Prenatal Development: Growth, Differentiation, and Their Disturbances
Authors
INTRODUCTION
Life is a phenomenon based on the strictly regulated alternation of selective and nonselective transcription of DNA and RNA. Selective transcriptions are coupled with proteosynthesis, nonselective with cell division.
Growth means increase in size due to an increase of existing structural (and functional) units.
Differentiation is a process whereby a relatively simple system is changed into a more complicated one. Differentiation is accomplished by formation of new structures (morphologic differentiation) and by formation of new chemical compounds (chemical differentiation).
Development is (related to biological systems) a process resulting from a selective, time-related switching on and off of genes.
Cell is the basic unit of life. The cell is a system of membranes, filaments and large molecules which prevent dissolved substances from mixing freely. There is no life without cells.
In different biological systems, growth and differentiation are closely related. In human biology, it is necessary to specify growth and differentiation of cells, tissues, and organs, the end result being growth and differentiation of human beings.
NORMAL PRENATAL GROWTH AND DIFFERENTIATION
Biological growth is accomplished by a preponderance of anabolic processes during which the size of the living system increases using already operating genes. Differentiation is related to the switching on of genes that were not operating previously. Organs increase in size via cellular hypertrophy and hyperplasia. Hypertrophy means an excessive increase in size; hyperplasia means an increase in the number of cells. A decrease in the size of a cell of an organ is known as atrophy.
During embryonal and fetal development, the fertilized oocyte changes into a complete organism representing the species by which the oocyte was produced. Differentiation and growth are genetically determined. All cells of an individual (under normal conditions) comprise the same set of basic genes. Gene expression in different cells is regulated by specific stimulatory and inhibitory peptides and proteins. The developmental regulatory mechanisms of gene expression are largely unknown.
The basic mechanisms of growth are (1) an increase in cell size and number, and (2) an increase in extracellular substances. Cell number is increased mainly via mitotic divisions. Cells that undergo mitotic divisions may be classified as life-long proliferating: they divide mitotically for the whole life span of the individual, and they divide in tissue cultures. In contrast, cells that undergo terminal differentiation divide only during a certain period of life of an individual. When terminal differentiation is complete, these cells do not divide, and they do not proliferate in tissue cultures.
The development of an individual is accomplished by a selective switching on and off of genes. The life span of every placental animal can be divided into two periods: prenatal and postnatal. The prenatal period begins with fertilization of the oocyte and ends with delivery. In humans, during the prenatal period, the age of the conceptus is calculated in one of the following ways:
Gestational age, calculated from the first day of the last menstrual period and used for clinical purposes.
“True” age (anatomic age), calculated from the date of supposed or known (e.g., in vitro) fertilization and used for anatomic purposes.
As, under normal conditions, the fertilization occurs around day 14 of a 28-day menstrual cycle, the gestational age of a normal full-term newborn is 40 weeks, whereas the anatomic age is 38 weeks.
Trimesters of Gestation
First trimester: Embryonal period 10 weeks
Fetal period 11–16 weeks
Second trimester: 17–28 weeks
Third trimester: 29–40 ± 2 weeks
The human prenatal period is divided into following periods:
- Pre-embryonal period includes fertilization, cleavage of oocyte, and formation of blastocyst. The pre-embryonal period ends at implantation, which occurs on day 7 postconception. During the pre-embryonal period, the conceptus is transported from the ovary, through the oviduct, into the uterine cavity.
- Embryonal period begins with blastogenesis (i.e., formation of germ layers).
- Blastogenesis includes bilaminar and trilaminar presomite stages of embryonal development, which are present from day 7 to day 20 postconception.
- Embryonal organogenesis (arbitrary) begins with formation of first somites (on day 19 or 20 postfertilization) and ends with the fusion of the eyelids, which occurs between days 56 and 60 postconception. During embryonal organogenesis (weeks 4–8 postconception), primordia of all organs are formed, and the embryo attains a specific human form. For an organism undergoing blastogenesis and organogenesis, the term embryo is used.
- Blastogenesis includes bilaminar and trilaminar presomite stages of embryonal development, which are present from day 7 to day 20 postconception.
- Fetal period. Starting with postconceptional week 9, or gestational week 11, the term fetus is used. The fetus is characterized by fused eyelids and distinct human somatic characteristics. The fetal period covers gestational weeks 11 to 26. During the fetal period, the total body weight (TBW) increases from approximately 5 to 500 g. Fetal period precedes embryonal period, during which a viable fetus is delivered.
At the beginning of the perinatal period, the eyelids separate and the eyes of the fetus reopen.
During the embryonal and fetal period, the fetus may be spontaneously aborted by premature uterine or tubal activity, or aborted by various medical procedures. The fetus is classified as aborted if its TBW is less than 500 g, and if at abortion it does not exhibit any vital signs, such as a beating heart and breathing. If the fetus with a TBW greater than 250 g has a heart beat and/or breath movements, the fetus is classified as an extremely immature newborn. The newborn is delivered (not aborted).
