Assessment of Gestational Age by Ultrasound
Authors
INTRODUCTION
Gestational age, synonymous with menstrual age, is defined in weeks beginning from the first day of the last menstrual period (LMP) prior to conception. Accurate determination of gestational age is fundamental to obstetric care and is important in a variety of situations. For example, antenatal test interpretation may be dependent on gestational age. Specifically, the level of α-fetoprotein in both amniotic fluid and maternal serum is related to gestational age and when dates are inaccurate test results will be incorrect and misleading.1 Similarly, the magnitude of increased optical density above baseline at 450 nm (delta OD 450) by amniotic fluid spectrophotometric measurement is used to predict the severity of fetal hemolytic disease in pregnancies complicated by rhesus isoimmunization.2,3 Test results are interpreted based on Liley's zones relative to gestational age. Again, inaccurate assessment of gestational age will lead to errors in assessing the severity of fetal sensitization by the delta OD 450. Fetal growth assessment, either clinically or by ultrasound evaluation, also relies on accurate assessment of gestational age. Fetal growth retardation or macrosomia may be missed or incorrectly diagnosed owing to errors in gestational age assignment. Interpretation of antenatal biophysical testing (non-stress tests and biophysical profiles) may be subject to variation with gestational age as well. Fetal heart rate reactivity and fetal breathing develop with advancing gestational age; therefore, the absence of these biophysical parameters may be interpreted as abnormal for fetuses in whom the gestational age has been overestimated. Obstetric management is also dependent on gestational age. Proper decisions regarding presumed preterm labor or postdate pregnancies are only possible when gestational age is accurately estimated. Likewise, timing of repeat cesarean section requires accurate assessment of dates.4,5 Ultrasound is a reliable method for establishing the length of pregnancy and in this way can improve obstetric care.
METHODS OF GESTATIONAL AGE ASSESSMENT
In the past gestational age was established by a combination of the historical information and the physical examination. Reliance was placed on the menstrual history and the maternal sensation of fetal movement (“quickening”). Other factors include assessment of uterine size by bimanual examination in the first trimester, initial detection of fetal heart tones by Doppler (10–12 weeks) or auscultation (19–21 weeks), and uterine fundal height measurement. However, both the history and the findings on physical examination are fraught with error, even in the best of circumstances (Table 1).6,7,8 It has been estimated that 20% to 40% of women cannot relate the LMP with certainty.6,7 Some of the reasons for this uncertainty include oligomenorrhea, metrorrhagia, bleeding in the first trimester of pregnancy, pregnancy following use of oral contraceptives or intrauterine devices, and becoming pregnant in the postpartum period. Hertz and co-workers9 reported that menstrual history was considered reliable in only 18% of women. In another report, even among women with known LMP, neonatal age assessment differed markedly from that assigned by certain menstrual dates in 15%.8 Physical examination also tends to be inaccurate, especially with advancing gestational age.10 Bimanual examination in the first trimester may be accurate within ±2 weeks; however, fundal height measurement, which is more commonly used to assess gestational age, is only accurate within ±4 to 6 weeks. Clearly, the inaccuracies of history and physical examination may limit their usefulness in assessment of gestational age. Methods that assess the time of ovulation or conception can accurately establish gestational age.11,12,13,14 Timed ovulation, either by basal body temperature recording or semiquantitative assessment of luteinizing hormone surge, predicts gestational age within ±4 to 6 days. Ovulation induction with agents such as clomiphene citrate and Pergonal, also accurately predicts gestational age. In vitro fertilization, with known date of conception, is likely the most accurate means of predicting gestational age (±1 day). However, in most pregnancies, the date of ovulation or conception cannot be as accurately predicted as outlined above and gestational age must be established by other methods.
