Cytopathology
Authors
INTRODUCTION
Cytologic examination of the exfoliative material of the cervicovaginal area of the female genital tract has had a tremendous impact in limiting the development of invasive squamous carcinoma of the uterine cervix, therefore reducing the mortality from cervical cancer. In 1943, George Papanicolaou at Cornell University Medical College laboratories initiated a program that would become valuable as a screening test in the United States and around the world.1, 2 At that time, Papanicolaou developed a numeric classification from Class I to Class V, which indicated the absence of atypical or abnormal cells (Class I); atypical cells but no evidence of malignancy (Class II); cells suggestive of, but not conclusive for malignancy (Class III); cells strongly suggestive of malignancy (Class IV); and unquestionable evidence of malignancy (Class V). With the development and refinement of cytologic diagnosis, many believed that the Papanicolaou classification was not adequate because it did not clearly identify the nature of the lesion.3 Several modifications to the original classes were introduced and were used without the uniformity necessary for reporting abnormalities found in the uterine cervix. In 1953, Reagan and colleagues3 introduced the term dysplasia to refer to preneoplastic abnormalities of squamous cells. This classification was further subdivided into mild, moderate, and severe; indicating the variable degrees of severity found within the atypical process. The advantage of this reporting system was the ability to use it for cytologic as well as histologic samples. In 1966, Richart4 introduced the term cervical intraepithelial neoplasia (CIN), which was subdivided into grades I, II, and III, and that could also be used for grading both cytologic and histologic samples.
In 1988, a new classification, The Bethesda System (TBS), was developed by consensus opinion at a workshop held at the National Cancer Institute in Bethesda, Maryland. The goal of TBS was to provide uniformity in the interpretation and reporting of cytologic material obtained from the cervix and vagina, and thus facilitate communication between the laboratory and the clinician. TBS nomenclature requires a statement of adequacy and a descriptive diagnosis. Its nomenclature reflects the current understanding of benign, preneoplastic, and neoplastic processes of the female genital tract, with equivalents in diagnostic histopathologic terminology. In 1991, a second workshop was held to evaluate the impact of TBS in actual practice and to modify it where necessary. One of the major recommendations of this second meeting was that precise criteria be formulated for both the diagnostic terms and the descriptors of specimen adequacy.5 After the successful incorporation of TBS 1991 into practice, more than 90% of US laboratories used some form of TBS in reporting cervicovaginal cytology.6 With the change in practice to increased utilization of new technologies and findings from research studies in subsequent years, the Bethesda 2001 workshop was convened to re-evaluate the TBS. After a preconference Internet bulletin board process of input and a 3-day workshop that included input from pathologists, cytotechnologists, gynecologists, family practitioners, epidemiologists, attorneys, public health physicians, and patient advocates, Bethesda 2001 was developed by a consensus process.7 Since that time, as additional experience with morphology on liquid-based preparations, further insights into HPV biology, and implementation of HPV vaccinations have ensued and as such, updated revisions to published guidelines have been made. The most recent TBS 2014 guidelines for cervical cancer screening, management of abnormal cervical cytology and cancer precursors are presented within this text.8 Smears without epithelial abnormalities, including those reported previously as benign cellular changes and reactive changes are classified as no intraepithelial lesion/malignancy, epithelial neoplastic processes are reported as squamous or glandular, and other non-neoplastic findings including organisms and endometrial cells (women >45 years of age) are reported descriptively (Table 1). TBS 2014 also includes guidelines for reporting ancillary tests, computerized screening, educational notes, and recommendations for follow-up. Ultimately it is left up to individual laboratories to incorporate these guidelines as best suited to their practices.
Table 1 The Bethesda System (TBS) 2014
| SPECIMEN |
| Specimen type |
| · Indicate conventional smear (Pap smear) vs. liquid-based preparation vs. other |
| Specimen adequacy |
| · Satisfactory for evaluation (describe presence or absence of endocervical/transformation zone component and any other quality indicators, e.g., partially obscuring blood, inflammation, etc.) |
| · Unsatisfactory for evaluation (specify reason) |
| – Specimen rejected/not processed (specify reason) |
| – Specimen processed and examined, but unsatisfactory for evaluation of epithelial abnormality because of (specify reason) |
| General categorization (optional) |
| · Negative for intraepithelial lesion or malignancy |
| · Other: See Interpretation/Result (e.g., endometrial cells in a woman ≥45 years of age) |
| · Epithelial cell abnormality: See Interpretation/Result (specify ‘squamous’ or ‘glandular’ as appropriate) |
| INTERPRETATION/RESULT |
| NEGATIVE FOR INTRAEPITHELIAL LESION OR MALIGNANCY (When there is no cellular evidence of neoplasia, state this in the General Categorization above and/or in the Interpretation/Result section of the report – whether or not there are organisms or other non-neoplastic findings) |
| Non-neoplastic findings (Optional to report optional to report; list not inclusive) |
| · Non-neoplastic cellular variations |
| – Squamous metaplasia |
| – Keratotic changes |
| – Tubal metaplasia |
| – Atrophy |
| – Pregnancy-associated changes |
| · Reactive cellular changes associated with: |
| – Inflammation (includes typical repair) |
| · Lymphocytic (follicular) cervicitis |
| – Radiation |
| – Intrauterine contraceptive device (IUD) |
| · Glandular cells status posthysterectomy |
| Organisms |
| · Trichomonas vaginalis |
| · Fungal organisms morphologically consistent with Candida spp. |
| · Shift in flora suggestive of bacterial vaginosis |
| · Bacteria morphologically consistent with Actinomyces spp. |
| · Cellular changes consistent with herpes simplex virus |
| · Cellular changes consistent with cytomegalovirus |
| Other |
| · Endometrial cells (in a woman ≥45 years of age) (Specify if “negative for squamous intraepithelial lesion”) |
| EPITHELIAL CELL ABNORMALITIES |
| Squamous cell |
| · Atypical squamous cells |
| – of undetermined significance (ASCUS) |
| – cannot exclude HSIL (ASC-H) |
| · Low-grade squamous intraepithelial lesion (LSIL) |
| – Encompassing: HPV/mild dysplasia/CIN 1 |
| · High-grade squamous intraepithelial lesion (HSIL) |
| – Encompassing: moderate and severe dysplasia, CIS; CIN 2 and CIN 3 |
| – With features suspicious for invasion (if invasion is suspected) |
| · Squamous cell carcinoma |
| Glandular cell |
| · Atypical |
| – Endocervical cells (NOS or specify in comments) |
| – Endometrial cells (NOS or specify in comments) |
| – Glandular cells (NOS or specify in comments) |
| · Atypical |
| – Endocervical cells, favor neoplastic |
| – Glandular cells, favor neoplastic |
| · Endocervical adenocarcinoma in situ |
| · Adenocarcinoma |
| – Endocervical |
| – Endometrial |
| – Extrauterine |
| – Not otherwise specified (NOS) |
| Other malignant neoplasms |
| · Specify the neoplasms |
| Adjunctive testing – Provide a brief description of the test method(s) and report the result so that it is easily understood by the clinician |
| Computer-Assisted Interpretation of Cervical Cytology – If case examined by an automated device, specify device and result |
| Educational Notes and Comments Appended to Cytology (optional) – Suggestions should be concise and consistent with clinical follow-up guidelines published by professional |
The 2014 Bethesda System and Bethesda Atlas, Third edition (Nayar R, Wilbur DC (Eds). The Bethesda System for Reporting Cervical Cytology. Definitions, Criteria, and Explanatory Notes. Springer, 2015)
TBS 2014 includes normal, inflammatory, and reactive changes all within the no intraepithelial lesion (NIL) category. TBS divides squamous intraepithelial neoplasia into two groups: low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HSIL). LSIL refers to mild dysplasia (CIN I) and condyloma acuminata (human papilloma virus [HPV]). HSIL refers to moderate (CIN II) and severe dysplasia (CIN III) as well as carcinoma in situ (CIS), which are all reported as HSIL without need to subclassify them into HSIL-moderate and HSIL-severe/CIS.
HPV vaccines have been approved for use as proven effective in clinical trials.9, 10, 11, 12 Two companies manufacture two versions of HPV vaccines. Gardasil, a quadrivalent vaccine containing viral L1 capsid proteins from HPV 6, 11, 16, and 18, is made by Merck and Co and was approved by the United States Food and Drug Administration (FDA) in 2006. Cervarix, a bivalent vaccine containing viral L1 capsid proteins from HPV 16 and 18, is made by GlaxoSmithKline. The bivalent vaccine is widely available in countries outside the US. Both vaccines have been shown to be effective in preventing CIN 2/3 as well as endocervical adenocarcinoma. Gardasil has been shown to be 100% efficacy against genital warts.11 The age of candidate for immunization ranges from 9 to 26 years.13 Side effects of quadrivalent vaccine include injection site reactions (pain, swelling, erythema and pruritus) and systemic effects (fever, nausea, dizziness, headache, gastroenteritis, and appendicitis) that were slightly more frequent than placebo controls.14, No deaths were determined to be vaccine or placebo related.14 Immunization with these vaccines will undoubtedly not only reduce the incidence of anogenital HPV-related diseases, but also likely other HPV-associated diseases such as oropharyngeal cancer.
SAMPLING TECHNIQUES
The accuracy of the Papanicolaou smear depends largely on obtaining an adequate cellular sample for examination. Several techniques can be used to obtain adequate samples of the uterine cervix, vagina, endocervix, and endometrial cavities.15 The adequacy does not solely or evenly primarily depend upon the device used, but often more importantly on the technique of the individual taking the specimen.
The most commonly used and accepted techniques are ectocervical scraping with the Ayre spatula, and endocervical brushing for transformation zone and endocervical canal sampling. The endocervical brush should gently be introduced into the cervical canal and gently rotated 180 degrees. If the brush is inserted with force and with a harsh back-and-forth movement, the smear obtained will be composed mainly of blood, distorted endocervical cells showing marked pulling/crush artifact, and muscle fibers, consequently the material will be inadequate for diagnostic evaluation. The modified Ayre spatula with an extended tip was developed to obtain endocervical sampling, however, it is now appreciated that other instruments are superior to the spatula in reliably obtaining transformation zone sampling. The endocervical broom can be used alone or in combination with other devices. Guidelines for taking an adequate conventional cervicovaginal smear are available.
Liquid-based methods are currently used by many physicians to collect and preserve the material collected from the cervix and vagina. Cytyc Corporation (ThinPrep System) and Tripath imaging (SurePath) are the two vendors offering FDA approved liquid-based technology for cervicovaginal specimens. Liquid-based preparations may decrease preanalytic errors by fixating the sample more rapidly (preventing air drying and better preservation), decreasing artifacts and obscuring cells, such as mucus, cellular debris and red blood cells (RBCs)/white blood cells (WBCs), and homogeneously mixing the sample. Data suggest that utilization of liquid-based technology increases the sensitivity for detection of preneoplastic/neoplastic lesions of the cervix.16, 17, 18, 19, 20 However, regular screening remains the most effective means of cancer prevention.
Hormonal evaluation was previously performed using a gentle scrape of the upper lateral vaginal wall, however, this method is now antiquated due to more current sophisticated laboratory methods. However, if an abnormality is encountered on the cervicovaginal smear, in relation to the patient’s age and menstrual history, a maturation index can be issued or a comment made regarding the maturation pattern being inconsistent with age and menstrual history.
Several techniques, such as Tao brush endometrial sampler, pipelle biopsy device, glass cannula, and rubber bulb have been developed to sample the endometrial cavity for cytologic evaluation.15, 21 None of the devices make screening for endometrial cancer feasible and no comprehensive screening program for endometrial cancer has been mounted to date.22 The TBS 2014 contains a category termed "other" for reporting benign endometrial cells in women aged ≥45 years (≥40 years in TBS 2001), with atypical endometrial cells reported as an epithelial cell abnormality.8 Historical evidence suggests that even this terminology leads to excessive investigation with little or no benefit from the detection of significant endometrial disease.8, 23 It is noted in the Bethesda System 2014 that cervical cytology is unreliable for the detection of endometrial lesions and should not be used to evaluate causes of suspected endometrial abnormalities.8
Handling of specimens
Proper preservation of cell detail is essential for accurate diagnostic assessment and interpretation. The most common method is the thin-layer, liquid-based method. Thin-layer, liquid-based methods do not require smear preparation by the clinician. The cell sample is placed directly into the liquid preservative per the manufacturer’s instructions and the thin-layer slide is prepared in the laboratory. In addition to making a thin-layer slide for cytologic assessment, the material from the vial can also be sent for ancillary testing such as HPV typing, as well as microbiologic evaluation for Chlamydia and Neisseria gonorrhea if clinically indicated.
If the patients do not have insurance and direct smears are selected, cervical and vaginal samples should be smeared rapidly and gently on a glass slide to avoid air drying of the cells, which may cause artifacts that can preclude adequate cytologic evaluation. Rapid immersion of the smear in 95% ethanol is the preferred method. Other alternatives for wet fixation include 100% methanol, 80% isopropanol, or denatured ethyl alcohol. When wet fixation is not possible, the most commonly used alternative method is spray fixation. The non-aerosol or pump method is preferable over aerosol spray fixatives.
Cervicovaginal smears should be obtained at midcycle to avoid the presence of large amounts of menstrual blood that can obscure the morphologic features of the epithelial cells. However, in some instances bloody smears are unavoidable, and hemolysis of red blood cells can be achieved. The smears can be air dried for approximately 15 minutes, rehydrated in saline solution for 15–30 seconds, and fixed in 95% alcohol. Papanicolaou staining would proceed in the usual manner. Once the smears are air dried they should promptly be delivered to the cytology laboratory and technical staff should be advised that the slides should be hydrated for 30 seconds prior to staining. It is important to note that this technique is not useful if there is copious mucus present within the sample.24 The problem of obscuring blood is largely resolved in liquid-based collection techniques.
Specimen adequacy
The most recent TBS 2014 has two adequacy categories: “satisfactory for evaluation” and “unsatisfactory for evaluation” (see Table 1). The “satisfactory but limited by” category has been eliminated. The presence or absence of endocervical/transformation zone (EC/TZ) component and any other quality indicators are provided immediately after the term “satisfactory for evaluation.” The unsatisfactory report includes reasons for the unsatisfactory designation. Criteria for adequacy evaluation on conventional and liquid-based smears have been provided by the 2014 TBS guidelines.8 The evaluation of adequacy is considered by many to be the single most important quality assurance component of TBS8 and adequacy is considered a central component in patient management guidelines.8
Satisfactory smears
An adequate conventional smear should have a minimum of approximately 8,000–12,000 well-preserved and well-visualized squamous epithelial cells. For liquid based preparations, an estimated minimum of 5000 well-visualized/well-preserved squamous epithelial cells should be seen. It is important to note that these cell ranges apply only to epithelial cells present. TBS 2014 allows certain discretion to be made to accept fewer cells in postmenopausal or postchemo/radiation patients, however, fewer than 2000 should be unsatisfactory in most circumstances.
Although “satisfactory but limited by…” has been removed from TBS, the laboratory has the option to add quality indicators (presence/absence of endocervical component, other obscuring factors, etc.) to the adequacy statement. At least 10 well-preserved endocervical or squamous metaplastic cells should be observed to report that a transformation zone component is present. The wording suggested by TBS 2014 is as follows:
SATISFACTORY FOR EVALUATION
The report should describe presence or absence of endocervical/transformation zone component and any other quality indicators, e.g., partially obscuring blood, inflammation, etc., as appropriate.
Unsatisfactory smears
For unsatisfactory specimens, the report should indicate whether or not the sample has been processed/evaluated by the laboratory. The wording suggested by TBS 2014 is as follows:8
UNSATISFACTORY FOR EVALUATION
A. Rejected specimen:
Specimen rejected (not processed) because _____ (specimen not labeled, slide broken, etc.)
B. Fully evaluated, unsatisfactory specimen:
Specimen processed and examined but unsatisfactory for evaluation of epithelial abnormality because of _____ (obscuring blood, obscuring bacteria, etc.)
Additional comments/recommendations, as appropriate
An abundance of intact or hemolyzed red blood cells and bacteria can obscure the diagnostic epithelial sample, precluding adequate cytologic evaluation.8 Other causes of inadequate specimens are the presence of few epithelial cells, the presence of only endocervical cells when the ectocervix was sampled,8 and the presence of significant degenerative changes. An unsatisfactory smear is considered to be unreliable for the evaluation of epithelial cell abnormalities; however, smears that are processed and evaluated by the laboratory may provide information such as presence of blood, inflammation, organisms, etc., which may be of some clinical importance. A longitudinal study found that unsatisfactory cervicovaginal smears were more commonly obtained from high-risk patients, and had significantly more SIL/cancer on follow-up compared to a cohort of patients with satisfactory index smears.25 Lower cellularity specimens may be acceptable in women who have undergone hysterectomy for malignancies, chemotherapy, or radiation therapy, as obtaining specimens with higher cellularity may not be possible in these circumstances.26 Judgment should be exercised when determining whether the specimen is unsatisfactory and whether early repeat cytology is indicated. Both the laboratory and clinician should monitor the number of unsatisfactory smears as a quality assurance measure. The preferred management for most women undergoing routine annual/biennial screening is a repeat smear in 12 months.27
The 2012 ASCCP Consensus Guidelines for the Management of Abnormal Cervical Cancer Screening Tests included adequacy management guidelines vetted by a national consensus conference.28, 29, The role of high-risk human papillomavirus (hrHPV) triage and co-testing was specifically considered. If HPV testing is done in unsatisfactory specimens and is positive, the woman will still require some additional follow-up (Fig. 1). These guidelines describe management of women with unsatisfactory cytology to recommend repeat cytology in 2–4 months. hrHPV triage testing is not recommended. Women with unsatisfactory cytology may receive treatment to resolve atrophy or obscuring inflammation prior to repeat cytology. Colposcopy is recommended when a woman has had two consecutive unsatisfactory cytology tests. Colposcopy can also be performed if the woman is known to be HPV16 or HPV18 positive by genotyping or if she is age 30 or greater and is hrHPV positive. An unsatisfactory Pap test that was not indicated according to the screening protocol (e.g., the patient was not due for her next cervical cancer screen) does not necessarily need to be repeated. Women who have had a hysterectomy with the removal of the cervix for benign disease do not generally benefit from screening.
{kind=link}
BETHESDA 2014 SYSTEM TERMINOLOGY
This is an optional component included within TBS 2014.8 It was designed to assist clinicians and/or their staff to triage cervical smear reports adequately and includes:
1. No intraepithelial lesion/malignancy: This category encompasses “benign cellular change/organisms” and “reactive cellular change.” The cytologic changes can be described under this category as “non-neoplastic findings.”
2. Epithelial cell abnormalities: This category is further specified as squamous, glandular or extrauterine/other.
3. Other: This category is for cases in which there are no cytologic abnormalities per se, however, the finding may indicate some risk of a preneoplastic or neoplastic condition (e.g., endometrial cells in a woman >45 years of age).
These three general categories are mutually exclusive; thus, if several findings are present, the general categorization should be based on the most clinically significant result.8
Interpretation/result
The Bethesda guidelines suggest cervical cytology to be used primarily a screening test, which in certain instances serves as a medical consultation by providing an interpretation/result that contributes to an overall diagnosis.8 Because an individual patient’s final diagnosis and subsequent management should integrate the clinical and laboratory results, in TBS 2001, the term “diagnosis” was replaced by “interpretation” or “result.” The subsequent guideline revisions and updates maintain this nomenclature.8
NONNEOPLASTIC CHANGES
Certain organisms (Trichomonas, fungi (yeast), shift in flora, Actinomyces, Herpes, CMV) are reported routinely by most laboratories; however, reporting of other non-neoplastic findings is variable, and remains optional under TBS 2014 guidelines.8
Organisms
Historically, reports in the literature have suggested that microorganisms that induce changes in the cervical epithelium may be potentiating the development of cervical neoplasia. Trichomonas vaginalis, Chlamydia trachomatis, and Herpes genitalis30, 31 cause inflammatory changes that are not infrequently associated with squamous intraepithelial lesions (SIL) and may produce fertile ground for the development of preneoplastic and neoplastic squamous lesions.
Normal bacterial flora
The vaginal flora is composed of multiple microorganisms. The most common include Lactobacillus vaginalis (Fig. 2), Streptococcus viridans, and Staphylococcus epidermidis. They thrive in an environment in which balance is established by hormones as well as physical influences, such as intrauterine devices. Occasionally, intrauterine devices influence the balance of the vaginal flora, causing symptoms and sometimes infection with Actinomyces.
{kind=link}
Changes caused by inflammation include metaplasia, surface reactions, such as hyperkeratosis, parakeratosis, and reparative processes. Frequently, the nuclei of the epithelial cells show enlargement, but the chromatin is fine, and cytoplasmic changes are variable. In other instances, degenerative changes occur. The background may show numerous neutrophils, a large number of bacterial forms, histiocytes, and debris. When this exudate obscures the surface of the epithelial cells, it is recommended to treat the infection and repeat the smears because dysplastic or malignant cells may be obscured beneath the white blood cells, bacteria, and debris.
Nonspecific vaginitis is commonly seen in patients harboring flora such as mixed bacteria or coccobacilli. Occasionally, cells show inflammatory changes in a background of rod-like bacteria that appear to be Döderlein’s bacilli. These bacteria belong to a heterogeneous group of organisms, and they morphologically resemble other microorganisms that may cause inflammatory changes in the epithelial cells. The presence of polymorphonuclear leukocytes in isolation is not an indication of inflammation, reactive changes in the epithelial cells are also necessary.
Bacteria
Gardnerella vaginalis – Gardnerella vaginalis, mobiluncus, and other anaerobic bacteria (bacterial vaginosis) may be found in asymptomatic women (40–50% of patients), and other women may develop leukorrhea and an inflammed vaginal mucosa. Smears show cells covered by bacteria, so called clue cells, against a background of feathery coccobacillary forms (Fig. 3).
{kind=link}
Actinomyces – Actinomyces species occur frequently in association with intrauterine device usage. Less frequently, the use of a pessary, tampons, or any type of foreign body left in place for long periods in the cervicovaginal area may elicit infection with these bacteria. Pelvic infection may occur in some patients. In Papanicolaou-stained smears, filamentous bacteria are seen, usually in clumps as well as single forms (Fig. 4).
{kind=link}
Chlamydia trachomatis – Chlamydia trachomatis infection is seen in cervicovaginal smears as cytoplasmic bacterial inclusions (Fig. 5). The false-positive rate is high for morphologic diagnosis, and mucus secretion in immature metaplastic cells, phagocytosed debris, and degenerative changes may be the source of erroneous diagnosis of C. trachomatis infection. Because morphologic distinction between these entities is poorly reproducible and not practical, more specific microbiologic assays (polymerase chain reaction [PCR], enzyme immunoassay [EIA]) are now used for identification of chlamydia. The FDA approved testing for chlamydia out of liquid-based collection devices.
