Neonatal Resuscitation
Authors
INTRODUCTION
The adaptation from intrauterine to extrauterine life involves a complex and rapid orchestration of physiologic changes. Within minutes of life, the newly born infant is subjected to multiple unfamiliar stimuli such as cold, light, and noise compared with the warm, dark environment of intrauterine life. In addition, the infant must make the transition from dependence on placental gas exchange to spontaneous air breathing and pulmonary gas exchange. Most often, this transition occurs without difficulty. However, multiple maternal, placental, mechanical, and fetal conditions exist that can jeopardize a smooth transition and signal the need for intervention. It is estimated that 5% to 10% of newly born infants will require some degree of active resuscitation for this transition to occur.1 Thus, an individual trained in neonatal resuscitation must be in attendance at every delivery. Furthermore, it is essential that these skilled personnel understand transitional physiology and the basic principles of resuscitation to intervene rapidly when needed in an attempt to prevent any long-term adverse sequelae. The purpose of this chapter is to discuss the physiology of the birth process and the basic approaches to neonatal resuscitation.
FETAL PHYSIOLOGY
The fetal environment is drastically different from that of the newly born infant. The fluid-filled amniotic sac creates a warm, cushioned space for the fetus. Fetal lung fluid, which is constantly secreted by the lung epithelium into the alveolar spaces,2 is crucial for fetal lung growth.3 This fetal lung fluid at term gestation is equivalent to the functional residual capacity of the newborn lung or 20 to 25 mL/kg. Fetal breathing actively propels this fluid out of the lungs,4 thus contributing to the amniotic fluid. Fetal respirations are also thought to strengthen the diaphragm and intercostal muscles in preparation for birth. During gestation, the placenta is the organ of gas exchange. However, after birth, the respiratory muscles take over the work of breathing and the lungs assume the responsibility of gas exchange and oxygenation.5
Fetal blood is relatively hypoxemic. The highest Pao2 is about 30 to 35 mm Hg, with an oxyhemoglobin saturation of approximately 75% to 85%. Yet, this level is adequate for fetal tissue oxygenation and growth owing to some compensatory mechanisms. First of all, oxygen consumption is lower in the fetus compared with that of the newly born infant. Second, the fetus has an increased red cell mass. Third, fetal hemoglobin has an increased affinity for oxygen.
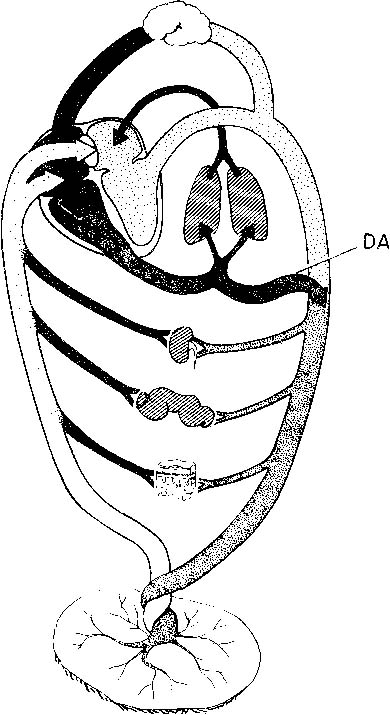
Fetal circulation is unique because the placenta is wholly responsible for respiration, nutrition, metabolism, and excretion. Oxygenated blood with the highest Pao2 therefore moves from the placenta through the umbilical vein to the fetus. From the umbilical vein, blood then flows through the ductus venosus into the inferior vena cava and subsequently into the right atrium. Approximately two thirds of this blood is shunted across the foramen ovale into the left atrium. This shunting occurs because the left atrial pressure is lower than that of the right atrium in the fetus. From the left atrium, the blood enters the left ventricle and subsequently the systemic circulation. The coronary and cerebral vessels arise directly off the aorta and thus are bathed with the best oxygenated blood available to the fetus.5
The remaining blood that does not flow across the foramen ovale mixes with the venous return from the superior vena cava and enters the right ventricle. From there, the blood flows into the pulmonary circulation, where it encounters high vascular resistance in part owing to the thick muscular coat of the small pulmonary arteries. Thus, only about 10% of this blood enters the pulmonary circulation. This blood volume allows for lung growth and development. The remaining 90% is shunted through the ductus arteriosus into the descending aorta. Blood then flows back to the placenta where metabolic by-products are exchanged for oxygen. Figure 1 depicts the normal fetal circulation.
{kind=link}
TRANSITION AT BIRTH
Owing to the interruption of umbilical venous flow with each contraction, the fetus experiences brief periods of asphyxia. This is manifested by intermittent and brief fetal bradycardia, which are temporally related to the contractions during normal labor. At birth, the ultimate asphyxiating event occurs as the umbilical cord is clamped. From that point forward, the neonate can no longer rely on the placenta for respiration. The neonate must undergo a rapid series of physiologic changes to function independently. Environmental stressors such as light, noise, and cold help the infant to make the transition to air breathing as respiratory effort increases. Air replaces the fluid-filled alveolar spaces. This event must be matched by increased pulmonary blood flow for effective gas exchange to occur.
In the days preceding spontaneous vaginal birth, fetal lung fluid production decreases.6 In addition, a circumferential chest squeeze that occurs with each contraction during labor helps to expel some fetal lung fluid out of the trachea. The majority of this fluid, however, is actively transported from the alveolar spaces across the pulmonary epithelium into the interstitium of the lung. This fluid then moves into the capillaries and the lymphatic system of the pulmonary circulation.7 Within 6 to 24 hours of life, fetal lung fluid is usually completely cleared. This process may take longer, however, in preterm births or after cesarean section deliveries. The normal decrease in fetal lung fluid does not transpire in the case of preterm delivery or operative delivery without prior labor.8,9 In addition, premature newborns with hyaline membrane disease and neonates with transient tachypnea of the newborn exhibit abnormal lung ion transport.10,11
The neonate experiences an increase in negative intrathoracic pressure, leading to lung expansion and increasing alveolar oxygenation as air replaces fetal lung fluid. This pressure is countered by lung compliance, lung fluid viscosity, and surface tension forces. Thus, large transpulmonary pressures are required for the first few breaths immediately after birth. As air enters the lungs, air-liquid interfaces are created that establish alveolar surface tension. Surface tension forces oppose alveolar expansion. Surfactant, a phospholipid-protein complex produced by type II pneumocytes, is deposited along alveolar surfaces, thus helping to decrease these surface tension forces and promote alveolar stability. As a result, less transpulmonary pressures are needed for subsequent breaths, and soon functional residual capacity is established.
