The Place of Vaginal Hysterectomy
Authors
INTRODUCTION
Hysterectomy can be performed in several ways and many techniques have been devised and modified to suit individual requirements. Laparoscopy has revived thought processes on choosing the best route and/or technique for hysterectomy, but has also confused many young and inexperienced gynecologists regarding the definitive criteria for selection. Fortunately, one can pick and choose the right technique except for in a small gray zone of cases between total laparoscopic hysterectomy (TLH) and total abdominal hysterectomy (TAH). What is often missed is which technique is ‘RIGHT’ for whom? For the patient or her operating surgeon? The decision should depend on what is the best for a given patient in given circumstances. No other factor should interfere in this holistic decision, keeping in mind the sage advice of Hippocrates: “If choicest is not chosen it is harm”. Our esteemed teacher Dr C.G. Saraiya used to tell us repeatedly: "If you can do no good, do no harm."
In this era of evidence based medicine clear scientific evidence exists to determine the superiority for selection between all three methods available, that is vaginal hysterectomy (VH), total laparoscopic hysterectomy – laparoscopic or laparoscopic assisted vaginal hysterectomy (TLH or LAVH), and abdominal hysterectomy (AH).
The evidence from various randomized controlled trials, observational studies, and meta-analyses is as follows:
- 2009 Cochrane Database Systemic Review1 which included only randomized controlled trials, comparing one surgical approach of hysterectomy with another and looked at the most beneficial and least harmful surgical approach to hysterectomy for women with benign gynecological conditions. Evidence concludes that no benefits accrue from TLH when compared with VH. TLH is accompanied by disadvantages of increased operation time – operation theater occupancy and higher complication rate. The conclusion drawn from all the parameters in this study is that VH should be performed in preference to AH where possible and where VH is not possible, TLH may avoid the need for AH.
- Donnez et al.2 presented a series of 3190 laparoscopic hysterectomies for benign disease from 1990 to 2006, wherein complications of TLH/LAVH were compared with those of AH and VH. The authors concluded that in experienced hands, TLH is safe, cost-effective, and without any increase in major complication rates. However, when VH can be performed safely, the laparoscopic method does not come into consideration. In other words, TLH can replace AH. Remarkably, they have reduced the incidence of AH to a paltry 3.8%.
- A prospective observational multicenter study was undertaken in France and 12 out of 15 university hospitals participated in it. The aim was to evaluate complications and the routes of hysterectomy for benign pathology. The results showed that the vaginal route is being increasingly used for hysterectomy in France and is the route of choice for benign disorders.3
- The EVALUATE hysterectomy study, a multicenter randomized trial showed TLH was associated with a significantly higher risk of major complications and took longer time than AH.4
- Several studies show a clear benefit of the vaginal route over the abdominal, and only when VH is not possible is TLH preferred, though it is associated with higher bladder and ureteric trauma. LAVH/TLH is the most expensive of all three methods.5, 6, 4, 7, 8, 9
Table 1 shows the choice of route and technique based on the benefits and disadvantages.10
Table 1. Which hysterectomy?
| Indications/associated situations
| Vaginal | Trial VH (tentative vaginal) | TLH/LAVH† | Abdominal† |
| Abnormal uterine bleeding (DUB) | 1C | 1A* | 1A |
|
| Adenomyosis | 1C | 1A* | 1A |
|
| Fibroid(s): uterus up to 12 weeks’ size | 1C |
|
|
|
| Endometrial hyperplasia with OR without atypia | 1C |
|
|
|
| Polyp: cervical/endometrial | 1C |
|
|
|
| Nulliparity | 1C | 1A* | 1A |
|
| Severe mental handicap | 1C |
|
|
|
| Cervical intraepithelial neoplasia III | 1C |
|
|
|
| Endometrial malignancy (early ‘Ca’ in high risk women) | 1C |
| 2A | 1A |
*For vaginal surgeons when size is >12 weeks and volume >250–300 cm3;†only when vaginal is contraindicated.
1C, first choice; 1A, first alternative; 2A, second alternative; LAVH, laparoscopically assisted vaginal hysterectomy; VH, vaginal hysterectomy; TLH, total laparoscopic hysterectomy. (Taken from Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:316)
In the USA, a country where litigation is very common, the American College of Obstetricians and Gynecologists (ACOG) recommends the following indications to use the laparoscope to assist vaginal surgery, i.e. by LAVH.11
1. Lysis of adhesions;
2. Treatment of pelvic endometriosis;
3. Difficult oophorectomy;
4. Fibroid that complicates VH;
5. Evaluation of abdominal/pelvic cavity.
In other words, opening of the abdomen is scientifically to be ignored in those situations. It equally means that (1) in the absence of adhesions or endometriosis, laparoscopic assistance is not required; (2) mere need for oophorectomy or presence of a fibroid does not mean that such cases are difficult or complicated to deal with. In the absence of uterine prolapse, this leaves wide scope for the vaginal route for hysterectomy in cases of benign gynecological conditions.
Cost, theater occupancy, and complications reduce the credibility and advantages of use of the laparoscope. In large studies of laparoscopic total hysterectomy a risk of 5% or more of trauma to ureters has been documented. Authors condemn surgical thoughts and actions of routine cystoscopy to evaluate the bladder and ureters after vaginal gynecologic surgery.12 Use of the vaginal route has been brought into the spotlight and is being reinvestigated with the introduction of laparoscopic technique, assisted or total.7, 10
Common indications for VH include:9, 10
- Abnormal uterine bleeding (DUB);
- Uterine adenomyosis;
- Uterine fibroid(s);
- Endometrial polyposis/hyperplasia;
- Uterine prolapse.
Uncommon indications include:
- Premalignant conditions of cervix and uterus;
- Early endometrial cancer in high risk women;
- Hydatidiform mole in multipara.
Associated conditions include:
- Nulliparity;
- Severe mental handicap;
- Surgery in the past;
- Conditions related to the abdomen: obesity.
ABNORMAL UTERINE BLEEDING (DYSFUNCTIONAL UTERINE BLEEDING): WHICH HYSTERECTOMY?
Dysfunctional uterine bleeding (DUB) with or without relaxation in the absence of contraindication is a universally acknowledged indication for VH.10 Jeffcoate13 stated that hysterectomy can easily be carried out by the vaginal route and this involves little risk and minimum complications. Studd14 found a paucity of literature concerning the role of hysterectomy in the treatment of menorrhagia. In abnormal uterine bleeding (AUB; DUB), there is usually an absence of any contraindication for VH. Unusually, when the uterine size exceeds 12 weeks and the uterine volume is greater than 250–300 cm3, the surgeon must consider debulking to facilitate VH, or consider LAVH.
ADENOMYOSIS: WHICH HYSTERECTOMY?
