Second-Trimester Surgical Abortion
Authors
INTRODUCTION
From the early reports of the Joint Program for the Study of Abortion (JPSA) published in the early 1970s, the medical community learned to its surprise that surgical abortion was safer in the early second trimester of pregnancy than the more widely used induction methods.1 Moreover, the JPSA study challenged the sacrosanct notion that a surgical abortion could not be performed at all in the period immediately following the first trimester (13–16 menstrual weeks). Conventional wisdom held that, following the first trimester, the physician must wait until the 16th or even 17th week of gestation, then apply an intra-amniotic solution of hyperosmolar saline, for example, to induce the abortion.
Although 'dilation and evacuation' ('D & E') abortions had been performed in England by Drs Sopher,2, Bierer,3 Finks,4 and Davis,5 it was not until the JPSA Study report was published in 1972 that this procedure was acknowledged in the United States. A 1977 report from the Centers for Disease Control confirmed the earlier JPSA findings.6 In December 1976, a paper describing the use of serial multiple Laminaria dilation of the cervix prior to surgical evacuation was presented at the annual meeting of the Association of Planned Parenthood Physicians, although the decision to accept the paper for presentation on the program was extremely controversial. The paper was published the following year in Advances in Planned Parenthood as the first clinical report of outpatient D & E procedures and first report of a serial multiple Laminaria treatment of the cervix prior to D & E in the early mid-trimester in the American literature.7 This protocol derived from earlier experience with the use of overnight Laminaria for first trimester procedures and the report of a serial multiple Laminaria protocol by Japanese physicians as described by Neubart.8, 9 Soon after, there were numerous reports confirming the safety of this procedure and its advantages over waiting until the 16th menstrual week of gestation to perform an abortion by the use of hypertonic saline solution.10, 11, 12, 13, 14, 15, 16, 17, 18, 19
D & E is now accepted as the method of choice in second-trimester abortion in the United States, although the details of how this is done vary from physician to physician and from clinical institution to clinical institution. Laminaria japonicum tents are often used, sometimes with a single application, and sometimes with multiple serial applications.7, 14, 19 Synthetic hygroscopic dilators are sometimes used in place of Laminaria.20, 21, 22 Misoprostol and mifepristone are being studied as a principal or adjunctive method of cervical dilation and/or induction of labor.23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34 Anesthesia is often administered locally; however, general anesthesia is also used.35, 36, 37, 38
The emphasis in this chapter is on the principles of surgical technique in second-trimester abortion from 13 through 26 menstrual weeks of gestation. Whereas the lower range may not be considered by some to be in the second trimester, the principles of operating in the 13–14 week range may have more in common with procedures performed at a later stage than with commonly used procedures in the early first trimester. The emphasis also is on outpatient practice in a freestanding clinic or private office setting. Detailed step-by-step methods are described in specialized texts and reports.39, 40, 41, 42, 43
GENERAL PRINCIPLES OF ABORTION TECHNIQUE
The first step in any surgical procedure and the management of its complications is prevention. Good surgical techniques tend to prevent complications and should be followed for any type of surgery. These include accurate preoperative diagnosis and evaluation, a high level of operator skill, sound sterile technique, atraumatic surgical technique, thorough removal of devitalized tissue, and careful postoperative supervision and follow-up.
Careful application of these principles can eliminate most sources of complications in surgical abortion. Although many believe that complications are inevitable, the best attitude is that all complications are preventable. Each complication must be examined to determine its source and possible means of prevention. The lessons thus derived should be applied immediately to the operating protocol.
PREOPERATIVE DIAGNOSIS AND EVALUATION
Preoperative diagnosis and evaluation of second-trimester abortion patients means answering several of the following questions:
- What is the length of gestation or actual fetal age?
- Is the pregnancy complicated by the presence of uterine abnormalities, multiple gestation, hydatidiform mole, or other conditions?
- Is the pregnancy complicated by the history or presence of concurrent medical or surgical conditions such as diabetes, pre-eclampsia, neurologic disorders, previous cesarean delivery, obesity, placenta previa, or cardiovascular disease?
OPERATOR SKILL
A high level of operator skill is at least as important in abortion as in any other surgical endeavor. Notwithstanding the availability of intraoperative real-time ultrasound, surgical abortion is a blind procedure that is performed by touch, and it requires awareness of the nuances of sensations provided by instruments, honesty, and caution. It requires excellent proprioception and depth perception. Competent orientation in the performance of an abortion is essential, but abortion, almost more than any other operation, demands experience to develop skill. Experience that is not interpreted honestly, however, becomes the mere repetition of mistakes. Practitioners must be brutally honest with themselves to make the necessary corrections from second to second while performing the procedure. Too much reliance on the ultrasound image can be a fatal trap.
- Did the forceps or suction tip pass through the uterine wall?
- Is the material grasped with the forceps unyielding?
- Is this material uterine wall or viscera and not fetal tissue?
- Is the patient merely agitated, or is she having a severe vasovagal episode?
- Is the patient agitated because she is hypovolemic or experiencing an amniotic fluid embolism?
A patient who is unconscious from general anesthesia or deeply sedated may not manifest signs or symptoms of these problems.
Competence in other aspects of pelvic surgery learned in residency training does not assure competence in abortion. Likewise, competence in first-trimester abortion by no means assures immediate competence in second-trimester surgical technique.
Operative competence in abortion comes through observation of an experienced and highly competent practitioner, through performance of early, uncomplicated abortion under direct supervision until confidence and smoothness are gained, and through practice.
STERILE TECHNIQUE
Sterile technique is often abandoned or neglected in some aspects of abortion care, partly because the risks of poor technique are underestimated. Although the germ theory of disease has fallen on hard times, it unquestionably has relevance to abortion technique.
Each abortion, no matter how carefully it is performed, results in a contaminated uterine cavity. Most women overcome this contamination through natural body defenses against infection; however, a more prudent point of view is that the operator must do everything possible to keep contamination to a minimum. This approach implies the use of individually sterilized specula, autoclaved instruments, face masks, and sterile gloves. The no-touch technique is essential, as is scrupulous attention to intraoperative sterile technique. Even when abortions are performed by highly experienced operators, tissue is retained often enough to require assiduous attention to this point. A clot or devitalized tissue within the uterus is a superb culture medium for bacteria.
In the early 1970s, with the advent of outpatient abortion clinics, the no-touch technique became popular with abortion practitioners performing first trimester abortions. This highly useful adaptation requires that the operator, after placement of the speculum and antiseptic cleansing of the vagina, touch only the grasping end or portion of the instrument on the sterile tray. After that part of the instrument is touched, it is kept away from the tips of any instruments that remain sterile and will be placed within the uterine cavity.
A common mistake seen in ambulatory clinics is the application of sterile operating room technique to this system; the result is complete contamination. For example, surgeons trained in operating room technique are accustomed to having the vagina and perineum prepared by a nurse or operating room technician before they enter the room. The surgeon wears a sterile gown and gloves, takes a sterile speculum from the tray, places it in a position in the patient's vagina after performing a bimanual examination, and proceeds with the operation. It does not matter whether the surgeon touches the speculum after that; it is sterile. The same operator need not pay attention to how the dilators are handled, because everything is sterile. The surgeon may touch the instruments on the end or in the middle or turn them around and back again with impunity.
Now place this operator in the outpatient clinic using a no-touch technique. The speculum is sterile and should be wrapped in its own package. The instrument tray is opened, and it is sterile inside. The patient has not been prepared in the standard operating room manner. After a bimanual examination is performed, the operator places the sterile speculum in the vagina, using at least one gloved hand. Regardless of whether the operator uses one or two sterile gloves, the speculum is no longer sterile at this point; the perineum has not been treated with antiseptic. Suppose that the operator works in a clinic that uses sterile gloves from this point in the procedure. The operator dons sterile gloves, applies antiseptic to the vagina with a sponge forceps and gauze, and prepares to begin the procedure. Just before doing so, the operator stops to adjust the speculum with gloved hands. At that point, the only reason for keeping the gloves on would be to protect the operator from the patient's fluids; certainly, the gloves no longer serve their original function.
The no-touch technique practiced without gloves can be used in performing first-trimester abortion safely, but it is even more likely to result in contamination that endangers the patient, and it is not an option in second-trimester abortion. In outpatient second-trimester abortion, the safest combination is a strict no-touch technique practiced with sterile gloves after the completion of initial (gloved) examination and antiseptic preparation. The increasing prevalence of human immunodeficiency virus infection, acquired immune deficiency syndrome, and other blood-borne diseases makes this practice even more necessary for the protection of both the patient and the operator.
ATRAUMATIC TECHNIQUE
One of the first principles in medicine is not to harm the patient. Surgeons of all types properly emphasize the gentle handling of tissue to minimize trauma to the patient's body. There is no reason why this excellent concept should not be pursued vigorously in abortion.
The primary source of trauma to the pelvic organs in abortion arises from perforation of the uterus and a related injury, cervical laceration. These injuries vary widely in severity and principal cause, but many must be ascribed to methods of cervical dilation. In second-trimester abortion, uterine injury often arises from the use of crushing forceps or the overly aggressive, forceful withdrawal of these forceps, but again, these injuries frequently can be traced to inadequate cervical dilation.
Such an obstacle to the act of emptying the uterus as the internal os requires close attention. In early pregnancy and even beyond, the internal os generally resists dilation by force. If there is an alternative to brute strength that tears tissue in a significant number of cases, why not use it?
