Transvaginal ultrasonography and female infertility
Authors
INTRODUCTION
Fertility potential is taken for granted by most men and women. For women and their partners who experience difficulties conceiving, efficient, effective methods to evaluate fertility status are required. Therapy should be readily available to help conception occur quickly. Occasionally, individuals request an assessment of their fertility status before they attempt to conceive or when planning conception. They may also be concerned about the length of time needed to conceive especially as women postpone conception beyond the age of optimal fertility into advanced reproductive ages.
Ultrasonographic imaging is an effective, easy to use, safe, and readily available noninvasive means to evaluate fertility potential. It has become one of the most useful tools available to assess the causes of infertility and to implement many of the treatments used to ameliorate infertility. Ultimately, ultrasonography improves the quality of care provided by the assisted reproductive technologies (ART) by facilitating rapid diagnosis and the visualization of changes in reproductive physiology required to direct therapy. The objective of this chapter is to provide clinicians with an overview of the practical applications of ultrasonography in the evaluation and management of women who are trying to conceive or who simply want to know if conception is possible.
The diagnosis of infertility
Conception typically occurs at a rate of 20–22% per cycle in women who are less than 35 years of age.1 Approximately 50% of women not practicing contraception conceive within 3 months, 60% by 6 months, 80% by 12 months, and 90% within 18 months when no specific attention was paid to the time of optimal fertility. However, conception rates of 76%, 90%, and 98% within 1, 3, and 6 cycles, respectively, were reported in a study of “fertility focused intercourse”.
Infertility is diagnosed when conception has not occurred following 12 months of unprotected sexual intercourse.2 Infertility is not uncommon and consequently, at some time in their reproductive years, 8–15% of North American couples between 15 and 45 years of age may experience subfertility or infertility.3 Physician evaluation typically is initiated after 12–18 months have elapsed without conception. Women who have menstrual abnormalities, a history of pelvic surgery, infection, or advanced reproductive age may be evaluated sooner. The Canadian Fertility and Andrology Society of Canada and the American Society for Reproductive Medicine have outlined best-practice guidelines for the optimal sequence of diagnostic investigations and therapeutic interventions for couples who present with infertility.4, 5
The age of the female partner is important when making decisions about when to begin investigations and therapy for infertility. Women at an advanced reproductive age may benefit from early investigation and more aggressive therapy because of the rapid decline of fertility potential after age 35 and minimal or absent fertility potential beyond 39–42 years. It becomes increasingly important to complete an infertility evaluation and initiate therapy before the 1 year of infertility guideline, primarily because the window of fertility potential is time-limited. Women at advanced reproductive ages will benefit from a rapid evaluation of their fertility potential and are most likely to use ART) to increase their opportunity to conceive. ART have come to rely upon the use of ultrasonography to perform the available fertility therapies.
Ultrasonographic examinations to evaluate and treat infertility
Infertility assessments involve evaluations for male-only and female-only factors that will contribute to the fertility potential for a couple. The initial evaluation involves taking a detailed history focusing on the duration of infertility, the couple’s knowledge about reproductive physiology, the woman’s menstrual and obstetrical history, endocrine status and general health history, and exposure to potential toxins. In addition, the family's genetic and fertility history are discussed. The male partner’s evaluation includes an assessment of general health, history of conception, and semen characteristics. An ultrasound examination of the female partner can be routinely included in the physical examination to plan the most appropriate investigations and therapy more effectively.6 It has been our experience that involving the couple in each ultrasound examination clarifies the nature of their infertility and helps most couples to understand the physiologic process underlying each therapy. It is useful for both partners to receive counseling together when reviewing the steps required for investigation of the etiology of their infertility, and their treatment options. It is also helpful to engage both partners when discussing the probability of conception and reviewing the time requirements and expenses inherent with each available therapeutic modality. Communication should be appropriate to each couple’s level of comprehension and making the time available for them to ask questions of the physician should not be overlooked. Couples need to understand the rationale for, and be involved in, decision-making at each stage of investigation and therapy so that they have realistic expectations. In most centers, fertility care is now provided by multidisciplinary teams where each team member has a role to play in the assessment, ongoing counseling, and therapies. It is important that each team member have a patient centered approach to their individual role in the provision of care team.
The primary use of imaging in infertility is to assist clinicians to diagnose the etiology of a couple’s infertility and to assist in the delivery of safe, effective treatments that will lead to a high probability of conception. It is common to use ultrasonography early in infertility investigations as it has replaced more invasive modes of investigation and it should now be considered a part of standard care for infertility. Cyclic uterine and ovarian changes can be instantly evaluated and abnormalities, such as cysts, tumors, fibroids, endometriomas, hydrosalpinges, and congenital abnormalities can be visualized easily to allow for appropriate therapeutic actions early in the care of the infertile couple.7 Antral follicle counts can be assessed at any age to look for a reduction in follicle population, a clinical marker of early perimenopause reflecting a reduction in fertility potential.8, 9, 10 Conversely, discovery of polycystic ovaries can stimulate investigations to diagnose polycystic ovary syndrome and prompt counseling about lifestyle modifications and risks of ovarian hyperstimulation and multiple ovulation following ovulation therapy. In addition, the viability, number, and location of gestational sacs may be visualized very early in pregnancy following ART.11, 12, 13 Ultrasonography has become an indispensable tool for clinicians to interpret images quickly and respond with timely, accurate decisions to deliver the most efficacious therapy.
Imaging with high-resolution transvaginal ultrasonography has allowed us to increase our knowledge of female reproductive processes. A high-resolution image is easily captured when the ultrasound transducer is placed in the vaginal fornix, millimeters away from the uterus, ovaries, and oviducts. Patient discomfort is minimized and examinations can be completed on short notice as a full bladder is not required. The resolution of contemporary images has made the detection of minute differences in the morphology of the female reproductive organs possible with the development of relatively high frequency (e.g., 5.0–9.0 MHz), curvilinear array transducers, color-flow Doppler, and three-dimensional technologies. Images taken transvaginally have far surpassed the images available with transabdominal imaging.
Imaging has become an integral part of patient care as more obstetrician/gynecologists are trained to perform ultrasonographic examinations. Gynecologic and infertility imaging is no longer the sole perview of the general radiologist. Many imaging modalities that initially began as research oriented investigations have now become part of everyday patient care. Some clinical applications still remain in the developmental phase. However, as new discoveries are made and new applications are developed, transvaginal ultrasonography will continue to be utilized routinely as a clinical tool.
DIAGNOSTIC USE OF ULTRASONOGRAPHY IN INFERTILITY INVESTIGATIONS: THE OVARY
Assessment of ovarian follicular development
Our perceptions of human follicle growth and ovulation have changed dramatically since high resolution ultrasonography has been available.14, 15 During the past 50 years, it has been accepted that folliculogenesis begins with recruitment of a group or cohort of follicles in the late luteal phase of the preceding menstrual cycle followed by visible follicle growth in the next follicular phase.16, 17, 18, 19 The group or cohort of follicles begins growth and by the mid-follicular phase, around day 7, a single dominant follicle appears to be selected from the group for accelerated growth. The dominant follicle continues to grow at a rate of about 2 mm per day.20 In women, a preovulatory follicle typically measures ~18–20 mm when a surge of luteinizing hormone (LH) is released from the pituitary to trigger ovulation; ovulation occurs approximately 36 hours after LH release.21, 22
According to the "propitious moment theory", the recruited follicles grow continuously until a gonadotropin surge is stimulated at exactly the right time in the cycle when follicles are mature.23, 24, 25, 26 This model of follicle growth portrayed the normal menstrual cycle as a 28 day cyclic event where a single dominant follicle grew within a single follicle wave, ovulation occurred on day 14 and the luteal phase terminated 14 days later. However, this model failed to explain why or how women had variable menstrual cycle lengths or anovulatory follicles. In 2003, the old model of the menstrual cycle was superseded when follicle growth was shown to occur in waves.14, 15
WAVE PATTERN OF FOLLICULOGENESIS
Wave dynamics of follicle growth recognized in fertile women have helped to explain features of the menstrual cycle that were neglected in the past. Two or three waves of follicles have been demonstrated within single menstrual cycles in women.14, 15, 27 The wave pattern was previously discovered and documented in the estrous cycle of numerous domestic species years before being recognized in women.25, 26, 28, 29 Each follicle wave is composed of a group of antral follicles with synchronous growth.14, 15 Typically, one follicle grows to a larger diameter and becomes the lead, dominant follicle of the group. New follicle waves appear at regular intervals within cycles and each of the waves is preceded by a small increase in FSH. Within each cycle, the earlier waves are consistently anovulatory, whereas the final wave ends with ovulation. In this fashion, a two wave cycle begins with growth and regression of the first wave of follicles without ovulation; however, a second wave of follicles grow and a preovulatory follicle ovulates from the second follicle wave. In a three wave pattern, the first two waves are composed of only anovulatory follicles, but the final wave ends with ovulation of its dominant preovulatory follicle. Similarly, a five wave menstrual cycle has been documented. It was comprised of four waves that did not ovulate, but the final fifth growth wave terminated with ovulation (Baerwald et al., personal communication). In anovulatory waves, follicles grow to a maximal diameter and regress. Anovulatory waves are classified as minor if antral follicles are small, <8 mm, or major if the largest follicle diameters are >10 mm. It is of clinical value to learn that the maximal size of many anovulatory follicles (14–20 mm) in (major) anovulatory waves that regressed spontaneously were comparable in size and echotexture to the preovulatory follicles that progressed to ovulation in a later wave.
The natural history of follicle waves provides an explanation for persistence of large anovulatory follicles in the early follicle phase. A large anovulatory follicle may begin growth within a luteal phase wave and persist into the next menstrual cycle. Serial imaging in the early to mid or late follicular phase can map the fate of the follicle as it grows, becomes atretic and regresses spontaneously with time. Understanding that folliculogenesis occurs in regular wave patterns has also provided an explanation for some women to have consistently long menstrual cycle lengths, as women with more than two follicle waves had progressively longer cycles than women with only two wave cycles. The variability in cycle lengths and the formation of anovulatory follicles in the anovulatory waves of normal menstrual cycles can now be recognized as physiologically normal processes.
PREOVULATORY FOLLICLES
It is easy to identify a lead or dominant follicle arising within a cohort of growing follicles by its larger diameter (Fig. 1). However, the process underlying how one follicle is physiologically selected to develop preferentially and to ovulate when the remaining follicles progress to atresia is not well elucidated.30, 31 It has been shown that the process of follicle selection does occur within the single ovarian cycle when a given ovulation takes place because follicles can be stimulated to grow by providing gonadotropin hormones during ovulation induction therapy.31, 32, 33 The follicle within the wave that is selected for preferential growth continues differentiation into a preovulatory structure that attains a fine, complex vascular network within the theca interna of the follicle wall.
 Fig. 1. Normal ovary during a natural menstrual cycle demonstrating normal follicle population and distribution on day 12 postmenstruation. A dominant follicle is visualized in the central portion of the image and several subordinate follicles from the wave (2–5 mm) are observed in the left lateral aspect of the ovary.
Fig. 1. Normal ovary during a natural menstrual cycle demonstrating normal follicle population and distribution on day 12 postmenstruation. A dominant follicle is visualized in the central portion of the image and several subordinate follicles from the wave (2–5 mm) are observed in the left lateral aspect of the ovary.
An understanding of the wave model of folliculogenesis is important when evaluating follicle growth during fertility assessments. The basal follicle population is identified routinely with ultrasonography and follicle growth may be evaluated serially to predict the time of ovulation and plan for insemination therapy. When a dominant follicle has reached a diameter of 18–20 mm, LH monitoring may be done to detect a preovulatory LH level in blood or urine; another option includes induction of ovulation with an injection of human chorionic gonadotropin (hCG). If a large (14–20 mm) follicle is seen early in the menstrual cycle at the time when basal follicle growth is assessed, a clinician must decide if this follicle has grown within a very short follicular phase of a two wave cycle and is competent to ovulate. Alternatively, an anovulatory follicle may develop within an anovulatory follicle wave and grow to an ostensibly preovulatory diameter but later spontaneously regresses before an ovulatory wave begins development. While computerized image analysis has been developed that can clarify whether a follicle is destined to be ovulatory or anovulatory, to date, ultrasound technology alone cannot provide this analysis yet.34
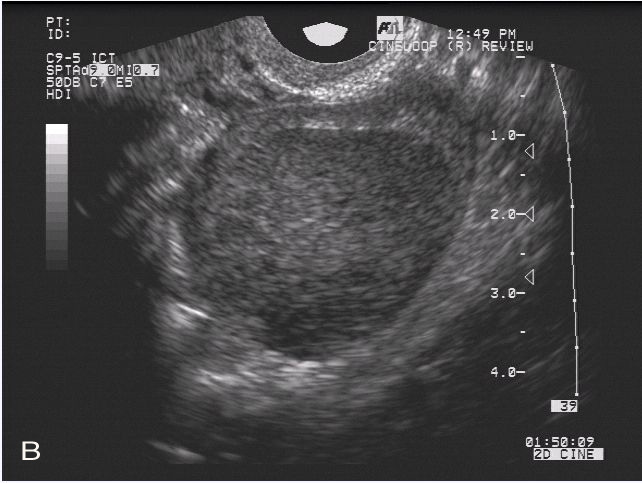
An atretic regressing follicle can be distinguished by its thin flaccid follicle wall and irregular follicle shape34 (Fig. 2). In order to assess whether a follicle is destined to ovulate, color flow Doppler interrogation can be used to differentiate the contrast between the increased vascularity of a healthy preovulatory follicle wall and the thin bright hyperechoic avascular wall of a follicle destined for atresia.34 In addition, the normal exponential increase in estradiol is observed during the growth of a healthy preovulatory follicle, whereas an anovulatory follicle tends to produce minimal estradiol. By identifying repetitive subtle defects in follicle growth, selection, and maturation, an ovarian etiology for infertility may replace a previous diagnosis of idiopathic infertility. Until computerized image analysis becomes available for routine clinical use, it is important to evaluate growing follicles carefully to predict their ovulation potential. Evaluation involves correlating the history of an individual’s menstrual cycle length and follicle wave dynamics with information derived from color flow Doppler imaging and estradiol assays. Follicles destined to ovulate tend to have vascular walls, clear antral fluid, produce an exponentially increasing amount of estradiol, and grow at a rate typical of other menstrual cycles for a given individual. An interpretation of folliculogenesis should be made to detect the deviation in normative growth patterns of anovulatory follicles in order to most effectively plan the best therapeutic modalities.
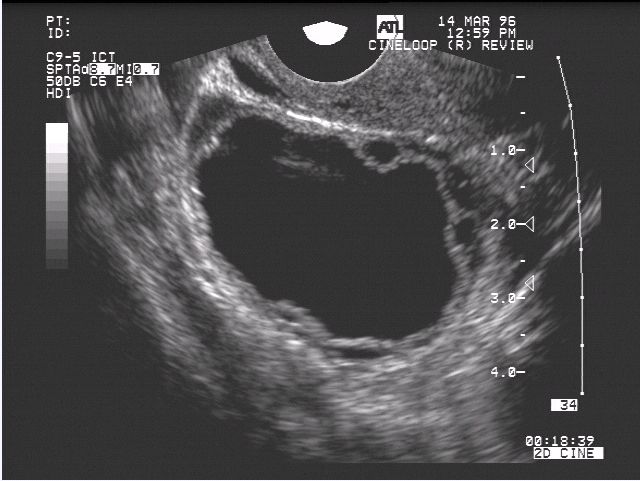 Fig. 2. Atretic follicle of preovulatory diameter. Note the thin follicle walls and sharp transition at the fluid-follicle wall interface. The shape of the large atretic follicle is compromised by small peripheral follicles.
Fig. 2. Atretic follicle of preovulatory diameter. Note the thin follicle walls and sharp transition at the fluid-follicle wall interface. The shape of the large atretic follicle is compromised by small peripheral follicles.
FOLLICULAR VASCULAR FLOW
The vascular network surrounding the dominant follicle can be appreciated easily with high-resolution color flow Doppler imaging (Fig. 3). The capillary structure of preovulatory follicles is physiologically different from subordinate follicles in that it is more extensive and vessels are permeable for nutrient/hormone exchange.35, 36, 37 The vascular tissue transfers gonadotropins, substrate, and hormones to the site of active ovarian metabolism allowing preferential follicle growth and development to continue. Doppler ultrasonography has been used to map the patterns of blood flow within the follicle wall of preovulatory follicles and during ovulation during natural menstrual cycles and ART cycles.38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49 Obvious changes in the peripheral vascular flow in the follicle wall can be observed from the onset of an LH surge to the time just prior to and during ovulation. Increased vascular flow from the base to the apex of the follicle wall have been demonstrated.35, 50 There is a gradual decrease in impedance to blood flow in the vasculature surrounding the follicle up to the onset of ovulation.51 Spectral Doppler flow waveforms have been generated in the perifollicular wall immediately before ovulation and are indicative of reduced resistance to vascular flow.38
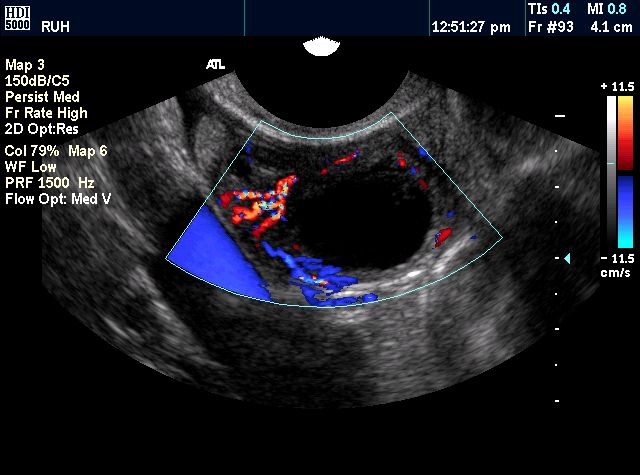 Fig. 3. Color flow Doppler image demonstrating perifollicular vascularity around a preovulatory follicle. Visualization of the complete paths of vascular flow around large follicles is challenging owing to the tortuous path of the vascular supply to the dominant follicle.
Fig. 3. Color flow Doppler image demonstrating perifollicular vascularity around a preovulatory follicle. Visualization of the complete paths of vascular flow around large follicles is challenging owing to the tortuous path of the vascular supply to the dominant follicle.
It would be clinically useful to use Doppler interrogation of individual follicles to predict the health of the follicle and developmental oocyte competence.43, 44, 48, 49, 52 There is some evidence in animal models that computer-assisted image analysis could adequately assess the probability that a follicle contains a competent oocyte.53, 54 Perifollicular vascularity has also been assessed in some human clinical ART programs.42, 43, 44, 47, 49, 52 Clinical pregnancy rates were higher when oocytes were retrieved from follicles with higher levels of vascular flow prior to oocyte retrieval compared to low levels of follicle vascular flow.44, 47, 49, 55 However, no differences were observed in the perifollicular vascularity and ovarian vascularity responses to ovarian stimulation between normal and poor responders in a clinical IVF study.48, 56, 57 While the relationship between perifollicular vascularity and pregnancy rates has been demonstrated in some laboratories, not all investigators regard vascular measurement to be a useful predictor. Further assessments of individual follicles and the probability of the fertilization of their oocytes are required before this modality can be included as a part of routine clinical care.42, 57 The role of power Doppler imaging to evaluate follicles before oocyte retrieval also is a possible means to assess follicle and oocyte competence, but the clinical utility has not been clarified at this time.
Ovulation and the corpus luteum
Before the wave dynamics of folliculogenesis were elucidated, ovulation was classically described as the terminal event in a follicle’s life that occurred on day 14 of a “standard 28 day menstrual cycle”.21, 24, 35, 58 Transabdominal ultrasound was the first mode of imaging used to investigate ovulation and ovarian physiology in vivo.59 Ovulation could be identified with transabdominal ultrasonography in 50–80% of natural menstrual cycles on day 14 of the “standard” menstrual cycle.60, 61, 62 However, with the introduction of high resolution ultrasonography, studies of folliculogenesis demonstrated that the corpus luteum could be imaged easily on the day of ovulation and throughout the luteal phase. Also, ovulation occurred on variable days of the cycle, not solely on the 14th day of the menstrual cycle.14, 15, 63, 64, 65
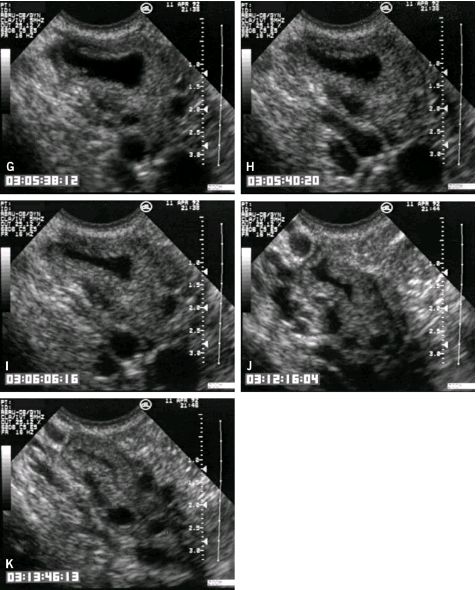
High resolution transvaginal ultrasonography has made it possible to visualize, in real-time, the process of follicle rupture and the evacuation of follicular fluid and the cumulus–oocyte complex63, 64 (Fig. 4). The time required for ovulation from the initial fluid leakage to the complete apposition of the follicle walls varied from less than 1 minute to more than 20 minutes. Evacuation of follicular fluid during ovulation averaged approximately 10 minutes. The new site of ovulation could be identified as soon as ovulation occurred by examining the external surface of the ovary for the point of rupture.
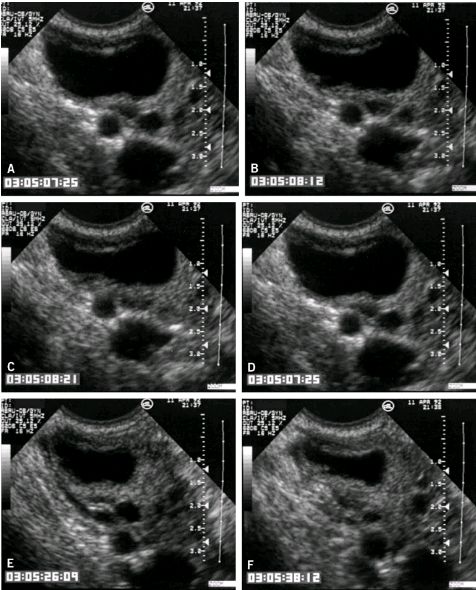 Fig. 4. Sequence of images (A–I) recorded during ovulation in situ. The images in the sequence were taken to represent the times at which 90%, 80%, 70%, and so on of the follicle fluid was extruded from the follicle. Time code markers are displayed in the lower left portion of the images.
Fig. 4. Sequence of images (A–I) recorded during ovulation in situ. The images in the sequence were taken to represent the times at which 90%, 80%, 70%, and so on of the follicle fluid was extruded from the follicle. Time code markers are displayed in the lower left portion of the images.
The corpus luteum is an endocrine gland responsible for helping to regulate the menstrual cycle and support early pregnancy. Cells of the preovulatory follicle wall contribute to the formation of the corpus luteum by structural and functional transformation that begins just prior to follicle rupture. Perifollicular capillaries fenestrate the basal lamina of the follicle wall, the basal lamina breaks down and luteal cells arise from theca interna and granulosa cells.66 Neoangiogenesis of the corpus luteum facilitates its endocrine gland activity. Vascular flow into the corpus luteum is an indicator of metabolic activity (Fig. 5). The enhanced vascular network facilitates the delivery of hormones such as LH and hCG to the luteal tissues and modulates its endocrine activity.67 As the corpus luteum develops after ovulation, an increase in the luteal tissue volume is noted and there is an increase of progesterone and estradiol concentration for at least 6 days.65, 68, 69
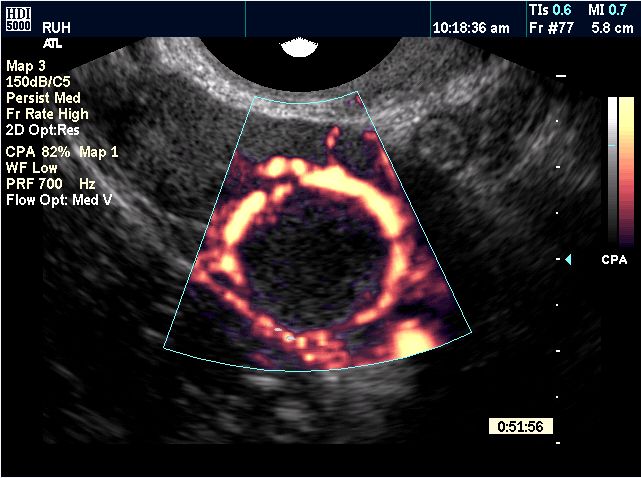 Fig. 5. Power flow Doppler image of a mature, mid-cycle luteal gland demonstrating marked periluteal vascular flow.
Fig. 5. Power flow Doppler image of a mature, mid-cycle luteal gland demonstrating marked periluteal vascular flow.
The corpus luteum can be recognized when the former “follicle walls” meet after follicle fluid is released and appear as two thickened slightly hypoechoic parallel tissue interfaces. To identify the corpus luteum with ultrasonography clearly, the interface of the apposing “walls” can be traced to the point of rupture at the outer edge of the ovary during the first week following ovulation. The corpus luteum becomes increasingly hypoechoic and thicker, reflecting the increasing vascularity of this highly metabolic tissue. Neovascularization of the corpus luteum begins immediately after evacuation of follicle fluid and appears with ultrasonography within 48–72 hours as a vascular ring surrounding the developing luteal tissue. As the corpus luteum matures, the ring of vascularity becomes more prominent on color flow and power Doppler interrogation (Fig. 6A and B). The degree of vascular perfusion of the corpus luteum is also apparent when observing the gray scale image of the corpus luteum. Darker tissue is seen during luteogenesis and neovascularization, whereas progression to a lighter gray is seen during luteal regression.65 Both color flow Doppler and gray scale imaging are useful for the identification of the corpus luteum.
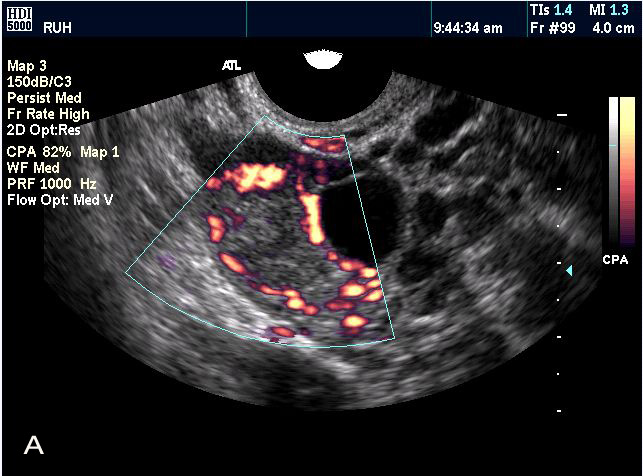 Fig. 6. Power (A) and color (B) flow Doppler images of recently ovulated follicles/new luteal glands on the day of ovulation.
Fig. 6. Power (A) and color (B) flow Doppler images of recently ovulated follicles/new luteal glands on the day of ovulation.
After the initial evacuation of the follicle fluid at ovulation, the corpus luteum can appear to refill with a hypoechoic or specular fluid so that the corpus luteum can appear to have an echoic central cystic cavity.61, 62, 65, 70 Detection of fluid within the cavity of a corpus luteum has been interpreted as a normal physiologic event related to either leakage of blood from the vascular follicle wall into the corpus luteum lumen following follicle rupture or extravasation of blood during luteogenesis. Fluid may be observed immediately following ovulation, and may subsequently decrease, remain, or increase in volume. The shape of a cystic area may vary from a thin line or ovoid shaped lumen to a round, cyst-like shape. The identity of a cystic corpus luteum can be confirmed as being distinct from a follicle by looking for the point of rupture on the external surface of the ovary during the first week after ovulation.65 After the point of rupture can no longer be identified, it may be difficult to differentiate between a cystic corpus luteum and an anovulatory follicle. Hence the easiest time to identify a corpus luteum is shortly after ovulation. Color flow Doppler ultrasonography can confirm greater vascular flow within the corpus luteum wall compared to the vascularity expected for a preovulatory follicle. When blood fills the corpus luteum lumen, the cystic corpus luteum is regarded as a corpus hemorrhagicum (Fig. 7).71 Blood cells, clot, protein, and cellular debris in the fluid of the corpus hemorrhagicum may lend a variable hyperechocity to the fluid-filled lumen.65, 67
 Fig. 7. Corpus hemorrhagicum demonstrating thick walls of peripheral luteal tissue and a central hemorrhagic clot with an interspersed fibrin network.
Fig. 7. Corpus hemorrhagicum demonstrating thick walls of peripheral luteal tissue and a central hemorrhagic clot with an interspersed fibrin network.
Degradation of vascular flow accompanies luteolysis, the regression of the corpus luteum in the late luteal phase of each menstrual cycle, in the absence of conception. Similarly, the corpus luteum and its activity also regress after the luteal-placental shift in the second trimester of pregnancy.66, 72 Consideration of this endocrine gland is integral to the assessment of women with infertility because the corpus luteum plays a role in regulating folliculogenesis and establishing and maintaining pregnancy.67 The corpus luteum’s most important endocrine activity is the synthesis of progesterone, which in turn is believed to regulate uterine muscle quiescence and endometrial differentiation and to suppress endometrial proliferation and facilitate secretory activity. If conception occurs, trophoblastic proteins and other maternal recognition of pregnancy factors enable the corpus luteum to maintain progesterone synthesis.