{kind=link}
Fungi
Candida albicans – Candida albicans is the most common fungus found in the cervicovaginal smear (Fig. 6). Yeast forms as well as pseudohyphae are commonly encountered. Diabetes, pregnancy, birth control pills, and antibiotic use may change the vaginal flora, and predispose patients to infection by this fungal agent. Fewer than 10% of mycotic vaginal infections are caused by other Candida species, namely, Torulopsis glabrata, which is morphologically similar to the yeast form of C. albicans.
{kind=link}
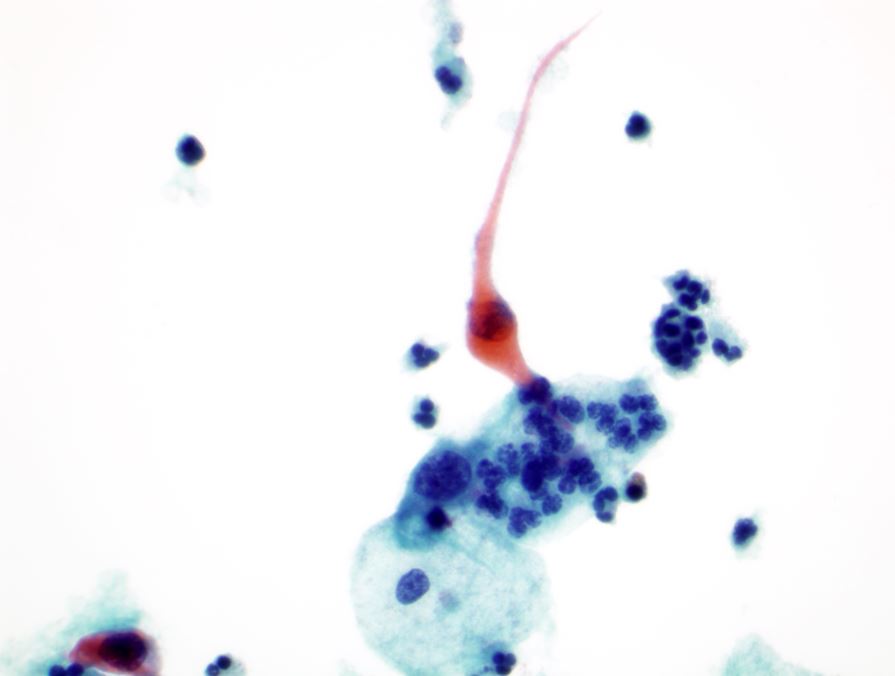
Flagellates
Trichomonas vaginalis – Trichomonas vaginalis infection may cause changes that range from minimal to severe. Fifty per cent of infected women are asymptomatic. The classic signs of inflammation are present in the epithelial cells and also in the background that contains variable amounts of debris and white blood cells. Small perinuclear halos may be seen in the squamous cells, but this finding is not pathognomonic of this infectious process. The organisms are seen as pear-shaped structures with a punctate, almond-shaped nucleus (Fig. 7). Without the presence of nuclei, a diagnosis of T. vaginalis cannot be made because fragments of cytoplasm of the intermediate squamous cells may resemble these flagellates. Leptothrix (Leptotrichia buccalis) are filamentous bacteria that frequently are associated with T. vaginalis (70–80% of cases) (Fig. 7). Certain forms of Döderlein’s bacilli are morphologically identical to Leptotrichia, and only through microbiologic culture can they be adequately identified.
{kind=link}
Viruses
The most common viral infections encountered in cervicovaginal smears are caused by papillomaviruses and herpes genitalis. Immunosuppression may be a setting for viral infection, such as HPV and herpes simplex, and also for the development of neoplasia.32 However, it was not until the 1970s that the tools of modern molecular biology were applied to the molecular characterization of the papillomavirus family that HPV,33 with more than 100 molecular types, emerged as the major player in the etiology of cervical neoplasia.
Papillomaviruses – Papillomaviruses are the principle etiology of cervical neoplasia (squamous cell and endocervical glandular cell).
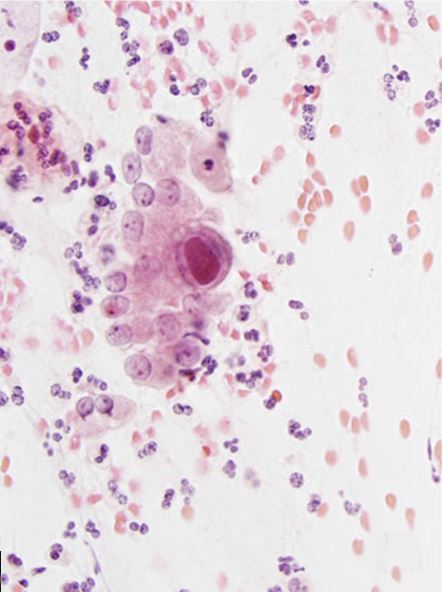
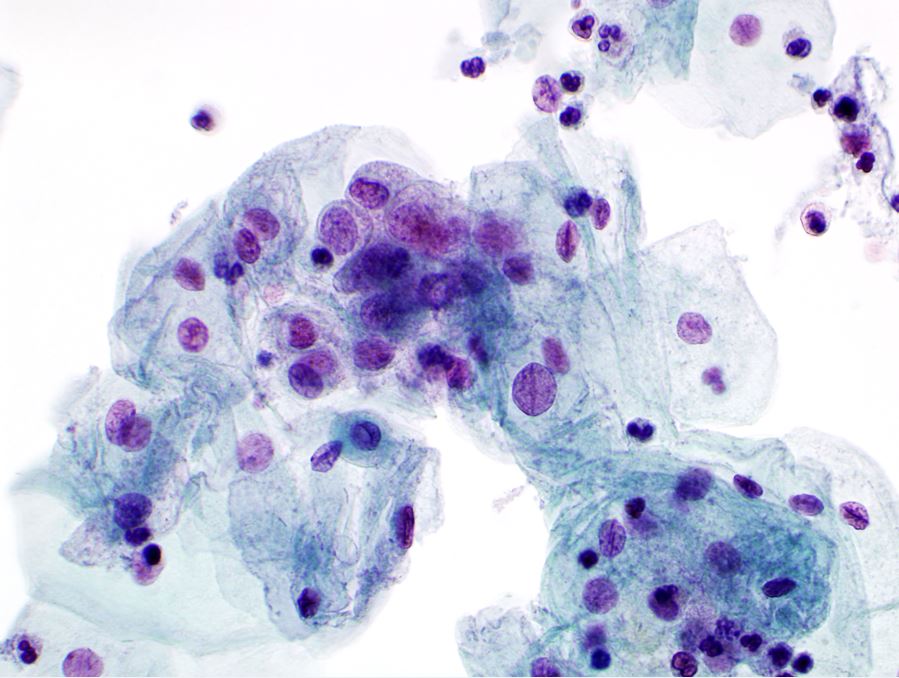
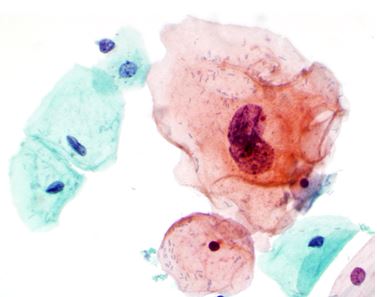
Herpes genitalis – Herpes genitalis infection occurs primarily by sexual transmission. Clinically symptomatic eruptions may occur. Typically, they are related to stress, the menstrual period, or unrelated diseases. Cytologically, the epithelial cells show multinucleation, ground-glass chromatin, and intranuclear inclusions in some cells (Fig. 8).
{kind=link}
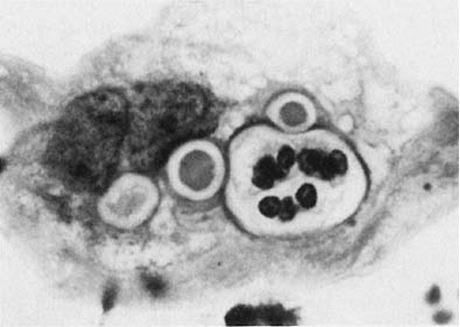
Cytomegalovirus – Cytomegalovirus (CMV) produces cytopathic effect most commonly in immunocompromised individuals. The CMV infected cells may sometimes be confused with tumor cells. However, the inclusions have characteristic central eosinophilic bodies and marginated material, creating a prominent halo around the central inclusion. In contrast to herpes viral effect, CMV can also show cytoplasmic inclusion in addition to intranuclear inclusions. The cytopathic effect of CMV affects mostly the endocervical glandular cells. CMV infection is usually not seen in squamous cells; however, it can infect a wide range of other epithelial, mesenchymal, lymphoid, and hematopoietic cells. Cytopathologic findings include cellular and nuclear enlargement as well as characteristic large eosinophilic intranuclear viral inclusions with a prominent halo (Fig. 9).8 Small cytoplasmic, basophilic inclusions can also be present.
{kind=link}
BENIGN/REACTIVE CHANGES
Inflammation and regenerative changes
A common finding in cervicovaginal smears is reparative change as a result of a variety of processes that may involve the glandular, metaplastic, and squamous epithelium.22 These changes are seen after damage to the mucosa and after radiation, chemotherapy, infections, or any condition that alters the tissue integrity. When a reparative process is present, cellular samples display monolayer sheets of elongated, large, immature cells with a regular arrangement and conserved polarity. The nuclei are enlarged and contain pale, powdery and evenly distributed chromatin and nucleoli. The cytoplasm is delicate and possibly thickened with possibly variable staining quality and ill-defined borders. Isolated atypical cells of a reparative nature are rare (Fig. 10).34 Inflammatory changes in epithelial cells are differentiated from dysplasia and carcinomas by the relative low content of chromatin, symmetrical nuclear outline, and low nuclear-cytoplasmic ratio. When inflammatory/repair cause epithelial atypia in either squamous or endocervical cells, the changes may be classified as atypical squamous cells (ASC) or atypical glandular cells (ACG). Follow-up is needed in these cases to make sure the atypia has regressed.
Differences exist between these proliferating cells and invasive squamous carcinoma, such as the absence of single atypical cells, macronucleoli, and tumor diathesis (Fig. 10). These features in addition to low nuclear-cytoplasmic ratio are important to differentiate reparative processes from nonkeratinized squamous cell carcinoma and the rare sarcomas.22
{kind=link}
Therapy changes
Several modalities of therapy affect malignant and benign cells, the latter at the vicinity or at a distance from the malignant neoplasm. The types of therapy include chemotherapy, immunotherapy, radiation therapy, and mechanical therapy. Therapy of any modality may cause changes in benign cells that can resemble malignant changes.
By examining cervicovaginal smears, short- and long-term radiation changes can be observed.22, 34, In benign cells, short-term changes usually are found within 6 months of irradiation. These changes consist of nuclear enlargement displaying degenerative changes (pallor chromatin, nuclear wrinkling or smudging, condensation of chromatin), prominent single or multiple nucleoli, abnormal mitosis, and multinucleation (Fig. 11). At the cytoplasmic level, there are varying degrees of vacuolization and/or polychromatic staining (Fig. 11). Cellular enlargement occurs, and a low nuclear-cytoplasmic ratio is maintained, a critical feature that helps the cytopathologist to recognize the affected cells as benign.34 Short-term changes can also be encountered in malignant cells shortly after treatment. However, with effective treatment, they regress approximately 1 month after the completion of therapy because of their exquisite sensitivity to radiation. During the first month, an exudate contains leukocytes and debris resulting from local necrosis. Mononucleated and multinucleated histiocytes are often present. Malignant cells that show radiation changes 6–8 weeks after treatment indicate persistence of the neoplasm. After this time, the presence of malignant cells without radiation changes indicates recurrence.
{kind=link}
The features seen with long-term radiation changes are reflected in cytologic smears by aberrant cells from the basal layers, displaying features including cellular enlargement, and atrophy. These changes can persist for several years, and vary from patient to patient. Under light microscopy, cytoplasmic vacuolization starts at the parabasal layers, and engulfment of polymorphonuclear leukocytes within some of the vacuoles are seen. Some of the cells acquire an abnormal staining quality referred to as amphophilia. The most important diagnostic characteristic change is significant enlargement of the epithelial cells, with otherwise normal features. Giant cell histiocytes, and reparative changes,35 are usually encountered. The effectiveness of radiation can be monitored by the assessment of several cellular features in cervicovaginal smears.22, 35, 36 The cytopathologist should observe the postradiation smear for increased cellular maturation, which is a warning sign for the development of de-novo intraepithelial neoplasia. Equally important is the detection of tumor diathesis, which may indicate persistence or recurrence of the tumor. True tumor diathesis has necrotic cells with nuclear and cytoplasmic fragmentation, hemolyzed blood, and debris; the presence of merely a “grungy” background is not sufficient to qualify.
Systemic chemotherapy may affect cells exfoliated from the cervicovaginal area. Cellular changes share many similarities to changes caused by ionizing radiation.34 Occasionally, the cells look highly abnormal and atypical. The key diagnostic features are relative maintenance of the amount of cytoplasm and the absence of mitotic figures.
Immunodeficiency, including that caused by immunosuppressive therapies, increases in the number of neoplasms at several body sites, including the vulva and cervix.37 The incidence of cervical neoplasms has been reported to reach a 14-fold increase compared with the incidence in the non-immunosuppressed population. It is advisable to have a baseline cervicovaginal smear to monitor the development of neoplasms during immunosuppressive therapy.37
Electrocautery of the uterine cervix produces coagulative cellular necrosis and significant inflammatory response by influx of polymorphonuclear leukocytes and lymphocytes.34, 37 These changes may mimic a tumor diathesis background. In addition, cervicovaginal smears may harbor atypical cells after electrocautery treatment for benign processes. Because these cells may persist for several weeks,38 a waiting period of 1–3 months should be allowed to permit the necrosis and healing process to occur.34, 38 These changes are not limited to the squamous epithelium; atypia of the endocervical cells is also encountered. For these reasons, a history of electrocautery as well as the date of therapy for neoplastic and nonneoplastic processes should be disclosed to the pathologist to avoid misinterpretation of cervicovaginal smears. Laser therapy has been used for years to eradicate dysplasia and CIS of the uterine cervix.39, 40 The carbon dioxide laser produces a localized intense heat that inactivates cellular components, interrupting the replication process at the cellular level.40 Laser therapy has several advantages over cryotherapy with respect to cervicovaginal smears. Because of the almost complete absence of bleeding and necrosis as well as the faster healing process, the inherent difficulties (atypical cells and inflammatory background) in cryotherapy are short-lived with laser treatment, and the cervicovaginal smears return to normal quickly.39, 40 The regenerative process takes place from the epithelial edges of the ulcer that is produced by the laser and fills the gap within 2 weeks. In spite of a positive Schiller’s test result, the cells desquamated from this site are easily recognized as benign.39 After approximately 6 weeks, Schiller’s test result becomes negative as the epithelium matures in the newly re-epithelialized site.
Benign surface reactions of squamous epithelium
Hyperkeratosis
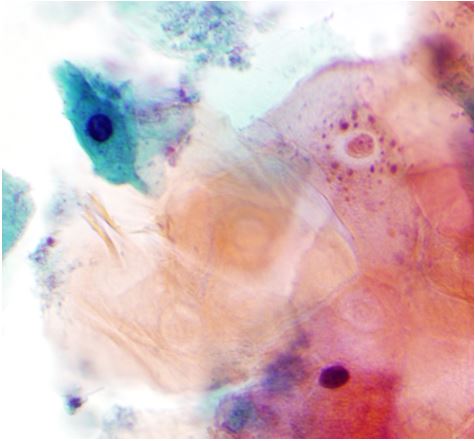
Under the influence of a variety of stimuli, the surface of the squamous epithelium may develop a granular layer and several layers of anucleated cells as a protective mechanism, a phenomenon referred to as hyperkeratosis. Clinically, this condition is seen as an area of leukoplakia; cytologically, the smears contain single or groups of anucleated squames (Fig. 12).41 The cells derived from the granular layer show keratohyalin cytoplasmic granules.
{kind=link}
Thick patches of those cells with irregular outlines seen consistently throughout the smear are of diagnostic importance. Keratohyalin granules and a few anucleated squamous cells are normally seen around midcycle, at the height of estrogenic stimulation and have no clinical significance. However, the presence of many of these cells, associated with patches of anucleated squames, indicates hyperkeratosis and presence of a granular layer in the cervical mucosa. Occasional anucleated cells on the edge of the slides or in the specimen should not be mentioned because they likely represent contamination from the patient’s vulva or from ungloved fingers handling the slides. It is thus advisable to report only cells with keratohyalin granules associated with anucleated squames that are intermixed with other normal components of the smears. Extensive hyperkeratosis, when appropriately identified, may be associated with underlying abnormal epithelium in 29% of patients.41
Parakeratosis
Parakeratosis is another type of surface reaction that is characterized by a proliferation of layers of small nucleated squamous cells with pyknotic nuclei. In smears, miniature keratinized squamous cells are seen, either singly or in sheets (Fig. 13). The nuclei are small and round or oval. The nuclear-cytoplasmic ratio is low. Parakeratotic cells without nuclear abnormalities can be seen in a variety of situations, such as inflammation, pessary use, and other processes that irritate the cervical mucosa. When they are enlarged and irregular, they are classified as atypical squamous cells or atypical parakeratosis. Atypical parakeratosis correlates with the presence of an underlying SIL or invasive carcinoma in approximately 40% of patients.42 Once a diagnosis of atypical parakeratosis is made, HPV test should be reflexed.
{kind=link}
Reserve cell hyperplasia
The endocervical canal is composed of mucus-producing cells as well as tall columnar cell that may be both ciliated and nonciliated. Normally, the endocervical epithelium is attached directly to the stroma without a basal layer. Under the mucosa, there are isolated immature totipotent cells that subsequently differentiate and give rise to endocervical cells. Under a variety of hormonal or physical stimuli, these germinative cells may proliferate, giving rise to reserve cell hyperplasia. Reserve cell hyperplasia may develop in young patients as a result of physical injury and in postmenopausal patients because of hormonal stimuli, or from hormones produced by the adrenal gland that are later metabolized to estrone. The cells desquamated from reserve cell hyperplasia have small nuclei, finely granular chromatin, and small amounts of cytoplasm. Caution should be taken not to over diagnose them as CIS in cytologic and histologic samples. They have a monomorphic appearance, lack hyperchromasia, and usually are seen in small, organized clusters. The differential diagnosis includes HSIL and small cell carcinoma. HSIL shows hyperchromatic nuclei with scant amounts of cytoplasm. The features of small cell carcinoma are similar to those of HSIL. However, tumor diathesis, that is necrosis, hemolyzed blood, and cellular debris, are associated with the invasive small cell carcinoma.
Squamous metaplasia
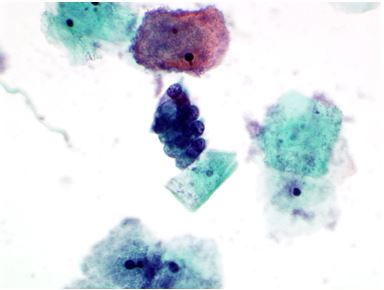
By a process of maturation, the reserve cells may acquire squamous features, and squamous metaplasia will replace the original glandular epithelium. The stimuli inducing those changes can be physical, inflammatory, or hormonal.43 Squamous metaplasia is a benign process found frequently in smears. The immature metaplastic cells may maintain the mucus-producing ability inherent to endocervical cells because they have a similar histogenesis. This feature mimics the appearance of atypical glandular cells, and may be difficult for the cytologist to identify. Immature metaplasia in single cells with nuclear enlargement only, may mimic high-grade squamous dysplasia (Fig. 14). As a benign component, it should be recognized for adequacy of sampling because its presence indicates adequate sampling of the transformation zone. However, preneoplastic and neoplastic changes may take place in a minority of metaplasia cases. In those instances, metaplastic dysplasia of varying degrees, HSIL, or nonkeratinized invasive squamous carcinoma may develop.
{kind=link}
Intrauterine device effect
The presence of an intrauterine device (IUD) in the endocervical and endometrial cavity causes an inflammatory response and subsequent irregular desquamation and shedding of these epithelial cells from these areas may mimic a glandular or squamous neoplasm. Squamous metaplasia showing variable degrees of maturation is frequently seen in ectocervical-endocervical smears.
Atypical glandular cells of endocervical44 or endometrial origin also may be encountered (Fig. 15).34, 45, They can be recognized as reactive or benign if clinical information about intrauterine device use is disclosed, avoiding false-positive results.45 A less common cell type, referred to as indeterminate, has been postulated as being of endometrial origin.46 Few of these cells are seen in a cervicovaginal smear, and they have a variety of features that distinguish them from CIS, such as multinucleation, presence of enlarged nucleoli, and absence of other atypical cells in the smear showing a spectrum of dysplastic changes. After removal of the device, these cells disappear from cervicovaginal smears after 1 month to 1 year.46
{kind=link}
Microglandular hyperplasia
Microglandular hyperplasia can be seen in patients taking oral contraceptives, in pregnancy, postpartum, the action of progestogenic stimulation on the endocervical epithelium, hyperestrogenism or exogenous estrogenic therapy. It is not considered to be a preneoplastic change. Florid microglandular hyperplasia in histologic sections may architecturally resemble clear cell adenocarcinoma.47 Lack of stromal invasion, rare mitosis, and intracellular glycogen excludes the diagnosis of malignancy. Microglandular hyperplasia is a common finding in cervicovaginal smears. The classic appearance of the smears is of numerous dispersed rounded endocervical cells (Fig. 16). Some show a pseudokeratinized appearance caused by ischemic necrosis; hence, the misnomer pseudoparakeratosis was used in the past. Cytologically, some cases may be mistaken for atypical squamous or atypical glandular cells.
{kind=link}
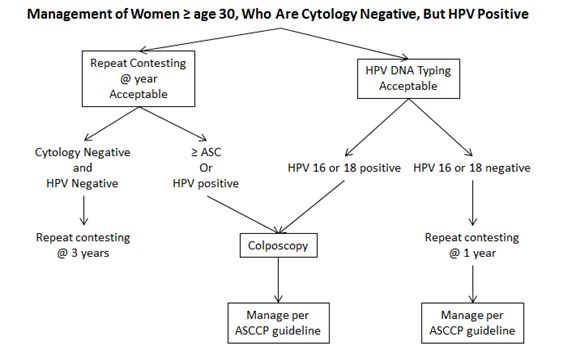
2012 ASCCP Guidelines further discuss management of women with negative cytology but with absent or insufficient EC/TZ component.28, 29, 48, For women aged 30 years and older, hrHPV testing is preferred (Fig. 17). If the hrHPV test is negative, routine screening interval is recommended. Repeat cytology in 3 years is acceptable if hrHPV testing is not performed. If hrHPV is positive, women should receive either genotyping or cotest in 1 year. For women aged 21–29 years, routine screening is recommended when cytology is reported as negative with absent EC/TZ component. hrHPV co-testing is not indicated in women aged 21–29 years; however, some women in this age group may electively undergo hrHPV primary screening using FDA-approved testing methods.
