexual satisfaction prior to any of the anatomical changes she may have noted since childbirth. Marital or relationship issues or concerns and an evaluation of her expectations of surgery and the reasoning why she is interested in the procedure should be discussed as well. Sexual dysfunction is very complex and multi-factorial and, of course, a surgical procedure to repair vaginal support and reduce the vaginal caliber, will not reverse or change psychological or psychosocial sexual dysfunction arising from previous abuse, primary anorgasmia, relationship issues, depression or other more complex psychological dysfunction.
In addition to a medical and psychosocial history, an adequate urogynecology history and physical exam must be completed. Sexual dysfunction related to a sense of a relaxed or loose vagina may be the first sign of the initial stages of pelvic floor dysfunction and prolapse, therefore an adequate history must be taken. We have actually found that as many as 50–75% of patients who present for vaginal rejuvenation, when asked, have symptoms including urinary incontinence, voiding dysfunction such as overactive bladder or difficult emptying, feelings of pressure or the sense that their organs are falling, defecatory dysfunction, or dyspareunia related to the uterus being hit during intercourse because of prolapse. It is vitally important to have an adequate understanding of the symptoms that prolapse can cause and we use validated questionnaires such as the UDI-6, IIQ-7, and the PISQ-IR[40] to evaluate patients for these symptoms as well as a general urogynecologic history form. If significant symptoms of urogynecologic pathology are present, they must be evaluated preoperatively so that they can be addressed properly during surgery. Any prolapse that is present, MUST be repaired properly at time of surgery including uterine/vault prolapse, enterocele, cystocele, or rectocele as vaginal rejuvenation procedures do NOT adequately treat these defects. The foundation of the pelvic floor support must be intact prior to any technique that will tighten the caliber of the vagina or introitus.
Surgical procedures