A corpus luteum can be observed in the ovaries throughout the luteal phase of the ovarian/menstrual cycle. The corpus luteum will regress with the onset of the next menses without conception or will persist through the first trimester of pregnancy. Following luteal regression, the corpus albicans may be visualized until the time of subsequent ovulation (Fig. 8).65 Occasionally, several corpora albicanthae may be observed from previous menstrual cycles. The location of small follicles surrounding the regressing corpora albicanthea may the influence their visualization.
 Fig. 8. Corpus albicans resulting from regression of a luteal structure from a previous cycle. Corpus albicans are typically visualized as hyperechoic structures within the ovary and they may occasionally appear to be more pronounced owing to the presence of surrounding follicles.
Fig. 8. Corpus albicans resulting from regression of a luteal structure from a previous cycle. Corpus albicans are typically visualized as hyperechoic structures within the ovary and they may occasionally appear to be more pronounced owing to the presence of surrounding follicles.
PROCESS AND RATIONALE FOR IDENTIFYING THE CORPUS LUTEUM
Examinations to confirm ovulation may help to clarify the etiology of infertility. A diagnosis of abnormal folliculogenesis and anovulation can direct the clinician to provide appropriate therapies such as ovulation induction or IVF. They may also help to provide an explanation for the etiology of infertility to the patients. An evaluation of ovulation in normative control patients and patients with idiopathic infertility has shown flaws in ovulation and luteogenesis.64, 65, 67, 69 Clinicians need to learn to identify the ultrasonographic characteristics of ovulation and luteogenesis so that the corpus luteum may be recognized in its various shapes and forms. The corpus luteum may be routinely identified in a clinical population by examining women with anticipated normal fertility potential. After the clinician has become adept at recognizing the corpus luteum, women with idiopathic infertility should be examined routinely to rule out flaws in ovulation and luteogenesis. The length of the luteal phase can be more carefully assessed when the date of ovulation has been confirmed with ultrasonography.
A skilled clinician can identify a recent ovulation (<24 hours) by confirming the site of rupture and tracing the rupture site to the apposed relatively avascular walls of the former follicle. At this stage, the echotexture of the corpus luteum tissue may not be markedly different from adjacent tissue, so identification of the point of rupture and wall apposition is important. It is imperative to distinguish between ovulation and dominant follicle regression because recent ovulation may prompt rapid insemination, whereas regression of a dominant follicle will prompt either further ovarian surveillance of follicle growth or initiation/change of ovulation induction therapy.
The corpus luteum undergoes marked neovascularity in the first 24 hours following ovulation. Color flow Doppler ultrasound can be used to demonstrate vascular flow, at a time when the point of rupture is still easily seen. In order to identify a cystic or hemorrhagic corpus luteum (corpus hemorrhagicum), the ovary should be examined within 1–3 days of ovulation to confirm that the point of rupture can be identified. The pressure from the cystic contents can give the cystic corpus luteum/corpus hemorrhagicum the appearance of thin walls and obscure the point of rupture later in the luteal phase. If a corpus luteum or corpus hemorrhagicum is suspected during high-resolution ultrasonographic examination but further confirmation is needed, a progesterone assay can verify whether a luteal phase level is present.62, 68, 73, 74 It may be difficult to recognize or confirm the presence of a corpus luteum without the availability of both high resolution transvaginal ultrasonography and color flow Doppler interrogation. It is important for clinicians to identify the corpus luteum routinely in women who are trying to conceive to verify the timing of sperm insemination, a normal luteal phase, and an absence of defects in folliculogenesis, so that ovarian etiologies for otherwise unexplained infertility can be ruled out.
Ovulation failure
It is important to recognize and diagnose the various forms of ovulatory failure and the ovarian pathology that can contribute to infertility. It is likely that there are many explanations for ovulation failure.
LUTEINIZED UNRUPTURED FOLLICLE
Transvaginal ultrasound has been used to describe the appearance of luteinized unruptured follicle (LUF) syndrome in detail.39, 40, 50 Following release of the preovulatory surge of LH, the preovulatory-size dominant follicle fails to rupture. This results in retention of the oocyte/cumulus complex is within the lumen of the LUF. The follicle wall thickens and attains gray scale and vascular features similar to luteal tissue (Fig. 9A and B). There is also a hazy indistinct border between the follicle fluid and the follicle wall. In addition, the point of follicle rupture, a characteristic that distinguishes the LUF from a cystic corpus luteum, is absent. Typically the mid-luteal progesterone concentration and basal body temperatures are lower than would be anticipated following normal ovulation. Menstrual flow does occur but menses are often lighter than usual. The mechanism for the formation of the LUF is uncertain and may include an ill-timed or attenuated release of the surge of LH or may be due to a defect in the follicle that makes it unresponsive to a normal LH surge such as aberrant or reduced receptors for LH.
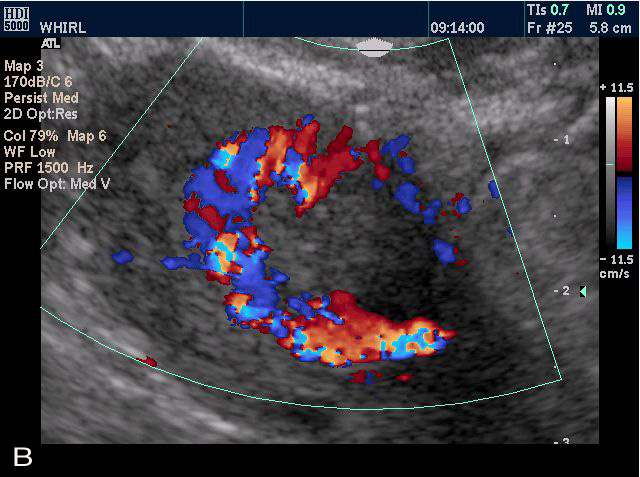
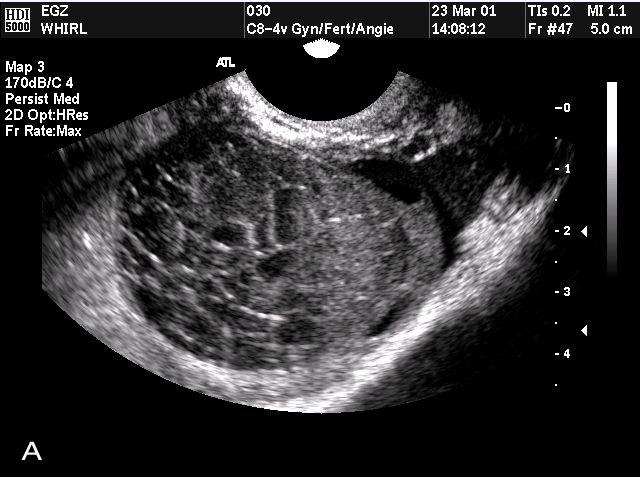 Fig. 9. Images from a woman who developed hemorrhagic anovulatory follicles during a study of natural cycle folliculogenesis and ovulation (A, B). There is evidence of extravasated blood in the lumen of the structures and the walls are thin did not develop any visual evidence of luteinization. Progesterone levels were below those accepted as clinically normal.
Fig. 9. Images from a woman who developed hemorrhagic anovulatory follicles during a study of natural cycle folliculogenesis and ovulation (A, B). There is evidence of extravasated blood in the lumen of the structures and the walls are thin did not develop any visual evidence of luteinization. Progesterone levels were below those accepted as clinically normal.
PERSISTENT ANOVULATORY FOLLICLE
Infertility can also be associated with growth of a dominant follicle beyond a preovulatory diameter and subsequent formation of a large anovulatory follicle cyst.39 No luteinization of the follicle wall occurs and the follicle wall is thin and displays marked hyperechocity (Fig. 10A). The follicular fluid remains clear/hypoechoic. Delamination of granulosa cells from the follicle wall can be observed on occasion. Cellular debris can be recognized as hyperechoic cellular debris floating within the follicle fluid (Fig. 10B). Follicle cysts remain static in diameter for one to many days before regression. It is presumed that anovulatory follicles continue to produce estrogen, which maintains endometrial growth. A decline in estrogen production with regression/atresia of an anovulatory follicle results in menstruation. A diagnosis of anovulation may be missed when the onset of menstruation coincides with a woman’s typical cycle length. Hence the duration of growth and regression of the anovulatory follicle may mimic a woman’s typical menstrual cycle length and menstruation will occur at an expected time. The onset of menses will mask anovulation unless ultrasonography has been used.
 Fig. 10. Failure of ovulation and development of “cystic” follicle. The follicle typically grows larger than the mean preovulatory follicle diameter of 23 mm, thin atretic follicle walls are observed and small flecks of particulate matter are frequently seen in the lumen or aggregated at the side of the structure.
Fig. 10. Failure of ovulation and development of “cystic” follicle. The follicle typically grows larger than the mean preovulatory follicle diameter of 23 mm, thin atretic follicle walls are observed and small flecks of particulate matter are frequently seen in the lumen or aggregated at the side of the structure.
Anovulatory follicles may continue growing to enlarged diameters. Menses would be expected to be delayed for as long as follicle regression fails to occur. A delay in the onset of menses and a negative pregnancy test can prompt a clinician to complete an ultrasound examination that will result in the visualization of an enlarged anovulatory follicle. In some cases, an anovulatory follicle will contain blood within the follicle lumen. Extravasation of blood from the capillaries of the follicle wall may give the follicular fluid a scattered fine echoic pattern as blood cells float or sediment in layers within the follicle lumen. This structure is referred to as a hemorrhagic anovulatory follicle. A hemorrhagic anovulatory follicle has thin bright walls and the luteal appearance of a LUF is absent (Fig. 11). Typically large anovulatory follicles regress spontaneously and rarely require further management.
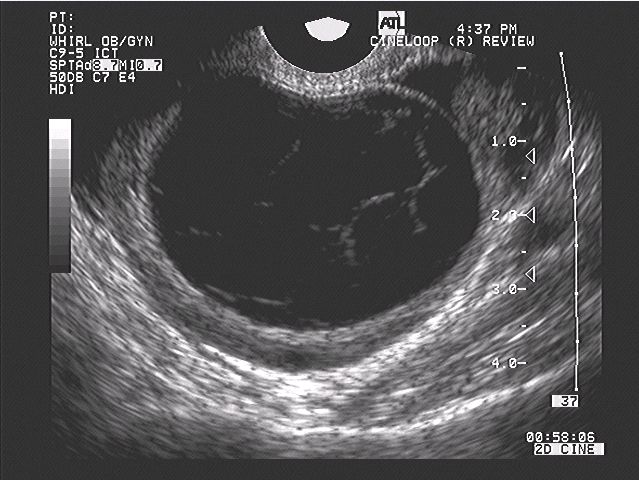 Fig. 11. Image of a hemorrhagic anovulatory follicle. Extravasated blood and an interspersed fibrin network are observed within the lumen. The walls of this structure are thin, echoic, and do not have the appearance of luteal tissue.
Fig. 11. Image of a hemorrhagic anovulatory follicle. Extravasated blood and an interspersed fibrin network are observed within the lumen. The walls of this structure are thin, echoic, and do not have the appearance of luteal tissue.
OTHER REASONS FOR ANOVULATION
Anovulation may result from many pathophysiological processes including hypothalamic suppression, polycystic ovary syndrome (PCOS), and endometriosis. Hypothalamic suppression may be idiopathic, acquired (with anorexia nervosa and exercise induced amenorrhea) or genetic (Kallman's syndrome). In cases of hypothalamic suppression, low levels of follicle stimulating hormone (FSH) and LH result in the absence of new follicle growth. Typically, the ovaries appear smaller than expected because of the absence of growing antral follicles and reduced stromal volume. Women with PCOS often may have anovulation and amenorrhea coexist. Numerous (more than 12 per ovary) small follicles 10 mm in diameter or less will be observed. The ovarian stroma appears abundant and slightly hyperechoic. The ovarian volume is increased due to an increase in the total number of follicles and stromal volume.The coexistence of endometriosis and anovulation may be diagnosed by the presence of ovarian endometrioma. Aberrant folliculogenesis may accompany endometriosis particularly when it resides in the ovaries. An endometrioma is recognized as a persistent ovarian cyst of variable size with a homogeneous hyperechoic and luminal fluid. The gray scale values of the luminal fluid of an endometrioma will vary with the thickness and water content of the cellular debris.
The possibility of an endometrioma and a dermoid/cystic teratoma should be considered when exploring the reason for a persistent ovarian cyst with hyperechoic luminal contents. A dermoid cyst is variable in its presentation such that it may mimic a simple cyst, an endometrioma or it may take on the appearance of a complex cystic-solid structure with or without hyperechoic calcified areas, due to the multiple tissue components typical of this common benign germ cell tumor. Careful surveillance of the ovary should be repeated for persistent ovarian cysts to determine whether there is spontaneous regression or to initiate a plan for appropriate medical and surgical intervention.
BENIGN OVARIAN NEOPLASIA
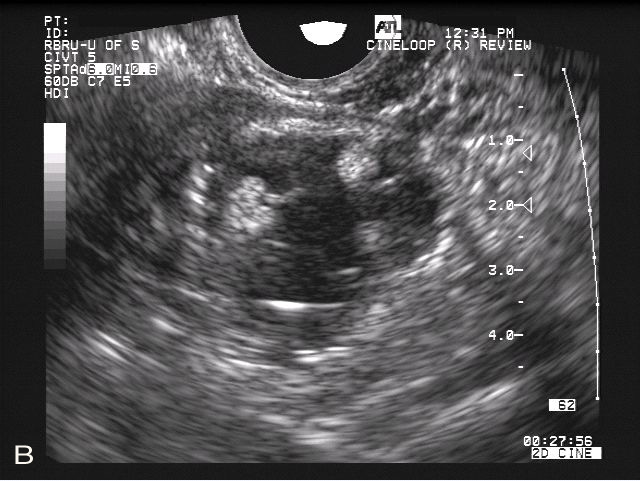
Benign cystic teratomas (dermoid cysts) are the most common germ cell tumor seen in women of reproductive age.75, 76 Frequently, the germ cell tissue develops into fully differentiated dermal tissue; hence it is often referred to as a “dermoid cyst” after its histological origin. It is common to find fat, epidermal glands with mucinous or serous fluid secretions, teeth or calcified tissue, hair, and even thyroid tissue comprising parts of the mass (Fig. 12A and B). Dermoid cysts should be diagnosed and excised in order to prevent cyst rupture.77 Dissemination of the mucin-containing luminal fluid has been known to cause profound chemical peritonitis.78, 79, 80 Ovarian torsion also is associated with ovarian enlargement due to dermoid cysts.77 This benign tumor is often seen bilaterally, and may be present in both ovaries concurrently. Dermoids vary in size at the time of presentation and multiple dermoid tumors may be found within the same ovary. Less than 1% undergo malignant degeneration.81 However, because of their unique presentation as complex cystic/solid masses, they may be mistaken for malignant disease in women of reproductive age.
 Fig. 12. Images of a small intraovarian dermoid cyst (A, B). The cyst is completely embedded in the ovary and is surrounded by focal areas of hyperechoicity. Small follicles are observed in the surrounding stroma. Folliculogenesis and ovulation were impaired in this ovary. The contralateral ovary demonstrated compensatory hypertrophy.
Fig. 12. Images of a small intraovarian dermoid cyst (A, B). The cyst is completely embedded in the ovary and is surrounded by focal areas of hyperechoicity. Small follicles are observed in the surrounding stroma. Folliculogenesis and ovulation were impaired in this ovary. The contralateral ovary demonstrated compensatory hypertrophy.
Ultrasonographic characteristics of benign cystic teratomas are not consistent because of the variability of tissues that may comprise them.82, 83 They may present as simple ovarian cysts with a hypoechoic cyst lumen or the luminal echotexture may be homogenous and specular with varying gray scale values as would be seen with viscous fluids such as mucin or old blood in a mucinous cystadenoma or an endometrioma. Solid tissue exhibits image characteristics similar to well-differentiated tissues, so a dermoid may appear cystic and solid. Other well-differentiated tissues such as bone or teeth will show the characteristic blockage of ultrasound wave transmission and refraction, respectively. Rapid enlargement due to an increase of luminal epithelial gland secretions into the cyst lumen may be observed following repeat assessments. Alternatively, dermoid structures may remain at a static small size for months to years. Lesions less than 5 cm have substantially less likelihood for malignancy.84
Dermoid cysts may be completely embedded within the ovary and may not be detected at laparoscopy or laparotomy, but may be visualized with ultrasonography (Fig. 12A). Doppler flow imaging studies have shown that vascular flow was detectable in only 24% of women diagnosed with a dermoid cyst.85 Dermoids commonly present in reproductive years, thus it is not uncommon to encounter them during the investigation and management of infertility patients. Careful observation with ultrasonography and with contrast enhancement will provide clues that may distinguish this pathology from sinister, poorly differentiated neoplasia and other benign conditions, so that the most appropriate and timely management can be executed.86, 87, 88
OVARIAN ENDOMETRIOMA
An estimated 10–25% of women are affected by endometriosis, a common benign gynecological affliction. Endometriosis is found in approximately 40% of women who present with infertility.89, 90 Endometriosis is comprised of implants of functional endometrium-like tissue that can be found on peritoneal surfaces of the reproductive organs, pelvis, and abdomen. The clinical presentation of endometriosis may be highly variable. Superficial, small implants, plaques or nodules do not appear to impair the mobility or movement of the fallopian tubes and ovaries. However, severe scarring and agglutination of the ovaries and oviducts by deep endometriosis implants may impair or prevent oocyte release and/or transfer to an oviduct.
Endometriomas are fluid-filled cysts that typically contain a “chocolate” colored fluid that is presumed to arise from sequestered menstrual effluent. Single or multiple endometrioma may be contained within one or both ovaries. Gray scale image characteristics may differ among endometriomas because the fluid compartment may vary in viscosity and cellular debris content. Typically, a homogenous granular-appearing echo texture of low amplitude is seen (Fig. 13A and B). Occasionally, wave-like motion, movement or swirling of the cyst contents may be visualized. It is useful to evaluate the ultrasonographic characteristics of persistent ovarian masses in order to differentiate an endometrioma from a dermoid cyst.
 Fig. 13. Images of ovarian endometrioma (A, B). The structure is hypoechoic and exhibits low amplitude uniformly distributed echotexture in the cavities of the cysts.
Fig. 13. Images of ovarian endometrioma (A, B). The structure is hypoechoic and exhibits low amplitude uniformly distributed echotexture in the cavities of the cysts.

The American Society of Reproductive Medicine has formulated diagnostic criteria for minimal to severe endometriosis to aid in standardized description of the types and locations of implants and associated scar tissue.91 It is hoped that standardization will direct research and management and lead to more focused results in evaluating the efficacy of various interventions. Pelvic pain may occur in women with minimal to severe disease; however, pain cannot be used to predict the amount or location of endometriosis implants. Severe pain may be present with minimal endometriosis and minimal or no pain may coexist with severe endometriosis. Only large implants on the ovaries that develop into endometriomas can be visualized reliably with ultrasonography.
Fertility potential is impaired when endometriosis distorts the oviducts and ovaries. However, the mechanisms by which endometriosis might lead to infertility are unclear. Minimal endometriosis does not involve either oviducts or ovaries. Ovarian endometriomas are believed to compromise fertility by disrupting folliculogenesis and ovulation, although the mechanism has not yet been elucidated. Management of endometriosis varies from medical therapy that involves continuous progestin use or suppression of estrogen stimulation of the endometriosis tissue. Neither therapy is amenable to concurrent fertility treatment. New medical therapy modalities including recombinant interleukin-2 combined with chronic gonadotropin releasing hormone (GnRH) analogue therapy appear promising and able to be combined with ART.92, 93 Surgical management may include thermal or laser ablation of implants with or without excision of implants.
Surgical intervention is considered conservative when reproductive potential is desired and maintaining the integrity of the ovary and oviduct are goals of therapy. However, complete surgical removal/ablation of endometriomas may result in damage to the ovary and/or adjacent oviduct and may impair ovarian function. Some clinicians have favored less aggressive surgical approaches and relied upon ultrasound-guided aspiration of endometriomas when IVF is anticipated.94 Ultrasonographic assessment of women with endometriosis should include comments about the position of the ovary and endometrioma relative to the position of adjacent reproductive structures and proximity to the cul-de-sac and bowel. It is helpful to determine whether a safe aspiration tract that would avoid bowel and major vessels can be made and whether the uterus lies between the upper vagina and an ovarian endometrioma when ultrasound-guided drainage of an endometrioma from a vaginal approach is anticipated.
OTHER BENIGN NEOPLASTIC OVARIAN MASSES
Ovarian fibromas are not encountered commonly, but present as a solid mid- gray scale ovarian mass. A cystadenoma may have a thick echogenic walls with clear to mucin-containing cyst contents. Cystadenomas may have both solid and cystic components and range markedly in size. However, they lack the vascular flow patterns seen in malignant lesions of the ovary. Contrast enhancement ultrasonography holds promise in differentiating between malignant and benign ovarian masses.87 Ultrasonography is an excellent modality to evaluate change in the size and characteristics of an ovarian mass over time.87, 88, 95 However, it must be emphasized that ultrasound imaging cannot take the place of histopathology to rule out malignant lesions.
Assessment of ovarian reserve
Predicting fertility potential has become important as women seek to use costly assisted reproductive technologies. This has become more critical as women attempt to conceive when they are older and less fertile.93, 96, 97, 98, 99 The term “ovarian reserve” has been used to describe the capacity of ovaries to respond to stimulation with gonadotropins and therefore predict fertility potential.100 Ultrasonography, endocrine tests, clomiphene citrate challenge tests, and GnRH agonist stimulation tests all have been used to predict the "ovarian reserve". Each of these methods attempts to determine whether the capacity to conceive is present from the perspective of ovarian function to predict the response to fertility therapy and plan the most efficacious and safe therapy.
THE ANTRAL FOLLICLE COUNT
Ultrasonography is routinely used to evaluate ovarian follicle number as a means to estimate ovarian reserve in women. A marked reduction in the number of antral follicles and the change of ovarian volume resulting from a decline in follicles may raise the suspicion for or confirm early ovarian failure.101, 102, 103, 104 Antral follicle counts may be estimated at specific times of the menstrual cycle and correlated to gonadotropin therapy responsiveness, either alone, or combined with IVF therapy.105, 106, 107, 108 A decreased ovarian reserve, reflected by low antral follicle counts has been used to predict a poor response to ovarian stimulation.104, 105, 106, 109, 110, 111, 112, 113, 114 Counts done between day 3 and 7 after menstruation have been used to predict how many follicles will develop with ovarian stimulation.104, 106, 109, 113, 114 A higher probability of poor ovarian stimulation occurred when women had fewer than five follicles under 10 mm in diameter prior to the onset of therapy.114 As women age, there is a gradual decline in the number of ovarian follicles and responsiveness to gonadotropin stimulation. A wide individual variation in ovarian response to exogenous gonadotropin stimulation occurs in women of advanced reproductive age.8, 96, 100, 102, 112
It remains unclear whether the probability of oocyte fertilization and pregnancy can be estimated by assessing the ovarian reserve with antral follicle counts. The capacity of an oocyte to be fertilized in older women has not been predicted solely by the age-related decline in antral follicle number.96, 100, 112 Some young women with low antral follicle counts and poor responsiveness to stimulation have a higher IVF conception rate than the rate of conception seen in older poor responders. A lower age-related risk for aneuploidy may contribute to the higher IVF conception rate observed in younger poor responders.96 While low antral follicle counts signal a poorer response to ovarian stimulation, additional predictors of ovarian reserve are needed to identify which oocyte has the capacity to be fertilized and progress to clinical pregnancy following ART.100
OVARIAN RESERVE AND HYPOTHALAMIC SUPPRESSION
Low antral follicle counts can alternatively signal hypothalamic suppression. Hypothalamic suppression is seen in women with Kallman’s syndrome, excessive exercise, stress, and anorexia nervosa. Women who have reduced follicle counts because there is no baseline endogenous stimulation of follicle growth tend to have an age-related response to stimulation and IVF once ovarian stimulation is initiated.
OVARIAN VOLUME AS A PREDICTOR OF OVARIAN RESERVE
Ovarian volume has been explored with two- and three-dimensional ultrasonography to quantitate ovarian reserve. The idea was that volume was believed to be dependent upon follicle number.102, 105, 107, 109, 110, 115 The decline in antral follicle counts has been directly correlated with a decline in ovarian volume with advancing age.100, 107, 108, 102 Decreased ovarian volume and absence of ovarian follicle activity has been observed in women with premature ovarian failure (POF) and hypothalamic suppression. The ovarian characteristics seen in POF and hypothalamic suppression are similar to those observed in menopause (Fig. 14). Ovarian volume can be used as an estimate of ovarian reserve and to predict ovarian responsiveness to stimulation and conception after hypothalamic suppression has been excluded.8, 96, 102, 116, 114
 Fig. 14. Image from a woman in premature ovarian failure. Only the stroma of the ovary is identified. A very few follicles of less than 1 mm diameter can be observed on the inferior aspect of the ovary.
Fig. 14. Image from a woman in premature ovarian failure. Only the stroma of the ovary is identified. A very few follicles of less than 1 mm diameter can be observed on the inferior aspect of the ovary.
ENDOCRINE TESTS OF OVARIAN RESERVE
Endocrine tests have been used to assess ovarian reserve.8, 96, 97, 99, 100, 101, 105, 108, 114, 115, 116 Day 3 FSH levels and antral follicle counts have been correlated with responsiveness to ovarian stimulation.8, 99, 104, 107, 108, 114, 115, 116 The poor response to ovarian stimulation with gonadotropins observed with decreased antral follicle counts tends to be accompanied by a rise in basal FSH levels and elevation of day 3 FSH levels is apparent with advancing age.96, 99, 100, 104, 108, 111, 112, 114 The elucidation of the wave model of human folliculogenesis has generated questions about the best time to assess an endocrine marker of ovarian reserve as multiple waves within a single menstrual cycle will have multiple FSH waves.14, 101 Other markers such as inhibin A and B, and mullerian inhibiting factor also show promise as predictors of ovarian reserve that may be superior to FSH assessments.101, 104, 106, 112, 115, 116 The clomiphene citrate challenge test and the GnRH stimulation test have also been explored as tests of ovarian reserve.99, 100, 101, 104, 115 Further work is required before clinicians can use an ovarian reserve test or apply multiple tests reliably to predict women's response to therapy and their probability of conception with or without ART therapy because none of the current markers of ovarian reserve have been independently predictive of ovarian response and conception.
INCREASED OVARIAN FOLLICLE NUMBER AND OVARIAN RESERVE
The observation of increased follicle number in women diagnosed with PCOS has generated some controversy about the use of follicle counts to reflect ovarian reserve. Follicle number is one of three diagnostic criteria for PCOS according to the 2003 Rotterdam consensus.117 Polycystic ovaries are identified when an antral follicle count is increased. Polycystic ovaries have been documented in women with elevated androgen levels due to PCOS, congenital adrenal hyperplasia (CAH) and in women receiving androgen therapy as a part of transgender sex reassignment.118 Polycystic ovaries have also been documented in some women with hyperprolactinemia, hypothalamic suppression, and in early adolescence prior to the onset of regular ovulation.
The risk for ovarian hyperstimulation and OHSS following induction of ovulation with exogenous gonadotropins is increased in women with PCOS and CAH. This observation supports the hypothesis that an increased follicle population is correlated with an increased responsiveness to ovarian stimulation. Little is known about age related changes of the polycystic ovary. It may be inappropriate to relate a decline in fertility potential to follicle number when the follicle population is originally increased because of an altered endocrine state. Women with increased follicle number may appear to have “normal”, neither increased nor decreased, antral follicle number at the time of physiological decline due to perimenopause. It is not known whether fertility potential is retained at an advanced reproductive age when women are stimulated with gonadotropins if their follicle counts decline from elevated to “normal” range. Similarly, if follicles can be stimulated to grow, it is not known whether the oocytes are competent to be fertilized and develop into healthy pregnancies. Neither is it known whether women of advanced reproductive age retain fertility potential when stimulated with gonadotropins at the time of decline from “increased” to “normal” antral follicle number. Hence, the use of follicle number to predict a reserve in fertility potential may apply only to the nonandrogenized, nonPCOS/nonCAH population until more investigation is completed.
Uses of ovarian ultrasonography in guiding infertility therapy
DETERMINING OPTIMAL TIMING FOR INSEMINATION AND PREDICTING OVULATION
The optimal time to schedule intercourse or perform an intrauterine insemination (IUI) in spontaneous and stimulated cycles can be estimated with ultrasound monitoring of the dominant follicle. Detailed ultrasound-based studies of preovulatory follicle growth rates have given us the ability to estimate the interval to ovulation from different preovulatory follicle diameters.14, 15, 21, 120, 121 Preovulatory follicles grow at approximately 1.6 mm per day during natural menstrual cycles and 1.8 mm per day during ovarian stimulation cycles. The mean diameter on the day prior to ovulation is 21.7 mm for natural cycles and similar preovulatory follicle diameters are observed in stimulation cycles.120, 121
Intrauterine insemination (IUI) is a simple, yet costly, procedure used to ensure that sufficient numbers of sperm are available at the time of ovulation. It is indicated to overcome sperm factors such as oligospermia, use of cryopreserved sperm or to synchronize insemination with ovulation. An IUI is typically scheduled on the same day as a positive urine test for the LH surge; however, the test cannot ensure whether ovulation has just occurred or will occur within 24 hours. Consequently scheduling of the IUI can be very hurried for the recipient and physician. Couples and their physicians find it more convenient to use ultrasonography to estimate when ovulation would be expected to plan insemination therapy or sexual activity. It is therefore imperative to ensure the most effective and efficient prediction of ovulation for IUI therapy. Definitive studies in equine animal model have been undertaken that effectively estimate the interval to ovulation, but similar data are not currently available in humans. However, data from human folliculogenesis studies and evidence from experimental animals can be used to presume that ovulation and timing of insemination procedures may be easily calculated.14, 15, 28, 120, 121, 122
Predicting the time of ovulation using ultrasonography is superior to the analysis of basal body temperature (BBT) charting or use of urinary luteinizing hormone (LH) assays. Typically, a BBT is used retrospectively to predict when ovulation may occur in subsequent menstrual cycles. Sexual activity is planned in advance of ovulation and is not required for conception following ovulation when the basal temperature rise indicative of luteal production of progesterone is appreciated. However, BBT interpretation is very subjective and cannot be relied upon to confirm the exact time of ovulation. More precise estimates of the date of ovulation are required when costly IUI of sperm is indicated.