{kind=link}
Fig. 17B. ASCCP guideline for cytology NIL.
{kind=link}
SQUAMOUS EPITHELIAL LESIONS
With increased sophistication in the field of cytopathology, it was found that analysis of cellular samples could provide a precise diagnosis that could be correlated with histologic samples. By sampling the surface of the abnormal mucosa, it is possible to evaluate the process of maturation from the basal to the uppermost layers.43 The stimulus that induces maturation is related directly to the degree of differentiation of the abnormal basal layers. The less differentiated cells will respond poorly to stimuli inducing maturation, and will emerge to the surface and a higher degree of abnormality will be seen when the surface is sampled.
Current terminology for squamous intraepithelial lesions
The 2014 Bethesda System8 suggests reporting squamous epithelial abnormalities as follows: atypical squamous cells of undetermined significance (ASC-US); atypical squamous cells/rule out HSIL (ASC-H); low-grade squamous intraepithelial lesion (LSIL); and high-grade squamous intraepithelial lesion (HSIL). Recently, some authors suggested adding one more category, LSIL, cannot exclude HSIL.49, 50,
A two-tiered terminology introduced in the 1988 TBS5 is still used today, which divides the spectrum of squamous epithelial abnormalities into LSIL and HSIL.8 LSILs encompass the cellular changes associated with the cytopathic effect of HPV, also referred to as koilocytotic atypia, and mild dysplasia/CIN I. HSILs encompass moderate dysplasia (CIN II) and severe dysplasia (CIS/CIN III). The dichotomous classification of SIL (LSIL/HSIL) is supported by current virologic, molecular, and clinical evidence that LSIL is generally a transient infection with HPV, and HSIL is more often associated with persistence of HPV and higher incidence of progression.8 In addition, data from the ASCUS/LSIL Triage Study (ALTS), has further supported the two-tier terminology by demonstrating that (1) LSIL/HSIL is a fairly reproducible breakpoint, (2) confirmed that subdividing HSIL into moderate and severe dysplasia is not reproducible, and (3) HPV cytopathic effect cannot be reliably separated from mild dysplasia/CIN I.5, 7, 8
Atypical squamous cells
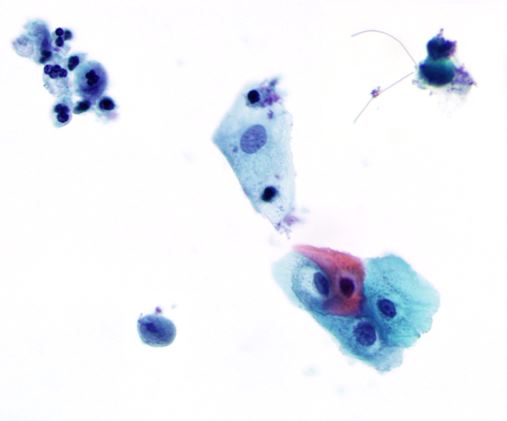
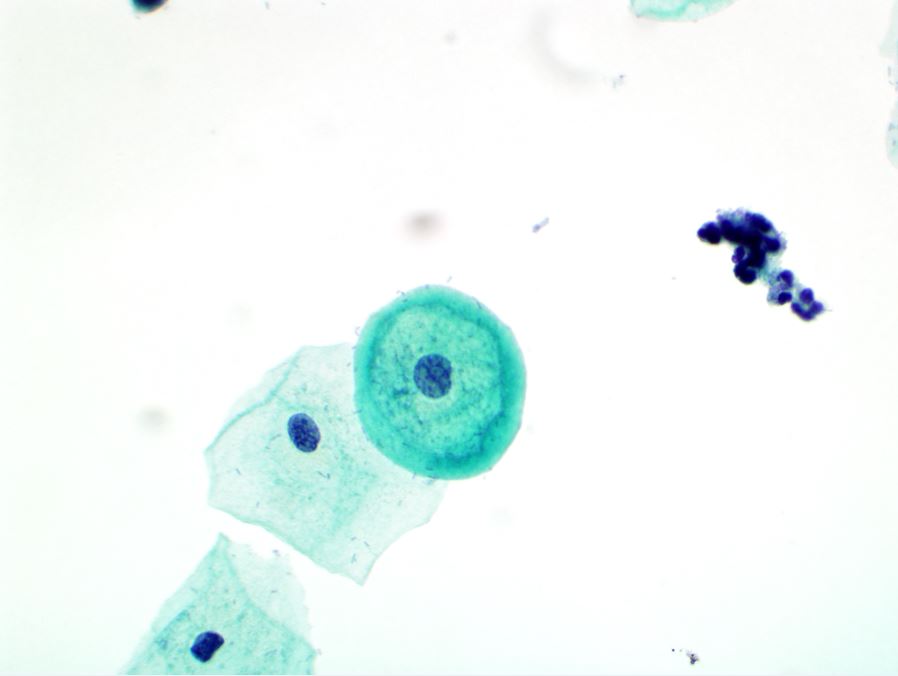
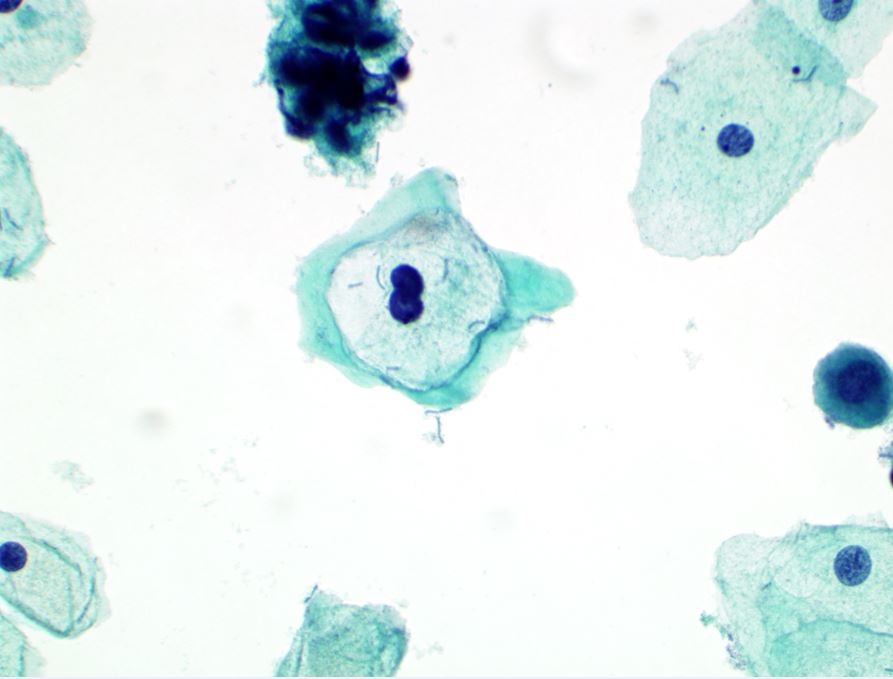
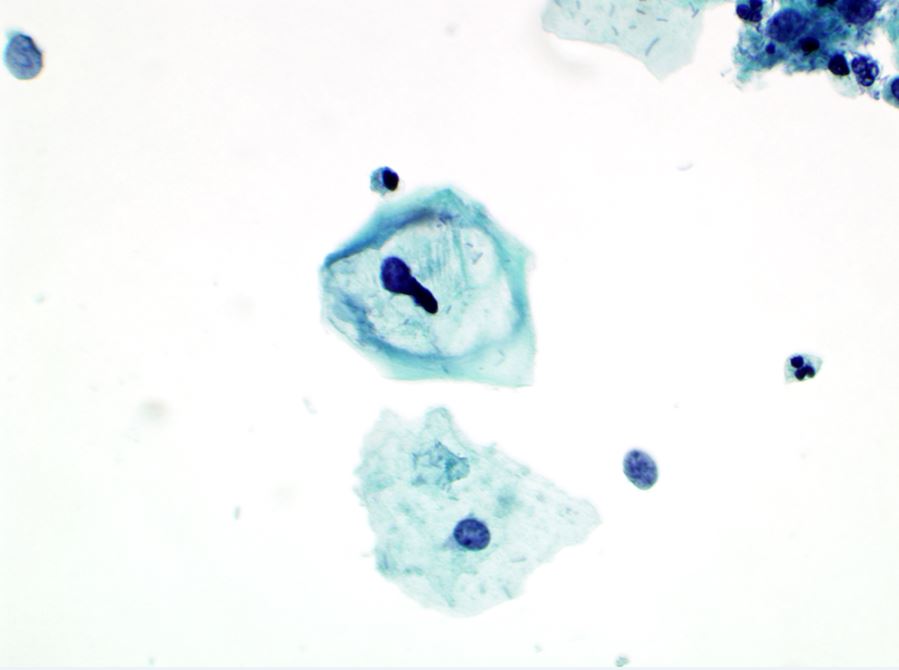
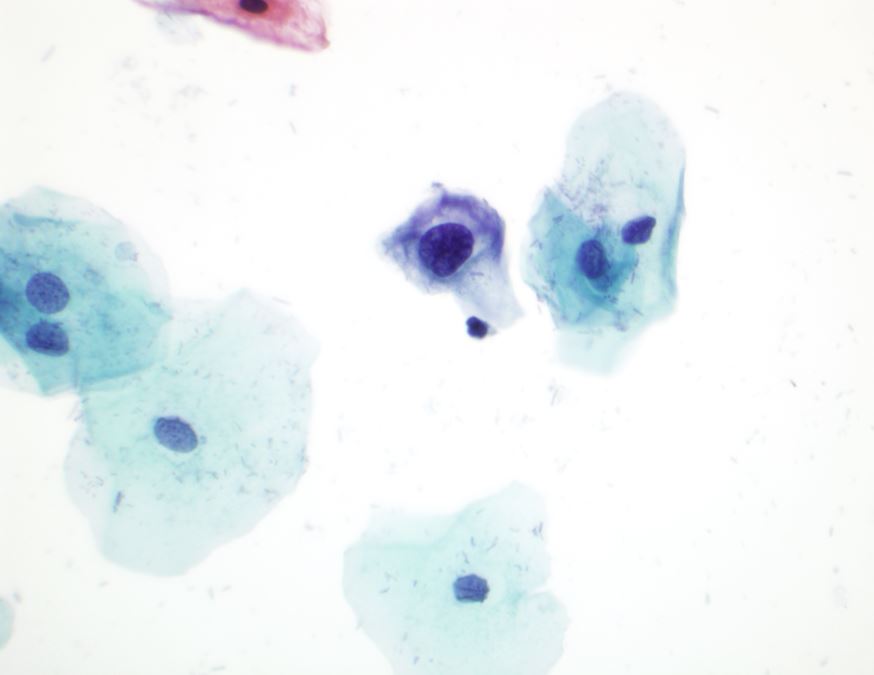
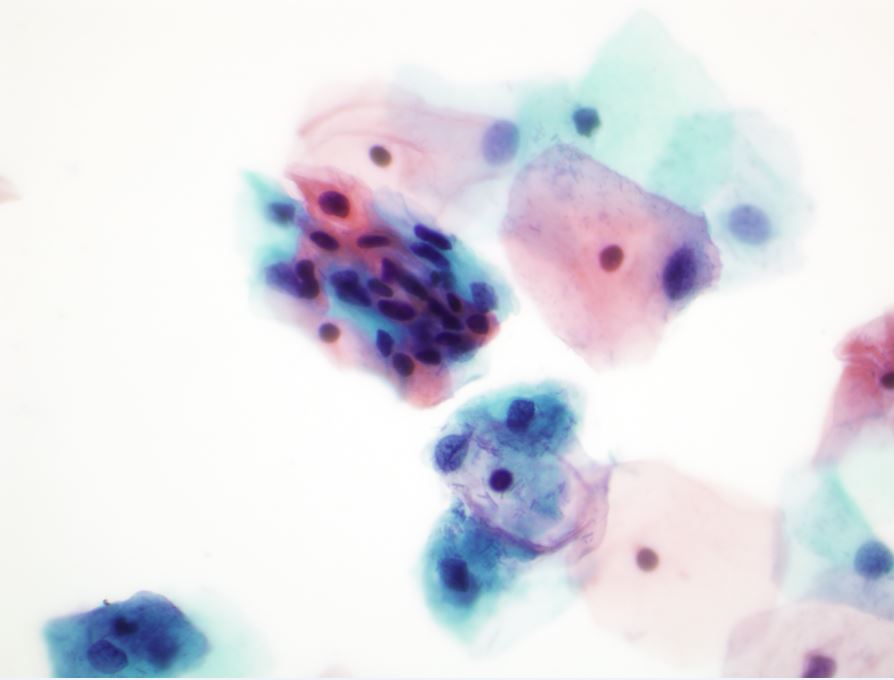
Atypical squamous cells of undetermined significance (ASCUS) – ASCUS represents squamous cell abnormalities that are more marked than those attributable to reactive changes but that quantitatively or qualitatively fall short of a definitive diagnosis of LSIL.8 The cellular changes in this category may represent a reactive/reparative/benign change or a more serious lesion; however, they cannot be unequivocally classified by the pathologists, and are thus interpreted to be of undetermined significance. The cellular changes include nuclear enlargement to two and half to three times that of a normal intermediate squamous cell nucleus in the vast majority (90–95%) of cases,8, 51 a slightly increased nuclear-cytoplasmic ratio; with possible variation in nuclear size and shape, and binucleation (Fig. 18). The nuclei may also show mild hyperchromasia, but the chromatin remains evenly distributed without granularity and nuclear outlines usually are smooth and regular.8 Rare cells with clear perinuclear halo with a peripheral rim of thickened cytoplasm, and slight nuclear enlargement and slight nuclear hyperchromasia are also classified as ASCUS (Fig. 18). Cytoplasmic vacuolization alone, without any nuclear atypia, is considered to be a benign cellular change and should not be classified as LSIL or ASCUS.8 The differential diagnosis is most often between benign reactive changes versus LSIL. TBS also encourages pathologists to qualify ASCUS as to whether a reactive process or SIL is favored,8 however in actual practice, a large number of these cases are reported as ASCUS, not otherwise specified (ASCUS-NOS).7, 8
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Parakeratotic cells shed singly or in three-dimensional clusters that demonstrate cellular pleomorphism (caudate or elongate shapes) and/or increased nuclear size and/or hyperchromasia should be categorized as ASCUS (atypical parakeratosis) or SIL depending on the degree of the cellular/nuclear abnormalities (Fig. 19).8
{kind=link}
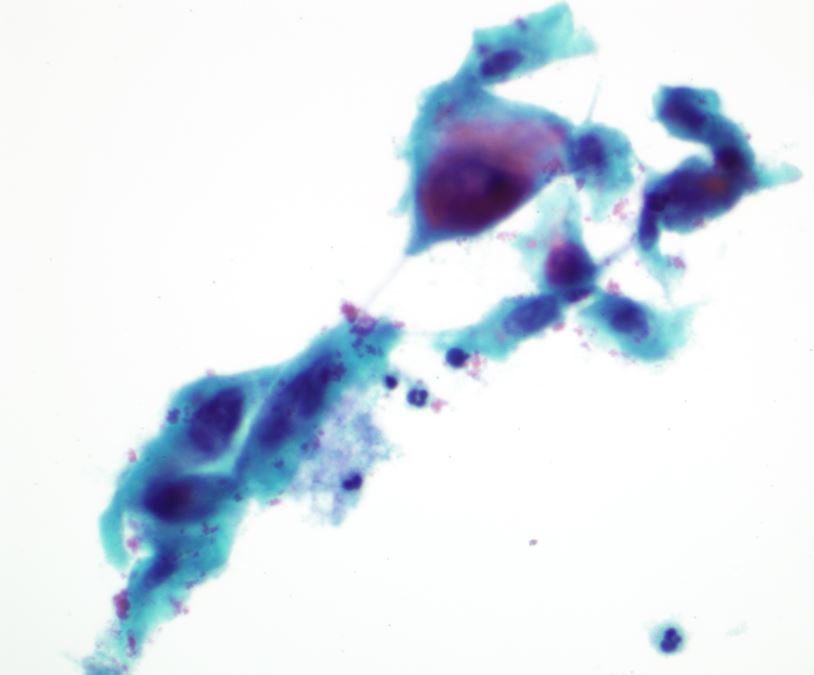
Marked cellular changes involving tissue fragments, or sheets of immature squamous cells, so-called atypical repair, also are included in the ASC category, but present a different cytologic picture (Fig. 20). In typical repair, cells occur primarily in monolayer sheets and syncytia and contain prominent nucleoli. However, nuclear piling, significant anisonucleosis, and irregularities in chromatin distribution that exceed changes seen in typical repair are considered to be ASCUS.8 The differential diagnosis is between exuberant reparative processes versus invasive carcinoma; however, typical repair lacks both a tumor diathesis and isolated abnormal cells seen in squamous cell carcinoma.
{kind=link}
A variety of reactive/degenerative cellular changes, such as degeneration, autolysis, etc., may be seen in an atrophic smear and occasionally they can mimic HSIL or squamous carcinoma. A diagnosis of ASCUS associated with atrophy should be considered if cells demonstrate: nuclear enlargement (at least two times normal), significant hyperchromasia, nuclear chromatin or membrane abnormalities, or marked pleomorphism in the form of tadpole or spindle cells.8
The subtle and subjective findings in specimens with ASC have resulted in poor reproducibility, compounding the difficulty in developing and illustrating strict criteria. In order for laboratories not to overuse this term, it is suggested that the frequency of ASCUS diagnoses should not exceed two to three times the rate of SIL in the same laboratory.8
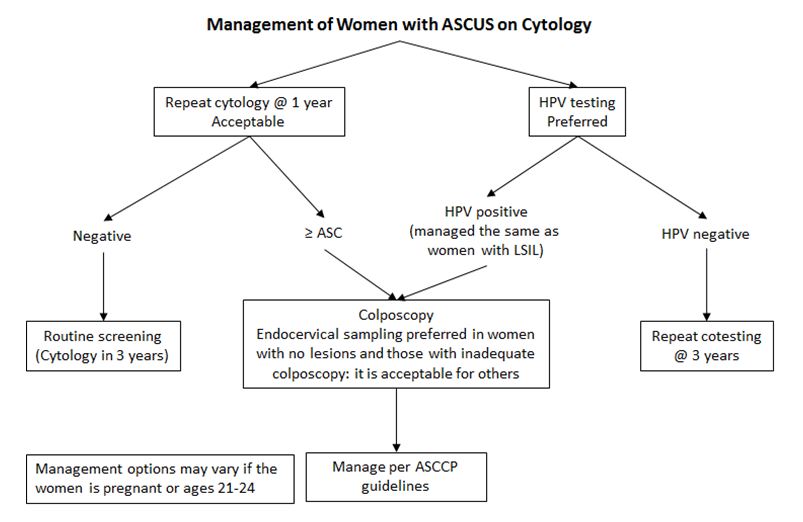
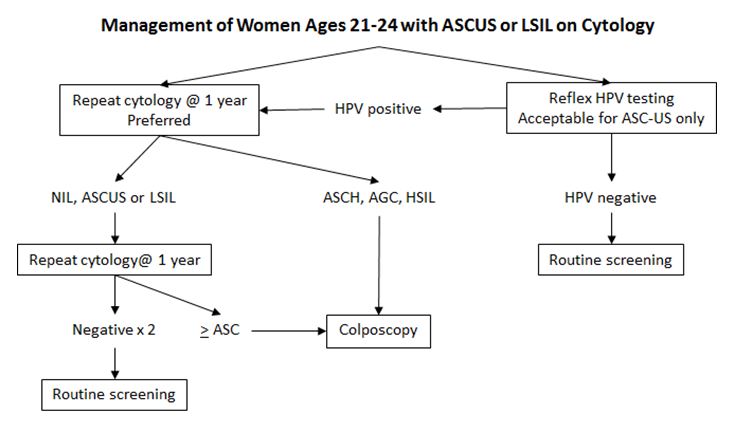
The 2012 ASCCP has published consensus guidelines for the management of women with ASCUS cytology (Fig. 21A and B).28, 29, 48 HPV testing is preferred, and repeat of cytology at 1 year is also acceptable (Fig. 21A). For patient ages 21–24, repeat of cytology at 1 year is preferred, and reflex HPV testing is acceptable (Fig. 21B). Further management depends on testing results.