The surgical procedure required is determined by the patient’s physical exam. Again, many women who present interested in vaginal rejuvenation type surgery, or surgery to correct a feeling of a loose or wide vagina, are found to have prolapse in the form of cystocele, rectocele or uterine/vault prolapse. In most instances it is POP-Q stage II or less, however, it is present and should be repaired. This is what determines what surgery will need to be done as the prolapse must be corrected first, prior to any rejuvenation procedures being completed and is really the first step in an overall repair or “rejuvenation” of the vagina and pelvic floor. If significant uterine/vault prolapse and/or anterior compartment (cystocele) defects are encountered, these typically should be repaired abdominally/laparoscopically/robotically prior to addressing the posterior compartment and the caliber of the vagina.
Rejuvenation of the vaginal canal and introitus
Repair of the posterior vaginal wall and the introitus are the key aspects to any vaginal rejuvenation procedure. Vaginal rejuvenation surgeries are alterations and modifications of vaginal repairs for prolapse that focus on the final diameter and caliber of the vagina and attempt to restore it back to its pre-childbirth state. They do, however, go far beyond the simple traditional posterior repairs and perineoplasty of old. The focus of these older procedures is simply to restore and reduce the bulge, whereas the focus of vaginal rejuvenation is to restore the caliber of the vagina and genital hiatus back to pre-childbirth state from the introitus all the way up to the apex. They are much more extensive and meticulous procedures. No drop-offs or dips should be felt and there should be no tension placed on the levators that causes lateral banding of the vagina. Additionally, the cosmetic appearance of the introitus and perineal body is also taken into account and requires intricate dissection and repair to not only restore function of the introitus, but also obtain an appearance that the woman desires (Fig. 2a–d). That look typically is one of the vaginal opening being closed, not gaping or wide open with a normal length perineal body that does not bulge out following the repair. This look is sometimes difficult to obtain, without making the introitus too tight, which will cause pain with intercourse.