ANALYSIS OF OVARIAN VASCULARITY IN THE EVALUATION AND THERAPIES FOR INFERTILITY
The ovarian vascular supply may be visualized as the vessels enter the ovarian hilus. Spectral Doppler studies have demonstrated lower resistance to blood flow in the ovary containing a preovulatory follicle or corpus luteum compared with the contralateral ovary. The highest resistance to blood flow was observed on day 1 of menses, whereas the lowest resistance occurred on the day of LH peak (surge).123 A clear relationship between the uterine and ovarian vascular indices with reproductive hormones, estradiol, progesterone, and others was not identified in a subsequent study.124 Further research is needed to address how vascularity and echotextural indices can be used together to predict the location and time of ovulation accurately and the probability that the oocyte released will be competent to develop into a clinical pregnancy.
Ovarian blood flow during ovarian stimulation has been evaluated to investigate an association between the vascular patterns and IVF outcomes prior to IVF oocyte retrieval using color flow and power flow Doppler interrogation in two- and three-dimensional ultrasonography.42, 52, 125, 126, 127, 128 In an initial study, peak velocity and resistive indices decreased as the diameter of follicles increased which was interpreted to mean that follicles become more vascular as they approach ovulation. Even with this evidence, the vascular indices were not able to be used to predict the IVF outcome for the follicles.125 However, it has been demonstrated that the vascular indices of follicles could be used to predict clinical outcomes during assisted reproduction cycles.42, 52, 126, 127 A strong correlation was observed between the level of follicular vascularity and oocyte recovery rates, thus it has been suggested that follicular blood flow may signal the appropriate time for hCG administration that will optimize oocyte recovery.45, 46, 127, 129
Vascular analysis of the ovary can be used during entire menstrual cycles and provide a rich source of information. Color Doppler may be used during serial examinations of the follicle wall to predict the reproductive potential of growing follicles. During the first 24 hours after ovulation, the corpus luteum is initially avascular, but neovascularization occurs quickly. Thereafter, the corpus luteum progressively increases in vascular activity in parallel with marked hormone production by the corpus luteum, especially progesterone. If a clinician completes surgery postovulation and encounters a corpus luteum, the marked vascularity appreciated with Doppler ultrasonography can be demonstrated. Marked bleeding of the corpus luteum will occur following instrumentation of the highly vascular tissue; hence, utmost care is taken when handling the postovulation ovary at surgery. Conversely, Doppler analysis of a corpus luteum can be used to demonstrate regression by reduced vascular flow when conception has not occurred even before menses has begun. The corpus luteum of pregnancy has a marked increase in vascular activity. It is therefore surprising that vascular activity has not been explored routinely and established as a part of daily clinical care when evaluating follicle growth and ovulation.
Polycystic ovary syndrome and infertility
DIAGNOSIS OF POLYCYSTIC OVARY SYNDROME
Polycystic ovary syndrome (PCOS) has been reported in 6–10% of women; however, its prevalence is likely underestimated because of the confusion surrounding recognition of this broad spectrum metabolic syndrome.130 Initially, PCOS was recognized in women who had a cluster of symptoms and signs, including obesity, infertility, hirsutism and severe menstrual irregularities, prolonged amenorrhea, and dysfunctional uterine bleeding. Myriad tests and hormonal ratios have arisen but no simple symptom complex or laboratory test has been universally sufficient to define PCOS. In 1990, the National Institute of Health criteria included androgen excess and anovulation/irregular menses to diagnose PCOS. As of 2003, the Rotterdam consensus required two of three criteria for diagnosis: polycystic ovaries, androgen excess, and menstrual irregularity. Ultrasound examination was needed to identify polycystic ovaries. The newer criteria provided a more flexible means to diagnose PCOS and supported the recognition of a number of PCOS phenotypes. However, some women have been diagnosed without having polycystic ovaries and others do not express the hyperandrogenism that appeared integral to the syndrome in the past; still others ovulate regularly and have normal fertility. The new criteria widened the opportunity for clinicians to make a diagnosis of PCOS in many more women, although it has also caused the phenotype to become very variable and an underlying cause remains elusive. Discussion on the merits of classification of PCOS on the basis of endocrine and metabolic criteria versus ultrasound criteria is ongoing.131, 132, 133, 134
The consequences of PCOS are so diverse that it is important to recognize PCOS early to initiate health prevention strategies.6, 132, 135, 136, 137, 138, 139, 140 Women with PCOS are at greater risk of developing diabetes, metabolic syndrome, uterine and breast cancer, and risk factors for heart disease. Familial inheritance has been documented in both male and female relatives, and it is likely that men who carry the genetic traits can pass them to female offspring and develop metabolic syndrome and heart disease themselves. Hyperinsulinemia is expressed by some but not all with PCOS and there are likely multifactorial genetic traits that contribute to PCOS that will explain the differences in presentation and severity of symptoms.130 Fetal imprinting is an attractive theoretical initiator for PCOS. PCOS has been induced in offspring who are exposed to androgens during fetal life in animal models. Childhood obesity was reduced in offspring whose mothers were able to apply strict glucose control and weight gain during gestation.141, 142, 143, 144, 145 The concept that there is a genetic change that occurs as a result of fetal imprinting and exposure to a specific fetal environment that may influence metabolism and the expression of obesity in offspring makes it even more important to diagnose and control PCOS prior to conception and early in life to prevent late onset diseases.
Polycystic ovary syndrome is often not recognized because of the broad spectrum of clinical presentations until women seek help from a reproductive endocrinologist for infertility.131, 132, 140 When hirsutism and anovulation/amenorrhea are present, PCOS may be recognized. However, the diagnosis may be overlooked in women who have less pronounced symptoms and signs. The ultrasound appearance of polycystic ovaries with the classical "string of pearls" may be the feature that makes the diagnosis of PCOS worth considering and the ultrasonographic morphology of polycystic ovaries may be recognized in most women with PCOS (Fig. 15). However, some women with the metabolic disorder may have normally appearing ovaries and some women with profoundly polycystic ovaries on ultrasound examination may not express the endocrine/metabolic phenotype seen with PCOS.133, 140
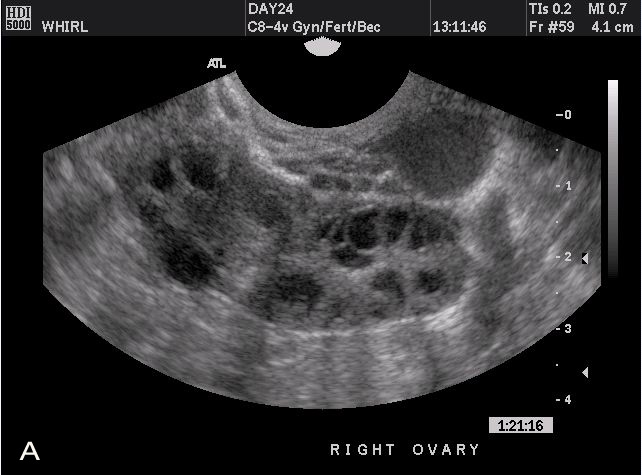 Fig. 15. Images from women with differing expressions of the four major subtypes of the metabolic syndrome associated with polycystic ovary syndrome (A–D). The images exhibit quite differing ultrasonographic appearances in the size and distribution of follicles within PCOS ovaries. A recent corpus luteum is clearly visible in the ovary in panel (D).
Fig. 15. Images from women with differing expressions of the four major subtypes of the metabolic syndrome associated with polycystic ovary syndrome (A–D). The images exhibit quite differing ultrasonographic appearances in the size and distribution of follicles within PCOS ovaries. A recent corpus luteum is clearly visible in the ovary in panel (D).



DEFINING POLYCYSTIC OVARY MORPHOLOGY BY ULTRASONOGRAPHY
An ultrasound examination is the gold standard for detecting/diagnosing polycystic ovaries. Developing a standardized definition that describes the appearance of polycystic ovaries adequately has been challenging.146 Descriptions have focused on stromal echogenicity, ovarian volume, and follicle numbers.133, 146 The criteria developed in 2000 included an ovarian volume of more than 9 cm3, more than 10 follicles between 2 and 8 mm, and increased stromal echogenicity.133 In 2003, the criteria were adapted to include an increased ovarian stroma of more than 5.5 cm² or a volume more than 11 cm3 and/or detection of more than 12 follicles between 2 and 9 mm diameter (mean of both ovaries).147 The Rotterdam consensus workshop set diagnostic criteria for PCOS which included ultrasound-based criteria for polycystic ovaries.148 The 2003, definition for polycystic ovaries was abbreviated by the committee to 12 or more follicles measuring 2–9 mm and/or an ovarian volume of more than 10 cm3.148
OVULATION INDUCTION IN WOMEN WITH PCOS
Women with PCOS are challenging when induction of ovulation is the best therapeutic approach. Numerous investigators have emphasized the benefits that arise from nutritional and exercise-based lifestyle modifications focused upon decreasing hyperinsulinemia and body mass index (BMI). A weight loss of as little as 5% has been shown to result in spontaneous ovulation. However, it is typically difficult to motivate women to achieve these goals. Insulin sensitizers, such as metformin, may be used to assist some women to begin ovulating regularly and maintain regular menses; although, most women may require 4–6 months therapy to induce regular ovulation.149, 150, 151, 152, 153, 154, 155
OVULATION INDUCTION AGENTS FOR WOMEN WITH PCOS
Clomiphene citrate, gonadotropins, and GnRH agonists are readily used with ultrasound monitoring of follicle growth and ovulation.156, 157, 158, 159 Ovulation induction medications impose many risks to women with PCOS including multiple ovulation, multifetal gestation, and ovarian hyperstimulation syndrome (OHSS). Consequently, ultrasonography is used to monitor the follicle response to these agents. Gonadotropin therapy is given if clomiphene citrate fails to induce ovulation and/or conception. Gonadotropins are more costly, time consuming, and impose greater risk than clomiphene citrate. Some women with PCOS will exhibit an exaggerated response to even the smallest doses of recombinant FSH and some will benefit from IVF rescue to prevent multiple ovulation, conception, and OHSS.6, 156, 160 It has been shown that combining metformin with clomiphene citrate or gonadotropins has made substantial therapeutic improvements.152, 154 Metformin appears to be responsible for increasing the rate of ovulation while decreasing the dosage of and time required for FSH induction of ovulation. An increased rate of conception decreased multiple pregnancy rates and decreased risk for OHSS are consequences of combining metformin with ovulation induction therapy. GnRH agonists have been suggested to prevent an unplanned LH surge and decrease the possibility of OHSS.161 Many investigators believe that the phenotype of the individuals with PCOS should be considered when determining which strategies will be best for ovulation induction and restoration of menstrual cyclicity.132, 149, 150, 151, 154, 156, 158, 160, 162
DIAGNOSTIC USE OF ULTRASONOGRAPHY IN INFERTILITY INVESTIGATIONS: THE OVIDUCT
Images of hydrosalpinx. Hydosalpinx is usually easily diagnosed as well-constrained fluid accumulation in the adnexae. In some cases, adhesions between the oviduct and ovary may be visualized.
Ultrasonographic visualization of the oviduct
The oviduct has tissue characteristics similar to adjacent bowel and may not be readily visualized. However, it is possible to locate and visualize the oviduct using anatomic principles. The oviducts can be traced by starting from their proximal origin at the uterine cornua (Fig. 16). The mesosalpinx lies parallel to each oviduct, contains the vascular network for each oviduct and can be identified using color flow Doppler interrogation. The fimbriae typically are not intimately attached to the mesosalpinx and can only be definitively identified when free fluid surrounds the infundibulum and helps to outline their delicate finger-like projections (Fig. 17). The oviduct and fimbria may be easily visualized within a fluid pocket following recent ovulation or small pockets of fluid may outline the lumen of the oviduct after an IUI or hysterosalpingogram. The entire length of the oviduct can usually be appreciated and the fimbria can be outlined during saline enhanced sonohysterography. It may be difficult, or impossible, to visualize an oviduct when loops of bowel distended with gas or intestinal contents are located between the ultrasound probe and the oviduct. It is often more difficult to visualize the left adnexa, especially if a woman has a high BMI, as fat lining large and small bowel impairs ultrasound wave transmission. Similarly, imaging is impaired when the uterus is acutely retroverted and the oviduct lies behind the uterus. However, a systematic review of the oviductal anatomy, proximally from the uterine cornuae, parallel to mesosalpingeal vessels, and distally around the ovaries will ensure the entire length of the oviducts is evaluated when searching for early ectopic pregnancies.
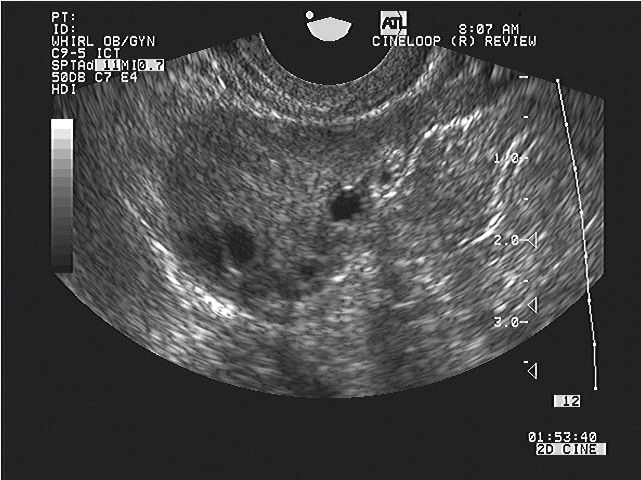 Fig.16. An image of an oviduct visualized from the uterine cornu to the fimbria. The ampulla, infundibulum and very fine interfaces representing the fimbria may be appreciated on the superior aspects of the ovaries.
Fig.16. An image of an oviduct visualized from the uterine cornu to the fimbria. The ampulla, infundibulum and very fine interfaces representing the fimbria may be appreciated on the superior aspects of the ovaries.
 Fig. 17. The fimbria of the oviduct are clearly visualized in free fluid surrounding the ovary following ovulation or hysterosalpinography.
Fig. 17. The fimbria of the oviduct are clearly visualized in free fluid surrounding the ovary following ovulation or hysterosalpinography.
OVIDUCTAL PATHOLOGY
Hydrosalpinges can be easily recognized with transvaginal ultrasonography.163 An oviduct that is dilated with fluid typically has long anechoic compartments in one plane that assume a roughly circular shape when visualized at 90° angles (Fig. 18). Dilated longitudinal (oviductal) fluid compartments can be traced from the uterine cornu, along the path of the mesosalpingeal vasculature, towards the ovaries. Color flow Doppler can help to identify the mesosalpinx and thereby locate the mid-portion of an abnormal oviduct. Some dilated anechoic areas may be outlined by septations or flower-like invaginations that have an appearance similar to bowel haustra. A small hydrosalpinx can be induced during sonohysterosalpingography or hysterosalpingography; the absence of a pre-procedure hydrosalpinx may indicate that there is a small opening at the fimbria that allows tubal fluid to drain and conveniently prevents pressure damage to the tubal luminal tissue. A randomized controlled clinical trial of women with hydrosalpinges diagnosed prior to IVF revealed that prophylactic salpingectomy or neosalpingostomy completed before IVF resulted in significantly increased pregnancy and live birth rates.164, 165 Hence, when a hydrosalpinx is recognized, neosalpingostomy with or without adnexa adhesiolysis or salpingectomy are recommended.
 Fig. 18. Images of hydrosalpinx (A, B). Hydrosalpinx is usually easily diagnosed as well-constrained fluid accumulation in the adnexae. In some cases, adhesions between the oviduct and ovary may be visualized.
Fig. 18. Images of hydrosalpinx (A, B). Hydrosalpinx is usually easily diagnosed as well-constrained fluid accumulation in the adnexae. In some cases, adhesions between the oviduct and ovary may be visualized.

Free fluid surrounding the oviduct and ovaries may sometimes allow visualization of peritubal and periovarian adhesions. Scar tissue may appear as hyperechoic foci and filmy strands of scar tissue may be outlined within adjacent fluid. Surgical exploration may be recommended to verify and treat tubo-ovarian adhesive disease that may impair fertility when hyperechoic foci are seen. The smooth surface of the oviduct may occasionally have irregularities or swellings that are indicative of scar tissue, endometriosis implants or salpingitis isthmica nodosum. Torsion of the oviduct is a rare pathological event that has been identified with ultrasound.166
DIAGNOSTIC USE OF ULTRASONOGRAPHY IN INFERTILITY INVESTIGATIONS: THE UTERUS
Uterine anatomy
The uterine body is comprised of myometrium enveloped in an outer thin, nonreactive layer of squamous epithelium called serosa and intracavitary glandular epithelium called endometrium. The cervix is attached to the uterine body and is composed of related, yet histologically distinct, tissues that include the endocervical glandular epithelium and squamous epithelium over the exocervix. The endometrium and myometrium respond to the reproductively active hormones, estrogen and progesterone, during the follicular and luteal phases of the menstrual cycle.
The endometrium
PROLIFERATION OF THE ENDOMETRIUM
During the reproductive years, the proliferative phase of menstrual cycles refers to estrogen-stimulated endometrial growth and proliferation. Estrogen production arises primarily from ovarian dominant follicle development prior to ovulation. However, estrogen also can be synthesized by the adrenal glands and adipose tissue, and in some disease states in hepatic tissue. Women with excess androgen secretion from untreated CAH or PCOS are not deficient in estrogen; adrenal and ovarian androgens are converted to estrogen in peripheral sites, primarily in adipose tissue. Even though ovarian activity is not the primary source of estrogen in women with CAH and PCOS, their endometrium responds to the estrogen by endometrial gland proliferation. The endometrium may also respond to exogenous estrogen prescribed as replacement therapy for premature ovarian failure, menopause, and hypothalamic suppression. Hence, regardless of the route by which estrogen is available, the uterus responds by endometrial proliferation.
POSTOVULATION ENDOMETRIUM
Endometrial proliferation is arrested after ovulation because progesterone secretion by the corpus luteum confers a different endometrial response. Under progesterone’s influence, endometrium stops proliferating. Endometrial glands branch extensively and differentiate into secretory tissue during the secretory or luteal phase of the cycle. The corpus luteum secretes primarily progesterone, although estrogen is also secreted in small amounts.167, 168, 169 If conception occurs, hormonal support for the endometrium is maintained by the corpus luteum until placental progesterone production begins.170 In the absence of conception, estrogen and progesterone decline as the corpus luteum regresses. Menstruation occurs with the loss of endometrial hormonal stimulation/support.
THE ENDOMETRIUM AS A HORMONAL BIOASSAY
Endometrial growth may be considered as a functional bioassay for ovarian hormonal activity and can be mapped with ultrasonography.27, 171, 172, 173, 174 During natural and ovarian stimulation cycles, the endometrium responds to the rising estrogen levels that accompany folliculogenesis. Following ovulation, or exogenous progesterone administration used routinely as luteal support during ART therapy, endometrial development may be mapped as it progresses from the proliferative to secretory phases. Exogenous hormones may be administered in some situations, such as cryopreserved embryo transfer or ovum donation IVF to induce endometrial proliferation and complete secretory changes to prepare the uterus for embryo implantation and pregnancy artificially. It is apparent that the uterus is a reactive tissue that rests in an atrophic state when hormones are withdrawn and responds when hormones are supplied because women who have entered menopause may receive exogenous hormones to prepare the uterus for embryo implantation.
The phase of the menstrual cycle can be estimated by examining endometrial patterns with ultrasonography (Fig. 19). Three distinct endometrial patterns are seen ultrasonographically during the follicular phase of the menstrual cycle. Immediately following menses, the endometrium displays an A pattern which is composed of a thin hyperechoic stripe of endometrial tissue. During the mid-to-late follicular phase, elevation in circulating estrogen results in differentiation of the stratum functionalis and basalis and gives rise to the B pattern endometrium in which two distinct layers of endometrium can be observed. The basalis remains hyperechoic while progressive darkening/hypoechocity of the stratum functionalis results in glandular proliferation reflecting the rise in estrogen. The C pattern is a triple stripe echotextural pattern. The stratum basalis remains somewhat hyperechoic while the adjacent functionalis layers develop more hypoechocity than in the B pattern. The interface of the two opposing functionalis layers creates a midline hyperechoic stripe. During the follicle phase of the menstrual cycle, a progressive increase in endometrial thickness accompanies the transformation from the A to B to C patterns in response to endometrial growth and differentiation. Following ovulation, the endometrium transforms to a D pattern. Growth and branching of the endometrial glands mediated by progesterone occurs and the endometrium becomes more hyperechoic and homogeneous, and continues to thicken during the luteal phase. Menstrual flow can be seen on ultrasonography and has been coined the M pattern.27, 172, 173, 175 Subtle endometrial contractions may be observed during the menstrual phase. Following menstruation, the stratum functionalis is diminished and the endometrium reassumes an A pattern.
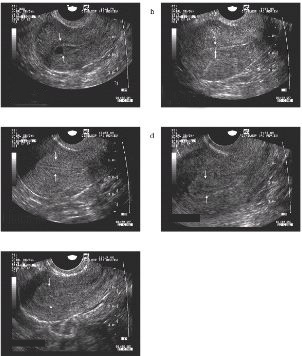 Fig. 19. Ultrasound images of the uterus taken in the mid-sagittal plane showing the five primary patterns of endometrial development (M, A–D). For orientation, the cervix is located just out of the image to the right of the image and the fundus is seen to the left of the image. (M pattern) Evidence of active menstrual bleeding is observed within the uterine lumen. (A pattern) A thin, simple hyperechoic single stripe is seen immediately following menstruation. (B pattern) Early follicular phase triple-line pattern indicative of increasing estradiol levels. (C pattern) Late follicular phase pronounced triple-line pattern with distinct separation of the stratum basalis and stratum functionalis is observed with the high estradiol levels associated with the periovulatory period. (D pattern) Postovulation heterogenous, fully secretory endometrial pattern indicative of luteinization and exposure of the endometrial tissues to progesterone. Arrows identify the stratum basalis-myometrium interface. (Reprinted with permission from Baerwald, Pierson. J Ultrasound Obstet Gynecol 2004;24:453-460.)
Fig. 19. Ultrasound images of the uterus taken in the mid-sagittal plane showing the five primary patterns of endometrial development (M, A–D). For orientation, the cervix is located just out of the image to the right of the image and the fundus is seen to the left of the image. (M pattern) Evidence of active menstrual bleeding is observed within the uterine lumen. (A pattern) A thin, simple hyperechoic single stripe is seen immediately following menstruation. (B pattern) Early follicular phase triple-line pattern indicative of increasing estradiol levels. (C pattern) Late follicular phase pronounced triple-line pattern with distinct separation of the stratum basalis and stratum functionalis is observed with the high estradiol levels associated with the periovulatory period. (D pattern) Postovulation heterogenous, fully secretory endometrial pattern indicative of luteinization and exposure of the endometrial tissues to progesterone. Arrows identify the stratum basalis-myometrium interface. (Reprinted with permission from Baerwald, Pierson. J Ultrasound Obstet Gynecol 2004;24:453-460.)
The morphological criteria used to define the endometrial echotextural changes have been correlated to circulating plasma estradiol levels. The endometrial patterns can be regarded as a functional bioassay. Each pattern is predictive of the estrogen and progesterone in circulation that occur in concert with the ovarian phases of folliculogenesis and luteogenesis.175, 176, 177 Hence, with ultrasonography clinicians can compare the phase-specific changes in ovarian follicle growth and ovulation with endometrial patterns to discern a cause for any discrepancy or unexpected phase mismatch. For example, the appearance of a dominant follicle at a diameter larger than appropriate for a preovulatory time combined with a thin, hyperechoic uterine endometrium signals low circulating levels of estradiol and would support a diagnosis of anovulation. The observation of C pattern endometrium in the absence of dominant follicles can alert a clinician to search for the site of recent ovulation. Conversely, a clinician may be prompted to investigate for endometrial pathology when marked endometrial thickening coexists with small follicle diameters of the early follicle phase. A mid-luteal endometrial thickness of more than 6 mm, typically at least 11 mm, is anticipated. The accuracy of ultrasonographic staging of the endometrium has been reported to be between 76% and 93% when considering classical histologic dating as the gold standard.175 Serial assessments to detect asynchronicity between the endometrial patterns and ovarian activity are useful to signal subtle defects in folliculogenesis and/or luteogenesis or aberrant endometrial growth. Early investigation into the nature of asynchronous growth and appropriate intervention can be prompted when the endometrium is used as a bioassay of ovarian hormone activity.
MEASURING THE ENDOMETRIUM
It is crucial to have a clear knowledge of the locations where measurements should be taken and an understanding about where calipers should be placed when measuring the thickness of the endometrium. Endometrial measurements should be done within 5–10 mm of the fundal aspect of the endometrial-myometrial interface with the uterus viewed in the mid-sagittal plane with the fundal aspect of the endometrium visible.27 A line is drawn perpendicular to the endometrial cavity from the myometrial-endometrial interface, across the endometrium, to the opposing endometrial–myometrial interface. Changes in the endometrial thickness during the menstrual cycle in clinically normal women are reflective of circulating levels of reproductively active hormones.27, 178, 179, 180
MYOMETRIUM
The myometrium does not appear to have easily identifiable ultrasonographic changes during the menstrual cycle in contrast with the numerous cyclic changes observed in the endometrium. The echotexture of the uterine body appears homogenous without cyclic changes. The vasculature can be easily defined within the broad ligament and is obviously prominent in women who have been pregnant. Progesterone mediates myometrial contractility quiescence, whereas progesterone withdrawal mediates increased myometrial contractility.181 The myometrium maintains volume and vascularity under the influence of estrogen, whereas the loss of estrogen results in a decline in myometrium volume that is restored if estrogen is made available again.
Congenital and acquired uterine abnormalities
Mullerian abnormalities of the uterus have been classified by the American Society of Reproductive Medicine in an attempt to standardize descriptions of the broad spectrum of anomalies seen in clinical practice (Fig. 20).182 High resolution transvaginal ultrasonography is valuable in diagnosing many uterine cavity anomalies. The types of anomalies include congenital anomalies, arcuate, unicornuate, bicornuate, and septate cavities as well as acquired intracavitary defects caused by uterine synechiae, polyps, and intracavitary fibroids.183, 184 Uterus didelphys can be demonstrated and is visualized as a complete duplication of two unicornuate uteri each with their own cervix. Uterus didelphys can be contrasted with a bicornuate uterus that has the appearance of two uterine cavities that join above a single cervix.185 Differentiating between septate and bicornuate uteri may also be challenging.185, 186 Both septate and bicornuate uteri have two upper uterine cavities that join with a single cavity above a single cervix. Transvaginal ultrasonography using sagittal/coronal imaging orientation will allow the identification of two endometrial cavities, at the right and left uterine cornu in both septate and bicornuate uteri. Occasionally there is a difference in size between the two cavities. The uterine horns coalesce with the central cavity as the uterus is imaged from the fundus towards the single cervix. The depth of the septum or the bicornuate uterine dimple determines the length of the horns and the single central cavity. Myometrium surrounds the endometrium within each horn of the bicornuate uterus. The myometrium may be readily apparent when the bicornuate uterus fuses with the central single endometrial cavity at a lower point in the uterus and less apparent when bicornuate cavities fuse closer to the fundus of the uterus. In the septate uterus, the myometrium is initially seen surrounding the uterine horns at the fundus. However, the myometrial tissue does not persist as a circular envelope around each horn as the uterus is imaged below the fundus. A layer of endometrium is present over the septum which gives the horns a similar appearance to the bicornuate uterine horns but the septum is observed medially between each apparent horn’s endometrial cavity. Magnetic resonance imaging (MRI) and direct visualization at laparoscopy are the gold standard techniques used to verify whether the cavity contour is due to a bicornuate or septate uterine anomaly.
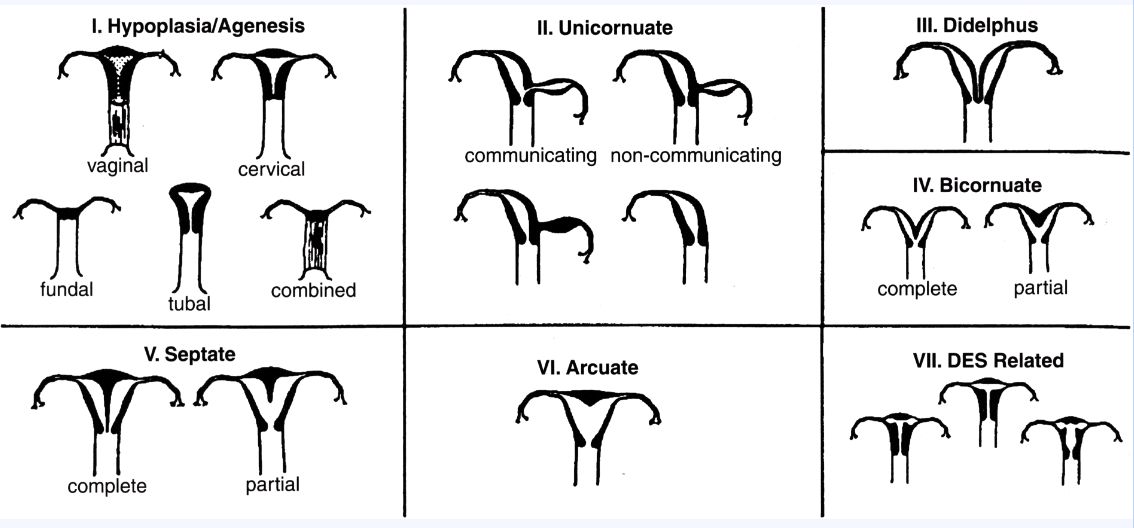 Fig. 20. American Society for Reproductive Medicine classification scheme for Mullerian anomalies. Reprinted with permission.