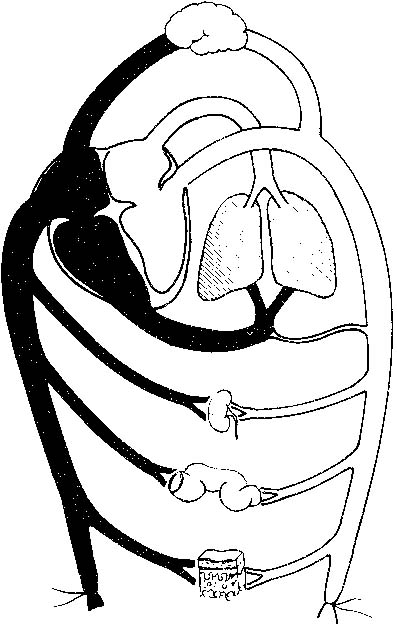
During the last trimester, the number of small blood vessels per unit of lung increases 10-fold, preparing the lungs to accept the 10-fold increase in blood per unit of lung that occurs at birth.12 At birth, pulmonary blood flow increases and pulmonary vascular resistance falls from that occurring in fetal life where it was equivalent to the systemic vascular resistance. Both the external and the luminal diameters of the small pulmonary arteries increase as the endothelial cells flatten and the smooth muscle spreads and relaxes.13 Subsequently, alveolar oxygenation increases, which in turn contributes to a further decline in pulmonary vascular resistance and a concomitant increase in pulmonary blood flow. This substantially larger volume of blood flow to the lungs, which had been only approximately 5% of cardiac output in utero, now returns to the left atrium. Left atrial pressure rises, which closes the one-way flap valve of the foramen ovale and prevents right-to-left shunting of blood. In essence, the foramen ovale functionally closes. As the pulmonary vascular resistance falls below systemic resistance, blood flow through the ductus arteriosus reverses. Owing to the increasing oxygen tension after birth, the ductus arteriosus functionally starts to close and eventually closes anatomically within several days of life. Closure of the ductus arteriosus then represents the terminal phase in the conversion of the fetal circulatory pattern to that of the newly born infant, in which the pulmonary and systemic circulations are separate. The circulation in the normal newly born infant who has successfully adapted to extrauterine life is shown in Figure 2.
{kind=link}
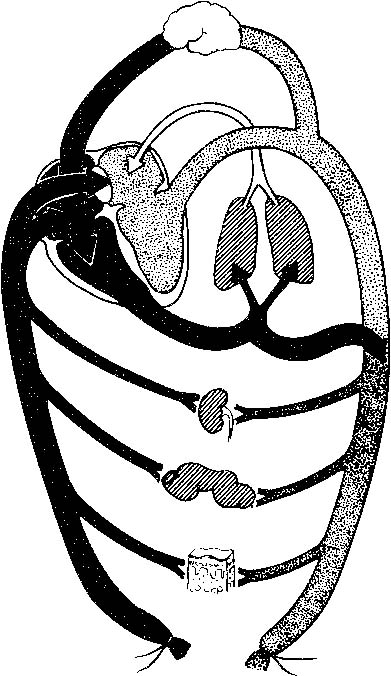
In the majority of births, these complex physiologic changes occur spontaneously and rapidly, resulting in a smooth transition from fetal to neonatal life. However, if any of the previously described changes are not accomplished successfully, the clinical syndrome of persistent pulmonary hypertension of the newborn may result. In this scenario, the pulmonary circulation continues to exhibit high resistance. Moreover, there are precursor smooth muscle cells in the nonmuscularized small pulmonary arteries that may rapidly differentiate into mature smooth muscle cells under hypoxic conditions.14 Thus, the circulatory pattern continues as in intrauterine life, but now without the benefit of the placenta because the umbilical cord has been clamped. Deoxygenated blood returning to the right side of the heart flows across the foramen ovale and the ductus arteriosus to the systemic circulation and organ tissues. Further hypoxemia and subsequent acidosis ensue, resulting in a vicious circle as pulmonary vascular resistance increases and progressively deoxygenated blood circulates. Figure 3 demonstrates the abnormal physiology of persistent pulmonary hypertension of the newborn. If significant hypoxemia and acidosis are present in utero, this decompensatory course may occur more quickly and may be harder to reverse. Systemic organ dysfunction and, more importantly, long-term neurologic compromise may result. Worldwide, greater than 5 million neonatal deaths occur yearly, and of these, birth asphyxia accounts for 19%.15 It is precisely for this reason that the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists have official policy statements that mandate the attendance at every delivery of personnel skilled in neonatal resuscitation.
{kind=link}
NEONATAL RESUSCITATION
Anticipation, adequate preparation, accurate evaluation, and prompt initiation of support are critical for a successful neonatal resuscitation. Communication between the obstetric and the pediatric services can augment this process of anticipation and adequate preparation immensely. As an adjunct, a prenatal consult with the family regarding short- and long-term management should be accomplished, as time permits. Parents should share their beliefs and be involved in the decision-making regarding the extent of resuscitation. This is especially critical in cases of extremely premature infants or infants with a potentially lethal congenital abnormality diagnosed prenatally. To ensure adequate preparation, ongoing communication between the obstetric and the pediatric services is essential. Important perinatal information includes details of maternal medical condition(s) and subsequent treatment as well as specific indicators of the fetal condition such as heart rate monitoring, lung maturity, and antenatal ultrasound findings.
Perinatal depression can arise as a result of antepartum, intrapartum, and/or postpartum problems during which the fetus becomes hypoxic, hypercarbic, and subsequently acidotic. The result of perinatal depression, regardless of the inciting event, is that the infant fails to initiate respirations or the respirations are insufficient to provide adequate gas exchange. Table 1 lists many of the numerous conditions that place the newly born infant at risk.
TABLE 1. Risk Factors Associated With the Need for Neonatal Resuscitation
Autopartum (Maternal) | Intrapartum | Postpartum |
Diabetes mellitus | Multiple gestation | Apnea |
Hypertension | Nonvertex presentation | Bradycardia |
Substance abuse | Postdates | Respiratory distress |
Vascular disease | Macrosomia/microsomia | Hypoperfusion |
Vasoactive medications | Maternal hypotension | Anemia |
Smoking | Placental abruptio or previa | Congenital anomaly |
Poor maternal weight gain | Cord accidents | Infection |
Myasthenia gravis | Maternal infection | Prematurity |
Sexually transmitted disease | Operative delivery | Birth trauma |
Prior fetal or neonatal demise | General anesthesia | |
No prenatal care | Poly/oligohydramnios | |
Chronic disease states | Fetal anomaly | |
Anemia | Isoimmunization | |
Hemorrhage | Prematurity | |
Maternal age > 35 yr | Prolonged labor | |
Maternal age < 15 yr | Meconium stained amniotic fluid | |
Abnormal fetal heart rate pattern | ||
Maternal sedation |
Faix RG: Neonatal resuscitation. In Donn SM, Faix RG (eds): Neonatal Emergencies. Mt. Cisco, NY, Futura Publishing, 1991
Equipment
Table 2 outlines the equipment necessary for most neonatal resuscitations. As many as 10% of newly born infant will require active resuscitation. The necessary equipment should therefore be readily available in the delivery room for every birth. All equipment should be checked at regular intervals as well as immediately prior to delivery. The expiration dates of the medications should be monitored periodically as well. The personnel responsible for the newly born infant should be familiar with the organization of the equipment to promptly initiate resuscitation and provide support.