Newborns are classified according to their TBW into four groups:
Group I: Extremely immature, with a TBW less than 500 g
Group II: Immature, with a very low birth weight
Group IIa: 500 to 800 g
Group IIb: 801 to 1000 g
Group III: A. TBW 1001 to 1500 g (immature)
B. TBW 1501 to 2500 g (premature)
C. TBW 2501 to 4000 g (full-term, normal; gestational age 38–42 weeks)
D. TBW 4001 g or heavier (macrosomic)
Group IV: Weight unknown
If the gestational age exceeds 42 gestational weeks, the newborn is called postmature. The newborn is small for gestational age, or intrauterine growth retarded (IUGR), if his TBW is less than minus two percentiles, related to the gestational age and standards of normal fetal growth.1 Neonatal mortality, birth weight, and gestational age are closely related.2
THE STAGING OF EMBRYONAL DEVELOPMENT
Streeter3 divided the human embryonal period into 23 developmental horizons, and his classification is the basis of the Carnegie staging system of human prenatal development.4
The Streeter term “horizon” was replaced in the newer classifications by the old term “stage” (used first by Mall5 in 1914). Each stage is characterized by defined external and internal features. Hamburger and Hamilton6 distinguished 46 stages in the chick. Staging of the development of Rana pipiens was published by Pollister7 and Moore in 1937. Table of “normal” development of a large number of animals published by Keibel and co-workers8 are almost forgotten. Jirásek9, 10 introduced the system of 10 standard comparative stages, where, in different animals, the corresponding prenatal stages were marked by the same system of numbers. Jirásek's comparative classification (J' staging) is based only on external developmental characteristics of quadrupled vertebrate embryos. This classification is simple and suitable for the staging of a large number of animals. The important feature distinguishing between embryonal and fetal period is the fusion of the eyelids (in most species).
The principles of the basic body architecture in all vertebrates is similar, and the presented comparative classification is the most simple for comparing human development with other vertebrates. The Carnegie staging system (originally Streeter's horizons3) and Jirásek's standard J' staging are compared in Table 1.
Table 1. Timetable and staging of human prenatal development
Periods | Anatomic age* (days) from conception | Gestational age† (weeks) of gestation | Length (mm) | External characteristics | Jin stage |
Preembryonal | 0–2 |
| 0.2 | Unicellular (fertilized oocyte) | 1 |
| 2–4 | 2–3 | 0.2 | Blastomeric (16–20 blastomeres, morula) | 2 |
| 4–7 |
| 0.4 | Blastodermic (blastocyst) | 3 |
Embryonal | Bilaminar embryo stage (round-shaped embryonic disc) | 4 | |||
Blastogenesis | (MLL) | ||||
7–15 |
| 0.1 | Bilaminar plate | 4–1 | |
| 4 |
| Primary yolk sac | 4–2 | |
| 0.2–0.4 | Secondary yolk sac | 4–3 | ||
Trilaminar embryo stage (pear-shaped embryonic disc) | 5 | ||||
15–17 | 0.4–1.0 | With primitive streak and notochordal process | 5–1 | ||
17–20 | 1.0–2.0 | With neural folds | 5–2 | ||
5 | Early somite stage (shoe-sole-shaped embryo) | 6 | |||
Organogenesis | 20–21 | 1.5–2.0 | Completely open neural groove | 6–1 | |
21–26 | 6 | 1.5–4.0 | Neural tube closing, both ends open | 6–2 | |
26–30 | 3–5 | One or both neuropores closed | 6–3 | ||
Stage of limb development (C-shaped embryo) | 7 | ||||
28–32 | 4–6 | Bud of proximal extremity | 7–1 | ||
31–35 | 7 | 5–8 | Buds of proximal and distal extremities | 7–2 | |
35–38 | 7–10 | Proximal extremity, two segments | 7–3 | ||
37–42 | 8–12 | Proximal and distal extremities, two segments | 7–4 | ||
42–44 | 10–14 | Digital rays, foot plates | 7–5 | ||
44–51 | 13–21 | Digital tubercles | 7–6 | ||
51–53 | 19–24 (CRL) | Digits, toe tubercles | 7–7 | ||
Late embryonal stage (embryo with differentiated extremities including fingers and toes) | 8 | ||||
52–56 | 8 | 22–25 | Eyes open | 8–1 | |
| 56–60 | 10 | 27–35 | Fusing eyelids | 8–2 |
Fetal | 60–182+ | 11–26 | 31–200 | Fetus with fused eyelids | 9 |
Perinatal | 170–266+ | 27–40 | 201–350 400–550 (CHL) | Third trimester fetus (newborn with open eyes) | 10 |
*Age from conception; †Age from 1st day of the last menstrual period
MLL, maximal longitudinal length
CRL, crown–rump length
CHL, crown-heel length
CHARACTERISTICS OF STANDARD PRENATAL VERTEBRATE STAGES
Prenatal development comprises the following 10 principal stages:
Stage 1: Unicellular stage of fertilization. This begins with fusion of cell membranes of the oocyte and sperm, ends with division of the oocyte into two blastomeres
Substage 1–2: Formation of male and female pronucleus and DNA synthesis
Substage 1–3: DNA synthesis within pronuclei
Substage 1–4: First mitosis, which results in formation of two first blastomeres
Stage 2: Cleavage of oocyte into blastomeres. This is the blastomeric (morula) stage.
Substage 2–1: Formation of first eight blastomeres (all of them are “external”)
Substage 2–2: Formation of morula with external and internal blastomeres
Stage 3: Blastocyst (in placental vertebrates) or blastula (in aplacental vertebrates) stage. The blastocyst (or blastula) is characterized by the presence of (1) a fluid-filled trophoblastic compartment (blastocoele) separated from the environment; and (2) “indifferent” embryonal stem cells contributing inner cell mass (embryoblast) to the blastocyst, or the blastoderm in vertebrates with a blastula stage. In mammals, the blastocyst is composed of trophoblast (trophoectoderm) and inner cell mass (embryoblast). The trophoblast contributes only the lining of the chorionic villi. All other components of the embryo—amnionic sac, yolk sac, embryonic disc of the future embryo—originate from the inner cell mass.
Stage 4: Bilaminar embryo is formed by ectoblast and endoblast (gastrula stage).