In every major series of surgical abortions, perforation of the uterus has been an important complication. Although perforation frequently is related to underestimation of gestational length, it is more likely to be related to uterine position and forcible dilation, especially in first-trimester abortion. The source of most perforations, forcible manual dilation, is obvious. There is an alternative to this method: dilation by means of Laminaria or other hygroscopic materials.3, 8, 40
Dilation of the cervix with Laminaria overnight or even for a few hours softens the cervix in addition to dilating it. The mechanism of this agent is incompletely understood, but it works.9, 20, 44, 45, 46 The need for force in even supplemental manual dilation is reduced, the need for anesthesia is reduced, the procedure time is shorter, and wider dilation permits the easier use of instruments, such as curettes, to assure uterine emptying. In second-trimester abortion, manual dilation is wholly inadequate.
In this case, atraumatic surgical technique does not mean that appropriate instruments may not be used. The curette is an indispensable instrument that, when used properly, can help to empty the uterus as no other instrument can (Figure 1). In addition, when handled properly, the curette is not much more likely to cause a perforation than is a flexible cannula.
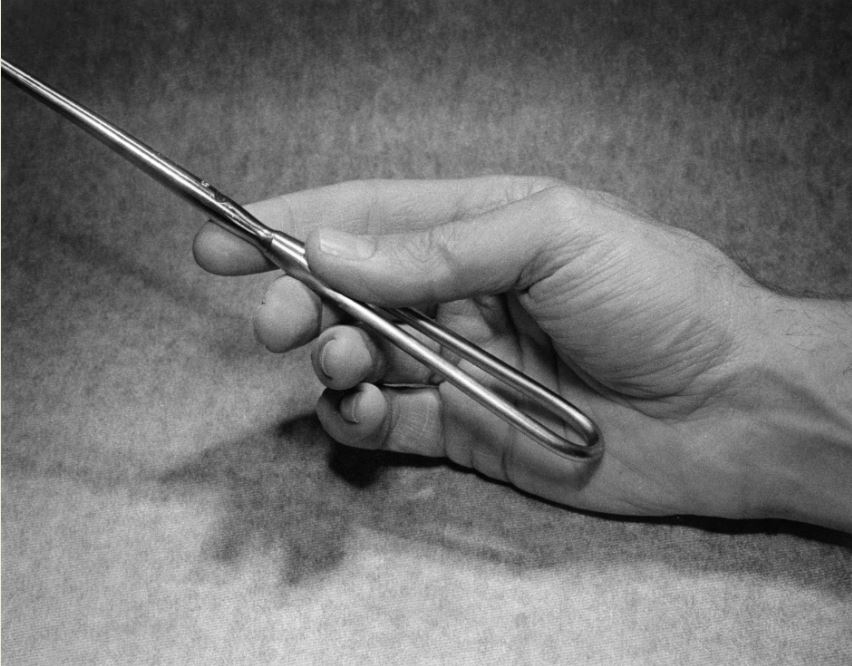 Fig. 1 The correct way to hold a curette
Fig. 1 The correct way to hold a curette
The key to atraumatic use of the curette is the proper method of holding it. The instrument must be held gently between two fingers. The grip must be firm enough for control, but relaxed enough to permit the instrument to slip back through the fingers on encountering the uterine fundus or other resistance.
The use of an atraumatic tenaculum, such as the side-curve Kelly instrument with an Allis (5 × 6) tip, accompanying Laminaria for dilation, will virtually eliminate cervical lacerations caused by tenacula. With proper Laminaria dilation, the tenaculum needs to be closed only one stop, again minimizing trauma.
REMOVAL OF DEVITALIZED TISSUE
The purpose of an abortion is to empty the pregnant uterus of its contents. This principle may seem too elementary to state, but the frequency with which it is ignored requires its mention. The underlying surgical principle that is applied to abortion is thorough removal of devitalized tissue. The reputation for danger that abortion acquired in the United States, at least in the first half of the 20th century, was from the many incomplete abortions that resulted in sepsis and death. In one recent major medical meeting, a prominent nurse practitioner stated quite firmly that the purpose of the abortion was to end the pregnancy but not to empty the uterus. Unfortunately, this declaration is a step backward in medical history, procedure and safety.
Modern applications of abortion technology sometimes overlook this important principle. The protocols for “medication abortion” in the first trimester depend on the patient’s uterus expelling the products of conception without any surgical procedure. While this happens most of the time, sometimes it does not, and the consequences can be severe complications leading to death.47, 48 Patients receiving amnioinfusion and/or medical induction in the second trimester are left to deliver the placenta on their own. This time-honored practice derived from classical obstetrics guarantees much higher major complication rates than are acceptable or necessary.49
Several factors contribute to attainment of the goal of complete uterine evacuation in surgical abortion. First, adequate dilation permits the use of appropriate instruments in second-trimester abortion. Second, routine exploration with ring forceps and curettage after second-trimester D & E abortion and removal of the placenta almost always yields tissue. The curette is a valuable tool for determining whether the uterine wall has been denuded of decidua and placental fragments. Vacuum aspiration with a large (12 mm) cannula completes the procedure. The application of vacuum aspiration with a large bore cannula prior to complete emptying of amniotic fluid and removal of both the fetus and placenta invites disruption of the placenta while amniotic fluid is present and results in a higher risk of amniotic fluid embolism.
POSTOPERATIVE CARE
Careful postoperative supervision and follow-up are important in any type of surgery. The fact that abortion patients frequently feel well within a few minutes after the abortion does not minimize the necessity of such care.
For postabortion patients, vital signs should be observed and recorded at frequent intervals, including immediately after the procedure, while the patient is on the operating table; on arrival at the recovery room; and once before departure from the recovery room.
Tissue obtained during the abortion procedure must be examined immediately, preferably by the physician. In all cases, it must be examined by the operating physician or a well-trained laboratory technician assigned to this task. The gross appearance of the tissue is far more informative for patient management than a laboratory slip obtained several days later. If the tissue is not consistent with the estimated length of gestation, the physician must evaluate the operative procedure to determine whether it was incomplete or irregular in some way. In the second trimester, it is especially important to examine the tissue for completeness including presence of the fetal calvarium, thorax, and all extremities. Placental tissue must be present in an appropriate quantity.
The single most critical postoperative observation in estimating gestational age in second-trimester abortion is fetal foot length. The gross weight of all tissue combined should also be obtained; if the fetus and placenta can be weighed separately, this should be done. A chemical balance scale can be used for optimum accuracy.
If possible, follow-up arrangements must be made with the patient before she leaves, especially if the patient is from a distant community or cannot be contacted once she leaves. Good follow-up is the best way to prevent a minor postoperative complication from becoming major or even fatal.
SPECIAL CONSIDERATIONS IN SURGICAL ABORTION
Anesthesia
The choice of anesthesia is an important one and a subject that remains controversial among abortion service providers. The primary issue is whether general or local anesthesia is to be used for surgical abortion, as opposed to amnioinfusion and/or medical induction methods. The medical literature shows that local anesthesia has its risks, but most of them have to do with the inappropriate application of toxic amounts rather than inherent dangers of the local anesthetic agent itself. Conversely, the dangers of general anesthesia are more significant. There appears to be no medical justification, other than uncontrolled epilepsy, severe mental retardation, or agitated psychosis, for the use of general anesthesia in abortion. Patient comfort and especially physician convenience are marginal indications for general anesthesia, considering the risks involved. The degree of bleeding experienced under general anesthesia is greater, the risk of perforation with injury to abdominal viscera is greater, and the risk of death from the aspiration of vomitus, among other factors, appears to be greater. The risk of death during abortion performed under general anesthesia is two to four times greater than under local anesthesia, and the risk of major complication is up to four times greater under general anesthesia.35, 36, 37, 38 These risks may be even greater for second-trimester D & E abortion.
Local anesthesia offers many advantages over general anesthesia:
- The patient is alert, responsive, and communicative both during and immediately after the procedure. She is able to report important symptoms that may signal the occurrence or onset of serious complications in time to prevent them from becoming more serious or even fatal.
- Generally, the patient feels well and has a clear head within minutes after the procedure. This rapid recovery is an important advantage for patients who have traveled long distances for the abortion and must leave for home soon after the procedure and recovery period.
- The gag reflex is not diminished under local anesthesia, whereas it is suppressed with general anesthesia. Abortion patients may have many characteristics, but one of them is occasional difficulty in following instructions not to eat or drink anything for a fixed number of hours before the abortion procedure.
- Patients who have had general anesthesia with previous abortions almost invariably have severe emotional problems dealing with the current abortion, in both the preoperative and operative phases. This phenomenon has become obvious and wholly predictable. For mental health reasons alone, general anesthesia may be contraindicated for abortion procedures.
- The use of general anesthesia eliminates physician–patient interaction during the abortion and insulates the physician from the patient's emotional experience. This loss is a serious problem for physicians and may make it extremely difficult for them to relate to the emotional problems encountered by abortion patients. It does nothing to enhance the physician's empathy for the patient's dilemma or the physician's understanding of the importance of this experience to the patient. This lack of interaction with the patient is seen as an advantage when the program objective is to see as many patients as possible in a short time and to minimize emotional stress for the physicians and their assistants.
Some surgical procedures require general anesthesia. Open heart surgery, major abdominal surgery, and major orthopedic surgery are among them; operative abortion is not.
'Conscious sedation' is another choice, in which the patient is only marginally conscious. Techniques and drugs for this procedure vary from practitioner to practitioner and from institution to institution. When conscious sedation borders on second or third stage of general anesthesia, however, the patient must be attended by an anesthesiologist or nurse anesthetist.