TABLE 2. Neonatal Resuscitation Equipment and Supplies
Suction Equipment
Bulb syringe
Mechanical suction
No. 5, 8, 10 French suction catheters
8 French feeding tube and 20-mL syringes
Meconium aspirator
Wall suction
Bag and Mask Equipment
Infant resuscitation bag with pressure-release valve or pressure manometer; the bag must deliver 100% oxygen
Face masks in premature and term infant sizes (No. 1, 2, 3) with cushioned rims
Oral airways
Oxygen source with intact flow meter and tubing
Intubation Equipment
Laryngoscopes with straight blades
No. 0—premature
No. 1—term
Extra bulbs and batteries for laryngoscope
Endotracheal tubes
2.5 mm—Infants < 1 kg
3 mm—Infants 1–2.5 kg
3.5 mm—Infants > 2.5 kg
Stylet
Scissors
Gloves
Medications
Epinephrine 1:10,000, 3- or 10-mL ampules
Naloxone hydrochloride 0.4 mg/mL in 1-mL ampules or 1 mg/mL in 2-mL ampules
Volume expanders
Whole blood
Fresh frozen plasma
Albumen (5%)/saline solution
Sodium bicarbonate 4.2% (5 mEq/10 mL)
Dextrose 10%, 250 mL
Sterile water 30 mL
Normal saline solution 30 mL
Other Equipment and Supplies
Radiant warmer
Stethoscope
Blood pressure monitor with appropriate cuffs
Adhesive tape
Syringes
Needles
Alcohol sponges
Umbilical catheterization tray
Umbilical tape
Umbilical catheters—3.5, 5 French
3-way stopcocks
5 French feeding tube
Cardiotachometer with electrocardiogram oscilloscope
Pressure transducer and monitor
Pulse oximeter
Modified from American Heart Association/American Academy of Pediatrics: Textbook of Neonatal Resuscitation. Dallas, 1991
Personnel
Many of the risk factors associated with the need for neonatal resuscitation are known. However, a fetus or newly born infant may experience unanticipated problems and require intervention to make a smooth transition to extrauterine life. Thus, an individual trained in neonatal resuscitation should be present at every delivery. Ideally, at least one person should solely be responsible for the newly born infant. Such personnel will vary according to local circumstances. For uncomplicated resuscitations, it is possible for one person to provide this support. However, if a high-risk delivery is anticipated in which significant resuscitative intervention may be necessary, at least one additional skilled person should be present. In addition, each infant of a multiple gestation should have separate personnel. It is also imperative that personnel attending deliveries maintain their resuscitative skills and familiarize themselves with any new guidelines as put forth by the American Academy of Pediatrics and the American Heart Association. In institutions in which resuscitations are uncommon, periodic mock codes may be helpful.
Steps to Resuscitation
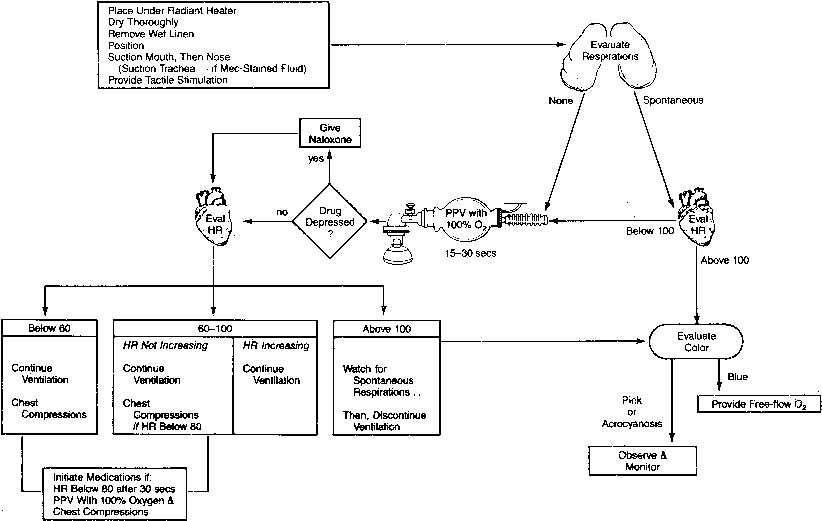
Figure 4 presents an overview of resuscitation of the newly born infant. The first step focuses on the prevention of cold stress. Cold stress induces peripheral vasoconstriction which if persists leads to increasing acidosis. In turn acidosis is a stimulus for pulmonary vasoconstriction thus setting the stage for persistent pulmonary hypertension of the newborn to develop. Cold stress occurs as the newly born infant leaves the warm liquid environment of the amniotic sac and uterus. Heat loss can be minimized by several maneuvers. The delivery room should be warm and free of drafts. The infant should be placed underneath a preheated, radiant warmer. The infant should be dried off thoroughly with warm blankets and wet blankets removed immediately. The head is proportionately larger than the body in newly born infants and is therefore a major source of heat loss. Therefore, the head should be covered with a hat. Hyperthermia should be avoided as well because it has been associated with perinatal respiratory depression. The ultimate goal is a neutral thermal environment. In this state, the infant maintains a normal core temperature, yet oxygen consumption is minimal.
{kind=link}
The next step focuses on clearing the airway. This is accomplished by using either a bulb syringe or a suction catheter. If time permits, the infant’s nares and mouth should be suctioned after delivery of the shoulders. If suctioning after delivery is needed, the mouth should be suctioned first because suctioning of the nose may lead to gagging and aspiration of oral secretions. In addition, infants are obligate nose breathers. When the mouth is suctioned, care should be taken to avoid vigorous suctioning of the posterior pharynx because this may cause laryngeal spasm and stimulate a vagal response with resultant apnea or bradycardia, thus delaying the onset of spontaneous breathing.
Most newly born infants require only these two steps to initiate adequate respirations and adapt successfully to extrauterine life. If respirations are ineffective, tactile stimuli such as gentle rubbing of the back or flicking of the heels may be added. Oxygen is indicated when cyanosis is present. Blow by oxygen at a flow of 5 L/min can be administered via a face mask and flow-inflating bag, an oxygen mask, or a hand cupped around oxygen tubing. The maximal inhaled concentration of oxygen is delivered by holding the oxygen source as close to the face as possible. Although there is some evidence to suggest that 100% oxygen may not be necessary, current guidelines recommend starting at that level and weaning as the infant responds (see controversies section). Thus, the goal of supplemental oxygen should be normoxia. This entire process of drying, suctioning, and stimulation should take less than 30 seconds. If an adequate response is not established, the subsequent steps of active resuscitation should be performed.