This is an ideal indication for VH, though quite often a definitive diagnosis and differentiation from DUB is made only after careful histopathological examination of the removed uterus.
The adenomyotic uterus can become unduly enlarged, be of more than 12 weeks’ size or of a volume greater than 250–300 cm3, contraindicating VH. The authors have come across uteri as large as 20–22 weeks and uterine volume greater than 500–600 cm3 purely due to adenomyosis. An experienced gynecologist can perform VH using heavy debulking through morcellation. For more than 3000 hysterectomies performed only for DUB and/or adenomyosis out of total 5655 hysterectomies, the author has not performed a single hysterectomy other than through the vaginal route.9 When VH is contraindicated because of size, LAVH/TLH should be considered. Abdominal hysterectomy should have no place for indications like AUB (DUB) and adenomyosis as size would uncommonly contraindicate VH or LAVH/TLH.
FIBROIDS AND ENLARGED UTERUS: WHICH HYSTERECTOMY?
The decision regarding the technique for hysterectomy in cases of fibroids and enlarged uterus due to benign cause, depends basically on the total uterine volume or size, based on preoperative clinical and reliable sonographic findings and not on the number of fibroids or mere presence of fibroid(s). For uterine size estimation, volume or gestational size close to 250–300 cm3 or 12 weeks, respectively, are useful, though when it comes to debulking, volume is more useful than size in gestational weeks.
When the uterine size exceeds 12 weeks and/or volume is greater than 250–300 cm3, experience in debulking can help. The location (and size of the largest fibroid) particularly its distance from internal os and endometrium is a useful guide,15 notwithstanding that hysterectomy should never be performed before both uterine arteries are well secured. The debulking procedures used are enucleation with or without morcellation with or without bisection of the uterus, besides myometrial coring and others (Table 2). A distally placed anterior wall and/or fundal myoma is likely to require extra attention; however, a rounded uterus with all three dimensions of 10 cm or more (Fig. 1) with an angle of around 90° between the lateral cervical and uterine borders contraindicates the vaginal route even for vaginal surgeons as it is likely to result in failure.15
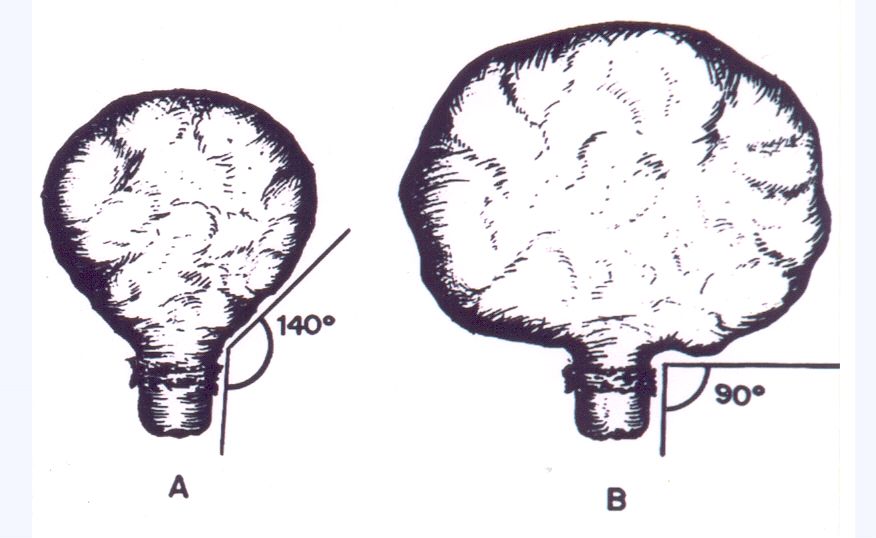 Fig. 1. The depicted angle between lateral cervical and uterine borders, greater than 140°, makes access and reach easier. Reduction in angle towards 90° makes access and reach very difficult or impossible. (From Sheth SS. Uterine fibroids. In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:88)
Fig. 1. The depicted angle between lateral cervical and uterine borders, greater than 140°, makes access and reach easier. Reduction in angle towards 90° makes access and reach very difficult or impossible. (From Sheth SS. Uterine fibroids. In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:88)
Table 2. Which route/technique when uterine size due to fibroids contraindicates vaginal hysterectomy
| Size/volume | Vaginal | Trial VH (tentative vaginal) | TLH/LAVH† | Abdominal† |
| Fibroids: uterus up to 14–16 weeks’ size/volume greater than 300–400 cm3 |
| 1A/1C* | 1C |
|
| Fibroids: uterus >16 and up to 20 weeks’ size/volume upto 500–≥600 cm3 |
| 1C* | 1C | 1A |
| Fibroids: uterus more than 20–24 weeks’ size/volume greater than 600–800 cm3 |
|
|
| 1C |
*For vaginal surgeons; †only when vaginal is contraindicated.
1C, first choice; 1A, first alternative; LAVH, laparoscopically assisted vaginal hysterectomy; VH, vaginal hysterectomy; TLH, total laparoscopic hysterectomy.
(Taken from Sheth SS. Uterine fibroids In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:91)
Thus, the scenario is crystal clear. For a uterus upto 12 weeks' size or 250–300 cm3 volume, it is in the best interest of patients to perform VH. For greater sizes or volumes, LAVH or TLH is ideal; however, vaginal surgeons can easily undertake much larger sized uteri for debulking and spare the abdomen. Only when TLH or LAVH becomes risky or very difficult, should the abdomen be opened for hysterectomy. No doubt, as experience increases, the size that contraindicates VH, will become proportionately greater, reducing the number of TLH or LAVH.
CERVICAL FIBROID: WHICH HYSTERECTOMY?
The presence of a cervical fibroid deserves extra care at hysterectomy by any of the techniques. The easiest to deal with is a posterior wall cervical fibroid and the least desirable is a large lateral wall cervical fibroid. As long as the total uterine volume and/or size does not contraindicate the vaginal route for hysterectomy, a cervical fibroid should not deter the gynecologist.
CERVICAL SUBMUCOUS MYOMATOUS POLYP: WHICH HYSTERECTOMY?
A cervical polyp or a large submucous myomatous polyp that extrudes from the cervical canal or arising from the cervical lip, fills the vagina partly or wholly and obscures speculum examination, is often subjected to AH (Fig. 2).10, 16, 17 Prima facie speculum findings in such a case will suggest that the vaginal route is not possible; at the same time the laparoscope is not helpful for the submucous polyp protruding from the cervix and seen at the vaginal end. Mattingly and Thompson18 consider AH to be contraindicated as there is an increased risk of infection as well as ureteral damage due to the dilated cervix, which is closer to the ureter. Bringing out a necrotic and infected polyp through the peritoneal cavity is also not desirable.