Dilation and evacuation
Since the 1972 report by Bierer and Steiner,3 numerous accounts of dilation and evacuation (D & E) series have appeared in the literature. One of the principal controversies among advocates of the D & E method is the manner of cervical dilation. The method described by Bierer and Steiner and used by Barr10 is manual dilation under anesthesia the day before the procedure, followed by placement of a number of Laminaria sticks. The Laminaria dilate the cervix overnight and permit the evacuation of the uterus with large forceps. Another common protocol, described best by Hanson,11 requires placement of several Laminaria in the cervix without manual dilation the afternoon before the abortion. This protocol uses the Laminaria as mechanical dilators, which they are not, and defeats the use of Laminaria over time to effect a gentle, atraumatic dilation of the cervix.
A protocol that I have adapted from the Japanese experience reported by Neubardt9 uses serial multiple Laminaria treatments over 2 days. Under this protocol, one or more Laminaria are placed in the cervix on day 1. They are removed and replaced by a larger number on day 2, and the uterus is evacuated with forceps on day 3 under paracervical block anesthesia. I use several variations of this method. Supplemental manual dilation is performed with oversized Pratt dilators or special Teflon dilators of my design.40 With some patients, this procedure is augmented by intrafetal injection of digoxin 2 mg or, historically, hyperosmolar urea on day 1 or day 2.19
In addition to dilation, application of Laminaria frequently results in almost complete effacement of the cervix, leading to easy evacuation of the uterus through a widely dilated cervix. A variety of forceps, some also of my design, are used for the evacuation.40
Aside from operator skill, the most critical single factor in the safe performance of second-trimester D & E abortion is correct determination of fetal age. This knowledge permits adequate preparation of the patient materials for the procedure. Ultrasonographic examination is essential for consistently accurate diagnosis.50, 51
The second most critical factor is adequate preparation of the cervix. This preparation includes dilation and softening over time. In some cases, acute mechanical dilation over a short time permits D & E abortion to be performed, but frequently it is less than optimum, and sometimes it is catastrophic.
A third factor is the availability of appropriate equipment and instruments for the performance of the procedure. Not having these instruments at critical points can result in unnecessary delays in completing the procedure, unnecessary blood loss, and unnecessary trauma to the patient.
In my opinion, the use of general anesthesia unnecessarily adds considerable hazard and risk to the performance of second-trimester D & E abortion. It is rarely justified.
Rupture of membranes
When the serial multiple Laminaria technique is used, membranes frequently will be visible through the external os just before the D & E procedure, particularly if the fetal age is more than 15 or 16 menstrual weeks. Even if the membranes are not visible, an important question is whether they should be ruptured before evacuation of the uterus is initiated.
It has been my practice to rupture membranes with a ring forceps, packing forceps, single-toothed tenaculum, or long curved Allis clamp just before the use of forceps in pregnancies that are beyond 12 menstrual weeks of gestation. A 12-mm cannula is inserted through the ruptured membranes and the amniotic fluid is allowed to drain as completely as possible without the application of vacuum aspiration. This procedure is routinely performed under direct ultrasound visualization in order to reduce the risk of uterine trauma, to avoid disruption of the placenta if it is low-lying, and to maximize the amount of amniotic fluid released. This action offers several advantages:
- It allows complete drainage of amniotic fluid for measurement or separation. Later, at the end of the operative procedure, fluid in the operating basin is almost all blood and can be measured exactly. This measurement is important if the patient loses enough blood to require volume replacement. In all cases, the information is a matter of more than casual interest. It is an important outcome measure in determining the acute or potential morbidity of the operation.
- Draining the amniotic fluid allows the uterus to contract, thereby helping to close the large venous sinuses and reducing blood loss. The uterine contents are close to the lower uterine segment.
- Removal of the fluid without a sudden hydrostatic change within the uterine cavity, along with closure of the venous sinuses, reduces the risk of amniotic fluid embolism. The danger of this outcome is heightened if placental abruption occurs while the uterus is full of amniotic fluid. Because amniotic fluid embolism is one of the major causes of morbidity and mortality in late abortion, this maneuver is an important means of preventing this potentially catastrophic complication.52 A large bore vacuum aspiration cannula and suction should not be applied prior to complete evacuation of the amniotic fluid as determined by ultasonographic confirmation.
Adjunctive infusion methods
A variety of adjunctive infusion methods have been studied that potentially add to the safety of D & E abortion. These methods include amnioinfusion of a hyperosmolar urea solution and intrafetal injection of digoxin or another feticidal agent.19, 53 Low complication rates have been achieved by a combined use of induced fetal demise, serial multiple laminaria dilation of the cervix, and intrauterine misoprostol placement following amniotomy and prior to induction of labor followed by uterine evacuation.23, 24 Gentle induction with the combination of oxytocin and misoprostol over a period of 1–2 hours frequently results in the presentation of a fetal part, which can be grasped with a single-toothed tenaculum or other instrument to permit a controlled, atraumatic delivery of the fetus and placenta with minimal blood loss. Administration of a pudendal/paracervical block with 20 ml of 1% lidocaine prior to this delivery or D & E provides a good level of analgesia for this procedure. A prior history of cesarean delivery contraindicates the use of oxytocin at the beginning of this process.
We have found that the insertion of 400 µg of misoprostol into the lower uterine segment following the release of all amniotic fluid is extremely helpful in obtaining cervical dilation and effacement and enhancing uterine contraction, especially for patients in whom a history of cesarean delivery contraindicates the use of oxytocin in the early stages of the procedure. We conducted a prospective, randomized controlled cohort study of 1204 patients from 18 to 38 menstrual weeks’ gestation and found that the amniotomy-to-procedure time was reduced by approximately 30 minutes for patients receiving the intrauterine misoprostol following amniotomy.24 This difference, significant at the >0.01 level, is shown in Figure 2:
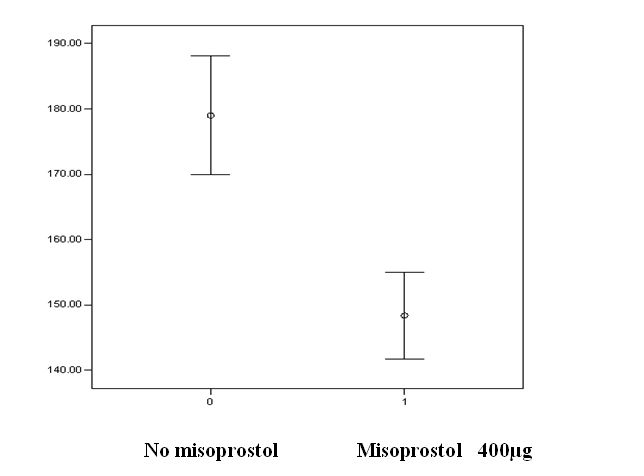 Fig. 2 Confidence intervals, amniotomy-to-procedure times, in minutes, misoprostol 400 μg (1) vs. no misoprostol (0)
Fig. 2 Confidence intervals, amniotomy-to-procedure times, in minutes, misoprostol 400 μg (1) vs. no misoprostol (0)
The operative protocol below was followed for the patients in this series. Although there are a few early second trimester patients in this series who experienced one overnight laminaria dilation of the cervix followed on the second day by a dilation and evacuation abortion procedure, nearly all patients with pregnancies of 15 menstrual weeks or greater experienced a 3 or 4 day multiple laminaria treatment of the cervix following induction of fetal demise on day 1 for those at 18 weeks or more. On the last (3rd or 4th) day, with an IV infusion in place, the laminaria were removed under direct vision, a long-acting paracervical block placed using 12 cc of 0.25% bupivacaine (Marcaine®), and amniotomy performed under direct ultrasound visualization. After insertion of a 12 mm plastic cannula into the uterus under ultrasound visualization, as much of the amniotic fluid as possible was allowed to drain out without the application of vacuum pressure. The amount of amniotic fluid was measured. This procedure was then followed by intrauterine placement of the misoprostol in every other patient following initial randomization. Except for patients with a history of cesarean delivery, 50 u of oxytocin was then added to a 1 liter bag of lactated Ringer’s solution for slow intravenous infusion to induce labor. Narcotic analgesia was applied parenterally for all patients according to pain level and tolerance. Blood pressure, pulse rate, and oxygen saturation levels were monitored at all times when the patient was in the operating room. Following these final preoperative preparations, the patient was transferred to a recovery room to await labor progress. Readiness to return to the operating room for the procedure depended on labor progress, presentation of a fetal part in the cervix, pain, or bleeding.
Upon transfer to the operating table, both a pudendal block and paracervical block were applied immediately using 20 cc of 1% lidocaine (Xylocaine®). The patient then experienced an assisted and controlled fetal delivery followed by immediate removal of the placenta by traction or with forceps. When fetal expulsion did not occur due to poor cervical dilation or uterine atony, the fetus and placenta were removed with forceps specially designed for this purpose.40 All operative procedures were guided by real-time ultrasound visualization. Evacuation of the uterus was always followed by forceps exploration and sharp curettage under ultrasound visualization. At the end of the procedure, 0.2 mg of methylergonovine maleate (Methergine®) was injected directly into the cervix. The patient was then transferred to the recovery room where she was observed for a period of 2 hours. After this, the patient was returned to the operating room where the uterus was palpated and visualized with ultrasound to confirm the presence of an endometrial stripe, and a sterile vaginal speculum was placed to allow visual inspection of the cervix. Any evidence of hematometra or retained tissue resulted in re-aspiration prior to discharge.