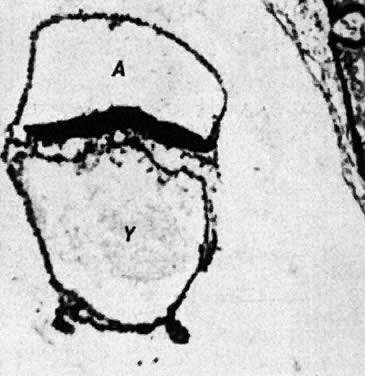
Substage 4–1: In humans, the embryo forms a bilaminar circular disc composed of ectoblast and endoblast located between the amnionic sac and the primary yolk sac.
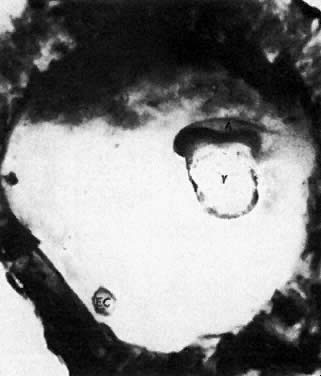
Substage 4–2: The disc is located between the amnionic sac and the secondary yolk sac.
Stage 5: Trilaminar embryo with axial structures is formed.
Substage 5–1: Primitive node
Substage 5–2: Primitive node, elongated notochordal process
Substage 5–3: Proliferative mesoblast
Stage 6: Embryos at this stage are characterized by differentiation of somites and closing neural tube (late notogenesis).
Substage 6–1: The neural groove is completely open
Substage 6–2: The neural tube exhibits both open ends (anterior and posterior neuropores, the heqart beat starts)
Substage 6–3: Anterior or both anterior and posterior neuropores are closed. No definitive limb buds are present. In humans, the anterior neuroporus closes at approximately day 26, the posterior one at day 28 postconception. (The embryonal blood circulation begins at this stage.)
Stage 7: Embryos at this stage exhibit morphogenesis of limbs (and face).
Substage 7–1: Bud of proximal extremity
Substage 7–2: Buds of proximal and distal extremities
Substage 7–3: Proximal extremity bisegmented, distal extremity remaining as an unsegmented bud
Substage 7–4: Proximal and distal extremities with two segments
Substage 7–5: Digital rays emanating from the proximal extremity
Substage 7–6: Digital tubercles, but toe rays, no tubercles
Stage 8: Late embryonal stage is characterized by distinct fingers and toes in mammals, eyes are open; eyelids develop (late embryonal stage). Fusing of eyelids is characteristic of the end of the embryonic period.
Substage 8–1: Digits and toe tubercles
Substage 8–2: Digits and toes, closed primary palate
Stage 9: Fetal stage. In mammals, the fetus has a characteristic species-specific external appearance; the eyelids are fused.
Stage 10: Perinatal stage. During this stage, the eyes reopen.
SCOPE OF HUMAN PRENATAL DEVELOPMENT
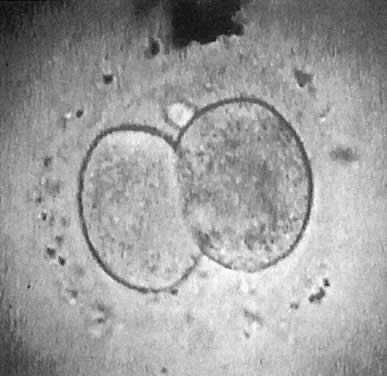
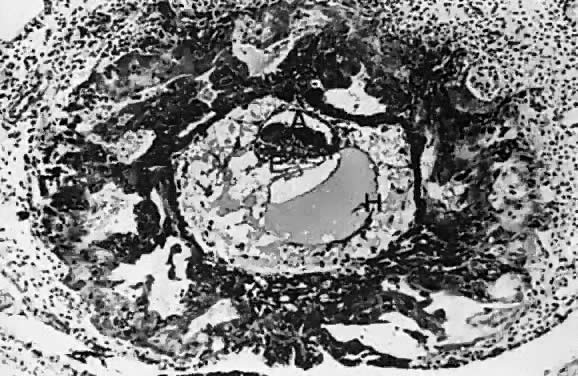
At fertilization, the oocyte is round, approximately 150 μm in diameter, and enclosed by zona pellucida. Zona pellucida is approximately 10 μm thick, composed of glycoproteins contributed by the oocyte during its growth, which occurs at the beginning of follicular growth.11, 12 The cleavage of the oocyte and the formation of the early blastocyst take place in the space limited by the zona pellucida. During the pre-embryonal stage (days 1–4) the conceptus is transported by the oviduct into the uterine cavity. During days 5 to 6, the blastocyst increases in size, and the zona pellucida ruptures and is rejected (hatching of oocyte). The diameter of the “free blastocyst” is approximately 200 μm. On day 7, the blastocyst implants into the edematous, compact (superficial) layer of the undecidualized functional layer of endometrium.13 The bilaminar embryonal disc, aged 7–14 days, is round and 0.2–0.7 mm in diameter. During blastogenesis, the term ectoblast, endoblast, and mesoblast may be used. Beginning with organogenesis (somite formation), these terms are replaced by ectoderm, endoderm, and mesoderm.
The trilaminar embryonal disc, aged 14–20 days, is pear-shaped and 0.5–2.5 mm long. Organogenesis begins with the formation of somites.
During stage 6, characterized by formation of somites and closure of the neural tube, the embryo becomes delineated by anterior, lateral, and posterior amnionic folds. The embryo becomes cylindric and 2–3 mm long. After closure of neural tube, as the primordium of central nervous system grows faster than the other portions of the embryo, the embryo bends ventrally and is C-shaped. At stage 7, the head, neck, trunk, and limbs become evident. The primary palate closes (substage 7–6), and human features are conclusive.