The ABCs (airway, breathing, circulation) that apply to older children and adults also apply to the neonate. If adequate respirations are not established despite drying, suctioning, and stimulation, additional resuscitative measures should be performed immediately. In fact, if there is any evidence of perinatal depression, vigorous resuscitation should be initiated earlier to counteract any hypoxemia or acidemia that may be present. Four percent of the newly born population requires bag mask ventilation with supplemental oxygen. The establishment of adequate ventilation must be emphasized because only a very small percentage will need chest compressions and medications.16 Indications for positive pressure ventilation administered either via bag and mask or via endotracheal tube include (1) an insufficient respiratory pattern manifested by gasping and/or apnea, (2) a heart rate that remains below 100 beats/min (bpm) for 30 seconds, and (3) persistent central cyanosis despite administration of 100% oxygen.17
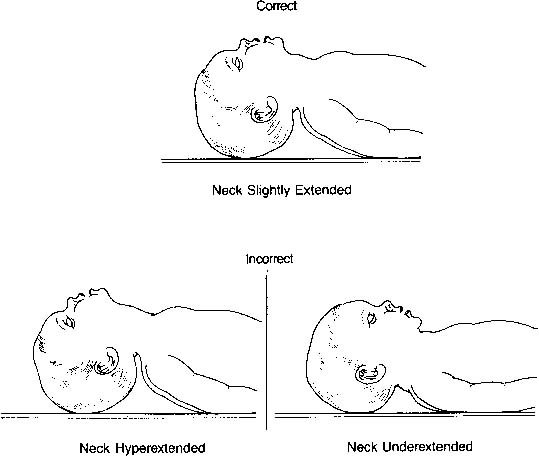
The airway is smaller and located more anteriorly than in older children and adults. Moreover, because the neonate’s head is proportionately larger than the body, the neck has a tendency to be flexed. The ideal position is described as the neutral or “sniffing” position. Both underextension (flexion) and hyperextension can obstruct flow through the airway as well as obstruct visualization of the vocal cords (Fig. 5). A blanket roll placed beneath the shoulder blades may be helpful; however, one must be careful not to hyperextend the neck.
{kind=link}
Two types of bags are available for neonatal resuscitation. A self-inflating (Ambu) bag is more convenient to use, especially for less experienced resuscitators. However, there are some limitations. An oxygen reservoir must be in place to deliver high concentrations of oxygen, otherwise mixing with room air occurs, thus limiting oxygen delivery to only 40%. In addition, the valve assembly in most of these bags allows oxygen flow only when the bag is compressed or squeezed. Thus, this type of bag cannot be used for blow by oxygen delivery. A flow-inflating (anesthesia) bag requires more experienced resuscitators. It requires continual flow for inflation and is susceptible to mechanical failure because multiple adjustments need to be considered. The flow of gas into the gas inlet as well as out through the flow-control valve must be adjusted. Lastly, a tight seal must be present between the mask and the infant’s face. At the other end of the spectrum, air leak syndromes such as pneumomediastinum, pneumothorax, or worse yet, pneumopericardium may occur because of the high pressures that can be delivered with this type of bag. The advantages, however, include the ability to provide a greater range of peak inspiratory pressures and more reliable control of oxygen concentration.
During bag mask ventilation, a tight seal is critical to administer an adequate amount of positive pressure. First, the right mask size should be chosen. It should cover the nose and mouth, but the eyes should remain uncovered. Face masks with an air-filled cushion help to enforce a tight seal without inflicting facial or ocular injury to the infant. Again, positioning of the infant is key. If the infant is not in the neutral position, flow of oxygen and positive pressure through the airway may be obstructed. In addition, it is helpful to hold the chin to the edge of the mask because this ensures a tight seal. This maneuver also elevates the angle of the jaw, which effectively brings the tongue forward and opens the airway.
Positive pressure ventilation should be administered at a rate of 30 to 60 bpm, whether via bag and mask or via an endotracheal tube. As noted previously, the first few breaths may require longer inflation times and a peak inflating pressure of 30 to 40 cm H2O for removal of fetal lung fluid and for alveolar expansion. Subsequent breaths will likely require less positive pressure. Therefore, the appropriate inflating pressure is that which is required to expand the chest and improve gas exchange. This is clinically demonstrated by chest rise, which should approximate 1/4 to 1/2 cm. If the infant initiates respirations, positive pressure should gradually be reduced and can be discontinued when a regular respiratory pattern is established. However, if chest movement does not occur despite correct infant positioning, an adequate seal, and an unobstructed airway or if significant peak inflating pressures are required, intubation should be performed. Prolonged ventilation often with high inflating pressures will be necessary if parenchymal pulmonary disease and/or persistent pulmonary hypertension of the newborn, regardless of the etiology, is present.
Visualization of the vocal cords and therefore intubation can be difficult in the newly born infant. Positioning of the infant is critical to optimize adequate visualization of this small and anteriorly located airway. Placing the infant in the neutral position cannot be overemphasized. As with the face masks, appropriately sized equipment must be used. Laryngoscope blades are available in two sizes—size 0 for preterm infants and size 1 for term infants. Table 3 shows the appropriate endotracheal tube size and depth of insertion based on gestational age and weight. A rough rule of thumb to determine the distance in centimeters to which the tip should be inserted is to add the number 6 to the infant’s weight in kilograms. In addition, the endotracheal tubes for neonates have a dark black line at the tip. Insertion of the endotracheal tube until this line just passes through the vocal cords should position the endotracheal tube above the carina. If a stylet is used, it is important to ensure that the stylet does not extend beyond the tip of the endotracheal tube because this may cause airway injury. The laryngoscope blade should be inserted into the vallecula or onto the epiglottis. The vocal cords should come into view as the laryngoscope blade is elevated superiorly. Cricoid pressure may be helpful because the airway is anteriorly located in the neonate. Correct placement should be checked initially by clinical means but should be confirmed by chest radiograph as soon as possible. Again, the chest should rise and fall with ventilation and the movement should be symmetric. As a correlate, breath sounds should be audible and symmetric throughout each lung field. It is important to listen not only anteriorly but also in both axillae. Breath sounds should not be audible over the stomach, and the stomach should not inflate. Condensation should be seen within the tube on exhalation. Some also advocate the use of an end-tidal carbon dioxide detector as a secondary confirmation of endotracheal intubation. Although false-negative results can occur, false-positive results are very unlikely.18 If there is any question whether the endotracheal tube is placed appropriately, direct visualization with a laryngoscope should be performed. The endotracheal tube should be secured as soon as correct placement is determined. Chest radiography should confirm that the endotracheal tube is located between the clavicles and the carina.
TABLE 3. Suggested Tracheal Tube Size and Depth of Insertion According to Weight and Gestational Age
Weight (gm) | Gestational Age (wk) | Tube Size (mm [ID]) | Depth of Insertion From Upper Lip (cm) |
<1000 | <28 | 2.5 | 6.5–7 |
1000–2000 | 28–34 | 3.0 | 7–8 |
2000–3000 | 34–38 | 3.5 | 8–9 |
>3000 | >38 | 3.5–4.0 | >9 |
ID, inner diameter.