Following the completion of the procedure, the fetus and placenta were examined immediately. Both were weighed separately using a balance beam scale, and observations were made when possible of the fetal anomaly that had been identified preoperatively. Measurements were taken to verify the length of gestation including fetal foot length, crown–rump length, rump–shoulder length, chest and abdominal diameter, and biparietal diameter if possible. Length of gestation was determined on the basis of previously established values.50, 51 Total operative blood loss was measured in graduated beakers.
All patients received routine antibiotic coverage after the abortion procedure, and those experiencing intrafetal injection also received chemoprophylaxis. The initial standard protocol was 100 mg of doxycycline orally immediately following the intrafetal injection, followed by 100 mg twice a day for 6 days. Patients allergic to doxycycline were given ampicillin or erythromycin. At discharge, patients were given metronidazole 500 mg twice a day for 5 days. Rh-immune globulin was administered to all patients who were Rh-negative.
In this series of 1204 patients, using the Centers for Disease Control definition of major complication (major unintended surgery; hemorrhage requiring transfusion; pelvic infection with 2 or more days of fever and a peak of at least 40ºC or with hospitalization for 11 or more days),54 there were no major complications.
MANAGEMENT OF COMPLICATIONS
Complications in abortion can be classified into five major categories: (1) error in the estimate of the length of gestation; (2) failure to empty the uterus; (3) failure to avoid trauma; (4) other iatrogenic complications; and (5) functional problems.
Error in the estimate of gestational length
An orderly review of the major sources of complications and their management must begin with a discussion of preoperative evaluation and accurate estimation of gestational length. One way to establish a positive diagnosis of pregnancy before early abortion is to perform a routine ultrasound examination with an abdominal or vaginal probe. This excellent procedure eliminates the guesswork and permits the exclusion or evaluation of more complicated diagnoses, such as hydatidiform mole and ectopic pregnancy.
A different problem occurs when the initiation of a procedure shows serious underestimation of the length of gestation. This problem may be prevented to some degree by routine ultrasound examination of patients whose pelvic examination shows a uterus that is large for dates or borderline between first and second trimester. The latter distinction is somewhat false because the operator encounters a spectrum of increasing difficulty from the 12th menstrual week on, and each week of gestation brings a different type of complexity. Familiarity with the techniques of early mid-trimester D & E abortion will help the practitioner to manage these situations.
It is embarrassing, not to mention dangerous to the patient, for the practitioner to begin what is presumed to be a routine first-trimester abortion only to be showered with amniotic fluid along with discovery that the 'uterus' is actually the 'fetal head'. It is even worse when the discovery proceeds to the realization that the woman is not in the second trimester but is about to deliver a baby that is near term.
Routine preoperative sonographic evaluation for diagnosis of gestational length, at minimum, has become the standard of care in both first- and second-trimester abortion. There is no justification for not performing this basic diagnostic evaluation.
Failure to empty the uterus
Intraoperative ultrasound has become an important adjunctive tool in second-trimester D & E abortion. Ultrasound does not supplant the proprioception necessary to careful application of surgical instruments, but it can reveal important facts about the location of major tissue to be removed and guide the placement of instruments.
A continued pregnancy, hemorrhage, and infection are the principal signs of failure to empty the uterus, with the latter two being the most common. A continued pregnancy may result from the causes described in the previous section or from an unsuspected uterine anomaly. It is a known complication of first trimester medical abortion.55, 56, 57, 58, 59, 60 Treatment in the case of failed medical abortion consists of a vacuum aspiration curettage procedure.
The signs and symptoms of retained tissue are cramping, heavy bleeding, and infection signaled by fever. Problems resulting from an incomplete abortion usually will occur within 1 week, if not sooner, but unusually heavy bleeding several weeks after the abortion should be considered evidence of retained tissue until proved otherwise. The most reliable indication of retained tissue is bleeding, particularly when prophylactic antibiotics have been given to the patient. As a rule of thumb, bleeding that is significantly heavier than the normal menstrual flow indicates re-aspiration. A history of sudden hemorrhage that then ceased is valuable. The intervening use of tampons may prevent the examiner from seeing the evidence of this bleeding, but the history alone suggests further study.
A high fever (102°F [39°C] or more) within 72 hours of abortion should be considered evidence of retained tissue with sepsis until proved otherwise. The patient should be treated by prompt re-aspiration followed by intravenous administration of antibiotics in combinations designed for anaerobic and microaerophilic bacteria.
After initial blood cultures, cefoxitin 1–2 g intravenously every 6–8 hours may be used. Other alternatives are combinations of clindamycin, chloramphenicol, or one of the cephalosporins with ampicillin or a penicillinase-resistant penicillin.
Milder infections indicated by a fever of less than 102°F (39°C) and moderate uterine tenderness may be treated with oral antibiotics and reaspiration. An excellent first choice is doxycycline 100 mg twice a day for 10 days, although Cipro® (ciprofloxacin hydrochloride) 250 mg b.i.d. for 5 days can also be used when doxycycline is not available.
Patients who experience cramps and moderate bleeding within a few days after abortion but whose symptoms do not seem severe may be advised to massage the uterus firmly while sitting on the toilet at intervals of 1–2 hours. Frequently, this treatment results in passage of small clots and relief of symptoms. If this remedy is not effective or if symptoms become worse, the patient should be seen for re-aspiration. When in doubt, re-aspiration is the treatment of choice.
The controversy concerning the use of prophylactic antibiotics in abortion continues.61, 62, 63 Many recommend the use of doxycycline 100 mg twice a day for 5 days after abortion as preemptive antibiotic therapy. The grounds for this recommendation are that, by definition, abortion cannot be a sterile operation, and every uterus is contaminated, no matter how careful the operator. Most patients overcome this contamination with natural resistance, but some do not. Because most abortion patients are young and experiencing their first pregnancy, the benefits of protecting their reproductive capability outweigh the disadvantages of routine antibiotic administration. Difficulty in obtaining doxycycline has led many physicians to give Cipro® (ciprofloxacin hydrochloride) 250 mg b.i.d. for 5 days as a routine postoperative antibiotic.
Failure to avoid trauma
There are various approaches to the management of uterine perforation, with treatment depending on the severity of perforation. When perforation of the uterine fundus is recognized before a first-trimester abortion procedure has begun, it may be managed by observation, treatment with oral antibiotics, and delay of the abortion for 2–3 weeks. Perforation occurring before second-trimester abortion is far more serious and normally requires laparotomy and repair.
Recognition of the perforation, however, may occur with the report of generalized abdominal pain by the patient during vacuum aspiration, in the case of the first-trimester abortion, or during instrumental evacuation of the uterus, in the case of second-trimester abortion. This event may be accompanied by the discovery of mesenteric fat in the aspirate or the appearance of small bowel in the forceps or vacuum cannula. Another sign of uterine injury is the presence of blood in the urine, which indicates not only uterine but bladder wall laceration. Such an event requires immediate laparotomy to repair damage to the bowel or other viscera and to complete the abortion under direct visualization of the uterus. If the patient is under general anesthesia, she can neither feel nor report pain that accompanies this potentially catastrophic complication before it becomes a catastrophe.
Perforation laterally into the uterine artery may be impossible to treat, except with hysterectomy or uterine artery ligation. There is no satisfactory way to staunch the bleeding or for the artery to contract. A catastrophic perforation of this type may not be evident for several hours after the abortion, when the patient, having left the recovery room in apparently good condition, goes into shock and dies.
Lacerations of the cervix at the level of the internal os may present the same set of problems seen with overly vigorous manual dilation. Immediate treatment may require digital pressure on the uterine arteries to control bleeding while intravenous oxytocin is administered and the patient is transported to the operating room for laparotomy and repair.
Cervical lacerations of the external os that result from tenaculum tears may be minimized by using Laminaria, but when they occur, they usually can be treated by closure with one or two sutures of 2-0 chromic material in a simple or figure-of-eight placement.
Other iatrogenic complications
Anesthesia deaths, however uncommon in comparison to other abortion-related deaths, continue to occur and are common enough to cause concern. Although attention has been focused on deaths from local anesthesia, complications and deaths from general anesthesia also have occurred. The common denominator in the deaths from local anesthesia has been toxic or unknown dose levels resulting in convulsions and cardiorespiratory arrest. The importance of staying within the toxic dose levels and avoiding direct intravascular injection cannot be overemphasized.
For example, it rarely is necessary to use more than 20 ml of 1% lidocaine (200 mg) for a paracervical block, or the equivalent. The addition of epinephrine 1:200,000 reduces absorption of this agent and also may reduce the risk of vasovagal reaction. As already noted, the use of Laminaria for dilation further reduces the need for local anesthesia. Only 2–4 ml of 1% lidocaine is necessary for the tenaculum site, and a total of 10–12 ml is necessary for the entire block (2 ml each at 3:00, 5:00, 7:00, 9:00, and 12:00). A deeper block may be given by injection of an additional 2 ml each at 10:00, 2:00, 5:00, and 7:00.
Management of anesthesia reactions caused by toxic doses consists principally of cardiopulmonary resuscitation and basic system support. Obvious allergic reactions may be managed by the administration of intravenous epinephrine, intramuscular diphenhydramine, and intravenous aminophylline, if necessary.
Deaths resulting directly from the use of general anesthesia, such as aspiration of vomitus, can be prevented by not using general anesthesia.