{kind=link}
{kind=link}
Atypical squamous cells: cannot exclude high-grade squamous intraepithelial lesions (ASC-H)
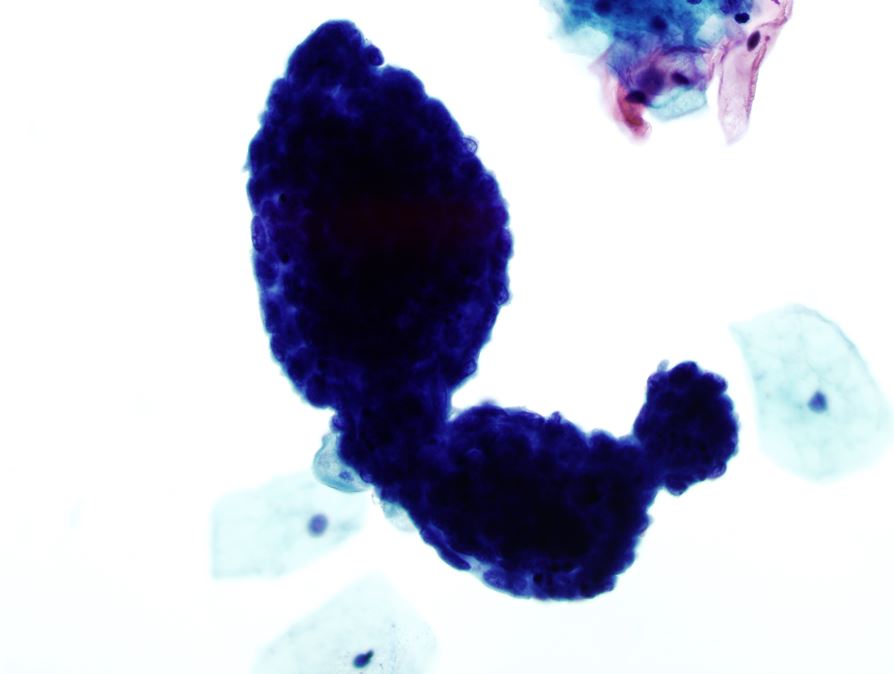
In a smaller number of ASC cases, 5–10% of all ASC, the atypical changes occur in less mature squamous metaplastic cells, previously called atypical metaplasia.7, 8 This category is classified as ASC-H, and reflects HSIL versus its imitators. Several patterns may be present within this category including atypical immature metaplastic cells, crowded sheets of cells, markedly atypical repair, severe atrophy, and postradiation changes that are concerning for recurrent or residual carcinoma. Nuclear enlargement approximates one and a half to two times the area of a mature squamous metaplastic nucleus, or three times the area of a normal squamous intermediate-cell nucleus (Fig. 22). In these cases, the differential diagnosis is between immature squamous metaplasia and HSIL; LSIL is not a diagnostic consideration.8
{kind=link}
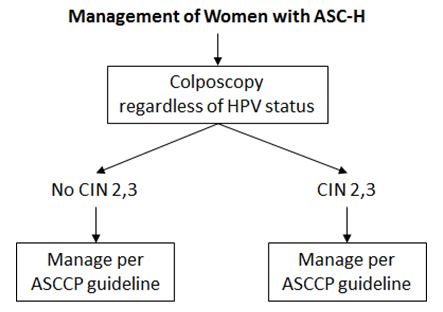
While there is interpreter variability in making the diagnosis of ASC, even among expert cytopathologists,52 studies suggest that ASC-H has a positive predictive value for histologic CIN II/III that is intermediate between ASC-US and HSIL. A woman with ASC-US has a 5–17% chance of having CIN II/III confirmed by biopsy, while CIN II/III is identified in 24–94% of those with ASC-H.51, 53, 54 The 2012 ASCCP guidelines recommend that management for women with ASC-H is referral for colposcopic evaluation (Fig. 23A).28, 29, 48 There is no role for HPV testing or repeat cytology. If no lesion is identified after colposcopic examination and sampling, a review of cytology, colposcopy, and histology results should be performed. If no CIN 2,3 lesions are identified in women ages 21–24 years with cytologic ASC-H and HSIL, the women should be followed by colposcopy and cytology at 6 month intervals for up to 2 years (Fig. 23B).
{kind=link}
{kind=link}
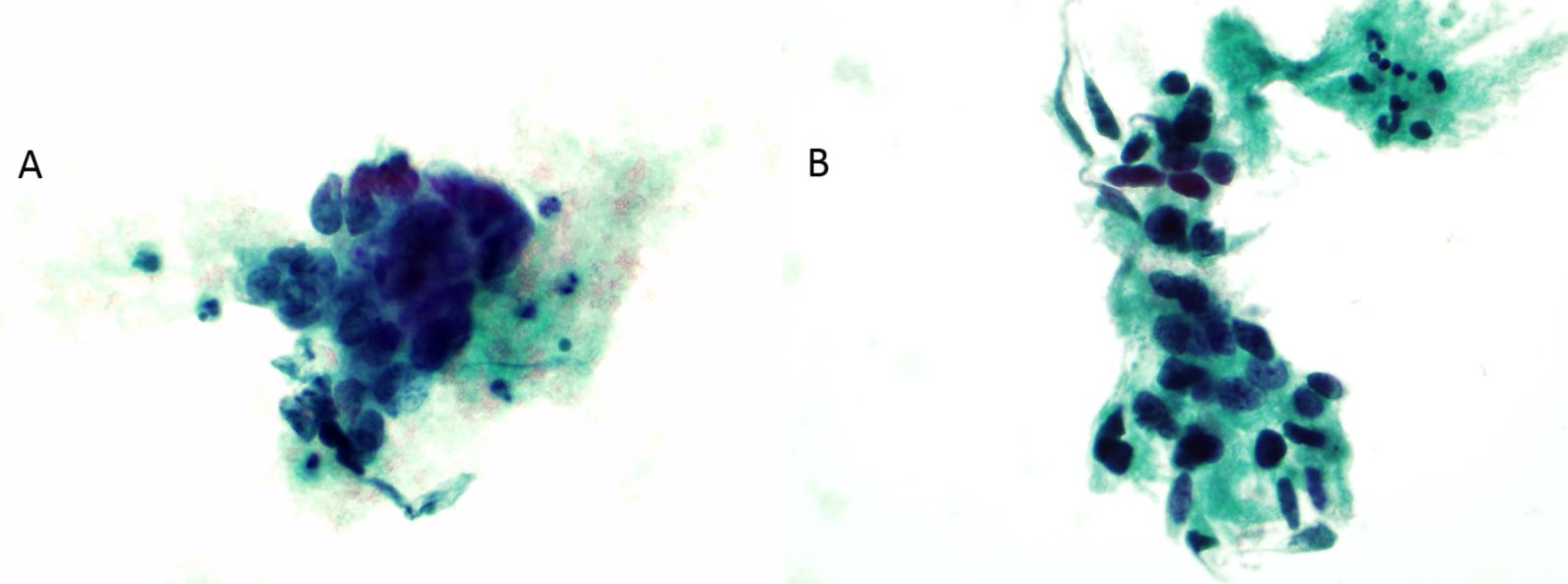
Low-grade squamous intraepithelial lesion (LSIL)
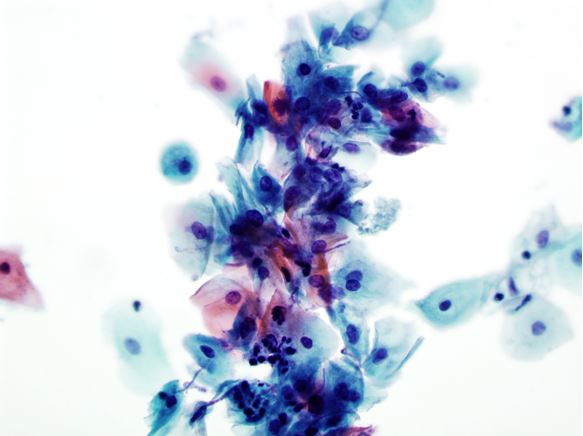
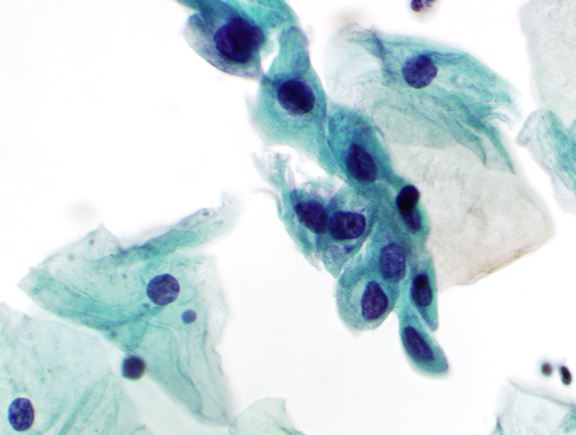
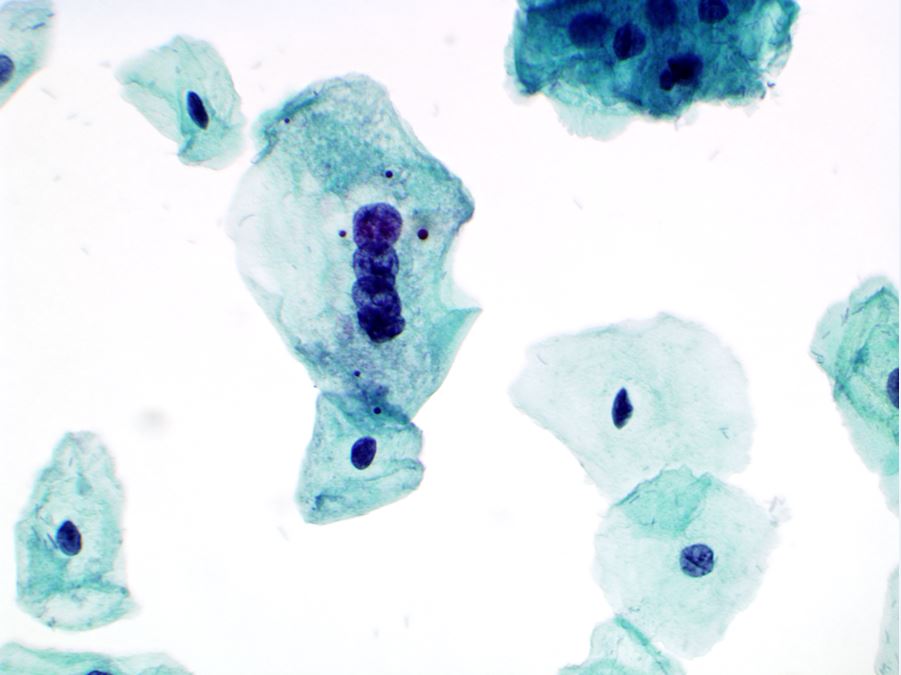
On histology, mild dysplasia is diagnosed when the lower one-third of the squamous epithelium does not show an adequate degree of differentiation. Corresponding cytologic samples show abnormal cells with mature or superficial-type cytoplasm.8 In LSIL, nuclear enlargement is at least three times the size of a normal intermediate cell nucleus. Although the nucleus is hyperchromatic, the chromatin is distributed uniformly or it may appear degenerated and smudged if associated with cytopathic changes induced by HPV (Fig. 24A). Squamous cells with cytologic features diagnostic of HPV cytopathic effect (koilocytes), are also interpreted as LSIL on cytologic smears (Fig. 24B). In these cases, the nucleus may not be enlarged, but is usually hyperchromatic and “wrinkled”, and the cells have a well-defined, clear, perinuclear cavity with a peripheral rim of thickened cytoplasm.
{kind=link}
{kind=link}
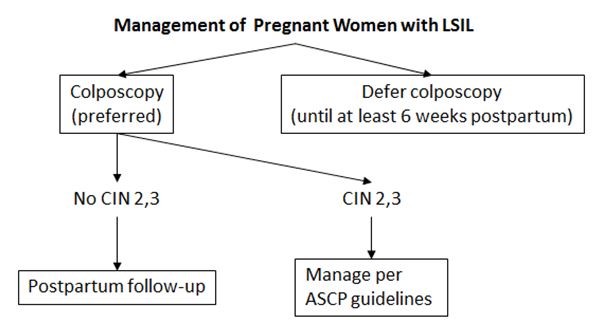
Most LSIL, especially in young women, will regress as a result of self-limited HPV infections;54, 55 however, approximately 15–30% of women with LSIL on cervical cytology will have CIN II/III on a subsequent cervical biopsy. The ALTS trial has shown that HPV DNA testing is not useful in triaging women with LSIL because 83% were positive for HPV.51 2012 ASCCP guidelines currently recommend colposcopy as the preferred management for women with LSIL and with either no HPV test or positive HPV test (Fig. 25A).28, 29, 48 For women with LSIL and negative HPV test, repeat cotest at 1 year is preferred, while colposcopy is also acceptable. Subsequent management will depend on whether a lesion is identified, whether the colposcopy is satisfactory, whether the woman is pregnant, and the repeat cotest results. For women aged 21–24 years with LSIL, the recommendation is the same as those women with ASCUS (Fig. 21B). Colposcopy is also preferred for pregnant women with LSIL, while colposcopy can be deferred until at least 6 weeks postpartum (Fig. 25B). Special recommendations for postmenopausal women, adolescents, and pregnant women are also outlined in the ASCCP consensus publication.
{kind=link}
{kind=link}
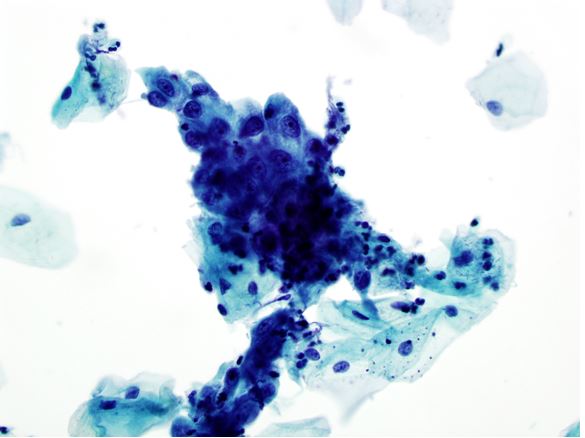
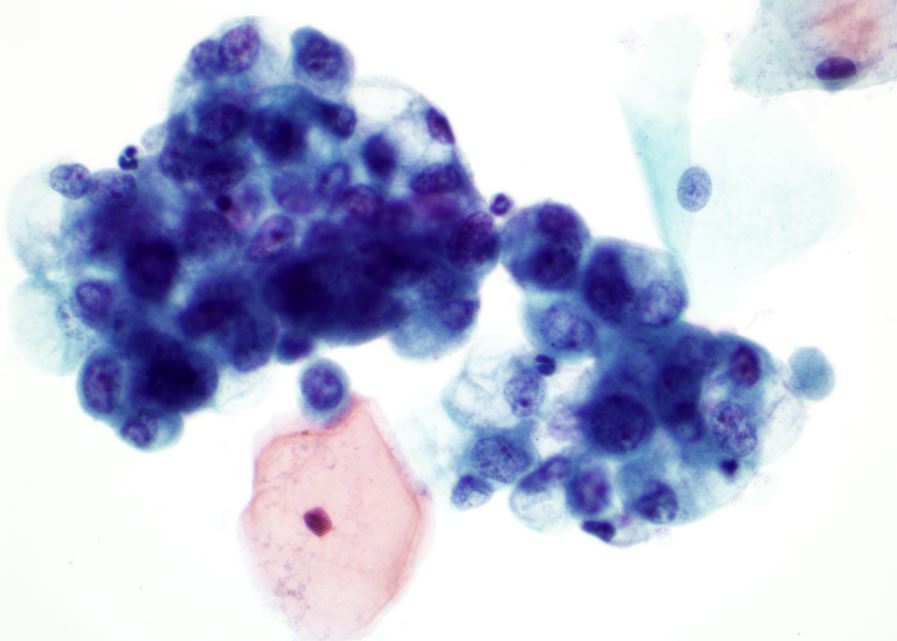
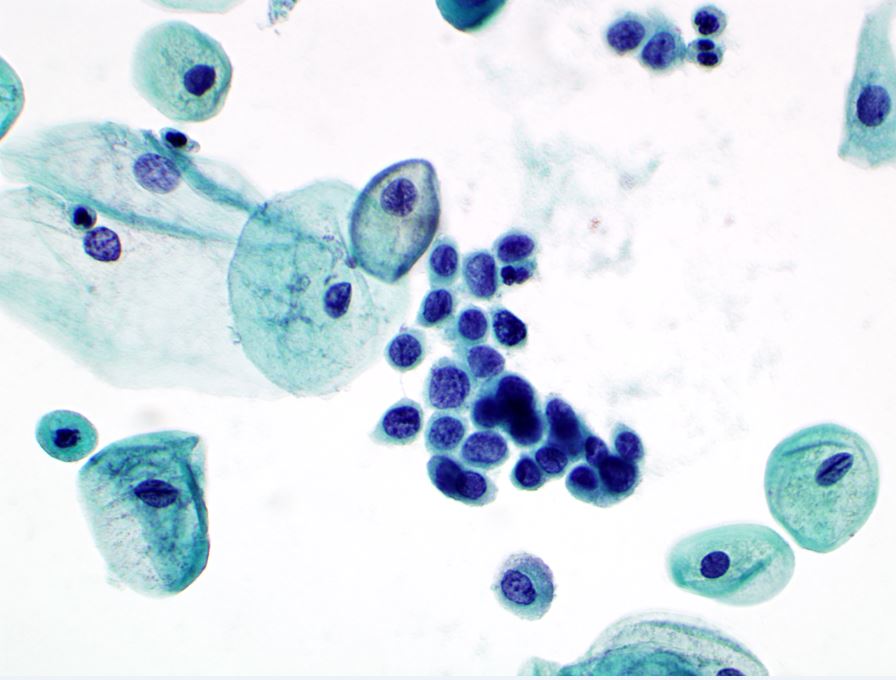
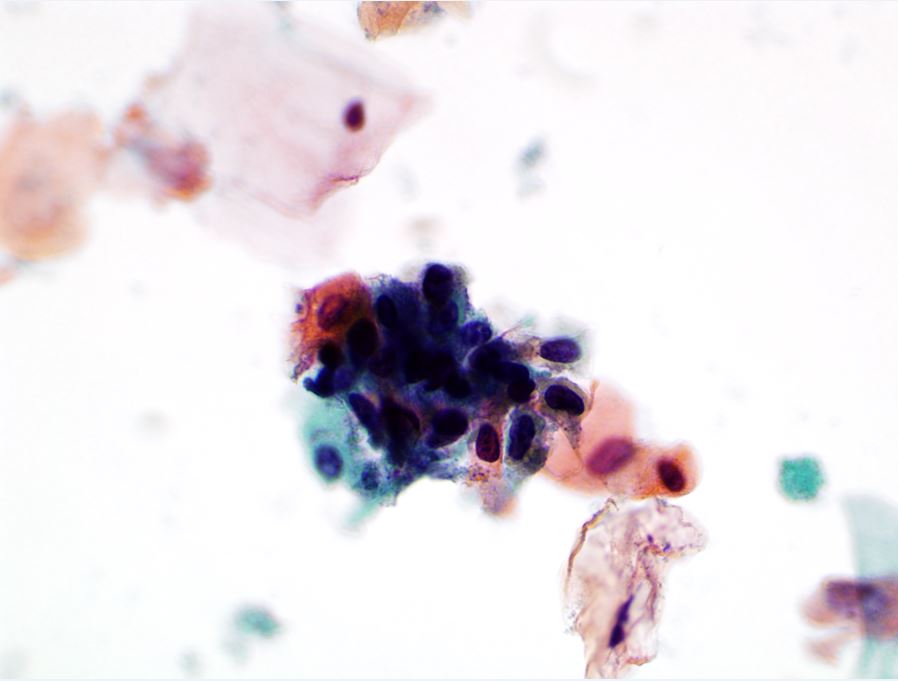
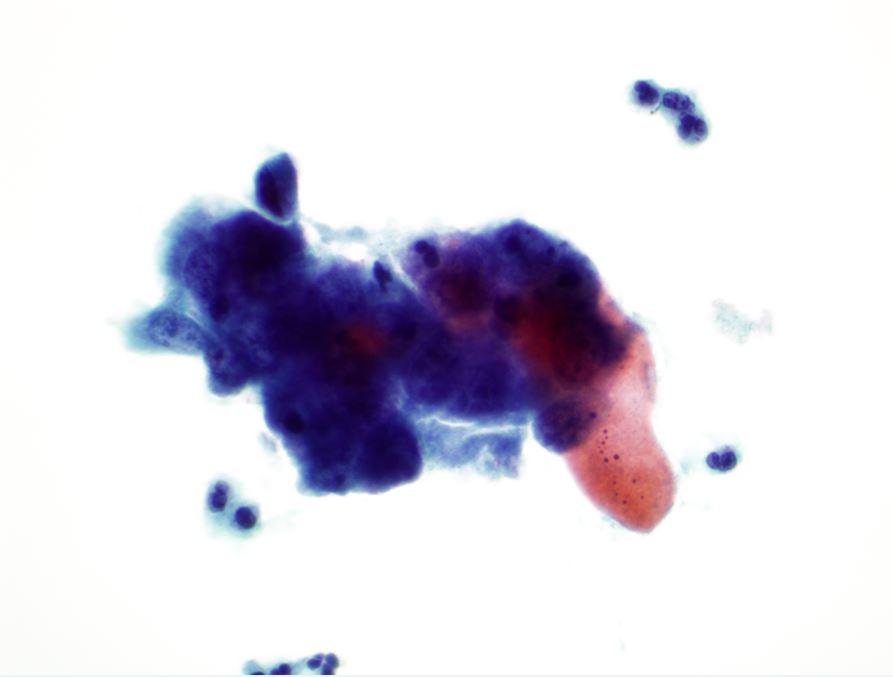
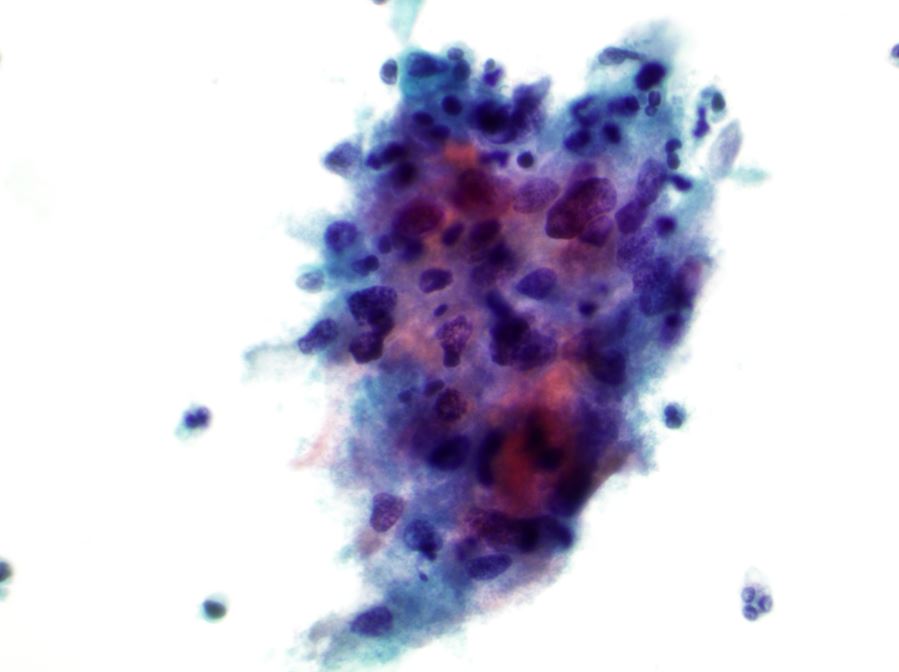
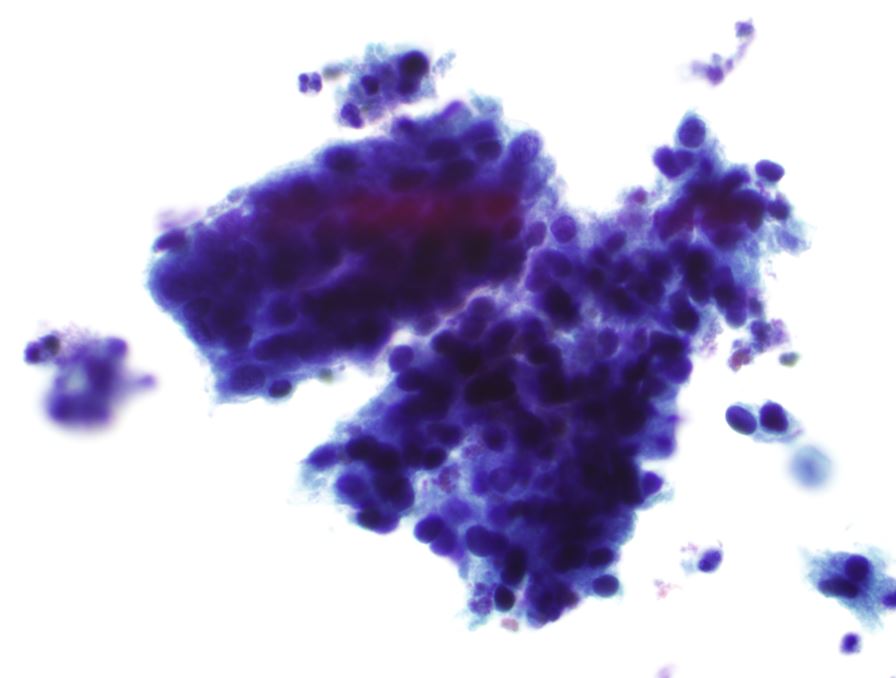
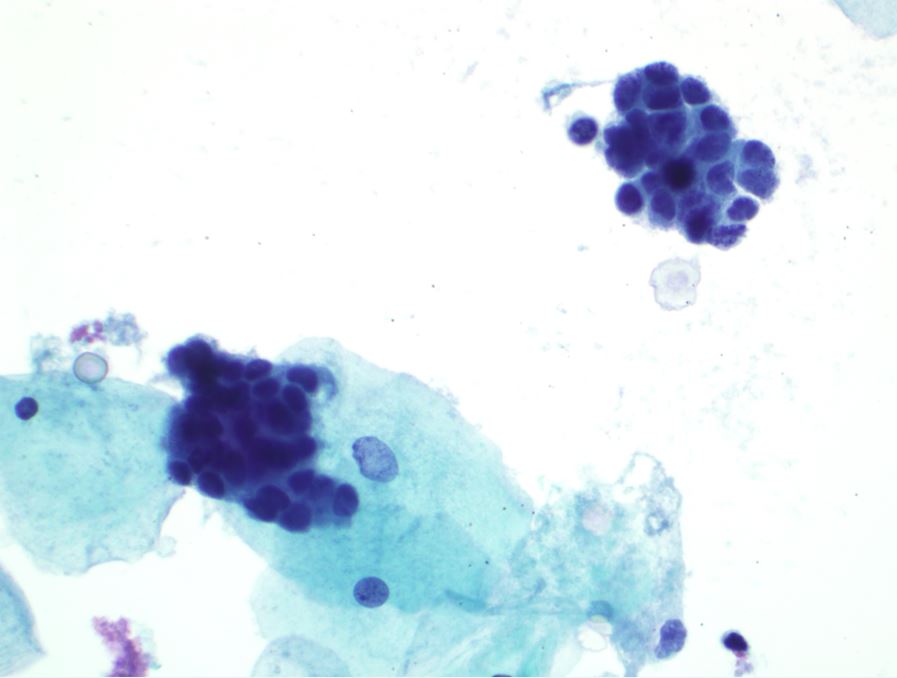
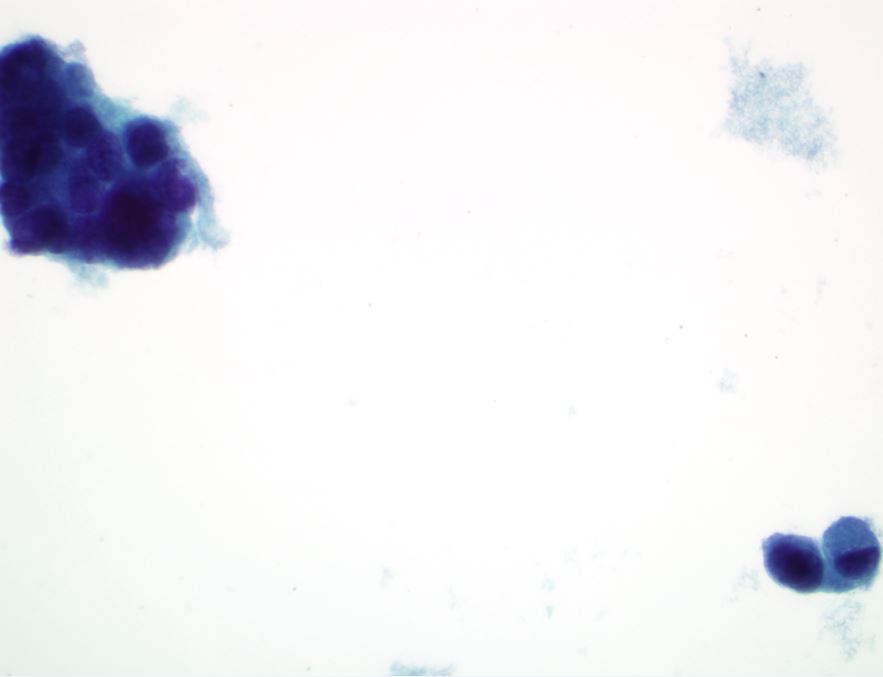
High-grade squamous intraepithelial lesion (HSIL)
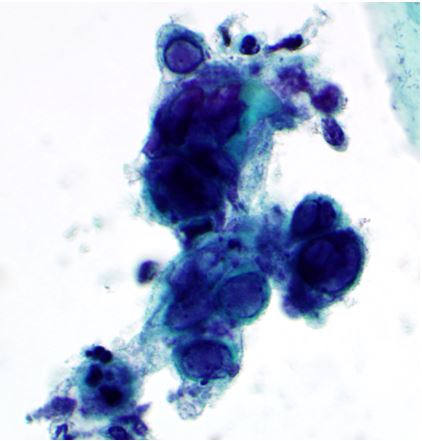
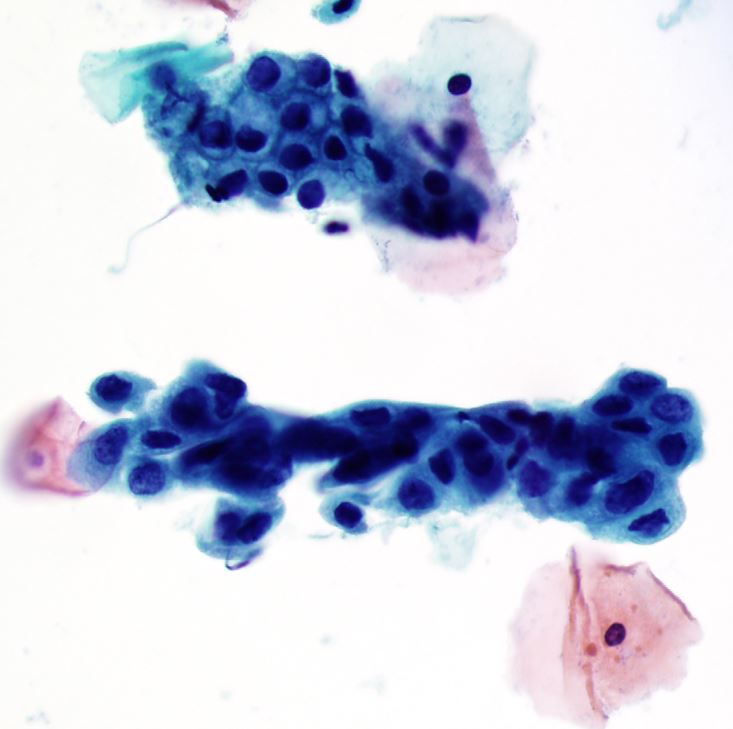
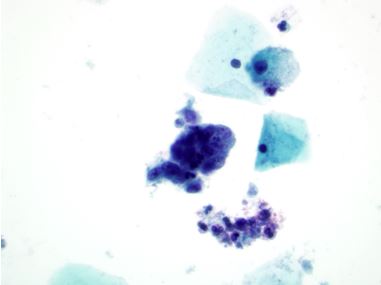
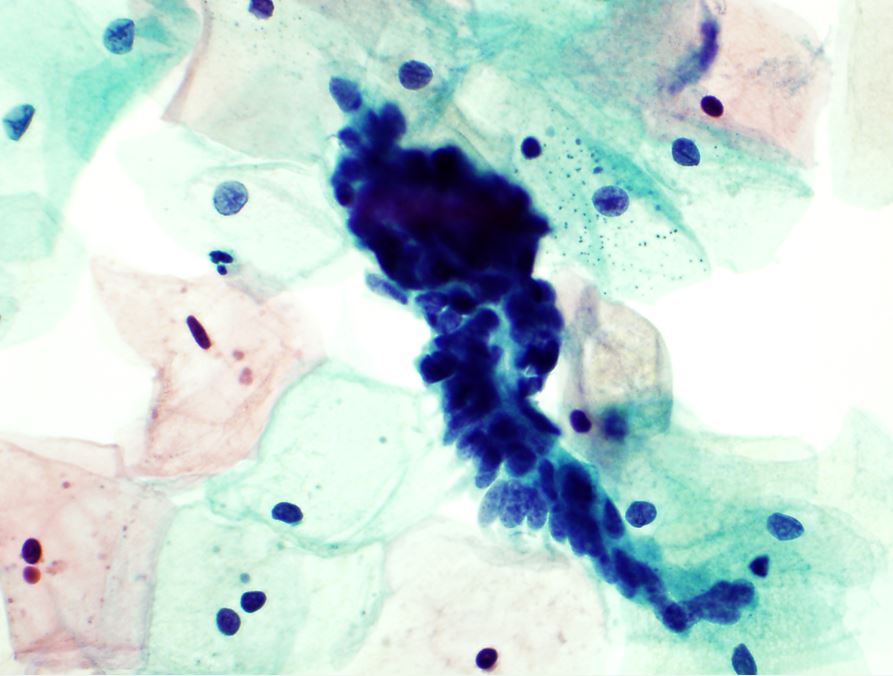
HSIL encompasses moderate and severe dysplasia/CIS which shows immature cells involve middle and upper thirds of squamous mucosa.8 Cytologically HSIL shows cells with less cytoplasm, larger, hyperchromatic nuclei containing granular or coarse chromatin, occasionally with asymmetrical nuclear outlines, and high nuclear to cytoplasmic ratio (Fig. 26A). The abnormal cells can be seen singly or in crowded, dark sheets/groups. HSIL may involve endocervical glands, in which prominent nucleoli may be seen (Fig. 26B). At times it may not be possible to exclude the possibility of invasive carcinoma and in such cases, the terminology for reporting this finding is “HSIL, with features suspicious for invasion.” The incidence of CIN II/III is estimated to be approximately four times that of invasive carcinoma.
{kind=link}
{kind=link}
{kind=link}
Features that favor a HSIL include higher nuclear/cytoplasmic ratios, greater irregularities in the outline of the nuclear envelope, coarsening of nuclear chromatin, and chromatin clumping. Cell size, overall is smaller in HSIL as compared to LSIL. The appearance of the cytoplasm is usually different in LSIL and HSIL cases. LSIL typically involves squamous cells with mature, intermediate, or superficial-type cytoplasm with well-defined polygonal cell borders, whereas cells from a HSIL have a more immature type of cytoplasm that can be lacy and delicate or dense/metaplastic, with rounded cell borders.8 When it is not possible to grade a SIL as low or high grade, a diagnosis of “SIL, grade cannot be determined” or “LSIL, cannot exclude HSIL or HSIL in a background of LSIL” can be rendered on the cervical smear. These patients should under colposcopy/biopsy.8, 53
2012 ASCCP guidelines recommend immediate loop electrosurgical excision procedure (LEEP) or colposcopy with endocervical assessment for women with HSIL (Fig. 27). Colposcopy is recommended for women aged 21–24 with HSIL-like ASC-H (Fig. 23B). If no CIN2,3 lesions are identified in women ages 21–24 years with cytologic ASC-H and HSIL, the women should be followed by colposcopy and cytology at 6 month intervals for up to 2 years.
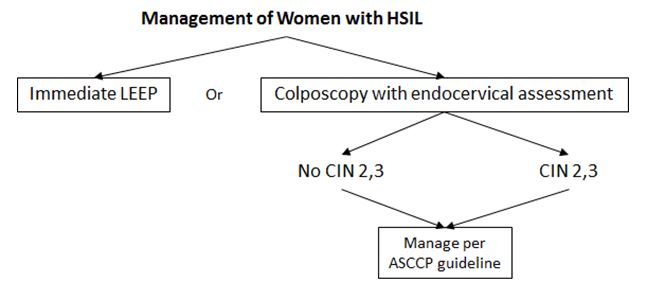{kind=link}
Progression and regression of squamous intraepithelial neoplasia
Spontaneous regression of ASCUS occurs with great frequency (68%),56, 57 LSIL regresses in 47% or more,43, 55, 56 and HSIL regresses in approximately 35–40% of cases.56 Most LSILs regress to normal or ASCUS within 6 months. Most severely abnormal lesions are destroyed by a variety of modalities of treatment. Only a small fraction of all dysplasias, left untreated, would progress to invasive cancer, but the risk increases with increasing grade of the lesion (7–10% for ASCUS, 15–21% for LSIL, and 23% for HSIL).56 Overall, precursor lesions of the cervix persist longer and progress more quickly in women with oncogenic HPV infections than in women without HPV.57 Average time of progression from ASCUS to LSIL or worse is shorter in women with no HPV infection (67.0 months) as compared to oncogenic HPV positive women (88.0 months).57 Average time of progression from LSIL to HSIL or worse is similarly shorter in women with no HPV infection (73.3 months) as compared to oncogenic HPV positive women (83.5 months).
Intraepithelial neoplasia in pregnancy
During the first trimester of pregnancy, dysplastic cells are smaller than in non-pregnant patients, thus giving the false impression of a higher grade of abnormality.58, 59 In the late stages of pregnancy, the size of the cells is comparable to the non-gravid population. The biologic growth rate is similar to that of the general population. Most cases of LSIL regress or remain stable during pregnancy.60 All cases of HSIL diagnosed antepartum persisted in the postpartum period, and 11% of patients with antepartum HSILs are found to have invasion noted 2–5 years after diagnosis of SIL in the antepartum. The possibility of undetected intraepithelial lesions may be higher than in non-pregnant patients because of a larger number of unsatisfactory smears.35 The 2012 ASCCP guidelines have specific recommendations for pregnant women with cytology abnormalities as discussed above.28, 29, 48