Posterior wall, introitus and rejuvenation
The posterior vaginal wall is the focus of any vaginal rejuvenation procedure. In a woman with a mild cystocele or mild relaxation of the anterior vaginal wall, a small anterior colporhaphy can be completed to take care of this prior to repair of the posterior wall. However, one needs to be very careful with this as if the repair of the anterior wall is too aggressive, it will lead to lateral banding and constriction of the vagina, before the posterior wall is even started.
An incision is made at the introitus, typically in trapezoid pattern, that will also be used in the perineoplasty portion of the procedure (Figure 3a, b). A small incision is then made in a vertical fashion on the posterior wall and the vaginal epithelium is dissected off the underlying rectovaginal fascia all the way laterally out to the levators (Figure 3c, 3d). The dissection must be taken all the way up to the apex of the vagina, as the repair needs to incorporate the entire posterior wall to restore the caliber of the full length of the vagina (Figure 3e). The dissection of the vaginal epithelium may be completed with as laser, as championed by Dr David Matlock, or completed utilizing more standard techniques with sharp scissors or electrocautery. Care must to be taken with any electrical energy source near the rectum. If a rectocele is present, the fascia is repaired in a site-specific fashion with delayed absorbable suture for the first layer of the repair. This may be a lateral repair of the defects, a midline placation or a combination (Figure 3f). The caliber of the vagina is then addressed by plication of the rectovaginal fascia in the midline with delayed absorbable sutures. Levator plication is avoided, however, the diameter of the vagina is constantly measured and several layers of plication may be needed to reduce the genital hiatus and reduce the caliber of the vagina to an appropriate level (Figure 3g–j). A small amount of vaginal epithelium is then excised and the incision closed in a running fashion.