Functional complications
To some degree, some complications of abortion seem to be independent of the operator's competence or thoroughness in approach. Some complications may be preventable, but the plan for prevention is not clear. These complications include uterine atony, uterine anomalies, post-abortion hematometra, vasovagal reaction, previously undiagnosed uterine wall adenomyosis, cardiopulmonary arrest not associated with anesthesia toxicity, amniotic fluid embolism with or without subsequent coagulopathy, postabortion amenorrhea, rhesus factor isoimmunization, postabortion depression, ectopic pregnancy, pre-existing infection or inflammation, and hydatidiform mole.64, 65, 66, 67, 68, 69, 70
Extremely heavy bleeding is not rare in later abortion; however, patients who are only 13–14 weeks or more from the last menstrual period, in poor nutrition, multiparous, or recently delivered of a term infant, not to mention patients with fibroids or placenta previa, may experience uterine atony and bleed briskly.
In the event of this type of hemorrhage, even if a perforation is not suspected, the first step in treatment may be to remove the speculum and place digital pressure over the uterine arteries bilaterally. If an intravenous line is not already in place (it should be), an assistant should start an intravenous line with Ringer's lactate solution and place at least 40–50 units of oxytocin in the bottle to run wide open through a minimum 18-gauge needle or the equivalent. Methylergonovine maleate may be given intramuscularly or directly into the cervix.
Once the situation appears to be under control, a ring or other smooth forceps should be placed gently into the uterine cavity to grasp placental tissue that may be remaining. Whether this approach succeeds or fails, it should be followed by insertion of the largest curet that the cervix will accept easily. Use of these two instruments should permit an evaluation of the situation as well as empty the uterus of remaining tissue. This maneuver will allow the uterus to continue to contract and further control bleeding. If a perforation has occurred, further damage is less likely to develop. As the uterus contracts, assuming that no perforation is present, suction may be applied to continue the process of evacuation.
Bleeding that persists after the uterine cavity appears to be empty may have one of three causes: (1) atony, (2) cervical trauma, or (3) disseminated intravascular coagulation (DIC) syndrome. A simple method for making the determination between the first two is to place a suction cannula tip well into the cavity to determine whether persistent bleeding occurs. If it does, the cause probably is atony. If no bleeding occurs until the suction cannula is withdrawn to the level of the internal os or cervical canal, the answer is apparent. The treatment is the same: manual compression and massage of the uterus accompanied by the administration of oxytocin and methylergonovine maleate. The insertion of 400 µg or more of misoprostol rectally may be helpful. The intramuscular administration of 15-methyl prostaglandin (Hemabate®) may be used as a last resort for the pharmacologic control of noncoagulopathic hemorrhage.
Continued heavy bleeding from either site (fundal or cervical) may indicate either perforation into the uterine artery, which requires operative intervention, or DIC syndrome.
The management of DIC syndrome first requires recognition. Coagulopathy should be anticipated or suspected whenever a second-trimester abortion patient experiences signs or symptoms of intraoperative amniotic fluid embolism (e.g. coughing, dyspnea, chest pain, cyanosis, convulsions, cardiorespiratory arrest) or when profuse bleeding from the fundus is accompanied by bleeding from needle puncture sites and the whole blood does not clot in a plain glass tube. Baseline studies of the following parameters should be obtained: serum fibrinogen level, fibrin split (degradation) product value, prothrombin and partial thromboplastin times, platelet count, hematocrit value, and hemoglobin level. If the uterus is empty, the bleeding should not persist for longer than 10–15 minutes with the combination of oxytocin, manual compression, and administration of methylergonovine maleate and 15-methyl prostaglandin. If bleeding persists, fresh whole blood may be given. The blood can be supplemented or substituted with fresh frozen plasma and packed cells or cryoprecipitate. A rising platelet count, rising fibrinogen value, or declining level of fibrin split products indicates recovery. Results of D-dimer (fibrin split product) and some other studies may remain abnormal for 12–24 hours.
Post-abortion hematometra usually refers to uterine atony or hypotonia occurring shortly after an otherwise uncomplicated early abortion, although this is sometimes seen in second-trimester patients, especially in patients who have difficulty in emptying their bladder.41, The patient typically reports uterine pain within an hour after the abortion, although this condition may take several hours to develop. On examination, the uterus is enlarged to 10–12 weeks' size, tender, and boggy. Signs of acute abdomen are absent. Reaspiration results in recovery of 50–200 ml of blood clots, no tissue, and immediate relief of symptoms. An excellent practice is intramuscular application of methylergonovine maleate as the re-aspiration is completed, followed by 3 days of oral medication.
Post-abortion hematometra can be prevented in most cases by routine intramuscular or intracervical administration of methylergonovine maleate 0.2 mg immediately upon completion of the abortion procedure and then by mouth three times a day for 3 days. When injectable methylergonovine maleate (Methergine® ) is not available for immediate postoperative administration, two tablets of misoprostol 200 µg may be inserted rectally with good effect.
In second trimester patients, it is critically important to assure that immediate postoperative bladder emptying is complete as verified by bimanual and ultrasound examination just before discharge. A full bladder in a patient unable to urinate prevents efficient uterine contraction, which can lead to hematometra, and which in turn can led to consumption coagulopathy. Catheterization with a simple 10 cm straight catheter allows full contraction of the uterus with a return of uterine tone and cessation of bleeding.
Post-abortion depression that is severe enough to require psychiatric treatment is rare, particularly if the abortion is conducted in a supportive atmosphere with preoperative counseling. Patients who experience this condition should be referred to a psychiatrist for extended treatment after evaluation by the abortion service personnel. Post-abortion psychosis without a history of pre-abortion psychiatric illness has not been reported.
Hydatidiform moles occur 1 in 1000 or more pregnancies, and the diagnosis usually is apparent preoperatively in the ultrasound examination. It is apparent to the physician during the abortion procedure, particularly if a clear plastic cannula is used for aspiration. The tissue is obvious, even in early pregnancy, but routine histopathologic examination should be obtained.
Management consists primarily of serial β subunit human chorionic gonadotropin titers until results are negative to exclude the existence of malignant trophoblastic material. Pregnancy should be prevented for the subsequent year, preferably through oral contraception because of its high level of effectiveness.
DISCUSSION
There are few fields of medicine that have evolved so rapidly and in so many ways during the past four decades as abortion services. The introduction of synthetic prostaglandins has resulted in many changes in practice since 1971. The introduction of mifepristone and misoprostol in the 1980s and 1990s has altered or, at least, expanded the approaches to first trimester abortion, and now, second trimester abortion. The best way to achieve cervical dilation and softening prior to abortion remains controversial: should one use rigid metal dilators as a sole method of dilation, some kind of hygroscopic agent such as Laminaria or Dilapan®, a strictly medical method such as mifepristone or misoprostol, or some combination of all these?7, 10, 11, 14, 15, 17, 22, 34, 71 How much damage is done to the cervix by acute manual dilation with metal dilators, how much does manual dilation add to the risk of uterine perforation, and is forceful dilation necessary?20, 44, 45, 46 Should prophylactic (or “pre-emptive”) antibiotics be given or not?61, 62, 63
Should anesthesia be by local or regional block, by general anesthesia, by “deep sedation,“ by “conscious sedation,” or some combination? This is an important choice because at least one study showed the most important causes of death in abortion over a 5-year period were anesthesia-related complications.72
General anesthesia contributes significantly to the death rate in labor and delivery, and reports indicate that local anesthesia is safer than general anesthesia in abortion.35, 36, 37, 38, 73 This being the case, what is the justification for general anesthesia in abortion? Abortion is safer than term delivery.74 Why add an unnecessary risk to abortion by using general anesthesia?
In one series of 62,125 abortions including over 11,000 second-trimester abortions under deep sedation with propofol without intubation, only one patient received endotracheal intubation, and there were no incidents of perioperative pulmonary aspiration.75 Other outcome variables and/or complications are not described. This series occurred in a large urban surgical abortion outpatient facility with significant institutional and financial support that is not normally available in smaller clinics and private physicians’ offices. The excellent results with the two variables obtained in this setting reflects superior – exceptional – anesthesia practice, but it does not mitigate the range of concerns and possible complications of general anesthesia (or “deep” or “conscious” sedation) in other settings. The universal objectives in second-trimester abortion are, first, safety for the patient, and second, relief of pain and comfort for the patient. The challenge is to obtain the maximum of both objectives at the same time.
Should the abortion be performed by D & E or by induction of labor?76, 77 Is this a useful distinction, or is it a false dichotomy? Does this dichotomy cause us to exclude other ways of looking at an eclectic approach determined by the patient’s peculiar need and set of risks?78 A protocol for late abortion that relies exclusively on induction of labor may result in situations in which completion of the abortion becomes impossible or cannot even begin. These situations include a prior history of cesarean delivery, the presence of complete placenta previa, low-lying placenta that results in uncontrollable bleeding, massive fibroids, breech or shoulder presentation of the fetus, uterine atony or hypotonia, hydrocephaly, or conjoined twins. The only recourse in some of these situations would be hysterotomy, which carries its own set of risks, or the availability of a physician skilled in D & E and the instruments that are necessary.