At the end of the embryonal period, the eyelids grow and their rims finally fuse, closing the eye fissure (days 56–60 postconception).
During the fetal period (gestational weeks 10–26, stage 9), the eyes of the fetus are closed. At the early human fetal period (gestational weeks 11–12), male and female differentiation of external genitalia occurs. The fetal weight increases from approximately 5 to 50 g. During the human midfetal period, the TBW increases from 51 g to approximately 250–300 g. During the late fetal period, the fetus weighs more than 300 g and less than 500 g (if live born), or less than 1000 g if aborted dead. Fetal increase in the weight of brain, lung, kidney, adrenal, thyroid, and placenta14 is presented in Table 2. Clinically, embryonal and fetal growth can be followed with great accuracy using ultrasound anthropometry.15, 16, 17
Table 2. Length and weight of the fetus and weight of some fetal organs in relation to gestational age
Organ weight (g) | |||||||
Gestational | TBW (g) | CRL (mm) | CHL (mm) | Adrenals | Brain | Heart | Kidneys |
16 | 117 | ||||||
| 120 | 175 | 0.86±0.08 | 30.7±5.6 | 1.38±0.57 | 1.72±0.57 | |
| 200* | ||||||
20 | 325 | 175 | 240 | 2.5 | 45–50 | 4.0 | |
24 | 500* | 1.96±1.2 | 71.0±15 | 3.60±1.5 | 4.42±1.65 | ||
| 640 | 215 | 295 | 3.2±3.8 | 112±36 | 9.0±4.0 | |
| 800* | 2.8±2.0 | 112.2±13.5 | 5.75±2.35 | 7.75±2.67 | ||
28 | 1000* | 3.32±2.5 | 139.2±29.0 | 7.19±3.0 | 10.1±3.4 | ||
| 1150 | 250 | 350 | 3.9–4.1 | 169±50 | 13±5 | |
32 | 1810 | 280 | 400 | 4.8–4.9 | 283±50 | 17±5 | |
36 | 2650 | 320 | 450 | 6.2–6.9 | 354±70 | 22±5 | |
40 | 3200 | 360 | 500 | 8.0–8.5 | 400±70 | 30±9 | |
*According to Shepard et al.14
TBW, total body weight; CRL, crown-rump length; CHL, crown-heel length.
Application of the same criteria for staging prenatal development of human, macaque monkey, rat, and mouse, which are commonly used in teratogenic experiments and drug testing, is given in Table 3. Human embryos at different developmental stages are depicted in Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, and Figure 16.
Table 3. Human prenatal development: comparison with experimental animals
Comparative stages (Jirásek J' stage) | Human | Macaques | Rat | ||||
Characteristic | Stage | Length | Age | Length | Age | Length | Age |
Unicellular | 1 | 0.2 | 0–2 | 0.15 | 1 | 1 | |
Blastomeric (16–20 blastomeres) | 2 | 0.2 | 2–4 | 0.15 | 2–4 | 2–3 | |
Blastodermic | 3 | 0.4 | 4–6 | 0.2–0.3 | 7–9 | 4–5 | |
Bilaminar embryo stage | |||||||
Bilaminar plate | 4–1 | 0.1 | 6–14 | 0.3 | 10–13 | 6–7 | |
Primary yolk sac | 4–2 | ||||||
Secondary yolk sac | 4–3 | 0.2–0.4 | |||||
Trilaminar embryo stage | |||||||
With primitive streak | 5–1 | 0.4–1.0 | 15–17 | 0.5 | 17–19 | 8–9 | |
With notochordal process | 5–2 | 1.0–2.0 | 17–20 | 1.5 | |||
Early somite stage | |||||||
Completely open neural groove | 6–1 | 1.5–2.0 | 20–21 | 1.9 | 21–24 | 9½ | |
Neural tube closing, both ends open | 6–2 | 1.5–4.0 | 21–26 | 4.0 | 24 | 1.3–3.0 | 10–10¾ |
One or both neurospores closed | 6–3 | 3–5 | 26–30 | 4.0–6.0 | 24–26 | 3–4.1 | 11 |
Stage of limb development | |||||||
Bud of proximal extremity | 7–1 | 4–6 | 28–32 | 6.0 | 26 | 4–4.5 | 11 |
Buds of proximal and | 7–2 | 5–8 | 31–35 | 8.0 | 27 | 4–6 | 11.5 |
Proximal extremity two segments | 7–3 | 7–10 | 35–38 | 5.8–8 | 13 | ||
Proximal and distal extremity two | 7–4 | 8–12 | 37–42 | 7–9 | 8–9.5 | 13½ | |
Digital rays, foot plates | 7–5 | 10–14 | 42–44 | 10 | 34 | 10 | 14 |
Digital tubercles | 7–6 | 13–21 | 44–51 | 9–11 | 36 | 12.5 | 15½ |
Digits, toe tubercles | 7–7 | 19–24 | 51–53 | 19 | 41 | 16 | 17 |
Late embryonal stage | |||||||
Differentiated extremities | 8–1 | 22–23 | 52–56 | 22 | 44 | 19 | 17½ |
Fusing eyelids | 8–2 | 27–35 | 56–60 | 39–44 | 52 | 22 | 19½ |
Fetal period | 9 | 31–200 | 60–182+ | 40–260 | 53–170 | 25 | 19–21 |
Perinatal period | 10 | 201–450 | 180–266+ | postnatal | postnatal | ||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
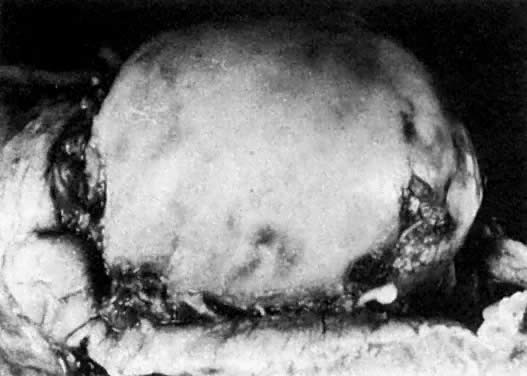
Prenatal development is influenced by various external factors. The prenatal sensitivity of an individual to external factors, including xenobiotics, varies according to the stage of development. Generally, if the mammalian embryo is exposed to damaging agents during blastogenesis (corresponding to human gestational weeks 3–4), either the embryo is killed and subsequently aborted, or it survives without any anatomic defects. If the embryo is exposed to nociceptive influences during the organogenic period (corresponding to human gestational weeks 5–10), the probability of anatomic malformations is high. Mechanical injuries causing amnionic ruptures and bleeding into the amnionic cavity, especially during gestational weeks 8–12, may produce limb amputations and facial disruptions related to blood clotting and, consequently, fibrin cords and deposits on the surface of the embryo or fetus (Fig. 17). The affected embryo usually survives and is not aborted, but it is malformed. During the fetal and perinatal periods, the probability of anatomic malformations decreases; however, damage to the brain and the sense organs (ears, eyes) can never be ruled out. Fetal death followed by abortion can occur at any stage of prenatal development. In humans, serious brain damage during the perinatal period becomes manifested relatively late postnatally as psychomotoric and mental retardation.