 Figure 2a Gaping introitus – pre-repair
Figure 2a Gaping introitus – pre-repair
 Figure 2b Gaping introitus – final repair
Figure 2b Gaping introitus – final repair
 Figure 2c Gaping introitus – pre-repair
Figure 2c Gaping introitus – pre-repair
 Figure 2d Postvaginoplasty rejuvenation
Figure 2d Postvaginoplasty rejuvenation
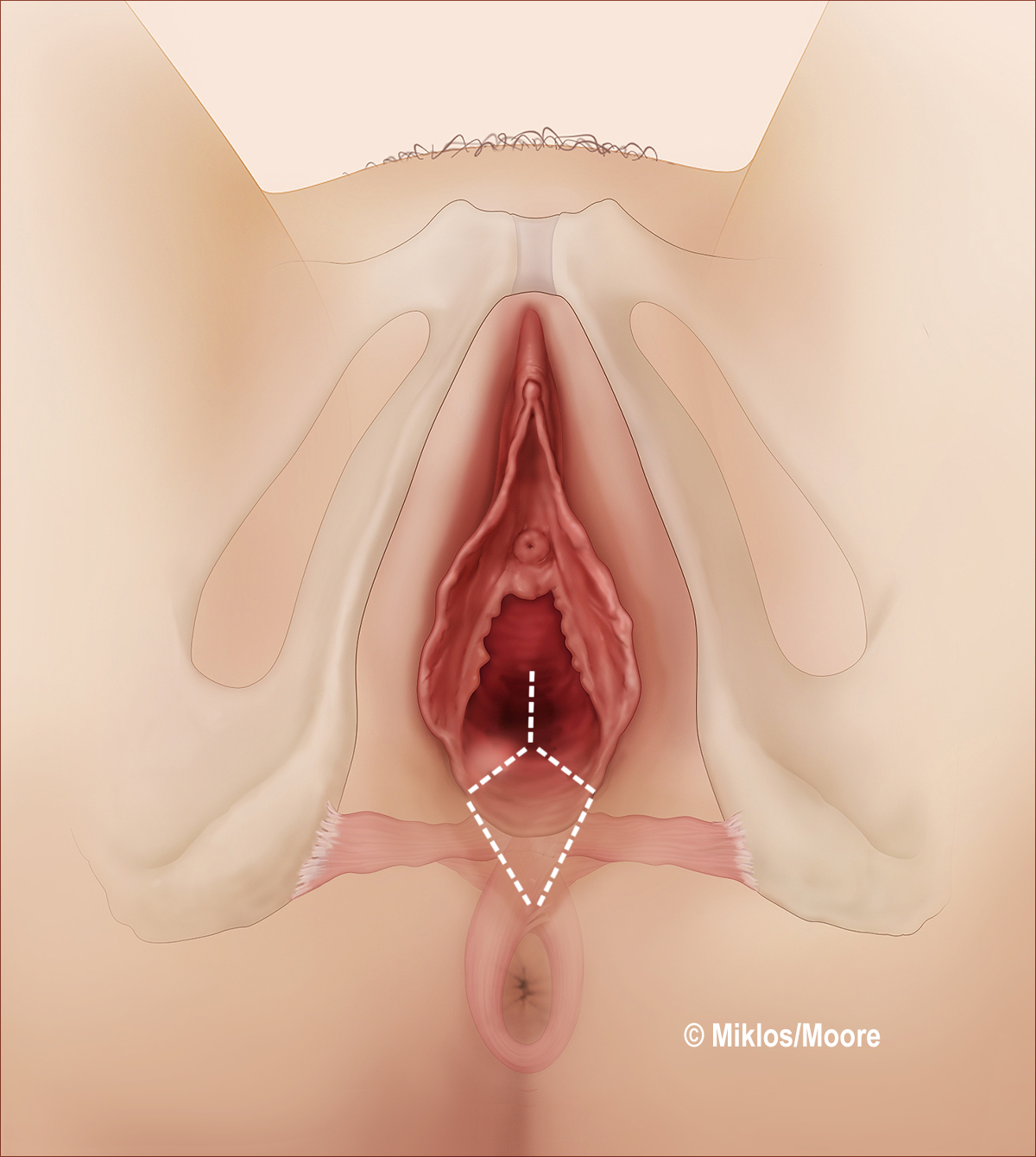 Figure 3a Initial incision
Figure 3a Initial incision
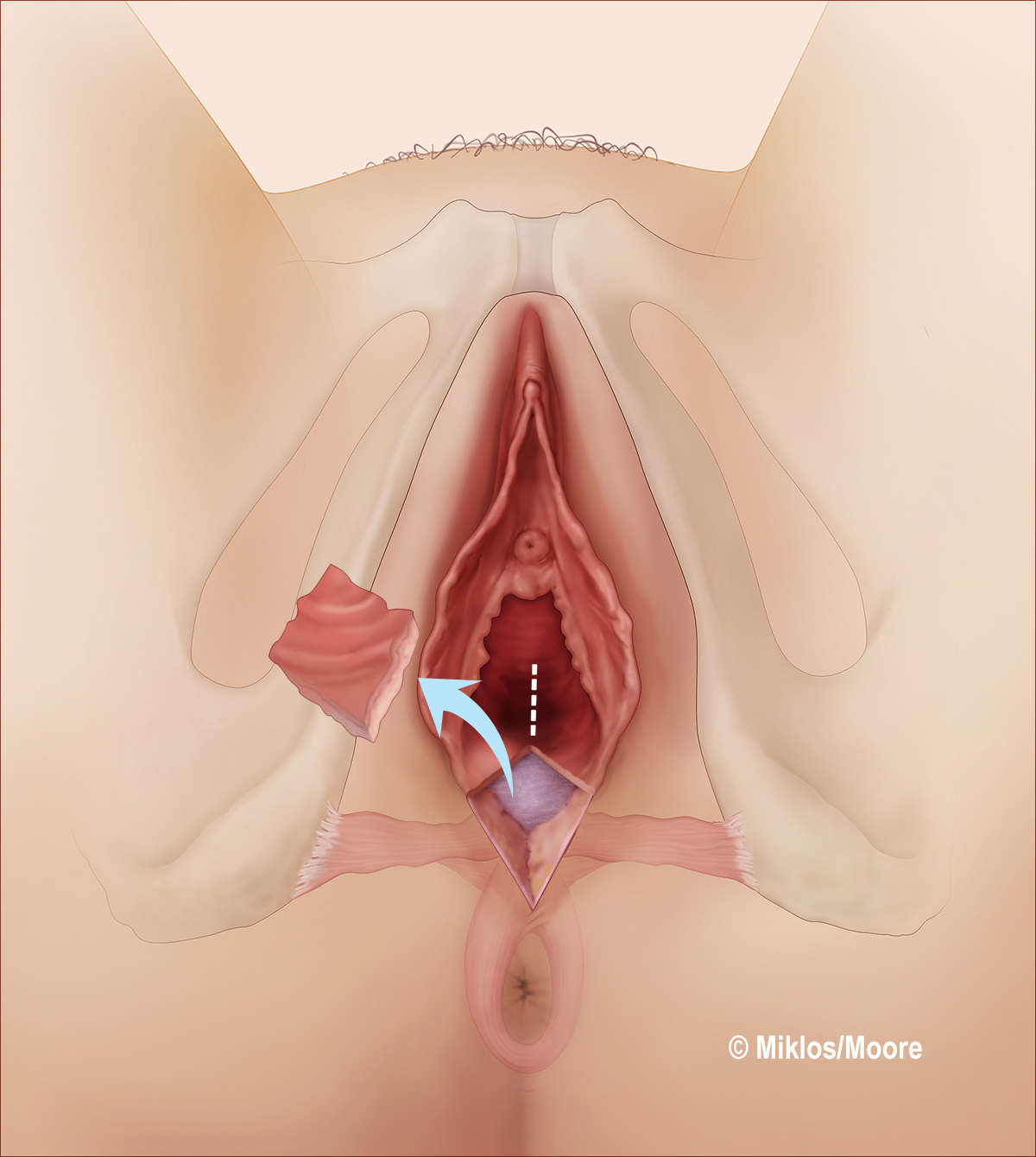 Figure 3b Trrapezoidal area of epithelium removed to begin procedure and ultimately to complete perineoplasty at end of precedure
Figure 3b Trrapezoidal area of epithelium removed to begin procedure and ultimately to complete perineoplasty at end of precedure
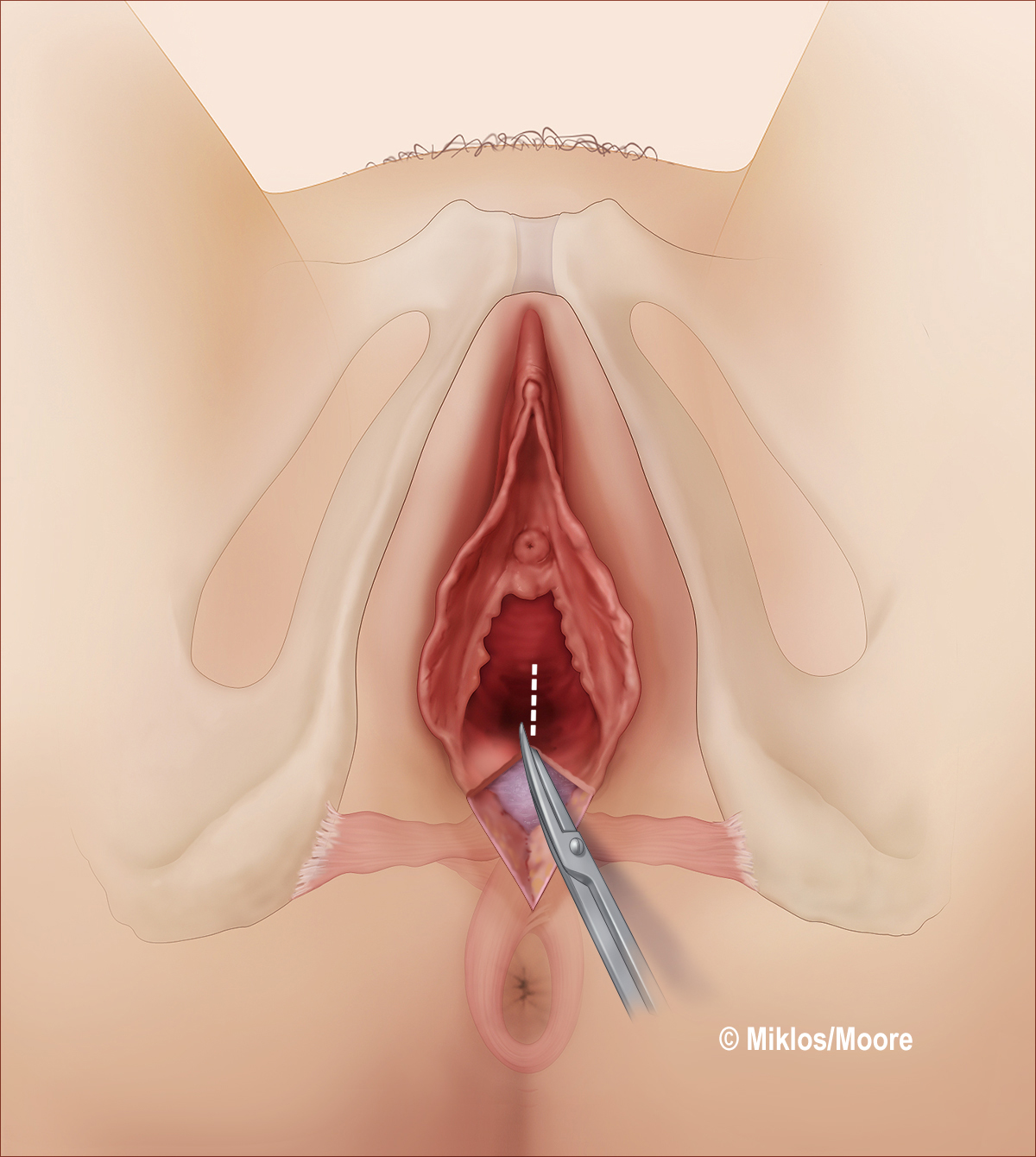 Figure 3c Incision extended vertically for 3–4 cm
Figure 3c Incision extended vertically for 3–4 cm
 Figure 3d Vaginal epithelium dissected off underlying rectovaginal fascia
Figure 3d Vaginal epithelium dissected off underlying rectovaginal fascia
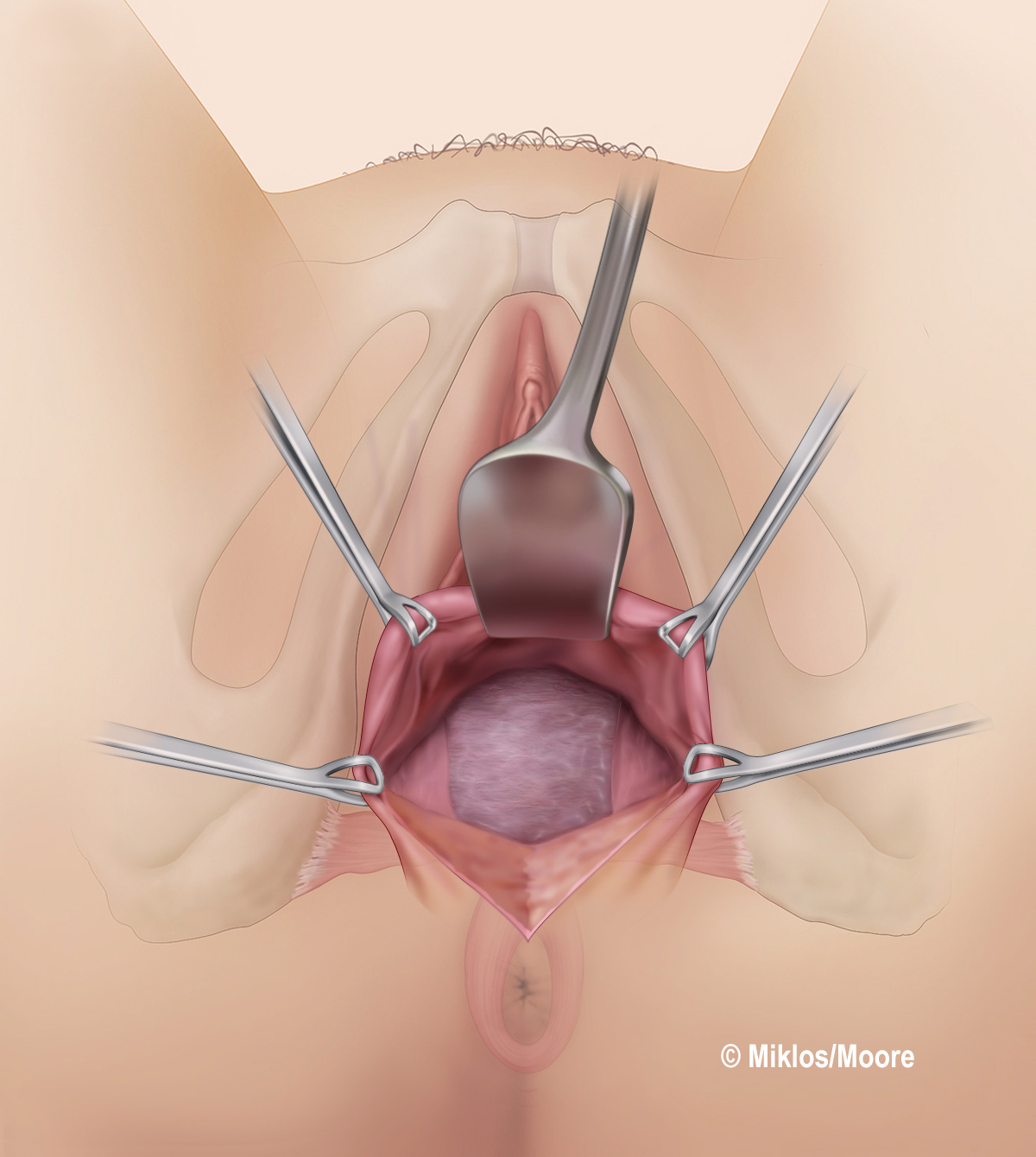 Figure 3e Breisky retractor placed under vaginal epithelium and the dissection tunelled all the way up to the apex of the vagina and laterally all the way out to the levators up to the level of the ischial spines
Figure 3e Breisky retractor placed under vaginal epithelium and the dissection tunelled all the way up to the apex of the vagina and laterally all the way out to the levators up to the level of the ischial spines
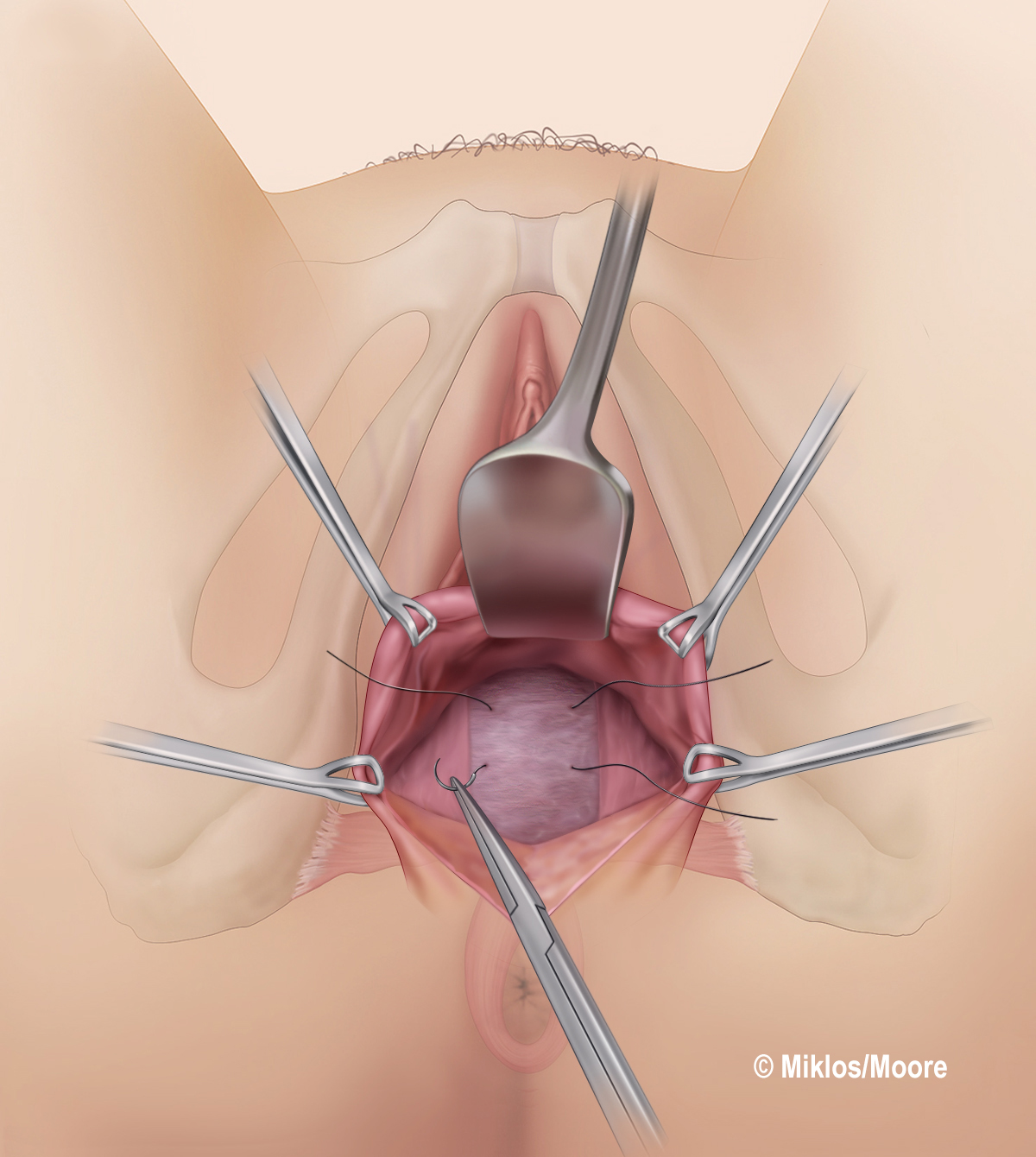 Figure 3f Initial plication sutures placed to reduce any rectocele that is present, i.e. reduction of the attenuated rectovaginal fascia or if site specific fascial defects are present, then this is where they would be repaired. Additionally, we ensure that the fascia is also attached laterally to the levators and there are no lateral defects
Figure 3f Initial plication sutures placed to reduce any rectocele that is present, i.e. reduction of the attenuated rectovaginal fascia or if site specific fascial defects are present, then this is where they would be repaired. Additionally, we ensure that the fascia is also attached laterally to the levators and there are no lateral defects