TABLE 1.Clinical Predictors of Gestational Age
| Estimated Range for |
Parameter | 95% of Cases |
In vitro fertilization | ±1 day |
Ovulation induction | ±4–6 days |
Luteinizing hormone surge indicator | ±4–6 days |
Basal body temperature | ±4–6 days |
Certain menstrual history | ±2 weeks |
Bimanual examination (first trimester) | ±2 weeks |
First fetal heart tones by Doppler | ±2 weeks |
“Quickening” | ±2–4 weeks |
First fetal heart tones by auscultation | ±2–4 weeks |
Fundal height measurement between | ±4 weeks |
18 and 32 weeks' gestation |
|
Fundal height measurement after 32 | ±4–6 weeks |
weeks' gestation |
|
The advent of ultrasound has allowed a more direct means of assessing fetal structures and development. Measurements of a wide variety of parameters have been devised to establish gestational age. Ultrasound assessment of gestational age is feasible in a majority of pregnancies and may be used to establish gestational age with greater accuracy than physical examination. In the first trimester, gestational sac mean diameter and crown-rump length measurements have become the primary means of evaluating gestational age.15,16,17,18,19 In the second and third trimesters, fetal head, body, and extremity measurements have been commonly used to assess gestational age. Those parameters most commonly measured include biparietal diameter,20,21,22,23,24,25,26,27,28 head circumference,29,30 abdominal circumference,31,32,33,34,35 and femur length.36,37,38,39 Although numerous other parameters have been measured and related to gestational age, few offer any improvement in the accuracy of gestational age assessment.40,41,42,43,44,45,46 In this chapter, the most widely used and accepted ultrasound-derived fetal growth parameters are discussed and a review of their accuracies and potential errors is presented.
First-Trimester Assessment
In the first trimester, the gestational sac mean diameter and crown-rump length are used to establish fetal age. Both parameters are useful because each measures a different aspect of the first-trimester pregnancy and may be used at different times during the first trimester.
GESTATIONAL SAC MEAN DIAMETER.
The gestational sac is the first identifiable structure routinely imaged in the first trimester. It is identified by transabdominal ultrasound as early as 5 weeks' gestation and may be seen as early as 4 weeks' gestation by transvaginal ultrasound.15,16,47 The gestational sac is an echo-free space containing the fluid, embryo, and extraembryonic structures. The sac is measured inside the hyperechoic rim, including only the echo-free space (Fig. 1). The gestational sac is imaged first in the longitudinal plane, obtaining long axis and anteroposterior measurements perpendicular to each other. Then, in the transverse plane at the level of the anteroposterior measurement, the width measurement is obtained. The three measurements are averaged to obtain the gestational sac mean diameter. Table 2 compares gestational ages from 5 to 12 weeks with the gestational sac mean diameters.15 The accuracy of gestational sac measurement as a predictor of gestational age has been evaluated in only one report and was found to be approximately ±1 week.16
TABLE 2. Gestational Sac Mean Diameter Measurements Relative to Gestational Age
Gestational Sac | Gestational Age | Gestational Sac | Gestational Age |
Mean Diameter (mm) | (weeks) | Mean Diameter (mm) | (weeks) |
10 | 5.0 | 30 | 7.9 |
11 | 5.2 | 31 | 8.0 |
12 | 5.3 | 32 | 8.2 |
13 | 5.5 | 33 | 8.3 |
14 | 5.6 | 34 | 8.5 |
15 | 5.8 | 35 | 8.6 |
16 | 5.9 | 36 | 8.8 |
17 | 6.0 | 37 | 8.9 |
18 | 6.2 | 38 | 9.0 |
19 | 6.3 | 39 | 9.2 |
20 | 6.5 | 40 | 9.3 |
21 | 6.6 | 41 | 9.5 |
22 | 6.8 | 42 | 9.6 |
23 | 6.9 | 43 | 9.8 |
24 | 7.0 | 44 | 9.9 |
25 | 7.2 | 45 | 10.0 |
26 | 7.3 | 46 | 10.2 |
27 | 7.5 | 47 | 10.3 |
28 | 7.6 | 48 | 10.5 |
29 | 7.8 | 49 | 10.6 |
(Hellman LF, Kobayashi M, Fillisti L et al: Growth and development of the human fetus prior to the twentieth week of gestation. Am J Obstet Gynecol 103:789, 1969. Reprinted with permission of CV Mosby, St. Louis.)
