Circumcision: Ritual and Surgery
Authors
INTRODUCTION
At a time when reasoning from real facts and accurate observations has taken place of idle theory in almost every other science... no apology seems necessary for trying the same method of reasoning, on this important subject, which has hitherto been too much governed by arbitrary custom, and ignorant prejudice—Charles White (1728–1813), A Treatise on the Management of Pregnant and Lying-in Women, London: Dilly, 1773, viii.
In the United States, circumcision is a common and persistently controversial surgical procedure.1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 14, 15 Despite opposition, the majority of American male neonates still undergo circumcision.3, 4, 5, 16, 17, 18 The circumcision controversy has entered a new phase with the recent publication of several linking circumcision status, neonatal urinary tract infection (UTI)19 and the likelihood of HIV infection in high-risk populations.20, 21, 22 The risk/benefit ratio for both infant and adult circumcision is now more complex and demanding of careful analysis. The purpose of this chapter is to discuss the indications and contraindications for the performance of circumcision among neonates and in early infancy (before 2 months of age). Further, the techniques and potential complications of this surgery are considered and the possible benefits and risks of the operation are reviewed. While no resolution of the various controversies is likely, a critical review of the extant data is helpful in understanding the basic issues and the types and strength of the available experimental and clinical data concerning circumcision and its potential role as a medical therapy.
In Western medical practice, circumcision is defined as the surgical removal of the foreskin of the penis to near the coronal sulcus. This normally results in a penis where most or all of the glans is exposed while the organ is flaccid. The term circumcision is derived from the Latin root word, circumcidere, which means to “cut around.”23, 24 Historically, in other cultures, many different types of ritual genital surgery including types of circumcision have been performed on males—and in some instances on females—at varying ages.
It is difficult to present a balanced review of neonatal circumcision. Unbiased authors are a rarity. Many of the available articles, especially those intended for a lay audience, include strongly stated opinions that either do not cite scientific data or, more commonly, cite only selected papers supportive of one view. Also, the various medical authors interpret important papers in very different manners. It cannot be anticipated that any concensus view will emerge from a review of the literature. There are however, important new data for review which concern risks and benefits.
In this brief paper the aims of the author are to review the anatomy, physiology and scientific data concerning circumcision and to discuss new information. The aim is to assist in routine management and counseling. The persisting problem for clinicians is how to evaluate the myriad of claims and counter claims concerning circumcision in the effort to present a balanced view for parents when they question whether neonatal or childhood circumcision is an appropriate choice for their infant.
HISTORY AND CULTURAL PRACTICES OF CIRCUMCISION
Removal of the foreskin is a procedure of obscure origin, practiced for more than 5000 years in many cultures.3, 5, 6, 25, 26, 27, 28, 29, 30 Herodotus, in his description of Egypt, noted that circumcision was already an “ancient custom.” Circumcisions are routinely practiced in many African societies, among Arabs, and in some Pacific Islander societies. In the United States Jews constitute the major religious group that routinely performs ritual circumcision. Traditionally, male Jewish neonates undergo ritual circumcision at 8 days of age by a specially trained individual, the Mohel. For Jews, circumcision represents a covenant between man and God, marks the Jewish male as unique, and provides a physical sign of acceptance into his culture.5, 31 Circumcision performed on males—as well as occasionally females—at or near puberty is part of various culturally important rites de passage common in many non-Western societies.5, 23, 32 In recent years, much has been written concerning serious health problems resulting from the universally condemned practice of various types of female circumcision—a subject that is beyond the scop;e of chapter.33, 34, 35
Recent years have witnessed a lively controversy concerning the continuation of the practice of circumcision.1, 7, 8, 9, 10, 11, 23, 32, 36 Although much of this controversy simply repeats existing data, information reported in the past 10 years—specifically that concerning urinary tract infection (UTI) and possible AIDS prevention—has injected additional, predictably controversial information into the debate. Pediatric groups periodically review circumcision practice. The general conclusion is that there remains insufficient evidence for routine neonatal surgeries, but that there is potential benefit for some individuals in cases involving true phimosis, urinary tract infection (UTI) and recurrent balanitis.11, 37, 38
Although data on the performance of circumcision is difficult to obtain, it appears that male neonatal circumcision was relatively uncommon in North America until the turn of the 20th century.28 For many years, approximately 75% of males in the United States were routinely circumcised at birth with minimal criticism of the practice.11 Despite the controversy, the current circumcision rate for neonates remains approximately 60% in the United States. The frequency with which circumcision is performed varies by race, socioeconomic status, and locale.39 The operation is most common among whites of higher socioeconomic status who reside in the Midwest. Whether overall US rates are falling or staying essentially the same is another in the list of unsettled controversies in the circumcision issue. Overall, the rate for the operation probably has declined in recent years, especially in the Western world. Reliable US data are, however, difficult to obtain. A reasonable estimate is the 75% or more of male neonates in the US undergo circumcision.14 In Europe, the pattern of practice is quite different.
Circumcision in the UK was relatively popular up through the 1930s, when approximately one.- third of English neonates underwent the procedure.26, 40 The percentage of UK neonates who were circumcised fell to less than 10% in the 1950s with the advent of the National Health Service.41 After this time, circumcision was no longer a reimbursable procedure, and an increasingly critical view of the value of routine neonatal circumcision developed among practitioners.26 Currently, the procedure is infrequently performed and only 2–10% of UK neonates are circumcised.42
There is considerable variation among other countries. In most European countries, especially Scandinavia, circumcision is uncommonly performed at birth except for ritual reasons.43 In Canada, the incidence of neonatal circumcision had been 55–66%, but it now has dropped to between 35% and 40%.44 Circumcision has been relatively common in Australia, where approximately 40% of Australian males are circumcised.45 In 1979, circumcision rates for New Zealand averaged approximately 25%, reflecting a decline from the previous generation, where rates of circumcision approached 75%.46
INDICATIONS AND CONTRAINDICATIONS
Nonreligious, routine neonatal circumcision is commonly proposed for a number of reasons. These arguments include, but are not limited to, the following:
Avoidance of phimosis and paraphimosis in later life
Improvement in penile hygiene
A reduction in the incidence of neonatal UTI
Prophylaxis against balanitis (inflammation of the glans penis) or balanoposthitis (inflammation of the glans penis and prepuce)
Avoidance of penile carcinoma
A reduction in the incidence of cervical cancer
A reduction in the incidence of sexually transmitted diseases (STDs) including HIV infection
Social reasons
Neonatal circumcision is considered as an elective surgical procedure. As with all surgical operations, there are both potential indications and established contraindications. Important contraindications, among others, include known or suspected bleeding disorders, prematurity, or other circumstances where the condition of the child is either unstable or uncertain.29 Routine circumcision should not be performed until after the first 12 hours (and preferably 24 hours) of life.39, 47 It is obviously prudent not to perform circumcision if skin lesions suggestive of local infection are present. Circumcision also is contraindicated in neonates with an anomaly of the external genitalia because the prepuce may be needed for subsequent plastic repair.6 Thus, if after a dorsal slit is performed during a circumcision operation, a previously unrecognized anomaly of the glans is revealed, the procedure should be terminated and a urologist consulted. True symptomatic phimosis is an uncommon, even rare diagnosis in neonates and is virtually never a valid indication for a newborn circumcision procedure (see definitions, below). In contrast, as is discussed later, the operation may be medically indicated in certain children proved to be at high risk for UTI because of various anomalies of the upper urinary tract, specifically those involving either reflux or obstruction. The issue of prophylaxis against cancer and STD's is discussed below.
NATURAL HISTORY: PREPUCE
Before establishing any opinions in the circumcision controversy, some knowledge of the normal development and physiology of the foreskin is required.6, 7, 28, 48, 49, 50 Embryologically, the prepuce appears at 8 weeks' gestation as an epidermal ring that subsequently grows over the surface of the glans penis. By the 20th week, formation of the prepuce is complete, with coverage of the entire glans and development of the definitive urethral opening. Initially, there is no separation between the glans and the prepuce. The epithelial surfaces are fused and lined with stratified squamous epithelium. The separation between glans and prepuce is a slow process. A plane of division develops progressively, accompanying the production of desquamated cells and keratin. The epithelial layer between the glans and foreskin usually is incomplete at birth. Thus, it is normal for the foreskin to be nonretractable in most male neonates28, 51, 52: in only 4% of neonates can the foreskin be retracted; in nearly one half, even the external urethral meatus cannot be visualized.6 As the child ages, the plane between foreskin and glans progressively separates.26 At 6 months, the prepuce is retractable in 20% of boys. By the age of 5 or 6, only about 10% of males have a foreskin that cannot be easily retracted. By puberty the incidence is approximately 1%.48
Phimosis
Despite the physical appearance of the prepuce in prepubertal males, the inability to retract the foreskin does not establish the diagnosis of phimosis.6, 26, 28, 48, 49, 51, 53 Wright49 defines “true” phimosis as “an abnormal degree of narrowing of the preputial opening causing obstruction to urine flow, or nonretractability persisting well into childhood.” When phimosis is suspected in younger children, it has been reported that many boys are successfully treated by the application of topical steroids (e.g., 0.05% betamethasone valerate). It is less clear whether such therapy results in a permanent cure. An adequate circumcision is also curative.
In summary, these data indicate that a nonretractable foreskin in boys less than 3 years of age is a normal finding. Uncommonly, such nonretractability is due to true phimosis.26, 54 Phimosis, if diagnosed later in a child's life, may respond to medical as opposed to surgical treatment , at least in some cases.
Penile Hygiene
Hygiene is a common reason cited by both parents and health professionals as a reason for circumcision, but dismissed in importance by other, qualified observers.3, 26, 48, 55, 56 Genital hygiene is complicated by parental reticence in the instruction of children concerning best practices, incomplete knowledge information concerning the natural history of the foreskin, and sociocultural differences in identification of foreskin-related problems.57 Most mothers and a surprisingly number of health professionals have a poor understanding of routine male genital hygiene and the normal anatomy of the foreskin.17, 55, 58 An arguement for circumcision is that it improves cleanliness by making access to the glans and adjacent areas easier.5, 59 Those opposed to circumcision counter, however, that simple retraction of the foreskin (when appropriate and possible) and cleansing with soap and water are all that generally is required for adequate cleaning. Yet, it is far easier to promote genital cleanliness than to achieve it. Irritative and inflammatory disorders clearly are more common in those uncircumcised in childhood and early adolescence, although most of these problems are minor.57, 60 In some individuals, for example, those at a high risk for diabetes, a stronger case can be made for removal of the prepuce because later in life the risk of penile infection is greater than in nondiabetic men. Whether routine neonatal surgery is indicated at a time when there is only a theoretic risk of diabetes is, however, open to question.