Modified from American Heart Association/American Academy of Pediatrics: Textbook of Neonatal Resuscitation. Dallas, 1994
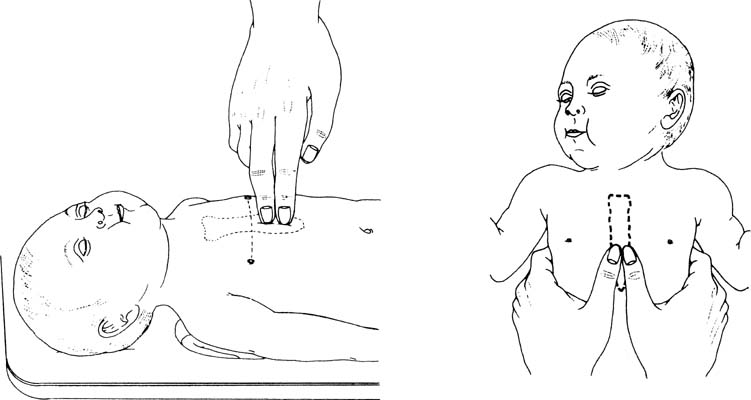
If the infant’s heart rate is absent or if after 30 seconds of effective ventilation the heart rate remains below 60 bpm, cardiac resuscitation should be initiated. Heart rate can be assessed by listening with a stethoscope over the precordium or feeling for pulsations at the base of the umbilical cord. External cardiac massage can be provided by two methods, as depicted in Figure 6. Compressions should be performed on the lower one third of the sternum immediately above the xiphoid process and should be deep enough to generate a palpable pulse. In most instances, this depth is one third of the anterior-posterior diameter of the infant’s chest. The two thumb-encircling hands technique is preferable because this results in better peak systolic and coronary perfusion pressure. However, because the hands surround the thorax with this maneuver, care must be taken to avoid limiting thoracic expansion during ventilation. As an adjunct, the most recent American Academy of Pediatrics/American Heart Association guidelines no longer recommend simultaneous ventilation and chest compressions. Instead a ratio of 3 compressions to 1 ventilation should be performed such that 120 events/min occur—90 compressions/min and 30 breaths/min.17 The infant should be reassessed 30 seconds after initiation of positive pressure ventilation and external cardiac massage. If the heart rate remains below 60 bpm, chest compressions should be resumed and resuscitative medications should be considered.
{kind=link}
Vascular Access
Placement of a peripheral venous catheter can be difficult and time-consuming in a well neonate. This difficulty is compounded if hypoxia or acidosis is present. Thus, in a depressed newly born infant, the umbilical vein presents a rapidly accessible route for the delivery of medications or volume expanders. The catheter should be inserted to a depth at which blood flows freely on aspiration, approximately 4 to 6 cm. This method ensures placement of the catheter below the liver and avoids potential damage from intrahepatic infusions. If, for some reason, the umbilical vein cannot be cannulated and peripheral access is unsuccessful, intraosseous access can be used as an alternative route for medications or volume expansion.19
Medications and Volume Expansion
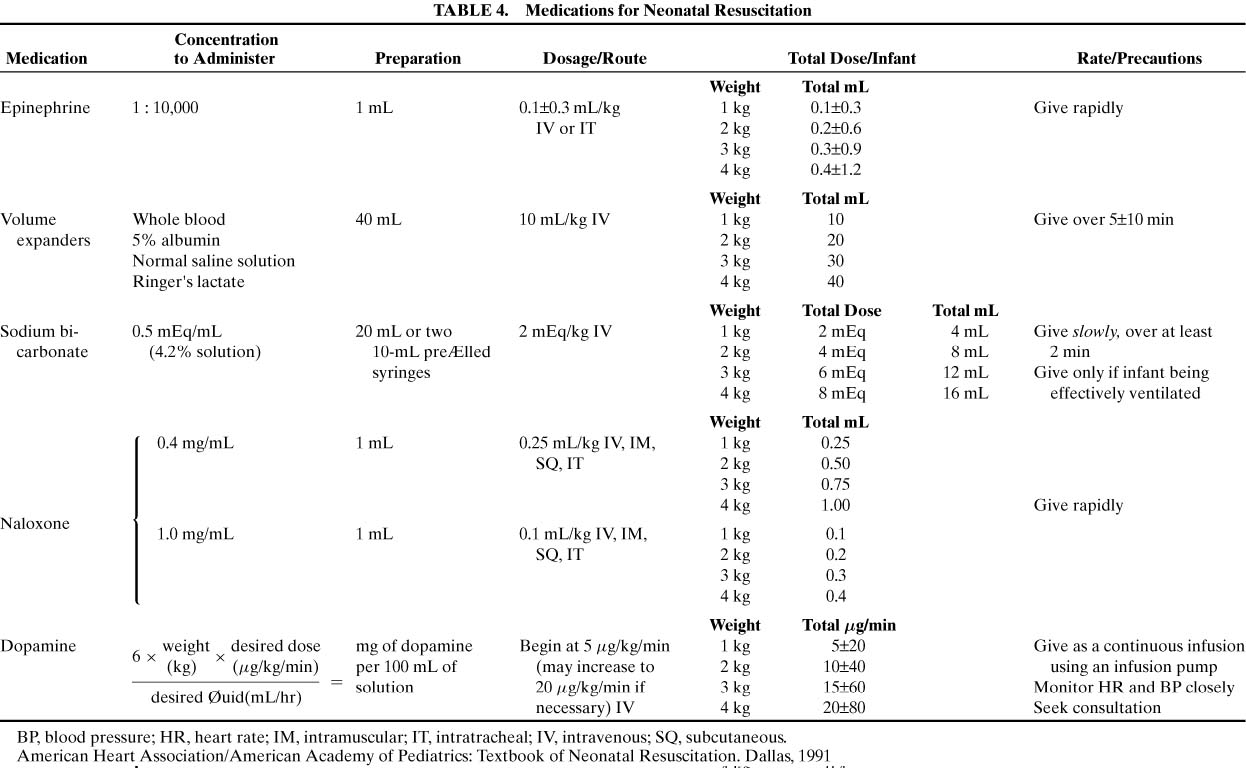
Bradycardia is often the result of inadequate lung inflation or severe hypoxia. Thus, adequate ventilation with supplemental oxygen is the most important step in correcting bradycardia. Drugs are rarely indicated in resuscitation of the newly born infant. Only if the heart rate remains at or below 60 bpm, despite a minimum of 30 seconds of adequate ventilation and chest compressions, should medications be administered. Table 4 lists the medications that may be required for neonatal resuscitation as well as their dosages and route(s) of administration.
TABLE 4. Medications for Neonatal Resuscitation
Click to View Larger Table
{kind=link}
The primary drug used in delivery room resuscitations is epinephrine. Use of epinephrine is indicated if there is asystole or if the heart rate remains below 60 bpm after 30 seconds of assisted ventilation and chest compressions. Epinephrine should be administered in a 1:10,000 dilution at a dose of 0.1 to 0.3 mL/kg. Although it can be given via an endotracheal tube, the intravenous route is preferable. If the infant’s response is suboptimal, epinephrine doses can be repeated every 3 to 5 minutes.
Hypovolemia owing to blood loss can prevent adequate response to resuscitation. Blood loss can occur with placental abruption, placenta previa, cord accidents, internal hemorrhage, twin-to-twin transfusion syndrome, or fetal-maternal hemorrhage. Clinical signs of hypovolemia include weak pulses, poor capillary filling, and low blood pressure but may not be present until 20% to 25% of the infant’s blood volume is depleted. Normal saline or Ringer’s lactate solution should be used at a starting dose of 10mL/kg given over 5 to 10 minutes. Type O-negative blood may be used instead if large-volume blood loss needs to be replaced. The dose may be repeated depending on the clinical response.