{kind=link}
The intrauterine survival of the conceptus depends mostly on uteroplacental and fetoplacental circulations. Fetal brain and kidneys are unimportant for intrauterine survival: fetuses with anencephaly or agenesis of both kidneys may develop till term. The early extrauterine survival of the newborn depends on respiratory and circulatory adaptations and on neurovegetative integrations. Obstruction of the intestinal passage and urination are tolerated in newborns for a period of 2–3 postnatal days.
FACTORS AFFECTING FETAL GROWTH AND DIFFERENTIATION
Fetal growth and differentiation may be modified by internal and external factors.
Ill-Defined Biological Factors
Growth retardation is more frequent in smoking mothers. Full-term newborns of smoking mothers are approximately 200 g lighter than newborns of nonsmokers.18 Regarding smokers and nonsmokers there are, however, also differences in socioeconomic status and other factors, such as maternal alcohol drinking and drug intake.
Regarding maternal height, weight, nutrition, and parity, there is a good correlation between the maternal weight and the placental and fetal size.19 Although the weights of newborns in the same sibship are highly correlated, the second infant tends to weigh more than the first. If the diet during the last trimester of pregnancy is inadequate, the fetal birth weight, length, and head circumference will be smaller. If the caloric intake is less than 400 cal/day, the gestational period will be shortened.20 In multiple gestations, the weight of newborns is usually decreased. In relation to the placental weight, twins are lighter than singletons. Placental size (active surface) seems to be a determinant of fetal growth. Growth-retarded fetuses tend to be heavier in relation to the weight of the placenta (i.e., have a higher fetal to placental weight ratio than normal fetuses).21, 22
Genes
The most important internal developmental factors are genes. Genes are classified as structural and regulatory. There are three types of structural genes: (1) house-keeping, related to the cellular life and cell cycle; (2) cell-typing, coding organ-specific characteristics of cells; and (3) cell-specific, coding specific secretory products of cells (e.g., hormones). Regulatory genes bind to DNA and regulate sequences of expression of other (structural) genes.
Many regulatory genes contain an approximately 180-nucleotide-long sequence known as the homeobox. The homeoboxes are shared by genes of very different animals, such as flies (Drosophila), chicks, mice, and humans. Homeobox genes code for the basic organization of the embryonal body.23, 24
Substances participating in growth and differentiation are gene products. These products have the following types of action:
Autocrine action: Substances act in the cells of their origin.
Paracrine action: Substances diffuse (spread) in the neighborhood of the cell (or tissue) of their origin. Some paracrine actions are correlated to embryonal inductions.
Endocrine actions: Substances are released from the cell of their origin into the blood stream.
Substances of Basic Developmental Significance
TRANSMEMBRANE MOLECULES.
During development, temporary cellular adhesions and transmembrane transports are related to “transmembrane” molecules, including integrins, syndecans, and cadherins. Integrins and syndecans are transmembrane proteoglycans.25, 26 The extracellularly oriented domain ends with a hydrophobic sequence with an amino group. The intracellular domain ends with a hydrophilic carboxy group. Integrins bind with extracellular matrix; the ligands for integrin alfa 3, beta 1 bind with collagen, laminin, and fibronectin. Syndecans bind to heparan sulfate, chondroitin sulfate, fibrin collagens, fibronectin, and tenascin. If the extracellular domain of syndecans is attached to the surface of an adjacent cell, the intracellular domain binds to the cytoskeleton. Syndecans participate in cellular polarization of epithelial cells in the basolateral cellular surface. Syndecans are present in epithelia as well as mesenchymal cells. Cadherins are Ca2+-dependent cell-to-cell adhesion molecules participating in morphogenesis and epithelial differentiation.