Squamous cell carcinoma
Invasive squamous cell carcinoma is the most common malignant neoplasm of the uterine cervix. The 2014 WHO terminology defines squamous cell carcinoma as “an invasive epithelial tumor composed of squamous cells of varying degrees of differentiation” and classifies squamous cell carcinoma into keratinizing, non-keratinizing, papillary, basaloid, warty, verrucous, squamo-transitional, and lymphoepithelioma-like categories.8, 61 These are histologic patterns that are often not distinct on cytologic specimens and the overall prognosis does not vary among the categories. Prognosis is more accurately defined predominantly by the stage of disease. The Bethesda System does not subdivide squamous cell carcinoma.8 Keratinizing squamous cell carcinoma usually presents as single cells and less commonly in cellular aggregates with variation in cell size and shape along with occasional spindle cells that contain characteristic orangeophilic cytoplasm (Fig. 28A and B). Marked nuclear size and membrane irregularity are present along with dense opaque nuclei. Chromatin is coarse and irregularly distributed, often with clearing. A tumor diathesis may also be present (Fig. 28C).8 Nonkeratinizing squamous cell carcinoma displays small single or aggregates of cells with poorly defined borders displaying cytologic features of HSIL (Fig. 28C).8 Nucleoli may be prominent and tumor diathesis is often present and can be a helpful diagnostic clue.
{kind=link}
{kind=link}
{kind=link}
Spindle squamous cell carcinoma is a poorly differentiated variant of squamous cell carcinoma characterized by pleomorphic, spindled, non-keratinizing cells. The differential considerations include sarcoma and malignant melanoma with spindle cell features.
GLANDULAR EPITHELIAL LESIONS
Current terminology for glandular lesions
The 2014 Bethesda System subclassifies glandular lesions into: (1) atypical, NOS; (2) atypical, favor neoplastic; (3) endocervical adenocarcinoma in situ; and (4) adenocarcinoma.8
Atypical glandular cells
Atypical glandular cells (AGC), whenever possible, should be categorized according to the site of origin, (endocervical or endometrial), as the clinical management for patients with glandular abnormalities may markedly differ depending upon the cell type. If it is not possible to confidently categorize cell type, the generic “atypical glandular cells/AGC” terminology is used. Further qualification “favor neoplastic” and “not otherwise specified/NOS” except in cases of endometrial cells, as reliable subclassification of this category is difficult.8 Initial management of all categories of AGC, with the exception of atypical endometrial cells, is colposcopy with adequate endocervical sampling.
Atypical endocervical cells (NOS or specify in comments) – At least 10 well-preserved endocervical or squamous metaplastic cells should be observed to report that a transformation zone component is present. The benign endocervical cells are present singly, in strips or in ”honeycomb” sheets, and columnar mucinous cells with basally located small round nuclei (Fig. 29).
{kind=link}
The diagnosis of atypical endocervical cells, NOS is rendered when endocervical cells display nuclear atypia that exceeds obvious reactive or reparative changes but lack unequivocal features of endocervical adenocarcinoma in situ or invasive adenocarcinoma.8 Atypical endocervical cells are arranged in sheets and strips with crowding, nuclear overlap, and pseudostratification. Atypical endocervical cells have enlarged nuclei varying in size and shapes, mild hyperchromasia, mild evenly distributed chromatin, slightly increased nuclear to cytoplasmic ratio (Fig. 30).
{kind=link}
Atypical endometrial cells (NOS or specify in comments) – Exfoliated endometrial cells are normal in a woman of reproductive age during menses and the proliferative phage (first 2 weeks of menstrual cycle). The finding of exfoliated endometrial cells should be reported in women over 45 years. In postmenopausal women, exfoliated endometrial cells are considered abnormal and raise the possibility of endometrial neoplasm. The cells are arranged in three-dimensional clusters, with some nuclei around the edge of clusters and showing double-contoured clusters (Fig. 31). The cells have a small nuclei similar in area to a normal intermediate squamous cell nucleus.8 The cytoplasm is scant with ill-defined cytoplasmic borders.
{kind=link}
The distinction of cytologically benign from atypical endometrial cells is based primarily on the criterion of increased in nuclear size.8 The cells are arranged in small groups, have slightly enlarged, mild hyperchromatic nuclei with chromatin heterogeneity, and have scant cytoplasm with occasional cytoplasmic vacuoles and will defined borders (Fig. 32).
{kind=link}
According to the 2012 ASCCP guidelines, women with diagnosis of atypical endocervical cells should be managed with colposcopy (with endocervical sampling) and endometrial sampling (Fig. 33).28, 29 Women with diagnosis of atypical endometrial cells should be managed with endometrial and endocervical sampling (Fig. 33).
{kind=link}
Atypical glandular cells, favor neoplastic
Atypical endocervical cells, favor neoplastic – The diagnosis of atypical endocervical cells, favor neoplastic is rendered when morphology of endocervical-like cells either quantitatively or qualitatively falls just short of an interpretation of endocervical adenocarcinoma in situ or is invasive adenocarcinoma.8
The abnormal endocervical-like cells are arranged in sheets, strips, glandular formation or feathering with nuclear crowding, or pseudostratification. The cells have enlarged and elongated, hyperchromatic nuclei with coarse chromatin, and increased nuclear to cytoplasmic ratio.8 Management of atypical endocervical cells, favor neoplastic is colposcopy.28, 29,
Endocervical adenocarcinoma in situ – Appropriate interpretation of endocervical adenocarcinoma in situ (AIS) should only be made when sufficient histologic criteria are present. An interpretation of “atypical endocervical/glandular cells, favor neoplastic” is appropriate to be used in cases where definitive evidence of carcinoma is difficult to assess.7, 8
Noninvasive high-grade endocervical glandular lesions are characterized by nuclear enlargement, hyperchromasia, chromatin abnormality, pseudostratification, and increased mitotic activity. Nuclear chromatin may be coarse or finely granular (Fig. 34).7 Cells may occur in sheets, clusters, pseudostratified strips, and rosettes with nuclear crowding and overlap, and loss of a well-defined honeycomb pattern. Architectural features of peripheral feathering, rosettes, and cell strips have a more subtle presentation.8 Most commonly the descriptive cytologic criteria described for AIS are for the endocervical form. Variant forms of AIS, although more uncommon, do exist. These include mucinous, intestinal, endometrioid, and clear cell, to name a few.62
{kind=link}
The management of AIS is colposcopy and adequate endocervical sampling (Fig. 33).28, 29, If histologic AIS is present on colposcopic biopsy, a total hysterectomy is the treatment of choice. If no evidence of invasive disease is identified, an excisional biopsy is recommended for further evaluation and clinical management.
Adenocarcinoma
Endocervical adenocarcinoma – Cytologic criteria for endocervical adenocarcinoma overlap significantly with those described previously for AIS, but adenocarcinoma may show additional features indicative of invasion.62 Typically abnormal cells are columnar cells that are present in single cells, two-dimensional sheets or three-dimensional clusters, and syncytial aggregates. Tumor cells display enlarged pleomorphic nuclei with irregular chromatin distribution, chromatin clearing, and often nuclear membrane irregularities. Cytoplasm is usually finely vacuolated. Abnormal squamous cells may also be present, representing a coexisting squamous lesion or perhaps the squamous component of an adenocarcinoma showing partial squamous differentiation.8 Mucinous carcinomas, including minimal deviation adenocarcinoma and well-differentiated mucinous adenocarcinoma (adenoma malignum), may be difficult to recognize in cytologic specimens.
{kind=link}
Adenoma malignum present cytologically with cells that closely resemble benign endocervical cells arranged in clusters, strips or large sheets, and few isolated cells. Cells are pseudostratified, lose polarity and nuclear crowding, and display a disorganized “drunken honeycomb” arrangement. Ultimately it is a spectrum of atypical nuclear changes that clenches the diagnosis.8 Individual cells are cuboidal to columnar, have abundant golden-yellow vacuolated cytoplasm containing neutral gastric/pyloric type mucin or goblet cell differentiation, bland nuclear features, and have low nuclear to cytoplasmic ratios.63, 64 Tumor diathesis and background mucin are present in the background. All these features assist in making the correct interpretation.