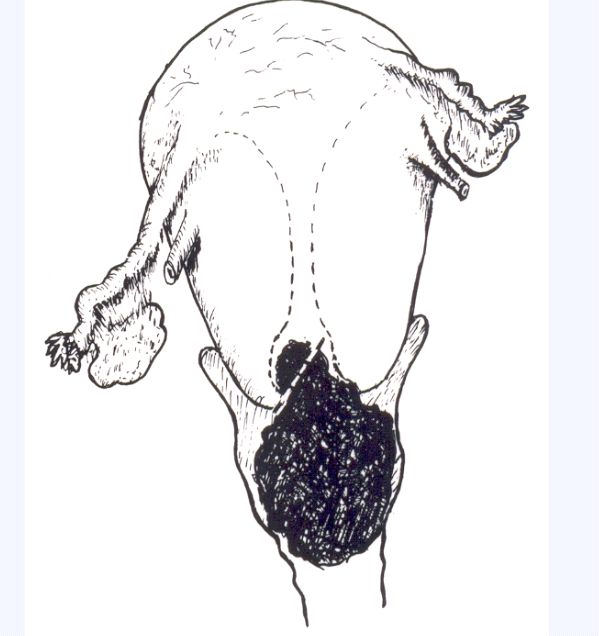 Fig. 2. The cervical polyp/fibroid (submucous myomatous polyp) fills almost all of the vagina and apparently contraindicates vaginal hysterectomy. Polypectomy close to its base (dotted line), followed by examination under anesthesia will favor vaginal hysterectomy. (From Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd J, eds. Vaginal Hysterectomy. London: Martin Dunitz Ltd, 2002:306).
Fig. 2. The cervical polyp/fibroid (submucous myomatous polyp) fills almost all of the vagina and apparently contraindicates vaginal hysterectomy. Polypectomy close to its base (dotted line), followed by examination under anesthesia will favor vaginal hysterectomy. (From Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd J, eds. Vaginal Hysterectomy. London: Martin Dunitz Ltd, 2002:306).
What can be of great help is careful assessment under anesthesia soon after vaginal myomectomy. If hysterectomy is required, it is advantageous to perform it vaginally at the same sitting as vaginal myomectomy so as to avoid repetition of anesthesia and hospitalization.
UTERINE PROLAPSE: WHICH HYSTERECTOMY?
The question of which hysterectomy to perform in cases of uterine prolapse should not arise. Hysterectomy should always be performed via the vaginal route even when this would not be the case in the absence of prolapse. It would be foolhardy even for a staunch laparoscopic surgeon to undertake TLH or LAVH which would be more invasive and less of a gynecological approach for what is a gynecological condition.
CARCINOMA IN SITU OF CERVIX: WHICH HYSTERECTOMY?
Severe dysplasia or carcinoma in situ or cervical intraepithelial neoplasia (CIN) grade III needs the careful attention of the gynecologist. Routine hysterectomy for carcinoma in situ cannot be recommended but patients who do not want children and who have margins of the cone involved may be treated by hysterectomy.19 Mitchell20 feels that VH is an excellent operation for carcinoma in situ when the involved areas in the cervix have been diagnosed by cone and the adjacent tissue mapped by colposcopy either within 48 hours or after 8 weeks.
Among several modalities of therapy, hysterectomy has a definite place. This should be by the choicest method i.e., via the vaginal route. The vaginal route offers excellent cuff21, 22, 23 and provides a significant advantage in the treatment of carcinoma in situ.24
Navratil24 did 339 hysterectomies for carcinoma in situ between 1946 and 1964; 76.4% of which were VH. We strongly feel that if the chosen treatment is hysterectomy and if it is not by a vaginal route, choice does not befit a gynecologic oncologist and it is not in the best interests of their patients.
Laparoscopic/abdominal route is not in the best interests of patient when:
- Uterine size is 12 weeks OR less;
- Uterine volume is 250–300 cm3 OR less;
- Adnexa are normal;
- Uterus is freely mobile.
Cancer cervix
Stage Ia1, early cancer with limited lymphatic invasion does not require anything more than hysterectomy. The ideal would be a minimally invasive vaginal hysterectomy. In these cases precision in making a diagnosis is very important.7
ENDOMETRIAL MALIGNANCY: WHICH HYSTERECTOMY?
The majority of endometrial cancer cases are treated by TAH with bilateral salpingo-oophorectomy and with or without lymph node dissection along with complete surgical staging. A large number of studies show that lymphadenectomy is not required in these cases as it adds to morbidity and does not improve survival rates.25, 26
In a select group of patients, minimally invasive VH proves advantageous providing adequate vaginal ‘cuff’, less morbidity, equivalent disease-free survival and overall good or improved survival. This will differentiate gynecological oncologist from others. Vaginal route is indicated for:
- Well differentiated or select moderately differentiated endometrial adenocarcinoma;
- Obese and/or hypertensive and/or diabetic women and/or women with compromised cardiopulmonary status;
- Myometrial invasion is less than one half. The authors prefer to draw a line, morally at less than one third myometrial invasion with frozen section study.
POSTMENOPAUSAL BLEEDING: WHICH HYSTERECTOMY?
Persistent or recurrent menopausal bleeding without endometrial pathology indicates hysterectomy, which in the absence of any contraindication should be by the vaginal route. The treatment of choice in these patients is hysterectomy and preferably bilateral salpingo-oophorectomy to spare the patient from future ovarian disease.
HYDATIDIFORM MOLE: WHICH HYSTERECTOMY?
In countries with a high prevalence of hydatidiform mole whenever prophylactic hysterectomy is part of the management, the least invasive and favored technique of VH should be considered, if not contraindicated.27
NULLIPARA: WHICH HYSTERECTOMY?
For many gynecologists, nulliparity per se is a sufficient reason to avoid the vaginal route. While laxity from multiparity can help the surgical procedure, tissue firmness as a result of the nulliparous state requires a different skill. To decide a technique other than VH based on a woman’s parity is irrational.
As long as the uterus is less than 12 weeks’ size, or volume less than 250–300 cm3, freely mobile and without adnexal pathology, vaginal hysterectomy is always possible. Whilst descent in a multipara is more evident, there is always sufficient descent (i.e., physiological descent) in a nullipara to permit satisfactory vaginal hysterectomy. Nulliparity can only add flavor to the surgical art and should not become an excuse to avoid the least invasive available route.
Tohic et al.28 reported a group of 300 nulliparous patients undergoing hysterectomy. VH was planned in 75.7% cases and the success rate amongst them was 92.1%. Agostine29 showed a 96% success rate in performing VH in nulliparous women.
SEVERE MENTAL HANDICAP: WHICH HYSTERECTOMY?