Sodium bicarbonate should be administered only after metabolic acidosis is documented despite establishment of adequate ventilation and circulation.20 Moreover, if ventilation is inadequate, respiratory acidosis will compound the metabolic acidosis as bicarbonate is converted to carbon dioxide. In a prolonged resuscitation, however, metabolic acidosis is likely to result owing to ongoing hypoxemia, peripheral vasoconstriction, and the accumulation of lactic acid. Correction of acidosis may increase pulmonary blood flow and may enhance the effect of epinephrine. A dose of 1 to 2 mEq/kg of a 0.5 mEq/mL solution should be infused slowly over a period of at least 2 minutes.
Narcotic drugs used to relieve labor pain are able to cross the placenta. Naloxone, a narcotic antagonist that does not depress respiratory activity, may be indicated in a newly born infant whose respiratory depression is due to maternal narcotic administration within 4 hours prior to delivery. It is contraindicated if there has been chronic maternal narcotic use because it may precipitate acute withdrawal symptoms in the neonate, including seizures. Although there are multiple routes of administration for naloxone, intramuscular delivery can only be performed after ventilation and circulation have been established. Repeat doses of naloxone may be necessary because the duration of action is shorter than that of the narcotics used for labor analgesia.
SPECIAL CONSIDERATIONS
Meconium-Stained Amniotic Fluid
Twelve percent of term deliveries are complicated by meconium staining of the amniotic fluid. Of these, 20% to 30% require tracheal suctioning.21 The presence of meconium is a symptom of possible significant fetal acidemia and stress. If this stress is significant in utero, the meconium may be aspirated into the airways before birth. Meconium aspiration syndrome develops in 2% to 33% of infants born through meconium-stained amniotic fluid.21,22 Meconium aspiration syndrome can be associated with the need for mechanical ventilation, persistent pulmonary hypertension of the newborn, neonatal seizures, and death. As soon as the head is delivered, the nares and pharynx should be suctioned thoroughly on the perineum or at the uterine incision regardless of whether the meconium is thin or thick. Additional suctioning may be necessary after the delivery. If the meconium is thin or if the infant is vigorous, tracheal suctioning will likely not be necessary unless respiratory distress subsequently develops. Moreover, if the infant is vigorous, visualization of the vocal cords may be difficult. As a result, esophageal or tracheal injury may occur. In fact, tracheal suctioning of the vigorous infant does not reduce the incidence of meconium aspiration syndrome or improve outcome.23 If the meconium is thick or particulate or if the infant is depressed, tracheal suctioning is necessary24 and should be performed before any stimulation or positive pressure ventilation is done. The endotracheal tube should be large enough to remove thick copious meconium yet fit easily into the trachea of the infant (see Table 3). A meconium aspirator should be placed directly onto the endotracheal tube and connected to suction at 80 to 100 cm H2O. This provides continuous suction during slow withdrawal of the endotracheal tube. If meconium is obtained, tracheal suctioning should be repeated with a clean endotracheal tube until meconium is no longer present, unless other resuscitation priorities take precedence. Once the airway is cleared, the infant can be dried and stimulated, and the stomach should be suctioned to prevent aspiration of swallowed meconium.
Extremely Premature Infant (Less Than 1000 g)
Whenever possible, these infants should be born in a perinatal center with skilled staff from the obstetric, anesthetic, and neonatal services present. The importance of an antenatal conference with the parents cannot be overemphasized. Both the physiologic immaturity and the lability of the preterm infant as well as the complications associated with preterm labor predispose this population to perinatal depression. Thus, it is not surprising that the incidence of perinatal depression is markedly increased among preterm infants. Several factors contribute to the difficult task of keeping these infants warm. They have decreased amounts of subcutaneous tissues and fat. Their skin is immature and prone to transepidermal heat and water loss, and they have a high ratio of surface area to body mass. Therefore, in addition to the usual thermoregulatory measures, some also advocate various devices such as warming blankets or polyethylene wrap to minimize heat loss in this vulnerable population of infants. These infants have decreased lung compliance, and many will require intubation either immediately or for the administration of exogenous surfactant. Care should used to avoid overventilation, which can interfere with cardiac output or, worse, lead to interstitial emphysema or air leak syndromes. Hypocarbia with aggressive ventilation can alter cerebral blood flow patterns. Excessive tidal volumes and chest compressions may increase the intracranial pressure. Excessive oxygen concentrations should also be avoided in these infants, given the concerns of reactive oxygen species and the possible associations with retinopathy of prematurity and chronic lung disease. The cerebral vasculature, particularly the germinal matrix, is very sensitive to rapid changes in intracranial pressure, blood volume, oxygen tension, and osmotic gradient. Thus, any of the interventions of advanced neonatal resuscitation may promote or exacerbate intracranial hemorrhage. The hypertension associated with epinephrine may increase the risk of intracranial hemorrhage. Rapid infusions of volume expanders or hyperosmolar solutions may be detrimental to the integrity of the cerebral vasculature.
Congenital Diaphragmatic Hernia
The incidence of congenital diaphragmatic hernia is 1 in 2000 to 5000 live births. In addition to the mortality of 40% to 50%, congenital diaphragmatic hernia is associated with the hidden mortalities of spontaneous abortion and stillbirth.25 Prenatal diagnosis is possible, but the rate of detection varies anywhere from 10% to 90%, depending on local antenatal ultrasound screening protocols and diagnostic accuracy. If the diagnosis is made prenatally, antenatal counseling with a neonatologist and a pediatric surgeon is of the utmost importance, allowing discussion of management and prognosis with the parents. If this condition is not evident prenatally, several clues may aid in the postnatal diagnosis. The abdomen may be flat or scaphoid, and bowel sounds may be audible in the chest. Heart sounds will be displaced,to the right if the defect is on the left (the more common situation) or vice versa. The infant with congenital diaphragmatic hernia may manifest only mild respiratory distress initially, but severe cyanosis and profound respiratory distress are more likely. During development, pulmonary hypoplasia occurs as a result of lung compression by the herniated bowel. Pulmonary vascular resistance remains elevated, causing the persistence of the right-to-left shunting of blood flow away from the lungs as in intrauterine life. The result is ongoing hypoxia, hypercarbia, and acidosis—the clinical syndrome of persistent pulmonary hypertension of the newborn. Intubation should be performed immediately. Furthermore, bag mask ventilation is contraindicated because air will expand the herniated bowel and exacerbate lung compression. To promote full expansion of the hypoplastic lung, a large gastric tube should be placed to low continuous suction to maintain decompression of the herniated bowel.
Abdominal Wall Defects
The risk of heat and water loss is increased in infants with either gastroschisis or omphalocele. The defect should be gently covered with plastic wrap placed over warm saline solution–soaked sterile gauze to protect the exposed bowel and to minimize heat and water loss. A clear sterile bag may be substituted for plastic wrap. Again, a large gastric tube should be placed to low continuous suction to decompress the bowel and avoid intestinal distention.