Neonatal Urinary Tract Infection
A potential benefit to circumcision is a reduction in the incidence of neonatal urinary tract infection.14, 15, 19, 61, 62, 63, 64 A series of studies of varying quality and design suggest a 10-fold reduction (1.12 vs 0.11%) in UTI incidence in circumcised versus uncircumcised young boys. Although the available data may be fairly read to support the existence of this effect, the clinical importance of this observation and the strength of this argument as a basis for routine circumcision remains, predictably, controversial.19, 65
A possible beneficial effect of circumcision on the incidence of UTIs was observed by Ginsberg and McCracken in 1982.66 They reported that 85% of a series of 100 male infants less than 8 months of age with UTIs were not circumcised. They went on to speculate concerning the possible association between a child's foreskin status and UTI risk.
Following this report, Wiswell and associates61, 67, 68 and others69, 70, 71 made similar observations in a series of both prospective and retrospective studies of varying quality. Spach and colleagues72 published additional data concerning UTI incidence in sexually active young men, again suggesting a relationship between foreskin status and the incidence of UTIs.
As an example of this literature, Wiswell and Smith61 in an 18-month study reviewed the medical records of 5261 infants delivered in a military medical center. In this group, 1919 of 2502 (77%) male neonates had been circumcised within 24 hours of birth with the use of the Plastibell device. Four hundred neonates were subsequently evaluated for possible UTIs during their first year of life. None of the male infants in the study had phimosis or balanitis. Of this group, 41 were diagnosed as having UTI, as confirmed by urine culture. Lethargy, irritability, poor feeding, fever, vomiting, and diarrhea were used as clinical indicators of possible infection. Infants with known urogenital anomalies that could predispose them to UTI were excluded. The overall incidence of UTI among male infants during the first year of life was significantly greater than the incidence among female infants (p < 0.01). The incidence of UTI among uncircumcised male infants (24 in 585 = 4.12%) was significantly greater statistically than the incidence among circumcised male infants (4 in 1919 = 0.21%; p < 0.05). Female infants and circumcised male infants had a statistically equivalent incidence of UTI (0.47% and 0.21%, respectively).
In theory, exposing the urinary meatus through circumcision reduces bacterial contamination of the glans and prepuce, and thus the possibility of secondary ascending infection.57, 62, 73 UTI in male neonates results largely from bowel bacteria (predominantly Proteus mirabilis and Escherichia coli), which colonize the prepuce.73 In a small number of cases and under the correct circumstances (e.g. refux, obstruction), ascending infection of the urinary tract follows. Apparently the P.-fimbriated strains of E. coli—responsible for more than 90% of infant pyelonephritis infections—bind to the prepuce.73, 74 In microbiology, fimbriae are microscopic hair-like projections arising from bacteria. These fimbriae adhere to the mucosa of the urogenital tract by nonspecific hydrophobic or electrostatic binding or by specific binding to glycoproteins or glycolipid receptors.
There are potentially important consequences of neonatal infection. Chronic urinary infection is a potentially serious condition. Renal injury due to UTI occurs predominantly during the first years of life.5 Children afflicted with pyelonephritis have the potential to develop serious renal complications, including hypertension (10%) and end-stage renal disease (2–3%).
How are these data to be interpreted? The incidence of UTI in male neonales is low; however, such infections can be difficult to diagnose and, as noted above, occasionally result in permanent renal damage.66 Although the positive effect of circumcision in reducing the frequency of UTI in male neonates is generally accepted (see, however, the critique by Thompson74), a debate remains concerning the implications of these data as used to support a program of routine neonatal circumcision. On a population basis, this circumcision benefit is small—due largely to the low incidence of UTI among young males. A question is whether this benefit is sufficient to outweigh the risks of the original surgical procedure. Chessare75 discussed several of these points in an attempt to develop a decision model to evaluate routine circumcision. Most would probably concur that the case for circumcision as a prophylaxis against UTIs is best made for infants with anatomic abnormalities of the urinary tract (e.g., vesicoureteric reflux), or a past history of recurrent UTIs because they are at an increased risk of ascending infection.19, 76, 77 The situations for the outwardly normal male remains moot.
Penile Carcinoma
Penile carcinoma occurs primarily in men with poor genital hygiene who are more than 50 years old. The greatest incidence is seen in underdeveloped countries.74, 78 This disease is responsible for approximately 0.3–0.5% of malignancies among men, with an incidence of 0.5 to 1.4 per 100,000 men.79 The incidence may be slowly declining.80 In the United States, 750–1000 cases are reported yearly. Although other factors are also important, an element of chronic irritation or infection is commonly associated with penile cancer.56, 79, 81 Clinical findings of affected individuals usually include phimosis with or without balanitis.78 The incidence of phimosis among patients with cancer of the penis varies in reported cases from 40% to 70%.79, 82, 83 The tumor occurs largely—but not invariably—in uncircumcised men.3, 5, 8, 81, 84, 85, 86, 87, 88, 89
Penile tumors are normally squamous cell cancers.90 These tumors spread primarily via lymphatic drainage and by local invasion. The disorder is usually treated with partial or complete penectomy, with or without groin dissection. Radiation therapy also is administered occasionally. These tumors prove fatal in approximately one third of patients, usually owing to the advanced stage common at the time of diagnosis.81
The relationship of penile cancer to circumcision is interesting. There have been uncommon cases of carcinoma of the shaft or glans penis in patients who had undergone circumcision in childhood or later in life, and rare cases of cancer in those who were circumcised as neonates.81, 83, 88, 91, 92 However, in men circumcised at birth, fewer than 10 cases of penile cancer have been reported in world literature.83 In the total of 1624 patients with penile cancer in the combined series of Wolbarst,93 Dagher and coworkers,87 Hardner and associates,94 and Riveros and Gorostiaga,95 none had been circumcised in infancy.
As an example of a series of penile cancer patients who had been circumcised previously outside the neonatal period; Bissada and colleagues92 described 15 cases of squamous cell cancer among patients who were circumcised in their mid teens. These patients had neoplastic lesions located on the dorsum of the shaft, apparently arising from the site of prior circumcision scars. The majority of these men were from an isolated area of Saudi Arabia (13 of 15) and had undergone “aggressive circumcision” by local practitioners—a technique apparently no longer practiced. The authors speculated that extensive scarring at the operative site was an inciting factor in tumorigenesis. In addition, the unusual nature of these tumors and the strict localization—both to anatomic site and country of origin—imply the influence of unique hereditary and environmental factors.
Not all etiologic factors of penile carcinoma are established. Differences in incidence among different populations have been observed. Several behavioral factors (e.g., smoking) and a variety of medical conditions (e.g., poor hygiene, chronic phimosis, human papillomavirus [HPV] infection) are associated with penile cancer.69 Clinical observation over many years and the data on the apparent protective effect of circumcision suggest that chronic irritation or infection, which frequently accompany phimosis with balanitis are major factors predisposing persons to tumor development, The unsettled question is the mechanism. Here, certain observations are pertinent. An important irritant factor in tumorigenesis is smegma, the potentially carcinogenic secretion that collects under the foreskin in the uncircumcised male population. However, if the smegma hypothesis is true, it is puzzling why neonatal circumcision is largely protective against cancer, whereas circumcision later in life is not. Smegma usually is not observed until near puberty.
Other cofactors are important in the pathogenesis of penile cancer, including a history of HPV infection (genital warts), smoking, multiple sexual partners, and a history of prior penile rash or chronic dermatitis.78, 84, 96 Another association is low socioeconomic status.79, 97 In theory, certain of these risk factors may act in synergy in tumorigenesis. The viral theory of tumor initiation is of particular interest. Penile cancer shares certain common risk factors with female genital cancers.97 It is theorized that human genital cancers may arise from deficient cellular control of HPV gene expression—a process perhaps assisted by other events such as exposure to chemical carcinogens in tobacco smoke.98 Whether or not the HPV hypothesis proves correct as a risk factor for penile cancer, the available data do support the identification of certain additional risk factors such as smoking. The observed protective effort of foreskin removal on the incidence of penile cancer must be multifactorial. This is suggested by the data reported by Bissada and colleagues68 and by a study of the varying incidence among different human populations.
It has been suggested that the incidence of penile cancer is so low that the loss of life as a complication of circumcision exceeds that from the development of malignant penile tumors.99 This claim, however, cannot withstand critical review. The recorded yearly deaths from penile cancer in the United States exceed 200, but in a 25-year review of a number of studies there have been only two documented cases of death as a complication of neonatal circumcision.
It is incontestable that penile cancer is a serious disease with substantial yearly mortality; however, it is a rara avis. A critical evaluation of the possible benefit of circumcision in preventing penile carcinoma requires a review of lifetime risks for penile cancer in an identified population (uncircumcised males, from birth to 85 years of age or older), rather than yearly incidence statistics. As an example of this type of analysis, Kochen and McCurdy100 estimated the cumulative lifetime risk for penile carcinoma based on Third National Cancer Survey incidence data (1971) as 1 in 600, with a median age of occurrence of 67 years. Based on these data, and assuming circumcision prevents most but not all penile carcinomas, a minimum of 600 to 1000 neonatal procedures would have to be performed to avoid a single case of penile cancer and threefold as many to avoid a single cancer death.87, 101 The reported lifetime risk for Danish men is 1 in 909.101 Some caution is necessary in reviewing data on incidence of genital tumors. As Persky79 pointed out, there is some degree of uncertainty in the international comparative statistics for penile cancer. On this basis, critics have charged that some incidence figures quoted are far too high and based on inaccurate statistics. Nonetheless, while conceding that penlie cancer is an uncommon condition and that some problems exist with international comparative data, the available information may be fairly read to indicate substantial differences in incidence due to a number of factors including, but not limited to, circumcision.
How are these data to be interpreted? Analysis of the best available evidence suggests that Cancer of the penis is strongly associated with chronic irritation and infection as well as other risk factors, and that it occurs largely, but not invariably, in the uncircumcised population. Most, but not all reviewers concur that complete neonatal circumcision virtually excludes the risk for penile carcinoma.5, 32, 81, 84 Presumably circumcision reduces the incidence of inflammation, and perhaps alters other unrecognized cofactors. It has been claimed, but not proved, that high personal standards for genital hygiene alone provides similar protection against cancer.9, 102 Whether these data concerning the effects of circumcision on the incidence of penile cancer strengthen or weaken the case for neonatal circumcision depends on how this information is weighed in terms of benefits versus risks.