As a rule severe mentally handicapped women are nulligravida and mostly with intact hymen. From a personal experience of VH without failure in more than 120 mentally handicapped nullipara with intact hymen, two facts emerge: (1) nullipara do have sufficient physiological uterine descent in the form of downward mobility; (2) even with intact hymen before an examination under anesthesia30 the nulliparous can undergo VH in absence of any contraindication.
HISTORY OF ABDOMINAL SURGERY: WHICH HYSTERECTOMY?
Mere history of pelvic surgery in the past does not determine the technique of hysterectomy. It is important to study the nature of the previous operation(s) which ultimately act as the deciding factor. A scarred abdomen can lead to inhibition for inserting the Veress needle or trocar, or the presence of an incisional hernia can tempt the surgeon to take the abdominal route to include hernia repair along with hysterectomy.
These operations can be broadly divided into four categories:17
- Operations performed on the uterus are the most important. Cesarean section, hysterotomy, and myomectomy demand extra care, but do not constitute absolute contraindications. Ventrofixation, an obsolete operation, contraindicates VH. In fact, such findings even in the absence of a ventrofixation operation in the past contraindicate VH.
- Sling operations for prolapse can make VH difficult, but not impossible.
- Operations performed on the tubes, ovaries, and broad ligament tissues give rise to a few flimsy adhesions reaching close to the upper pedicle, but these are easily separable and do not hinder surgery. They do not contraindicate VH.
- Operations performed on structures or organs other than the genital tract, such as adhesiolysis, or operations involving the intestines, gall bladder, urinary tract (but not the bladder) are in no way to be treated as contraindications.
Encountering any adhesion that holds the uterus inseparably or involves the possibility of traumatizing a hollow organ should be an indication to abandon the vaginal route and complete the operation abdominally or by using laparoscopic assistance.
It has been observed that when the bladder is adherent following a past cesarean, it is almost always in the central three-fifths and not in the lateral one-fifth. In addition, magnetic resonance imagung (MRI) studies (Figs. 3 and 4),31 as well as natural anatomy at the level of the cervical isthmus through different planes, show the availability of a distinct space medially between the uterocervical surface and the bladder until they come extremely close to each other in the midline,17 and laterally continuing between the leaves of the broad ligament (Fig. 5).31 Khung32 and Sizzi and Rossetti (laparoscopic surgeons)33 state that in cases of hysterectomy in patients with severe adhesions and multiple cesarean sections “A safer approach is from the lateral part of the cervix from a space firstly described as the uterocervical broad ligament space for the vaginal approach to hysterectomy in uteri with previous cesarean sections.”
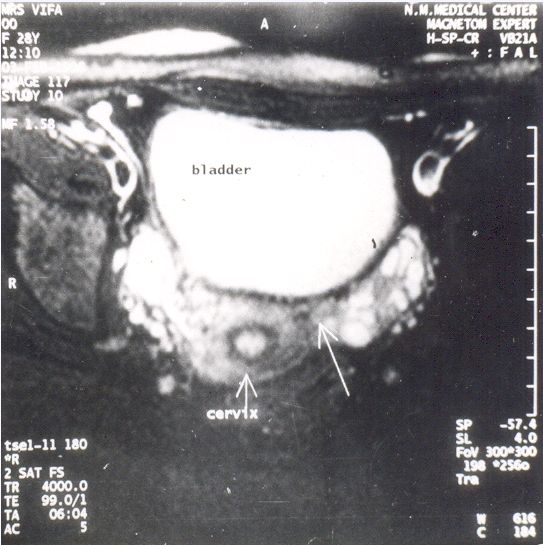 Fig. 3. Transverse section MRI at the isthmic level shows clear space between the bladder in front and the uterocervical surface behind, with continuity laterally between the two leaves of the broad ligament. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:137)
Fig. 3. Transverse section MRI at the isthmic level shows clear space between the bladder in front and the uterocervical surface behind, with continuity laterally between the two leaves of the broad ligament. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:137)
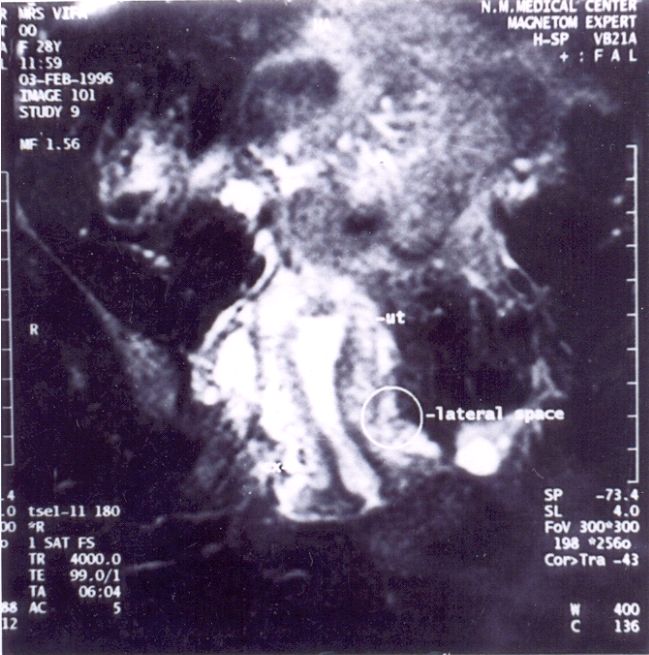 Fig. 4. Coronal section MRI shows a distinct vacant space medial to the line joining the maximally bulging uterus above and the cervix below with its continuity laterally. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:137)
Fig. 4. Coronal section MRI shows a distinct vacant space medial to the line joining the maximally bulging uterus above and the cervix below with its continuity laterally. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:137)
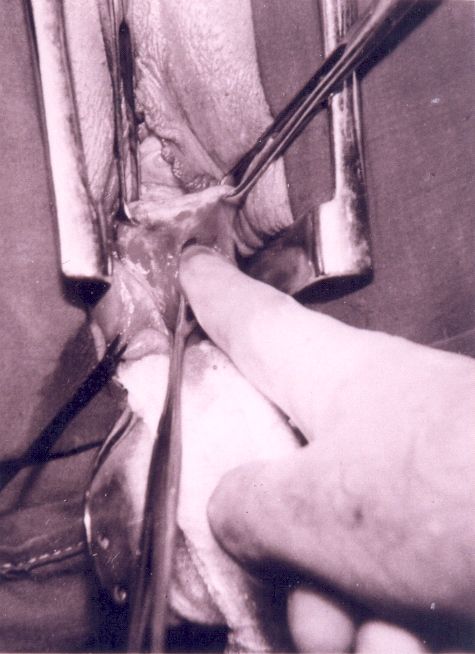 Fig. 5. At vaginal hysterectomy, the finger is on the uterocervical surface, with the bladder anteromedially, as it insinuates further between the two leaves of the broad ligament. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:138)
Fig. 5. At vaginal hysterectomy, the finger is on the uterocervical surface, with the bladder anteromedially, as it insinuates further between the two leaves of the broad ligament. (From Sheth SS. An approach to vesicouterine peritoneum through a new surgical space. J Gynecol Surg 1996;12:138)
The author has routinely used this surgical window for almost 20 years to obtain access to the vesicouterine space during vaginal hysterectomy in women with a previous history of cesarean section, including many with multiple previous cesarean sections and/or myomectomy or even a history of uterine rupture in the past.