GROWTH FACTORS
Growth factors are peptides, or proteins that regulate cellular proliferation and differentiation.27, 28 The most important growth factors fit into the the following families:
- Insulin family: insulin and insulin-like growth factors (IGF-I, IGF-II, relaxin, nerve growth factor, human placenta lactogen [hPL]). Prenatally, insulin is the main factor regulating fetal growth
- Transforming growth factor family: TGF-β1 müllerian inhibiting substance (MIS), inhibins A and B, activins
- Platelet-derived growth factor family
- Epidermal growth factor family
- Heparin-binding growth factor family: acid fibroblast growth factors and basic fibroblast growth factors
Growth factors first bind to their specific cellular receptors. The interaction of growth factor and receptor induces a specific gene expression (within minutes), followed by initiation of DNA and/or RNA synthesis.
Next, growth factors trigger intracellular messengers, including phosphoproteins (phospholipase C, phosphatidyl inositol). Some growth factors exhibit a protein tyrosinase and protein kinase C activity. Cytokines (e.g., lymphokines, interleukins, tumor necrosis factor, fibronectin) are important factors of programmed cell death (apoptosis), endothelial proliferation, and specific cell differentiation.
ENERGY FOR DEVELOPMENT
Development depends on energy. The bulk of the energy required for growth and differentiation is produced by mitochondria. The mitochondria contain their own mitochondrial genome. All mitochondria in an individual are maternally derived. Disturbances of the mitochondrial genome are maternally inherited.29 Glycolysis is the principal pathway by which high-energy phosphates are formed, and CO2 and water are byproducts. Using anaerobic glycolysis, 2 mol of adenosine triphosphate (ATP) are produced from 1 mol of glucose; in contrast, by much more effective aerobic glycolysis, 36 mol of ATP are formed from 1 mol of glucose. Mammalian prenatal development occurs under hypoxic conditions in an environment that is well balanced for pH and temperature.
DISTURBANCES OF FETAL GROWTH AND DIFFERENTIATION
The pathogenic classification of congenital disorders of growth and differentiation is as follows:
- Disorders of the nuclear genome (errors of nuclear DNA and chromosomes):
- Chromosomal disorders (disorders of number and shape of chromosomes)
- Monogenic disorders (with mendelian inheritance: autosomal-dominant, autosomal-recessive, X-linked, or Y-linked)
- Chromosomal disorders (disorders of number and shape of chromosomes)
- Disorders of the mitochondrial genome (maternally inherited)
- Multifactorial sporadic disorders related to teratogen and sporadic anomalies and malformations of unknown etiology.
Teratogens are classified as biological, chemical, and physical:
- Biological teratogens are maternal diseases, such as diabetes and some infections.
- Chemical teratogens are toxic chemicals, including some medicaments.
- Physical teratogens are high temperature, ionizing radiation (x-rays), and mechanical injuries.
The most frequent chromosomal disorders are trisomy of chromosome 21 (Down's syndrome), trisomy of chromosome 13 (Patau's syndrome), and trisomy of chromosome 18 (Edward's syndrome).30 Trisomies of other autosomes are lethal and are aborted usually during the first trimester of pregnancy. The most common trisomy occurring in spontaneous abortions is trisomy of chromosome 16. The second most frequent aneuploidy in spontaneous abortions is monosomy X (karyotype 45,X). Such affected individuals exhibit Turner's syndrome and are usually aborted (more than 90% of the time). Other viable trisomies of sex chromosomes are 47,XXY (Klinefelter's syndrome), 47,XYY syndrome, and 47,XXX syndrome. Fetuses with triploidy (69 chromosomes, XXX, or XXY, or XYY) have severe IUGR, multiple anomalies, and malformation, and are usually aborted dead.
Monogenic defects include metabolic as well as dysmorphic disorders. Some are characterized by specific metabolic and morphologic sequences related to storage of excessive metabolites. Combinations of more or less constant anomalies and malformations are classified as syndromes or sequences. The number of monogenic syndromes (all exhibiting mendelian inheritance) that exhibit disturbances of growth and differentiation exceeds several thousand.31
Diseases related to errors of the mitochondrial genome are characterized by myopathies, cardiomyopathies, retinopathy, and encephalopathy. The defects are related to the metabolism of ATP. The defects include substrate transport (carnitine), energy conservation (ATP), and cytochrome deficiencies.32 Mitochondrial disorders are maternally inherited.29
Multifactorial anomalies and malformations are sporadic, affected by hereditary background (predisposition).
Biological Teratogens
DIABETES MELLITUS.
There is a definitive increase in malformation among offspring of diabetic mothers. There are two groups of anomalies related to maternal diabetes: malformation and fetopathy. The increased frequency of malformations can be correlated with inadequate treatment of diabetes during the first trimester of pregnancy. The most common malformations are “caudal regressions,” such as sacral and femoral agenesis and neural tube defects.33, 34 An increased abortion rate was not documented.35
In fetuses of diabetic mothers with inadequately treated hyperglycemia during the third trimester, the characteristic feature is diabetes fetopathy. Such fetuses are supplied with excessive glucose. Glucose diffuses across the placental barrier and triggers insulin synthesis and release from the fetal pancreatic β-cells. Excessive fetal glucose utilization due to an excessive maternal glucose supply increases the growth of the placenta and fetus. In fetuses of diabetic mothers exhibiting excessive growth, there is accumulation of fat and visceromegaly of the heart and liver. The amount of body water, which is approximately 78% of TBW in normal newborn, is decreased to approximately 70%.32, 36
INFECTIONS IN GESTATION.