Circumcision and Cervical Cancer
Data concerning the relationship, if any, between cervical cancer and circumcision are confusing and contradictory.5, 84, 103, 104, 105, 106, 107, 108 Important known etiologic factors in cervical cancer include age at first intercourse, number of partners, frequency of intercourse, and HPV exposure. In theory, because foreskin status could affect viral carriage and the incidence of chronic penile infection, it might be a factor in female genital cancer. The problem is in identifying and then assessing the anatomy and penile hygiene of all of a woman's sexual partners over a prolonged period.109, 110 Any study connecting foreskin status and female genital cancer is unreliable unless the anatomy of the male partner is determined by actual examination. Further, there are variations in foreskin length in those never subjected to circumcision. Surprisingly, many men are uncertain whether they have ever undergone the operation; also, some men who have undergone a circumcision procedure still have foreskins partially covering the glans and thus are effectively uncircumcised.103, 111 Unfortunately, there are no standards for the evaluation of the extent of male circumcision. No reasonable conclusions can be reached from a review of these data except to state that an association between foreskin status and cervical carcinoma is unproved and, given the nature of the problem, perhaps unprovable.103, 105, 107, 108
Sexually Transmitted Diseases
The association between foreskin status and the transmission of STDs (e.g., HIV, syphilis, gonorrhea, herpes, chlamydia, HPV) remains complex.3, 10, 20, 21, 22, 110, 112, 113, 114 Anecdotal reports from military experience, and several studies from STD or military clinics suggest that the uncircumcised population has a higher incidence of STDs.3, 113, 114, 115 Other studies have noted no protective effects of circumcision and, in fact, a higher frequency of some disorders (e.g., genital warts, nongonococcal urethritis, and genital herpetic lesions) among the circumcised population.114, 116 Differences in marital status, sexual practices, level of education, use of condoms, frequency of exposure to STDs, and foreskin status strongly influence these data, and the available studies differ in how well such variables are accounted for in their statistical analyses.
There are now three published randomized clinical trials that indicate that male circumcision reduces new HIV infection by 50% or more.20, 21, 22 These impressive data have provided the impetus for reconsideration of adult circumcision as part of the anti-HIV programs in eastern and southern Africa in sites where HIV prevalence is high.117, 118 119 120 121 The theory is that the presence of a foreskin increases the risk of HIV infection due to lack of keratinization of the inner mucosal surface and the high density of HIV target cells at that area.122 It is perhaps not a surprise that the implications of these observations for changes in public policy remain controversial.123How might a difference in foreskin status influence the risk of STDs? Smith113 speculates that the prepuce may actually be protective against nongonococcal urethritis by providing both a physical and immunologic barrier to infection. Alternatively, it is argued that the circumcised population has a less favorable environment for the entrapment of irritative or infective particles under the foreskin and are thus at a reduced risk. In theory, repeated microtrauma to the intact foreskin during coitus might result in lesions that increase the risk of infectivity if the appropriate agent is present. Finally, preexisting balanitis in the uncircumcised population could injure tissue under the foreskin, thus predisposing these men to secondary infection.113 Other data strengthen the possible association between STDs and foreskin status. For example, although the carriage rate for Candida is apparently equal between the circumcised and uncircumcised populations, symptomatic infection is more common among those with a foreskin. It appears that a cost of being uncircumcised is a higher frequency of irritative and inflammatory disorders of the glans penis. It cannot be proved convincingly that circumcision provides protection against either syphilis or gonorrhea: however, recent data suggest that the risk of HIV infection is substantially reduced by circumcision, at least in selected high risk populations 20, 21, 22, 117
In summary, it remains unclear whether circumcision offers an effective protection against a variety of STDs. Although a substantial body of data suggest that it does, additional information is needed to reach firm conclusions.
Social Factors
Circumcision decisions are governed more by social norms, the foreskin status of the father, and cultural expectations than by pronouncements by health professionals, “foreskin crusaders,” or learned bodies.114, 116, 124, 125, 126 Herrara and associates126, 127 remarked on the social valuation of circumcision and counted it an important factor in influencing the decision to have the procedure performed. The desire of the family for a male child to be “like father” is often an important factor in influencing the parents to decide on circumcision. Critics suggest other, less laudatory motivations for circumcision.9, 128, 129 including ignorance and financial incentives to the practitioner.
THE CIRCUMCISION PROCEDURE
Circumcision is commonly performed with the use of either specially designed clamps or disposable plastic stents. Instruments commonly employed include the Gomco (Yellen)130 and Mogen clamps and the Plastibell. All of these devices are designed to isolate the foreskin from underlying structures, protecting the glans from injury. These devices are those most frequently employed in the United States. Many other specialized instruments for circumcision have been described, however.5
In this section, newborn circumcision with the Gomco clamp is discussed in detail. Much of the illustrated technique is the same, regardless of the type of clamp or stent chosen. As with other operative procedures, surgeons should master one technique fully, develop familiarity with an alternative approach for unusual circumstances and be prepared to manage complications. Regardless of the surgical method chosen, the requirements for initial parental counseling and consent, the appropriate choice of cases, meticulous aseptic technique, and adequate analgesia remain the same.
Pain Perception and Anesthetic Technique
There is good evidence that neonates perceive pain. Neonates respond to the stress of unanesthetized circumcision by increased cortisol levels131, 132 and various changes in biophysical behavior.133, 134, 135, 136, 137, 138, 139 Not surprisingly, neonates who receive adequate anesthesia or analgesia while undergoing circumcision cry less, are less agitated and have less perturbation in other biophysical parameters than those without.131, 140, 141 How best to achieve safe and adequate pain relief is the issue.
The routine use of an anesthetic for circumcision is strongly encouraged because substantial data now exists documenting safety.142 The literature includes descriptions of a number of simple techniques employing either local, injectable anesthetics or anesthetic creams or ointments.143, 144, 145, 146 Several recommendations are discussed below.
A brief review of the anatomy of the nerves to the penis is helpful in understanding modern techniques for blocking the perception of pain. Anatomically, the nerves serving the penis include the pudendal (S2–S4) nerve and the pelvic anatomic plexus. The principal nerve supply to the prepuce is provided by the dorsal branches of the pudendal nerve. At the penile root, the dorsal nerves, arteries, and veins are located anteriorly at the 2- and 10-o'clock positions, and lie 3–5 mm beneath the skin (Fig. 1). Ramifications of the nerve begin approximately 1 cm beyond the penile root. Thus, to be successful, a nerve block needs to be given anteriorly at the penile base, with particular attention to the avoidance of vascular injury. It also is possible to inject an anesthetic for a purely local block, as opposed to a nerve block145 or to apply a local anesthetic as a cream or gel.142, 143, 146, 147 The latter technique is discussed in greater detail below.
|
For several years we have employed a penile block technique using 0.5 mL or less of 1% or 0.5% lidocaine without epinephrine administered via a tuberculin syringe fitted with a fine-gauge needle (26–27 gauge). We usually dilute the standard 1% lidocaine solution with an equal volume of sterile saline and mix the solution by tilting the syringe. The skin around the base of the penile shaft is then cleansed, and a bleb of 0.2–0.4 mL of the 0.5% (or 1%. if preferred, lidocaine solution is injected subcutaneously at the 10- and 2-o'clock positions on both sides of the dorsal shaft140, 141, 148 (see Fig. 1). These injections usually result in a dense local block in 80–90% of cases; however, it is important to wait for 3–5 minutes after the drug is administered until the block is fully developed. As a practical matter, we usually prepare the lidocaine solution and make the injections as the first part of the procedure. Then we open the surgical kit, prep the operative field and arrange the instruments. Because these preliminaries consume several minutes, the anesthesia block usually is established by the time the surgeon is prepared to proceed with the operation.
Although injected local anesthetic has been used successfully for nerve block in a large number of cases with minimal evidence of complications, there are,however, several important precautions.131, 135, 136, 137, 140, 141, 144, 148, 149 The operator must be certain not to inject the drug into either the dorsal vein or artery because this could lead to adverse systemic reactions. Epinephrine containing solutions should never be used because of the possible risk of inducing acute penile ischemia.149 Only a short acting local anesthetic such as lidocaine should be used for injection, and the total volume should not exceed 1 mL of the 1% solution. Substantial data indicate that this dose is safe. Fontaine and co-workers144 have reported on 1022 cases of lidocaine dorsal nerve block. In this series, no instances of lidocaine toxicity, vascular compression, or voiding delays were observed. The complication rate was 1.2%. The problems consisted of 11 instances of minor, local ecchymoses at the injection site, with 1 case involving more significant bleeding. All of these proved to be of trivial clinical consequence.
Published experience with drugs other than lidocaine for neonatal circumcision is limited.140 Hematomas and gangrene of the skin at the glans have been reported when bupivacaine was used for a dorsal penile block.150 These cases involved older children (13 months and 3 years) undergoing circumcision with general anesthesia. The children subsequently received dorsal local anesthesia blocks for postoperative analgesia. In these cases, it is unclear whether it was the agent used, the technique of administration (i.e., vessel compression by use of excessive volume), or the surgical events that were responsible for the observed complications.150 Local injection of another local anesthetic, prilocaine, has been associated with methemoglobinemia.151, 152 The use of this drug as an injectable anesthetic should be avoided.
Topical anesthetics using either a 4% or a 30% lidocaine cream141, 143 or a eutectic mixture (i.e., with a melting point less than room temperature) of 2.5% prilocaine and 2.5% lidocaine prepared as an emulsion (EMLA Cream)153 also have been reported to be effective for circumcision.146 In this technique, approximately 0.1 mL EMLA cream is applied directly to the prepuce with a swab. The area treated is then covered with a lightly occlusive gauze dressing and left for 45–60 minutes before the procedure is attempted.9 As noted above, local injections of prilocaine should not be performed because of the risk of methemoglobinemia. Absorption of EMLA cream is safe in this regard. The prolonged period from EMLA cream administration until the anesthetic effect develops, however, makes this form of treatment much less practical then the injectable local anesthetics. Also, the EMLA induced anesthetic effect is less intense.142
There are other possible alternatives to the use of an injectable or topical anesthetic. Blass and Hoffmeyer154 described the use of a sucrose-flavored pacifier during circumcision. This technique appears to have some efficacy—at least as reflected in the observation of reduced neonatal crying during the procedure. Whether the positive effect observed was due to the sucrose acting by opioid mediation or to the benefits of nonnutritive sucking is less clear.145 Oral acetaminophen (10–15 mg/kg orally or 15–20 mg/kg rectally) also can be used to reduce postoperative pain. This compound has the advantage of proven efficacy and safety for treatment of noncircumcision-related pain.155 The one available placebo-controlled study of acetaminophen conducted in neonales undergoing circumcision, however, indicates that the drug is ineffective for operative and immediate postoperative discomfort, whereas it does retain some efficacy in controlling the discomfort that occurs several hours after surgery.156
To reprise, local anesthesia is strongly recommended. The data best supports the use of an injectible.139, 142 If an injectable local anesthetic is used there are several simple precautions to follow . Only non-epinephrine-containing solutions are used. The needle must neither enter the dorsal vein of the penis nor penetrate into the shaft itself. When the needle is inserted into the correct subcutaneous plane lateral to the penile shaft, the tip is easily movable, and little, if any, resistance to injection is noted when the plunger of the syringe is depressed. The needle tip should not be advanced beyond 0.5 cm below the skin surface. Care must also be taken to inject only small volumes of fluid, avoiding vessel injury by direct compression. The vessels at the site of injection are in a restricted compartment, and interference with penile circulation, though rare, is a possible complication if too large a volume is vigorously injected.46
Preoperative Management of the Neonate
Once an anesthetic has been chosen and administered, several other steps should be taken. Traditionally, to reduce the possibility of vomiting or aspiration, the child is denied oral intake for at least 1 hour preceding the operation. This is a reasonable precaution that we generally follow, but for which no reliable data exist. Not all experienced clinicians, however, follow this practice. Holding a neonate NPO for an excessive period of time may well be unnecessary, and hunger contributes to the child's overall distress.30 The easiest way to proceed is to simply perform the operation immediately prior to the next feeding.