Fig. 20. American Society for Reproductive Medicine classification scheme for Mullerian anomalies. Reprinted with permission.
Clinical management differs between septate and bicornuate uterine morphologies. While the bicornuate uterus is implicated in fetal malpresentation, early pregnancy loss is uncommon and infertility is not attributed to the bicornuate uterine anomaly. In contrast, hysteroscopic ablation of the uterine septum is completed to avoid early recurrent miscarriage and very early preterm delivery in the second and early third trimesters of pregnancy. It is imperative that the exact nature of each anomaly is clarified because the application of conservative or surgical management depends upon the character of the uterine anomalies and their clinical presentation.
Evaluating uterine abnormalities
A transvaginal ultrasound examination of the uterus may be performed in the consultant’s office at the time of an initial infertility consultation.6, 183, 184, 186, 187, 188 An evaluation of the myometrium and endometrium can be performed simultaneously to determine the position of uterine fibroids relative to the endometrium and the oviducts. A preoperative examination of the uterus may be completed to plan surgical procedures and predict intraoperative difficulties. For example, with the excision of intramural fibroids, preoperative assessment may predict that excision of fibroids lying adjacent to the large uterine arteries and veins may result in marked blood loss. Alternatively, excision of fibroids adjacent to the oviductal ostia may increase the risk for postoperative occlusion of an oviduct. The uterine body shape and uterine cavity contour are evaluated to identify congenital uterine anomalies. Some intracavitary defects can be recognized with routine ultrasonographic examinations. However, additional information can be gained by completing a sonohysterogram (sonoHSG) in the office. Many conditions are better evaluated with sonoHSG, a saline insufflation of the uterine cavity, because of the capacity to examine the endometrium and myometrium simultaneously with real-time ultrasonography. For example, it is possible to use saline insufflation to demonstrate that a rudimentary uterine horn does not communicate with the cavity of its adjacent unicornuate uterus. Occasionally, the addition of color flow Doppler can delineate tissue planes and the vascular supply of the myometrium and fibroids. The information derived from an ultrasound examination may also be combined with images acquired with MRI. The MRI also can be used to define anatomy while avoiding ionizing radiation, dye contrast, and potential infection. However, the substantial procedural cost to complete an MRI may make it less available to clinicians and patients. Imaging with ultrasonography at the time of referral and subsequent appointments is a relatively low cost, convenient office procedure which will provide a great deal of information and contribute to timely diagnoses.
Fibroids (leiomyomata)
Ultrasonography has enhanced the imaging of uterine fibroids.182, 183, 187, 189 The location and size of leiomyomata can be mapped within the myometrium to aid in infertility investigations (Fig. 21). Occlusion of a proximal oviduct may occur when leiomyomata grow within the uterine cornu and exert pressure or occlude the intramural portion of the oviduct. Fibroids may also significantly change the uterine cavity contour and impair embryo implantation. Fibroid size and location may be mapped to determine the degree of extension into the uterine cavity, proximity to the uterine cornu/proximal oviduct and relative position in relation to larger intrauterine blood vessels and bowel with standard transvaginal ultrasound examination, sonoHSG and color flow Doppler interrogation.
 Fig. 21. Intramural leiomyomata are frequently visualized. Examples of fibroids which compromise the contours of the endometrial cavity are shown (A–D). Refraction artifacts resulting from tissue density interfaces and the texture of the fibroids often aid in their identification.
Fig. 21. Intramural leiomyomata are frequently visualized. Examples of fibroids which compromise the contours of the endometrial cavity are shown (A–D). Refraction artifacts resulting from tissue density interfaces and the texture of the fibroids often aid in their identification.


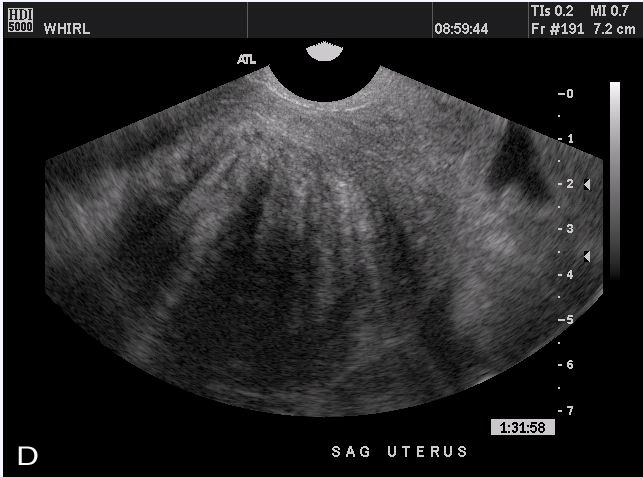
There are many theories that attribute infertility and recurrent pregnancy loss to leiomyomas. Implantation failure and early pregnancy loss have been accredited to an intrauterine inflammatory response mediated by myomas. Implantation failure has been associated with the placentation over myomas. Early pregnancy wastage may occur in the presence of very large or multiple small leiomyoma that cause marked pre-pregnancy uterine enlargement. With marked pre-pregnancy uterine enlargement, very early preterm expulsion of viable intrauterine contents, early preterm spontaneous rupture of membranes, and very early labor may be related to failure of uterine expansion. Ultrasonography may be helpful to delineate causes of and therapies for reproductive failure when leiomyomas are present.
Leiomyomata may be examined serially to evaluate changes in diameter and echotexture facilitating a conservative watch and see management approach with medications or surgery. GnRH agonist (GnRHa) therapy will decrease uterine vascularity and temporarily decrease uterine size. Thus, GnRHa is commonly used to decrease blood loss and fibroid size prior to surgical intervention to excise uterine fibroids. Surgical excision of myomas may be completed hysteroscopically, laparoscopically or at laparotomy. Uterine leiomyomatosis, a condition that often results in infertility and abnormal uterine bleeding, is recognized when numerous small leiomyomata are seen and little or no nonmyomatous tissue can be demonstrated between the myomas. Leiomyomatosis causing infertility is difficult to manage. Conservative management may include both medical and surgical therapies, that is, the use of GnRHa to shrink myomas and excision, respectively. To evaluate the value, risk of, and most optimal method for surgical excision most effectively, a careful preoperative map of myomas should be completed to assess the relationship of myomas to adjacent great vessels, oviducts, uterine cavity, and bowel.
Endometrial synechiae
The endometrium is a self-regenerating tissue that generally is resistant to damage.182, 190, 191 The basal layer of endometrium may be damaged by infection or removed by instrumentation. Synechiae, that is, scar tissue, may form between areas where destruction of basal endometrium has occurred. Adhesions may extend across the uterine cavity and may obliterate or obstruct the cavity. Endometrial damage may be suspected when portions of, or the entire, endometrial surface remains thin and irregular in contour and hyperechoic throughout the cycle rather than changing patterns in association with the reproductively active hormones. Synechiae may be visualized only when fluid is insufflated through the cervix during sonoHSG or at the time of menstrual flow, and may appear as thin strands of tissue extending from opposite endometrial walls. Clinically, a history of miscarriage, dilatation and curettage surgery or endometritis/salpingitis often precedes the formation of endometrial synechiae. Light or absent menses, recurrent early pregnancy loss or failure to conceive may occur following the formation of intrauterine synechiae/scarring. Synechiae occur commonly following elective endometrial ablation or resection. While implantation is impaired when endometrium is damaged or absent, if conception does occur, abnormal placentation may result in placenta accreta, percreta, and increta.192 Diagnosis is made by HSG or sonoHSG. Confirmation of the diagnosis and treatment involves sonohysterography and hysteroscopic evaluation of the uterine cavity, hysteroscopic adhesiolysis and postsurgical extended estrogen therapy. Simultaneous ultrasound guidance is often required.190, 193, 194 Sonohysterosalpingography has been used to treat synechiae for persistent infertility and synechiae following hysteroscopic surgical repair.195 Reproductive outcomes following surgical excision of uterine synechiae are varied and include a resumption of menses and pregnancy, although there is a greater risk for abnormal placentation with conception.182, 192, 196, 197, 198
Adenomyosis
Adenomyosis is diagnosed when endometrial glands and stroma distinct from and not confluent with the endometrial cavity are found in uterine myomatous tissue.199 The gold standard for diagnosis is histological examination of areas of suspected adenomyosis which is typically done after hysterectomy. Conservative approaches include the use of ultrasonography or MRI to make a diagnosis without surgery.200, 201, 202, 203 Combining transabdominal ultrasound with hysterosalpingography has not yet been useful to diagnose adenomyosis; however, transvaginal ultrasound examinations have been more successful in making a presumptive diagnosis of adenomyosis.189, 204 Color flow mapping of the myometrium with transvaginal ultrasonography has been used by some specialized centers to evaluate adenomyosis.205, 206
Gartner’s duct cysts
Embryologic remnants of the Wolffian duct system may occasionally form Gartner’s duct cysts. These cysts form when there is incomplete resolution of the embryonic mesonephric ducts that may remain within a line that extends from the broad ligament to paracervical tissue. Cysts typically remain small and range from 2 to 10 mm. They are generally painless and asymptomatic structures that are seen en passant as single or multiple hypoechoic spherical structures along the lateral margins of the cervix or uterus. Treatment is generally not required.
DIAGNOSTIC USE OF ULTRASONOGRAPHY IN INFERTILITY INVESTIGATIONS: THE CERVIX
The cervix is the anatomic extension of the uterus that lies within the upper vaginal canal and is visualized cephalad or below the lower uterine body. There is no obvious discrete visual line that determines where the uterine corpus ends and the cervix begins and the general consensus is an anatomic definition. The paired uterine arteries lie lateral to the uterus, just above the level of the internal os of the cervix. However, there are histologically distinct characteristics in the glandular cells within the cervix that differentiate it from the lower uterine glandular epithelium. The full length of the cervix can also be easily demonstrated during pregnancy when amniotic fluid and membranes have a supracervical location within the uterine cavity.
Nabothian cysts
Nabothian cysts can be appreciated during ultrasound examination at the level of the exocervix. Nabothian cysts of varying diameters are common at the external surface of the cervix. These hypoechoic simple cysts form when normal cervical glands become blocked. Nabothian cysts are not neoplastic and generally serve no pathological or physiological purpose. The echotexture of the cervix and nabothian cysts may appear similar to the echotexture of an ovary with reduced ovarian follicle population seen in perimenopausal women. Ultrasonographic inquiry may be directed to the cul de sac area when searching for ovaries that are difficult to visualize. It is possible to mistake the cervix with nabothian cysts for an ovary and follicle.
Postoperative cervical damage
Surgical procedures or traumatic delivery may result in cervical damage that may impair cervical integrity. Examples of sources of cervical trauma include vaginal delivery with the application of forceps, precipitous vaginal delivery resulting in cervical laceration, cervical dilatation prior to completion of uterine curettage or hysteroscopy, and cone biopsy surgery.207, 208, 209, 210, 211, 212 Cone biopsies are completed to gain large tissue samples for histopathological diagnosis of cervical neoplasia.207, 213, 214, 215 Cone biopsy surgery is done typically in women who present with high grade squamous intraepithelial lesions of the cervix (HSIL). The cone-shaped tissue is excised for histologic confirmation that dysplastic changes in cervical epithelium are limited to the epithelium and invasive cancer is absent. Cone biopsies are also recommended when discrepancies exists among cervical cytology, cervical biopsy histology, and direct visual inspection of the cervix at colposcopy. Cone biopsy is an excellent therapeutic maneuver for noninvasive and microinvasive lesions of the cervix as complete excision of cervical lesions can be ensured when a margin of normal tissue remains in the biopsied tissue and are used to stage cervical cancer when microinvasive disease is confirmed. Fertility potential may be retained if conception is desired when cervical cancer is limited to microinvasive disease (stage Ia). However, concern has been raised that cervical surgery can impair cervical integrity and predispose women to preterm delivery by inducing cervical incompetence.207 Ultrasonography plays little role in the assessment of the integrity of the cervix prior to conception; however, ultrasonographic examinations may be useful during pregnancy to monitor for signs of impending cervical incompetence.
Cervical incompetence
Cervical incompetence is defined by the occurrence of preterm, painless, cervical dilatation, without uterine contractions, resulting in delivery of a live fetus.216 Cervical incompetence is clinically difficult to recognize because, by definition, it is an asymptomatic condition. It often occurs prior to the gestational age when fetal survival is possible, i.e. prior to 24 weeks of gestational age during the second trimester of pregnancy. Prior cervical surgery may predispose some, but not all, women to cervical incompetence. Other women with cervical incompetence may have no history of cervical surgery. Tests to predict cervical incompetence and preterm labor/delivery have been recommended, although no single test to date has sufficient predictive value to support its widespread use. Transvaginal ultrasound measurements of cervical dilatation/length may be most useful to predict abnormal early cervical dilatation in women with a history consistent with cervical incompetence.217, 218, 219, 220, 221, 222, 223, 224, 225, 226 Assessment of the cervical length and dilatation by ultrasound examination remains a promising screening tool for cervical incompetence.
Cervical length and cerclage during the first trimester of pregnancy
Accurate cervical length measurements are needed to make an early diagnosis of cervical incompetence.217, 218, 219, 220, 221, 223, 224, 225, 227 Cervical length can be estimated by digital examination of the cervix or by ultrasonographic measurements; although, ultrasonographic measurements may be considerably less subjective than those derived from manual examinations. Cervical length measurements are completed to predict the onset of cervical shortening that accompanies cervical dilatation. A change in cervical length must be documented to diagnose cervical incompetence. An inverse relationship between cervical length and preterm delivery has been observed with increased routine performance of second trimester ultrasound examinations. Ultrasonographic evidence of cervical shortening to less than 2 cm is considered a risk factor for cervical incompetence. An effective screening tool is needed to predict cervical changes that lead to painless cervical dilatation in order to prevent pregnancy wastage. Ongoing ultrasound-based research studies may clarify the utility of serial ultrasound monitoring of cervical length/dilatation to predict cervical incompetence and establish optimal timing for surgical intervention.224
Cervical cerclage surgery is performed to prevent early preterm delivery.225, 226, 228 Briefly, a ring of suture material is placed circumferentially around the cervix to reinforce the cervical ring and prevent dilatation. Prophylactic cerclage is performed for women with a history of cervical incompetence. Typically, cerclage is completed transvaginally at the end of the first trimester of pregnancy when fetal viability is confirmed and the risk of miscarriage is reduced. Risks of intrapartum cerclage include uterine irritability and contractions that can lead to miscarriage and very early preterm rupture of membranes.229 Hence, only women with a high probability of cervical incompetence should receive a cerclage. Emergency cerclage may be indicated when clinical examination reveals progressive painless cervical dilatation in the second trimester of pregnancy and may be attempted prior to full cervical dilatation even following prolapse of a portion of the chorioamniotic sac into the vagina, although the risk of rupture of the sac is elevated.230, 231, 232, 233, 234 Prophylactic cerclage can be placed transabdominally prior to conception by laparotomy or laparoscopic surgery.235, 236 Abdominal cerclage is used for recalcitrant cervical incompetence not responsive to vaginal cerclage or in cases of radical cervical surgeries where little or no cervical tissue remains, for example, following extensive cone biopsy or trachelectomy.
Clinical indications for prophylactic vaginal or abdominal cerclage include history of cervical incompetence in pregnancy or following specific cervical surgeries where the cervix is completely or almost completely excised.222, 225, 226, 232, 237, 238 There is no evidence to support the use of prophylactic cerclage for only ultrasound-based cervical shortening. Cerclage appears to prevent preterm delivery in patients with three or more fetal losses occurring prior to the third trimester of pregnancy.225, 228, 234, 236, 239 Recommendations have been made to limit cerclage to women with a prior history consistent with cervical incompetence plus demonstration by ultrasonographic examination of cervical shortening prior to 22 to 24 weeks’ gestation. Two thirds of cerclage procedures have been avoided and no risk of preterm delivery has occurred since the recommendations have been implemented.
Trachelectomy
Women with newly diagnosed invasive cervical cancer confined to the cervix may elect to retain the opportunity to conceive by undergoing trachelectomy surgery.240, 241, 242, 243, 244, 245, 246, 247 Trachelectomy involves removal of the cervix and the formation of a neocervical ostium which will facilitate menstrual flow and sperm insemination. Prior to trachelectomy, a radical hysterectomy was the surgical treatment for cervical cancer confined to the cervix, to diagnose the extent of spread of cancer into adjacent lymphatic tissue and to ensure the removal of cancer while preserving ovarian activity. Transabdominal cerclage is typically placed at the time of trachelectomy surgery to offset the opportunity for cervical incompetence and preterm delivery. Delivery is accomplished by cesarean section. Preterm delivery is common following trachelectomy, regardless of whether cerclage was completed at the time of initial fertility-sparing cervical surgery.248, 249, 250 Consequently, multiple gestations have a poorer outcome because of their inherent increased risk for early preterm delivery. Once fertility potential is no longer desired, a hysterectomy may be completed.
Fertility assessment and ART assistance may be required to facilitate conception following trachelectomy.251 Cervical stenosis may require instrumentation and intrauterine insemination. An evaluation of the intrauterine cavity contour and oviductal patency can be demonstrated in a clinician’s office by sono-HSG when ART is contemplated. A small catheter is placed through the neocervical ostium to fill the uterine cavity with saline and insufflate each oviduct. A simultaneous endovaginal ultrasound examination is done to examine the soft tissue structures of the pelvis. Inspection of the uterine cavity contour for anomalies and demonstration of oviductal patency may be done prior to initiating intrauterine sperm insemination or as part of an investigation of infertility following trachelectomy. During pregnancy, serial evaluations for cervical competence and integrity of the cerclage sutures can be completed using transvaginal ultrasonography.252
THE EVALUATION OF THE UTERINE CAVITY AND OVIDUCTS IN INFERTILITY
Structural abnormalities or anatomic distortion of the uterus or endometrial cavity may be the reason for implantation failure, spontaneous abortion, preterm labor, preterm rupture of membranes, and pregnancy malpresentation.253 An optimal fertility evaluation should include an assessment of tubal patency and the uterine cavity contour.254 It has been estimated that uterine abnormalities are associated with up to 10% of infertility and the proportion with uterine abnormalities rises up to 32% in women with secondary infertility.255, 256 The increase in the proportion of women with secondary infertility who have uterine abnormalities suggests that anomalies are acquired, and may be caused by first trimester abortion, uterine instrumentation or operative delivery.
Sonohysterosalpingography/hysterosalpingosonography (sonoHSG)
A sonoHSG is an enhanced ultrasonographic procedure that involves the insufflation of saline into the uterine cavity with simultaneous transvaginal ultrasonography. Saline is an ideal contrast medium. It is hypoechoic and enhances imaging through the medium, while remaining physiologically nonreactive. Saline distends the uterine cavity and contrasts with the endometrium, making it easy to visualize the contour of the lumen, endometrial folds, polyps, and synechiae. SonoHSG can be used to evaluate the uterine cavity and tubal patency very effectively in a clinical office. Ionizing radiation is not required and the risk of allergic reaction to contrast agents is avoided. SonoHSG is best performed during the follicular phase of the menstrual cycle, prior to ovulation. At this time, the endometrium is physiologically thin, transmission of any menstrual effluent into the peritoneal cavity is avoided and there is no chance of disrupting or dislodging an oocyte, embryo or early pregnancy.257
It is possible that sonoHSG will replace standard hysterosalpingography (HSG) in the initial assessment of the uterine cavity contour and tubal patency.258, 259 The HSG has been used historically to evaluate the uterine cavity contour and oviductal patency in women presenting with infertility. The HSG involves introduction of a radio-opaque contrast dye and fluoroscopic imaging in a radiology suite. Women with abnormal uterine bleeding or recurrent pregnancy loss are more frequently evaluated with sonoHSG than HSG.260 The sensitivity of sonoHSG is superior to the HSG to diagnose intrauterine abnormalities.261
Sonohysterographic technique
Sonohysterosalpingography involves the instillation of sterile injectable grade physiologic saline into the uterus with a catheter while simultaneously examining the soft tissues of the reproductive organs with transvaginal ultrasonography.262, 263 Saline can be delivered transcervically with a rigid catheter designed for sonoHSG. The catheter does not require the use of a cervical tenaculum. A separate port is available for insufflation of a 0.5–1.0 ml intrauterine balloon that prevents the catheter from being expelled during insufflation. Alternatively, saline may be introduced with less expensive catheters, such as a pediatric feeding tube; however, no intrauterine balloon is available and the tube may be dislodged during ultrasonography. A pediatric foley catheter may suffice for insufflation as it has a balloon; however, its flexibility makes it more difficult to thread through the cervix.
The sonoHSG can be performed with the woman in a semirecumbent lithotomy position for added comfort and to allow the woman to watch the ultrasound screen as the procedure is completed. A speculum is placed in the vagina and the cervix is visualized for cleansing with antiseptic. Catheter insertion is completed immediately following cleansing. The catheter is handled using sterile technique and the ports must be protected from contamination during handling. The balloon port is loaded with 1.0 ml of injection grade physiologic sterile saline and the balloon inflated to test its integrity. The balloon is then deflated for transcervical insertion. The catheter lumen also is loaded with saline, then temporarily clamped to avoid insufflation of air. The catheter is inserted transcervically to a depth of approximately 4 cm so that the balloon rests in the uterine cavity beyond the internal os of the cervix. Optimal positioning of the balloon occurs when the balloon is inflated with only approximately 0.75 ml to minimize uterine discomfort. The speculum is then removed leaving the catheter resting within the uterine lumen. Slight traction is occasionally required to position the balloon properly. The saline insufflation port rests outside the vaginal introitus and a syringe containing saline is attached to the lumen port. The lumen is then unclamped and ready for insufflation.
The transvaginal ultrasound probe is gently inserted in the vagina alongside the saline insufflation catheter. The hypoechoic catheter balloon is easily visualized in the uterine cavity and the location of each ovary/fallopian tube is determined (Fig. 22). Images of the uterine cavity are captured for documentation in both sagittal and transverse planes while saline is instilled through the catheter into the uterus (Fig. 23). After insufflation of the uterine cavity is done, attention is quickly directed to each fallopian tube to determine whether distension and intraperitoneal flow occurs. This should be visualized in women with patent oviducts.262, 264 Microbubbles within the saline are usually present after loading saline into the insufflation syringe; however, they can be hyperaccentuated by shaking the saline prior to loading the syringe. The hyperechoic solution may be easily visualized as it moves through the fallopian tube.265 Fluid may be observed to swirl as it collects outside the fimbria and the fimbria may be clearly outlined when surrounded by free insufflated saline (Fig. 24).
 Fig. 22. Midsagittal image of the uterus with a hysterosalpingosonography catheter demonstrating correct placement of the balloon cuff. Instillation of saline has been initiated and the tip of the catheter is observed in the fluid to the left of the cuff.
Fig. 22. Midsagittal image of the uterus with a hysterosalpingosonography catheter demonstrating correct placement of the balloon cuff. Instillation of saline has been initiated and the tip of the catheter is observed in the fluid to the left of the cuff.
 Fig. 23. Midsagittal (A) and transverse (B) images of a normal uterine cavity following instillation of saline. The fluid-endometrium interface is smooth and symmetrical.
Fig. 23. Midsagittal (A) and transverse (B) images of a normal uterine cavity following instillation of saline. The fluid-endometrium interface is smooth and symmetrical.

 Fig. 24. Free fluid collection in the cul-de-sac following successful demonstration of oviductal patency. Oviductal fimbria are clearly observed in the collected fluid.
Fig. 24. Free fluid collection in the cul-de-sac following successful demonstration of oviductal patency. Oviductal fimbria are clearly observed in the collected fluid.
When fluid passes through each oviduct, tubal distension is minimal in normal oviducts. A hydrosalpinx is identified by moderate tubal distension that persists after insufflation is stopped. Color flow Doppler interrogation in two or three dimensions may be used to visualize movement of fluid through the oviducts if the perception of oviductal patency is not apparent or is uncertain.266, 267 Accumulation of fluid at the cul-de-sac will be apparent if at least one oviduct is patent. Therefore positioning the patient in a semi-sitting position will ensure that the cul-de-sac is lower than the remainder of the pelvis and abdomen. Attention should be directed to both oviducts to discern bilateral patency. Following inspection of the oviducts, attention is re-directed to the lower uterine cavity. Fluid instillation is continued while simultaneously deflating the balloon and visualizing the endometrial cavity.
Mild discomfort may be appreciated by some women during the sonoHSG saline insufflation. However, patients who have had prior HSG have commented that the sonoHSG is more comfortable and much more tolerable than their experience with the HSG. This may be due to the use of saline in place of contrast agents for visualization, the use of smaller catheters, and because a tenaculum is not required for most women undergoing sonoHSG.
Indications for sonohysterography
The sonoHSG has many advantages. The size, shape, and contour of the uterine cavity can be observed in both sagittal and transverse planes and related to the position of adjacent structures, the ovaries, and other pelvic anatomy. Discovering a normal uterine cavity with sonoHSG is almost as reliable as diagnostic operative hysteroscopy.178, 256, 261, 268, 269, 270 Filling defects such as synechiae, polyps or fibroids can be identified, measured and localized to anterior and posterior surfaces of the endometrium and oriented to the right or left cornua, mid-body or cervical regions (Fig. 25). In addition, distortion of the uterine cavity by large masses can be critically appraised with sonoHSG. For example, when a mass protrudes into the cavity, the site of attachment to the uterus can be illustrated as either an intramural fibroid mass arising from a wide base or a subserosal fibroid with a pedunculated attachment. An intracavitary mass may be demonstrated on HSG but it is typically not possible to determine whether the mass is an intramural or subserosal fibroid. The sonoHSG has the capacity to demonstrate the anomalies of the myometrium and endometrium simultaneously.
 Fig. 25. Images of endometrial polyps and adhesions recorded during hysterosalpingosonography (A–D). sonoHSG is very helpful in identifying small and large lesions that are difficult to appreciate on unenhanced ultrasonography.
Fig. 25. Images of endometrial polyps and adhesions recorded during hysterosalpingosonography (A–D). sonoHSG is very helpful in identifying small and large lesions that are difficult to appreciate on unenhanced ultrasonography.



The distendability of the uterine cavity during saline insufflation may reflect the capacity for uterine growth and expansion of the uterine cavity during pregnancy. Cavity distension with sonoHSG can be observed as normal, reduced or absent and correlated to the patient’s clinical history. As an example, limited endometrial cavity expansion observed with leiomyomatosis, large intracavitary and multiple intramural fibroids are correlated with a higher probability of recurrent pregnancy loss or preterm delivery. Assessment of the myometrium during the sonoHSG can assist a clinician to assess the feasibility of surgery to ameliorate myometrial pathology. Hence, the sonoHSG may be used to assess the capacity of the uterus to distend and correlate distension with myometrial anomalies that may alter uterine growth and expansion during pregnancy.
Examination with ultrasonography and simultaneous saline insufflation can be useful when differentiating between two commonly identified abnormalities: septate and bicornuate uteri (Fig. 26).186, 188 The indentation in the exterior uterine surface contour of a bicornuate uterus can be noted while examining the myometrium enveloping each uterine horn. The thickness, length, and relationship of a septum to the fundal myometrium also can be clarified. Color flow or power Doppler interrogation may help by verifying the anticipated vascularity of the fundal myometrium of a bicornuate uterus, whereas septae are typically relatively avascular.271 Three-dimensional sonoHSG allows volumetric data to be re-interrogated in many planes, although the coronal plane appears to the most informative in identifying the anatomic relationships.272

Fig. 26. Transverse image of a bicornuate uterus taken during sonoHSG. The nature of the uterine cavity is revealed by the instillation of saline.
Contrast enhanced hysterosalpingography (HyCoSy)
A contrast medium such as EchovistTM may improve imaging of the oviducts when saline is insufficient.266, 273 This specific purpose contrast medium contains a hyperechoic mixture of microbubbles and microparticles of galactose. The stabilized mixture enhances visualization of the fluid. Tubal anatomy can be identified more easily during insufflation and the flow of the contrast agent can be easily observed as it moves through the oviducts and swirls while exiting the fimbrial ends. However, contrast medium is not widely available for clinical use in many countries.
THERAPEUTIC USES OF ULTRASONOGRAPHY IN INFERTILITY
Ovarian stimulation and assisted reproductive technologies
MONITORING THE COURSE OF OVARIAN STIMULATION
As assisted reproductive technologies have evolved, countless protocols for ovarian stimulation have been developed for numerous etiologies of infertility. Ovarian stimulation was first introduced to provide therapy for anovulation. Innovations in ultrasonography and hormonal assays have allowed clinicians to assess multiple follicle development and ovulation rapidly and more easily. The capacity to provide ultrasound examinations and oocyte retrieval within an office setting has facilitated a move away from hospital-centered fertility care. Hormones to stimulate follicle growth and prepare the uterus for pregnancy can be self-administered as subcutaneous injections, thereby freeing women from attending clinics daily to receive their medication. The use of endovaginal ultrasonography to monitor follicle growth during ovarian stimulation has been the most important innovation that has significantly advanced the provision of assisted reproductive technologies.