Early in gestation, every infection that occurs during the organogenic period (gestational weeks 5 to 10), can be teratogenic without the infectious agent being passed to the embryo, if the mother's body temperature exceeds 39°C.37, 38
The most dangerous infections known to pass from the mother to the fetus and to produce malformations are toxoplasmosis,39 rubella,40 cytomegalovirus,41 and herpesvirus42 (TORCH); syphilis; and varicella.43
Chemical Teratogens
The potential consequences of intake of teratogenic substances are IUGR, fetal malformations, fetal demise, and spontaneous abortion. The action of a teratogen is related to the developmental period of the embryo or fetus at the time of its intake by the mother. The following are recognized human teratogens:
Aminoglycosides (gentamicin)
Androgenic steroids
Coumarin anticoagulants
Cytostatics such as chlorambucil, aminopterin, and methotrexate (folate antagonists)
Diethylstilbestrol*
Ethyl alcohol
Lithium
Methimazol
Organic mercurials
Polychlorinated biphenyls (PCBs)
Streptomycin
Thalidomide
Toluene
Trimethadione-related anticonvulsant agents (hydantoins)
Valproic acid
Vitamin A congeners*Diethylstilbestrol is the only known tranplacental carcinogen
For the spectrum of malformations related to a known teratogen, the term disruption is applied.
Physical Teratogens
Physical teratogens are hyperthermia, ionizing radiation (x-rays), and mechanical injuries.
Hyperthermia,43 or a temperature greater than 39°C, occurring during gestational weeks 4–8 is associated with neural tube defects, microcephaly, and microphthalmia.37
Ionizing radiation has serious adverse developmental effects related to the period of gestation at exposure.44 The period in human development most sensitive to this teratogen is 18–36 days postconception. The most frequent malformations are microcephaly and neural tube defects. The minimal dose is estimated to be 20 cGy (approximately 20 rads, or 20 rem). The long-term effects of irradiation are leukemia and other malignancies.
Mechanical injuries to the fetus are usually caused by car accidents; some may be associated with chorionic villus sampling, early amniocentesis, or gynecologic surgeries in pregnancy. The consequence of mechanical injuries may be intra-amnionic bleeding and/or disruption of the amnion (without rupture of chorion), oligohydramnion, detachment of the placenta followed by a retroplacental hematoma, and uterine bleeding. Abortion occurs in most cases of serious accidents. Oligohydramnion is associated with the oligohydramnion sequence: deformities of the face and limbs, pulmonary hypoplasia, and breach presentation at birth.45 (Most cases of oligohydramnion are related to renal agenesis and/or urethral obstructions; such cases are not of mechanical origin.) Uterine anomalies are a relatively frequent cause of fetal deformities, manifested by auricular and craniofacial deformations, torticollis, and deformations of limbs.46
LOCAL GROWTH DISTURBANCES
Local disturbances of growth and development are classified as anomalies, deformities, dysplasias and malformations. Anomalies are quantitative or positional deviations from “normal,” such as IUGR, low-set ears, hypertelorism, hypotelorism, excessive weight, cryptorchidism, arched palate, low hair line, and hypoplasia of nails. Deformities are changes in form related to mechanical pressure. Dysplasias and dysgenic changes are related to disturbed histogenesis of affected organs. Malformations are developmental changes presenting structures that are not present in “normal” individuals. Minor malformations are compatible with life; however, major malformations if left untreated endanger the survival of the affected newborn. Examples of minor malformations are lip pit, extra digits, extra toes, and mild hypospadias. Examples of major malformations are anencephaly and other neural tube defects, orofacial clefts, amputations of limbs, and phocomelia.
Local congenital growth disturbances, asymmetries, and enlargements are related to edema, cellular proliferation, vascular anomalies including angiomas and arteriovenous aneurysms, and defects in innervation. Congenital asymmetric atrophy may result from vascular and nervous insults.
Many fetuses exhibiting abnormalities of growth and differentiation can be recognized clinically by methods of prenatal diagnosis. The following are the most valuable methods:
Ultrasound examination, which allows accurate anthropometric measurements, including a check-up of skeletal and basic morphologic development
Chromosomal analysis of the conceptus (karyotyping) using cells from chorionic villi (gained by chorionic villous sampling), or cells from amnionic fluid (gained by amniocentesis)
Genetic analysis using isolated DNA from chorionic villi (obtained by chorionic villous sampling), other fetal tissues, or fetal blood
In special cases of fetal disorders, ultrasound-guided biopsy specimens of fetal tissue (e.g., skin, liver, muscles) and blood.
Analysis of fetal DNA in maternal blood represents a basic line of enquiry for prenatal diagnostis in the future.
Prenatal diagnosis of congenital disorders is a fast-growing field with a fascinating future and consequences.