Positioning of the infant for the procedure is important. Some of the discomfort the infant experiences during circumcision is due to restriction of movement and exposure to cold. When available, we prefer to use a plastic circumcision board fitted with Velcro restraints. Only the legs are restrained, not the upper extremities. Arm movement does not interfere with the procedure. We find that infants are less distressed when their arms are free. The circumcision board is positioned under a radiant heat source if available, to maintain warmth. If the restraint board is either not available or not desired, an assistant may simply hold the infant in a supine, frog-legged position for the operation. We favor having an assistant present during the procedure to provide either a finger or a pacifier to help soothe and reassure the infant during the operation as well as to obtain additional equipment or dressings for the surgeon, if required.
Surgical Technique
An important responsibility of the surgeon is to check the surgical instruments before beginning the procedure. The Gomco clamp includes a number of parts (bell, base, top plate with yoke, nut), and the operator should be confident that all are present and working correctly. Several technical problems may be encountered with the clamp, requiring the surgeon to request a new instrument before the surgery is attempted. The bell may become nicked or grooved by heavy use, the base plate may warp with age, the screw threads may not work easily, or the clamp may have been assembled with an incorrect bell size for the clamp base. Any of these reasons should prompt the surgeon to reject the clamp and request a replacement.
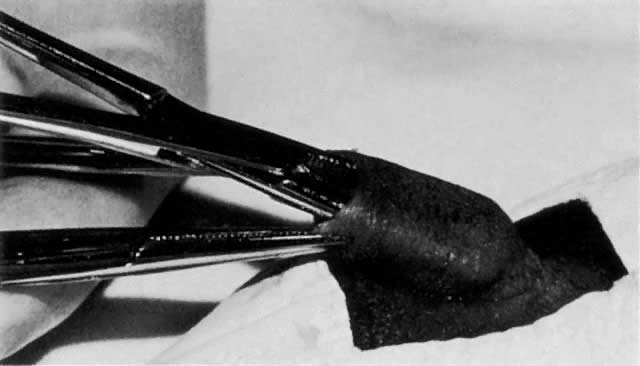
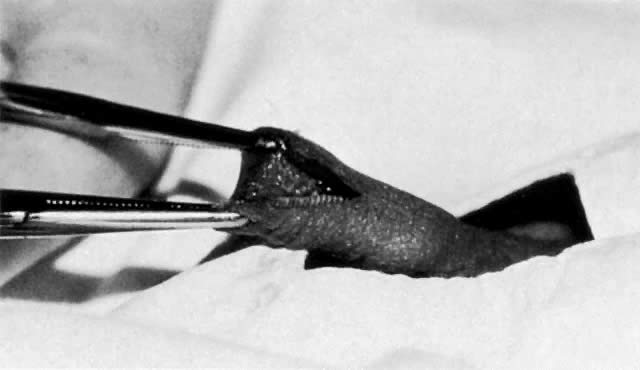
After correct positioning of the child is ensured, the genitalia are cleansed with a povidone-iodine solution or whatever skin preparation is standard for the institution. After the local anesthetic is administered and the instruments are checked, the surgeon proceeds with the operation. The operative field is draped. We favor a small triangular drape with a circular hole for the phallus. The extreme edges of the foreskin are first grasped with mosquito clamps, carefully avoiding trauma to the glans. Next, the plane between the glans and foreskin is developed by gentle dissection using a blunt probe or hemostat tip (Fig. 2). A dorsal slit is then performed. Using a straight mosquito-type hemostat, the anterior foreskin is crushed longitudinally in the midline. The clamp is removed, and the compressed area is divided with scissors. Because the clamp crushes the tissue, this is usually a bloodless incision (Fig. 3). In making the dorsal slit, close attention is paid to the posterior blade of the scissors to avoid damage to the meatus, which can result in a hypospadias or epispadias or possibly predispose the infant to subsequent fistula formation.30 Care is necessary in applying this initial clamp for another reason: The indentation made by the mosquito clamp for the dorsal slit serves as the marker for the length of skin to be excised from the shaft. The foreskin is quite flaccid and it is easy to mobilize excessive tissue, leading to an overestimate of the extent of skin to be drawn up in the Gomco clamp and removed. Excision of too much tissue results in inadvertent denuding of the shaft, which can necessitate secondary suturing. Kaplan6 described an alternative technique to judge the length of skin to be removed: The location of the coronal sulcus is simply marked on the skin of the penis with a pen before beginning the operation.
|
|
Once the dorsal slit is performed, the skin edges are grasped with fine-bladed clamps. The Gomco clamp bell is next inserted under the incised prepuce, entering the potential space between the glans and foreskin (Fig. 4). Usually some twisting and maneuvering is necessary to set the bell correctly. If the usually available bell size (1.3 cm) is too large, the smaller (1.1 cm) size clamp is substituted. The correct bell size for the overwhelming majority of neonates is 1.3 cm. The 1.1 cm bell is uncommonly needed; the 1.6-cm` clamp size is also available, but is virtually never required for neonatal procedures.
|

When correctly applied, the rim of the Gomco bell lies below the apex of the original dorsal slit, slightly distending the prepuce. Once the bell is in place, the clamp is assembled. The foreskin is carefully drawn up between the bell and body of the clamp using the mosquito hemostats. Once the Gomco is fully assembled and before compression is applied, the operator checks to be certain that the full length of foreskin marked by the original dorsal slit is drawn into the clamp and that the application is symmetric. If the apex of the original dorsal slit is not included in the skin removed, an unsightly cleft and a site for potential bleeding results. Once the surgeon is satisfied, and after assuring that the foot of the clamp is correctly inserted into the base plate, the finger nut of the clamp is firmly screwed in place. This crushes the foreskin between the bell and body of the clamp. The isolated, avascularized foreskin is then excised with a scalpel (Fig. 5). Electrocautery should never be used for this purpose because of the possibility of extensive injury to the penis. The clamp is left in place for several minutes to ensure hemostasis. Operators vary greatly in recommending how long the clamp should be allowed to remain.29 Yellen recommended waiting for 5 minutes;130 however, many surgeons remove the clamp immediately after completing the procedure.
|

After the clamp is disassembled and the bell teased off, the glans and shaft are observed carefully. Slight oozing is common. Persistent oozing from the glans is a common, minor complication due to the disruption of small vascular connections between the glans and the prepuce. Gentle pressure with a saline-moistened sponge for 2–5 minutes usually controls the ooze. Direct suturing of the glans is counterproductive and not recommended. Bleeding from the foreskin edge that is not responsive to simple pressure is best controlled by silver nitrate sticks, oxidized cellulose pledgets, orlocal thrombin applications combined with gentle pressure. If bleeding still persists, which is uncommon, the placement of several small sutures of 5–0 or 6–0 polyglycolic acid may be necessary. Suturing also is indicated if the skin edge has drawn away from the corona, revealing a raw or denuded area on the penile shaft. For many years bleeding that was unresponsive to simple pressure was treated with topical applications of epinephrine (solutions of 1:10,000 or less), applied to the gauze sponges used for compression. Recently, a controversy has developed about the routine use of such epinephrine-soaked sponges to control bleeding. An uncommon complication of this procedure is absorption, and systemic symptoms or evidence of local ischemia have been observed.157, 158 Such untoward reactions from local epinephrine applications are rare; however, we believe that simple, direct pressure and selective suturing remain the best treatments for postcircumcision bleeding, and conclude that epinephrine solutions should be used sparingly, if at all (see section on Complications of Circumcision, below).
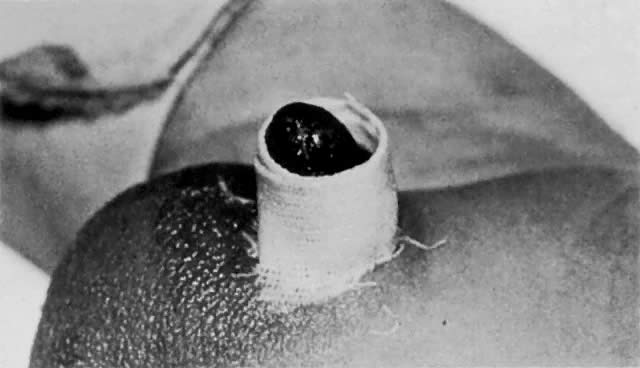
Once hemostasis is adequate, a nonocclusive gauze dressing impregnated with petroleum jelly is simply wound loosely around the penile shaft and glans to prevent adherence of the operative field to the diaper (Fig. 6). A constrictive dressing has the potential to obstruct either normal urination or penile blood flow.30, 159 The child is then comforted, rediapered, and returned to the mother for holding or feeding. Normally, we intermittently observe the operative site for 1 hour to be certain that hemostasis is adequate.
|
Providing the family with a prepared form outlining care of the penis during the healing phase is good practice.30 The parents are encouraged to call if questions or problems occur within the initial 24–48 hours. Circumcisions normally heal within several days. No specific care is required other than simply light washing. The best practice is to leave the original dressing on until it falls off. For several days, petroleum jelly or A and D ointment is applied lightly to the glans every time the diaper is changed. Parents should be instructed that adherent sebum or clot are not to be vigorously removed from the penis, but should simply be allowed to spontaneously dissolve. Petroleum jelly or A and D ointment from unit dose foil packets is applied to the glans as a dressing during the healing phase.
Circumcision also can be performed without the use of a crushing clamp. The Plastibell stent can be employed, or a “freehand” technique similar to that illustrated by Howat can be used.51 The latter technique is sometimes necessary if the circumcision is performed on a small child. In occasional cases where the infant's genitals are small, even the 1.1-cm Gomco clamp may prove simply too large. The best technique in such cases is to advance the foreskin beyond the glans and to crossclamp it, with special attention paid to avoiding injury to the unprotected glans. The redundant skin is then excised, and the operative site is examined for bleeding.