The first stimulation protocols for women who were anovulatory were intended to induce single follicle growth, a single ovulation, and conception. Clomiphene citrate tablets could be taken orally to induce folliculogenesis and ovulation, had few side effects, and allowed some women to ovulate and conceive. Urinary derived human menopausal gonadotropins (hMG) containing FSH and LH were introduced for women who did not respond to clomiphene citrate. The hMG-derived FSH was administered by daily intramuscular injection during the entire course of therapy. Later hMG were injected subcutaneously with no change in efficacy. A substantial increase in ease of administration of the gonadotropins was accompanied by a decrease in discomfort associated with subcutaneous injections making it easy to encourage women to adopt self-administration of their ovarian stimulation medications. Ultrapure recombinant gonadotropins (rFSH, rLH) were produced for subcutaneous administration and were regarded as free from human urinary derived contaminants and believed to be more efficacious than hMG.274 Follicle growth was monitored with ultrasonography when FSH therapy was prescribed to facilitate adjustments in medication dosage. High resolution transvaginal ultrasonography was introduced and became the standard technique for rapid, noninvasive monitoring of follicle growth in a clinician’s office.275 Ultrasonography became an indispensable examination tool to monitor the number of growing follicles in an effort to induce ovulation while reducing the incidence of multiple ovulation, multifetal gestation, and ovarian hyperstimulation syndrome (OHSS). FSH doses were increased or decreased according to each woman’s ovarian response, as assessed by serial ultrasound examinations, to control the number of growing dominant follicles, and ultimately prevent ovarian hyperstimulation.275 Evaluation of serum estradiol levels was incorporated into stimulation protocols as an imperfect predictor of the number of follicles that responded to hMG and rFSH. The combination of follicle growth monitored and observation of estradiol levels was used to identify the optimal time for administration of human chorionic gonadotropin (hCG) to induce ovulation.
A critical step for ART has been to establish optimal timing of hCG administration. It remains imperative to identify the preovulatory period when follicles are most receptive to hCG induction of ovulation or the final stages of follicle maturation for IVF. We rely on our understanding of the ovarian physiology of natural cycles and look to the size of the preovulatory follicle and circulating estradiol levels when LH is released spontaneously. Ideally, the optimal time for administration of hCG is at the stage of follicle development that will support the final stages of folliculogenesis and oogenesis and yield the highest quality oocytes.276 Typically, 5000–10,000 IU hCG is given to induce ovulation when the largest preovulatory follicle reaches a diameter of approximately 18–20 mm. However, ovulation has been observed from subordinate follicles that were only 14 mm in diameter when the largest follicle’s diameter was used to determine when to administer hCG. It is apparent that follicle size alone is not the sole predictor of oocyte maturity and the competence of follicles to respond to hCG. Three-dimensional image analysis has been useful to demonstrate that individual follicles display ultrasonographically detectable features of physiologic competence. While ultrasonographic examinations have been used primarily to evaluate follicle diameters, ultrasound-based studies are needed to explore the capacity for computer-assisted analysis of ultrasound images of preovulatory follicles to elucidate physiological characteristics that will predict the optimal time for hCG administration and oocyte competence.
ASSISTED REPRODUCTIVE TECHNOLOGY PROTOCOLS FOR OVARIAN STIMULATION
Ovarian stimulation protocols were adapted for infertile women who ovulated regularly in order to provide ART for numerous etiologies of infertility. Couples with unexplained infertility, identified by at least 2 years of infertility, regular ovulation, normal reproductive anatomy, and adequate sperm concentration were encouraged to use FSH therapy and intrauterine insemination. The goal of therapy was to overcome unexplained infertility by stimulating growth of multiple mature follicles by the administration of supraphysiologic levels of FSH, inducing multiple ovulation with hCG, and introducing a higher concentration of motile sperm by intrauterine insemination than would occur with coital activity at the time of ovulation. IVF was encouraged to allow women with obstructed, damaged or absent oviducts to conceive. Exogenous FSH stimulation for IVF was designed to initiate growth of supraphysiologic numbers of follicles to ensure an adequate supply of oocytes was available for fertilization and numerous embryos were formed for embryo transfer and embryo cryopreservation. In the IVF laboratory, oocytes are isolated from the aspirated follicular fluid and inseminated with motile sperm. Resulting embryos are identified and transferred transcervically to the woman’s uterine cavity.
The scope of IVF therapy enlarged as therapy became focused upon ameliorating male factor infertility with the introduction of intracytoplasmic sperm microinsemination (ICSI). Ovarian stimulation was used in the female partner of couples experiencing male factor infertility, multiple follicles were stimulated to develop, oocytes were collected and each individual oocyte inseminated with a single sperm with the aid of microscopic injection techniques. Ovarian stimulation is now routinely performed to provide numerous oocytes for IVF and ICSI therapies. IVF and ICSI have become standard practice for treatment of severe oligozoospermia, male antisperm antibodies, and unexplained fertilization failure following traditional IVF. IVF plus ICSI has also been used to ensure embryo fertilization for women at advanced maternal ages where fertilization failure is more common. Traditional IVF therapy has played a role in facilitating conception with surrogate pregnancy, unexplained infertility, oocyte donation, and preimplantation genetics. Ovarian stimulation protocols have incorporated hCG or recombinant hCG (rhCG) to induce ovulation or to plan oocyte retrieval at specific times. GnRH agonists and antagonists are used to prevent spontaneous LH release for women completing IVF oocyte retrieval. Clinical assessment of the growth of the entire follicle cohort and response to GnRH agonist or antagonist therapies has facilitated more accurate control of the time when hCG is administered. For IVF, oocyte retrieval is typically scheduled 34–36 hours after hCG. Intrauterine sperm insemination is typically scheduled approximately 36 hours after hCG when spontaneous ovulation is anticipated. Ultrasonography is a crucial part of each ovarian stimulation protocol and has become a routine, convenient office-based modality used to monitor progress, ensure safety, and maintain an appropriate ovarian response.
The goal of ovarian stimulation is to induce sufficient numbers of follicles to grow and facilitate the development of mature competent oocytes within each dominant follicle that can be either released spontaneously or retrieved just prior to ovulation for IVF. Ovarian stimulation protocols are tailored to suit the needs of each individual according to their mode of therapy and according to the responsiveness of an individual to the agents used to induce follicle growth. Women may respond in entirely divergent manners to exogenous FSH. For example, women with PCOS may hyperstimulate and be at greater risk of developing OHSS postovulation with lower doses of FSH. In contrast, in women regarded as poor responders, stimulation of multiple follicle growth may not occur despite administration of high levels of FSH. Ultrasonography is required to monitor changes in multiple growing follicles during FSH therapy. Estradiol levels are also used to monitor the growth of multiple follicles even though all follicles likely do not contribute equally to systemic estradiol concentrations. A presumption is made that elevated estrogen arises primarily from the largest growing follicles that have reached advanced stages of development and are capable of responding to hCG. The ideal time to administer hCG is at the stage of follicle development that will support the final stages of folliculogenesis and oogenesis and yield the highest quality of oocytes for spontaneous ovulation or IVF retrieval.276, 277, 278
The size of the preovulatory follicle at the time of LH release in natural cycles has been the best predictor for a high-quality oocyte in young fertile women. Similarly, follicle size has been the best predictor for oocyte maturity in stimulated cycles. The probability of oocyte fertilization and the ability of an embryo to implant and develop into a successful pregnancy each have relied on a physiologically mature, competent oocyte.42, 52, 279, 280, 281, 282 The highest fertilization rates with IVF are achieved from mature oocytes, but fertilization following in vitro maturation (IVM) of immature oocytes is also possible.283, 284 In vitro, it is difficult to grow follicles from early stages to maturity because of the challenges in reproducing the necessary biochemical cell support present in the microenvironment of the maturing follicle. However, significant progress is being made. Oocytes retrieved from follicles less than 10 mm in diameter and subjected to IVM have been used to increase the number of embryos available for transfer.285 Additional laboratory evaluation of oocytes retrieved for IVF-IVM that will result in optimal fertilization and cleavage rates is needed before determining the timing of oocyte retrieval and the ultrasonographic characteristics of immature antral follicles that will respond to IVM.284, 286, 287, 288, 289
PERIFOLLICULAR VASCULARITY
Power Doppler evaluation of perifollicular vascularity to predict the developmental competence of human oocytes has been explored during ovarian stimulation.42, 46, 52 During follicle growth, the rate of blood flow within perifollicular tissue increases. The microenvironment of the oocyte changes allowing oocytes competent to undergo fertilization to develop. Early follicular phase measurements of perifollicular blood flow have been correlated with higher clinical pregnancy rates. In addition, computer-assisted analyses of ultrasound-generated images of preovulatory follicles have been well correlated with the ability of an oocyte to be fertilized in animal models. In humans, similar work has not been reported.53
FOLLICLE GROWTH RATE ASSESSMENT
It has been clinically useful to evaluate individual follicle growth rates in natural and ovarian stimulation cycles.290 Clinicians have been able to adjust ovarian stimulation protocols to ensure an optimal number of growing follicles and prevent OHSS when evaluations were made early in therapy.291, 292, 293 However, reports of follicle growth rates have been conflicting. One of the earliest studies reported faster growth rates during ovarian stimulation compared with natural cycles.294 A mathematical equation developed to evaluate follicular growth rate later concluded that follicle growth rates were similar between spontaneous cycles and hMG stimulation cycles.295 Another study reported that the growth rate of follicles helped to estimate the time of ovulation accurately during stimulation cycles where a pregnancy had been established.296 Detailed evaluations of follicle growth have shown an approximately 1.5 mm per day growth rate when observed during natural cycles, with oral contraceptive use and during ovarian stimulation.176, 177 A mathematical model has been developed to predict follicle growth in response to ovarian stimulation by using daily observations of follicle growth rates.14, 15, 176, 177, 297, 298 The rate of follicle growth may prove to be the most accurate predictor for the maturity of ova. However, follow-up work has not yet been done in this area. It will be challenging to combine daily detailed ultrasound measurements with work in an embryology laboratory. Individually mapped follicles need to be correlated to a per follicle fertilization and conception outcome and final clinical pregnancy outcome.
Ovarian hyperstimulation syndrome
Ovarian hyperstimulation syndrome (OHSS) arises as a complication of ovarian stimulation, may have serious consequences, and is almost completely iatrogenic. Spontaneous OHSS is seen rarely.292, 293, 299, 300, 301 In OHSS, the ovaries markedly increase in size depending on the number and size of enlarging follicular cysts (Fig. 27). Ultrasonographic examination reveals thin, hyperechoic follicle walls and hypoechoic fluid makes up the cystic interior.39, 293, 302 Marked vascular perfusion of the follicle walls is revealed with color flow Doppler interrogation. The ovaries enlarge excessively and may reach diameters greater than 10 cm. Individual cysts may display an internal echotexture consistent with hemorrhage. Accumulation of ascites fluid in the cul-de-sac or around the ovaries may be apparent on transvaginal ultrasound examination. In severe cases of OHSS, pleural effusion at the lung bases may be demonstrated with transthoracic ultrasonography.
 Fig. 27. Transvaginal ultrasound image of a woman with moderate OHSS. Both ovaries are enlarged and are observed in the posterior cul-de-sac. The ovaries are in close contact and displace the uterus anteriorly. Both ovaries contain several large unruptured follicles.
Fig. 27. Transvaginal ultrasound image of a woman with moderate OHSS. Both ovaries are enlarged and are observed in the posterior cul-de-sac. The ovaries are in close contact and displace the uterus anteriorly. Both ovaries contain several large unruptured follicles.
Prevention, or reduction in the severity of OHSS may be possible with thoughtful management of ovarian stimulation.303, 304 The risk for OHSS during ovarian stimulation may be limited by carefully assessing the size of the growing follicle population and adjusting/decreasing the dosage of exogenous gonadotropins to regulate follicle growth.305, 306, 302, 307, 308 The severity of OHSS may be restricted by “coasting” techniques where gonadotropins are withheld for 1–3 days while awaiting a decline in growth of small and medium range follicles in the hope of gaining fewer mature dominant follicles receptive to hCG.306, 309, 310, 311, 312, 313
Severe OHSS may be prevented or substantially reduced by canceling the administration of hCG and preventing immediate conception. Pregnancy also may be prevented by canceling insemination or embryo transfer. OHSS appears to be driven by hCG administration and rising hCG from a clinical pregnancy exacerbates the condition. Alternative management strategies to prevent pregnancy and thereby prevent potentially severe OHSS may include IVF aspiration of mid-range and large diameter follicles after hCG injection, fertilization of oocytes and subsequent cryopreservation of all embryos. Once follicle regression has occurred and the danger of OHSS is no longer imminent, embryo transfer can be completed by utilizing an appropriate cryopreserved embryo transfer protocol.302, 309, 310, 311, 314 A reduction in severity of OHSS may possibly result when transfer is restricted to a single embryo in selected cases.304, 308, 315 Prevention of OHSS also may be accomplished by utilizing in vitro maturation (IVM) of immature oocytes aspirated from immature antral follicles.316 IVM therapy can circumvent FSH ovarian stimulation for women at high risk for hyperstimulation. Other strategies under investigation to prevent or reduce OHSS include the use of GnRH agonists to trigger ovulation, dopamine agonists to impede phosphorylation of vascular endothelial growth factor receptor 2, and the use of volume expanders such as hydroxyethyl starch.311, 317, 318
Assessment of the ovaries postovulation/oocyte retrieval may provide clues of imminent OHSS. The patient and clinician can then be prepared to provide additional surveillance and to administer appropriate therapy that will avoid serious morbidity and mortality.291, 302, 319, 320, 321, 322, 323 The combination of a rise in levels of circulating estradiol with enlargement of anovulatory follicles immediately following ovulation/retrieval are signals of impending OHSS. Typically, estradiol levels fall and anovulatory follicles regress in diameter immediately following ovulation or oocyte retrieval. As OHSS progresses, ovarian enlargement is accompanied by the symptoms of pelvic fullness and a variable presentation of pain or discomfort. Abdominal pressure increases as intravascular fluids move into the abdominal cavity and create ascites. Some of the abdominal pressure and pain may be relieved by transvaginal ultrasound-directed aspiration of ascites fluid or transabdominal ultrasound-guided paracentesis. Intravenous rehydration therapy will ensure adequate uteroplacental perfusion during early pregnancy and prevent renal compromise. Replacement of intravascular fluid with an appropriate intravenous volume of isotonic fluids and protein will also prevent hemoconcentration. Anticoagulation is indicated when a rise in hematocrit is recognized, as hemoconcentration may increase the risk for venous thrombosis. Pleural effusion may also accompany the development of severe ascites. Ovarian enlargement and ascites typically do not resolve for weeks; however, symptoms usually begin to subside substantially following fluid/protein replacement and aspiration of ascites fluid. Therapy can be completed for women on an outpatient basis if early signs of OHSS are recognized.315, 322
Ovarian torsion can occur following OHSS and is accompanied by severe pain. Torsion should be investigated rigorously with color flow Doppler imaging to confirm the diagnosis and initiate early surgical intervention to prevent the need for oophorectomy.302, 324, 325 Early recognition of OHSS and initiation of therapy can obviate many complications and reduce the morbidity and mortality previously associated with this side effect of ovarian stimulation.
Ultrasound-guided oocyte retrieval for in vitro fertilization
Technological innovations in ultrasonography have been integral to the advancement of oocyte retrieval for IVF therapy. The concept of IVF initially involved oocyte retrieval in a hospital operating room with the patient under general anesthesia. Oocyte retrieval was a rate-limiting step when IVF was first initiated as it required the use an operating theater at specific times, often conflicting with and competing for, the resources of other more “urgent” hospital-based surgeries. Oocyte retrieval was time-consuming and expensive because endoscopic surgery was required. Also, the oocytes were exposed to the high concentrations of carbon dioxide used for endoscopic abdominal insufflation. Surveillance of the ovaries during laparoscopic retrieval was initially accomplished with transurethral, transvesicular, and transabdominal ultrasound guidance or by direct laparoscopic vision prior to the introduction of video laparoscopy.326, 327, 328, 329, 330, 331, 332, 333, 334, 335, 336, 337 Conscious sedation replaced general anesthesia in the clinic-based procedure room. Transvaginal ultrasound probes were fitted with a needle guide to facilitate aspiration of follicle fluid and oocytes and echo-reflecting tipped needles were developed. The combination placed high visibility needles in the imaging field facilitating direct imaging of the ovaries and follicles as the needle was advanced. Accurate tracking of the aspiration needles for follicle aspiration has contributed to the safety and effectiveness of transvaginal oocyte aspiration.327, 330, 331, 335, 336, 338, 339, 340, 341
Ultrasound-guided oocyte retrieval is now a routine in IVF.337 Oocyte retrieval is most often completed in a clinic setting using short-acting intravenous analgesia and/or conscious sedation for patient comfort. The woman can be awake and accompanied by her partner during the aspiration because she can remain awake and comfortable. A re-usable, sterile needle guide is attached to the ultrasound probe and inserted into the vagina. The ovaries are visualized and the dominant follicles identified. An aspiration needle is introduced via the guide, inserted through the vaginal fornix, and directed to the ovaries so that many ovarian follicles can be sequentially aspirated without reinsertion of the needle (Fig. 28). A biopsy guide-line may be set up on the ultrasound monitor to simplify needle insertion. Most aspiration needles are etched with a band of a highly reflective surface at the needle tip and the tip is easily visualized as it is directed into the ovary and maneuvered into each follicle. Follicle fluid containing the oocyte–cumulus complex is aspirated using gentle suction applied by a calibrated vacuum pump into a sterile tube until the follicle walls collapse. The needle can be moved within the follicle to ensure complete evacuation before moving to the next follicle. All follicles are aspirated in one ovary before the needle is withdrawn and re-inserted into the remaining ovary.
 Fig. 28. Ultrasound guided oocyte retrieval. The oocyte collection needle is visualized entering into a large follicle. Etching around the tip of the needle enhances its visualization. The image is presented in the standard medical imaging orientation. (Image courtesy of Dr Roger Stronell.)
Fig. 28. Ultrasound guided oocyte retrieval. The oocyte collection needle is visualized entering into a large follicle. Etching around the tip of the needle enhances its visualization. The image is presented in the standard medical imaging orientation. (Image courtesy of Dr Roger Stronell.)
Oocyte retrieval may be accomplished with either single or double lumen needles. Because double lumen needles have two parallel aspiration ports, they are larger in diameter and may create more discomfort than single lumen needles.337 Double lumen needles were introduced to allow a constant infusion of media into the follicle during aspiration from one lumen while the second lumen aspirated the follicle fluid and infused media. This approach ensures oocyte collection by establishing turbulent flow within the follicle and assists in dislodging or removing the oocyte–cumulus complex from the follicle wall. Single lumen needles are preferred by most centers as a simpler, less time consuming procedure that produces an equivalent rate of oocyte retrieval.337, 342, 343 When follicle flushing is desired with the use of a single lumen needle, the follicle is emptied by aspiration then medium is transferred into the follicle with a syringe through the same lumen. This is followed by re-aspiration. Turbulence can be created by a back-and-forth motion with the syringe plunger while the medium is introduced and is easily imaged. Complication rates of oocyte retrieval are quite low, likely because oocyte retrieval is completed with real-time ultrasound guidance.327, 332, 339, 344, 345, 346, 347, 348
THE EMPTY FOLLICLE SYNDROME
“Empty follicle syndrome” has been described as the failure to retrieve any oocytes at follicle aspiration for IVF. Failure to retrieve oocytes reportedly occurs in 1–7% of cycles.337, 349 Multifactorial technical and biological etiologies for empty follicle syndrome have been considered. It appears that biological conditions may contribute to poor follicle maturation and failure of the oocyte–cumulus complex to separate from the follicle wall in many cases. Other possible explanations include inappropriate dosage or time of administration of hCG, the trigger for follicle maturation and ovulation. Poor quality hCG medication also has been implicated. Alternatively, repetitive occurrences of empty follicle syndrome may point to an underlying ovarian dysfunction apparent only when oocyte retrieval for IVF was attempted.349 Faulty oocyte retrieval technique has been suggested as a cause for intraperitoneal or intraovarian loss of oocytes. Inappropriate timing for oocyte aspiration and insufficient aspiration pressure have been considered. The double lumen aspiration needles were introduced to free oocytes from the follicle walls and increase the probability of successful oocyte retrieval during ultrasound-guided IVF follicle aspiration; however, retrieval rates are nearly identical in most centers.
ULTRASOUND-GUIDED EMBRYO TRANSFER
Embryo transfer can be completed with ultrasound guidance or without by using a “clinical touch” technique. Clinicians remain divided in their opinion regarding the utility of each approach for embryo transfer.350, 351, 352, 353, 354, 355, 356, 357, 358 Ultrasound guidance may be used for all transfers, or may be used only during a mock transfer done prior to the IVF cycle. Alternatively, ultrasound guidance may be used in selected patients only when there is difficulty with the clinical touch approach.356, 358, 359 A randomized controlled trial and meta-analyses have suggested that transabdominal ultrasound-guided transfers significantly increased the rates of pregnancy but did not affect the rates of miscarriage, ectopic pregnancy, and multiple pregnancy.357, 360, 361, 362 Further evidence and clinical experience will be required before a consensus is reached regarding the best modality of embryo transfer that will optimize rates of implantation. When the clinical touch technique is used, a speculum is placed in the vagina to permit visualization of the cervix while the woman is in lithotomy position. Culture medium is used to cleanse the cervix and remove mucus secretions before inserting the embryo catheter. In the IVF laboratory, the embryo is placed in a transfer catheter within a small fluid droplet and moved from the laboratory to the patient for insertion into the uterine cavity.350, 356, 363, 364, 365, 366, 367, 368, 369, 370, 371 An adjustable marker on the catheter tubing is positioned approximately 4 cm from the catheter tip to correspond with an estimate of the length from the external to the internal os of the cervix. The marker is used to guide the depth of insertion of the catheter through the cervix into the uterus to avoid touching the fundus. Some clinicians complete a mock transfer to pre-determine the distance from the external cervix to the fundus of the uterine cavity and to rehearse the technique required for catheter insertion. Others may also use ultrasonography during the mock transfer to visualize the location of the catheter, and then use clinical touch during the embryo transfer.
Many clinicians prefer to use ultrasonography to guide their embryo transfers in the belief that this technique will increase the probability of conception. During ultrasound-guided transfers, a transvaginal ultrasound transducer is placed suprapubically on the lower abdomen to facilitate imaging through a partially filled urinary bladder.359, 369, 372The uterine cavity and cervix are easily recognized using a 3–4 MHz large aperture transducer which is positioned in a sagittal plane. The path of the transfer catheter can be imaged with ultrasonography during insertion. The embryo transfer catheter tip is visualized as two parallel hyperechoic lines outlining the small hypoechoic fluid pocket of culture medium containing embryos. The catheter tip is imaged in real-time and is used to guide the movement of the catheter through the cervix into the uterine cavity. An easy to image transfer catheter may be used to simplify imaging.373 This technique facilitates insertion and allows the clinician to place the embryos in the optimal site for implantation. The fluid droplet is easily visualized as it is slowly and gently expelled from the transfer catheter into the uterine cavity (Fig. 29).374 Transvaginal ultrasonography can be used in place of transabdominal imaging although it is not as widely used.370, 375 There is currently no consensus regarding the optimal position of embryo transfer within the uterine cavity.353, 354, 376, 377, 378
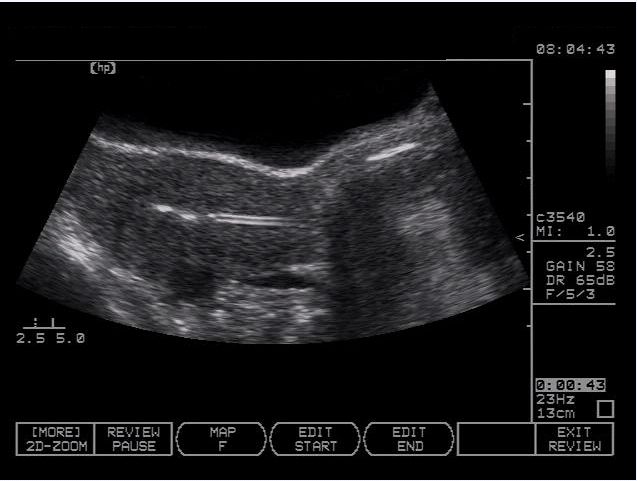 Fig. 29. Embryo transfer is enhanced by the use of ultrasound guidance to place the embryos at the optimal uterine location. The small hyperechoic areas distal to the catheter tip represent microbubbles of air expelled from the transfer pipette and serve to visualize embryo placement. (Image courtesy of Dr Roger Stronell.)
Fig. 29. Embryo transfer is enhanced by the use of ultrasound guidance to place the embryos at the optimal uterine location. The small hyperechoic areas distal to the catheter tip represent microbubbles of air expelled from the transfer pipette and serve to visualize embryo placement. (Image courtesy of Dr Roger Stronell.)
Endometrial assessment at the time of embryo transfer
Attempts to relate the endometrial thickness and pattern with the probability of implantation following IVF have been made in many studies.179 The literature on endometrial receptivity is abundant and contradictory. Definitive studies are required before we will be able to formulate any sort of conclusion regarding the predictive value of an endometrial assessment. Vascular and three-dimensional imaging studies also have been initiated to find markers for endometrial receptivity that may increase conception rates during ART therapies.
SPECTRAL DOPPLER AND COLOR FLOW DOPPLER ULTRASONOGRAPHY AS PREDICTORS OF UTERINE RECEPTIVITY
Doppler studies of the uterine arteries include spectral, color flow, and power modalities. The earliest studies using spectral Doppler analysis evaluated the resistance flow by measuring the pulsatility index (PI), resistance index (RI), maximum velocity (Vmax), and the systolic to diastolic ratio (S/D ratio).379 To detect directional motion of blood that moves either toward or away from an ultrasound transducer, color flow Doppler imaging is utilized and the motion is displayed as a color in real-time images. An overlay of all motion in all directions is displayed with power Doppler as a color overlay upon two- or three-dimensional ultrasound images.379, 380
Many investigators have been interested in the predictive value of uterine artery blood flow in ART imaging. RI for prediction of uterine receptivity has been examined in a small study, but no differences could be determined between women who conceived and those who did not conceive.381 The categorization of PI of the uterine arteries into low, medium or high resistance was not useful in distinguishing conception from nonconception cycles; however, it was apparent that no pregnancies occurred in the high PI group.382 A significantly lower pregnancy rate was seen in the 10% of patients who had an elevated PI, which can be considered a measure of the impedance of the uterine artery to vascular flow.383 In women who were completing cryopreserved embryo transfers, the RI was inconclusive, although a failure to conceive was associated with an absent or low diastolic flow and the PI was lower in women who became pregnant.384 When women completed IVF with GnRH downregulation, the uterine artery vascular impedance measured by RI, from the onset of stimulation until embryo transfer, was not capable of differentiating who would conceive during the treatment cycle.385 However, measurements prior to starting hMG showed a higher RI in women who did not conceive, and a PI of greater than 0.79 was presumed to indicate a poor uterine vasculature. Changing hormone states during stimulation cycles were reflected in the measurements. There was a trend towards an increase in resistance with downregulation and declining estradiol. A decrease in resistance occurred with estradiol elevation during follicle growth. A rise in resistance to flow was observed after hCG administration, whereas a decrease in resistance was noted following progesterone production. It is apparent that varying hormone states alter the resistance to blood flow.
In another IVF study, RI and PI were generally lower in conception cycles although there was an overlap in the confidence intervals.386 The lowest probability of conception (10% conception rate per embryo transfer, seen in 9% of the treatment cycles) was predicted by a PI greater than 3.3 and an RI greater than 0.95 before embryo transfer. This observation suggests that substantially increased uterine artery impedance could explain only some of the failed implantation that occurs following IVF. Similarly, an IVF-ICSI study also failed to demonstrate any differences between conception and nonconception for the PI on the day of embryo transfer.387 A critical review of literature prior to 1996 showed that some ultrasonographically detectable criteria were associated with negative pregnancy outcomes but measures of vascular perfusion did not have prognostic value.388 However, a lower PI was seen in women who conceived compared to those who did not conceive in a subsequent study.389
Color flow and power Doppler have been explored for their potential to predict the likelihood of conception following IVF. Color flow data were more predictive of conception than were measures of endometrial perfusion, where the PI and Vmax were not different between conception and nonconception cycles on the day of hCG administration.390 Absent subendometrial vascular flow, consistent with poor vascular penetration, was associated with failure of implantation. The influences of endometrial vascularity on IVF implantation rates assessed with color and power Doppler on the day of embryo transfer were interpreted to mean that sub- and intraendometrial vascular flow were mandatory to maintain a pregnancy.391, 392 Power Doppler imaging was used to correlate pregnancy rate with endometrial flow in women with an endometrial thickness of 10 mm or more by measuring the maximal area that showed evidence of endometrial motion: a color area less than 5 mm2 was associated with a lower pregnancy rate.391 There were no differences in spiral and uterine artery flow and the incidence of absent spiral artery flow in the endometrium between pregnant and nonpregnant women.393
IMAGING-BASED UTERINE SCORING SYSTEM
In the mid-1990s, a uterine scoring system was proposed to predict uterine sensitivity in the spirit of creating a uterine biophysical scoring system.394, 395 Points were assigned for various criteria which were then summed into an index. Uterine scores which included endometrial thickness, endometrial pattern, PI, RI, color Doppler, and other vascular indices were compared for women who did or did not conceive. The scoring system has not been adopted because no predictive value for the scoring system emerged.