CROWN-RUMP LENGTH.
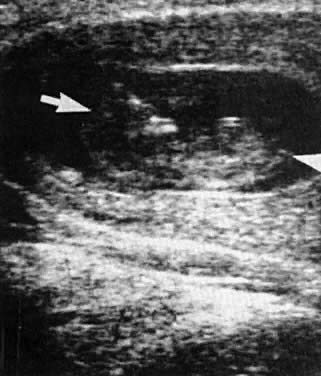
The crown-rump length (CRL) is a measurement of the embryo, usually identified at 6 to 7 weeks' gestation.17,48 The embryo is measured along its longest axis to obtain the CRL measurement (Fig. 2). Crown-rump length may be used to accurately date pregnancy between 7 and 13 weeks' gestation. The technique involves measurement of the fetal length from the tip of the cephalic pole to the tip of the caudal pole. The fetus should be at rest and assuming its natural curvature. At 5 to 6 weeks' gestation, distinct landmarks cannot always be identified but heart motion usually can be detected centrally. As the pregnancy continues, the head can be easily identified from the rest of the body. After 12 weeks' gestation excessive curvature of the fetus may lead to erroneous shortening of CRL measurement; therefore, other measurements, such as the biparietal diameter, should be used to estimate gestational age.
The correlation between sonographic CRL values and dates was first reported by Robinson and Fleming, who obtained CRLs in pregnancies of women with certain menstrual histories.17 Drumm and associates18 performed a similar study; however, their patients fulfilled more stringent dating criteria. These early studies suggested that gestational age assessment by CRL was extremely accurate, approaching ±3 to 4 days. Subsequent studies have suggested that the CRL is somewhat less accurate; however, the accuracy is still within ±5 to 7 days.49,50,51,52 Most recently, MacGregor and co-workers19 evaluated CRL measurements in pregnancies of women with known dates of ovulation and reported data that differed from those of the previous two studies. Table 3 summarizes the results of these three studies evaluating gestational age relative to CRL.
TABLE 3.Crown-Rump Length Measurements Relative to Gestational Age in Three Studies
| MacGregor et | Robinson and | Drumm et |
Crown-Rump | alGestational Age | FlemingGestational Age | alGestational Age |
Length(cm) | (Weeks + Days) | (Weeks + Days) | (Weeks + Days) |
1.0 | 7 + 5 | 7 + 0 | 6 + 6 |
1.1 | 7 + 6 | 7 + 1 | 7 + 1 |
1.2 | 8 + 0 | 7 + 3 | 7 + 2 |
1.3 | 8 + 1 | 7 + 4 | 7 + 3 |
1.4 | 8 + 1 | 7 + 5 | 7 + 4 |
1.5 | 8 + 2 | 7 + 6 | 7 + 5 |
1.6 | 8 + 3 | 8 + 0 | 7 + 6 |
1.7 | 8 + 4 | 8 + 1 | 8 + 0 |
1.8 | 8 + 5 | 8 + 2 | 8 + 1 |
1.9 | 8 + 5 | 8 + 3 | 8 + 2 |
2.0 | 8 + 6 | 8 + 4 | 8 + 3 |
2.1 | 9 + 0 | 8 + 5 | 8 + 4 |
2.2 | 9 + 1 | 8 + 6 | 8 + 5 |