COMPLICATIONS OF CIRCUMCISION
In experienced hands, the immediate risks of circumcision are low but not completely negligible.5, 6, 28, 160, 161 The incidence of any complication related to circumcision is reported to vary from 0.1% to 55%.5, 54, 162, 163, 164, 165, 166 When outliers are excluded, the best overall estimate of the complication rate is between 2 and 10% with most problems being minor. The reasons for this remarkably wide variance include different methods of study, varying clinical definitions for certain complications (e.g., bleeding; see below), and type of follow-up performed. Most reported complications of circumcision are minor.57, 161 In the frequently-quoted studies of Wiswell and Hachey,68, 95, 152 cases performed in military hospitals were studied retrospectively, and an early complication rate of 0.19% was reported. The most frequent problems in this and most other series include bleeding, surgical trauma, and superficial infection. One should note that the incidence of complications reported in such hospital population studies generally do not accurately identify late-developing problems. Follow-up series involving large numbers of infants to judge both short- and long-term complications are not available.
Because different series define bleeding complications of circumcision in various ways, the reported incidence varies from 0.1% to 35%.6, 54 Serious blood loss is an uncommon problem. Shulman and colleagues164 reported bleeding as a cause for hospitalization in only 1 in 800 cases. In our experience, hemorrhage is virtually never a serious issue unless the child has a clotting deficiency or a skin separation from the glans has occurred. A family history of a bleeding disorder is a contraindication to the performance of elective circumcision. In this setting, no procedure should be considered until it is certain that the child has normal coagulation studies. As discussed above in the Surgical Technique section, the treatment for the vast majority of cases complicated by slight oozing is gentle, direct pressure with a saline-moistened sponge. More significant bleeding may require suturing or more prolonged compression with or without the use of silver nitrate sticks, coagulation-promoting agents, or vasoconstriction agents. The use of epinephrine-soaked pledgets to control postoperative ooze is best abandoned. However, if epinephrine is used, only dilute solutions should be applied for brief periods, and the child must be observed closely for local and systemic effects. As mentioned above, dressings encircling the shaft should be applied loosely; tight wrapping can cause obstruction either of vascular return from the glans or, potentially, of normal micturition.
Occasional wound infection is an inevitable consequence of circumcision, as it is with any surgical procedure.6, 162 The frequency of circumcision-related infection is not precisely known. Again, a great deal depends both on the definition used to establish this diagnosis and on operative technique. In a large series of cases, Gee and Ansell162 reported an incidence of clinical infection in 23 of 5521 cases (0.42%). Of these 23 infections, 19 (83%) were related to the Plastibell circumcision device; the remaining 4 were associated with Gomco clamp procedures. Of the 19 (21%) neonates with Plastibell-related infections, 4 had fever or irritability and 1 had positive blood cultures. Patel165 observed that 8% of the circumcisions performed in his series were “infected,” without defining the means of diagnosis. One infection was labeled “severe,” and antibiotics were administered; the remainder presumably responded to local measures. Rarely, unusually severe or life-threatening infections occur after circumcision. These include necrotizing fasciitis,167 Fournier's syndrome,168 septicemia and meningitis,169, 170, 171
Another possible surgical complication of circumcision is an inadequate operation.6 This includes a number of surgical misadventures, including either failure to remove enough skin or, more commonly, partial denuding of the shaft by excessive skin excision. If too much skin is removed, the remaining skin can retract, revealing a gap between the severed skin edge and the glans. In the most extreme cases, the shaft is virtually entirely denuded as well as a variable amount of the preputial epithelium, resulting in a pseudomicrophallus: the result is a concealed or “toad-in-the-hole” penis after healing.6, 51, 72, 172 This complication is generally easily managed initially, as long as there is no injury to the glans and the shaft is not entirely denuded. Bleeding sites from the edges are clamped and, if necessary, sutured. If the escaped skin edge can be sutured to the sulcus without marked distortion of the shaft, this is performed. If this is not possible or if for other reasons an adequate primary repair cannot be achieved either skin grafting is performed or the area is simply kept clean and allowed to granulate in.173 Occasionally, if too little skin is removed secondary phimosis results from formation of a circular cicatrix at the incised prepuce edge; recircumcision is required.
Bridging of the skin of the shaft to the glans can also occur.6, 174 Such adhesions can make erection painful and can result in skin tunnels where smegma accumulates and irritation or localized infection develops. It is unclear whether these adhesions result from incomplete separation of the glans from the prepuce during initial circumcision or develop secondarily as a restfit of injury of the glans with subsequent adherence of the penile skin during healing. If these lesions are symptomatic the treatment is simple excision.
Offsetting the apparent benefits from circumcision in reducing the risk of inflammation of the glans or foreskin is the occasional complication of inflammation of the urinary meatus. This is presumably due to exposure of the glans to ammonia splitting organisms in the neonate's diapers. It has been claimed that the incidence of mental inflammation in circumcised neonales varies from 5% to 30%. Meatitis may rarely result in symptomatic mental stenosis. The incidence of this disorder is impossible to estimate accurately, but it is clearly uncommon. Symptomatic meatal stenosis normally responds to passive dilation, and surgical revision is uncommonly required.175, 176
Long-term morbidity figures for circumcision are difficult to obtain because of the extremely varied means of reporting and study. Similarly, data on psychologic complications extending into later life are largely anecdotal and impossible to interpret. It must be stated that there are a substantial number of individuals who believe that circumcision has had an adverse effect on their lives.4, 9, 128, 129 Although the fervor of these beliefs cannot be denied, objective data is lacking. There are only anecdotal data and opinion (strong opinion usually) on the long-term effects of circumcision on male sexual function.16, 59, 177, 178, 179 It has been variously claimed that circumcision aids or hinders sexual performance and that the presence of foreskin is a barrier or asset to vaginal penetration.6, 179, 180 Perhaps not surprisingly, the lack of data has been no hindrance to speculation in the literature concerning this issue.
Other complications of circumcision are quite uncommon. These include meatal ulceration or stenosis: formation of fistulas between the urethra and the glans; various penile injuries, including injuries or amputation of the glans or shaft; serious infection6, 181; and bizarre complications, such as gastric rupture182 or keloid formation at the operative site.183 Obstructive uropathy from an occlusive dressing applied after circumcision also has been reported, as has dislocation of Plastibell rings, resulting in injury to the skin of the penile shaft.6, 184, 185 Auerbach and Scanlon186 reported a recurrent pneumothorax in a neonate circumcised at day 5 who had a spontaneous pneumothorax at birth. Presumably, infant distress and crying led to a recurrence. Inclusion cysts, penile lymphadenoma, and uterocutaneous fistulas also have been rarely reported.6 The ultimate complication for any surgical procedure is death. Neonatal circumcision has a mortality rate of approximately 1–2 per 1,000,000 procedures, owing largely to rare complications of serious infection or to general anesthesia. The latter is a problem for procedures performed outside the neonatal period.6, 100, 161, 166, 187
AVOIDANCE OF COMPLICATIONS
Most of the serious complications of circumcision are related to operator inexperience, undue haste in performance of the procedure, rare idiosyncratic reactions to drugs, or uncommon infections.5, 6, 163 Many, but not all of these problems are preventable. In large clinical centers, for reasons of convenience, circumcision often is assigned to the younger and frequently the most inexperienced members of the hospital staff. Thus, neophyte surgeons commit the classic errors in circumcision year after year. These procedures should be performed by those who are experienced, aware of potential problems, and prepared to handle complications. As noted, in experienced hands, the incidence of complications from circumcision, while never zero, is extremely low.
DISCUSSION
In considering the advisability of neonatal circumcision, several issues are pertinent. Does neonatal circumcision prevent or simply create problems? If there is a case to be made for neonatal circumcision, it must be made as a prophylactic measure. Neonates are remote from the period of life when STDs are an important issue or sexual performance is a major concern. Phimosis and inflammation are not a problem for uncircumcised neonates, and it is uncommon for foreskin problems to present substantial difficulties for the developing child. A related concern is the process whereby the parents make a life-long decision concerning the genital health and function of the child at a time when he is unable to participate in the decision. The issue hinges on whether it is appropriate to promote universal circumcision at a time of life when immediate indications are usually absent, or rather to perform circumcision only when it is indicated (e.g., a child at high risk for UTI) or as required later in life for specific medical problems.
Correctly performed neonatal circumcision does obviate the need for subsequent circumcision in childhood or adulthood, yet there remain cases in which either recircumcision or revision of the original procedure is required. Between 2% and 10% of uncircumcised males will require some form of foreskin procedure during their lifetime, usually for an inflammatory disorder (e.g., balanoposthitis). Most reviewers would accept recurrent balanoposthitis as an indication for circumcision in young males. The incidence of this condition is reported to be approximately 4% in boys aged up to 14 years, but not all of these cases will be recurrent. The etiology is not always determined; a specific organism is identified in only approximately 30% of cases.
There are data that can help place some of these risks and presumed benefits into perspective.3, 56, 57, 188 Fergusson and co-workers188 studied more than 500 New Zealand boys from birth to 8 years of age. The children were seen at birth, 4 months, and thereafter annually until 8 years of age as part of a larger study of child health and development that did not focus on the issue of circumcision. The results were interesting. During infancy, the incidence of penile problems when considered in the large categories of inflammation, phimosis, inadequate circumcision requiring revision, or postoperative infection after circumcision was higher among the circumcised boys. By ages 1 through 8 years, however, the incidence of these complications was higher among the uncircumcised boys. Most of these problems were described as “relatively minor,” and 64% were resolved after a single medical consultation.