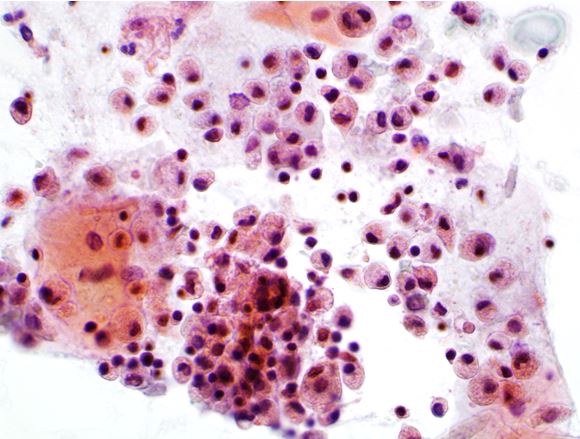
Endometrial adenocarcinoma – Endometrial adenocarcinoma typically displays cells occurring singly or in tight small clusters. In well-differentiated tumors, nuclei are slightly enlarged as compared to non-neoplastic endometrial cells. Nuclei typically become progressively larger with increasing tumor grade.8 Difficulty arises with low grade tumors as they tend to shed few abnormal cells with minimal cytologic atypia, these cases typically are interpreted as atypical endometrial cells. Cytologic findings include loss of nuclear polarity and variation in nuclear size with nuclei displaying hyperchromasia, irregular chromatin distribution, and chromatin clearing most notable in high-grade tumors.65 Cytoplasm is typically scant, cyanophilic, and often vacuolated. Isolated cells or small groups of tumor cells may show intracytoplasmic neutrophils.65 A finely granular tumor diathesis is occasionally observed and when present is a helpful diagnostic feature. High-grade endometrial serous carcinomas morphologically resemble their ovarian counterpart with features including fragmented papillary architecture and large cells displaying marked pleomorphism and prominent nucleoli.8
{kind=link}
OTHER MALIGNANT NEOPLASMS, SPECIFY THE NEOPLASMS
Malignant neoplasms, aside from squamous cell carcinoma and adenocarcinoma, do not routinely involve the uterine cervix.66 Often these malignancies are part of a larger diffusely metastatic disease process. Metastatic tumors to the uterine cervix are seen rarely, owing to the nature of the lymphatic drainage and low vascularity of the cervix.67 However, when present, tumor cells involve cervical sampling as exfoliated cells, or via direct sampling of tumors that involve the cervix or vagina by direct extension. Recognition of a limited rare number of tumors may help decrease the potential for misinterpretation.
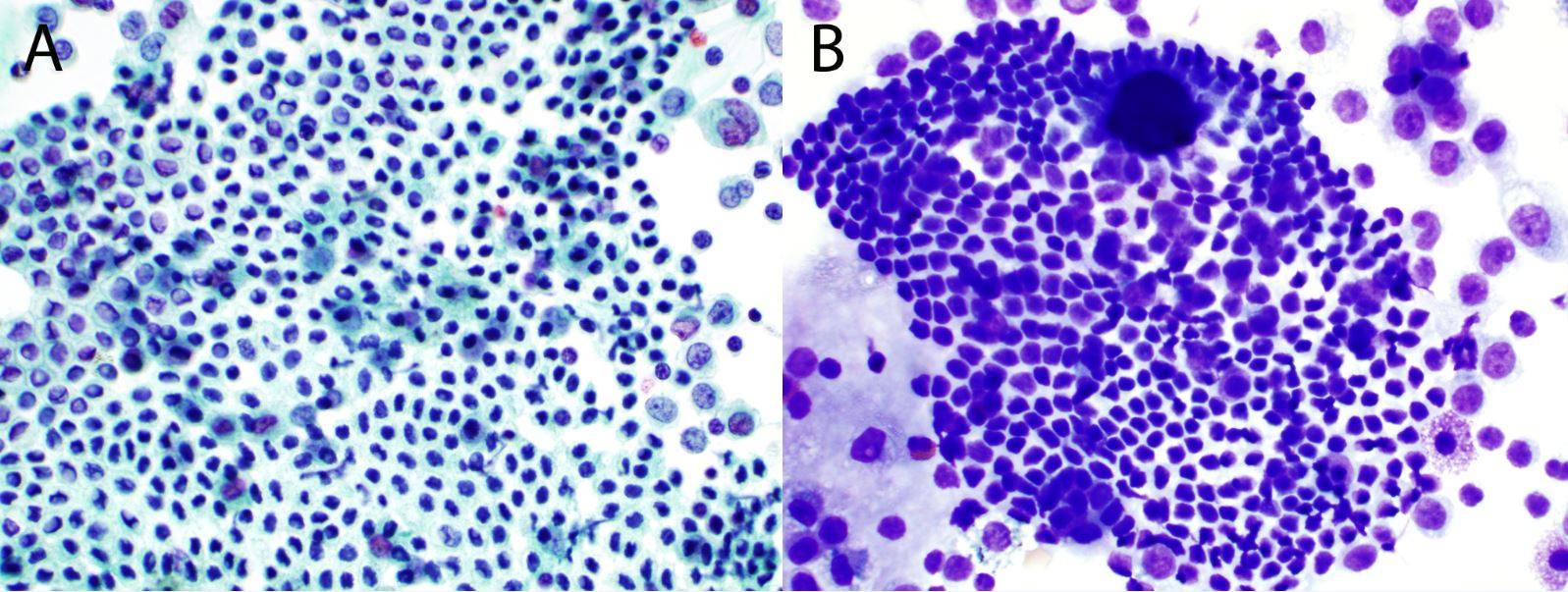
Small cell carcinoma
Small cell carcinoma consists of uniform small cells with scant cytoplasm seen singly and in loosely cohesive groups with nuclear molding and crush artifact (Fig. 37). The nuclei are angulated and hyperchromatic with granular chromatin and inconspicuous nucleoli. Background necrosis and mitotic figures are common and helpful features. Small cell carcinoma of the cervix is strongly associated with HPV 16 and 18, an association not found at other primary sites throughout the body. Poorly differentiated squamous carcinoma with small cells morphologically resembles a high-grade squamous intraepithelial lesion and may be confused with neuroendocrine/small cell carcinoma.8 These cells have less crush artifact than those of small cell carcinoma along with more cytoplasm, greater cytoplasmic density, better definition of cell borders, and coarsely granular chromatin.68
{kind=link}
Clear cell carcinoma
Clear cell adenocarcinoma of the cervix is a rare tumor that occurs most commonly in daughters of women who received diethylstilbestrol during pregnancy. Cervical cytology specimens show sheets of cells arranged in clusters or papillae with cells containing delicate, vacuolated, glycogen-rich cytoplasm, naked nuclei within a “tigroid” background. The nuclei are large, pale, and round with prominent nucleoli.69 HPV has been detected in 40% of both DES- and non-DES-associated clear cell carcinomas cases.
Adenosquamous carcinoma
Glassy cell carcinoma of the cervix is a rare variant of poorly differentiated adenosquamous carcinoma, typically affecting younger patients and is associated with HPV types 18 and 16. Tumor cells are arranged in sheets and clusters and contain abundant “ground glass-like” cytoplasm and large pleomorphic nuclei with coarse irregular chromatin and distinctive prominent nucleoli.70
Carcinosarcoma/malignant Mullerian mixed tumor (MMMT)
Carcinosarcoma/MMMT is an uncommon, highly aggressive tumor that arises in the endometrium and may involve the cervix by polypoid extension into the lower uterine segment and cervical os. The tumor is composed of malignant epithelial and mesenchymal components, ultimately exfoliated malignant cells from the endometrium may yield malignant cells in a cervical cytology sample. The malignant epithelial component often resembles poorly differentiated endometrioid (most common), or other epithelial cells types including clear cell, and serous carcinoma (Fig. 38).8 Cytologic samplings are usually hypercellular and show high-grade malignant tumor cells.
{kind=link}
Sarcoma
Primary sarcomas of the female genital tract are rare and when present most commonly arise in the uterine corpus. Sarcomas may be pure or mixed with epithelial components and usually present with degenerated, sparse tumor cells in the cervical sample. Most pure sarcomas present with undifferentiated, pleomorphic, multinucleated, and/or bizarre cells that cannot be further subtyped.8 If present, characteristic cytologic features such as spindle or round blue cell cytomorphology may suggest the specific type of sarcoma and as always, immunohistochemistry may help further subcategorize the sarcoma if sufficient diagnostic material is present.61
Metastatic malignancies
Most patients with metastatic tumors involving a cervical sample have a history of a malignancy, only rarely is cervical involvement the initial disease manifestation. Extrauterine carcinomas may spread to the cervix, or be present in a cervical cell sample in multiple ways. The most common source of cervical involvement by secondary carcinoma is direct extension from pelvic tumor (bladder, rectum, endometrium). Lymphatic, hematogenous and exfoliated metastases from GI, lung, or breast sources to the cervix are much less frequent.68
Metastatic breast carcinoma shows cohesive cluster of gladular cells, possible showing a glandular or three-dimensional cell ball in ductal carcinoma, and single or linear strips of small cells with eccentric small nuclei and possible intracytoplasmic lumen in lobular carcinoma (Fig. 39).
{kind=link}
PERITONEAL WASHINGS
Peritoneal washing cytology performed during surgery or second-look laparoscopy for carcinoma is used by gynecologic oncologists for the management of patients with gynecologic malignancies, specifically ovarian and endometrial carcinomas.71, 72 It can also be used in cervical carcinoma, but is a relatively insensitive technique for detecting advanced cervical disease.73 The presence of malignant cells in serous effusions signifies spread of disease beyond the organ of origin, substages the neoplasm, and is associated with significant therapeutic and prognostic implications.
Cytology is more sensitive in detecting ovarian carcinoma in ascites than in peritoneal washings, as well as in patients with peritoneal metastasis greater than 0.5 cm. Accurate subclassification of neoplasms into benign and malignant types can be rendered in the peritoneal cytology specimens of most of the patients.
The malignant cells may be few in number and might be unrecognized among a large population of mesothelial cells and/or macrophages. The false-negative rate for cytology in serous effusions is believed to be approximately 20%.74 Other factors that contribute to the high false-negative rate include infrequent exfoliation of malignant cells, interpretative errors, and poor distribution of peritoneal washings. Mesothelial cells can also show reactive changes which can be misinterpreted as malignant cells. The false-positive rate of cytology in the evaluation of serous effusions has been reported to be as high as 4.5%,75 with the main reason for false-positive diagnosis being the misinterpretation of reactive mesothelial cells as malignant epithelial cells. As a positive peritoneal washing diagnosis leads to treatment with chemotherapy in many instances, diagnostic accuracy is critical.
Benign cells
BENIGN MESOTHELIAL CELLS
Peritoneal and abdominal cavity are lined with mesothelial cells. Mesothelial cells taken by force in washings are arranged in monolayers assuming a mosaic-like appearance. The nuclei are monomorphic, round or oval and possibly contain prominent nucleoli, and dense, double tour cytoplasm with “skirt” pattern (Fig. 40A). Intercellular space (window) is obviously observed. Hyperplasia of mesothelial cells may show papillary proliferation with Psammomatous calcification (Fig. 40B), differential of which includes papillary serous carcinoma of ovary or fallopian tube.67 They are commonly found in specimens obtained from patients with pelvic inflammatory disease. Reactive mesothelial cells show prominent nucleoli and possibly binucleation, which may mimic poorly differentiated carcinoma.
{kind=link}
{kind=link}
BENIGN GLANDULAR CELLS
The most important pitfall in the examination of peritoneal cytology specimens in women involves benign epithelial proliferations.52 To avoid erroneous readings, the cytopathologists should be familiar with the morphologic features of benign-reactive, low-grade tumors, and Müllerian inclusions and intraperitoneal chemotherapy effect.71, 75, 76 Müllerian inclusions are tubular or papillary fronds arranged in single layers and embedded in the uterine serosa, omentum, or pelvic lymph nodes.77, 78, 79 The epithelial component resembles the epithelium of the fallopian tubes, endometrium, or endocervix. These structures may shed clusters of cells in single rows surrounding Psammoma bodies. This feature is a common source of confusion, and these structures can easily be diagnosed as well-differentiated adenocarcinoma in peritoneal/pelvic washings by a less experienced cytopathologist.75, 76 These benign glandular cells are columnar cells that are present in strips or acinar pattern, have round or oval nuclei located at one pole, with evenly distributed granular nuclei and smooth nuclear membrane, and delicate or vacuolated cytoplasm (Fig. 41). Hemosiderin laden macrophages are seen in endometriosis (Fig. 41). Glandular cells from endosalpingiosis have cilia and ciliocytophthoria (Fig. 42). Glandular cells from endometriosis may mimic well-differentiated adenocarcinoma.
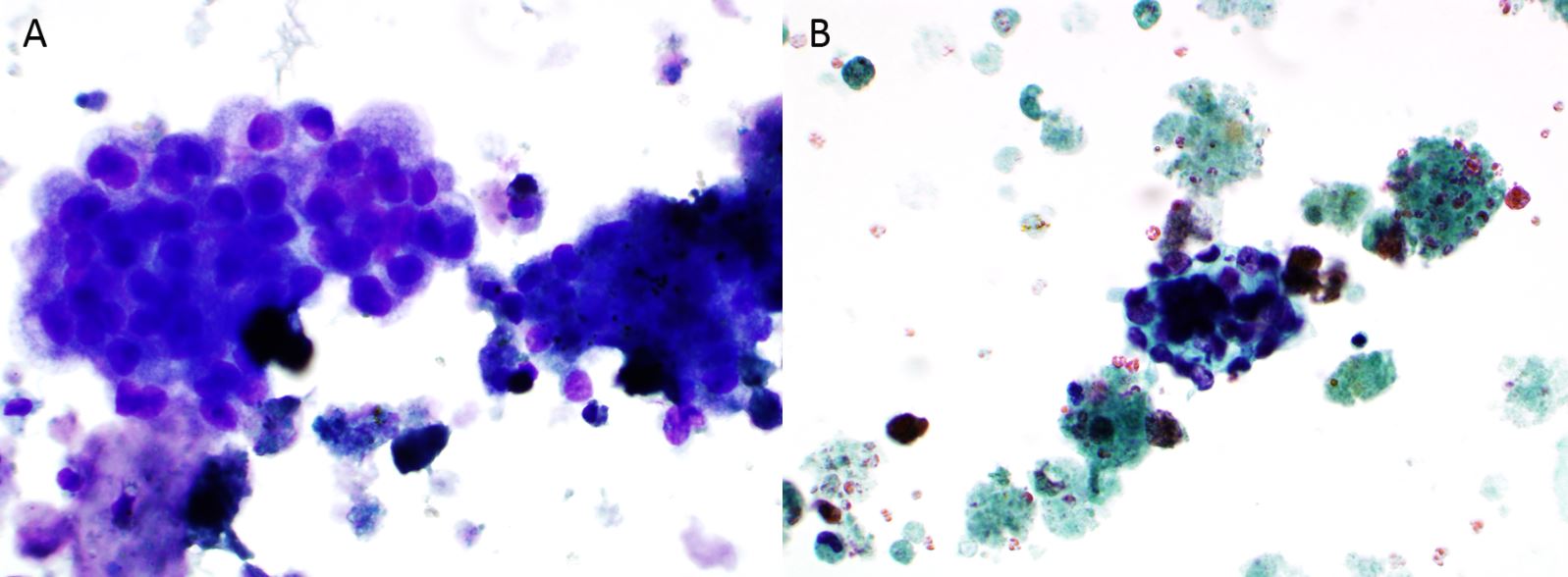{kind=link}
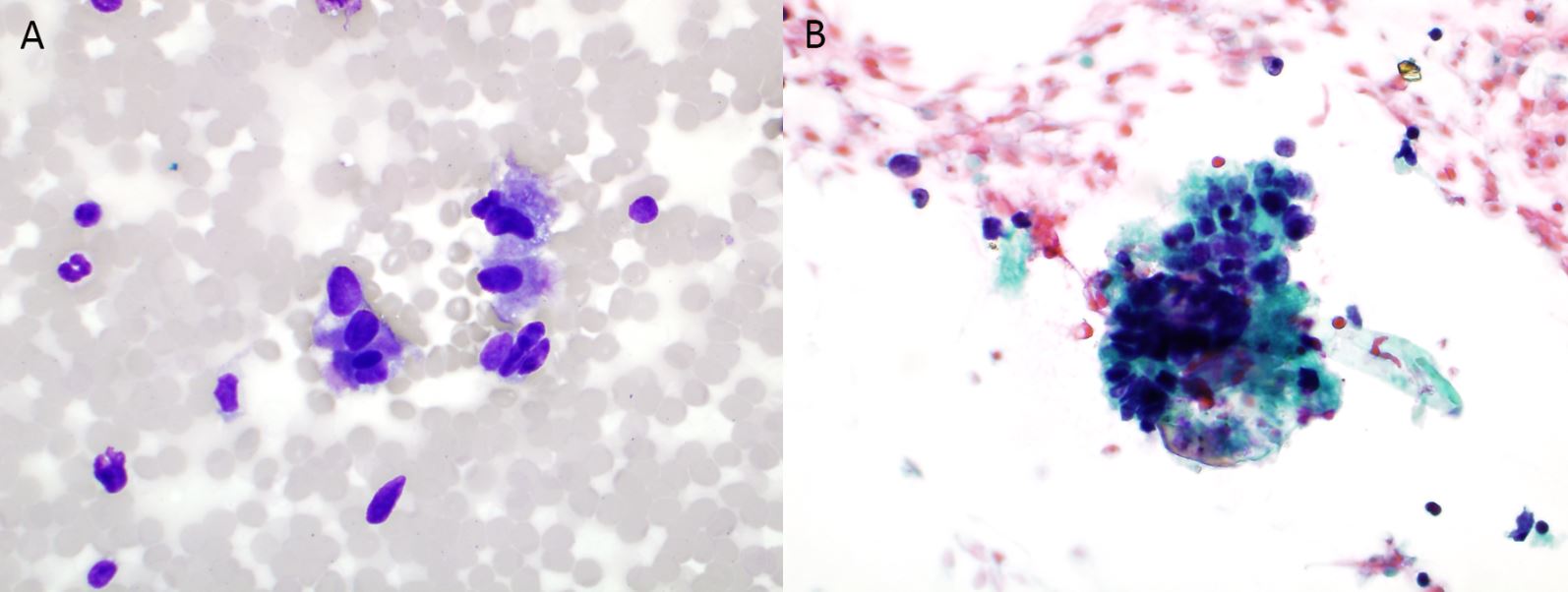{kind=link}
Malignant neoplasms
SEROUS TUMORS
A malignant finding on peritoneal washing in patients harboring ovarian carcinoma is of major importance for substaging this type of neoplasm, especially early ovarian cancer, where presence of malignant cells warrants assignment to stage IC or IIC and indicates a poorer prognosis.71 The most common ovarian tumor seen in peritoneal washing is serous neoplasm. The tumor cells are present singly or in papillary, acinar, nests or three-dimensional clusters (Fig. 43A and B). Most serous neoplasms are high grade and polygonal in shape, with prominent nucleoli, and dense or vacuolated cytoplasm. Psammomatous calcification may be seen. The differential includes papillary proliferation of mesothelial cells. The IHC performed on cellblock may help to distinguish serous tumor from mesothelial cells, as serous tumor is positive for PAX-8, ER, p53, BerEP4, and monoclonal CEA, while mesothelial cells are positive for calretinin and CK5/6 (Fig. 43C and D). Both serous tumor and mesothelial cells are positive for WT-1 and D2-40. The diagnosis of serous tumor is suitable in pelvic washing or peritoneal fluid cytology, to avoid using the term of high grade serous carcinoma before diagnosis of ovarian serous tumor.
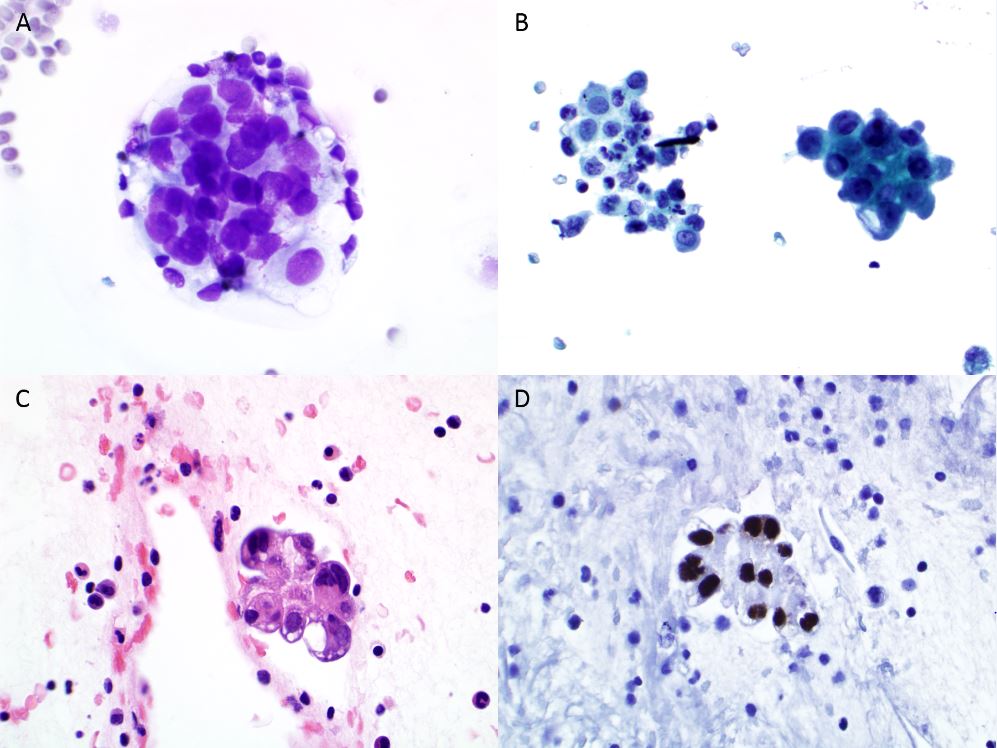{kind=link}
ENDOMETRIOID ADENOCARCINOMA
Between 5% and 15% of patients with endometrial carcinoma have positive peritoneal cytology, and this may be the only manifestation of extrauterine spread of the tumor and positive cytology upstages patients to IIIA. The literature regarding the significance of this spread has varied, with some studies reporting higher recurrence, and others noting lack of significance in predicting recurrence or death.72, 80, Some studies have shown that when disease is confined to the uterus, positive peritoneal cytology does not adversely affect prognosis.80, 81, However, the weight of evidence in larger studies with multivariate analysis, supports the presence of malignant cells in peritoneal washings of patients with endometrial carcinoma to be a significant predictor of poor prognosis in all disease stages.82
The malignant metastatic endometrial adenocarcinoma cells are morphologically different from mesothelial cells collected by saline washings during laparoscopy, laparotomy, or culdocentesis. The adenocarcinoma cells float in peritoneal effusions and acquire a globular or acinar appearance (Fig. 44A and B). The cells are columnar in shape, have moderate amount of delicate or vacuolated cytoplasm, and have round, hyperchromatic nuclei containing coarse chromatin and prominent nucleoli. In cell blocks of these washings, strips of mesothelial cells assume a coiled appearance during the centrifugation, mimicking papillary-like fronds and acinar-like formations suggestive of adenocarcinoma. Immunohistochemical stains can help to distinguish metastatic endometrioid adenocarcinoma from mesothelial cells. Endometrioid adenocarcinoma cells are positive for ER, PAX-8, BerEP4, B72.3, monoclonal CEA and MOC31, while mesothelial cells are positive for WT-1, calretinin, CK5/6 and D2-40.