The methods of and motives for induced fetal demise have changed from the use of hyperosmolar saline in the early 1970s to hyperosmolar urea solution in the 1980s to induction of fetal demise by intra-amniotic or intrafetal digoxin. The latter practices are controversial, with some practitioners using intrafetal digoxin routinely for reasons of patient safety,23, 24, 79, 80, 81, 82 others using intra-amniotic digoxin,83, 84, 85, 86, 87 and yet others denouncing these techniques as dangerous, unethical and unnecessary.78, 88 There is additional controversy in the medical community concerning whether the injection of digoxin, whether intrafetal or intraamniotic, should occur transabdominally or transvaginally.89, 90, 91, 92, 93, 94 Some of the controversy rests on which technique will yield the best results for research objectives.95 Shall the patient decide whether induced fetal demise should occur?96 Does leaving this medical decision to the patient mean that it is simply a personal choice with no medical consequences or changes in risk? Does the report that induced fetal demise makes the procedure easier for the surgeon matter and should prevail in this decision?97
The method of causing fetal demise by preoperative umbilical cord transection (UCT) used by Finks4 and then abandoned in the United Kingdom was recently re-introduced in the United States, but the use of this procedure was ended for reasons of safety.98, 99, 100, 101
Is the placenta removed by cord traction or with forceps immediately following delivery or removal of the fetus, or is the time-honored “third stage of labor” observed while waiting for the placenta to be expelled spontaneously?102, 103 Immediate removal has been our standard practice in late abortion for over 40 years, and the efficacy of this concept is beginning to penetrate the conventional practice of obstetrics.104
Is blood loss estimated or measured? The two amounts may be quite different, and knowing the actual amount of blood loss may be necessary to give the patient proper treatment.105
Is amniotic fluid released before the induction or D & E is begun? Amniotic fluid embolism is a known risk of pregnancy, and it is a cause of death or serious morbidity in second trimester abortion.52, 69, 70 While it may seem too obvious to state, amniotic fluid that has been allowed to drain out of the uterus into a basin cannot go to the patient’s heart and lungs and cause immediate death, and neither can it cause a terrifying and possible fatal coagulopathy. The simple act of releasing the amniotic fluid preoperatively may not be a 100% guarantee against these calamities, but will clearly minimize the risk.
D & E in second trimester clearly transfers the emotional stress of the abortion procedure from the patient to the operator, by contrast with earlier saline abortions accompanied by expulsion of a fetus that might show signs of life. Isn’t this in the interest of the patient?106 Isn’t that one of the main aims of medical practice?
The medical issues of late abortion have been confounded by the passage into law by the US Congress of a prohibition of the so-called “Partial-Birth Abortion Act,” which caused some practitioners to begin including induced fetal demise in their protocol in order to avoid prosecution under this law.88 What are the ethical implications and consequences of a medical decision by physicians and practice being determined or even guided by a state or federal law passed and signed into law by legislators and executives who are wholly ignorant of medical issues? What are the ethical implications of physicians accepting this instruction?
There is a need for late abortions because of delayed diagnosis of fetal abnormality or genetic defect.53, 77, 80, 107, 108 Some abnormalities do not become apparent until very late in pregnancy such as after the 30th week, and some physicians withhold critical diagnostic information from patients because of their opposition to the patient’s having an abortion. These patients may find themselves in a desperate situation as they search for someone who can terminate the afflicted pregnancy. This search can be restricted by state or national laws and by the lack of physicians willing or able to perform such a procedure. Failed medical abortion in early pregnancy sometimes presents as an advanced pregnancy. How best is this to be managed?57
We do not even agree on what to call what we are doing.109, 110 What is an “elective abortion?” Are there “compulsory” or “involuntary” abortions? Does the phrase “elective abortion” mean that the abortion is of no medical consequence or is comparable to cosmetic surgery? What is a “late abortion?” What is a “late-term abortion,” as it is frequently called; what does that mean? Grimes pointed out that the definition of abortion is “expulsion or removal of fetus before it is viable,” and therefore, termination of the pregnancy in the last few weeks or months is not an “abortion” but a “termination of pregnancy.” Yet the term “abortion” is widely used for these cases, and the distinctions are not clear. When is a fetus “viable?” It may depend on the level of sophistication of medical care in the patient’s place of residence. How important is the definition of “viability” of the fetus in the decision by the woman to terminate the pregnancy or for the physician to help her do so? These are difficult and important questions that may have many answers or no answers that are universally accepted.
What about the twin pregnancy in which one twin is healthy and the other afflicted with a catastrophic diagnosis? If the woman wants to have one healthy baby and not carry the other fetus to term, and does not wish to terminate the desired pregnancy completely, how is that accomplished? The possibilities are medically difficult and fraught with profound ethical issues.111
The need for late abortion will continue to grow as more women seek to become pregnant in the last few years of their reproductive lives and the advances in diagnosis of fetal abnormalities continues to advance at warp speed.53, 80, 111, 112 The maternal mortality ratio is increasing in the United States, partly because an increasing number of older women are stricken with cardiovascular and other disease that are age-related.113, 114 Spontaneous fetal death in utero and/or spontaneous fetal demise in advanced pregnancy presents a problem of surgical and management which can be remedied immediately with a minimum risk of complications by D & E and adjunctive measures.53, 77, 80, 112, 115, 116, 117 What is the best choice for a patient afflicted with pre-eclampsia?118 What are the effects of labor induction or D & E for termination of pregnancy on obstetrical management in later desired pregnancies?119, 120, 121
The general characteristics of women in the reproductive age range have changed dramatically over the past 50 years. There are comparatively more women having their first pregnancies, and any pregnancies, in the later years of their reproductive lives, they are more likely to have high risk pregnancies that require intervention in the form of late abortion, and the success of these pregnancies may depend more than previously on the correct management of previous pregnancies that ended in induced abortion.
CONCLUSION
For the first time in human history, safe abortion is available for women who choose to or need to terminate a pregnancy. This is a remarkable development over the past 50 years. There has been a series of significant steps in the evolution in both first and second trimester abortion during this time. Good medical practice requires adherence to the highest standards of medical care and surgical practice including a high level of operator skill, sound preoperative diagnosis, careful attention to sterile technique and the prevention of infection, gentle handling of tissue, and conscientious follow-up care with the efficacious management of complications. Second-trimester surgical abortion requires the utmost attention to these principles and details because the consequences of failure can be so immediate and catastrophic.
Second-trimester abortion will continue to be needed as an essential component of women’s health care for many reasons, and these include advanced pregnancy in very young, inexperienced, adolescent women who may have been sexually abused, adult women who discover a pregnancy advanced to beyond the first trimester, women whose advanced pregnancy is an acute threat to life and health, and women in the later reproductive years whose pregnancies are afflicted with serious medical disorders or catastrophic fetal abnormality. These pregnancies can be safely terminated in a variety of ways; second-trimester surgical abortion is an essential method that must be available within the medical community.
REFERENCES
Tietze C, Lewit S: Joint Program for the Study of Abortion (JPSA): Early medical complications of legal abortion. Stud Fam Plann 3: 97, 1972 |
|
Life magazine February 27, 1970 |
|
Bierer I, Steiner V: Termination of pregnancy in the second trimester with the aid of Laminaria tents. Med Gynaecol Sociol 6: 9, 1972 |
|
Finks AA: Mid-trimester abortion. The Lancet 301:263, 1973 |
|
Davis G: Mid-trimester abortion. The Lancet 300:1026, 1973 |
|