Herzog and Alverezs retrospectively studied 545 children aged 4 months to 12 years. Of this group, 272 were uncircumcised and 273 had been circumcised at birth. Foreskin problems occurred in 14.3% of the uncircumcised subjects. Balanitis and irritation were the most common complaints. Complications were reported in 5.9% of the circumcised subjects. The authors reported that most complications were minor, although paraphimosis and symptomatic phimosis occurred in seven uncircumcised children of the 272 infants who were not circumcised at birth, 21 (8%) were circumcised subsequently: 5 for phimosis, 3 for balanitis, 1 for a chancre, and 1 for possible UTI: no medical indication was given for the remaining 11 procedures. In reviewing a similar population, Williams and Kapila54 reported phimosis and balanitis as the most frequent childhood problems among uncircumcised boys. Similar findings were described by Fakjian and associates189 in a series of uncircumcised adult males attending a Veterans Administration hospital dermatology clinic. In general, circumcision of adults usually is performed for the indications of phimosis or paraphimosis, intractable balanitis, and sexual dysfunction.164
The best arguments to support neonatal circumcision are penile cleanliness, avoidance of circumcision in adulthood, prophylaxis against UTI in high risk populations and, perhaps, and prevention of HIV infection. As previously discussed, uncircumcised prepubertal males do have a higher incidence of penile complications (largely irritation and infection) than do circumcised males: however, most such problems prove minor.57 A reduction in the risk for penile carcinoma is also a likely benefit of circumcision: however, the incidence of cancer of the penis is low, and its etiology is believed to be multifactorial. It has been claimed but not proved that adequate genital hygiene among the uncircumcised population results in a risk of penile carcinoma equal to that in the circumcised population.83
The eventual fate of routine neonate circumcision in the United States is unsettled. Social factors remain important in the decisions made by families. When most parents are asked why they favor circumcision, their answers include hygiene, convenience, vague statements of supposed medical advantage, and the father's foreskin status.124, 190 Lack of understanding about appropriate penile hygiene and physiology is widespread among both physicians and parents, contributing to the persisting popularity of circumcision. Studies claiming to present a “balanced” view of circumcision suggest that counseling by health professionals has limited impact on the decision to circumcise.126, 129 The limited influence of “learned” advice in altering the frequency of circumcision is not surprising, considering that many parents do not perceive the opinions of health professionals as critical to their decision.124
In the effort to review circumcision from the viewpoint of societal benefit or detriment, various types of cost–utility analyses have been conducted. Not surprisingly the results were varied depending on how the various components in the analyses were weighed.75, 191, 192 While most of these analyses do not provide support for a program of routine neonatal circumcision, some do.
Given the extensive controversy, it is not surprising that the literature includes descriptions of various techniques to restore an appearance of uncircumcision to those who have concluded that their original operation was an error.193 It should be noted that a desire to reverse circumcision for personal or social reasons is by no means a new phenomenon—methods of reconstructing the prepuce date at least as far back as the 1st century AD, when Celsus, the Roman medical writer first described a practical technique.193, 194
The debate about circumcision will continue. Those who oppose it do so largely from a belief that the procedure is traumatic to the neonate, unethical to perform, unnecessarily dangerous, and potentially detrimental to sexual function.4, 5, 9, 18, 42, 177 The riposte is that when circumcision is performed by competent surgeons the complication rate, while never zero, is very low and most problems are minor.5, 56, 60 It must not be overlooked that there are recent data concerning UTI risk, AIDS prevention and penile inflammatory complications indicating benefits, for circumcision.20, 21, 22, 56, 68, 195 There are other issue of importance. Despite extensive discussion in the literature and clear evidence of safety and efficacy too many practitioners continue to perform circumcisions without the use of local anesthesia.139, 196, 197, 198, 199, 200 There are abundant data indicating that the procedure is safely performed under various forms of local anesthesia, reducing neonatal distress.139, 142
For clinicians who perform circumcisions, several important points should be pondered. Circumcision in the developed world is an elective procedure. A case for its nonritual performance may not be convincing to all practitioners. Circumcision proponents must also recognize the weakness of some of the arguments made in the past to justify circumcision, The proponents of neonatal circumcision must accept that most surgical complications are avoidable and due to poor technical performance. This is especially true in medical centers where the least experienced practitioners often perform many of the procedures. In all instances, parents considering circumcision deserve careful and balanced counseling concerning the advantages and disadvantages of the procedure.8, 201, 202, 203 Preferably, this discussion should begin before labor and delivery and be part of regular antepartum care.
REFERENCES
Thompson HC: Editorial: The value of neonatal circumcision: An unanswered and perhaps unanswerable question. Am J Dis Child 137: 939, 1983 |
|
Grossman EA, Posner NA: Surgical circumcision of neonates: A history of its development. Obstet Gynecol 58: 1, 1977 |
|
Garvin CH, Persky L: Circumcision: Is it justified in infancy? J Natl Med Assoc 58: 233, 1966 |
|
Milos MF, Macris D: Circumcision: A medical or a human rights issue? J Nurse Midwifery 37: 87S, 1992 |
|
Grossman EA, Posner NA: The circumcision controversy: An update. Obstet Gynecol Annu 13: 181, 1984 |
|
Kaplan GW: Circumcision—an overview. Curr Probl Pediatr 7: 1, 1977 |
|
Gelbaum I: Circumcision: To educate, not indoctrinate—a mandate for certified nurse-midwives. J Nurse Midwifery 37: 97S, 1992 |
|
Robson WL, Leung AK: The circumcision question. Postgrad Med 91: 237, 1992 |
|
Wallerstein E: Circumcision: Ritual surgery or surgical ritual? Med Law 2: 85, 1983 |
|
Wiswell TE: Routine neonatal circumcision: A reappraisal. Am Fam Physician 41: 859, 1990 |
|
American Academy of Pediatrics: Report of the Task Force on Circumcision: Policy statement. Pediatrics 103: 686-693, 1999 |
|
Alanis MC, Lucidi RS: Neonatal circumcision: a review of the world's oldest and most controversial operation. Obstet Gynecol Surv. 2004 May;59(5):379-95. |
|
Hill G, Geisheker JV: Edgar Schoen does not represent the North American view of male circumcision. Arch Dis Child. 2006 Jan;91(1):92. |
|
Schoen EJ. Circumcision for preventing urinary tract infections in boys: North American view. Arch Dis Child 2005: 90: 771-772. |
|
Malone PSJ. Circumcision for preventing urinary tract infection in boys: European view. Arch Dis Child 2005:90:773-774. |
|
Lubchenco LO: Routine neonatal circumcision: A surgical anachronism. Clin Obstet Gynecol 23: 1135, 1980 |
|
Larsen GL, Williams SD: Postneonatal circumcision: Population profile. Pediatr 85: 808, 1990 |
|
Metcalf TJ, Osborn LM, Moriani EM: Circumcision: 2 year study of current practices. Clin Pediatr 22:575; 1983 |
|
Singh-Grewal D, Macdessi J, Craig J: Circumcision for the prevention of urinary tract infection in boys: a systematicreview of randomised trials and observational studies. Arch Dis Child. 2005 Aug;90(8):853-8. Epub 2005 May 12. |
|
Bailey RC, Moses S. Parker CB. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007 369:643-56 |
|
Gray RH, Kigozi G, Serwadda D et al: Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet. 2007 Feb 24;369(9562):657-66. |
|
Auvert B, Taljaard D, Lagarde E et al: Randomized, controlled intervention trial of male circumcision for reduction ofHIV infection risk: the ANRS 1265 Trial. PLoS Med. 2005 Nov;2(11):e298. Epub 2005 Oct 25. |
|
Cohen Y: Circumcision: Myth, ritual, operation. Med J Malaysia 39: 210, 1984 |
|
The Compact Edition of the Oxford English Dictionary, p 418. Oxford: Oxford University, 1986 |
|
Katz J: A question of circumcision. Int Surg 62: 490, 1977 |
|
Gairdner D: The fate of the foreskin: A study of circumcision. Br Med J 2: 1433, 1949 |
|
Waszak S J: The historical significance of circumcision. Obstet Gynecol 51: 499, 1978 |
|
Nasrallah PF: Circumcision: Pros and cons. Symposium on Genital Urinary Problems in Office Medicine. Prim Care 12: 593, 1985 |
|
Warnet E, Strashin E: Benefits and risks of circumcision. Can Med Assoc J 125: 967, 1981 |
|
Gelbaum I: Circumcision: Refining a traditional surgical technique. J Nurse Midwifery 38: 18S, 1993 |
|
Genesis 17: 10: Holy Bible. King James Version. Chicago, Spencer Press, 1947 |
|
Bolande RP: Ritualistic surgery—circumcision and tonsillectomy. N Engl J Med 290: 591, 1969 |
|
Lightfoot-Klein H, Shaw E: Special needs of ritually circumcised women patients. J Obstet Gynecol Neonat Nurs 20: 102, 1991 |
|
Monjok E, Essien EJ, Holmes L Jr: Female genital mutilation: potential for HIV transmission in sub-Saharan Africaand prospect for epidemiologic investigation and intervention. Afr J Reprod Health. 2007 Apr;11(1):33-42. |
|
Bikoo M: Female genital mutilation: classification and management. Nurs Stand. 2007 Oct 24-30;22(7):43-9; quiz 50. |
|
American Academy of Pediatrics: Report of the Ad Hoc Task Force on Circumcision. Pediatrics 56:610, 1975 |