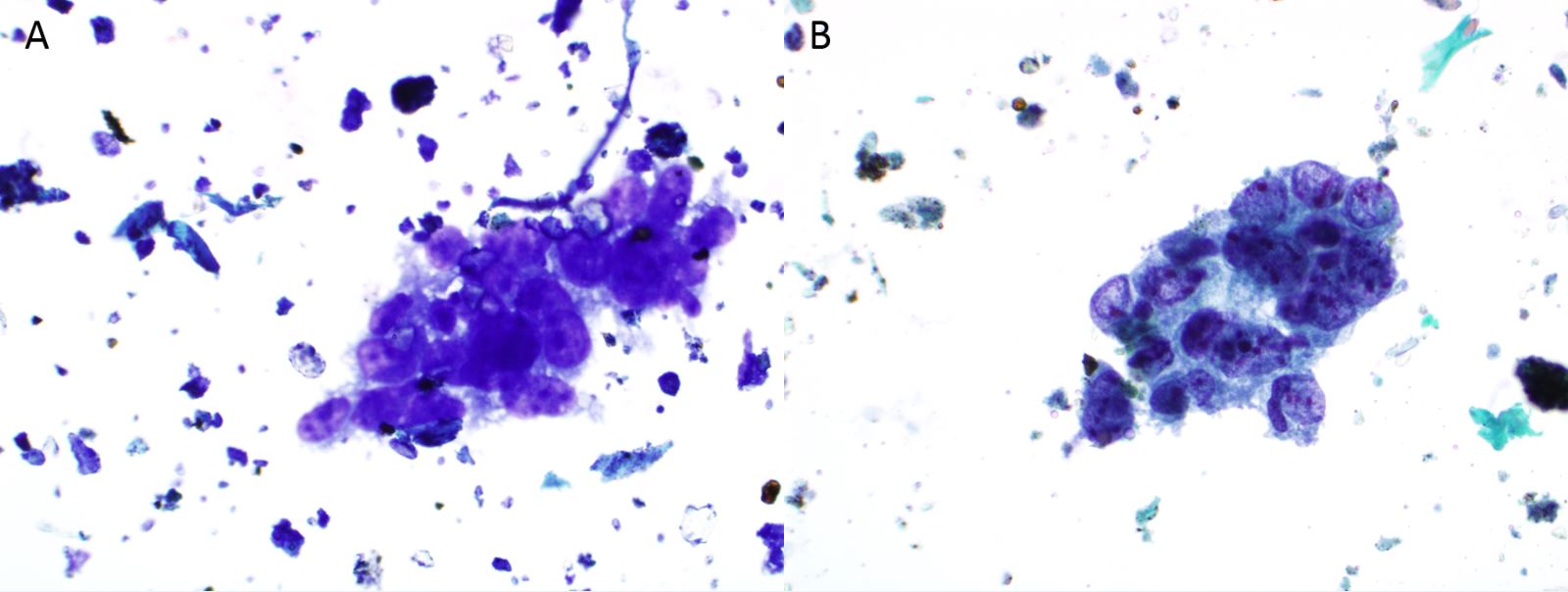{kind=link}
FINE-NEEDLE ASPIRATION OF THE OVARY
Fine needle aspiration (FNA) biopsy of the ovary is generally an uncommonly performed procedure as onco-gynecologists insist upon surgery in most cases. However, FNA can be useful in initial evaluation, prior to treatment, for evaluation of recurrent or metastatic tumors, for advanced inoperable tumors, or for more routine ovarian cysts and neoplasms. When both preservation of ovarian function in young women and assessment of the nature and spreading pattern of malignant tumors are necessary, FNA of ovarian neoplasms is indicated. It can also be used in workup of primary neoplasms, biopsy of superficial masses in patients with known prior disease, follow-up of irradiated patients, and follow-up of patients undergoing chemotherapy.83 FNA of ovarian tumors can be performed through the vagina, rectal mucosa, or percutaneously through the abdominal wall and guided by CT scan or ultrasound. FNA has an accuracy of approximately 90% and an overall low complication rate.84 Occasionally, infection was reported.
Aspiration of non-neoplastic ovarian cysts usually is performed in lesions that are up to 4–5 cm in diameter. Squamous cells and colonic cells from the vagina, rectum, and mesothelial cells are frequent components of the aspirate, which should be identified precisely, and not misdiagnosed as cells arising from a teratoma or mucinous neoplasm. Despite the potential disadvantages, FNA biopsy has an important role to play in the diagnosis and management of ovarian masses. When results are combined with radiological assessment of the nature of the tumor, FNA can serve as a highly efficient means of rapid diagnosis of ovarian neoplasms.
Nonneoplastic lesions
Nonneoplastic lesions comprise endometrioid, follicular, and corpus luteum cysts. Surface epithelial inclusions, paraovarian, and paratubal serous cysts yield clear fluid as well as degenerated epithelial cells. In aspirates, they are indistinguishable from one another, and clinical correlation is necessary to establish their precise nature.85
ENDOMETRIOID CYSTS AND ENDOMETRIOSIS
Aspirates of endometriosis contain hemosiderin-laden histiocytes and clusters of endometrial cells in varying stages of degeneration, seen against a background of debris (Fig. 41). Not all of these elements are consistently present in aspirates from patients with endometriosis. However, the presence of histiocytes and clinical suspicion by the gynecologist point toward this diagnosis. After multiple bleeding episodes, the epithelium may become hyperplastic and highly atypical, mimicking adenocarcinoma in cytology samples and possibly result in a false positive diagnosis. To compound the problem some types of uterine (papillary serous) and ovarian (clear-cell) adenocarcinomas can arise in association with endometriosis. Also the presence of extensive adhesions may also mimic ovarian neoplasia radiologically.
FOLLICULAR CYSTS AND CORPUS LUTEUM CYSTS
Most frequently, patients seek medical care because of menstrual disturbances related to increased estrogenic stimulation produced by these cysts. Aspiration of follicular cysts yields clusters and single cells with a high nuclear-cytoplasmic ratio and granular chromatin mimicking cells originating from neuroendocrine tumors (Fig. 45). Mitotic figures may be sparse or present in high numbers.86 Nuclear grooving also may be observed. The differential diagnosis with cystic granulosa cell tumors is based on the identification of Call-Exner bodies in granulosa cell tumor. Luteinized follicular cysts may show nuclear atypia in postpartum patients and also in young, cyclic patients. The cells have moderate granular cytoplasm.
{kind=link}
Fig. 45. Follicular cyst. FNA cytospin of the ovary (A: Diff-Quik stain, x600; B: Papanicolaou stain, x600; C Surgical resection, H&E stain, x600).
Aspiration of corpus luteum cysts may show luteinized cells (granulosa), which have abundant foamy or granular cytoplasm, and small, eccentric and oval or round nuclei (Fig. 46A and B). Atypia can be seen.
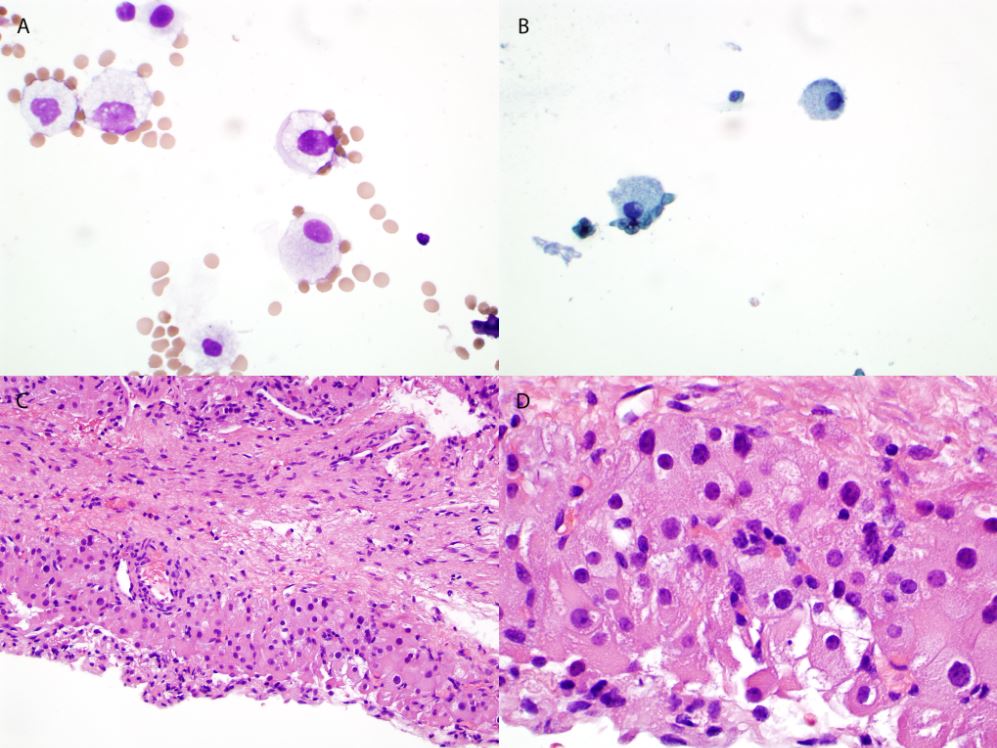{kind=link}
Neoplastic cysts
Serous, mucinous, endometrioid, and clear cell tumors of the ovary are for the most part cystic lesions in adults. The most common neoplasm is the serous type. FNA biopsy of neoplastic cysts is limited to tumors with adhesions to the pelvis, caused by malignant infiltration and tumors with known metastasis. Mobile cystic lesions larger than 4 cm usually are not aspirated because they may represent neoplastic processes that when punctured, may seed the pelvic peritoneum.
SEROUS TUMORS
Serous tumors are subclassified into benign serous cystadenoma, borderline serous tumor, and low grade or high grade serous carcinoma. FNAs of benign serous cystadenoma usually yield serous fluid and single or strips of cuboidal or columnar glandular cells (some with cilia) with basally located small round nuclei containing evenly distributed, granular chromatin, smooth nuclear membrane, and A scant to moderate amount of delicate or vacuolated cytoplasm, as well as ciliocytophthoria (Fig. 47). FNA cytology of borderline tumor or carcinoma shows pleomorphic columnar or polygonal cells arranged singly or in papillary, acinar or three-dimensional clusters, with hyperchromatic nuclei containing prominent nucleoli and irregular nuclear membrane, moderate dense or vacuolated cytoplasm (Fig. 48). Psammoma bodies may be encountered in aspirates and necrotic materials may be seen. It is impossible to distinguish serous borderline tumor from serous carcinoma, which depends on identification of stromal invasion on surgical resection specimen.
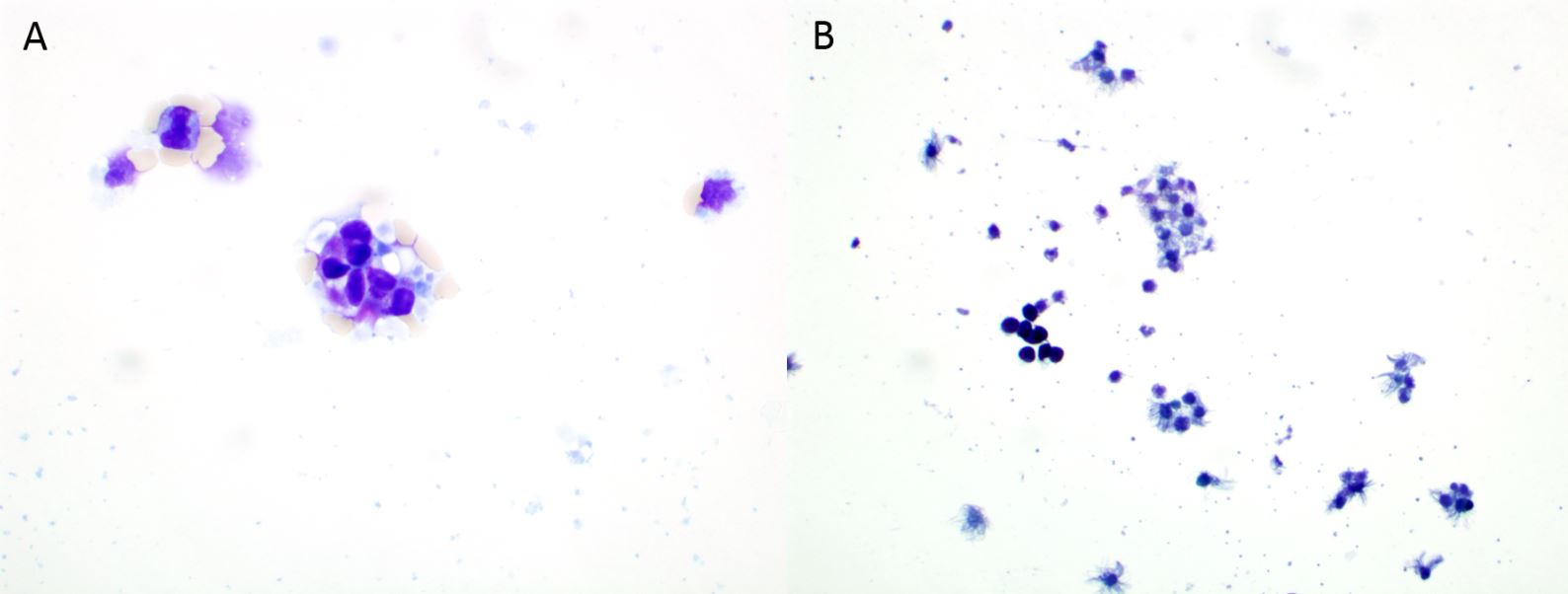{kind=link}
{kind=link}
MUCINOUS TUMORS
Mucinous tumors are also subclassified into benign mucinous cystadenoma, borderline tumor, and carcinoma. Borderline tumors are further subclassified into intestinal type and endocervical type. FNA of mucinous tumors yield a variable amount of mucin, macrophages, and maybe paucicellular for mucinous cells. Mucinous cells may resemble histiocytes in cystic fluid. FNA of benign mucinous cystadenoma usually yield strips of columnar cells with basally located small round nuclei containing fine granular chromatin and intracytoplasmic mucin, possible goblet cells (Fig. 49). Usually, FNA biopsies of borderline tumors are more cellular, and tumor cells are arranged in papillary or acinar architectures and have variably shaped, more pleomorphic nuclei with prominent nucleoli and irregular nuclear membrane (Fig. 50). Well-differentiated mucinous malignant tumors are difficult to differentiate in aspirates from borderline tumors of the ovary. Ovarian mucinous tumors must be separated from metastatic mucinous tumor from the gastrointestinal tract and pancreas. Immunostains may help to distinguish ovarian mucinous tumor from metastatic adenocarcinoma (Table 2).87
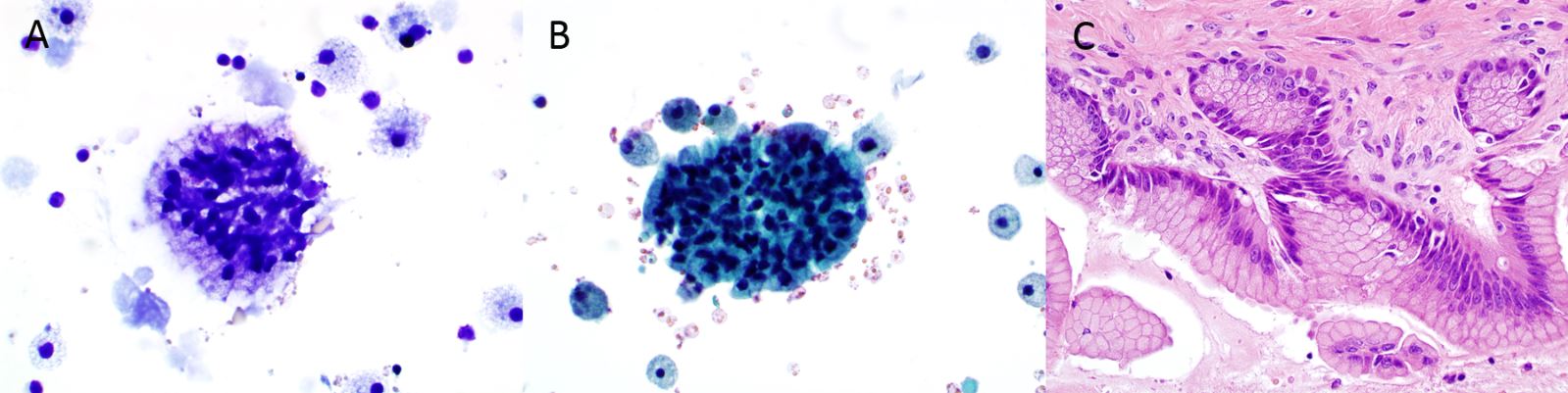{kind=link}
Fig. 49. FNA of ovarian benign mucinous cystadenoma (A: Diff-Quik stain, x600; B: Papanicolaou stain, x600; C: Surgical resection, H&E stain, x400).
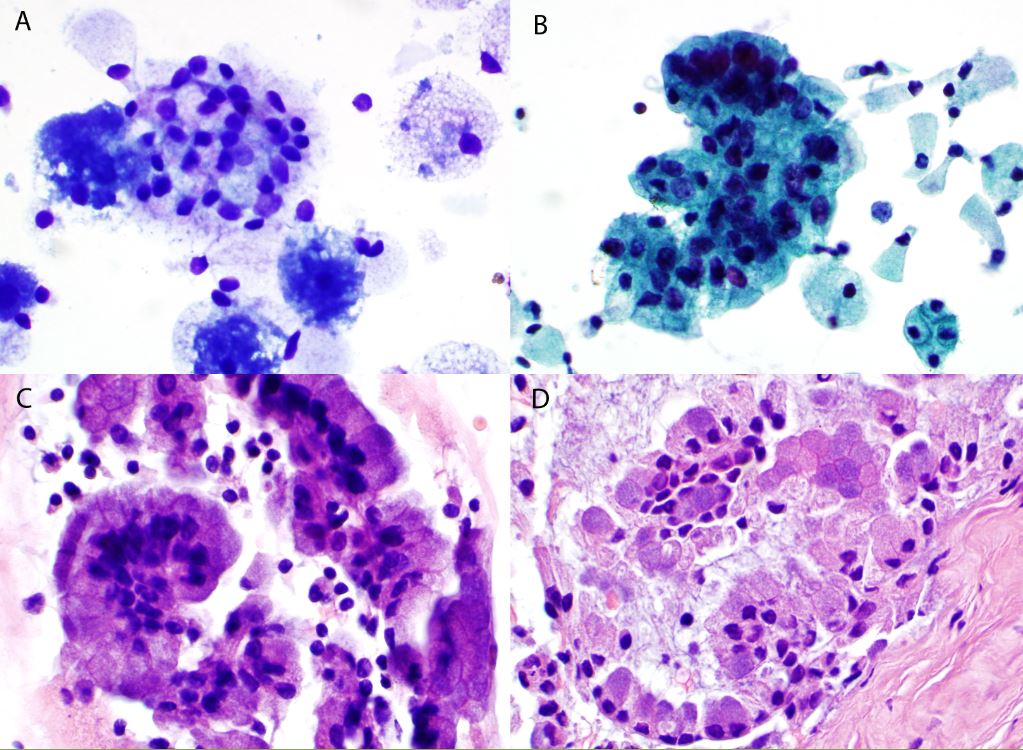{kind=link}
Table 2. Expression of immunohistochemical (IHC) markers in ovarian mucinous cystic neoplasm (MCN) and metastatic colorectal adenocarcinoma
| MCN | CDX-2 | PDX-1 | CA-125 | CK7 | CK20 |
| Ovarian MCN-intestinal | 29% | 100%* | 0% | 100%* | 100%* |
| Ovarian MCN-endocervical | 0% | 0% | 100%* | 100%* | 0% |
| Colorectal adenocarcinoma | 100%* | 33% | 0% | 0% | 100%* |
All tumors were negative for TTF-1, D2-40 and WT-1.
*P <0.01.
ENDOMETRIOID ADENOCARCINOMA
FNA aspirates from endometrioid adenocarcinoma of the ovary show clusters of columnar cells that are arranged in tubular/acinar architectures, have eccentric nuclei containing coarse chromatin and prominent nucleoli, and moderate delicate cytoplasm (Fig. 44). Mitoses and necrosis can be seen. High grade endometrioid adenocarcinoma can mimic serous type neoplasms in aspirates. The tumor cells are immunoreactive for PAX-8, ER, monoclonal CEA and vimentin, which are helpful for diagnosis of endometrioid adenocarcinoma. Testing of microsatellite instability and/or Immunohistochemical testing for mismatch repair genes (MLH1, MSH2, PMS2 and MSH6) should be performed.
OTHER OVARIAN TUMORS
FNA of teratoma may show squamous cells and keratin, ciliated glandular cells, etc.
Sex-cord stromal and germ cell tumor components can be identified and diagnosed on cytology, however, accurate classification is dependent on the adequacy of sampling.
MESTASTATIC MALIGNANCIES
The most common sites of origin of metastatic ovarian tumors include the gastrointestinal tract (stomach, colon, pancreas, and appendix), breast, and hematopoetic system. Ovarian involvement is seen at autopsy in about 10% of breast cancer cases, with bilateral metastasis in approximately 80% of those cases. Identification of the tumor as adenocarcinoma is easily done on cytology, however, establishing the origin may require immunohistochemical stains and clinical correlation. Signet ring cell type of morphology is often seen in Krukenberg tumors. In cases in which a primary tumor has been diagnosed previously, comparison of the histologic features with those of the primary tumor can establish whether the cells aspirated from the ovary are part of a primary or metastatic process.88 Gastric adenocarcinomas are immunoreactive for CK7 and less frequently immunoreactive for CK20 and CDX2 (Fig. 51), and colorectal adenocarcinomas are immunoreactive for CK20 and CDX2, and immunonegative for CA125.87 In contrast, mucinous tumors of the ovary are immunoreactive for CK7, CK20, CA125, PAX-8 and ER.87 Therefore, the immunoprofile is useful to distinguish ovarian mucinous tumor from gastric adenocarcinoma. Breast adenocarcinomas are immunoreactive for BRST2, GATA3 and mammaglobin, while ovarian tumors are positive for PAX-8, which are useful to distinguish metastatic breast adenocarcinoma from ovarian tumors.