Grimes DA, Schulz KF, Cates W Jr et al: Midtrimester abortion by dilation and evacuation: A safe and practical alternative. N Engl J Med 296: 1141, 1977 |
|
Hern WM, Oakes AG: Multiple Laminaria treatment in early midtrimester outpatient suction abortion: A preliminary report. Adv Plann Parent 12: 93, 1977 |
|
Hern WM: Laminaria in abortion: Use in 1368 patients in first trimester. Rocky Mountain Med J 72: 390, 1975 |
|
Neubart S: The Japanese Experience. In Neubardt S, Schulman H: Techniques of Abortion, 1st ed,. p 139. Boston, Little, Brown & Co, 1972 |
|
Barr MM: Midtrimester abortion 12–20 weeks by dilatation and evacuation method under local anesthesia. Adv Plann Parent 13: 16, 1978 |
|
Hanson MS: Midtrimester abortion: Dilatation and extraction preceded by Laminaria. In Zatuchni GI, Sciarra JJ, Speidel JJ (eds): Pregnancy Termination: Procedures, Safety, and New Developments, p 191. New York, Harper & Row, 1979 |
|
Hern WM: Midtrimester abortion. In Obstetrics and Gynecology Annual,1981, Ralph M. Wynn, Ed. Appleton-Century-Crofts, New York, 1981 |
|
Stubblefield PC: Laminaria and other adjunctive methods. In Berger GS, Brenner WE, Keith LG (eds): Second Trimester Abortion: Perspectives After a Decade of Experience, p 135. Boston, John Wright & Sons, 1981 |
|
Hern WM: Outpatient second-trimester D & E abortion through 24 menstrual weeks' gestation. Adv Plann Parent 16: 7, 1981 |
|
Allman A, Stubblefield PG, Parker K et al: Midtrimester abortion by Laminaria and vacuum evacuation on a teaching service: A review of 789 cases. Adv Plann Parent 16: 1, 1981 |
|
CadeskyKI, Ravinsky E, Lyons ER: Dilation and evacuation: A preferred method of midtrimester abortion. Am J Obstet Gynecol 139: 329, 1981 |
|
Peterson WF, Berry FN, Grace MR et al: Second trimester abortion by dilation and evacuation. Obstet Gynecol 62: 185, 1983 |
|
Hern WM: First and second trimester abortion techniques. Current Problems in Obstetrics and Gynecology 6, 1983. |
|
Hern WM: Serial multiple laminaria and adjunctive urea in late outpatient second trimester dilatation and evacuation abortion. Obstet Gynecol 63: 543, 1984 |
|
Robinson G: A comparative study of Dilapan and Laminaria for treatment of the cervix prior to serial dilation for termination of first trimester pregnancy. Presented at the National Abortion Federation Annual Meeting, San Diego, CA, April 13, 1992 |
|
Hern, W.M.: Cervical treatment with Dilapan prior to second trimester dilation and evacuation abortion: A pilot study of 64 patients. American Journal of Gynecologic Health 7(1):15-18, 1993. |
|
Hern, W.M.: Laminaria versus Dilapan osmotic cervical dilators for outpatient dilation and evacuation abortion: Randomized cohort comparison of 1001 patients. Am J Obstet Gynecol 171:1324, 1994. |
|
Hern WM: Laminaria, induced fetal demise and misoprostol in late abortion. Int J Gynecol Obstet 75:279, 2001. |
|
Hern WM: Misoprostol as an adjunctive medication in late surgical abortion. Int J Gynecol Obstet 88:327, 2005 |
|
Goldberg AB, Drey EA, Whitaker AK, Kang MS, Meckstroth KR, Darney PD: Misoprostol compared with laminaria before early second-trimester surgical abortion: a randomized trial. Obstet Gynecol 106:234, 2005 |
|
Bartz D, Maurer R, Allen RH, Fortin J, Kuang B, Goldberg AB: Buccal misoprostol compared with synthetic osmotic cervical dilator before surgical abortion: a randomized controlled trial. Obstet Gynecol 122:57, 2013 |
|
Dickinson JE, Jennings BG, Doherty DA: Mifepristone and oral, vaginal, or sublingual misoprostol for second-trimester abortion: a randomized controlled trial. Obstet Gynecol 123:1162, 2014 |
|
Goldberg AB, Fortin JA, Drey EA et al: Cervical preparation before dilation and evacuation using adjunctive misoprostol or mifepristone compared with overnight osmotic dilators alone: A randomized controlled trial. Obstet Gynecol 126:599, 2015 |
|
Kapp N, Borgatta L, Stubblefield P et al: Mifepristone in Second-Trimester Medical Abortion. Obstet Gynecol 107:1304, 2007 |
|
Shaw KA, Nicole J, Shaw JG et al: Mifepristone-Misoprostol dosing interval and effect on induction abortion times: A systematic review. Obstet Gynecol 121:1335. 2013 |
|
Elami-Suzin M, Freeman MD, Porat N et al: Mifepristone followed by misoprostol or oxytocin for second-trimester abortion. Obstet Gynecol 122:815, 2013 |
|
Paris A, Sonalkar S, Kattan D et al: Mifepristone and Misoprostol compared with osmotic dilator insertion before surgical abortion at 15-18 weeks. Obstet Gynecol 123:5S 2014 |
|
Dickinson J, Jennings B, Dhorty DA: Mifepristone and oral, vaginal, or sublilngual misoprostol for second-trimester abortion: A randomized controlled trial. Obstet Gynecol 123:1162, 2014 |
|
Fox MC, Krajewski CM: SFP Guideline: Cervical preparation for second-trimester surgical abortion prior to 20 weeks’ gestation. Contraception 89:75, 2014 |
|
Grimes DA, Schultz KF, Cates W Jr et al: Local versus general anesthesia: Which is safer for performing suction curettage abortions? Am J Obstet Gynecol 135: 1030, 1979 |
|
Peterson HB, Grimes DA, Cates W Jr et al: Comparative risk of death from induced abortion at <12 weeks' gestation performed with local versus general anesthesia. Am J Obstet Gynecol 141: 763, 1981 |
|
McKay HT, Schulz KF, Grimes DA: Safety of local versus general anesthesia for second-trimester dilatation and evacuation abortion. Obstet Gynecol 66: 661, 1985 |
|
Atrash HK, Cheek TG, Hogue CJR: Legal abortion mortality and general anesthesia. Am J Obstet Gynecol 158: 420, 1988 |
|
Hern WM. Evolution of second trimester abortion techniques. In Prevention and Treatment of Contraceptive Failure, U. Landy and S.S. Ratnam, eds. New York: Plenum Press, 1986. |
|
Hern WM: Abortion Practice. Philadelphia: JB Lippincott Co., 1984; Boulder: Alpenglo Graphics, 1990 |
|
Grimes DA: Surgical management of abortion. In Thompson JD, Rock JA (eds): TeLinde's Operative Gynecology, 7th ed, p 337. Philadelphia, JB Lippincott, 1992 |
|
Stubblefield PG, Carr-Ellis S, Borgatta L: Methods for induced abortion. Obstet Gynecol 104:174, 2004 |
|
Paul M, Lichtenberg E, Borgatta L et al (eds): Management of Unintended and abnormal pregnancy. Oxford: Wiley-Blackwell, 2009. |
|
Tokarz RD, Wiliford JF, Soderstrom RM: Mobility of fluid as a factor in acute therapeutic dilatation of the human cervix. Adv Plann Parent 16: 22, 1981 |
|
Schulz KF, Grimes DA, Cates W Jr: Measures to prevent cervical injury during suction curettage abortion. Lancet 1:1t82, 1983 |
|
Grimes DA, Schulz KF, Cates W Jr: Prevention of uterine perforation during curettage abortion. JAMA 251:2108, 1984 |
|
Fischer M, Bhatnagar J, Guarner J et al: Fatal toxic shock syndrome associated with Clostridium sordelli after medical abortion. N Engl J Me 353:2342, 2005 |
|
Green MF. Fatal infections associated with mifepristone-induced abortion. N Engl J Med 353:2317, 2005 |
|
Prolova AI, Stout MJ, Tuuli MG et al: Duration of the third stage of labor and risk of postpartum hemorrhage. Obstet Gynecol 127:951, 2016 |
|
Hern WM, Miller WA, Paine L et al: Correlation of sonographic cephalometry with clinical assessment of fetal age following early midtrimester D & E abortion. Adv Plann Parent 13: 14, 1978 |
|
Hern WM: Correlation of fetal age and measurements between 10 and 26 weeks of gestation. Obstet Gynecol 63: 26, 1984 |
|
Lawson HW, Atrash HK, Franks AL: Fatal pulmonary embolism during legal induced abortion in the United States from 1972 to 1985. Am J Obstet Gynecol 162: 986, 1990 |
|
Hern WM, Zen C, Ferguson KA et al: Outpatient abortion for fetal anomaly and fetal death from 15 to 34 menstrual weeks' gestation: Techniques and clinical management. Obstet Gynecol 81: 301, 1993 |
|
Grimes DA, Schulz KF, Cates W Jr et al: The Joint Program for the Study of Abortion/CDC: a preliminary report. In Hern WM, Andrikopoulos B, editors. Abortion in the Seventies. p 41. New York: National Abortion Federation, 1977 |
|
Spitz IM, Bardin CW, Benton L et al: Early pregnancy termination with mifepristone and misoprostol in the United States. New Engl J Med 338:1241, 1998 |
|
Kahn JG, Becker BJ, MacIsaac L, et al. The efficacy of medical abortion: a meta-analysis. Contraception 61:29, 2000 |
|
Reeves M, Kudva A, Creinin M. Medical abortion outcomes after a second dose of misoprostol for persistent gestational sac. Contraception 78:332, 2008 |
|
El-Refaey H, Rajasekar D, Abdalla M et al: Induction of abortion with mifepristone (RU 486) and oral or vaginal misoprostol. N Engl J Med 332:983, 1995 |
|
Schaff EA, Fielding SL, Eisinger SH et al: Low-dose mifepristone followed by vaginal misoprostol at 48 hours for abortion up to 63 days. Contraception 61:41, 2000 |
|
Winikoff B, Dzuba I, Creinin M, et al: Two distinct oral routes of misoprostol in mifepristone medical abortion. Obstet Gynecol 112:1303, 2008 |
|
Hodgson JE, Major B, Portmann K et al: Prophylactic use of tetracycline for first trimester abortions. Obstet Gynecol 45: 574, 1975 |
|
Darj E, Stralin EB, Nilsson S: The prophylactic effect of doxycycline on postoperative infection rate after first-trimester abortion. Obstet Gynecol 70: 755, 1987 |
|
Levallois P, Rioux JE: Prophylactic antibiotics for suction curettage abortion: Results of a clinical controlled trial. Am J Obstet Gynecol 158: 100, 1988 |
|
Ben-Ami I, Fuchs N, Schneider D et al: Coagulopathy associated with dilation and evacuation for second-trimester abortion. Acta Obstet Gynecol Scand 91:10, 2012 Doi:10.1111/j.1600-0412.2011.01296x |