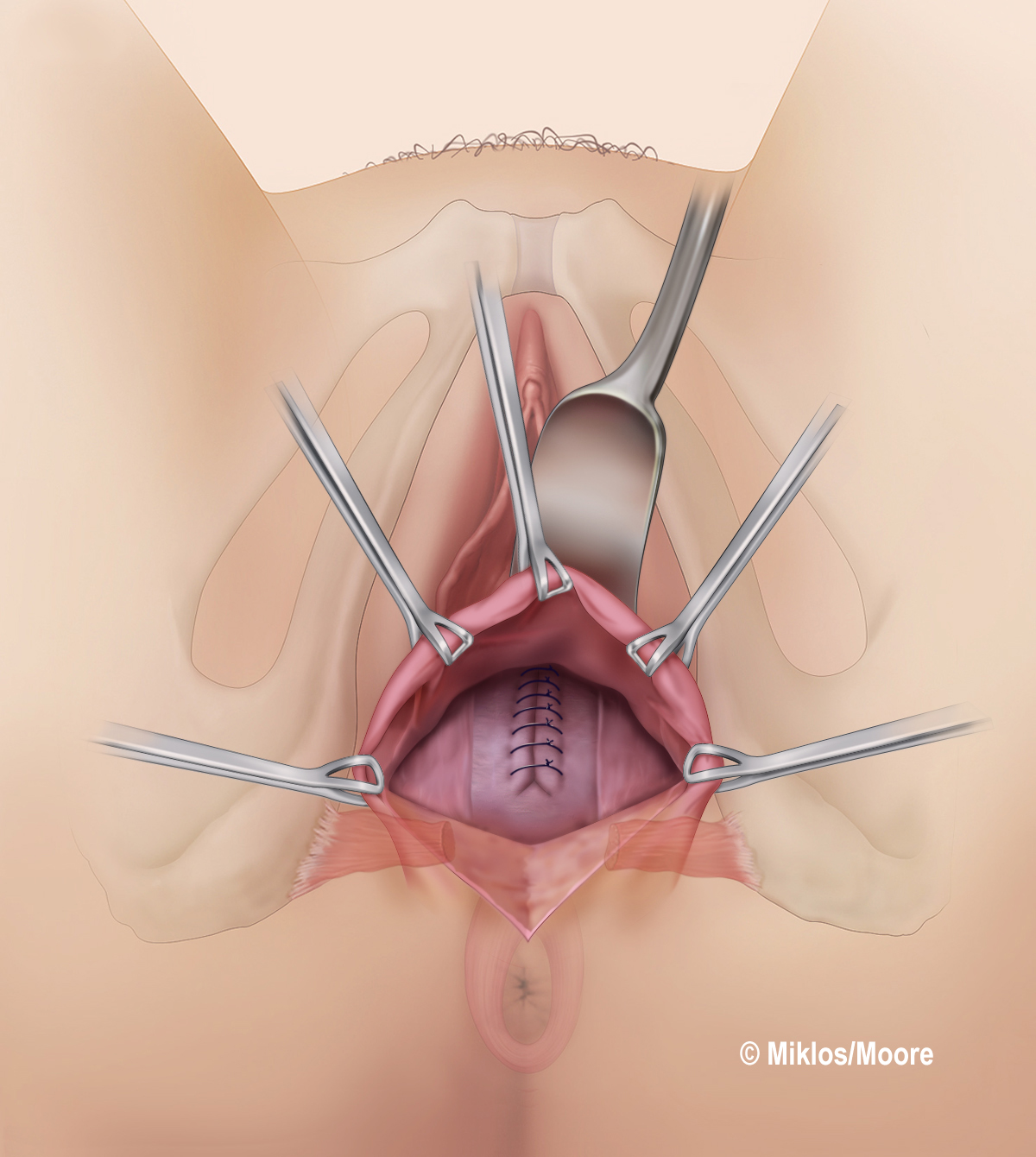 Figure 3g The rectocele is reduced and repaired
Figure 3g The rectocele is reduced and repaired
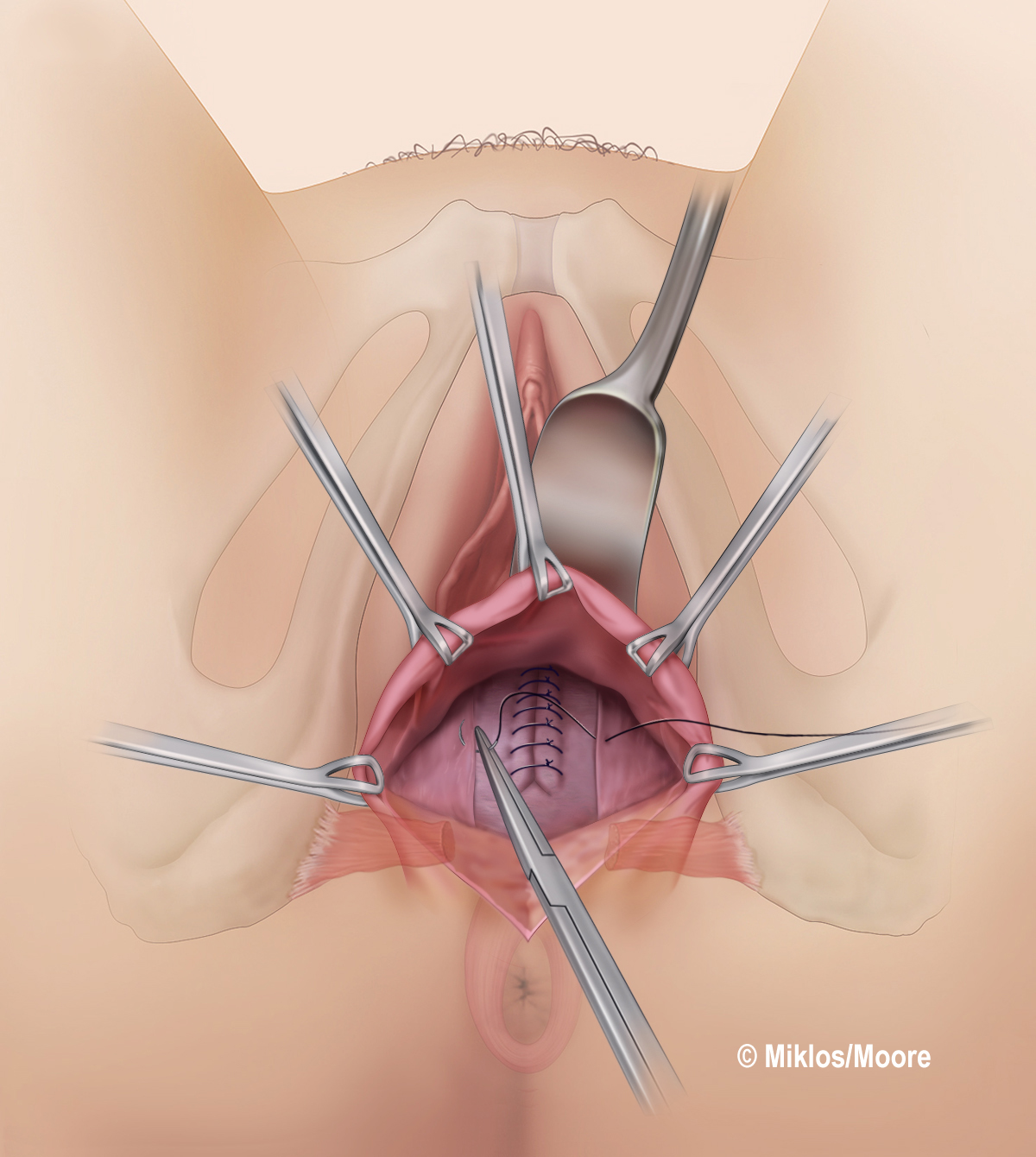 Figure 3h Second layer of plication sutures now placed to address vaginal caliber
Figure 3h Second layer of plication sutures now placed to address vaginal caliber
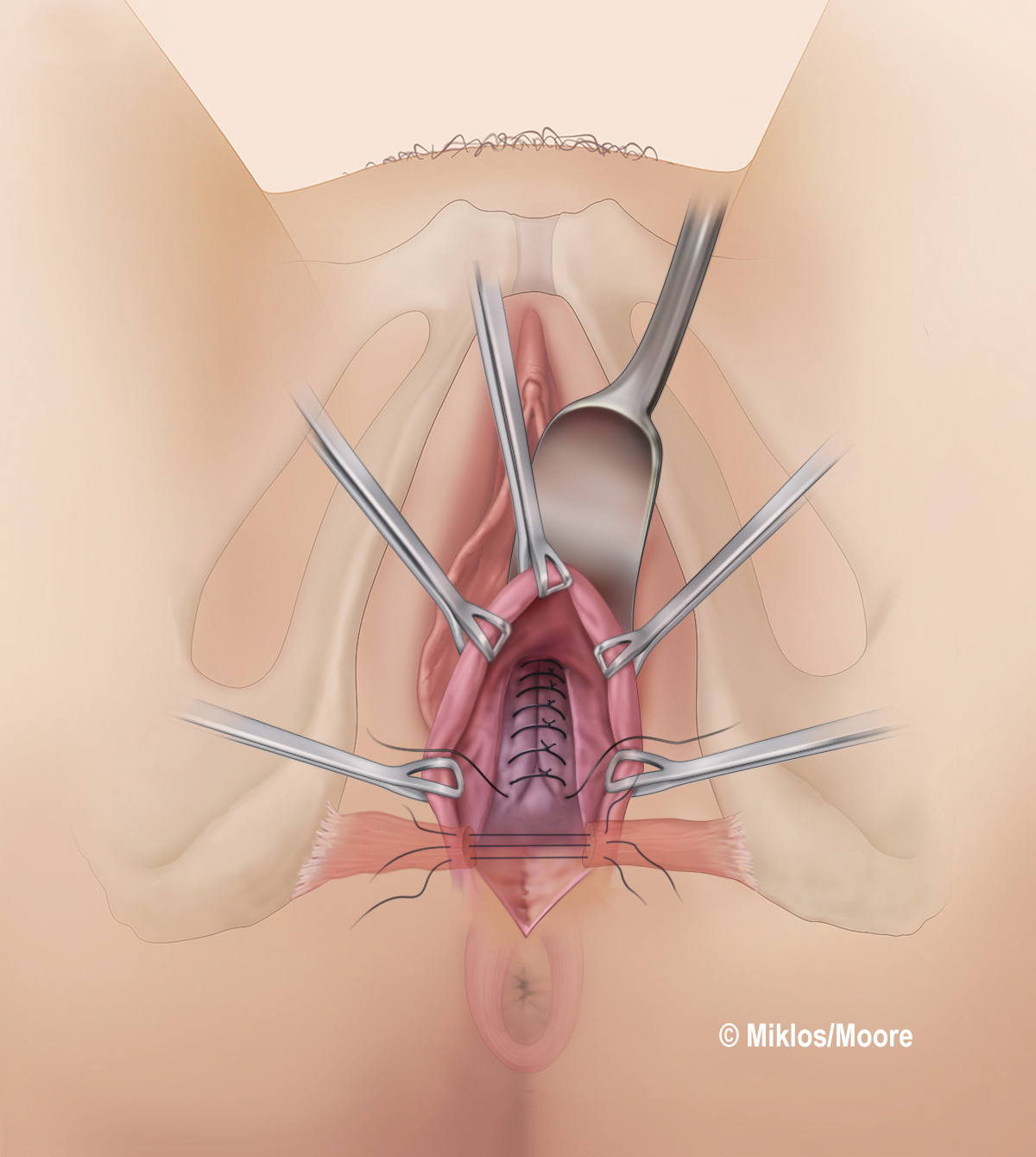 Figure 3i Vaginal caliber reduced and checked closely with digital exam. Caliber should be from the hymenal ring up to the apex
Figure 3i Vaginal caliber reduced and checked closely with digital exam. Caliber should be from the hymenal ring up to the apex
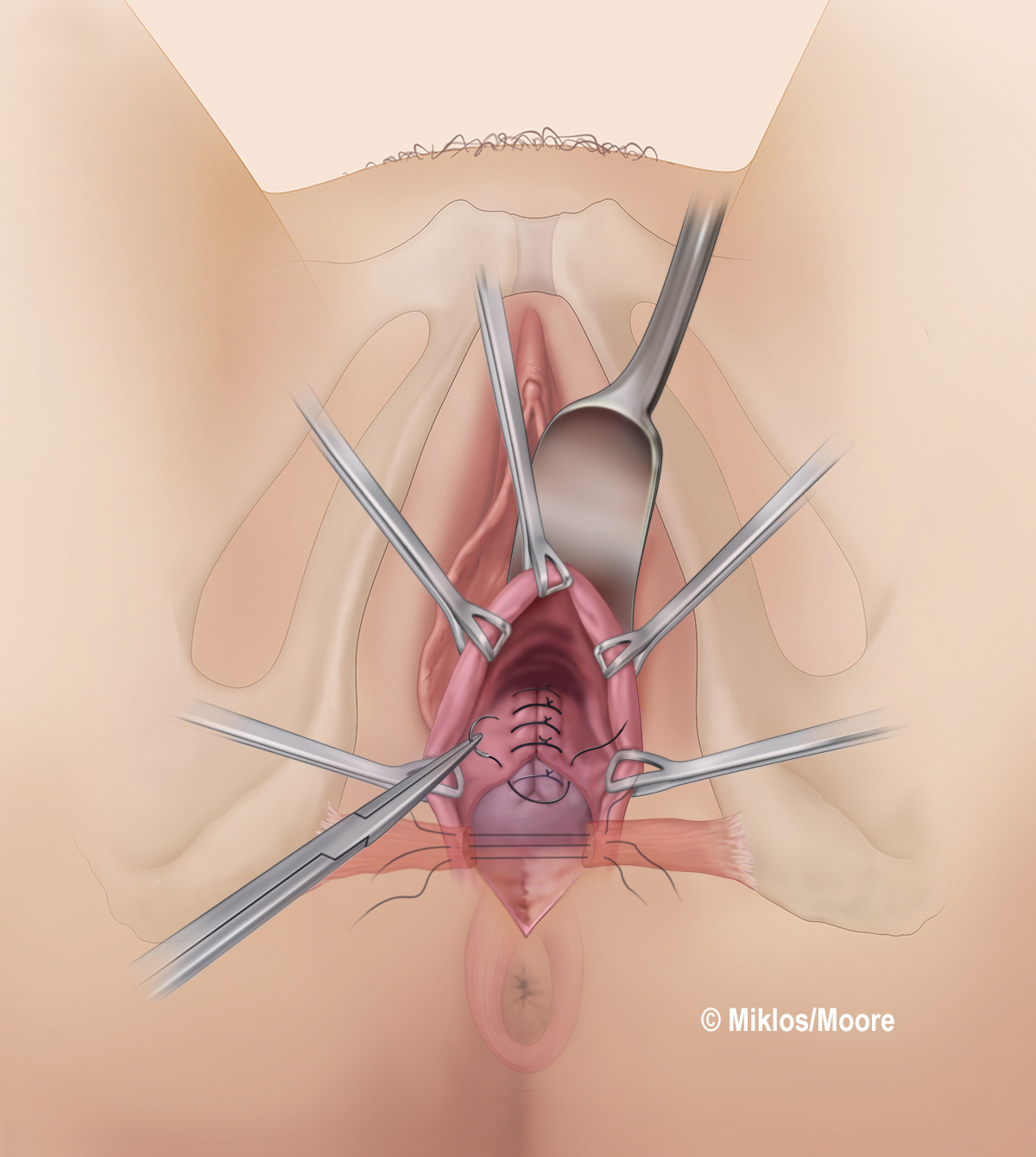 Figure 3j Distal sutures are placed and transverse perineal muscles are now being brought back together to build up the perineal body
Figure 3j Distal sutures are placed and transverse perineal muscles are now being brought back together to build up the perineal body
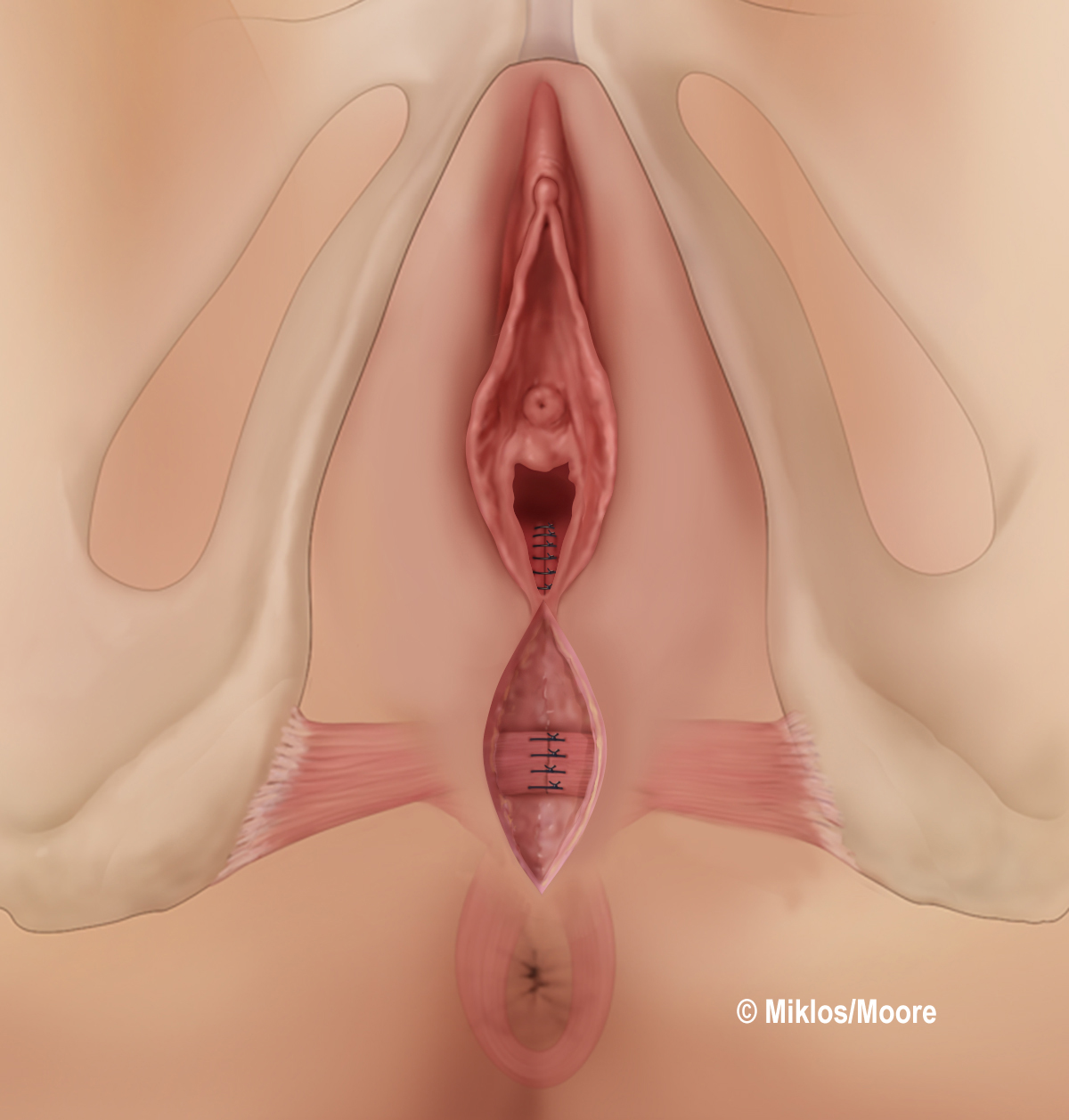 Figure 3k Perineal muscles re-approximated
Figure 3k Perineal muscles re-approximated
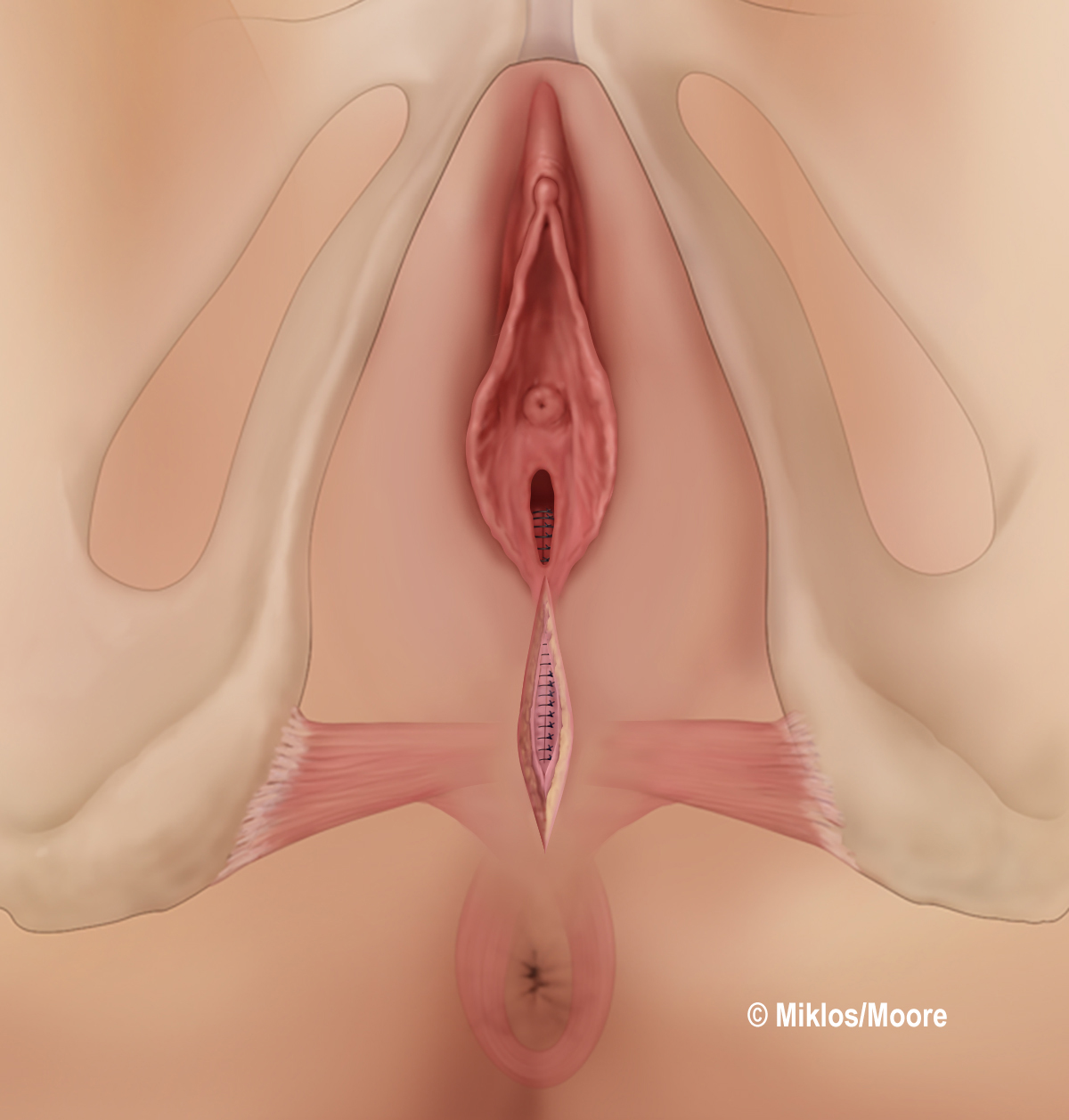 Figure 3l Perineum now closed typically in 3–4 more layers with delayed absorbable sutures
Figure 3l Perineum now closed typically in 3–4 more layers with delayed absorbable sutures
 Figure 3m Final appearance
Figure 3m Final appearance
A perineoplasty is then completed, involving a very meticulous and detailed dissection out laterally to obtain the lacerated edges of the deep and superficial transverse perineal muscles and bringing them back together in the midline to achieve uniformity at the same level of the posterior wall repair. The inferior edges of the labia majora that will make up the posterior forchette of the vaginal opening must be marked at the beginning of the procedure so that these edges match up during the closure to form the vaginal opening. An appropriate amount of skin must also be excised from the perineum and introitus to result in a cosmetically pleasing appearance of the opening of the vagina for the patient. A multilayer closure (typically this may involve 4 or 5 layers) is completed at the perineum and introitus (Figure 3k–m).