THREE-DIMENSIONAL IMAGING OF THE ENDOMETRIUM
In the late 1990s, three-dimensional ultrasonography was introduced and has become a part of most advanced imaging systems. Because several methods are employed to provide three-dimensional information, studies using differing systems do not consistently compare similar endpoints or imaging techniques.396 Regardless, with the availability of three-dimensional imaging of the endometrium it has been possible to pursue new and potentially superior predictors of endometrial receptivity for implantation in ART.397
Endometrial volume on the day of embryo transfer was assessed by three-dimensional ultrasonography and correlated with conception. No general relationship was found that would predict conception in one study; however, another group found a lower rate of conception when the endometrial volume was less than 2 ml and no conceptions were observed when the volume was under 1 ml.397, 398 No predictive value was found for measurements of estradiol levels or endometrial thickness with endometrial volume.397, 398 In addition, the probability of pregnancy could not be correlated with either endometrial volume or thickness. Attention was then directed to three-dimensional power flow Doppler to consider endometrial perfusion as a predictor of conception.380, 393, 399, 400 The subendometrial flow index (FI) was the strongest predictive factor of IVF success. Three-dimensional spiral artery blood flow measurements performed at the onset of ovarian stimulation in women who conceived had a lower RI and higher three-dimensional FI compared with women who did not conceive.380[393 Three-dimensional ultrasonography has been useful to assess the endometrial volume following stimulation and the subendometrial flow prior to stimulation; however, a predictive index of the capacity to conceive has not been demonstrated.
ESTIMATES OF ENDOMETRIAL RECEPTIVITY: THREE-DIMENSIONAL ULTRASONOGRAPHY AND VASCULAR FLOW
Poor endometrial receptivity has been postulated to explain reduced or absent rates of implantation in women. Transvaginal color Doppler and three-dimensional power Doppler ultrasonography studies of uterine artery vascularity and endometrial volume were observed to identify markers for endometrial receptivity.380 A high PI in the uterine arteries was correlated with an absence of conception and a lower PI accompanied conception. In the subendometrial tissue, the three-dimensional vascular flow index of spiral arteries was higher and RI was lower with conception. Poststimulation, reduced three-dimensional endometrial volume was associated with a lower implantation rate. More endometrial perfusion on the day of embryo transfer was considered an indicator for endometrial receptivity. However, a healthy embryo physiologically capable of implantation with appropriate hormonal support is necessary for conception even when endometrial receptivity is present.
A large part of the capacity to conceive rests with the integrity of the embryo and the hormonal support of the endometrium. Therefore, it has been suggested that it is inappropriate to anticipate that imaging of the uterine tissues can predict all etiologies of implantation failure.401
Evidence for nonuterine factors contributing to implantation failure has been seen with the attrition of apparently healthy embryos supported in blastocyst culture media. If the uterine environment can be assessed with ultrasonography to exclude a potentially poor uterine environment, the clinician can divert attention elsewhere to improve conception rates. The prime candidates for intervention include hormonal support of the uterine environment and the combined influence of ovarian stimulation protocols and the laboratory support of gametes and embryos. Research in imaging needs to be directed at evaluating the effects of hormonal changes upon the uterus to optimize endometrial receptivity in women with detectable markers of a poor endometrium as defined by vascular indices and endometrial volume.
ANALYSIS OF UTERINE MOTION
Uterine motion can be easily seen as waves of uterine myometrial and endometrial contraction throughout the menstrual cycle.181, 402, 403, 404, 405, 406, 407, 408 Uterine contractions measured in the late follicular phase, at the time of hCG administration, oocyte retrieval, and in the early- and mid-luteal phases have shown a decline in contraction frequency from the late follicular to mid-luteal phase. The chronology is consistent with the timing of blastocyst transfer (7 days after hCG).409, 410, 411, 412, 413 It appears that contractions decrease in frequency under the influence of progesterone and it has been hypothesized that relaxation of the uterine musculature occurs at the time of anticipated implantation.405, 414
An analysis of uterine motion has been completed by capturing real-time digital images of the endometrium over a 5–10 minute interval. Computer analysis was completed using the pixel data from a single line of the endometrium, taken once or twice per second. Pixel data from the single line were concatenated and graphed to show the velocity and amplitude of endometrial contractions in a fashion conceptually similar to M-mode ultrasonography (Fig. 30). Uterine motion analyses have been correlated to conception rate. An analysis of subendometrial contractions was then initiated to predict patterns that were associated with successful conception and to determine how modulating contraction frequency might alter the probability of pregnancy.406, 409, 415, 410, 412 Lower pregnancy rates were associated with high frequency uterine contractions on the day of embryo transfer.406, 408, 415 However, another group reported no association between conception and the frequency of uterine contractions at any time during IVF therapy.416 Progesterone was perceived as the hormone responsible for a decline in the frequency of uterine contractions in the luteal phase. Progesterone supplementation after oocyte retrieval but prior to embryo transfer was postulated to enhance implantation by promotion of local vasodilatation, relaxation, and quiescence of the uterine muscle by inducing nitric oxide synthesis in the decidua and to reduce contractions responsible for expulsion or displacement of the embryo.413, 417, 414 The frequency of uterine contractions was affected by progesterone administration. An earlier decline in contraction frequency was observed when progesterone was initiated at the time of oocyte retrieval compared with a later start at the time of embryo transfer.413 However, no change in pregnancy rate was reported in a small study evaluating the initiation of progesterone on the day of retrieval and day 2 transfer.417 No evaluation has been reported that was designed to test the hypothesis that progesterone-induced decreases in uterine contractility will enhance implantation/conception at the time of blastocyst transfer or during cryopreserved embryo transfer cycles.
 Fig. 30. Motion analysis graph demonstrating endometrial contractility over time. The amplitude and frequency of the contractions may be easily visualized and measured.
Fig. 30. Motion analysis graph demonstrating endometrial contractility over time. The amplitude and frequency of the contractions may be easily visualized and measured.
Surveillance for ectopic pregnancy following assisted reproductive technologies
Ectopic implantation can occasionally occur following ART. Ectopic pregnancies have occurred concurrently with intrauterine pregnancies when multiple oocytes or embryos are available for implantation. Ectopic gestations can arise regardless of embryo transfer into apparently favorable areas within the uterine cavity.418 This may occur because of an inherent abnormality in the ectopic location that makes implantation possible, perhaps after infection has altered the surface anatomy of the ectopic site. Ectopic implantation may also occur because the embryo is able to move out of the uterine cavity. It is unclear whether specific transfer areas exist within the uterine cavity that favor intrauterine implantation. Alternatively, perhaps the process of introduction and removal of the transfer catheter and release of the embryo/fluid pocket are responsible for creating turbulence within the cavity that may predispose embryos to move to ectopic sites. Three-dimensional ultrasonography has been an ideal modality to investigate implantation and conception following embryo transfer and may be helpful in guiding embryo catheter placement to the optimal sites for embryo placement during transfer as well as elucidating uterine anatomical sites and transfer techniques that predispose to ectopic implantation.367, 419
CONCLUSION
Ultrasonography has advanced our knowledge of the physiology of the female reproduction and has permitted remarkable therapeutic advances in the management of infertility. The portability and remarkable technological advances of the instrumentation have allowed clinicians to employ rapid access to a high resolution imaging modality in a noninvasive manner. Imaging is being used for diagnostic purposes and has been integral in abbreviating the interval required to make a diagnosis of the etiology of infertility. Therapeutic protocols for infertility rely on rapid, accurate ultrasound imaging to direct changes in medication dosages and to plan the time for insemination and IVF procedures. The outcome of fertility therapies also involves ultrasound imaging, so that clinical pregnancy and gestation number can be determined and the course of pregnancy can be surveyed. Ultrasonography has allowed us to understand folliculogenesis, ovulation, luteal function, uterine response, conception, and implantation, and to apply this knowledge to explain and explore normal reproduction, infertility, and contraceptive technologies. As the technology of ultrasonography continues to evolve, we anticipate this indispensible tool will continue to shape our knowledge and enhance our ability to care for women.
REFERENCES
Hilgers, T. W., K. D. Daly, et al. (1992). "Cumulative pregnancy rates in patients with apparently normal fertility and fertility-focused intercourse." J Reprod Med 37(10): 864-6. |
|
Wilcox, A. J., C. R. Weinberg, et al. (1995). "Timing of sexual intercourse in relation to ovulation. Effects on the probability of conception, survival of the pregnancy, and sex of the baby." N Engl J Med 333(23): 1517-21. |
|
Mosher, W. and W. Pratt (1991). "Fecundity and infertility in the United States: Incidence and trends." Fertility and Sterility 56: 1517-1521. |
|
ASRM Guideline. Aging and infertility in women. Fertil Steril, 2006. 86(5 Suppl 1): p. S248-52. |
|
Belisle, S. and R. A. E. Pierson (2002). CFAS Consensus Document for the Investigation of Infertility. Montreal, Quebec, Canadian Fertility and Andrology Society. |
|
Chizen, D. R. and R. A. Pierson (2004). Tranvaginal Ultrasonography at First Consultation Assists Management of Infertility. International Federation of Fertility Societies18th World Congress on Fertility and Sterility, Montreal, Quebec, IFFS 2004. |
|
Timor-Tritsch, I. and S. Ruttem (1989). Transvaginal ultrasonography in the management of infertility. In: Kurjak A (ed) Ultrasound and Infertility. . Boca Raton, CRC Press. |
|
Erdem, M., A. Erdem, et al. (2003). "Age-related changes in ovarian volume, antral follicle counts and basal follicle stimulating hormone levels: comparison between fertile and infertile women." Gynecol Endocrinol 17(3): 199-205. |
|
Santoro, N., B. Isaac, et al. (2003). "Impaired folliculogenesis and ovulation in older reproductive aged women." J Clin Endocrinol Metab 88(11): 5502-9. |
|
Chow, G. E., A. R. Criniti, et al. (2004). "Antral follicle count and serum follicle-stimulating hormone levels to assess functional ovarian age." Obstet Gynecol 104(4): 801-4. |
|
Fossum, G., V. Davajan, et al. (1988). "Early detection of pregnancy with transvaginal ultrasound." Fertility and Sterility 49: 788-791. |
|
Goldstein, S., S. JR, et al. (1988). "Very early pregnancy detection with endovaginal ultrasound." Obstetrics and Gynecology(72): 200-204. |
|
Rempen, A. (1990). "Diagnosis of viability in early pregnancy with vaginal sonography." Journal of Ultrasound in Medicine 9: 711-715. |
|
Baerwald, A. R., G. P. Adams, et al. (2003). "Characterization of ovarian follicular wave dynamics in women." Biol Reprod 69(3): 1023-31. |
|
Baerwald, A. R., G. P. Adams, et al. (2003). "A new model for ovarian follicular development during the human menstrual cycle." Fertil Steril 80(1): 116-22. |
|
Gougeon, A. and B. Lefevre (1983). "Evolution of the diameters of the largest healthy and atretic follilces during the human menstrual cycle." Reproduction and Fertility 69: 497-502. |
|
Gougeon, A. (1993). Dynamics of human follicular growth: a morphologic perspective. Comprehensive Endocrinology: The Ovary. E. Adashi and P. Leung. New York, Raven Press: 21-39. |
|
Pellicer, A., P. Gaitin, et al. (1998). "Ovarian Follicular Dynamics: from basic science to clinical practice." Journal of Reproductive Immunology 39: 29-61. |
|
McGee, E. and A. Hsueh (2000). "Initial and Cyclic Recruitment of Ovarian Follicles." Endocrine Reviews 21(2): 200-214. |
|
Baerwald, A.R., R.A. Walker, and R.A. Pierson, Growth rates of ovarian follicles during natural menstrual cycles, oral contraception cycles, and ovarian stimulation cycles. Fertil Steril, 2009. 91(2): p. 440-9. |
|
Bomsel-Helmreich, O. (1985). "Ultrasound and the preovulatory human follicle." Oxford Rev Reprod Biol 7: 1-72. |
|
Hanna, M. D., D. R. Chizen, et al. (1994). "Characteristics of follicular evacuation during human ovulation." J Ultrasound Obstet Gynaecol 4: 488-493. |
|
Gougeon, A. (1979). "Qualitative changes in medium and large antral follicles in the human ovary during the menstrual cycle." Annals Biol Anim Bioch Biophys 19(5): 1464-1468. |
|
Baird, D. T. (1987). "A model for follicular selection and ovulation: Lessons from superovulation." J Steroid Biochem 27: 15-23. |
|
Adams, G. P., R. L. Matteri, et al. (1992). "Association between surges of follicle-stimulating hormone and the emergence of follicular waves in heifers." Journal of Reproduction and Fertility 94: 177-188. |
|
Adams, G. P. and R. A. Pierson (1995). "Bovine Model for Study of Ovarian Follicular Dynamics in Humans." Theriogenology 43: 113-120. |
|
Baerwald, A. R. and R. A. Pierson (2004). "Endometrial development in association with ovarian follicular waves during the menstrual cycle." Ultrasound Obstet Gynecol 24(4): 453-60. |
|
Ginther, O. J., E. L. Gastal, et al. (2004). "Comparative study of the dynamics of follicular waves in mares and women." Biol Reprod 71(4): 1195-201. |
|
Ginther, O. J., M. A. Beg, et al. (2005). "Systemic concentrations of hormones during the development of follicular waves in mares and women: a comparative study." Reproduction 130(3): 379-88. |
|
Ginther, O. J. (2000). "Selection of the dominant follicle in cattle and horses." Anim Reprod Sci 60-61: 61-79. |
|
Ginther, O. J., M. A. Beg, et al. (2001). "Follicle selection in monovular species." Biol Reprod 65(3): 638-47. |
|
Gougeon, A. (1986). "Dynamics of follicular growth in the human: A model from preliminary results." Hum Reprod 1: 81-87. |
|
Greenwald, G. S. and P. F. Terranova (1988). Follicular selection and its control. The Physiology of Reproduction. E. Knobil and J. Neill. New York, Raven Press: 387-446. |
|
Rezaei, E., A. R. Baerwald, et al. (2007). Ultrasonographic Image Analysis of Human Dominant and 1st Subordinate Ovarian Follicles. Proceedings of the 53rd Annual Conference of the Canadian Fertility and Andrology Society, Halifax, Nova Scotia, Canada, Canadian Fertility and Andrology Society |
|
Guraya, S. S. (1985). Biology of Ovarian Follicles in Mammals. New York, Springer-Verlag. |
|
Carson, R., J. Findlay, et al. (1986). "Relative levels of thecal blood flow in atretic and non-atretic ovarian follicles of the conscious sheep." Aust J Exper Biol Med Sci 64: 381-387. |
|
Moor, R. M. and R. F. Seamark (1986). "Cell signalling, permeability, and microvascular changes during follicle development in mammals. 69:927-943." J Dairy Sci 69: 927-943. |
|
Pierson, R. A. (1992). From ovulation to implantation. Color Doppler Imaging in Obstetrics and Gynecology. R. Jaffe and S. L. Warsof. New York, McGraw Hill, Inc.: 35-59. |
|
Pierson, R. and D. Chizen (1994). Ultrasonography of Normal and Aberrant Ovulation. Imaging in Infertility and Reproductive Endocrinology. R. Jaffe, R. Pierson and J. Abramowicz. Philadelphia, J.B. Lippincott: 155-166. |
|
Brannstrom, M., U. Zackrisson, et al. (1998). "Preovulatory changes of blood flow in different regions of the human follicle." Fertil Steril 69: 435-442. |
|
Kuspesic, S., L. Merce, et al. (2000). Colour Doppler studies from ovulation to implantation. An Illustrated Textbook and Reference for Clinicians. The Parthenon Publishing Group, New York |
|
Van Blerkom, J. (2000). "Intrafollicular influences on human oocyte developmental competence: perifollicular vascularity, oocyte metabolism and mitochondrial function." Hum Reprod 15 Suppl 2: 173-88. |
|
Borini, A., A. Maccolini, et al. (2001). "Perifollicular vascularity and its relationship with oocyte maturity and IVF outcome." Ann N Y Acad Sci 943: 64-7. |
|
Borini, A., A. Tallarini, et al. (2004). "Perifollicular vascularity monitoring and scoring: a clinical tool for selecting the best oocyte." Eur J Obstet Gynecol Reprod Biol 115 Suppl 1: S102-5. |
|
Shrestha, S. M., M. F. Costello, et al. (2004). "Longitudinal assessment of ovarian perifollicular and endometrial vascularity by power Doppler ultrasound in pregnant and non-pregnant cycles in the IVF setting." J Assist Reprod Genet 21(11): 387-95. |
|
Shrestha, S. M., M. F. Costello, et al. (2006). "Power Doppler ultrasound assessment of follicular vascularity in the early follicular phase and its relationship with outcome of in vitro fertilization." J Assist Reprod Genet 23(4): 161-9. |
|
Jayaprakasan, K., H. Al-Hasie, et al. (2008). "The three-dimensional ultrasonographic ovarian vascularity of women developing poor ovarian response during assisted reproduction treatment and its predictive value." Fertil Steril. |
|
Palomba, S., T. Russo, et al. (2008). "Perifollicular vascularity assessment for selecting the best oocytes for in vitro fertilization programs in older patients." Fertil Steril 90(4): 1305-9. |
|
Robson, S. J., M. Barry, et al. (2008). "Power Doppler assessment of follicle vascularity at the time of oocyte retrieval in in vitro fertilization cycles." Fertil Steril 90(6): 2179-82. |
|
Martinuk, S. D., D. R. Chizen, et al. (1992). "Ultrasonographic morphology of the human preovulatory follicle wall prior to ovulation." Clin Anat 5: 1-14. |
|
Abramowicz, J. S., R. Jaffe, et al. (1994). Transvaginal Color dopppler Ultrasonography in the Assessment of Uterine and Ovarian Blood Flow. In: Imaging in Infertility and Reproductive Endocrinology. R. Jaffe, R. A. Pierson and J. A. Abramowicz. Philadephia, J.B. Lippincott: 167-178. |
|
Van Blerkom, J., M. Antczak, et al. (1997). "The developmental potential of the human oocyte is related to the dissolved oxygen content of follicular fluid: association with vascular endothelial growth factor levels and perifollicular blood flow characteristics." Hum Reprod 12: 1047-1055. |
|
Vassena, R., G. P. Adams, et al. (2003). "Ultrasound image characteristics of ovarian follicles in relation to oocyte competence and follicular status in cattle." Anim Reprod Sci 76(1-2): 25-41. |
|
Siddiqui, M. A., M. Almamun, et al. (2009). "Blood flow in the wall of the preovulatory follicle and its relationship to pregnancy establishment in heifers." Anim Reprod Sci 113(1-4): 287-92. |
|
Acosta, T. J., K. G. Hayashi, et al. (2003). "Local changes in blood flow within the preovulatory follicle wall and early corpus luteum in cows." Reproduction 125(5): 759-67. |
|
Kan, A., E. H. Ng, et al. (2006). "Perifollicular vascularity in poor ovarian responders during IVF." Hum Reprod 21(6): 1539-1544. |
|
Palomba, S., T. Russo, et al. (2006). "Clinical use of the perifollicular vascularity assessment in IVF cycles: a pilot study." Hum Reprod 21(4): 1055-61. |
|
Leerentveld, R. A., I. VanGent, et al. (1985). "Ultrasonographic assessment of Graafian follicle growth under monofollicular and multifollicular conditions in clomiphene citrate stimulated cycles." Fertil Steril 40: 461-65. |
|
Hackelöer, B. J., R. Fleming, et al. (1979). "Correlation of ultrasonic and endocrinologic assessment of human follicular development." Am J Obstet Gynecol 135: 122-129. |
|
Nitschke-Dabelstein, S. and B. Hackelöer (1980). "Ovulation and corpus luteum formation observed by ultrasonography." Ultrasound in Medicine and Biology 1: 33-39. |
|
Queenan, J. T., G. D. O'Brien, et al. (1980). "Ultrasound scanning of ovaries to detect ovulation in women." Fertil Steril 34: 99-105. |
|
Lenz, S. (1985). "Ultrasonic study of follicular maturation, ovulation and development of corpus luteum during normal menstrual cycles." Acta Obstet Gynecol Scand 64(1): 15-9. |
|
Pierson, R., S. Martinuk, et al. (1990). Ultrasonographic visualization of human ovulation. 7th Reinier de Graaf Symposium, Maastricht, Netherlands, Excerpta Medica. |
|
Hanna, M. D., D. R. Chizen, et al. (1994). "Characteristics of follicular evacuation during human ovulation." J Ultrasound Obstet Gynaecol 4: 488-493. |
|
Baerwald, A. R., G. P. Adams, et al. (2005). "Form and function of the corpus luteum during the human menstrual cycle." Ultrasound Obstet Gynecol 25(5): 498-507. |
|
Stouffer, R. (1996). Corpus luteum formation and demise. Philadelphia. |
|
Parsons, A. K. (2001). "Imaging the human corpus luteum." J Ultrasound Med 20(8): 811-9. |
|
Bourne, T. H., H. Hagstrom, et al. (1996). "Ultrasound studies of vascular and morphological changes in the human corpus luteum during the menstrual cycle." Fertil Steril 65(4): 753-8. |
|
Guerriero, S., S. Ajossa, et al. (2005). "Luteal dynamics during the human menstrual cycle: new insight from imaging." Ultrasound Obstet Gynecol 25(5): 425-7. |
|
Geisthovel, F., U. Skubsch, et al. (1983). "Ultrasonographic and endocrinological studies of ovarian function." Ultrasound Med Biol Suppl 2: 603-8. |
|
Corner, G. W., Jr. (1956). "The histological dating of the human corpus luteum of menstruation." Am J Anat 98(3): 377-401. |
|
Hagstrom, H. G., M. Hahlin, et al. (1996). "Regulation of corpus luteum function in early human pregnancy." Fertil Steril 65(1): 81-6. |
|
Zalud, I. and A. Kurjak (1990). "The assessment of luteal blood flow in pregnant and non-pregnant women by transvaginal color Doppler." J Perinat Med 18(3): 215-21. |
|
Miyazaki, T., M. Tanaka, et al. (1998). "Power and colour Doppler ultrasonography for the evaluation of the vasculature of the human corpus luteum." Hum Reprod 13(1O): 2836-41. |
|
Jermy, K., C. Luise, et al. (2001). "The characterization of common ovarian cysts in premenopausal women." Ultrasound Obstet Gynecol 17(2): 140-4. |
|
de Silva, K. S., S. Kanumakala, et al. (2004). "Ovarian lesions in children and adolescents--an 11-year review." J Pediatr Endocrinol Metab 17(7): 951-7. |
|
Comerci, J. T., Jr., F. Licciardi, et al. (1994). "Mature cystic teratoma: a clinicopathologic evaluation of 517 cases and review of the literature." Obstet Gynecol 84(1): 22-8. |
|
Stuart, G. C. and J. P. Smith (1983). "Ruptured benign cystic teratomas mimicking gynecologic malignancy." Gynecol Oncol 16(1): 139-43. |
|
Phupong, V., T. Sueblinvong, et al. (2004). "Ovarian teratoma with diffused peritoneal reactions mimicking advanced ovarian malignancy." Arch Gynecol Obstet 270(3): 189-91. |
|
Maiti, S., Z. Fatima, et al. (2008). "Ruptured ovarian cystic teratoma in pregnancy with diffuse peritoneal reaction mimicking advanced ovarian malignancy: a case report." J Med Case Reports 2: 203. |
|
Bal, A., H. Mohan, et al. (2007). "Malignant transformation in mature cystic teratoma of the ovary: report of five cases and review of the literature." Arch Gynecol Obstet 275(3): 179-82. |
|
Caspi, B., U. Elchalal, et al. (1995). "Preoperative sonography in detecting small benign cystic teratomas." Int J Gynaecol Obstet 48(1): 75-8. |
|
Caspi, B., Z. Appelman, et al. (1997). "The growth pattern of ovarian dermoid cysts: a prospective study in premenopausal and postmenopausal women." Fertil Steril 68(3): 501-5. |
|
Yamanaka, Y., Y. Tateiwa, et al. (2005). "Preoperative diagnosis of malignant transformation in mature cystic teratoma of the ovary." Eur J Gynaecol Oncol 26(4): 391-2. |
|
Zalel, Y., B. Caspi, et al. (1997). "Doppler flow characteristics of dermoid cysts: unique appearance of struma ovarii." J Ultrasound Med 16(5): 355-8. |
|
Kurjak, A., S. Kupesic, et al. (2002). "Ultrasonic assessment of the peri- and postmenopausal ovary." Maturitas 41(4): 245-54. |
|
Fleischer, A. C., A. Lyshchik, et al. (2008). "Contrast-enhanced transvaginal sonography of benign versus malignant ovarian masses: preliminary findings." J Ultrasound Med 27(7): 1011-8; quiz 1019-21. |
|
Kupesic, S. and B. M. Plavsic (2006). "Early ovarian cancer: 3-D power Doppler." Abdom Imaging 31(5): 613-9. |
|
Kinkel, K., K. A. Frei, et al. (2006). "Diagnosis of endometriosis with imaging: a review." Eur Radiol 16(2): 285-98. |
|
ASRM, T. P. C. o. t. A. S. f. R. M. (2006). "Endometriosis and infertility." Fertility Sterility 86(suppl4): s156-60. |
|
ASRM, A. S. f. R. M. ( 1997). "Revised American Society for Reproductive Medicine classification of endometriosis: ." Fertil Steril 67: :817-21. |
|
Acien, P., G. Perez-Albert, et al. (2005). "Treatment of endometriosis with transvaginal ultrasound-guided drainage under GnRH analogues and recombinant interleukin-2 left in the cysts." Gynecol Obstet Invest 60(4): 224-31. |
|
Pinnelli, A. and M. Di Cesare (2005). "Human fertility: sociodemographic aspects." Contraception 72(4): 303-7. |
|
Dechaud H, Dechanet C, Brunet C, Reyffmann L, Hamamah S, Hedon B. Endometriosis and In vitro Fertilization: A Review. Gynecological Endocrinology 11:717-721 (2009) |
|
Kurjak, A., H. Shalan, et al. (1993). "Stage I ovarian cancer by transvaginal color Doppler sonography: a report of 18 cases." Ultrasound Obstet Gynecol 3(3): 195-8. |
|
Tarlatzis, B. C. and L. Zepiridis (2003). "Perimenopausal conception." Ann N Y Acad Sci 997: 93-104. |
|
Swanton, A. and T. Child (2005). "Reproduction and ovarian ageing." J Br Menopause Soc 11(4): 126-31. |
|
Allen, V. M., R. D. Wilson, et al. (2006). "Pregnancy outcomes after assisted reproductive technology." J Obstet Gynaecol Can 28(3): 220-50. |
|
Rowe, T. (2006). "Fertility and a woman's age." J Reprod Med 51(3): 157-63. |
|
Bukman, A. and M. J. Heineman (2001). "Ovarian reserve testing and the use of prognostic models in patients with subfertility." Hum Reprod Update 7(6): 581-90. |
|
Bukulmez, O. and A. Arici (2004). "Assessment of ovarian reserve." Curr Opin Obstet Gynecol 16(3): 231-7. |
|
Wallace, W. H. and T. W. Kelsey (2004). "Ovarian reserve and reproductive age may be determined from measurement of ovarian volume by transvaginal sonography." Hum Reprod 19(7): 1612-7. |
|