2.3 | 9 + 1 | 8 + 6 | 8 + 6 |
2.4 | 9 + 2 | 9 + 0 | 9 + 0 |
2.5 | 9 + 3 | 9 + 1 | 9 + 1 |
2.6 | 9 + 4 | 9 + 2 | 9 + 2 |
2.7 | 9 + 4 | 9 + 3 | 9 + 3 |
2.8 | 9 + 5 | 9 + 3 | 9 + 3 |
2.9 | 9 + 6 | 9 + 4 | 9 + 4 |
3.0 | 9 + 6 | 9 + 5 | 9 + 5 |
3.1 | 10 + 0 | 9 + 6 | 9 + 6 |
3.2 | 10 + 1 | 9 + 6 | 10 + 0 |
3.3 | 10 + 2 | 10 + 0 | 10 + 0 |
3.4 | 10 + 2 | 10 + 1 | 10 + 1 |
3.5 | 10 + 3 | 10 + 1 | 10 + 2 |
3.6 | 10 + 4 | 10 + 2 | 10 + 3 |
3.7 | 10 + 4 | 10 + 3 | 10 + 3 |
3.8 | 10 + 5 | 10 + 3 | 10 + 4 |
3.9 | 10 + 6 | 10 + 4 | 10 + 5 |
4.0 | 10 + 6 | 10 + 5 | 10 + 5 |
4.1 | 11 + 0 | 10 + 5 | 10 + 6 |
4.2 | 11 + 1 | 10 + 6 | 11 + 0 |
4.3 | 11 + 1 | 11 + 0 | 11 + 0 |
4.4 | 11 + 2 | 11 + 0 | 11 + 1 |
4.5 | 11 + 3 | 11 + 1 | 11 + 2 |
4.6 | 11 + 3 | 11 + 1 | 11 + 2 |
4.7 | 11 + 4 | 11 + 2 | 11 + 3 |
4.8 | 11 + 5 | 11 + 3 | 11 + 4 |
4.9 | 11 + 5 | 11 + 3 | 11 + 4 |
5.0 | 11 + 6 | 11 + 4 | 11 + 5 |
5.1 | 12 + 0 | 11 + 4 | 11 + 5 |
5.2 | 12 + 0 | 11 + 5 | 11 + 6 |
5.3 | 12 + 1 | 11 + 5 | 12 + 0 |
5.4 | 12 + 1 | 11 + 6 | 12 + 0 |
5.5 | 12 + 2 | 11 + 6 | 12 + 1 |
5.6 | 12 + 3 | 12 + 0 | 12 + 2 |
5.7 | 12 + 3 | 12 + 1 | 12 + 2 |
5.8 | 12 + 4 | 12 + 1 | 12 + 3 |
5.9 | 12 + 4 | 12 + 2 | 12 + 3 |
6.0 | 12 + 5 | 12 + 2 | 12 + 4 |
6.1 | 12 + 6 | 12 + 3 | 12 + 5 |
6.2 | 12 + 6 | 12 + 3 | 12 + 5 |
6.3 | 13 + 0 | 12 + 4 | 12 + 6 |
6.4 | 13 + 0 | 12 + 4 | 12 + 6 |
6.5 | 13 + 1 | 12 + 5 | 13 + 0 |
6.6 | 13 + 2 | 12 + 5 | 13 + 0 |
(MacGregor SN, Tamura RK, Sabbagha RE et al: Underestimation of gestational age by conventional crown-rump length growth curves.Obstet Gynecol 70:344, 1987.Reprinted with permission of American College of Obstetricians and Gynecologists)
Variations in the measurement of CRL can be attributed to differences in fetal growth patterns. Such differences are related to factors similar to those that influence birth weight curves, including maternal age and parity, prepregnancy maternal weight, geographic location, and population characteristics.53,54,55 Indeed, the existence of subpopulations with altered CRL growth patterns has been suggested by previous reports.56,57 Technical factors can also lead to errors in CRL measurements. These include incorporation of the yolk sac or lower limbs in the CRL measurement, excessive curling or extension of the fetus, and tangential section of the trunk.17 Despite these potential sources of error, CRL measurement is an accurate and useful method of assessing gestational age in the first trimester.