When a repair is primarily for vaginal relaxation for sexual function it becomes a much more meticulous dissection and repair as the surgeon has to constantly be judging and measuring vaginal caliber to try to restore the entire vaginal length to its pre-childbirth state. If this is not done, then the results will be poor and the patient's sexual function may not change or she will be worse secondary to pain, vaginal shortening, scar tissue formation and/or constrictions.
Postoperative care
Routine postoperative care is given to patients undergoing vaginal surgery. Many of the procedures are undertaken on an outpatient basis and the surgery is completed under spinal or general anesthesia. A pudendal block may also be completed prior to or during the procedure to help decrease postoperative pain. Vaginal packing is left in for a short period of time and removed prior to the patient being discharged. Routine instructions for vaginal surgery are given to the patient and she is seen in follow-up at 4 weeks postoperatively. The vaginal introitus and caliber are assessed and if felt necessary the patient will begin perineal massage in warm water bath for 1–2 weeks prior to resuming sexual relations.
Risks/complications
The potential complications of vaginal rejuvenation are infection, bleeding, wound dehiscence, dyspareunia, inadequate tightening, introital narrowing, and rectoperineal fistula. According to a study of 248 women by Goodman et al., 24% of women had temporary stricture of vaginal apex, 1% wound dehiscence, 2% excessive postoperative pain, 2% inadequate tightening, 1% microtearing of the perineum with intercourse at 1 year follow-up, 2% introital over-tightening, and 2% bleeding after first sexual intercourse.[41]
Conclusion
Vaginal rejuvenation surgery is one of the latest trends in elective vaginal surgery for women. It is a repair of the vaginal caliber in women who suffer from decreased vaginal sensation or of feelings of a loose or wide vagina that affects their sexual life. In many instances, women who present with these symptoms are found to have other pelvic pathology such as prolapse that must also be addressed during any repair contemplated. Sexual dysfunction or decreased sexual sensation may be the first symptoms that women suffer from in the progression of prolapse and therefore a proper exam is vital prior to any repair. We have ample evidence that prolapse and vaginal relaxation can create sexual dysfunction and that repair may reverse these changes in many women. It is important to note that when dealing with sexual dysfunction due to vaginal laxity alone, the surgical repair must be very meticulous and exact in order to enhance sensation and function and not impair it. This sums up the statement “The Art of Surgery”!
COSMETIC VAGINAL SURGERY – AESTHETIC SURGERY OF THE EXTERNAL VAGINA AND VULVA
Introduction
There have been many studies and much research on the relationship between a woman’s body image and her sexual function. However, little research exists on the relationship between a woman's genital image and her sexual function. Realizing one's genital image is part of one's body image; it is easy to understand how many women might feel sexually inhibited if they are not comfortable with the appearance of their vagina, vulva or external genitalia. A survey of 3627 women found that women with positive body images reported more sexual activity, initiation of sexual activity, orgasm, sex with lights on, and greater comfort undressing in front of their partners, trying new sexual behaviors and pleasing their partner.41
Cosmetic vaginal surgery is currently steamrolling its way into mainstream culture. However, as with every new trend there are always those who oppose change. There have been many negative comments and editorials written suggesting that both the doctors and the patients should not be pursuing cosmetic vaginal surgery.42, 43, 44 Many of those who imposingly opine are often ignorant of the patient and their disposition as well as their medical conditions and their associated symptoms.45 Patients can suffer from a variety of physical and emotional symptoms. Physical symptoms are usually associated with wearing certain types of clothing, engaging in activities such as walking, jogging, exercise, and bicycling, and finally intercourse. Yet other patients are afflicted with emotional problems such as embarrassment, anxiety and a loss of self-esteem.
Cosmetic vaginal surgery does not always begin and end with labia minora reduction surgery, i.e. labiaplasty. There are many different techniques which can be applied to enhance a woman's genital cosmetic image. To understand the techniques a basic understanding of the external genitalia is essential before undertaking surgical procedures.
Anatomy
The vulva is made up of the external genitalia including the mons pubis, clitoris, prepuce or clitoral hood, labia minora, labia majora, urethral meatus, hymen and vestibule (Figure 4). The mons pubis is the adipose laden area that lies superior to the pubic symphysis. This area is naturally covered with pubic hair and is a natural cushion during the impact of intercourse. The adipose area of the mons is contiguous with that of the hair bearing labia majora. The labia majora are found bilaterally and converge both anteriorly above the clitoral prepuce and posteriorly at the perineum. The prepuce is actually the clitoral hood and acts like a protective covering over the clitoral gland. Usually the very distal tip of the clitoris remains uncovered and exposed.
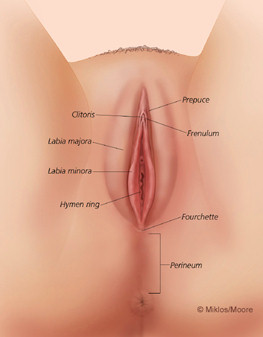 Figure 4 Normal external anatomy
Figure 4 Normal external anatomy
The labia minora are bilateral mucosal-cutaneous refolds located between the labia majora and vulvar vestibule. While there is a wide range of normal anatomic variants, in general, the labia minora are semicircular with a 3-cm long base and a free edge extending from the clitoris to the posterior commissure. The medial mucosal surface is derived from the primitive urogenital sinus and is shiny and pink. The free edge and the lateral cutaneous surface are derived from the urethral folds and are more deeply pigmented.46 However, the deeper pigment tends to be a darker pink initially and then begins to darken with hormonal changes often but not always associated with pregnancy. Obviously just like any other part of the human body there are multiple normal variants of this anatomy. Just like a nose all the structures can be anatomically similar but cosmetically dissimilar. The most common of all described cosmetic vaginal surgery is labia minora reduction or labiaplasty.46, 47, 48, 49
Labia minora reduction (labiaplasty)
Labia minora protruding past the distal edge of the labia majora can be of concern to women. As mentioned above this condition can constitute a functional or cosmetic problem. Such an enlargement can be bilateral or unilateral in nature (Figures 5 and 6). Labia enlargement can be congential as described by Caparo50 and Radman51 or can also be the result of androgenics hormones, manual stretching, and chronic irritation.50, 51, 52, 53
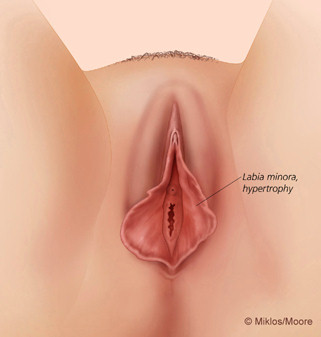 Figure 5 Labia minora hypertrophy
Figure 5 Labia minora hypertrophy
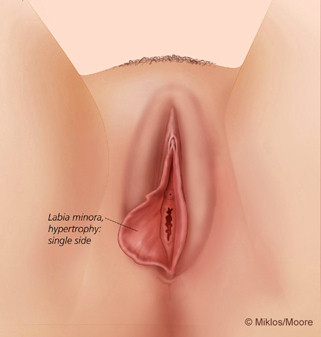 Figure 6 Unilateral labia minora hypertrophy
Figure 6 Unilateral labia minora hypertrophy
Rouzier et al. reported on 163 women who received labia reduction surgery. The primary reason for patients requesting this surgery was aesthetic dissatisfaction in 87% of cases, discomfort in clothing in 64%, discomfort when taking part in sports in 26% and entry dyspareunia by invagination of the protuberant tissue in 43%.47 A study of 131 patients undergoing labia minora reduction surgery revealed the patients indications for having the surgery: 37% strictly cosmetic reasons, 32% strictly for physical symptoms and 31% a combination of cosmetic reasons and physical symptoms.50
Although there are still few papers on labial reduction surgery, there are a number of different techniques described in the literature. The two most commonly utilized techniques are known as: excision or contouring technique and the wedge resection technique. The authors employ both techniques depending upon the patients' requests and desires. If the patients prefer to keep the darkened pigmented labial border, we tend to utilize the wedge resection technique. However, it has been the authors’ experience that most of their patients prefer to have a pinker or lighter look to the edges of their labia. In this situation, in an attempt to fulfill the desires of the patient, we utilize the contouring technique.49
The contouring or excisional technique is a more time consuming operation and directly excises the edge of the labia minora (Figure 7a–d). Though all surgeries are surgeon dependent, this operation is less reproducible than the wedge technique because it requires more artistic aptitude. There are multiple skin folds that need to be excised, reduced and brought together to achieve a natural anatomic appearance of the entire external vulvar region. The edges should be contoured or removed in an artistic fashion instead of the commonly described term amputation. The term amputation seems to suggest the protruding labia should just be “cut off” in a straight vertical fashion, which does not result in aesthetically pleasing results and can cause pain and discomfort. The procedure should not be completed with this type of “amputation” technique. Time and care should be put into the incision and the excision of the protruding aspect of the labia. It should be removed in a curvilinear fashion at the level or below the level of the labia majora. The amount of tissue removed should be in direct correlation to the patient’s desire. Aggressive excision can result in complete amputation resulting in an undesirable result (Figure 8). The results of a contouring surgery should be aesthetically pleasing yet address any associated physical dysfunction. Most women state that they do not want their labia minora to protrude beyond the majora and are interested in a smooth, sleak appearance of the external vulva. This was confirmed in a recent study of 550 women who presented for labial reduction surgery at our specialty center in Atlanta. Of the 550 women who were presenting for labial reduction, 97.8% of them desired for their labia minora to be reduced to the level of or below the level of the labia majora.54
 Figure 7a Preoperative labioplasty
Figure 7a Preoperative labioplasty
 Figure 7b Postlabioplasty (same patient as Fig. 7a)
Figure 7b Postlabioplasty (same patient as Fig. 7a)
 Figure 7c Preoperative labioplasty
Figure 7c Preoperative labioplasty
 Figure 7d Postlabioplasty (same patient as Fig. 7c)
Figure 7d Postlabioplasty (same patient as Fig. 7c)
 Figure 8 Botched labioplasty
Figure 8 Botched labioplasty
The authors utilize the wedge resection technique in patients who wish to maintain the darkened skin edges of the labia. The technique was first described in the literature by Alters in 1998, where he utilized the technique on four patients.44 In this case series it is suggested that excision or contouring the protuberant edges removes the natural contour and color. Interestingly many patients do not feel that the darkened skin edges are a normal color but instead the result of aging and hormonal changes. No different than the skin discoloration that happens on hands or the areola of the breast. This was also confirmed in a recent study of 550 women presenting for labiaplasty at our center in Atlanta. Of the 238 women 72% of women felt their skin edges were dark or pigmented and 96% preferred that their skin edges be pink following the procedure.54 The authors feel the wedge technique is less time consuming and requires less artistic impression, however, it does not address the excess prepuce that is a problem with many women presenting with labial hypertrophy (Figure 9).