In the absence of a contraindication, history of a cesarean in the past should never deter the operator from taking the vaginal route. At present the only scientifically acceptable modus operandi to get access to the vesicouterine peritoneum in the woman with cesarean section in the past is through the uterocervical broad ligament space. If doubt or anxiety persists, VH can be undertaken as TRIAL VH or after laparoscopic evaluation and confirmation of favorable pelvic findings.
PREVIOUS VAGINAL OPERATIONS: WHICH HYSTERECTOMY?
History of a vaginal operation in the past per se does not contraindicate hysterectomy by any technique excepting operations like vesicovaginal fistula (VVF) repair, rectovaginal fistula (RVF) repair, and Fothergill’s operation. In such cases an attempt to perform VH is to invite bladder or rectal injury. Some other vaginal operations which were undertaken in the past may require extra care.
OOPHORECTOMY REQUIRED: WHICH HYSTERECTOMY?
When bilateral oophorectomy is also required at hysterectomy, the choice of hysterectomy should not be influenced by the need for oophorectomy but should depend totally on the choice of hysterectomy. If the vaginal route has been chosen, it should remain so and oophorectomy should be performed vaginally at VH.
If hysterectomy can be performed vaginally, neither route for the hysterectomy should be changed to other than vaginal nor ovaries be preserved, when they need to be removed, simply because hysterectomy is to be performed vaginally. When oophorectomy is genuinely difficult and it is mandatory to remove ovaries, one could add laparoscopic assistance. In fact, one can comfortably deal with even benign mobile adnexa for salpingo-oophorectomy at vaginal hysterectomy.7, 34
TOTAL OR SUBTOTAL HYSTERECTOMY
Several prospective, randomized trials from United States, England, Holland, and Denmark suggest that preservation of the cervix does not help bladder, bowel, and sexual function. In a prospective, randomized trial 4.6% of those who underwent total hysterectomy were incidentally found to have high grade cervical displasia.35
Authors wonder at laparoscopic surgeons commending subtotal hysterectomy. Is hysterectomy subtotal because of lack of surgical confidence to safeguard ureters and bladder at laparoscopic surgery and later advocating better sex life and/or preserving uterosacral ligaments intact, as if it were a marketing device? Morrow36 rightly asks: “Is the conventional wisdom that teaches that the cervix be removed with the uterus to be disregarded for the technology costs and reduced recovery time?”
We recommend subtotal or supracervical hysterectomy only when (1) ureter and/or colon are at risk of trauma because of dense adhesions; (2) the anesthetist requests a quick completion of the surgery in interest of patient; or (3) the woman is keen to preserve her cervix.
EXAMINATION UNDER ANESTHESIA
The findings of an examination under anesthesia (EUA) performed just before the start of hysterectomy serves as the gold standard for a decision as to which route and technique is appropriate for hysterectomy.7 EUA is performed only after placing the patient in the lithotomy position and not in supine position, by careful speculum examination using a vulsellum or tenaculum on the cervix and bimanual examination.
After placing Sims speculum both of the lips of the cervix should be caught separately with one vulsellum on each and the anterior and posterior fornices systematically assessed to determine the laxity of the vaginal mucosa and its rugosities, any puckering or dimpling. If the vaginal mucosa is tautly held back at the site of the bladder and rectal reflections, caution is needed whilst opening the pouch. Puckering or retraction of the posterior vaginal mucosa at the site of the posterior pouch indicates pelvic inflammatory disease or endometriosis. The latter may form a dimple at the site contraindicating the vaginal route.37 Traction on the cervix reveals, as a rule, physiological descent in all women without pelvic pathology including all nulliparous women.
Bimanual examination is done to assess the size of the uterus, uterine mobility, to confirm adnexal normalcy and judge the availability of uterus-free space in the pelvis.
TRIAL VAGINAL HYSTERECTOMY
A “trial of forceps” in obstetrics is used when there is a possibility of vaginal delivery, at the same time keeping facilities for cesarean section ready, if required. Comparable to this is the concept of a “trial vaginal hysterectomy” first described in 199317 with a facility for laparoscopic assistance and/or laparotomy kept on stand-by.
After careful EUA, there are times when it is felt that if a VH is attempted, it may succeed. Thereafter, an attempt is made to proceed via vaginal route as “trial VH”. Those likely to fall in this category are: (1) those with an enlarged uterus with a volume greater than 250–300 cm3 or 12 weeks' size; (2) those who have had a cesarean section in the past; (3) nulliparous women; or (4) an operating surgeon with doubt and anxiety in the absence of any clear contraindication for VH.