|
Royal Australasian College of Physicians. Paediatrics and Child Health Division. Policy statement on circumcision, 2002. [ .racp.edu.au/hpu/paed/circumcision] |
|
Canadian Paediatric Society. Neonatal circumcision revisited. Fetal and Newborn Committee, Canadian Paediatric Society. Can Med Assoc J 1996; 154:769-80. |
|
Slaby AR, Drizd T: Circumcision in the United States. Am J Public Health 75i878, 1985 |
|
Carne S: Incidence of tonsillectomy, circumcision and appendectomy among RAF recruits. Br Med J 2: 19, 1956 |
|
Calnan M, Douglas JWB, Goldstein H: Tonsillectomy and circumcision: Comparison of two cohorts. Int J Epidemiol 7: 79, 1978 |
|
Editorial: The case against neonatal circumcision. Br Med J 1:1163, 1979 |
|
Hofvander Y. Letter: New law on male circumcision in Sweden. Lancet. 2002 359; (Feb 16), 630. |
|
Wirth JL: Current circumcision practices: Canada. Pediatrics 66: 705, 1980 |
|
Wirth JL: Statistics on circumcision in Canada and Australia. Am J Obstet Gynecol 130: 236, 1978 |
|
Shannon FT, Hotwood LJ, Fergusson DM: Infant circumcision. N Z Med J 2: 283, 1979 |
|
Ruff ML, Clarke TA, Harris JP et al: Myocardial injury following immediate postnatal circumcision. Am J Obstet Gynecol 144: 851, 1982 |
|
Oster J: Future fate of the foreskin: Incidence of preputial adhesions, phimosis and smegma among Danish school boys. Arch Dis Child 43: 200, 1968 |
|
Wright JE: Further to “the further fate of the foreskin.” Med J Aust 160: 134, 1994 |
|
Medical indications for childhood circumcision. Drug Ther Bull 31:99, 1993 |
|
Howat JM: Circumcision. Nurs Times 72: 1434, 1976 |
|
Lan JKT, Chung RMC: An outpatient observation of the foreskin among Chinese children in Hong Kong. Singapore Med J 24: 93, 1982 |
|
Griffiths D, Frank JD: Inappropriate circumcision referrals by GPs. J Roy Soc Med 85: 324, 1992 |
|
Williams N, Kapila L: Complications of circumcision. Br J Surg 80: 1231, 1993 |
|
Osborn LM, Metcalf TJ, Mariani EM: Hygienic care in uncircumcised infants. Pediatrics 67: 365, 1981 |
|
Schoen EJ: Urologist and circumcision of newborns. Urology 40: 99, 1992 |
|
Herzog LW, Alverez SR: The frequency of foreskin problems in uncircumcised children. Am J Dis Child 140: 254, 1986 |
|
Fox GN: Care of uncircumcised children. West J Med 142: 270, 1985 |
|
St. John-Hunt D: Circumcision of the newborn: Is it good preventive medicine? Med J Aust 1: 1100, 1967 |
|
Schoen EJ: The status of circumcision of newborns. N Engl J Med 322: 1308, 1990 |
|
Wiswell TE, Smith FR: Decreased incidence of urinary tract infections in circumcised male infants. Pediatrics 75: 901, 1985 |
|
Winberg J, Gothefors L, Bollgren et al: The prepuce: A mistake of nature? Lancet 1:598, 1989 |
|
Zorc JJ, Levine DA, Platt SL et al: Clinical and demographic factors associated with urinary tract infection in youngfebrile infants. Pediatrics. 2005 Sep;116(3):644-8. |
|
Nayir A. Circumcision for the prevention of significant bacteriuria in boys. Pediatr Nephrol 2001; 16: 1129-1134. |
|
Kwak C, Oh SJ, Lee A, Choi H. Effect of circumcision on urinary tract infection after successful antireflux surgery. BJU Int 2004, 94:627-629. |
|
Ginsburg CM, McCracken GH: Urinary tract infections of young infants. Pediatrics 69: 409, 1982 |
|
Wiswell TE, Miller GM, Gelston HM et al: The effect of circumcision status on periurethral bacterial flora during the first year of life. J Pediatr 113: 422, 1988 |
|
Wiswell TE, Hachey WE: Urinary tract infections and the uncircumcised state: An update. Clin Pediatr 132: 130, 1993 |
|
Herzog LW: Urinary tract infections and circumcision. Am J Dis Child 143: 348, 1989 |
|
Rushton HG, Maid M: Pyelonephritis in male infants: How important is the foreskin? J Urol 148: 733, 1992 |
|
Kashani IA, Faraday R: The risk of urinary tract infection in uncircumcised male infants. Int Pediatr 4: 44, 1989 |
|
Spach DH, Stapleton AE, Stamm WE: Lack of circumcision increases the risk of urinary tract infection in young men. JAMA 267: 679, 1992 |
|
Fussell EN, Kaack B, Cherry R et al: Adherence of bacteria to human foreskin. J Urol 140: 997, 1988 |
|
Thompson RS: An opposing view: Possible relationship between lack of circumcision and symptomatic urinary tract infection. J Fam Pract 31: 189, 1990 |
|
Chessare JB: Circumcision: Is the risk of urinary tract infection really the pivotal issue? Clin Pediatr 100, 1992 |
|
Wiswell TE, Tencer HL, Welch CA et al: Circumcision in children beyond the neonatal period. Pediatrics 92: 791, 1993 |
|
Bollgren I, Winberg J: Letter: Is it time for Europe to reconsider newborn circumcision? Acta Pediatr Scand 80: 575, 1991 |
|
Hellberg D, Valentin J, Eklund T et al: Penile cancer. Is there an epidemiological role for smoking and sexual behaviour? Br Med J 295: 1306, 1987 |
|
Persky L: Epidemiology of cancer of the penis. Recent Results Cancer Res 60: 97, 1977 |
|
Frisch M, Friis S, Kjaer SK et al: Falling incidence of penis cancer in an uncircumcised population (Denmark). BMJ 1995 Dec 2;311(7018):1471. |
|
Schoen EJ: The relationship between circumcision and cancer of the penis. Cancer J Clin 41: 306, 1991 |
|
Hanash KA, Furiow WL, Utz TC et al: Carcinoma of the penis: A clinicopathologic study. J Urol 104: 291, 1970 |
|
Boczko S, Freed S: Penile carcinoma in circumcised males. NY State J Med 12: 1903, 1979 |
|
Maden C, Sherman KJ, Beckman AM et al: History of circumcision, medical conditions, and sexual activity and risk of penile cancer. J Natl Cancer Inst 85: 19, 1993 |
|
Dean AL Jr: Epithelioma of the penis. J Urol 83: 252, 1935 |
|
Lenowitz H, Graham AP: Carcinoma of the penis. J Urol 56: 458, 1946 |
|
Dagher R, Selzer ML, Lapides J: Carcinoma of the penis and the anticircumcision crusade. J Urol 110: 79, 1973 |
|
Leiter E, Lefkovits AM: Circumcision and penile carcinoma. NY State J Med 75: 1520, 1975 |
|
Swafford TD: Circumcision and the risk of cancer of the penis. Am J Dis Child 139: 112, 1985 |
|
Persky L, deKernion J: Carcinoma of the penis. CA Cancer J Clinic 36: 258, 1986 |
|
Rogus B J: Squamous cell carcinoma in a young circumcised man. J Urol 138: 861, 1987 |
|
Bissada KN, Morcos RR, EI-Senoussi M: Post-circumcision carcinoma of the penis: I. Clinical aspects. J Urol 135: 283, 1986 |
|
Wolbarst AL: Circumcision and penile carcinoma. Lancet 1: 150, 1932 |
|
Hardner GJ, Bhaualaph T, Murphy GP et al: Carcinoma of the penis: Analysis of therapy in 100 consecutive cases. J Urol 108: 428, 1972 |
|
Riveros M, Gorostiaga R: Cancer of the penis. Arch Surg 85: 377, 1962 |
|
Daling JR, Sherman K J, Hislop TG et al: Cigarette smoking and the risk of anogenital cancer. Am J Epidemiol 135: 180, 1992 |
|
Brinton LA, Jun-Yao L, Shou-De Ret al: Risk factors for penile cancer: Results from a case-control study in China. Int J Cancer 47:504, 1991 |
|
Zur Hausen H: intracellular surveillance of persisting viral infections: Human genital cancer results from deficient cellular control of papillomavirus gene expression. Lancet 2: 489, 1986 |
|
Kochen M, McCurdy SA: Letter to editor: Circumcision. Am J Dis Child 133: 1079, 1979 |
|
Kochen M, McCurdy S: Circumcision and the risk of cancer of the penis: A lifetable analysis. Am J Dis Child 134: 484, 1980 |
|
Swafford TD: Letter to editor: Circumcision and the risk of cancer of the penis. Am J Dis Child 139: 112, 1985 |
|
Preston EN: Wither the foreskin? JAMA 213: 1853, 1970 |
|
Lilienfield AM, Graham S: Validity of determining circumcision status by questionnaire as related to epidemiologic studies of cancer of the cervix. J Natl Cancer Inst 21: 713, 1958 |
|
Barrasso R, De Brux J, Croissant O et al: High prevalence of papillomavirus-associated penile intraepithelial neoplasia in sexual partners of women with cervical intraepithelial neoplasia. N Engl J Med 317:916, 1987 |
|
Terris M, Wilson F, Nelson JH: Relation of circumcision to cancer of the cervix. Am J Obstet Gynecol 117: 1056, 1973 |
|
Dunn JE, Buell P: Association of cervical cancer with circumcision of the sexual partner. J Natl Cancer Inst 22: 749, 1959 |
|
Onuigbo WIB: Carcinoma of the uterine cervix in Nigerian Igbos. Gynecol Oncol 4: 255, 1976 |
|
Aitken-Swan J, Baird D: Circumcision and cancer of the cervix. Br J Cancer 19: 217, 1965 |
|
Hira SK, Kamanga J, Macuacua R et al: Genital ulcers and male circumcision as risk factors for acquiring HIV-1 in Zambia. J Infect Dis 1: 584, 1990 |
|
Taylor PK, Rodin P: Herpes genitalis and circumcision. Br J Vener Dis 51: 274, 1975 |
|
Schlossberger NM, Turner RA, Irwin CE: Early adolescent knowledge and attitudes about circumcision: Methods and implications for research. J Adolesc Health 12: 293, 1991 |
|
Parker JDJ, Banatvala JE: Herpes genitalis and circumcision. Br J Vener Dis 43: 211, 1967 |
|
Smith GL, Greenup R, Takafuji ET: Circumcision as a risk factor for urethritis in racial groups. Am J Public Health 77: 452, 1987 |
|
Cook LS, Koutsky LA, Holmes KK: Circumcision and sexually transmitted diseases. Am J Public Health 84: 197, 1994 |
|
Parker SW, Stewart AJ, Wren NM et al: Circumcision and sexually transmitted disease. Med J Aust 2: 288, 1983 |
|
Wilson RA: Circumcision and venereal disease. Can Med Assoc J 56: 54, 1947 |
|
Karim QA. Editorial: Prevention of HIV by male circumcision. BMJ 2007: 335:4-5 (7 July), doi:10.1136/bmj.39245.491169.BE |
|
McNeil D G Jr. Circumcision halves HIV risk, US agency finds. [www.nytimes.com/2006/12/14/health/14hiv.html] |
|
Short RV. New ways of preventing HIV infection: thinking simply, simply thinking. :Philos Trans R Soc Lond B Biol Sci 2006 May 29; 361(1469):811-20. |
|
Williams BG, Lloyd-Smith JO, Gouws E et al: The potential impact of male circumcision on HIV in Sub-Saharan Africa. PLoS Med. 2006 Jul;3(7):e262. |
|
Westercamp N, Bailey RC: Acceptability of male circumcision for prevention of HIV/AIDS in sub-SaharanAfrica: a review. AIDS Behav 2007 May;11(3):341-55. Epub 2006 Oct 20. |
|