OUTCOMES AND ETHICAL ISSUES
The decision to withdraw support is undeniably one of the most challenging and difficult decisions a physician encounters. Although a significant number of infants born in unexpectedly poor condition are “successfully” resuscitated, several studies suggest that approximately half of these infants will not survive despite maximal resuscitative efforts.26,27,28 Yet, of the survivors, two thirds to three fourths are neurodevelopmentally normal at follow-up of 2 to 5 years. Furthermore, a significant number of children who develop cerebral palsy do not have significantly low Apgar scores (Table 5). From these data, it is difficult to judge when resuscitation should be discontinued. Nevertheless, Casalaz and colleagues28 have identified some indicators of poor outcome both in terms of survival and subsequent neurodevelopment that may aid in this decision-making process. These include Apgar scores at 5 and 10 minutes at or below 3, pH less than 7 in the first 2 hours of life, absence of heart beat at 5 minutes, and the occurrence of seizures in the first 24 hours of life.28 Seizures occurring in the first 12 hours are particularly ominous and early electroencephalographic abnormalities, possibly a sign of early seizures, may equally predict poor outcome.29 A lack of response to aggressive resuscitation for more than 10 minutes is associated with an extremely poor prognosis for survival and neurologically intact outcome.26,27,28 In cases in which the prognosis is dismal, ongoing communication with the family is critical. In addition, it is valuable as in the situations of the extremely low-birth-weight infants to continue to reassess new interventions and their effect on outcome data. For example, multicenter clinical trials are currently in progress in an attempt to elucidate the possible beneficial effects of selective head cooling after perinatal asphyxia.
TABLE 5. Apgar Score
Sign | 0 | 1 | 2 |
Heart rate | Absent | Below 100 | Over 100 |
Respiratory rate | Absent | Slow, irregular | Good, crying |
Muscle tone | Flaccid | Some flexion of extremities | Active motion |
Reflex irritability | No response | Grimace | Vigorous cry |
Color | Pale | Cyanotic | Completely pink |
A related issue occurs with respect to those infants at what is considered the threshold of viability. For this population of infants, survival is highly dependent on gestational age and birth weight. However, this is complicated by the fact that assessment of gestational age is accurate to only within 1 to 2 weeks. Some studies showed that nearly all infants born before 26 weeks’ gestation or with a birth weight at or below 750 g died even if they initially responded to cardiopulmonary resuscitation. In a large cohort of infants, Finer and coworkers30 observed increased mortality rates. For infants 501 to 1500 g, survival was less likely if either cardiac compressions or epinephrine was administered in the delivery room. However, again survival was dependent on gestational age: 23.9% for the 401- to 500-g infants, 44.4% for the 501- to 750-g infants, and 82.5% for the 1251- to 1500-g infants. The incidence of severe intracranial hemorrhage, although more significant in the aggressively resuscitated group, was not as dependent on gestational age. In fact, approximately half of the infants receiving aggressive intervention in the delivery room had no evidence of intracranial hemorrhage. Nearly half of the survivors delivered at a gestational age of 23 to 26 weeks develop some degree of neurodevelopmental disability, ranging from a mild learning disorder to severe cerebral palsy and/or total blindness.31,32,33 Unfortunately, it is impossible to determine in the delivery room what, if any, disabilities a particular infant will develop. Important factors include the infant’s response to therapy and the presence of certain complications such as severe intracranial hemorrhage. If there is any question of gestational age or prognosis, it seems reasonable to provide aggressive resuscitative support because this allows for further assessment of the infant. The few exceptions include infants with a confirmed gestational age of less than 23 weeks, birth weight less than 400 g, anenecephaly, or confirmed trisomy 13 or 18 syndrome. If response to resuscitation is poor or if complications develop, withdrawal of support may be provided. As previously emphasized, it is helpful to have an ongoing dialogue with the family in these circumstances. To continue to intervene appropriately, continual reassessment of the available clinical data is vital.
CONTROVERSIAL ISSUES REQUIRING FURTHER INVESTIGATION
Laryngeal Mask Airway
These masks, which fit over the laryngeal inlet, have been shown to be effective in newly born term infants, but data on their use in small preterm infants are limited.34 It has some disadvantages: providers need further training for proper use and it cannot be used for tracheal suctioning of meconium or the administration of resuscitative medications. If bag mask ventilation is ineffective or attempts at tracheal intubation are unsuccessful, the laryngeal mask airway may be an effective alternative for establishing an airway during resuscitation of the newly born infant.
Room Air Versus 100% Oxygen
Several animal studies and two human studies have shown that room air might be as beneficial as 100% oxygen for neonatal resuscitation. Saugstad and colleagues35 found that infants in the room air group had a shorter time either to first cry or to sustained respiratory pattern and a significantly higher Apgar score at 1 minute compared with those in the 100% oxygen group. In a similar study, Ramji and associates36 observed that, despite similar Apgar scores at 1 minute, infants in the room air group had higher 5-minute Apgar scores and shorter time to first cry compared with those in the 100% oxygen group. Intuitively, 100% oxygen seems appealing to deliver oxygen to hypoxic tissues and in fact it may have advantages such as the promotion of pulmonary vasodilatation. However, the disadvantages are currently being delineated. There may be a delay in spontaneous ventilation, increased oxygen consumption, or alterations in cerebral circulation. Much of the focus has concentrated on the generation of oxygen free radicals and the effect that oxidative stress can have on cell growth and apoptosis.37,38,39 Of concern is the fact that markers of increased oxidative stress may be present not only immediately after birth but also as long as 28 days afterward.40 However, the clinical significance of the existence of these markers in human neonates is not known. Also, despite the short-term outcome differences in the human newborn resuscitation trials, there was no improvement in the ultimate clinical outcome. More evidence is required to show that room air is superior to 100% oxygen or that 100% oxygen is significantly more detrimental than room air in the long term. The goal of supplemental oxygen is normoxia. Again, adequate ventilation cannot be overemphasized. Thus, the current body of evidence supports the use of 100% oxygen in the acute resuscitation of the newly born infant. Oxygen use should subsequently be monitored by pulse oximetry and/or blood gases and individualized accordingly.
High-Dose Epinephrine via Endotracheal Tube
Less effective levels may occur when epinephrine is administered intratracheally than intravenously. The hypertensive effect is exaggerated with doses of epinephrine higher than those currently recommended by the American Heart Association/American Academy of Pediatrics. However, in animal studies, these doses are also associated with lower cardiac output, myocardial damage, and an increased risk of intracranial hemorrhage.41 Of particular concern, then, is the use of higher-dose epinephrine in premature infants, a population already at risk of intracranial hemorrhage. Thus, the current guidelines recommend the same dose of epinephrine, if needed in neonatal resuscitation, whether delivered intratracheally or intravenously.