REFERENCES
Brenner WE, Edelman DA, Hendricks CH et al: A standard of fetal growth for the United States of America. Am J Obstet Gynecol 126: 555, 1976 |
|
Lubchenko LO, Dearls DT, Brazie JV: Neonatal mortality rate: Relationship to birthweight and gestational age. J Pediatr 81: 814, 1972 |
|
Streeter GL: Developmental horizons in human embryos. Contributions to Embryology, Washington, DC, Carnegie Institute, 1951 |
|
O'Rahilly R, Muller F: Developmental stages in human embryos: Including a revision of Streeter's horizons and a survey of the Carnegie collection, p 637. Washington, DC, Carnegie Institute, 1987 |
|
Mall PP: On stages of development of human embryos from 2 to 25 mm long. Anat Anz 46: 78, 1914 |
|
Hamburger V, Hamilton HL: A series of normal stages in the development of the chick embryo. J Morphol 95: 501, 1954 |
|
Pollister AW, Moore JA: Tables for the normal development of Rana sylvatica. Anat Rec 68: 486, 1937 |
|
Keibel F et al: Normentafeln zur Entwicklungsgeschichte der Wirbeltiere I–XIV. Fischer, Jena, 1910-1914 |
|
Jirásek JE: Atlas of human prenatal morphogenesis. The Hague, Martinus Nijhoff, 1983 |
|
Jirásek JE: Prenatal development: Growth and differentiation. In Sciarra JJ (ed): Gynecology and Obstetrics. Philadelphia, Harper and Row, 1982 |
|
Bliel JD, Wasserman PM: Structure and function of the zona pellucida. Dev Biol 76: 185, 1980 |
|
Wasserman PM: Early events in mammalian fertilization. Ann Rev Cell Biol 3: 109, 1987 |
|
Hertig AT, Rock J: Two human ova of the pre-villous stage, having a developmental age of about seven and nine days respectively, Vol 557, p 65. Contributions to Embryology, Washington, DC, Carnegie Institute, 1945 |
|
Shepard T et al: Organs weight standards for human fetuses. Pediatric Pathol 8: 513, 1988 |
|
Brown HL et al: Ultrasonic recognition of the smallfor-gestational age fetus. Obstet Gynecol 69: 631, 1987 |
|
Campbell S, Pearce JM: The prenatal diagnosis of fetal structural anomalies by ultrasound. Clin Obstet Gynecol 10: 475, 1983 |
|
Warsof S et al: The present routine ultrasound screening. Clin Obstet Gynecol 10: 446, 1983 |
|
Crosby WM et al: Fetal malnutrition: An appraisal of correlated factors. Am J Obstet Gynecol 128: 22, 1977 |
|
Thomson AM et al: The assessment of fetal growth. Br J Obstet Gynecol 75: 903, 1968 |
|
Stein Z, Susser M: The Dutch famine 1944-1945, and the reproductive process. Pediatr Res 9: 70, 1975 |
|
Gruenwald P: Growth of the human fetus. Am J Obstet Gynecol 94: 112, 1966 |
|
McKeown T, Record RG: The influence of placental size on foetal growth in man with special reference to multiple pregnancy. J Endocrinol 9: 418, 1953 |
|
Bianchi ME et al: The DNA binding site of HMGI protein is composed of two similar segments (HMG boxes), both of which have counterparts in other eukaryotic regulatory proteins. EMBO J 11: 1055, 1992 |
|
Lewis EB: Clusters of master control genes regulate the development of higher organisms. JAMA 267: 1524, 1992 |
|
Bernfield M, Saunderson RD: Syndecan, a developmentally regulated cell surface proteoglycan that binds extracellular matrix and growth factors. Phil Trans R Soc Lond B 327: 171, 1990 |
|
Ruohslati E: Integrins. J Clin Invest 87: 1, 1991 |
|
DiErcole AJ: Growth factors and development. In Polin RA, Fox WW (eds): Fetal and Neonatal Physiology. Philadelphia, WB Saunders, 1992 |
|
Dinarelo CA, Mier JW: Lymphokines. N Engl J Med 317: 940, 1987 |
|
Wallace DC: Maternal genes: Mitochondrial diseases. Birth Defects Orig Art Ser 23: 137, 1987 |
|
Kalousek DK, Fitch N, Paradice BA: Pathology of the Human Embryo and Previable Fetus. New York, Springer-Verlag, 1990 |
|
McKusick VA: Mendelian Inheritance in Man: Catalogs of Autosomal Dominant, Autosomal Recessive and X-Linked Phenotype, 10th edn. Baltimore, John Hopkins University Press, 1992 |
|
Cole HS: Problems in management of infants of diabetic mothers. In Camerini-Davlos RA, Cole HS (eds): Early Diabetes in Early Life. New York, Academic Press, 1975 |
|
Kucera J: Rate and type of congenital anomalies among offspring of diabetic women. J Reprod Med 7: 61, 1971 |
|
Milunsky A et al: Prenatal diagnosis of neural tube defects: The importance of serum α-fetoprotein in diabetic pregnant women. Am J Obstet Gynecol 142: 1030, 1982 |
|
Kalter H: Diabetes and spontaneous abortion: A historical review. Am J Obstet Gynecol 156: 1243, 1987 |
|
Hill DJ, Milner RDG: Insulin as a growth factor. Pediatr Res 9: 879, 1985 |
|
Layde PM et al: Maternal fever and neural tube defects. Teratology 21: 105, 1980 |
|
Warkany J: Teratogen update: Hyperthermia. Teratology 33: 356, 1986 |
|
Feldman HA: Toxoplasmosis. Med Prog 279: 1371, 1968 |
|
Menser MA, Reye RDK: The pathology of congenital rubella. Pathology 6: 215, 1974 |
|
Hanshaw JB: Developmental abnormalities associated with congenital cytomegalovirus infection. In Woollam (ed): Advances in Teratology, Vol 4, pp 62–63. New York, Academic Press, 1970 |
|
Nahmias AJ et al: Herpes simplex virus infection of the fetus and newborn. Prog Clin Biol Res 3: 63, 1975 |
|
Shepard T, Siwth (ed): Catalog of Teratogenic Agents. Baltimore, John Hopkins University Press, 1989 |
|
Mole RH: Irradiation of the embryo and fetus. Br J Radiol 60: 17, 1987 |
|
Thomas IT, Smith DW: Oligohydramnios, the cause of non-renal features of Potter's syndrome, including pulmonary hypoplasia. J Pediatr 84: 811, 1974 |
|
Dunn PM: Congenital postural deformities. Br Med Bull 32: 71, 1976 |