 Figure 9 Labioplasty – wedge technique
Figure 9 Labioplasty – wedge technique
Redundant lateral prepuce
In our practice approximately 80% of patients also complain of redundant prepuce when they consult for labia minora reduction (Figure 10). This is strictly a cosmetic problem and not a functional problem. We have not had patients complain of symptoms from redundant lateral prepuce except occasionally feeling that it has a negative effect on clitoral sensation. On examination patients will often point out the lateral excessive tissue which is adjacent to the clitoral hood bilaterally or that the clitoral hood is elongated and hangs down a great deal below the majora. If the patient wants to have her labia minora reduced via a contouring technique, often the redundant prepuce will inhibit the surgeon from getting good cosmetic results unless the prepuce redundancy is reduced or removed. The reason why the redundant prepuce becomes an issue is because of its anatomic insertion. The origin of the prepuce starts laterally to the prepuce and then inserts usually at an acute angle into the lateral aspect of the labia minora (Figure 11). An excision of the labia minora without addressing the redundant prepuce can result in poor cosmesis (Figure 12).
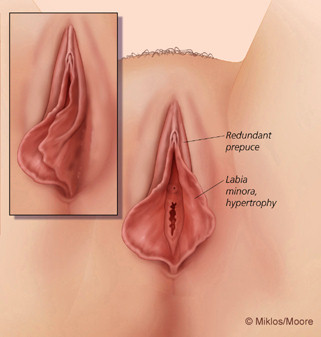 Figure 10 Redundant prepuce
Figure 10 Redundant prepuce
 Figure 11 Botched labioplasty
Figure 11 Botched labioplasty
 Figure 12a Elongated clitoral hood
Figure 12a Elongated clitoral hood
 Figure 12b Labia hypertrophy with elongated hood
Figure 12b Labia hypertrophy with elongated hood
Excess superior prepuce reduction (clitoral hood lift)
As described above we have coined the term “redundant prepuce” in patients who have an extra layer of prepuce lateral or adjacent to the clitoral hood. Patients with excess prepuce have excessive prepuce at its normal antatomic position. In other words the prepuce is in the right spot but there is just an excessive amount of it or have an elongation of the clitoral hood itself (Figure 12a and b). Excess superior prepuce or clitoral hood elongation may be a purely cosmetic issue or patients may complain of difficulty accessing the clitoris thus making clitoral orgasms difficult to achieve. Surgical resection, if done correctly, can bring favorable results for patients with excess prepuce. Performed incorrectly it can result in hypersensitivity and chronic pain or even severe scar limiting any access to the clitoris.
Labia majora reduction
Patients complain of “drooping”, “sagging” or “hanging” majora or the majora is just too large and protruding in appearance. Many women state that this skin is very loose and makes the appearance of the external vaginal area appear “old”. They are looking for a youthful “plumpness” of the labia majora, without much laxity or wrinkling. The sagging labia majora may be the result of weight gain and weight losses which seem to be often associated with pregnancy or in patients who have had bariatric surgery. The saggy skin of the labia majora may be the result of stretching during the weight gain and then with sudden weight loss the skin hangs because it has lost some of its elastisicity. It can also occur due to aging and/or childbearing (Figure 13).
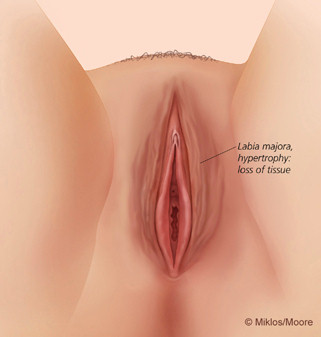 Figure 13 Sagging labia majora
Figure 13 Sagging labia majora
Still others complain of enlarged labia majora and on examination do not have sagging skin. These patients tend to have taut skin because it is filled with excessive adipose deposits. This in essence results in lipodystrophy of the labia majora and labia majora hypertrophy. In many cases, women who have had abdominoplasties and/or liposuction of the abdominal region, end up with an asymmetrically enlarged mons pubis. This area also in many cases has excess deposits of fatty tissue and if not reduced at time of abdominoplasty, ends up protruding out or hanging down. These patients often complain they cannot wear tight clothing or they are embarrassed in a swimming garment because they feel as if their vulva and/or mons is protruding. These patients can benefit from liposuction of the mons pubis and labia majora areas (Figure 14a and b).
 Figure 14a Labia majora hypertrophy
Figure 14a Labia majora hypertrophy
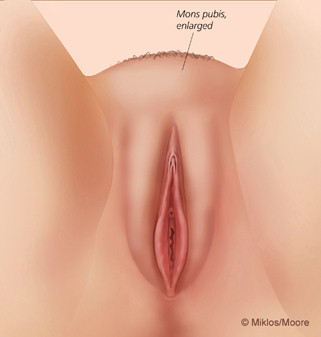 Figure 14b Excess labia majora and mons fat
Figure 14b Excess labia majora and mons fat
Labia majora convergence
Cosmetic surgical patients are very consumer savvy and often are quite specific about their cosmetic desires. Many of our patients will have pictures and/or medical illustrations, which represent their desired cosmetic results. Another common request we have coined “labia majora convergence” surgery. Patients can have labia majora divergence both anteriorly at the mons pubis or directly anterior to the clitoral hood and posteriorly at the perineum (Figure 15a and b). Surgical correction of the divergence results in convergence of both or either the anterior division of posterior aspect of the labia majora.
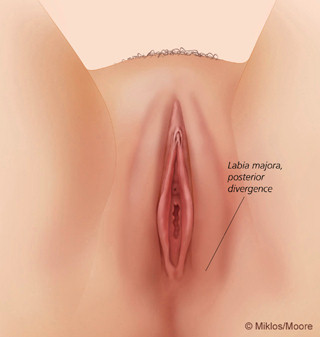 Figure 15a Labia majora posterior divergence
Figure 15a Labia majora posterior divergence
 Figure 15b Labia majora anterior divergence
Figure 15b Labia majora anterior divergence
Combined vulvar procedures
Many patients request and ultimately require combined procedures to achieve their desired results. When completing labia majora reduction concomitantly with labia minora reduction, the surgeon needs to be very careful in keeping the incisions separated to prevent the incisions from healing together. Typically the minora are completed first and then the majora (Figure 16a–d).
 Figure 16a Preoperative labia minora and majora
Figure 16a Preoperative labia minora and majora
 Figure 16b Labia monira incision lines
Figure 16b Labia monira incision lines
 Figure 16c Labia majora reduction incision lines
Figure 16c Labia majora reduction incision lines
 Figure 16d Postoperative labia minora and majora reduction
Figure 16d Postoperative labia minora and majora reduction
Conclusion
Cosmetic vaginal surgery is a newly emerging frontier in our dynamic and body image conscious society. Still in its infancy this discipline will continue to mature and take on a life of its own. Partially spurred by our ever pervasive process of globalization, the internet, the desire to “anti-age” and remain youthful in appearance and function, cosmetic vaginal surgery is here to stay. A woman’s desire to enjoy life to its fullest requires a good body image and sometimes a little surgical help might be necessary to help maintain that body image.