Weiss HA. Male circumcision as a preventive measure against HIV and other sexually transmissed diseases. Sexually transmitted diseases and urinary tract infections. Curr Opin Infect Dis 2007: 20(1) 66-72. |
|
Van Howe RS, Svoboda JS, Hodges FM: HIV infection and circumcision: cutting through the hyperbole. J R Soc Health 2005 Nov;125(6):259-65. |
|
Stein MT, Marx M, Taggart SL et al: Routine neonatal circumcision: The gap between contemporary policy and practice. J Fam Pract 15: 47, 1982 |
|
Maisels MJ, Hayes B, Conrad S, Chez RA: Circumcision: The effect of information on parental decision making. Pediatrics 71: 453, 1983 |
|
Herrera AJ, Cochran B, Herrera A et al: Parental information and circumcision in highly motivated couples with higher education. Pediatrics 71: 233, 1983 |
|
Herrera AJ, Hsu AS, Salcedo UT et al: Role of parental information in the incidence of circumcision. Pediatrics 70: 597, 1982 |
|
Bigelow J: The Joy of Uncircumcising: Restore your Birthright and Maximize Sexual Pleasure. Aptos, CA, Hourglass Book Publishing, 1992 |
|
Ritter TJ: Say No to Circumcision: 40 Compelling Reasons Why You should Respect Birthright and Keep your Son Whole. Aptos, CA, Hourglass Book Publishing, 1992 |
|
Yellen HS: Bloodless circumcision of the newborn. Am J Obstet Gynecol 30: 146, 1935 |
|
Stang H J, Gunnar MR, Snellman L et at: Local anesthesia for neonatal circumcision: Effects on distress and cortisol response. JAMA 259: 1507, 1988 |
|
Gunner MR, Fish RO, Malone S: The effects of a pacifying stimulus on behavioral and adrenocorticai response to circumcision in the newborn. J Am Acad Child Psychiatry 23: 34, 1984 |
|
Rawlings D J, Miller PA, Engel RR: The effects of circumcision on transcutaneous PO2 in term infants. Am J Dis Child 134: 676, 1980 |
|
Anders TF, Chaleman RJ: The effects of circumcision on sleep-wake states in human neonates. Psychosom Med 30: 174, 1974 |
|
Arnett RM, Jones JS, Horger EO III: Effectiveness of 1% lidocaine dorsal penile block in infant circumcision. Am J Obstet Gynecol 163: 1074, 1990 |
|
Williamson PS, Williamson ML: Physiologic stress reduction by a local anesthetic during newborn circumcision. Pediatrics 1: 36, 1983 |
|
Holve RL, Bromberger PJ, Goreman HD et al: Regional anesthesia during newborn circumcision: Effect on infant pain response. Clin Pediatr 22: 813, 1983 |
|
Dixon S, Snyder J, Holve R et al: Behavioral effects of circumcision with and without anesthesia. J Dev Behav Pediatr 5: 246, 1984 |
|
Garry DJ, Swoboda E, Elimian A et al: A video study of pain relief during newborn male circumcision. J Perinatol. 2006 Feb;26(2):106-10. |
|
OMIT |
|
Kirya C, Werthman MW: Neonatal circumcision and penile dorsal nerve block: A painless procedure. J Pediatr 92: 998, 1978 |
|
Brady-Fryer B, Wiebe N, Lander JA: Pain relief for neonatal circumcision. Cochrane Database Syst Rev 2004 Oct 18;(4): CD004217. |
|
Lehr VT, Cepeda E, Frattarelli DA et al: Lidocaine 4% cream compared with lidocaine 2.5% and prilocaine 2.5% or dorsal penile block for circumcision. Am J Perinatol. 2005 Jul;22(5):231-7. |
|
Fontaine P, Dittberner D, Scheltema KE: The safety of dorsal penile nerve block for neonatal circumcision. J Fam Pract 39: 243, 1994 |
|
Maciello AL: Anesthesia for neonatal circumcision: Local anesthesia is better than dorsal penile nerve block. Obstet Gynecol 75: 834, 1990 |
|
Benini F, Johnston CC, Faucher D et al: Topical anesthesia during circumcision in newborn infants. JAMA 270: 850, 1993 |
|
Weatherstone KB, Rasmussen LB, Erenberg A et al: Safety and efficacy of a topical anesthetic for neonatal circumcision. Pediatrics 92: 710, 1993 |
|
Fontaine P, Toffler WL: Dorsal penile nerve block for newborn circumcision. Am Fam Pract 43: 1327, 1991 |
|
Shoen EJ, Fischell AA: Pain in neonatal circumcision. Clin Pediatr 30: 429, 1991 |
|
Sara CA, Lowry CJ: A complication of circumcision and dorsal nerve block of the penis. Anaesth Intensive Care 13: 79, 1984 |
|
Mandel S: Methemoglobinemia following neonatal circumcision. JAMA 261: 702, 1989 |
|
Ozbek N, Sarikayalar F: Toxic methaemoglobinaemia after circumcision. Eur J Pediatr 152: 80, 1993 |
|
Physician Desk Reference: EMLA Cream, p 544. Montvale, NJ, Medical Economics Data Production, 1995 |
|
Blass EM, Hoffmeyer LB: Sucrose as an analgesic for newborn infants. Pediatrics 87: 215, 1991 |
|
Ipp MM, Gold R, Greenberg S et al: Acetaminophen prophylaxis of adverse reactions following vaccination of infants with diptheria-pertussis-tetanus toxoids-polio vaccine. Pediatr Infect Dis J 6: 721, 1987 |
|
Mor A, Eshel G, Aladjem M et al: Tachycardia and heart failure after ritual circumcision. Arch Dis Child 62: 80, 1987 |
|
Kaplan GW: Complication of circumcision. Urol Clin North Am 10: 543, 1983 |
|
Braren V: Letter to the editor: Circumcision complication. Clin Pediatr 18: 639, 1979 |
|
Sterenberg N, Golan J, Ben-Hur N: Necrosis of the glans penis following neonatal circumcision. Plast Reconstr Surg 68: 237, 1981 |
|
Poland RL: The question of routine neonatal circumcision. N Engl J Med 322: 1312, 1990 |
|
Wiswell TE, Geschke DW: Risk from circumcision during the first month of life compared with those for uncircumcised boys. Pediatrics 83: 1011, 1989 |
|
Gee WF, Ansell JS: Neonatal circumcision: A ten-year overview: With comparison to the Gomco clamp and the Plastibell device. Pediatrics 58: 824, 1976 |
|
Shulman J, Ben-Hut N, Neuman Z: Surgical complications of circumcision. Am J Dis Child 107: 149, 1964 |
|
Griffiths DM, Atwell JT, Freeman NV: A prospective study of the indications and morbidity of circumcision in children. Eur Urol 11: 184, 1985 |
|
Patel H: The problem of routine circumcision. Can Med Assoc J 95: 576, 1966 |
|
Speert H: Circumcision of the newborn, an appraisal of its present status. Obstet Gynecol 2: 164, 1953 |
|
Woodside JR: Necrotizing fasciitis after neonatal circumcision. Am J Dis Child 134: 301, 1980 |
|
Sussman SJ, Schiller RP, Shashilumar VL: Fournier's syndrome: A report of three cases and review of the literature. Am J Dis Child 132: 1189, 1978 |
|
Cleary TG, Kohl S: Overwhelming infection with group B beta-hemolytic Streptococcus associated with circumcision. Pediatrics 64: 301, 1979 |
|
Annunziato D, Goldblum LM: Staphylococcal scalded skin syndrome: A complication of circumcision. Am J Dis Child 132: 1187, 1978 |
|
Procopis PG, Kewley GD: Complication of circumcision. Med J Aust 1: 15, 1982 |
|
Radhakrishnan J, Reyes HM: Penoplasty for buried penis secondary to “radical” circumcision. J Pediatr Surg 19: 629, 1984 |
|
Sotolongo JR, Hoffman S, Gribetz ME: Penile denudation injuries after circumcision. J Urol 133: 102, 1985 |
|
Sathaye UV, Goswami AK, Sharma SK: Skin bridge—a complication of paediatric circumcision. Br J Urol 66: 214, 1990 |
|
Berry CD, Cross RC: Urethral meatal caliber in circumcised and uncircumcised males. Am J Dis Child 92: 52, 1956 |
|
Clair DL, Cladamone AA: Pediatric office procedures. Urol Clin North Am 15: 715, 1988 |
|
Morgan WKC: Penile plunder. Med J Aust 1: 102, 1967 |
|
Valentine RJ: Adult circumcision: A personal report. Med Aspects Hum Sex 8: 31, 1974 |
|
Harnes JR: The foreskin saga. JAMA 217: 1241, 1971 |
|
Falliers CJ: Circumcision. JAMA 24: 2194, 1978 |
|
Audry G, Buis J, Vazquez MP et al: Amputation of penis after circumcision—penoplasty using expandable prosthesis. Eur J Pediatr Surg 4: 44, 1994 |
|
Connelly KP, Shropshire LC, Salzberg A: Gastric rupture associated with prolonged crying in a newborn undergoing circumcision. Clin Pediatr 560, 1992 |
|
Warwick DJ, Dickson WA: Keloid of the penis after circumcision. Postgrad Med 69: 236, 1993 |
|
Datta NS, Zinner NR: Complication from Plastibell circumcision ring. Urology 9: 57, 1977 |
|
Eason JD, McDonnell, Clark G: Male ritual circumcision resulting in acute renal failure. Br Med J 309: 660, 1994 |
|
Auerbach MR, Scanlon JW: Recurrence of pneumothorax as a possible complication of elective circumcision. Am J Obstet Gynecol 132: 583, 1978 |
|
King LR: Neonatal circumcision in the US in 1982. J Urol 128: 1135, 1982 |
|
Fergusson DM, Lawton JM, Shannon FT: Neonatal circumcision and penile problems: an 8-year longitudinal study. Pediatrics 81: 537, 1988 |
|
Fakjian N, Hunter S, Cole GW et al: An argument for circumcision: Prevention of balanitis in the adult. Arch Dermatol 126: 1046, 1990 |
|
Lovell JE, Cox J: Maternal attitudes toward circumcision. J Fam Pract 9:8ll, 1979 |
|
Gunjuts TG, Humphrey JBC, Taras HL et al: Routine neonatal circumcision: A cost-utility analysis. Med Decis Making 11:282, i991 |
|
Cadman D, Gafni A, McNamee J: Newborn circumcision: An economic perspective. Can Med Assoc J 131: 1353, 1984 |
|
Schneider J: Circumcision and “uncircumcision.” S Afr Med J 50: 556, 1976 |
|
Rubin JP: Celsus' decircumcision operation: medical and historical implications. Urology 16: 121, 1980 |
|
Winberg J: Is routine circumcision advised in boys with obstructive uropathy in order to prevent urinary tract infection? Pediatr Nephrol 5: 178, 1991 |
|
Zweitter J: Teaching residents circumcision. Fam Med 26: 4, 1994 |
|
Wellington N, Rieder MJ: Attitudes and practices regarding analgesia for newborn circumcision. Pediatrics 92: 541, 1993 |
|
Ryan CA, Finer NN: Changing attitudes and practices regarding local analgesia for newborn circumcision. Pediatrics 94: 230, 1994 |
|
Fontaine P: Local anesthesia for neonatal circumcisions: Are family practice residents likely to use it? Fam Med 22: 371, 1990 |
|
Toffler WL, Sinclair AE, White KA: Dorsal penile nerve block during newborn circumcision: Underutilization of a proven technique? J Am Board Fam Pract 3: 171, 1990 |
|
Herrera AJ, Macaraeg AL: Physicians' attitudes toward circumcision. Am J Obstet Gynecol 148: 825, 1984 |
|
Herrera AJ, Trouern-Trend JBG: Routine neonatal circumcision. Am J Dis Child 133: 1069, 1979 |
|
Brownlee HJ, Coble WR: Neonatal circumcision: Attitudes and practices of United States Air Force Physicians. Mil Med 149: 462, 1984 |