|
Upadhyay UD, Desai S, Zlidar V et al: et al: Incidence of emergency department visits and complications after abortion. Obstet Gynecol; 175:175, 2015 |
|
Roncari D, Politch JA, Sonalkar S et al: Inflammation or infection at the time of second trimester induced abortion. Contraception 87:67, 2013 |
|
Steward R, Melamed A, Kim R et al: Infection and extramural delivery with use of digoxin as a feticidal agent. Contraception 85:150, 2012 |
|
Nucatola D, Roth N, Gatter M: A randomized pilot study on the effectiveness and side-effect profiles of two doses of digoxin as fetocide when administered intraamniotically or intrafetally prior to second-trimester surgical abortion. Contraception 81:67, 2010 |
|
Guidotti RJ, Grimes DA, Cates W Jr. Fatal amniotic fluid embolism during legally induced abortion, United States, 1972 to 1978. Am J Obstet Gynecol 141:257, 1981 |
|
Cates W Jr, Boyd C, Halvorson-Boyd G et al: Death from amniotic fluid embolism and disseminated intravascular coagulation after a curettage abortion. Am J Obstet Gynecol 141:346, 1981 |
|
Dabash R, Chelli H, Hajri S et al: A double-blind randomized controlled trial of mifepristone or placebo before buccal misoprostol for abortion at 14-21 weeks of pregnancy. Int J Gynecol Obstet 130:40, 2015 |
|
Lawson HW, Frye A, Atrash HK, et al: Abortion mortality, United States, 1972 through 1987. Am Jo Obstet Gynecol 171:1365, 1994. |
|
Hawkins JL, Chang J, Palmer SK et: Anesthesia-related maternal mortality in the United States: 1979-2002. Obstet Gynecol 117:69, 2011 |
|
Raymond EG, Grimes DA: The comparative safety of legal induced abortion and childbirth in the United States. Obstet Gynecol 119 (pt 1):215, 2012 |
|
Dean G, Jacobs AR, Goldstein RC, et al: The safety of deep sedation without intubation for abortion in the outpatient setting. J Clin Anesth 23:437, 2011 doi: 10.1016/j.jclinane.2011.05.001. Epub 2011 Aug 9. |
|
Whitley KA, Trinchere K, Prutsman W et al: Midtrimester dilation and evacuation versus prostaglandin induction: a comparison of composite outcomes. AJOG 205:386.e1, 2011 |
|
Bryant A, Stuart G, Grimes DA: Dilation and evacuation vs. labor induction for fetal indications: A retrospective cohort study. Contraception; 82:207, 2010 |
|
Grimes DA, Stuart GS, Raymond EG: Feticidal digoxin injection before dilation and evacuation abortion: Evidence and ethics. Contraception 85:140, 2012 |
|
Diedrich J and Drey D: Induction of fetal demise before abortion: Clinical Guidelines. Society of Family Planning. Contraception 81:462, 2010 |
|
Hern WM: Fetal Diagnostic Indications for Second and Third Trimester Outpatient Pregnancy Termination. Prenatal Diagnosis 34: 438, 2014 Online versions at http://onlinelibrary.wiley.com/doi/10.1002/pd.4324/full http://onlinelibrary.wiley.com/doi/10.1002/pd.4324/pdf |
|
Dean G, Colarossi L, Lunde B et al: Safety of digoxin for fetal demise before second-trimester abortion by dilation and evacuation. Contraception 85:144, 2012 |
|
Molaei M, Jones HE, Weiselberg T et al: Effectiveness and safety of digoxin to induce fetal demise prior to second-trimester abortion. Contraception 77:223, 2008 |
|
Drey EA, Thomas LJ, Benowitz NL et al: Safety of intra-amniotic digoxin administration before late second-trimester abortion by dilation and evacuation. Am J Obstet Gynecol 182:1063, 2000 |
|
Jackson RA, Teplin VL, Drey EA et al: Digoxin to facilitate late second-trimester abortion: a randomized, masked, placebo-controlled trial. Obstet Gynecol 97:471, 2001 |
|
Shakya B, Chaudhary P, Tumbajamghe M et al: Intra-amniotic digoxin for fetal anomaly in second and early third trimester. NJOG 17:48, 2014 |
|
Borgatta L, Betstadt SJ, Reed A et al: Relationship of intraamniotic digoxin to fetal demise. Contraception 81:328, 2010 |
|
Steward R, Gatter M, Nucatola D: The safety of digoxin as a feticidal agent. Contraception 82:184, 2010 |
|
Denny C, Persad G, Gates E. Offensive defensive medicine: The ethics of digoxin injections in response to the partial birth abortion ban. Contraception 90:304, 2014 |
|
Denny CC, Baron MB, Lederle L et al: Induction of fetal demise before pregnancy termination: practices of family planning providers. Contraception 92:241, 2015 |
|
Tocce K, Sheeder J, Edwards LJ et al: Effectiveness and safety of transvaginal administration of digoxin to induce fetal demise prior to second-trimester abortion. Contraception 84:311, 2011 |
|
Batra P, Sridhar A, Kim C et al: Transabdominal versus transvaginal digoxin administration prior to second-trimester abortion: Interim analysis of a randomized ilot study of patient preference. Contraception 90:301, 2014 |
|
Gariepy AM, Chen BA, Hohmann HL et al: Transvaginal administration of intraamniotic digoxin prior to dilation and evacuation. Contraception 87:76, 2013 |
|
Tocce K, Sheeder JL, Edwards LJ et al: Feasibility, effectiveness and safety of transvaginal digoxin administration prior to dilation and evacuation. Contraception 88:706, 2013 |
|
White K, Nucatola D, Westhoff C: A randomized trial of intra-fetal versus intra-amniotic digoxin prior to second-trimester pregnancy termination. Contraception 88:435, 2013 |
|
Micks E, O’Day D, Naluai-Cecchini T et al: Effects of digoxin and delayed dilation and evacuation of fetal tissue quality: maximizing opportunities for research participation. Contraception 92:367, 2015 |
|
Gariepy A, Chen B, Hohmann H et al: Reluctance to receive optional feticidal digoxin. Contraception 84:313, 2011 |
|
Roth N, Gatter M, Nucatola D: Digoxin-induced fetal death increases surgeon-perceived ease of second-trimester surgical abortion. Contraception 80:201, 2009 |
|
Tocce K, Nielson K, Sheeder J et al: Evaluation of umbilical cord transection to induce fetal demise prior to second-trimester abortion. Contraception 84:311, 2011 |
|
Tocce K, Leach KK, Teal SB: Umbilical cord transection to induce fetal demise prior to second-trimester D & E abortion. Contraception 88A:712, 2013 |
|
Rowlands S, Oloto E: Serious adverse effects of umbilical cord transection to induce fetal demise prior to second-trimester D & E abortion. Contraception 88:472, 2014 |
|
Tocce K, Leach KK, Teal SB: Umbilical cord transection to induce fetal demise prior to second-trimester D & E abortion: in reply. Contraception 89:473, 2014 |
|
Barrera G, Blum J, Cherine M et al: Understanding postpartum hemorrhage: Its frequency and treatment. Int J Gynecol Obstet 107S2 S1-S92: S24, 2009 |
|
Green J, Borgatta L, Sia M et al: Intervention rates for placental removal following induction abortion with misoprostol. Contraception 76:310, 2007 |
|
Rosenstein MG, Vargas JE, Drey E et al: Ultrasound-guided instrumental removal of the retained placenta after vaginal delivery. Am J Obstet Gynecol 211:180.e1-180.e3, 2014 |
|
Test E, Pearlson G, Drey E et al: Estimated versus quantitative blood loss during dilation and evacuation. Contraception 92:367, 2015 |
|
Hern WM, Corrigan B: What about us? Staff reactions to D & E. Adv Plann Parent 15:3, 1980 |
|
Goldberg AB: When pregnancy must end in the second trimester. Obstet Gynecol 123:1153, 2014 |
|
Hume H, Chasen S: Trends in timing of prenatal diagnosis and abortion for fetal chromosomal abnormalities. AJOG S388 poster Session V, 2015 |
|
Janiak E, Goldberg AB: Eliminating the phrase “elective abortion”: why language matters. Contraception 93: 89, 2016 |
|
Grimes DA, Stuart G: Abortion jabberwocky: the need for better terminology. Contraception 81:93, 2010 |
|
Hern WM: Selective termination for fetal anomaly/genetic disorder in twin pregnancy at 32+ menstrual weeks. Fetal Diagnosis and Therapy 19: 292, 2004 |
|
Bryant AG, Grimes DA, Garrett JN et al: Second-trimester abortion for fetal anomalies or fetal death: Labor induction compared with dilation and evacuation. Obstet Gynecol 117:788, 2011 |
|
Zane S, Creanga AA, Berg CJ et al: Abortion-related mortality in the United States: 1998-2010. Obstet Gynecol 126:258, 2015 |
|
Creanga AA, Berg CJ, Syverson C et al: Pregnancy-related mortality in the United States, 2006-2010. Obstet Gynecol 125:5, 2015 |
|
Edlow AG, Hou MY, Maurer R et al: Uterine evacuation for second-trimester fetal death and maternal morbidity. Obstet Gynecol 117(2 pt 1):307, 2011 |
|
Mendez-Figueroa H, Chauhan S, Sibai B: Significance of the absence of amniotic fluid from the cervical os with preterm premature rupture of membranes. AJOG Poster Session III AJOG January S223, 2015 |
|
Mark AG, Edelman A, Borgatta L: Second-trimester postabortion care for ruptured membranes, fetal demise, and incomplete abortion. Int J Gynecol Obstet 129:98, 2015 |
|
Duvekot J, Bax C, Bloemenkamp K et al: Temporizing management versus termination of pregnancy in women with severe pre-eclampsia at 28-34 weeks (TOTEM-Trial). AJOG Supplement S246 Poster Session III, 2015 |
|
Little S, Bartz D, Janiak E et al: Second trimester dilation and evacuation: a risk factor for preterm birth? AJOG; January S223, Poster session III, 2015 |
|
Wou K, Gotha L, Harding L et al: Obstetrical outcomes following induction of labor with misoprostol for the purpose of termination of pregnancy: a five-year retrospective study. AJOG; S326 Poster session IV, 2016 |
|
Jackson JE, Grobman WA, Henry E et al: Mid-trimester dilation and evacuation does not increase the risk for severe subsequent pregnancy complications. Int J Gynecol Obstet 96:12, 2007 |