REFERENCES
Goodman MP. Female cosmetic genital surgery. Obstet Gynecol 2009;113(1):154 [DOI: 10.1097/AOG.0b013e318190c0ea] |
|
Pardo JS, Solà VD, Ricci PA, Guiloff EF, Freundlich OK. Colpoperineoplasty in women with a sensation of a wide vagina. Acta Obstat Gynecol Scand 2006;85(9):1125 |
|
Kent D, Pelosi MA. Vaginal Rejuvenation: An in-depth look at the history and technical procedure. Am J Cosmet Surg 2012;29(2):97. |
|
Dobbeleir JM, Landuyt KV, Monstrey SJ. Aesthetic surgery of the female genitalia. Semin Plast Surg 2011;25(2):130 [DOI: 10.1055/s-0031-1281482] |
|
DeLancey JO, Kearney R, Chou Q, Speights S, Binno S. The appearance of levator ani muscle abnormalities in magnetic resonance images after vaginal delivery. Obstet Gynecol 2003;101(1):46 |
|
Lien KC, Mooney B, DeLancey JO, Ashton-Miller JA. Levator ani muscle stretch induced by simulated vaginal birth. Obstet Gynecol 2004;103(1):31 |
|
Allen RE, Hosker GL, Smith AR, Warrell DW. Pelvic floor damage and childbirth: a neurophysiological study. Br J Obstet Gynaecol 1990;97(9):770 |
|
Dietz HP. Pelvic floor trauma following vaginal delivery. Curr Opin Obstet Gynecol 2006;18(5):528 |
|
DeLancey JO. The hidden epidemic of pelvic floor dysfunction: Achievable goals for improved prevention and treatment. Am J Obstet Gynecol 2005;192(5):1488 |
|
Mant J, Painter R, Vessey M. Epidemiology of genital prolapse: Observations from the oxford family planning association study. Br J Obstet Gynaecol 1997;104(5):579 |
|
Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the women's health initiative: Gravity and gravidity. Am J Obstet Gynecol 2002;186(6):1160 |
|
Brubaker L, Handa VL, Bradley CS, Connolly A, Moalli P, Brown MB, Weber A; Pelvic Floor Disorders Network. Sexual function 6 months after first delivery. Obstet Gynecol 2008;111(5):1040 [DOI: 10.1097/AOG.0b013e318169cdee] |
|
Signorello LB, Harlow BL, Chekos AK, Repke JT. Postpartum sexual functioning and its relationship to perineal trauma: A retrospective cohort study of primiparous women. Am J Obstet Gynecol 2001;184(5):881 |
|
WU JM, Hundley AF, Visco AG. Elective primary cesarean delivery: Attitudes of urogynecology and Maternal-Fetal medicine specialists. Obstet Gynecol 2005;105(2):301 |
|
Basson R, Berman J, Burnett A, Derogatis L, Ferguson D, Fourcroy J, Goldstein I, Graziottin A, Heiman J, Laan E, Leiblum S, Padma-Nathan H, Rosen R, Segraves K, Segraves RT, Shabsigh R, Sipski M, Wagner G, Whipple B. Report of the international consensus development conference on female sexual dysfunction: definitions and classifications. J Urol 2000;163(3):888 |
|
Pauls RN, Segal JL, Silva WA, Kleeman SD, Karram MM. Sexual function in patients presenting to a urogynecology practice. Int Urogynecol J Pelvic Floor Dysfunct 2006;17(6):576 |
|
Ellerkmann RM, Cundiff GW, Melick CF, Nihira MA, Leffler K, Bent AE. Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol 2001;185(6):1332 |
|
Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J 2013;24(11):1783 [DOI: 10.1007/s00192-013-2169-9] |
|
Novi JM, Jeronis S, Morgan MA, Arya LA. Sexual function in women with pelvic organ prolapse compared to women without pelvic organ prolapse. J Urol 2005;173(5):1669 |
|
Botros SM, Abramov Y, Miller JJ, Sand PK, Gandhi S, Nickolov A, Goldberg RP. Effect of parity on sexual function: an identical twin study. Obstet Gynecol 2006;107(4):765 |
|
Srikrishna S, Robinson D, Cardozo L, Cartwright R. Experiences and expectations of women with urogenital prolapse: a quantitative and qualitative exploration. BJOG 2008;115(11):1362 [DOI: 10.1111/j.1471-0528.2008.01842.x.] |
|
Barber MD, Visco AG, Wyman JF, Fantl JA, Bump RC. Sexual function in women with urinary incontinence and pelvic organ prolapse. Obstet Gynecol 2002;99(2):281 |
|
Rogers RG, Kammerer-Doak D, Darrow A, Murray K, Qualls C, Olsen A, Barber M. Does sexual function change after surgery for stress urinary incontinence and/or pelvic organ prolapse? A multicenter prospective study. Am J Obstet Gynecol 2006;195(5):131 |
|
Stoutjesdijk JA, Vierhout ME, Spruijt JW, Massolt ET. Does vaginal reconstructive surgery with or without vaginal hysterectomy or trachelectomy improve sexual well being? A prospective follow-up study. Int Urogynecol J Pelvic Floor Dysfunct;17(2):131 |
|
Paraiso MF, Barber MD, Muir TW, Walters MD. Rectocele repair: a randomized trial of three surgical techniques including graft augmentation. Am J Obstet Gynecol 2006;195(6):1762 |
|
Handa VL, Zyczynski HM, Brubaker L, Nygaard I, Janz NK, Richter HE, Wren PA, Brown MB, Weber AM; Pelvic Floor Disorders Network. Sexual function before and after sacrocolpopexy for pelvic organ prolapse. Am J Obstet Gynecol 2007;197(6):629 |
|
Komesu YM, Rogers RG, Kammerer-Doak DN, Barber MD, Olsen AL. Posterior repair and sexual function. Am J Obstet Gynecol 2007;197(1):101 |
|
Azar M, Noohi S, Radfar S, Radfar MH. Sexual function in women after surgery for pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct;19(1):53 |
|
Kuhn A, Brunnmayr G, Stadlmayr W, Kuhn P, Mueller MD. Male and female sexual function after surgical repair of female organ prolapse. J Sex Med 2009;6(5):1324 [DOI: 10.1111/j.1743-6109.2009.01229.x.] |
|
Bradner S, Monga A, Mueller MD, Herrmann G, Kuhn A. Sexual function after rectocele repair. J Sex Med 2011;8(2):583 [DOI: 10.1111/j.1743-6109.2010.02101.x.] |
|
Lakeman MM, Laan E, Roovers JP. The effects of prolapse surgery on vaginal wall sensibility, vaginal vasocongestion, and sexual function: A prospective single centre study. Neurourol Urodyn 2013;30 [DOI: 10.1002/nau.22491.] |
|
Thibault F, Costa P, Thanigasalam R, Seni G, Brouzyine M, Cayzergues L, De Tayrac R, Droupy S, Wagner L. Impact of laparoscopic sacrocolpopexy on symptoms, health-related quality of life and sexuality: a medium-term analysis. BJU Int 2013;112(8):1143 [DOI: 10.1111/bju.12286.] |
|
Kim SR, Moon YJ, Kim SK, Bai SW. Changes in sexual function and comparison of questionnaires following surgery for pelvic organ prolapse. Yonsei Med J 2014;55(1):170 [DOI: 10.3349/ymj.2014.55.1.170.] |
|
Tunuguntla HS, Gousse AE. Female sexual dysfunction following vaginal surgery: a review. J Urol 2006;175(2):439 |
|
Özel B, White T, Urwitz-Lane R, Minaglia S. The impact of pelvic organ prolapse on sexual function in women with urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 2006;17(1):14 |
|
Pardo J, Sola V, Ricci P. Colpoperineoplasty for vaginal relaxation: a follow up study. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:S147. |
|
Adamo C, Corvi M. Cosmetic mucosal vaginal tightening (lateral colporrhaphy): improving sexual sensitivity in women with a sensation of wide vagina. Plastic and reconstructive surgery. 2009;123(6):212e-213e. [PMID: 19483551 DOI: 10.1097/PRS.0b013e3181a3f5dd] |
|
Matlock D, Simopolous A. The Application of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) to Laser Assisted Anterior and Posterior Colporrhaphy with Perineorraphy. A Pilot Study. World congress on female & male cosmetic genital surgery; 2011; Las Vegas, Nevada. |
|
Goodman MP, Placik OJ, Benson III RH, Miklos JR, Moore RD, Jason RA, Matlock DL, Simopoulos AF, Stern BH, Stanton RA, Kolb SE, Gonzalez F. A large multicenter outcome study of female genital plastic surgery. J Sex Med 2010;7(4pt1):1565 [DOI: 10.1111/j.1743-6109.2009.01573] |
|
Moore RD, Gretchen MK, Miklos JR, Chinthakanan O. Evaluation of sexual function outcomes in women undergoing vaginal rejuvenation/vaginoplasty procedures for symptoms of vaginal laxity/decreased vaginal sensation utilizing validated sexual function questionnaire (PISQ-12). Surg Technol Int 2014;24:253 |
|
Ackard DM, Kearney-Cooke A, Peterson CB. Effect of body image and self-image on women’s sexual behaviors. Int J Eat Disord. 2000 Dec;28(4):422-9. |
|
Liao LM, Creighton SM. Requests for cosmetic genitoplasty: How should healthcare providers respond? Br Med J 2007; 334, 1090-92. |
|
Tracy E. Elective Vulvoplasty: A bandage that might hurt. Ob Gyn 2007; 109(5):1179-1180. |
|
Pauls RN. Nip, tuck and rejuvenate; the latest frontier for the gynecologic surgeon. Int Urogynecol J Pelvic Floor Dysfunc; 2007; 18 (8): 841-42. |
|
Miklos JR, Moore, RD. Labiaplasty of the labia minora: patients’ indications for pursuing surgery. J Sex Med 2008; 5(6):1492-5. |
|
Goldstein AT, Romanzi LJ. Z-plasty Reductional Labiaplasty. J Sex Med 2007;4:550-553. |
|
Rouzier R, Louis-Sylvestre C, Paniel BJ, Haddad B. Hypertrophy of labia minora : experience with 163 reductions. Am J Obstet Gynecol 2000 : 182 ;35-40. |
|
Choi HY, Kim KT. A new method for aesthetic reduction of labia minora (the deepithelialized reduction labioplasty). Plast Reconstr Surg 2000: 105;419-422. |
|
Alter GJ. A new technique for aesthetic labia minora reduction. Ann Plast Surg 1998;40:287-290 |
|
Caparo VJ. Congenital anomolies. Clin Obstet Gynecol 1971;14:988. |
|
Radman HM. Hypertrophy of the labia minora. Obstet Gynecol 1978;48 (suppl):78S. |
|
Chavis WM, LaFerla JJ, Niccolini R. Plastic repair of elongated, hypertrophic labia minora. A case report. J Reprod Med 1989;34:373. |
|
Kato K, Kondo A, Gotoh M. Hypertrophy of labia minora in myelodysplastic women. Labioplasty to ease clean intermittent catheterization. Urology 1988;31:294. |
|
Miklos JR, Moore RD. Postoperative Cosmetic Expectations for Patients Considering Labiaplasty Surgery: Our Experience with 550 Patients. Surg Technol Int. 2011 Dec 1;XXI:170-174. |