Broekmans, F. J., M. Faddy, et al. (2005). "Ovarian reserve and reproductive age may be determined from measurement of ovarian volume by transvaginal sonography." Hum Reprod 20(4): 1114-5; author reply 1115-6. |
|
Vladimirov, I. K., D. M. Tacheva, et al. (2005). "Prognostic value of some ovarian reserve tests in poor responders." Arch Gynecol Obstet 272(1): 74-9. |
|
Syrop, C. H., J. D. Dawson, et al. (1999). "Ovarian volume may predict assisted reproductive outcomes better than follicle stimulating hormone concentration on day 3." Hum Reprod 14(7): 1752-6. |
|
Bancsi, L. F., F. J. Broekmans, et al. (2002). "Predictors of poor ovarian response in in vitro fertilization: a prospective study comparing basal markers of ovarian reserve." Fertil Steril 77(2): 328-36. |
|
Erdem, A., M. Erdem, et al. (2002). "Age-related changes in ovarian volume, antral follicle counts and basal FSH in women with normal reproductive health." J Reprod Med 47(10): 835-9. |
|
Tufan, E., K. Elter, et al. (2004). "Assessment of reproductive ageing patterns by hormonal and ultrasonographic ovarian reserve tests." Hum Reprod 19(11): 2484-9. |
|
Lass, A., J. Skull, et al. (1997). "Measurement of ovarian volume by transvaginal sonography before ovulation induction with human menopausal gonadotrophin for in-vitro fertilization can predict poor response." Hum Reprod 12(2): 294-7. |
|
Lass, A. and P. Brinsden (1999). "The role of ovarian volume in reproductive medicine." Hum Reprod Update 5(3): 256-66. |
|
Bancsi, L. F., F. J. Broekmans, et al. (2004). "Impact of repeated antral follicle counts on the prediction of poor ovarian response in women undergoing in vitro fertilization." Fertil Steril 81(1): 35-41. |
|
Derman, S. G. and D. B. Seifer (2003). "In vitro fertilization in the older patient." Curr Womens Health Rep 3(5): 375-83. |
|
Durmusoglu, F., K. Elter, et al. (2004). "Combining cycle day 7 follicle count with the basal antral follicle count improves the prediction of ovarian response." Fertil Steril 81(4): 1073-8. |
|
Hendriks, D. J., B. W. Mol, et al. (2005). "Antral follicle count in the prediction of poor ovarian response and pregnancy after in vitro fertilization: a meta-analysis and comparison with basal follicle-stimulating hormone level." Fertil Steril 83(2): 291-301. |
|
Erdem, M., A. Erdem, et al. (2004). "Comparison of basal and clomiphene citrate induced FSH and inhibin B, ovarian volume and antral follicle counts as ovarian reserve tests and predictors of poor ovarian response in IVF." J Assist Reprod Genet 21(2): 37-45. |
|
Hansen, K. R., A. C. Thyer, et al. (2005). "Reproductive ageing and ovarian function: is the early follicular phase FSH rise necessary to maintain adequate secretory function in older ovulatory women?" Hum Reprod 20(1): 89-95. |
|
Rotterdam Consenus 2003 PCOS. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS) Hum Reprod 19 :(1) 41-47. |
|
Pache, T.D., et al., Ovarian morphology in long-term androgen-treated female to male transsexuals. A human model for the study of polycystic ovarian syndrome? Histopathology, 1991. 19(5): p. 445-52. |
|
Pache, T.D., et al., Ovarian morphology in long-term androgen-treated female to male transsexuals. A human model for the study of polycystic ovarian syndrome? Histopathology, 1991. 19(5): p. 445-52. |
|
Baerwald, A. R., R. A. Walker, et al. (2004). "Growth and Regression Rates of Ovarian Follicles during Natural Menstrual Cycles and Oral Contraception Cycles." Proceedings of the International Federation of Fertility Societies18th World Congress on Fertility and Sterility, Abstracts: 115. |
|
Baerwald, A.R., R.A. Walker, and R.A. Pierson, Growth rates of ovarian follicles during natural menstrual cycles, oral contraception cycles, and ovarian stimulation cycles. Fertil Steril, 2009. 91(2): p. 440-9. |
|
Carnevale, E., C. Checura, et al. (2002). The Use of Computer-Assisted Image Analysis to Determine the Interval Before and After Ovulation in Mares. 48th Annual Conference of the American Association of Equine Practitioners, Orlando, FL. |
|
Collins, W., D. Jurkovic, et al. (1991). "Ovarian morphology, endocrine function and intra-follicular blood flow during the peri-ovulatory period." Hum Reprod 6: 319-324. |
|
Tinkanen, H., E. Kujansuu, et al. (1995). "The association between hormone levels and vascular resistance in uterine and ovarian arteries in spontaneous menstrual cycles-a Doppler ultrasound study." Acta Obstet Gynecol Scand 74: 297-301. |
|
Balakier, H. and R. D. Stronell (1994). "Color Doppler assessment of folliculogenesis in in vitro fertilization patients." Fertil Steril 62: 1211-1216. |
|
Nargund, G., T. Bourne, et al. (1996). "Associations between ultrasound indices of follicular blood flow, oocyte recovery and preimplantation embryo quality." Hum Reprod 11: 109-113. |
|
Oyesanya, O. A., J. H. Parsons, et al. (1996). "Prediction of oocyte recovery rate by transvaginal ultrasonography and color Doppler imaging before human chorionic gonadotropin administration in in vitro fertilization cycles." Fertil Steril 65: 806-809. |
|
Lovrec, V. G., V. Vlaisavljevic, et al. (2001). "Dependence of the in-vitro fertilization capacity of the oocyte on perifollicular flow in the preovulatory period of unstimulated cycles." Wien Klin Wochenschr 113 Suppl 3: 21-6. |
|
Altundag, M., R. Levi, et al. (2002). "Intraovarian stromal artery Doppler indices in predicting ovarian response." J Reprod Med 47(11): 886-90. |
|
Goodarzi, M. O. and R. Azziz (2006). "Diagnosis, epidemiology, and genetics of the polycystic ovary syndrome." Best Pract Res Clin Endocrinol Metab 20(2): 193-205. |
|
Pache, T. D., W. C. Hop, et al. (1991). "Transvaginal sonography and abnormal ovarian appearance in menstrual cycle disturbances." Ultrasound Med Biol 17(6): 589-93. |
|
Dewailly, D., A. Duhamel, et al. (1993). "Interrelationship between ultrasonography and biology in the diagnosis of polycystic ovarian syndrome." Ann N Y Acad Sci 687: 206-16. |
|
Atiomo, W. U., S. Pearson, et al. (2000). "Ultrasound criteria in the diagnosis of polycystic ovary syndrome (PCOS)." Ultrasound Med Biol 26(6): 977-80. |
|
Glueck, C. J., R. Papanna, et al. (2003). "Incidence and treatment of metabolic syndrome in newly referred women with confirmed polycystic ovarian syndrome." Metabolism 52(7): 908-15. |
|
Goodarzi, M. O., S. Erickson, et al. (2003). "Relative impact of insulin resistance and obesity on cardiovascular risk factors in polycystic ovary syndrome." Metabolism 52(6): 713-9. |
|
Goodarzi, M. O. and S. G. Korenman (2003). "The importance of insulin resistance in polycystic ovary syndrome." Fertil Steril 80(2): 255-8. |
|
Ibanez, L., A. Ferrer, et al. (2004). "Insulin sensitization early after menarche prevents progression from precocious pubarche to polycystic ovary syndrome." J Pediatr 144(1): 23-9. |
|
Salmi, D. J., H. C. Zisser, et al. (2004). "Screening for and treatment of polycystic ovary syndrome in teenagers." Exp Biol Med (Maywood) 229(5): 369-77. |
|
Stoesser, K. (2004). "Treatment of polycystic ovary syndrome in adolescents." Am Fam Physician 70(3): 447. |
|
Chang, W. Y., E. S. Knochenhauer, et al. (2005). "Phenotypic spectrum of polycystic ovary syndrome: clinical and biochemical characterization of the three major clinical subgroups." Fertil Steril 83(6): 1717-23. |
|
Pettitt, D. J., P. H. Bennett, et al. (1991). "Abnormal glucose tolerance during pregnancy in Pima Indian women. Long-term effects on offspring." Diabetes 40 Suppl 2: 126-30. |
|
Mingrone, G., M. Manco, et al. (2008). "Influence of maternal obesity on insulin sensitivity and secretion in offspring." Diabetes Care 31(9): 1872-6. |
|
Mitchell, G. A. (2009). "Genetics, physiology and perinatal influences in childhood obesity: view from the Chair." Int J Obes (Lond) 33 Suppl 1: S41-7. |
|
Perez-Pastor, E. M., B. S. Metcalf, et al. (2009). "Assortative weight gain in mother-daughter and father-son pairs: an emerging source of childhood obesity. Longitudinal study of trios (EarlyBird 43)." Int J Obes (Lond). |
|
Wright, C. S., S. L. Rifas-Shiman, et al. (2009). "Intrauterine exposure to gestational diabetes, child adiposity, and blood pressure." Am J Hypertens 22(2): 215-20. |
|
Pache, T. D., J. W. Wladimiroff, et al. (1992). "How to discriminate between normal and polycystic ovaries: transvaginal US study." Radiology 183(2): 421-3. |
|
Jonard, S., Y. Robert, et al. (2003). "Ultrasound examination of polycystic ovaries: is it worth counting the follicles?" Hum Reprod 18(3): 598-603. |
|
Balen, A. H., J. S. Laven, et al. (2003). "Ultrasound assessment of the polycystic ovary: international consensus definitions." Hum Reprod Update 9(6): 505-14. |
|
Baillargeon, J. P., M. J. Iuorno, et al. (2003). "Insulin sensitizers for polycystic ovary syndrome." Clin Obstet Gynecol 46(2): 325-40. |
|
Barbieri, R. L. (2003). "Metformin for the treatment of polycystic ovary syndrome." Obstet Gynecol 101(4): 785-93. |
|
Haas, D. A., B. R. Carr, et al. (2003). "Effects of metformin on body mass index, menstrual cyclicity, and ovulation induction in women with polycystic ovary syndrome." Fertil Steril 79(3): 469-81. |
|
Lord, J. M., I. H. Flight, et al. (2003). "Metformin in polycystic ovary syndrome: systematic review and meta-analysis." Bmj 327(7421): 951-3. |
|
Seli, E. and A. J. Duleba (2004). "Treatment of PCOS with metformin and other insulin-sensitizing agents." Curr Diab Rep 4(1): 69-75. |
|
Tasdemir, S., C. Ficicioglu, et al. (2004). "The effect of metformin treatment to ovarian response in cases with PCOS." Arch Gynecol Obstet 269(2): 121-4. |
|
Hahn, S., S. Benson, et al. (2006). "Metformin treatment of polycystic ovary syndrome improves health-related quality-of-life, emotional distress and sexuality." Hum Reprod. |
|
Balen, A. (2000). "Ovulation induction for polycystic ovary syndrome." Hum Fertil (Camb) 3(2): 106-111. |
|
Sovino, H., T. Sir-Petermann, et al. (2002). "Clomiphene citrate and ovulation induction." Reprod Biomed Online 4(3): 303-10. |
|
Balen, A. (2003). "Ovulation induction - optimizing results and minimizing risks." Hum Fertil (Camb) 6(2 Suppl): S42-51. |
|
Qublan, H. S. and H. Y. Malkawi (2005). "Metformin in the treatment of clomiphene citrate-resistant women with high BMI and primary infertility: clinical results and reproductive outcome." J Obstet Gynaecol 25(1): 55-9. |
|
Amin, M., O. Abdel-Kareem, et al. (2003). "Minireview: Up-date management of non responder to clomiphene citrate in polycystic ovary syndrome." Kobe J Med Sci 49(3-4): 59-73. |
|
Cardone, V. S. (2003). "GnRH antagonists for treatment of polycystic ovarian syndrome." Fertil Steril 80 Suppl 1: S25-31; discussion S32-4. |
|
Chang, W. Y., E. S. Knochenhauer, et al. (2005). "Phenotypic spectrum of polycystic ovary syndrome: clinical and biochemical characterization of the three major clinical subgroups." Fertil Steril 83(6): 1717-23. |
|
Tessler, F. N., R. R. Perrella, et al. (1989). "Endovaginal sonographic diagnosis of dilated fallopian tubes." AJR Am J Roentgenol 153(3): 523-5. |
|
Strandell, A., A. Lindhard, et al. (2001). "Hydrosalpinx and IVF outcome: cumulative results after salpingectomy in a randomized controlled trial." Hum Reprod 16(11): 2403-10. |
|
Sabatini, L. and C. Davis (2005). "The management of hydrosalpinges: tubal surgery or salpingectomy?" Curr Opin Obstet Gynecol 17(4): 323-8. |
|
Richard, H. M., 3rd, R. B. Parsons, et al. (1998). "Torsion of the fallopian tube: progression of sonographic features." J Clin Ultrasound 26(7): 374-6. |
|
Baerwald AR, Adams GP, Pierson RA. Form and function of the corpus luteum during the human menstrual cycle. Ultrasound Obstet Gynecol. 2005 25(5):498-507. |
|
van den Driesche S, Smith VM, Myers M, Duncan WC. Expression and regulation of oestrogen receptors in the human corpus luteum. Reproduction. 2008 135(4):509-17. |
|
Wuttke W, Theiling K, Hinney B, Pitzel L. 1998. Regulation of steroid production and its function within the corpus luteum. Steroids 1998 63(5):299-305. |
|
Valentin L, Sladkevicius P, Laurini R, Söderberg H, Marsal K. Uteroplacental and luteal circulation in normal first-trimester pregnancies: Doppler ultrasonographic and morphologic study. Am J Obstet Gynecol. 1996 Feb;174(2):768-75. |
|
Fleischer, A. C., C. M. Herbert, et al. (1986). "Sonography of the endometrium during conception and nonconception cycles of in vitro fertilization and embryo transfer." Fertil Steril 46(3): 442-7. |
|
Fleischer, A. C., G. C. Kalemeris, et al. (1986). "Sonographic depiction of the endometrium during normal cycles." Ultrasound Med Biol 12(4): 271-7. |
|
Forrest, T. S., M. K. Elyaderani, et al. (1988). "Cyclic endometrial changes: US assessment with histologic correlation." Radiology 167(1): 233-7. |
|
Persadie, R. J. (2002). "Ultrasonographic assessment of endometrial thickness: a review." J Obstet Gynaecol Can 24(2): 131-6. |
|
Lindenberg, A. (1994). Ultrasonographic Assessment of the Endometrium during the Normal Menstrual Cycle. Imaging in Infertility and Reproductive Endocrinolgy R. Jaffe, R. A. Pierson and J. A. Abramowicz. Philadelphia, J.B. Lippincott: 47-61. |
|
Baerwald, A. R., R. A. Walker, et al. (2004). "Growth and Regression Rates of Ovarian Follicles during Natural Menstrual Cycles and Oral Contraception Cycles." Proceedings of the International Federation of Fertility Societies18th World Congress on Fertility and Sterility, Abstracts: 115. |
|
Baerwald, A. R., R. A. Walker, et al. (2004). "Growth Rates of Ovarian Follicles during Natural Menstrual Cycles and Ovarian Stimulation Cycles." Proceedings of the 50th Annual Conference of the Canadian Fertility and Andrology Society: 68. |
|
Fleischer, A. C. (1997). "Optimizing the accuracy of transvaginal ultrasonography of the endometrium." N Engl J Med 337(25): 1839-40. |
|
Pierson, R. (2003). "Imaging the Endometrium: Are There Predictors of Endometrial Receptivity? ." Journal of Obstetrics and Gynecology Canada 25: 360-368. |
|
Pierson, R. A. (2003). "Imaging the endometrium: are there predictors of uterine receptivity?" J Obstet Gynaecol Can 25(5): 360-8. |
|
de Vries, K., E. A. Lyons, et al. (1990). "Contractions of the inner third of the myometrium." Am J Obstet Gynecol 162(3): 679-82. |
|
Taylor, E. and V. Gomel (2008). "The uterus and fertility." Fertil Steril 89(1): 1-16. |
|
Malini, S., C. Valdes, et al. (1984). "Sonographic diagnosis and classification of anomalies of the female genital tract." J Ultrasound Med 3(9): 397-404. |
|
Daya, A. (1994). Ultrasonographic Evaluation of Uterine Anomalies. Imaging in Infertility and Reproductive Endocrinology. R. Jaffe, R. A. Pierson and J. A. Abramowicz. Philadelphia, J.B. Lippincott: 63-94. |
|
Reuter, K. L., D. C. Daly, et al. (1989). "Septate versus bicornuate uteri: errors in imaging diagnosis." Radiology 172(3): 749-52. |
|
Braun, P., F. V. Grau, et al. (2005). "Is hysterosalpingography able to diagnose all uterine malformations correctly? A retrospective study." Eur J Radiol 53(2): 274-9. |
|
Valdes, C., S. Malini, et al. (1984). "Ultrasound evaluation of female genital tract anomalies: a review of 64 cases." Am J Obstet Gynecol 149(3): 285-92. |
|
Salle, B., P. Sergeant, et al. (1996). "Transvaginal hysterosonographic evaluation of septate uteri: a preliminary report." Hum Reprod 11(5): 1004-7. |
|
Siedler, D., F. C. Laing, et al. (1987). "Uterine adenomyosis. A difficult sonographic diagnosis." J Ultrasound Med 6(7): 345-9. |
|
Lo, S. T., P. Ramsay, et al. (2008). "Endometrial thickness measured by ultrasound scan in women with uterine outlet obstruction due to intrauterine or upper cervical adhesions." Hum Reprod 23(2): 306-9. |
|
Yu, D., Y. M. Wong, et al. (2008). "Asherman syndrome--one century later." Fertil Steril 89(4): 759-79. |
|
Khopkar, U., R. M. Williams, et al. (2006). "Morbid adhesion of the placenta after hysteroscopic lysis of intrauterine adhesions." Fertil Steril 86(5): 1513 e1-3. |
|
Bellingham, F. R. (1996). "Intrauterine adhesions: hysteroscopic lysis and adjunctive methods." Aust N Z J Obstet Gynaecol 36(2): 171-4. |
|
Yang, J. H., M. J. Chen, et al. (2008). "Office hysteroscopic early lysis of intrauterine adhesion after transcervical resection of multiple apposing submucous myomas." Fertil Steril 89(5): 1254-9. |
|
Taniguchi, F. and H. Suginami (2008). "Pregnancy and delivery following sonohysterographic lysis to treat recurrence after hysteroscopic lysis of severe intrauterine adhesions: a case report." Clin Exp Obstet Gynecol 35(3): 215-7. |
|
March, C. M. and R. Israel (1981). "Gestational outcome following hysteroscopic lysis of adhesions." Fertil Steril 36(4): 455-9. |
|
Siegler, A. M. and V. G. Kontopoulos (1981). "Lysis of intrauterine adhesions under hysteroscopic control. A report of 25 operations." J Reprod Med 26(7): 372-4. |
|
Preutthipan, S. and V. Linasmita (2000). "Reproductive outcome following hysteroscopic lysis of intrauterine adhesions: a result of 65 cases at Ramathibodi Hospital." J Med Assoc Thai 83(1): 42-6. |
|
Tamai, K., K. Togashi, et al. (2005). "MR imaging findings of adenomyosis: correlation with histopathologic features and diagnostic pitfalls." Radiographics 25(1): 21-40. |
|
Atri, M., C. Reinhold, et al. (2000). "Adenomyosis: US features with histologic correlation in an in-vitro study." Radiology 215(3): 783-90. |
|
Bromley, B., T. D. Shipp, et al. (2000). "Adenomyosis: sonographic findings and diagnostic accuracy." J Ultrasound Med 19(8): 529-34; quiz 535-6. |
|
Atzori, E. (2003). "Sonography for the diagnosis of adenomyosis." Ultrasound Obstet Gynecol 21(6): 626-7. |
|
Dueholm, M. (2006). "Transvaginal ultrasound for diagnosis of adenomyosis: a review." Best Pract Res Clin Obstet Gynaecol. |
|
Lone, F. W., M. Balogun, et al. (2006). "Adenomyosis: not such an elusive diagnosis any longer." J Obstet Gynaecol 26(3): 225-8. |
|
Ascher, S. M., R. C. Jha, et al. (2003). "Benign myometrial conditions: leiomyomas and adenomyosis." Top Magn Reson Imaging 14(4): 281-304. |
|
Harmanli, O. H., S. A. Bevilacqua, et al. (2005). "Adenomyosis interferes with accurate ultrasonographic detection of uterine leiomyomas." Arch Gynecol Obstet 273(3): 146-9. |
|
Berghella, V., L. Pereira, et al. (2004). "Prior cone biopsy: prediction of preterm birth by cervical ultrasound." Am J Obstet Gynecol 191(4): 1393-7. |
|
Crane, J. M. and S. Healey (2006). "Use of misoprostol before hysteroscopy: a systematic review." J Obstet Gynaecol Can 28(5): 373-9 |
|
Parikh, R., S. Brotzman, et al. (2007). "Cervical lacerations: some surprising facts." Am J Obstet Gynecol 196(5): e17-8. |
|
Sung, P. L., K. C. Chao, et al. (2007). "Postconization cervical perforation during laparoscopic surgery." Taiwan J Obstet Gynecol 46(1): 71-2. |
|
Hefler, L., A. Lemach, et al. (2009). "The intraoperative complication rate of nonobstetric dilation and curettage." Obstet Gynecol 113(6): 1268-71. |
|
Melamed, N., A. Ben-Haroush, et al. (2009). "Intrapartum cervical lacerations: characteristics, risk factors, and effects on subsequent pregnancies." Am J Obstet Gynecol 200(4): 388 e1-4. |
|
Spitzer, M., A. E. Chernys, et al. (1998). "Indications for cone biopsy: pathologic correlation." Am J Obstet Gynecol 178(1 Pt 1): 74-9. |
|
El-Toukhy, T. A., S. Mahadevan, et al. (2001). "Cold knife cone biopsy--a valid diagnostic tool and treatment option for lesions of the cervix." J Obstet Gynaecol 21(2): 175-8. |
|
Miroshnichenko, G. G., M. Parva, et al. (2009). "Interpretability of excisional biopsies of the cervix: cone biopsy and loop excision." J Low Genit Tract Dis 13(1): 10-2. |
|
Althuisius, S. M., G. A. Dekker, et al. (2000). "Cervical incompetence prevention randomized cerclage trial (CIPRACT): study design and preliminary results." Am J Obstet Gynecol 183(4): 823-9. |
|
Guzman, E. R., A. M. Vintzileos, et al. (1997). "The natural history of a positive response to transfundal pressure in women at risk for cervical incompetence." Am J Obstet Gynecol 176(3): 634-8. |
|
Sherif, L. S. and H. M. Shalan (1997). "Detection of pregnant women at risk of cervical incompetence by transvaginal sonography during straining." J Obstet Gynaecol Res 23(4): 353-7. |
|
Takeda, S., K. Kuromaki, et al. (1997). "The management of cervical incompetence with protruded membranes into the vagina by vaginal irrigation with granulocyte elastase inhibitor: ulinastatin and PVP-iodine solution." J Obstet Gynaecol 17(1): 45-8. |
|
Campioni, P., S. Goletti, et al. (1998). "Diagnostic imaging in cervical incompetence." Rays 23(4): 637-48. |
|
Kassanos, D., E. Salamalekis, et al. (2001). "The value of transvaginal ultrasonography in diagnosis and management of cervical incompetence." Clin Exp Obstet Gynecol 28(4): 266-8. |
|
Drakeley, A. J., D. Roberts, et al. (2003). "Cervical stitch (cerclage) for preventing pregnancy loss in women." Cochrane Database Syst Rev(1): CD003253. |
|
Owen, J., J. D. Iams, et al. (2003). "Vaginal sonography and cervical incompetence." Am J Obstet Gynecol 188(2): 586-96. |
|
Higgins, S. P., L. H. Kornman, et al. (2004). "Cervical surveillance as an alternative to elective cervical cerclage for pregnancy management of suspected cervical incompetence." Aust N Z J Obstet Gynaecol 44(3): 228-32. |
|
Althuisius, S. M. and G. A. Dekker (2005). "A five century evolution of cervical incompetence as a clinical entity." Curr Pharm Des 11(6): 687-97. |
|
Tudur-Smith, C., A. L. Jorgensen, et al. (2005). "Individual patient data meta-analysis : Cervical stitch (cerclage) for preventing pregnancy loss in women." BMC Pregnancy Childbirth 5(1): 5. |
|
Chao, A. S., A. Chao, et al. (2008). "Ultrasound assessment of cervical length in pregnancy." Taiwan J Obstet Gynecol 47(3): 291-5. |
|
Acharya, G., B. Eschler, et al. (2006). "Noninvasive cerclage for the management of cervical incompetence: a prospective study." Arch Gynecol Obstet 273(5): 283-7. |
|
Audu, B. M., C. M. Chama, et al. (2003). "Complications of cervical cerclage in women with cervical incompetence." Int J Gynaecol Obstet 83(3): 299-300. |
|
Fliegner, J. R. (1997). "Emergency cervical cerclage for cervical incompetence." J Obstet Gynaecol 17(6): 602. |
|
Kurup, M. and J. W. Goldkrand (1999). "Cervical incompetence: elective, emergent, or urgent cerclage." Am J Obstet Gynecol 181(2): 240-6. |
|
Matijevic, R., B. Olujic, et al. (2001). "Cervical incompetence: the use of selective and emergency cerclage." J Perinat Med 29(1): 31-5. |
|
Althuisius, S. M., G. A. Dekker, et al. (2003). "Cervical incompetence prevention randomized cerclage trial: emergency cerclage with bed rest versus bed rest alone." Am J Obstet Gynecol 189(4): 907-10. |
|
Cockwell, H. A. and G. N. Smith (2005). "Cervical incompetence and the role of emergency cerclage." J Obstet Gynaecol Can 27(2): 123-9. |
|
Anthony, G. S., R. G. Walker, et al. (1997). "Transabdominal cervico-isthmic cerclage in the management of cervical incompetence." Eur J Obstet Gynecol Reprod Biol 72(2): 127-30. |
|
Kjollesdal, M., S. Nielsen, et al. (2005). "Laparoscopic cervico-uterine cerclage using polypropylene mesh for the treatment of cervical incompetence." Acta Obstet Gynecol Scand 84(8): 823-4. |
|
Althuisius, S., G. Dekker, et al. (2002). "Cervical Incompetence Prevention Randomized Cerclage Trial (CIPRACT): effect of therapeutic cerclage with bed rest vs. bed rest only on cervical length." Ultrasound Obstet Gynecol 20(2): 163-7. |
|
Althuisius, S. M., G. A. Dekker, et al. (2002). "Cervical incompetence: a reappraisal of an obstetric controversy." Obstet Gynecol Surv 57(6): 377-87. |
|
Sheiner, E., A. Bashiri, et al. (2004). "Preterm deliveries among women with MacDonald cerclage performed due to cervical incompetence." Fetal Diagn Ther 19(4): 361-5. |
|
Shepherd, J. H., R. A. Crawford, et al. (1998). "Radical trachelectomy: a way to preserve fertility in the treatment of early cervical cancer." Br J Obstet Gynaecol 105(8): 912-6. |
|
Abu-Rustum, N. R., N. Neubauer, et al. (2008). "Surgical and pathologic outcomes of fertility-sparing radical abdominal trachelectomy for FIGO stage IB1 cervical cancer." Gynecol Oncol 111(2): 261-4. |
|
Chuang, L. T., D. L. Lerner, et al. (2008). "Fertility-sparing robotic-assisted radical trachelectomy and bilateral pelvic lymphadenectomy in early-stage cervical cancer." J Minim Invasive Gynecol 15(6): 767-70. |
|
Abu-Rustum, N. R., N. Neubauer, et al. (2008). "Surgical and pathologic outcomes of fertility-sparing radical abdominal trachelectomy for FIGO stage IB1 cervical cancer." Gynecol Oncol 111(2): 261-4. |
|
Pareja, F. R., P. T. Ramirez, et al. (2008). "Abdominal radical trachelectomy for invasive cervical cancer: a case series and literature review." Gynecol Oncol 111(3): 555-60. |
|
Plante, M. (2008). "Vaginal radical trachelectomy: an update." Gynecol Oncol 111(2 Suppl): S105-10. |
|
Olawaiye, A., M. Del Carmen, et al. (2009). "Abdominal radical trachelectomy: Success and pitfalls in a general gynecologic oncology practice." Gynecol Oncol 112(3): 506-10. |
|
Wong, I., W. Justin, et al. (2009). "Assisted conception following radical trachelectomy." Hum Reprod 24(4): 876-9. |
|
Ishioka, S., T. Endo, et al. (2007). "Pregnancy-related complications after vaginal radical trachelectomy for early-stage invasive uterine cervical cancer." Int J Clin Oncol 12(5): 350-5. |
|
Jolley, J. A., L. Battista, et al. (2007). "Management of pregnancy after radical trachelectomy: case reports and systematic review of the literature." Am J Perinatol 24(9): 531-9. |
|
Lee, K. Y., H. A. Jun, et al. (2007). "Successful twin pregnancy after vaginal radical trachelectomy using transabdominal cervicoisthmic cerclage." Am J Obstet Gynecol 197(3): e5-6. |
|
Boss, E. A., R. J. van Golde, et al. (2005). "Pregnancy after radical trachelectomy: a real option?" Gynecol Oncol 99(3 Suppl 1): S152-6. |
|
Petignat, P., C. Stan, et al. (2004). "Pregnancy after trachelectomy: a high-risk condition of preterm delivery. Report of a case and review of the literature." Gynecol Oncol 94(2): 575-7. |
|
Grimbizis, G., M. Camus, et al. (2001). "Clinical implications of uterine malformations and hysteroscopic treatment results." Human Reproduction Update 7(1): 161-174. |
|
Medicine, P. C. o. t. A. S. f. R. (2004). "Optimal Evaluation of the Infertile Female." Fertility and Sterility 82(Supplement 1): S169-S172. |
|
Collins, J. and P. Woodward (1995). "Radiological evaluation of infertility." Seminars in Ultrasound, CT and MRI 16: 304-316. |
|
Alatas, C., E. Aksoy, et al. (1997). "Evaluation of intrauterine abnormalities in infertile patients by sonohysterography." Human Reproduction Update 12(3): 487-490. |
|
Wolman, I., A. Groutz, et al. (1999). "Timing of sonohysterography in menstruating women." Gynecol Obstet Invest 48(4): 254-8. |
|
Roma Dalfo, A., B. Ubeda, et al. (2004). "Diagnostic value of hysterosalpingography in the detection of intrauterine abnormalities: a comparison with hysteroscopy." AJR Am J Roentgenol 183(5): 1405-9. |
|
Simpson, W. L., Jr., L. G. Beitia, et al. (2006). "Hysterosalpingography: a reemerging study." Radiographics 26(2): 419-31. |
|
Hamilton, J. A., A. J. Larson, et al. (1998). "Routine use of saline hysterosonography in 500 consecutive, unselected, infertile women." Hum Reprod 13(9): 2463-73. |
|