Second- and Third-Trimester Assessment
BIPARIETAL DIAMETER.
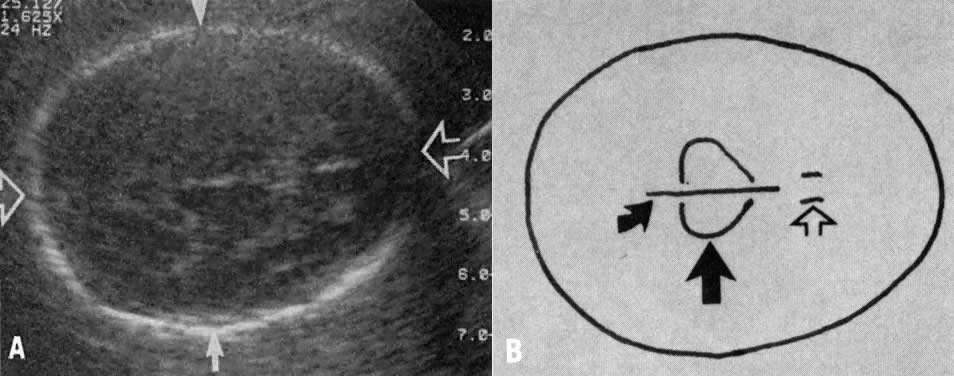
The biparietal diameter (BPD) is one of the most commonly measured parameters in the fetus. Campbell was the first investigator to link fetal BPD to gestational age20; however, since this original report, numerous publications on this subject have appeared in the literature.20,21,22,23,24,25,26,27,28,58,59,60,61,62,63 The BPD may be rapidly and reproducibly measured by ultrasound examination from 12 weeks' gestation until the end of pregnancy. The BPD is imaged in the transaxial plane of the fetal head at a level depicting thalami in the midline, equidistant from the temporoparietal bones and usually the cavum septum pellucidum anteriorly (Fig. 3).58,59 Although several methods have been used to measure BPD, the most commonly accepted method is measurement from leading edge to leading edge (outer-to-inner) (see Fig. 3).
Gestational age assignment is based on the mean BPD; however, a single BPD encompasses a range of ages in which most fetuses of that size are most likely to fall (Table 4).23 The accuracy of fetal age assessment based on BPD is dependent on gestational age.22,23,27,28,51,58 Between 12 and 26 weeks' gestation, the BPD is accurate to within ±10 to 11 days. After 26 weeks' gestation, the accuracy of BPD measurement progressively decreases and is ±3 weeks near term. A number of factors may contribute to variation or inaccuracy in the BPD measurement. Biologic variation, for example, may occur because of differences in maternal age, parity, prepregnancy weight, geographic location, and specific population characteristics. Technical factors including interobserver error, different techniques of measurements, and single versus multiple measurements may likewise influence the accuracy of BPD in assessing gestational age.60,61,62 Although most dating curves show the same general relationship between BPD and gestational age, there are often significant differences in gestational age assignment for any particular BPD measurement. Furthermore, BPD measurement is most accurate in assessing gestational age when the head shape is appropriately ovoid. If the head is unusually rounded (brachycephalic) or unusually elongated (dolicocephalic), BPD measurements would overestimate or underestimate gestational age, respectively. To determine whether head shape is appropriate, Hadlock and co-workers64 compared the BPD and the frontooccipital diameter. The ratio of these diameters is called the cephalic index (CI), with a mean value of 0.78 and a normal range (±2 SD) of 0.70 to 0.86. In the fetus with an abnormal cephalic index (noted in <2% of fetuses prior to 26 weeks' gestation), dates may be estimated more accurately using other fetal parameters, such as head circumference.