LAPAROSCOPIC EVALUATION
Laparoscopic evaluation is indicated in patients where there is reason to believe that trial VH may fail and/or to gain confidence during the early part of the learning curve. This will pave the way to success.11
It is recommended:
- When VH appears possible (i.e., not contraindicated) but the surgeon has some doubt or apprehension about adhesions or pathology, e.g., history of cesarean in past or early endometriosis;
- Adnexal pathology (Fig. 6): when an experienced vaginal surgeon plans to excise a benign, mobile, adnexal mass at VH and undertake as trial vaginal route, laparoscopy will confirm the earlier findings, exclude suspicion of malignancy and tuberculosis, and help to evaluate the possibility of removal of the uterus via the vaginal route.9, 38
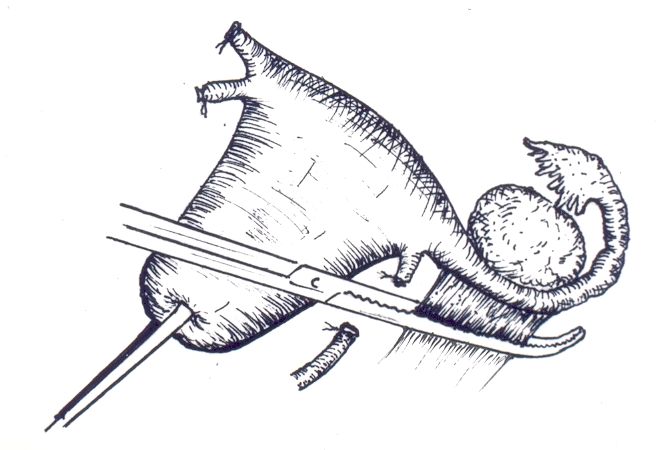 Fig. 6. Round ligament cut separately, away from the uterus and clamp applied on infundibulo-pelvic ligament to perform prophylactic slapingo-oophorectomy. (From Sheth SS. Adnexectomy for benign pathology at vaginal hysterectomy without laparoscopic assistance. Br J Obstet Gynaecol 2002;109:1402)
Fig. 6. Round ligament cut separately, away from the uterus and clamp applied on infundibulo-pelvic ligament to perform prophylactic slapingo-oophorectomy. (From Sheth SS. Adnexectomy for benign pathology at vaginal hysterectomy without laparoscopic assistance. Br J Obstet Gynaecol 2002;109:1402)ROLE OF PREOPERATIVE UTERINE VOLUME
When the uterus is more than 150–200 cm3 in volume or approximately 8–10 weeks' size, it is desirable that the operator religiously relies on a reliably measured uterine volume rather than clinically measured uterine size. Size as measured by gestational fundal height can easily misguide and lead to unexpected difficulty during vaginal hysterectomy. Uterine volume is a better measure of uterine size than its fundal height. Even with the same fundal heights, uterine volumes can grossly vary and therefore will offer different levels of ease or difficulty to the surgeon.39
In the absence of contraindication, volume less than 250–300 cm3 does not require laparoscopic assistance. A volume greater than 250–300 cm3 will indicate trial VH for progressive learning. Vaginal surgeons need to draw a line depending on his/her surgical skills and limitations. No doubt with experience and indulgence the limits may rise. Similarly, laparoscopic surgeons need to decide on the uterine volume/size above which laparotomy is to be preferred. Uterine size greater than 22–24 weeks size or with volume greater than 600–700 cm3 can make TLH risky, difficult and/or time consuming. No doubt, pelvic tissues through their laxity and relaxed state contribute to the ‘give’ obtained after severance of lateral attachment. Uterine size and its bulge due to fibroids and/or adenomyosis can encroach on the free space laterally towards the pelvic wall and thus reduce the uterus-free space and its availability. 17 There is no substitute for experience in these circumstances.
CONTRAINDICATIONS TO VAGINAL HYSTERECTOMY
Common absolute contraindications to VH are:
- Uterus more than 12 weeks’ size or uterine volume more than 250–300 cm3;
- Restriction of uterine mobility;
- Adnexal pathology.
Uncommon absolute contraindications to VH are:
- Cervix flush with the vagina or Fothergill’s operation which can make the cervix look missing or absent;
- Inaccessible cervix: uncommonly, after repeated uterine surgery, particularly, cesarean section, there are dense adhesions between the uterocervical surface, the bladder and the lower abdominal wall which makes the cervix inaccessible to an approach by the vaginal route. These adhesions (Fig. 7)40 can be anticipated by simple speculum examination by the presence of Sheth’s cervicofundal sign.7 and elicited clinically by seculum examination. With a rise in the cesarean section rate, gynecologists should be aware of such adhesions and diagnostic clinical signs (Fig. 8);7
- Vesicovaginal and/or rectovaginal fistula repair;
- Invasive cancer of the cervix beyond stage Ia1.
 Fig. 7. Classic adhesions following cesarean section seen at laparotomy. Deaver’s retractor and Allis forceps on the skin marking at the umbilical level close to the upper end of the right paramedian incision. The uterine fundus is well above half way between the symphysis pubis and the umbilicus. (From Sheth SS, Goyal MV, Shah N. Uterocervical displacement following adhesions after cesarean section. J Gynecol Surg 1997;13:144)
Fig. 7. Classic adhesions following cesarean section seen at laparotomy. Deaver’s retractor and Allis forceps on the skin marking at the umbilical level close to the upper end of the right paramedian incision. The uterine fundus is well above half way between the symphysis pubis and the umbilicus. (From Sheth SS, Goyal MV, Shah N. Uterocervical displacement following adhesions after cesarean section. J Gynecol Surg 1997;13:144)
 Fig. 8. Speculum examination in a woman with a past cesarean section shows a stretched and pulled up posterior vaginal wall and unseen cervix, high up behind pubic symphysis. This points the diagnosis of adhesions shown in Figure 7. (From Sheth SS. Vaginal hysterectomy. In: Prof. S. Arulkumaran, (Guest Editors R. Thakar & I. Manyonda) eds. Best Practice and Research – Clinical Obstetrics and Gynecology. USA: Elsevier Ltd, 2005;19:313)
Fig. 8. Speculum examination in a woman with a past cesarean section shows a stretched and pulled up posterior vaginal wall and unseen cervix, high up behind pubic symphysis. This points the diagnosis of adhesions shown in Figure 7. (From Sheth SS. Vaginal hysterectomy. In: Prof. S. Arulkumaran, (Guest Editors R. Thakar & I. Manyonda) eds. Best Practice and Research – Clinical Obstetrics and Gynecology. USA: Elsevier Ltd, 2005;19:313)
Associated conditions like adnexal pathology and broad ligament fibroid can rule out the vaginal route and leave the choice to LAVH/TLH or AH. However, it should be noted that vaginal surgeons can attempt and succeed at adnexectomy for benign pathology or broad ligament myomectomy vaginally and thus spare the woman from unnecessarily invasive alternatives.38, 41
COMPLICATIONS
The complication rate for AH is 70% higher than that for VH.42 Wound infection, which is unlikely after VH, can add 3.5 days to the hospital stay after AH.43 The VALUE study concludes that laparoscopic techniques tend to be associated with higher complication rates than other methods.44 However, the collaborative review of sterilization study (CREST) report shows an overall rate of bleeding of 2.6% with VH and of 1.6% with AH.45 The chances of leaving behind a sponge are remote with VH, with the use of a long gauze or roller gauze hanging partially on the speculum being helpful.
Dane et al.46 studied a group of 103 women undergoing VH for benign causes other than prolapse. Transabdominal ultrasonography was carried out 24–72 hours after surgery to assess the presence of vault hematomas. They concluded that sonographic detection of vaginal vault fluid collection is common (19.4% in their study) after hysterectomy but such a finding is rarely an indication for additional treatment. Vault hematoma after VH is often discussed in the literature. In the authors' series of 5655 cases of VH there were 28 cases of vaginal bleeding (postoperative) which were managed by vaginal packing (three under anesthesia).9 None required laparotomy. Though febrile morbidity was increased in cases with vault hematoma, the number of such patients was too small to be significant. The authors strongly do not recommend routine pelvic sonography for vault hematoma in the postoperative period of VH.