REFERENCES
Saugstad OD: Practical aspects of resuscitating newborn infants. Eur J Pediatr 157(Suppl 1):S11, 1998 |
|
Strang LB: Fetal lung liquid: Secretion and reabsorption. Physiol Rev 71:991, 1991 |
|
Alcorn D, Adamson TM, Lambert TF, et al: Morphological effects of chronic tracheal ligation and drainage in the fetal lamb lung. J Anat 123:649, 1977 |
|
Harding R, Sigger JN, Wickham PJ, et al: The regulation of flow of pulmonary fluid in fetal sheep. Respir Physiol 57:47, 1984 |
|
Nelson NM: Respiration and circulation before birth. In Smith CA, Nelson NM (eds): The Physiology of the Newborn Infant. pp 15, 117 Springfield, IL, Charles C Thomas, 1976 |
|
Kitterman JA, Ballard PL, Clements JA, et al: Tracheal fluid in fetal lambs: Spontaneous decrease prior to birth. J Appl Physiol 47:985, 1979 |
|
O’Brodovich H: Epithelial ion transport in fetal and perinatal lung. Am J Physiol 261:C555, 1991 |
|
Bland RD, Carlton DP, Scheerer RG, et al: Lung fluid balance in lambs before and after premature birth. J Clin Invest 84:568, 1989 |
|
Bland RD, Bressack MA, McMillan DD: Labor decreases the lung water content of newborn rabbits. Am J Obstet Gynecol 135:364, 1979 |
|
Barker PM, Gowen CW, Lawson EE, et al: Decreased sodium ion absorption across nasal epithelium of very premature infants with respiratory distress syndrome. J Pediatr 130:373, 1997 |
|
Gowen CW Jr, Lawson EE, Gingras J, et al: Electrical potential difference and ion transport across nasal epithelium of term neonates: Correlation with mode of delivery, transient tachypnea of the newborn, and respiratory rate. J Pediatr 113:121, 1988 |
|
Levin D, Rudolph A, Heymann M, et al: Morphological development of the pulmonary vascular bed in fetal lambs. Circulation 53:144, 1976 |
|
Haworth SG, Hall SM, Chew M, et al: Thinning of fetal pulmonary arterial wall and postnatal remodelling: Ultrastructural studies on the respiratory unit arteries of the pig. Virchows Arch 411:161, 1987 |
|
Meyrick B, Reid L: The effect of continued hypoxia on rat pulmonary arterial circulation. An ultrastructural study Lab Invest 38:188, 1978 |
|
World Health Organization: World Health Report, 1995. p 21, Geneva, Switzerland, WHO, 1997 |
|
Perlman JM, Risser R: Cardiopulmonary resuscitation in the delivery room. Arch Paediatr Adolesc Med 149:20, 1995 |
|
American Academy of Pediatrics/American Heart Association: Textbook of Neonatal Resuscitation. Dallas, American Heart Association/American Academy of Pediatrics, 1994 |
|
Aziz HF, Martin JB, Moore JJ: The pediatric disposable end-tidal carbon dioxide detector role in endotracheal intubation in newborns. J Perinatol 19:110, 1999 |
|
Ellemunter H, Simma B, Trawoger R, et al: Intraosseous lines in preterm and full term neonates. Arch Dis Child Fetal Neonatal Ed 80:F74, 1999 |
|
Hein HA: The use of sodium bicarbonate in neonatal resuscitation: Help or harm? Pediatrics 91:496, 1993 |
|
Wiswell TE, Fuloria M: Resuscitation of the meconium-stained infant and prevention of meconium aspiration syndrome. J Perinatol 19:234, 1999 |
|
Wiswell TE, Tuggle JM, Turner BS: Meconium aspiration syndrome: Have we made a difference? Pediatrics 85:715, 1990 |
|
Wiswell TE: Meconium in the Delivery Room Trial Group: Delivery room management of the apparently vigorous meconium-stained neonate: Results of the multicenter collaborative trial. Pediatrics 105:1, 2000 |
|
Greenough A: Meconium aspiration syndrome: Prevention and treatment. Early Hum Dev 41:183, 1995 |
|
Davis CF, Sabharwal AJ: Management of congenital diaphragmatic hernia. Arch Dis Child Fetal Neonatal Ed 79:F1, 1998 |
|
Jain L, Ferre C, Vidyasagar D, et al: Cardiopulmonary resuscitation of apparently stillborn infants. J Pediatr 118:778, 1991 |
|
Yeo CL, Tudehope DI: Outcome of resuscitated apparently stillborn infants: A ten year review. J Paediatr Child Health 30:129, 1994 |
|
Casalaz DM, Marlow N, Speidel BD: Outcome of resuscitation following unexpected apparent stillbirth. Arch Dis Child Fetal Neonatal Ed 78:F112, 1998 |
|
Van Lieshout HB, Jacobs JW, Rotteveel JJ, et al: The prognostic value of the EEG in asphyxiated newborns. Acta Neurol Scand 91:203, 1995 |
|
Finer NN, Horbar JD, Carpenter JH: Cardiopulmonary resuscitation in the very low birth weight infant: The Vermont Oxford network experience. Pediatrics 104:428, 1999 |
|
Emsley HCA, Wardle SP, Sims DG, et al: Increased survival and deteriorating developmental outcome in 23 to 25 week old gestation infants, 1990-4 compared with 1984-9. Arch Dis Child Fetal Neonatal Ed 78:F99, 1998 |
|
O’Shea TM, Klinepeter KL, Goldstein DJ, et al: Survival and developmental disability in infants with birth weights of 501 to 800 grams, born between 1979 and 1994. Pediatrics 100:982, 1997 |
|
Lefebvre F, Glorieux J, St-Laurent-Gagnon T: Neonatal survival and disability rate at 18 months for infants born between 23 and 28 weeks of gestation. Am J Obstet Gynecol 174:833, 1996 |
|
Gandini D, Brimacombe JR: Neonatal resuscitation with the laryngeal mask airway in normal and low birth weight infants. Anesth Analg 89:642, 1999 |
|
Saugstad OD, Rootwelt T, Aalen O: Resuscitation of asphyxiated newborn infants with room air or oxygen: An international controlled trial: The Resair 2 study. Pediatrics 102:E1, 1998 |
|
Ramji S, Ahuja S, Thirupuram S, et al: Resuscitation of asphyxic newborn infants with room air or 100% oxygen. Pediatr Res 34:809, 1993 |
|
Kutzsche S, Kirkeby OJ, Rise IR, et al: Effects of hypoxia and reoxygenation with 21% and 100% oxygen on cerebral nitric oxide concentration and microcirculation in newborn piglets. Biol Neonate 76:153, 167 1999 |
|
Halliwell B, Aruoma OI: DNA damage by oxygen-derived species: Its mechanism and measurement in mammalian systems. FEBS Lett 281:9, 1991 |
|
Conner EM, Grisham MB: Inflammation, free radicals, and antioxidants. Nutrition 12:274, 1996 |
|
Vento M, Asensi M, Sastre J, et al: Resuscitation with room air instead of 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics 107:642, 2001 |
|
Burchfield DJ, Preziosi MP, Lucas VW, et al: Effect of graded doses of epinephrine during asphyxia-induced bradycardia in newborn lambs. Resuscitation 25:235, 1993 |