Soares, S. R., M. M. Barbosa dos Reis, et al. (2000). "Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases." Fertil Steril 73(2): 406-11. |
|
Fleischer, A., J. Cullinan, et al. (1997). Special procedures in gynecology: Sonohysterography and Sonohysterosalpingography. New York, Lippincott, Williams & Williams. |
|
Dessole, S., M. Farina, et al. (2001). "Determining the best catheter for sonohysterography." Fertil Steril 76(3): 605-9. |
|
Schwarzler, P., H. Concin, et al. (1998). "An evaluation of sonohysterography and diagnostic hysteroscopy for the assessment of intrauterine pathology." Ultrasound Obstet Gynecol 11(5): 337-42. |
|
Exacoustos, C., E. Zupi, et al. (2003). "Hysterosalpingo-contrast sonography compared with hysterosalpingography and laparoscopic dye pertubation to evaluate tubal patency." J Am Assoc Gynecol Laparosc 10(3): 367-72. |
|
Sladkevicius, P., K. Ojha, et al. (2000). "Three-dimensional power Doppler imaging in the assessment of Fallopian tube patency." Ultrasound Obstet Gynecol 16(7): 644-7. |
|
Zalel, Y., D. Soriano, et al. (2000). "Contribution of color Doppler flow to the ultrasonographic diagnosis of tubal abnormalities." J Ultrasound Med 19(9): 645-9. |
|
Volpe, E., G. Zuccaro, et al. (1996). "Transvaginal sonographic tubal patency testing using air and saline solution as contrast media in a routine infertility clinic setting." Journal of Ultrasound in Obstetrics and Gynecology 7: 43-48. |
|
Chenia, F., G. J. Hofmeyr, et al. (1997). "Sonographic hydrotubation using agitated saline: a new technique for improving fallopian tube visualization." Br J Radiol 70(836): 833-6. |
|
Brown, S., C. Coddington, et al. (2000). "Evaluation of outpatient hysteroscopy, saline infusion hysterosonography, and hysterosalpingography in infertile women: a prospective, randomized study." Fertility and Sterility 74: 1029-1034. |
|
Sparac, V., S. Kupesic, et al. (2001). "Histologic architecture and vascularization of hysteroscopically excised intrauterine septa." J Am Assoc Gynecol Laparosc 8(1): 111-6. |
|
Lev-Toaff, A. S., L. W. Pinheiro, et al. (2001). "Three-dimensional multiplanar sonohysterography: comparison with conventional two-dimensional sonohysterography and X-ray hysterosalpingography." J Ultrasound Med 20(4): 295-306. |
|
Dietrich, M., A. Suren, et al. (1996). "Evaluation of tubal patency by hysterocontrast sonography (HyCoSy, Echovist) and its correlation with laparoscopic findings." J Clin Ultrasound 24(9): 523-7. |
|
Daya, S. (2003). "Methodologic pitfalls in assessing the efficacy of recombinant follicle-stimulating hormone versus human menopausal gonadotropin in assisted reproduction." Fertility and Sterility 80(5): 1100-1104. |
|
Tarlatzis, B. C., N. Laufer, et al. (1984). "The use of ovarian ultrasonography in monitoring ovulation induction." J In Vitro Fert Embryo Transf 1(4): 226-32. |
|
Requena, A., F. Neuspiller, et al. (2001). "Endocrinological and ultrasonographic variations after immature oocyte retrieval in a natural cycle." Hum Reprod 16(9): 1833-7. |
|
Nagai, S., T. Yasumizu, et al. (1997). "Effect of oocyte retrieval from a small leading follicle in fixed-schedule in vitro fertilization program." J Obstet Gynaecol Res 23(2): 165-9. |
|
van Gestel, I., M. M. Ijland, et al. (2005). "Endometrial waves in in vitro fertilization cycles: a validation study." Fertil Steril 83(2): 491-3. |
|
Kitai, H., N. Inagaki, et al. (1997). "A study on the correlation between maturation and quality of human oocytes." Hum Cell 10(4): 263-70. |
|
Salha, O., D. Nugent, et al. (1998). "The relationship between follicular fluid aspirate volume and oocyte maturity in in-vitro fertilization cycles." Hum Reprod 13(7): 1901-6. |
|
Huang, F. J., H. W. Huang, et al. (2002). "The maturity of human cumulus-free oocytes is positively related to blastocyst development and viability." J Assist Reprod Genet 19(12): 555-60. |
|
Merce, L. T., S. Bau, et al. (2006). "Assessment of the ovarian volume, number and volume of follicles and ovarian vascularity by three-dimensional ultrasonography and power Doppler angiography on the HCG day to predict the outcome in IVF/ICSI cycles." Hum Reprod 21(5): 1218-26. |
|
Lin, Y. C., S. Y. Chang, et al. (2003). "Human oocyte maturity in vivo determines the outcome of blastocyst development in vitro." J Assist Reprod Genet 20(12): 506-12. |
|
Picton, H. M., M. A. Danfour, et al. (2003). "Growth and maturation of oocytes in vitro." Reprod Suppl 61: 445-62. |
|
Triwitayakorn, A., S. Suwajanakorn, et al. (2003). "Correlation between human follicular diameter and oocyte outcomes in an ICSI program." J Assist Reprod Genet 20(4): 143-7. |
|
Russell, J. B. (1998). "Immature oocyte retrieval combined with in-vitro oocyte maturation." Hum Reprod 13 Suppl 3: 63-70; discussion 71-5. |
|
Thornton, M. H., M. M. Francis, et al. (1998). "Immature oocyte retrieval: lessons from unstimulated IVF cycles." Fertil Steril 70(4): 647-50. |
|
Russell, J. B. (1999). "Immature oocyte retrieval with in-vitro oocyte maturation." Curr Opin Obstet Gynecol 11(3): 289-96. |
|
Picton, H. M., S. E. Harris, et al. (2008). "The in vitro growth and maturation of follicles." Reproduction 136(6): 703-15. |
|
Baerwald, A. R., R. A. Walker, et al. (2009). "Growth rates of ovarian follicles during natural menstrual cycles, oral contraception cycles, and ovarian stimulation cycles." Fertil Steril 91(2): 440-9. |
|
Al-Shawaf, T. and J. G. Grudzinskas (2003). "Prevention and treatment of ovarian hyperstimulation syndrome." Best Pract Res Clin Obstet Gynaecol 17(2): 249-61. |
|
Delbaere, A., G. Smits, et al. (2004). "New insights into the pathophysiology of ovarian hyperstimulation syndrome. What makes the difference between spontaneous and iatrogenic syndrome?" Hum Reprod 19(3): 486-9. |
|
Delbaere, A., G. Smits, et al. (2005). "Understanding ovarian hyperstimulation syndrome." Endocrine 26(3): 285-90. |
|
DeCherney, A. H. and N. Laufer (1984). "The monitoring of ovulation induction using ultrasound and estrogen." Clin Obstet Gynecol 27(4): 993-1002. |
|
Rossavik, I. K. and W. E. Gibbons (1985). "Variability of ovarian follicular growth in natural menstrual cycles." Fertil Steril 44(2): 195-9. |
|
Zegers-Hochschild, F., C. Gomez Lira, et al. (1984). "A comparative study of the follicular growth profile in conception and nonconception cycles." Fertil Steril 41(2): 244-7. |
|
Singh, J., G. P. Adams, et al. (2003). "Promise of new imaging technologies for assessing ovarian function." Anim Reprod Sci 78(3-4): 371-99. |
|
Sarty, G. E. and R. A. Pierson (2005). "Mathematical Modelling of Ovarian Follicle Growth for the Prediction of Ovarian Response to Superstimulation." Mathematical Biosciences 198: 80-96. |
|
Smits, G., O. Olatunbosun, et al. (2003). "Ovarian hyperstimulation syndrome due to a mutation in the follicle-stimulating hormone receptor." N Engl J Med 349(8): 760-6. |
|
Avecillas, J. F., T. Falcone, et al. (2004). "Ovarian hyperstimulation syndrome." Crit Care Clin 20(4): 679-95, ix. |
|
Budev, M. M., A. C. Arroliga, et al. (2005). "Ovarian hyperstimulation syndrome." Crit Care Med 33(10 Suppl): S301-6. |
|
Delvigne, A. and S. Rozenberg (2003). "Review of clinical course and treatment of ovarian hyperstimulation syndrome (OHSS)." Hum Reprod Update 9(1): 77-96. |
|
Delvigne, A. and S. Rozenberg (2002). "Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review." Hum Reprod Update 8(6): 559-77. |
|
Aboulghar, M. (2009). "Prevention of OHSS." Reprod Biomed Online 19(1): 33-42. |
|
Pierson, R. and D. Chizen (1994). Ultrasonography of Normal and Aberrant Ovulation. Imaging in Infertility and Reproductive Endocrinology. R. Jaffe, R. Pierson and J. Abramowicz. Philadelphia, J.B. Lippincott: 155-166. |
|
Danninger, B., M. Brunner, et al. (1996). "Prediction of ovarian hyperstimulation syndrome by ultrasound volumetric assessment [corrected] of baseline ovarian volume prior to stimulation." Hum Reprod 11(8): 1597-9. |
|
Lass, A. (2003). "Monitoring of in vitro fertilization-embryo transfer cycles by ultrasound versus by ultrasound and hormonal levels: a prospective, multicenter, randomized study." Fertil Steril 80(1): 80-5. |
|
Orvieto, R. (2005). "Can we eliminate severe ovarian hyperstimulation syndrome?" Hum Reprod 20(2): 320-2. |
|
D'Angelo, A. and N. Amso (2002). ""Coasting" (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome." Cochrane Database Syst Rev(3): CD002811. |
|
D'Angelo, A. and N. N. Amso (2002). "Embryo freezing for preventing ovarian hyperstimulation syndrome: a Cochrane review." Hum Reprod 17(11): 2787-94. |
|
Chen, D., L. Burmeister, et al. (2003). "Ovarian hyperstimulation syndrome: strategies for prevention." Reprod Biomed Online 7(1): 43-9. |
|
Mansour, R., M. Aboulghar, et al. (2005). "Criteria of a successful coasting protocol for the prevention of severe ovarian hyperstimulation syndrome." Hum Reprod 20(11): 3167-72. |
|
Garcia-Velasco, J. A., V. Isaza, et al. (2006). "Coasting for the prevention of ovarian hyperstimulation syndrome: much ado about nothing?" Fertil Steril 85(3): 547-54. |
|
Fukaya, T., S. Chida, et al. (1994). "Treatment of severe ovarian hyperstimulation syndrome by ultrafiltration and reinfusion of ascitic fluid." Fertil Steril 61(3): 561-4. |
|
Delvigne, A. and S. Rozenberg (2002). "Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review." Hum Reprod Update 8(6): 559-77. |
|
Mikkelsen AL. Strategies in human in-vitro maturation and their clinical outcome. Reprod Biomed Online. 2005 May;10(5):593-9. |
|
Busso, C. E., J. Garcia-Velasco, et al. (2009). "Prevention of OHSS - dopamine agonists." Reprod Biomed Online 19(1): 43-51. |
|
Kol, S. and J. Dor (2009). "Prevention of OHSS: GnRH agonist versus HCG to trigger ovulation." Reprod Biomed Online 19(1): 59-60. |
|
Myrianthefs, P., C. Ladakis, et al. (2000). "Ovarian hyperstimulation syndrome (OHSS): diagnosis and management." Intensive Care Med 26(5): 631-4. |
|
Cobellis, L., E. Pecori, et al. (2003). "Ovarian hyperstimulation syndrome: distinction between local and systemic disease." Gynecol Endocrinol 17(2): 95-9. |
|
Jakimiuk, A. J., A. Fritz, et al. (2007). "Diagnosing and management of iatrogenic moderate and severe ovarian hyperstymulation syndrome (OHSS) in clinical material." Folia Histochem Cytobiol 45 Suppl 1: S105-8. |
|
Jayaprakasan, K., M. Herbert, et al. (2007). "Estimating the risks of ovarian hyperstimulation syndrome (OHSS): implications for egg donation for research." Hum Fertil (Camb) 10(3): 183-7. |
|
Chen, S. U., C. D. Chen, et al. (2008). "Ovarian hyperstimulation syndrome (OHSS): new strategies of prevention and treatment." J Formos Med Assoc 107(7): 509-12. |
|
Auslender, R., O. Lavie, et al. (2002). "Coiling of the ovarian vessels: a color Doppler sign for adnexal torsion without strangulation." Ultrasound Obstet Gynecol 20(1): 96-7. |
|
Ben-Ami, M., Y. Perlitz, et al. (2002). "The effectiveness of spectral and color Doppler in predicting ovarian torsion. A prospective study." Eur J Obstet Gynecol Reprod Biol 104(1): 64-6. |
|
Dellenbach, P., I. Nisand, et al. (1985). "Transvaginal sonographically controlled follicle puncture for oocyte retrieval." Fertil Steril 44(5): 656-62. |
|
Schulman, J. D., A. Dorfmann, et al. (1985). "Outpatient in vitro fertilization using transvaginal oocyte retrieval and local anesthesia." N Engl J Med 312(25): 1639. |
|
Cohen, J., C. Debache, et al. (1986). "Transvaginal sonographically controlled ovarian puncture for oocyte retrieval for in vitro fertilization." J In Vitro Fert Embryo Transf 3(5): 309-13. |
|
Hamberger, L., M. Wikland, et al. (1986). "Laparoscopy versus ultrasound guided puncture for oocyte retrieval." Acta Eur Fertil 17(3): 195-8. |
|
Hammarberg, K., L. Enk, et al. (1987). "Oocyte retrieval under the guidance of a vaginal transducer: evaluation of patient acceptance." Hum Reprod 2(6): 487-90. |
|
Russell, J. B., A. H. DeCherney, et al. (1987). "A new transvaginal probe and biopsy guide for oocyte retrieval." Fertil Steril 47(2): 350-2. |
|
Schulman, J. D., A. D. Dorfmann, et al. (1987). "Outpatient in vitro fertilization using transvaginal ultrasound-guided oocyte retrieval." Obstet Gynecol 69(4): 665-8. |
|
Feldberg, D., J. A. Goldman, et al. (1988). "Transvaginal oocyte retrieval controlled by vaginal probe for in vitro fertilization: a comparative study." J Ultrasound Med 7(6): 339-43. |
|
Gembruch, U., K. Diedrich, et al. (1988). "Transvaginal sonographically guided oocyte retrieval for in-vitro fertilization." Hum Reprod 3 Suppl 2: 59-63. |
|
Wikland, M., L. Enk, et al. (1988). "Oocyte retrieval under the guidance of a vaginal transducer." Ann N Y Acad Sci 541: 103-10. |
|
Wiseman, D. A., W. B. Short, et al. (1989). "Oocyte retrieval in an in vitro fertilization-embryo transfer program: comparison of four methods." Radiology 173(1): 99-102. |
|
Feichtinger, W. (1992). "Current technology of oocyte retrieval." Curr Opin Obstet Gynecol 4(5): 697-701 |
|
Kemeter, P. and W. Feichtinger (1986). "Trans-vaginal oocyte retrieval using a trans-vaginal sector scan probe combined with an automated puncture device." Hum Reprod 1(1): 21-4. |
|
Sterzik, K., W. Jonatha, et al. (1987). "Ultrasonically guided follicle aspiration for oocyte retrieval in an in vitro fertilization program: further simplification." Int J Gynaecol Obstet 25(4): 309-14. |
|
Yuzpe, A. A., S. E. Brown, et al. (1989). "Transvaginal, ultrasound-guided oocyte retrieval for in vitro fertilization." J Reprod Med 34(12): 937-42. |
|
Ragni, G., G. C. Lombroso, et al. (1991). "Echoguided transvaginal oocyte retrieval: effective and easy to learn technique." Acta Eur Fertil 22(2): 89-90. |
|
Kingsland, C. R., C. T. Taylor, et al. (1991). "Is follicular flushing necessary for oocyte retrieval? A randomized trial." Hum Reprod 6(3): 382-3. |
|
Knight, D. C., J. P. Tyler, et al. (2001). "Follicular flushing at oocyte retrieval: a reappraisal." Aust N Z J Obstet Gynaecol 41(2): 210-3. |
|
Barak, Y., J. B. Lessing, et al. (1988). "The development of an efficient ambulatory in vitro fertilization (IVF) and embryo transfer (ET) program using ultrasonically guided oocyte retrieval." Acta Obstet Gynecol Scand 67(7): 585-8. |
|
Christiaens, F., C. Janssenswillen, et al. (1998). "Comparison of assisted reproductive technology performance after oocyte retrieval under general anaesthesia (propofol) versus paracervical local anaesthetic block: a case-controlled study." Hum Reprod 13(9): 2456-60. |
|
Ng, E. H., B. Miao, et al. (2002). "Anxiolytic premedication reduces preoperative anxiety and pain during oocyte retrieval. A randomized double-blinded placebo-controlled trial." Hum Reprod 17(5): 1233-8. |
|
El-Shawarby, S., R. Margara, et al. (2004). "A review of complications following transvaginal oocyte retrieval for in-vitro fertilization." Hum Fertil (Camb) 7(2): 127-33. |
|
Tummon, I., C. Newton, et al. (2004). "Lidocaine vaginal gel versus lidocaine paracervical block for analgesia during oocyte retrieval." Hum Reprod 19(5): 1116-20. |
|
Bustillo, M. (2004). "Unsuccessful oocyte retrieval: technical artefact or genuine 'empty follicle syndrome'?" Reprod Biomed Online 8(1): 59-67. |
|
Kan, A. K., H. I. Abdalla, et al. (1999). "Embryo transfer: ultrasound-guided versus clinical touch." Hum Reprod 14(5): 1259-61. |
|
Lindheim, S. R., M. A. Cohen, et al. (1999). "Ultrasound guided embryo transfer significantly improves pregnancy rates in women undergoing oocyte donation." Int J Gynaecol Obstet 66(3): 281-4. |
|
Prapas, Y., N. Prapas, et al. (2001). "Ultrasound-guided embryo transfer maximizes the IVF results on day 3 and day 4 embryo transfer but has no impact on day 5." Hum Reprod 16(9): 1904-8. |
|
Coroleu, B., P. N. Barri, et al. (2002). "The influence of the depth of embryo replacement into the uterine cavity on implantation rates after IVF: a controlled, ultrasound-guided study." Hum Reprod 17(2): 341-6. |
|
Coroleu, B., P. N. Barri, et al. (2002). "The usefulness of ultrasound guidance in frozen-thawed embryo transfer: a prospective randomized clinical trial." Hum Reprod 17(11): 2885-90. |
|
Garcia-Velasco, J. A., V. Isaza, et al. (2002). "Transabdominal ultrasound-guided embryo transfer does not increase pregnancy rates in oocyte recipients." Fertil Steril 78(3): 534-9. |
|
de Camargo Martins, A. M., R. L. Baruffi, et al. (2004). "Ultrasound guidance is not necessary during easy embryo transfers." J Assist Reprod Genet 21(12): 421-5. |
|
Sallam, H. N. (2004). "Should embryo transfer always be performed under ultrasound guidance?" Ultrasound Obstet Gynecol 24(4): 383-6. |
|
Shamonki, M. I., S. D. Spandorfer, et al. (2005). "Ultrasound-guided embryo transfer and the accuracy of trial embryo transfer." Hum Reprod 20(3): 709-16. |
|
Matorras, R., E. Urquijo, et al. (2002). "Ultrasound-guided embryo transfer improves pregnancy rates and increases the frequency of easy transfers." Hum Reprod 17(7): 1762-6. |
|
Buckett, W. M. (2003). "A meta-analysis of ultrasound-guided versus clinical touch embryo transfer." Fertil Steril 80(4): 1037-41. |
|
Sallam, H. N. and S. S. Sadek (2003). "Ultrasound-guided embryo transfer: a meta-analysis of randomized controlled trials." Fertil Steril 80(4): 1042-6. |
|
Li, R., L. Lu, et al. (2005). "Abdominal ultrasound-guided embryo transfer improves clinical pregnancy rates after in vitro fertilization: experiences from 330 clinical investigations." J Assist Reprod Genet 22(1): 3-8. |
|
Strickler, R. C., C. Christianson, et al. (1985). "Ultrasound guidance for human embryo transfer." Fertil Steril 43(1): 54-61. |
|
Leong, M., C. Leung, et al. (1986). "Ultrasound-assisted embryo transfer." J In Vitro Fert Embryo Transf 3(6): 383-5. |
|
al-Shawaf, T., R. Dave, et al. (1993). "Transfer of embryos into the uterus: how much do technical factors affect pregnancy rates?" J Assist Reprod Genet 10(1): 31-6. |
|
al-Shawaf, T., D. Yang, et al. (1993). "Ultrasonic monitoring during replacement of frozen/thawed embryos in natural and hormone replacement cycles." Hum Reprod 8(12): 2068-74. |
|
Baba, K., O. Ishihara, et al. (2000). "Three-dimensional ultrasound in embryo transfer." Ultrasound Obstet Gynecol 16(4): 372-3. |
|
Coroleu, B., O. Carreras, et al. (2000). "Embryo transfer under ultrasound guidance improves pregnancy rates after in-vitro fertilization." Hum Reprod 15(3): 616-20. |
|
Rijnders, R. J., B. W. Mol, et al. (2000). "Use of ultrasound guidance during embryo transfer." Hum Reprod 15(11): 2449. |
|
Anderson, R. E., N. L. Nugent, et al. (2002). "Transvaginal ultrasound-guided embryo transfer improves outcome in patients with previous failed in vitro fertilization cycles." Fertil Steril 77(4): 769-75 |
|
Biervliet, F. P., P. Lesny, et al. (2002). "Transmyometrial embryo transfer and junctional zone contractions." Hum Reprod 17(2): 347-50. |
|
Tang, O. S., E. H. Ng, et al. (2001). "Ultrasound-guided embryo transfer: a prospective randomized controlled trial." Hum Reprod 16(11): 2310-5. |
|
Letterie, G. S., L. Marshall, et al. (1999). "A new coaxial catheter system with an echodense tip for ultrasonographically guided embryo transfer." Fertil Steril 72(2): 266-8. |
|
Mansour, R. T. and M. A. Aboulghar (2002). "Optimizing the embryo transfer technique." Hum Reprod 17(5): 1149-53. |
|
Kojima, K., M. Nomiyama, et al. (2001). "Transvaginal ultrasound-guided embryo transfer improves pregnancy and implantation rates after IVF." Hum Reprod 16(12): 2578-82. |
|
Hale, L. (2001). "Embryo transfer: how to ensure correct placement in utero." Reprod Fertil Dev 13(1): 95-8. |
|
Schoolcraft, W. B., E. S. Surrey, et al. (2001). "Embryo transfer: techniques and variables affecting success." Fertil Steril 76(5): 863-70. |
|
Pope, C. S., E. K. Cook, et al. (2004). "Influence of embryo transfer depth on in vitro fertilization and embryo transfer outcomes." Fertil Steril 81(1): 51-8. |
|
Zagzebski, J. (1996). Essentials of Ultasound Physics. New York, C.V. Mosby. |
|
Kupesic, S., I. Bekavac, et al. (2001). "Assessment of endometrial receptivity by transvaginal color Doppler and three-dimensional power Doppler ultrasonography in patients undergoing in vitro fertilization procedures." J Ultrasound Med 20(2): 125-34. |
|
Sterzik, K., D. Grab, et al. (1989). "Doppler sonographic findings and their correlation with implantation in an in vitro fertilization program." Fertil Steril 52(5): 825-8. |
|
Steer, C. V., S. Campbell, et al. (1992). "The use of transvaginal color flow imaging after in vitro fertilization to identify optimum uterine conditions before embryo transfer." Fertil Steril 57(2): 372-6. |
|
Serafini, P., J. Batzofin, et al. (1994). "Sonographic uterine predictors of pregnancy in women undergoing ovulation induction for assisted reproductive treatments." Fertil Steril 62(4): 815-22. |
|
Tekay, A., H. Martikainen, et al. (1995). "Blood flow changes in uterine and ovarian vasculature, and predictive value of transvaginal pulsed colour Doppler ultrasonography in an in-vitro fertilization programme." Hum Reprod 10(3): 688-93. |
|
Bassil, S., J. P. Magritte, et al. (1995). "Uterine vascularity during stimulation and its correlation with implantation in in-vitro fertilization." Hum Reprod 10(6): 1497-501. |
|
Cacciatore, B., N. Simberg, et al. (1996). "Transvaginal Doppler study of uterine artery blood flow in in vitro fertilization-embryo transfer cycles." Fertil Steril 66(1): 130-4. |
|
Aytoz, A., F. Ubaldi, et al. (1997). "The predictive value of uterine artery blood flow measurements for uterine receptivity in an intracytoplasmic sperm injection program." Fertil Steril 68(5): 935-7. |
|
Friedler, S., J. G. Schenker, et al. (1996). "The role of ultrasonography in the evaluation of endometrial receptivity following assisted reproductive treatments: a critical review." Hum Reprod Update 2(4): 323-35. |
|
Yokota, A., A. Nakai, et al. (2000). "Changes in uterine and ovarian arterial impedance during the periovulatory period in conception and nonconception cycles." J Obstet Gynaecol Res 26(6): 435-40. |
|
Zaidi, J., S. Campbell, et al. (1995). "Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program." Ultrasound Obstet Gynecol 6(3): 191-8. |
|
Yang, J., M. Wu, et al. (1999). "Association of endometrial blood flow as determined by a modified colour Doppler technique with subsequent outcome of in-vitro fertilization." Human Reproduction 14(6): 361-366. |
|
Maugey-Laulom, B., M. Commenges-Ducos, et al. (2002). "Endometrial vascularity and ongoing pregnancy after IVF." Eur J Obstet Gynecol Reprod Biol 104(2): 137-43. |
|
Schild, R. L., C. Knobloch, et al. (2001). "Endometrial receptivity in an in vitro fertilization program as assessed by spiral artery blood flow, endometrial thickness, endometrial volume, and uterine artery blood flow." Fertil Steril 75(2): 361-6. |
|
Applebaum, M. (1995). "The uterine biophysical profile." Ultrasound Obstet Gynecol 5(1): 67-8. |
|
Salle, B., V. Bied-Damon, et al. (1998). "Preliminary report of an ultrasonography and colour Doppler uterine score to predict uterine receptivity in an in-vitro fertilization programme." Hum Reprod 13(6): 1669-73. |
|
Pierson, R. A. (1999). Three-Dimensional Ultrasonography of the Embryo and Fetus. Fetal and Neonatal Ultrasonography. R. Jaffe and T. H. Bui. New York, Parthenon Publishing Group: 317-326. |
|
Raga, F., F. Bonilla-Musoles, et al. (1999). "Assessment of endometrial volume by three-dimensional ultrasound prior to embryo transfer: clues to endometrial receptivity." Hum Reprod 14(11): 2851-4. |
|
Schild, R. L., D. Indefrei, et al. (1999). "Three-dimensional endometrial volume calculation and pregnancy rate in an in-vitro fertilization programme." Hum Reprod 14(5): 1255-8. |
|
Schild, R. L., S. Holthaus, et al. (2000). "Quantitative assessment of subendometrial blood flow by three-dimensional-ultrasound is an important predictive factor of implantation in an in-vitro fertilization programme." Hum Reprod 15(1): 89-94. |
|
Wu, H. M., C. H. Chiang, et al. (2003). "Detection of the subendometrial vascularization flow index by three-dimensional ultrasound may be useful for predicting the pregnancy rate for patients undergoing in vitro fertilization-embryo transfer." Fertil Steril 79(3): 507-11. |
|
Kupesic, S. (2001). "The present and future role of three-dimensional ultrasound in assisted conception." Ultrasound Obstet Gynecol 18(3): 191-4. |
|
Martinez-Gaudio, M., T. Yoshida, et al. (1973). "Propagated and nonpropagated myometrial contractions in normal menstrual cycles." Am J Obstet Gynecol 115(1): 107-11. |
|
Lyons, E. A., P. J. Taylor, et al. (1991). "Characterization of subendometrial myometrial contractions throughout the menstrual cycle in normal fertile women." Fertil Steril 55(4): 771-4 |
|
Ijland, M. M., J. L. Evers, et al. (1996). "Endometrial wavelike movements during the menstrual cycle." Fertil Steril 65(4): 746-9. |
|
IJland, M. M., J. L. Evers, et al. (1997). "Velocity of endometrial wavelike activity in spontaneous cycles." Fertil Steril 68(1): 72-5. |
|
Fanchin, R., C. Righini, et al. (2000). "New look at endometrial echogenicity: objective computer-assisted measurements predict endometrial receptivity in in vitro fertilization-embryo transfer." Fertil Steril 74(2): 274-81. |
|
van Gestel, I., I. J. MM, et al. (2003). "Endometrial wave-like activity in the non-pregnant uterus." Hum Reprod Update 9(2): 131-8. |
|
Lesny, P. and S. R. Killick (2004). "The junctional zone of the uterus and its contractions." Bjog 111(11): 1182-9. |
|
Fanchin, R., C. Righini, et al. (1998). "Uterine contractions at the time of embryo transfer alter pregnancy rates after in-vitro fertilization." Hum Reprod 13(7): 1968-74. |
|
Lesny, P., S. R. Killick, et al. (1998). "Uterine junctional zone contractions during assisted reproduction cycles." Hum Reprod Update 4(4): 440-5. |
|
Fanchin, R., J. M. Ayoubi, et al. (2000). "Hormonal influence on the uterine contractility during ovarian stimulation." Hum Reprod 15 Suppl 1: 90-100. |
|
Fanchin, R., J. M. Ayoubi, et al. (2001). "Uterine contractility decreases at the time of blastocyst transfers." Hum Reprod 16(6): 1115-9. |
|
Fanchin, R., C. Righini, et al. (2001). "Effects of vaginal progesterone administration on uterine contractility at the time of embryo transfer." Fertil Steril 75(6): 1136-40. |
|
Bulletti, C. and D. de Ziegler (2005). "Uterine contractility and embryo implantation." Curr Opin Obstet Gynecol 17(3): 265-76. |
|
Fanchin, R., C. Righini, et al. (1998). "Uterine contractions at the time of embryo transfer alter pregnancy rates after in-vitro fertilization." Hum Reprod 13(7): 1968-74. |
|
Vlaisavljevic, V., M. Reljic, et al. (2001). "Subendometrial contractility is not predictive for in vitro fertilization (IVF) outcome." Ultrasound Obstet Gynecol 17(3): 239-44. |
|
Baruffi, R., A. L. Mauri, et al. (2003). "Effects of vaginal progesterone administration starting on the day of oocyte retrieval on pregnancy rates." J Assist Reprod Genet 20(12): 517-20. |
|
Sieck, U. V., K. A. Jaroudi, et al. (1997). "Ultrasound guided embryo transfer does not prevent ectopic pregnancies after in-vitro fertilization." Hum Reprod 12(9): 2081-2. |
|
Letterie, G. S. (2005). "Three-dimensional ultrasound-guided embryo transfer: a preliminary study." Am J Obstet Gynecol 192(6): 1983-7; discussion 1987-8. |