CONCLUSION
In choosing a hysterectomy technique in women with benign gynecological conditions without prolapse, there is no doubt that the vaginal route is safest, least invasive, economical, cosmetic, and natural route (Table 3).10 This has the best scientific evidence in its favor and is the route of choice for most women. Unfortunately, however, the vaginal route (though backed by strong evidence) is used in less than 40% of cases instead of the desirable and possible 70–90%.
Table 3. Comparative outcomes of the different types of hysterectomy
|
| VH | LAVH / TLH | TAH |
| Total relief – amenorrhea | Same | Same | Same |
| Morbidity | Least |
|
|
| Hospital stay | Short | Short | Maximum |
| Economical | Most | Least |
|
| Expertise needed and learning curve |
| Maximum | Least |
| Invasive | Least |
| Maximum |
| Access | Minimal |
| Maximum |
| High-risk patients | Safest |
|
|
| No. of indications/patients covered | Widest |
|
|
| Urinary tract trauma | Least | Maximum |
|
| Mortality | Least |
|
|
VH, vaginal hysterectomy; LAVH, laparoscopic assisted vaginal hysterectomy; TLH, total laparoscopic hysterectomy; TAH, total abdominal hysterectomy.
(From Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:317)
Teaching institutes which should ideally be pacesetters, unfortunately perform most of the hysterectomies abdominally. Unless senior gynecologists indulge and inculcate the right norms, juniors will never learn. Young gynecologists in teaching hospitals should have someone to emulate and learn the skill from and master the art of performing a VH.
The vaginal orifice is the route provided by nature and surgery for removal of the uterus through a natural orifice is feasible in upto 70–90% of cases. No doubt in 10–30% cases the operator is coaxed to go beyond and that is either towards laparoscopic assistance or in opening the abdomen. Every hysterectomy should be planned primarily by the vaginal route and, unless contraindicated, be performed via the vaginal route.7, 9
In the time of “natural orifice surgery” (NOS), VH is the one of the oldest existing NOS and should be thought of in most of the patients requiring removal of the uterus.
“Our doubts are traitors and make us lose the good, we oft might win by fearing to attempt” by Shakespeare is so true and applicable for all those who do not perform VH in the absence of contraindication and have doubt about succeeding. Gynecologists must come forward and adopt this route in larger numbers than they are doing at present. Flow chart in Figure 9 distinctly shows operative plan to apply in practice.10
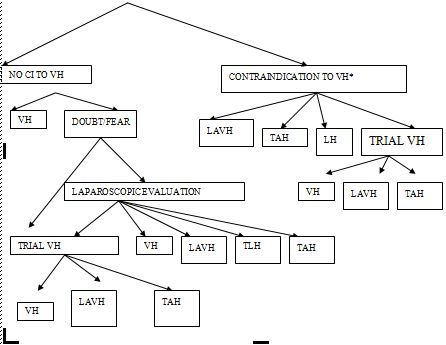 Fig. 9. Clinical examination, pelvic sonography finding and assessment under anesthesia. VH, vaginal hysterectomy; CI, contraindication; LAVH, laparoscopic assisted vaginal hysterectomy; TAH, total abdominal hysterectomy; LH, total laparoscopic hysterectomy.*will depend on the experience and inclination/vaginal surgeon. (Taken from Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:315)
Fig. 9. Clinical examination, pelvic sonography finding and assessment under anesthesia. VH, vaginal hysterectomy; CI, contraindication; LAVH, laparoscopic assisted vaginal hysterectomy; TAH, total abdominal hysterectomy; LH, total laparoscopic hysterectomy.*will depend on the experience and inclination/vaginal surgeon. (Taken from Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd JWW, eds. Vaginal Hysterectomy. London: Martin Dunitz, 2002:315)
Nonavailability or nonaccessibility of laparoscope or laparoscopists in 80% of world population, only adds strength to the crystallized scientific evidence that the vaginal route is the least invasive, most safe, and economical form amongst the available routes and techniques of hysterectomy.47 No wonder Jones48 insists on “Encourage the increased use of VH because of low morbidity, rapid postoperative recovery and cost savings”.
For any given indication for hysterectomy, in the absence of any contraindication to undertake VH, the response or reply to the question ‘Which technique for hysterectomy?’ is ‘vaginal’. There is no iota of doubt that only when vaginal hysterectomy is ruled out, all other forms of hysterectomy are second best alternatives. When VH, LAVH or TLH are ruled out, the gynecologist can open the abdomen, and take out the uterus.
If hysterectomy is possible by all three methods, abdominal, vaginal and laparoscopic, the order of merit in which to choose is vaginal, failing which laparoscopic is the next choice, and failing that the choice is the abdominal route.9
REFERENCES
Nieboer TE, Johnson N, Lethaby A, Travender E, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2009 8;(3):CD003677. |
|
Donnez O, Jadoul P, Squifflet J, Donnez J. A series of 3190 laparoscopic hysterectomies for benign disease from 1990 to 2006: evaluation of complications compared with vaginal and abdominal procedures. BJOG 2009; 116:492-500 |
|
David-Montefiore E, Rouzier R, Chapron C , et al. Surgical routes and complications of hysterectomy for benign disorders: a prospective observational study in French university hospitals. : Hum Reprod.2007; 22(1):260-5. |
|
Garry R, Fountain J, Mason S, et al. The eVALuate study: two parallel randomised trials, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy. BMJ 2004;328:129 |
|
Johnson N, Barlow D, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003677. |
|
Magos A. Presented at XIX FIGO World Congress. South Africa, October 2009. |
|
Sheth SS. Vaginal hysterectomy. Best Practice and Research – Clinical Obstetrics and Gynecology. Edited by Prof. S. Arulkumaran, (Guest Editors R. Thakar & I. Manyonda) USA. Elsevier Ltd. 2005;Vol.19 (3),307-32. |
|
Lenihan JP, Kovanda C, Cammarano C. Comparison of laparoscopic-assisted vaginal hysterectomy with traditional hysterectomy for cost effectiveness to employers. Am. J Obstet Gynecol 2004; 190: 1714-1722. |
|