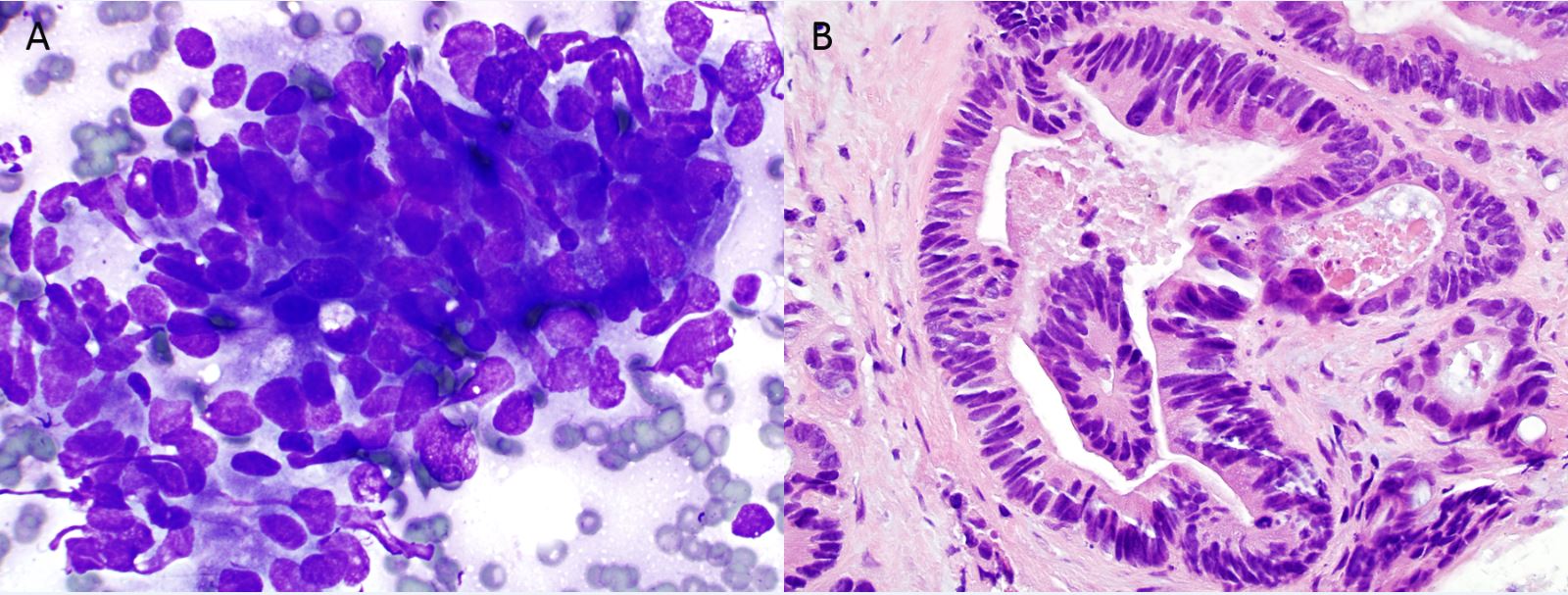{kind=link}
Lymphoma in the ovary is, for the most part, a secondary/metastatic neoplasm. Up to 25% of women dying with lymphoma are shown to have ovarian involvement. The occurrence of lymphomas primarily arising in the ovaries has long been debated as the origin of lymphomas requires the presence of preexisting benign lymphoid infiltrates in the ovary. It is postulated that reactive lymphocytes may secondarily populate the ovary in response to various ovarian lesions, including endometriosis, pelvic inflammatory disease, cysts, or benign/malignant neoplasms.89
FNA cytology in the staging of gynecologic malignancies
Under radiologic guidance, FNA biopsy is used in gynecologic oncology in the evaluation of intra-abdominal and pelvic masses and also for any superficially palpable masses/lymph nodes. FNA biopsy can be utilized for primary diagnosis or staging/recurrence/detection of metastasis in various malignancies. FNA biopsy for detection of metastatic disease has a high sensitivity and specificity.90 Reports have shown accurate ovarian cancer identification in 85–95% of cases, while the proportion of false-positive reports in histopathologically benign cases varied from 0 to 5%.91 FNA cytology of ovarian masses may also not only be used for diagnosis and classification of ovarian neoplasms, but may also be used for DNA analysis and detection of prognostic markers, thereby providing information regarding biological behavior of the tumors. The cytologic appearance of metastatic gynecologic malignancies is similar to the morphology of the primary tumor. Further immunohistochemical staining and molecular studies, if indicated, should always be correlated clinically to confirm the origin of metastasis
REFERENCES
Traut HF, Papanicolaou GN. Cancer of the Uterus: The Vaginal Smear in Its Diagnosis. Cal West Med. Aug 1943;59(2):121-122 |
|
GN P. Atlas of Exfoliative Cytology 1943 |
|
Reagan JW, Seidemann IL, Saracusa Y. The cellular morphology of carcinoma in situ and dysplasia or atypical hyperplasia of the uterine cervix. Cancer. Mar 1953;6(2):224-234. |
|
Richart RM. Influence of diagnostic and therapeutic procedures on the distribution of cervical intraepithelial neoplasia. Cancer. Nov 1966;19(11):1635-1638. |
|
Kurman RJ, Henson DE, Herbst AL, Noller KL, Schiffman MH. Interim guidelines for management of abnormal cervical cytology. The 1992 National Cancer Institute Workshop. JAMA. Jun 15 1994;271(23):1866-1869. |
|
Davey DD, Zaleski S, Sattich M, Gallion H. Prognostic significance of DNA cytometry of postirradiation cervicovaginal smears. Cancer. Feb 25 1998;84(1):11-16. |
|
Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA. Apr 24 2002;287(16):2114-2119. |
|
Nayar R, Wilbur DC. The Bethesda System for Reporting Cervical Cytology. 3 ed. Switzerland: Springer; 2014. |
|
Koutsky LA, Ault KA, Wheeler CM, et al. A controlled trial of a human papillomavirus type 16 vaccine. N Engl J Med. Nov 21 2002;347(21):1645-1651. |
|
Koutsky LA. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervicallesions. . The New England Journal of Medicine. 2007;356(19):1915-1927. |
|
Garland SM, Hernandez-Avila M, Wheeler CM, et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N Engl J Med. May 10 2007;356(19):1928-1943. |
|
Rambout L, Hopkins L, Hutton B, Fergusson D. Prophylactic vaccination against human papillomavirus infection and disease in women: a systematic review of randomized controlled trials. CMAJ. Aug 28 2007;177(5):469-479. |
|
Ault KA. Human papillomavirus vaccines: an update for gynecologists. Clin Obstet Gynecol. Sep 2008;51(3):527-532. |
|
Barr E, Tamms G. Quadrivalent human papillomavirus vaccine. Clin Infect Dis. Sep 1 2007;45(5):609-607. |
|
Naylor B. Cytopathology of the uterus: historical perspectives. Vol 1. 2 ed. Chicago: ASCP Press; 1997. |
|
Weintraub J, Morabia A. Efficacy of a liquid-based thin layer method for cervical cancer screening in a population with a low incidence of cervical cancer. Diagn Cytopathol. Jan 2000;22(1):52-59. |
|
Papillo JL, Zarka MA, St John TL. Evaluation of the ThinPrep Pap test in clinical practice. A seven-month, 16,314-case experience in northern Vermont. Acta Cytol. Jan-Feb 1998;42(1):203-208. |
|
Ashfaq R, Gibbons D, Vela C, Saboorian MH, Iliya F. ThinPrep Pap Test. Accuracy for glandular disease. Acta Cytol. Jan-Feb 1999;43(1):81-85. |
|
Gupta PK, Baloch ZW, Cobbs C, Bibbo M. Processing liquid-based gynecologic specimens: comparison of the available techniques. Acta Cytol. Nov-Dec 2001;45(6):995-998. |
|
Bishop JW, Kaufman RH, Taylor DA. Multicenter comparison of manual and automated screening of AutoCyte gynecologic preparations. Acta Cytol. Jan-Feb 1999;43(1):34-38. |
|
Kipp BR, Medeiros F, Campion MB, et al. Direct uterine sampling with the Tao brush sampler using a liquid-based preparation method for the detection of endometrial cancer and atypical hyperplasia: a feasibility study. Cancer. Aug 25 2008;114(4):228-235. |
|
Koss LG. Diagnostic Cytology and Its Histopathologic Bases. 5 ed. Philadelphia: Lippincott Williams & Wilkins; 2006. |
|
El-Fakharany M, Meroueh C, Kurella S, Mazzara P. Reporting endometrial cells in Papanicolaou smears of women age 40 and older: a qualifying educational note could prevent unnecessary follow-up biopsy. Acta Cytol. Mar-Apr 2007;51(2):178-182. |
|
Chan JK, Kung IT. Rehydration of air-dried smears with normal saline. Application in fine-needle aspiration cytologic examination. Am J Clin Pathol. Jan 1988;89(1):30-34. |
|
Ransdell JS, Davey DD, Zaleski S. Clinicopathologic correlation of the unsatisfactory Papanicolaou smear. Cancer. Jun 25 1997;81(3):139-143. |
|
Davey DD, Cox JT, Austin RM, et al. Cervical cytology specimen adequacy: patient management guidelines and optimizing specimen collection. J Low Genit Tract Dis. Apr 2008;12(2):71-81. |
|
Davey DD, Austin RM, Birdsong G, et al. ASCCP Patient Management Guidelines: Pap Test Specimen Adequacy and Quality Indicators. J Low Genit Tract Dis. Jul 2002;6(3):195-199. |
|
Massad LS, Einstein MH, Huh WK, et al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. Obstet Gynecol. Apr 2013;121(4):829-846. |
|
Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. J Low Genit Tract Dis. Jul 2012;16(3):175-204. |
|
Morse AR, Coleman DV, Gardner SD. An evaluation of cytology in the diagnosis of herpes simplex virus infection and cytomegalovirus infection of the cervix uteri. J Obstet Gynaecol Br Commonw. May 1974;81(5):393-398. |
|
Matas AJ, Simmons RL, Najarian JS. Chronic antigenic stimulation, herpesvirus infection, and cancer in transplant recipients. Lancet. Jun 7 1975;1(7919):1277-1279. |
|
Matas AJ, Simmons RL, Kjellstrand CM, Buselmeier TJ, Najarian JS. Increased incidence of malignancy during chronic renal failure. Lancet. Apr 19 1975;1(7912):883-886. |
|
Bosch FX, Munoz N. Human papillomavirus and cervical neoplasia: a critical review of the epidemiological evidence. IARC Sci Publ. 1989(94):135-151. |
|
Meisels A, Morin C. [Morphology of lesions of the uterine cervix and human papillomaviruses]. Arch Anat Cytol Pathol. 1997;45(5):261-267. |
|
Vooijs PG, Elias A, van der Graaf Y, Veling S. Relationship between the diagnosis of epithelial abnormalities and the composition of cervical smears. Acta Cytol. May-Jun 1985;29(3):323-328. |
|
Gupta S, Mukherjee K, Gupta YN, Kumar M. Sequential radiation changes in cytology of vaginal smears in carcinoma of cervix uteri during radiotherapy. Int J Gynaecol Obstet. Aug 1987;25(4):303-308. |
|
Beral V, Newton R. Overview of the epidemiology of immunodeficiency-associated cancers. J Natl Cancer Inst Monogr. 1998(23):1-6. |
|
Bukovsky A, Zidovsky J. Cytologic phenomena accompanying uterine cervix electrocoagulation. Acta Cytol. May-Jun 1985;29(3):353-362. |
|
Allen JM, Stein DS, Shingleton HM. Regeneration of cervical epithelium after laser vaporization. Obstet Gynecol. Dec 1983;62(6):700-706. |
|
Bellina JH, Seto YJ. Pathological and physical investigations into CO2 laser - tissue interactions with specific emphasis on cervical intraepithelial neoplasm. Lasers Surg Med. 1980;1(1):47-69. |
|
Williamson BA, DeFrias D, Gunn R, Tarjan G, Nayar R. Significance of extensive hyperkeratosis on cervical/vaginal smears. Acta Cytol. Sep-Oct 2003;47(5):749-752. |
|
Abramovich CM, Wasman JK, Siekkinen P, Abdul-Karim FW. Histopathologic correlation of atypical parakeratosis diagnosed on cervicovaginal cytology. Acta Cytol. May-Jun 2003;47(3):405-409. |
|
Vooijs GP. Comprehensive Cytopathology. Philadelphia: WB Saunders; 1991. |
|
Pillay B, Gregory AR, Subbiah M. Cytopathologic changes associated with intrauterine contraceptive devices. A review of cervico-vaginal smears in 350 women. Med J Malaysia. Mar 1994;49(1):74-77. |
|
Risse EK, Beerthuizen RJ, Vooijs GP. Cytologic and histologic findings in women using an IUD. Obstet Gynecol. Nov 1981;58(5):569-573. |
|
Gupta PK, Burroughs F, Luff RD, Frost JK, Erozan YS. Epithelial atypias associated with intrauterine contraceptive devices (IUD). Acta Cytol. Sep-Oct 1978;22(5):286-291. |
|
Matias-Guiu X, Lerma E, Prat J. Clear cell tumors of the female genital tract. Semin Diagn Pathol. Nov 1997;14(4):233-239. |
|
Fontaine PL, Saslow D, King VJ. ACS/ASCCP/ASCP guidelines for the early detection of cervical cancer. Am Fam Physician. Sep 15 2012;86(6):501, 506-507. |
|
Elsheikh TM, Kirkpatrick JL, Wu HH. The significance of "low-grade squamous intraepithelial lesion, cannot exclude high-grade squamous intraepithelial lesion" as a distinct squamous abnormality category in Papanicolaou tests. Cancer. Oct 25 2006;108(5):277-281. |
|
Jones HW, 3rd. Impact of the Bethesda System. Cancer. Nov 15 1995;76(10 Suppl):1914-1918. |
|
Solomon D, Schiffman M, Tarone R, group AS. Comparison of three management strategies for patients with atypical squamous cells of undetermined significance: baseline results from a randomized trial. J Natl Cancer Inst. Feb 21 2001;93(4):293-299. |
|
Stoler MH, Schiffman M, Atypical Squamous Cells of Undetermined Significance-Low-grade Squamous Intraepithelial Lesion Triage Study G. Interobserver reproducibility of cervical cytologic and histologic interpretations: realistic estimates from the ASCUS-LSIL Triage Study. JAMA. Mar 21 2001;285(11):1500-1505. |
|
Wright TC, Jr., Cox JT, Massad LS, Twiggs LB, Wilkinson EJ, Conference AS-SC. 2001 Consensus Guidelines for the management of women with cervical cytological abnormalities. JAMA. Apr 24 2002;287(16):2120-2129. |
|
Sherman ME, Solomon D, Schiffman M, Group ALTS. Qualification of ASCUS. A comparison of equivocal LSIL and equivocal HSIL cervical cytology in the ASCUS LSIL Triage Study. Am J Clin Pathol. Sep 2001;116(3):386-394. |
|
Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. Feb 12 1998;338(7):423-428 |
|
Melnikow J, Nuovo J, Willan AR, Chan BK, Howell LP. Natural history of cervical squamous intraepithelial lesions: a meta-analysis. Obstet Gynecol. Oct 1998;92(4 Pt 2):727-735. |
|
Schlecht NF, Platt RW, Duarte-Franco E, et al. Human papillomavirus infection and time to progression and regression of cervical intraepithelial neoplasia. J Natl Cancer Inst. Sep 3 2003;95(17):1336-1343. |
|
He GF, Bian ML, Wang Y, Liu XY. Cervical cytological screening and management in pregnant and postpartum women. Chin Med Sci J. Dec 2005;20(4):242-246. |
|
Onuma K, Saad RS, Kanbour-Shakir A, Kanbour AI, Dabbs DJ. Clinical implications of the diagnosis "atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion" in pregnant women. Cancer. Oct 25 2006;108(5):282-287. |
|
Kaplan KJ, Dainty LA, Dolinsky B, et al. Prognosis and recurrence risk for patients with cervical squamous intraepithelial lesions diagnosed during pregnancy. Cancer. Aug 25 2004;102(4):228-232. |
|
Kurman RJ, Carcangiu ML, Herrington CS, Young RH. Tomours of the uterine cervix. In: Kurman RJ, Carcangiu ML, Herrington CS, Young RH, eds. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC; 2014:169-206. |
|
Wilbur DC. Benign changes and minics of malignant and premalignant epithelial lesions. In: Wilbur DC, Henry MR, eds. Bynecologic Cytopathology. Chicago: CAP Press; 2008:25-68. |
|
Granter SR, Lee KR. Cytologic findings in minimal deviation adenocarcinoma (adenoma malignum) of the cervix. A report of seven cases. Am J Clin Pathol. Mar 1996;105(3):327-333. |
|
Kusanagi Y, Kojima A, Mikami Y, et al. Absence of high-risk human papillomavirus (HPV) detection in endocervical adenocarcinoma with gastric morphology and phenotype. Am J Pathol. Nov 2010;177(5):2169-2175. |
|
Guidos BJ, Selvaggi SM. Detection of endometrial adenocarcinoma with the ThinPrep Pap test. Diagn Cytopathol. Oct 2000;23(4):260-265. |
|
Khalbuss WE, Pantanowitz L, Monaco SE. Cytomorphology of unusual primary tumors in the Pap test. Cytojournal. 2013;10:17. |
|
Ioffe O, Henry MR. The uterine cervix. In: Silverberg SG, DeLellis RA, Frable WJ, LiVolsi VA, Wick MR, eds. Principles and practice of surgical pathology and cytopathology. Vol 2. 4th ed. New York: Churchill Livingstone; 2006:1931-1984. |
|
Witkiewicz AK, Wright TC, Ferenczy A, Ronnett BM, J. KR. Carcinoma and other tumors of the cervix. In: J. KR, Ellenson LH, M. RB, eds. Blaustein's pathology of the female genital tract. 6th ed. Now York: Springer; 2011:254-303. |
|
Thomas MB, Wright JD, Leiser AL, et al. Clear cell carcinoma of the cervix: a multi-institutional review in the post-DES era. Gynecol Oncol. Jun 2008;109(3):335-339. |
|
Reis-Filho JS, Fillus Neto J, Schonemann E, Sanderson A, Schmitt FC. Glassy cell carcinoma of the uterine cervix. Report of a case with cytohistologic and immunohistochemical study. Acta Cytol. May-Jun 2001;45(3):407-410. |
|
Shield P. Peritoneal washing cytology. Cytopathology. Jun 2004;15(3):131-141. |
|
Mlyncek M, Uharcek P. Peritoneal cytology in endometrial cancer. Neoplasma. 2005;52(2):103-108. |
|
Zuna RE, Hansen K, Mann W. Peritoneal washing cytology in cervical carcinoma. Analysis of 109 patients. Acta Cytol. Sep-Oct 1990;34(5):645-651. |
|
Lin O. Challenges in the interpretation of peritoneal cytologic specimens. Arch Pathol Lab Med. May 2009;133(5):739-742. |
|
Sneige N, Fanning CV. Peritoneal washing cytology in women: diagnostic pitfalls and clues for correct diagnosis. Diagn Cytopathol. 1992;8(6):632-640; discussion 640-632. |
|
Sneige N, Fernandez T, Copeland LJ, Katz RL. Mullerian inclusions in peritoneal washings. Potential source of error in cytologic diagnosis. Acta Cytol. May-Jun 1986;30(3):271-276. |
|
Chen KT. Benign glandular inclusions of the peritoneum and periaortic lymph nodes. Diagn Gynecol Obstet. Fall 1981;3(3):265-268. |
|
Hsu YK, Parmley TH, Rosenshein NB, Bhagavan BS, Woodruff JD. Neoplastic and non-neoplastic mesothelial proliferations in pelvic lymph nodes. Obstet Gynecol. Jan 1980;55(1):83-88. |
|
Zinsser KR, Wheeler JE. Endosalpingiosis in the omentum: a study of autopsy and surgical material. Am J Surg Pathol. Mar 1982;6(2):109-117. |
|
Fadare O, Mariappan MR, Hileeto D, Wang S, McAlpine JN, Rimm DL. Upstaging based solely on positive peritoneal washing does not affect outcome in endometrial cancer. Mod Pathol. May 2005;18(5):673-680. |
|
Kyrgiou M, Chatterjee J, Lyus R, Amin T, Ghaem-Maghami S. The role of cytology and other prognostic factors in endometrial cancer. J Obstet Gynaecol. Oct 2013;33(7):729-734. |
|
Zaino RJ, Kurman RJ, Diana KL, Morrow CP. Pathologic models to predict outcome for women with endometrial adenocarcinoma: the importance of the distinction between surgical stage and clinical stage--a Gynecologic Oncology Group study. Cancer. Mar 15 1996;77(6):1115-1121. |
|
Layfield LJ, Heaps JM, Berek JS. Fine-needle aspiration cytology accuracy with palpable gynecologic neoplasms. Gynecol Oncol. Jan 1991;40(1):70-73. |
|
Layfield LJ, Berek JS. Fine-needle aspiration cytology in the management of gynecologic oncology patients. Cancer Treat Res. 1994;70:1-13. |
|
Ramzy I, Delaney M. Fine needle aspiration of ovarian masses. I. Correlative cytologic and histologic study of celomic epithelial neoplasms. Acta Cytol. Mar-Apr 1979;23(2):97-104. |
|
Selvaggi SM. Fine-needle aspiration cytology of ovarian follicle cysts with cellular atypia from reproductive-age patients. Diagn Cytopathol. 1991;7(2):189-192. |
|
Lin X, Lindner JL, Silverman JF, Liu Y. Intestinal type and endocervical-like ovarian mucinous neoplasms are immunophenotypically distinct entities. Applied immunohistochemistry & molecular morphology : AIMM / official publication of the Society for Applied Immunohistochemistry. Oct 2008;16(5):453-458. |
|
Hajdu SI, Melamed MR. Limitations of aspiration cytology in the diagnosis of primary neoplasms. Acta Cytol. May-Jun 1984;28(3):337-345. |
|
Crasta JA, Vallikad E. Ovarian lymphoma. Indian J Med Paediatr Oncol. Jan 2009;30(1):28-30. |
|
Bonfiglio TA, MacIntosh PK, Patten SF, Jr., Cafer DJ, Woodworth FE, Kim CW. Fine needle aspiration cytopathology of retroperitoneal lymph nodes in the evaluation of metastatic disease. Acta Cytol. Mar-Apr 1979;23(2):126-130. |
|
Bandyopadhyay A, Chakraborty J, Chowdhury AR, Bhattacharya A, Bhattachrya P, Chowdhury M. Fine needle aspiration cytology of ovarian tumors with histological correlation. J Cytol. Jan 2012;29(1):35-40. |