Sheth SS. The scope of Vaginal hysterectomy. Eur jobs & Gyne & Reprod. Biol. :2004;115:224-230. |
|
Sheth SS. Vaginal or abdominal hysterectomy? In: Sheth SS, Studd JWW, eds. Vaginal hysterectomy . London: Martin Dunitz Ltd., 2002, pp 301-320. |
|
ACOG. Appropriate use of laparoscopically assisted vaginal hysterectomy (Committee Opinion). Compendium of selected publication. Washington DC (USA): The American College of Obstetricians & Gynecologists Women’s Health Care Physicians. 2006; pp 13-14. |
|
Sharon A, Auslander R, Brandes-Klein O, Alter Z, Kaufman Y, Lissak A. Cystoscopy after total or subtotal laparoscopic hysterectomy: The value of a routine procedure. Obstet & Gynecol Survey. 2006; 61: 511-512. |
|
Jeffcoate. Hysterectomy and its aftermath. In: Jeffcoate’s principles of gynecology. Revised by Tindall V R. London: Butterworths, 1987: pp 706-709 |
|
Studd J W W. Hysterectomy and menorrhagia. Bailliere’s Clin Obstet Gynecol 1989;3:415-424 |
|
Sheth SS. Uterine Fibroids. In: Sheth SS, Studd JWW, eds. Vaginal hysterectomy . London: Martin Dunitz Ltd., 2002, pp 79-94. |
|
Sheth SS, Shinde L. Vaginal Hysterectomy for Myomatous Polyp. J. Gynecol. Surgery 1993; 9: 101-103. |
|
Sheth S S. Vaginal hysterectomy. In: Studd J. Progress in Obstetrics and Gynaecology – 10th ed. London: Churchill Livingstone, 1993;317-40. |
|
Mattingly R F, Thompson J D. (eds) Te Linde’s operative gynecology. 8 ed. Pniladelphia: J B Lippincott 1985: pp 225-230, 548-555 |
|
Copplesonn M. Cervical intraepithetial neoplasia gynaecologic oncology. Fundamental principles and clinical practice. New York: Churchill Livingstone, 1981: pp 457-464 |
|
Mitchell G W. Benign and malignant disease of the breast. In: Mattingly R F, Thomapson J D, eds Te Linde’s operative gynecology. 8th ed. Philadelphia: J B Lippincott 1985: pp 183-202 |
|
Navratil E. In: La prophylaxie en gynaecologic et obstetrique. Tome I. Conferences et rapports du congress international de gynecologic et d’obstetrique. George, Geneva: Librairie de Universite, 1954 |
|
Kempers R D, Hunter J S Jr, Welch J S. Indications for vaginal hysterectomy. Obstet Gynecol 1959; 13:677-682 |
|
Smith L R, Pratt J H. Vaginal hysterectomy in the geriatric patients. Obstet Gynecol 1959; 14:84-91 |
|
Navratil E. The place of vaginal hysterectomy. J Obstet Gynaecol Br Commonwlth 1965; 72:841-846 |
|
Jones HW. New Developments in the surgical management of early endometrial cancer (Editorial). Obstet & Gynecol. 2009; 114: 2-3. |
|
Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomized study. The Lancet 2009 (10 January); 373: 125-136. |
|
Sheth SS. Prophylactic vaginal hysterectomy for benign hydatidiform mole. Int. J Gynecol & Obstet. 2007; 96: 38-39 |
|
Tohic AL, Dhainaut C, Yazbeck C, et al. Hysterectomy for benign uterine pathology among women without previous vaginal delivery. Obstet Gynecol, 2008 Apr;111(4):829-37 |
|
Agostine A, Bretelle F, Cravello L et al. Vaginal hysterectomy in nulliparous women without prolapse: a prospective comparative study. Int J Obstet Gynecol 2003; 110:515-518 |
|
Sheth S S; Malpani A. Vaginal hysterectomy for the management of menstruation in mentally retarded women. Int J Gynaecol Obset 1991;35:319-321. |
|
Sheth SS. An approach to Vesicouterine Peritoneum through a New Surgical Space. J Gynecol Surg. 1996; 12: 135-140. |
|
Khung TTG. Use of Sheth’s uterocervical broad ligament space for vaginal hysterectomy in a patient with history of caesarean section. Malaysian J of Obstet & Gynaecol 1995;4:39-42. |
|
Sizzi O, Rossetti A. Overcoming technical limits to laparoscopic hysterectomy. J of Gynecologic and Surgical Endoscopy. 2005. |
|
Sheth S S: The place of oophorectomy at vaginal hysterecomy: Br J Obstet & Gynecol 1991; 98: 662-666. |
|
Learman L. Summit RL. Varner ER, McNeeley GS, Goodman-Gruen D, Richter HE et al. A randomized comparison of total or supracervical hysterectomy: Surgical complications and clinical outcomes. Obstet Gynecol Survey 2004; 59: 90-91. |
|
Morrow CP, Mishell DR, Kirschbaum RH et al. Operative gynecology In 1994 year book of Obstet Ggynecol. Cap 11 257-283, Mosby St. Louis. USA. |
|
Sheth SS. Vaginal dimple: a sign to diagnose endometriosis. J Obstet Gynecol 1991; 2:292 |
|
Sheth SS. Adnexectomy for benign pathology at vaginal hysterectomy without laparoscopic assistance. Br. J Obstet Gynecol. 2002; 109:1401-1405. |
|
Sheth SS. Preoperative sonographic estimation of uterine volume: An aid to determine the route of hysterectomy. J. Gynecol Surgery 2002;18:13-22 |
|
Sheth SS, Goyal MV, Shah N. Uterocervical displacement following adhesions after caesarean section. J Gynecol Surg. 1997; 13: 143-147. |
|
Sheth SS. Broad ligament myomectomy at vaginal hysterectomy without laparoscopic assistance. Journal of Gynecol Surgery. 2007; 23: 133-142. |
|
Dicker RC, Greenspan JR, Strauss LT et al. Complications of abdominal and vaginal hysterectomy among women of reproductive age in the United States: the collaborative review of sterilization. Am J Obstet Gynecol 1982; 144:841-848. |
|
Soper DE, Bump RC, Hurt WG. Wound infection after abdominal hysterectomy: Effect of the depth of subcutaneous tissue. Am J Obstet & Gynecol. 1995; 173: 465-471. |
|
Maresh MJ, Metcalf MA, McPherson K, et al. The VALUE national hysterectomy study: description of the patient and their surgery. Br J Obstet Gynecol 2002;109:302-12. |
|
Harris WJ. Early complication of abdominal and vaginal hysterectomy. Obstet Gynecol Surv. 1995; 50: 795-805. |
|
Dane C, Dane B, Cetin A. et al Sonographically diagnosed vault hematomas following vaginal hysterectomy and its correlation with postoperative morbidity: Infect Dis Obstet Gynecol. 2009;2009:91708 |
|
Sheth SS, Paghdiwalla K. Do we need the laparoscopic route? J Obstet & Gynaecol of India. 2001; .51: 25-30. |
|
Whiteman MK, Hillis SD, Jamieson DJ, Morrow B, Podgornik MN,Brett KM, Marchbanks PA. Inpatient Hysterectomy Surveillance in the United States, 2000-2004. Obstetrical & Gynecological Survey 2008; 63: 304-305. |