TABLE 4. Biparietal Diameter Measurements Relative to Gestational Age
| Menstrual |
| Menstrual |
BPD (cm) | Age (weeks) | BPD (cm) | Age (weeks) |
2.6 | 13.6 | 6.4 | 25 |
2.7 | 13.8 | 6.5 | 25.3 |
2.8 | 14 | 6.6 | 25.7 |
2.9 | 14.2 | 6.7 | 26 |
3.0 | 14.4 | 6.8 | 26.3 |
3.1 | 14.7 | 6.9 | 26.7 |
3.2 | 15 | 7.0 | 27 |
3.3 | 15.2 | 7.1 | 27.3 |
3.4 | 15.4 | 7.2 | 27.7 |
3.5 | 15.7 | 7.3 | 28 |
3.6 | 16 | 7.4 | 28.3 |
3.7 | 16.3 | 7.5 | 28.7 |
3.8 | 16.7 | 7.6 | 29 |
3.9 | 17 | 7.7 | 29.4 |
4.0 | 17.3 | 7.8 | 30 |
4.1 | 17.7 | 7.9 | 30.4 |
4.2 | 18 | 8.0 | 31 |
4.3 | 18.3 | 8.1 | 31.4 |
4.4 | 18.7 | 8.2 | 32 |
4.5 | 19 | 8.3 | 32.3 |
4.6 | 19.3 | 8.4 | 32.7 |
4.7 | 19.7 | 8.5 | 33 |
4.8 | 20 | 8.6 | 33.4 |
4.9 | 20.3 | 8.7 | 34 |
5.0 | 20.7 | 8.8 | 34.6 |
5.1 | 21 | 8.9 | 35.3 |
5.2 | 21.3 | 9.0 | 36 |
5.3 | 21.6 | 9.1 | 36.4 |
5.4 | 21.8 | 9.2 | 37.3 |
5.5 | 22 | 9.3 | 37.7 |
5.6 | 22.3 | 9.4 | 39 |
5.7 | 22.7 | 9.5 | 40 |
5.8 | 23 | 9.6 | 40.3 |
5.9 | 23.3 | 9.7 | 40.7 |
6.0 | 23.7 | 9.8 | 41 |
6.1 | 24 | 9.9 | 41.7 |
6.2 | 24.3 | 10.0 | 42.3 |
6.3 | 24.7 |
|
|
(Sabbagha RE, Hughey M: Standardization of sonar cephalometry and gestational age. Obstet Gynecol 52:402, 1978. Reprinted with permission of American College of Obstetricians and Gynecologists)
HEAD CIRCUMFERENCE.
The head circumference (HC) measurement may be used to estimate gestational age in a similar manner to BPD measurement (Table 5).30 Although tracing of the outer perimeter of the head (by trackball on the ultrasonic equipment or by digitizer) is the most reliable means of measuring HC, the following formula using biparietal and fronto-occipital diameters may be used to calculate HC with a maximum error of 6%:63,65
TABLE 5.Head Circumference Measurements Relative to Gestational Age
Head | Menstrual | Head | Menstrual |
Circumference | Age | Circumference | Age |
(cm) | (weeks) | (cm) | (weeks) |
8.0 | 13.4 | 22.5 | 24.4 |
8.5 | 13.7 | 23.0 | 24.9 |
9.0 | 14.0 | 23.5 | 25.4 |
9.5 | 14.3 | 24.0 | 25.9 |
10.0 | 14.6 | 24.5 | 26.4 |
10.5 | 15.0 | 25.0 | 26.9 |
11.0 | 15.3 | 25.5 | 27.5 |
11.5 | 15.6 | 26.0 | 28.0 |
12.0 | 15.9 | 26.5 | 28.1 |
12.5 | 16.3 | 27.0 | 29.2 |
13.0 | 16.6 | 27.5 | 29.8 |
13.5 | 17.0 | 28.0 | 30.3 |
14.0 | 17.3 | 28.5 | 31.0 |
14.5 | 17.7 | 29.0 | 31.6 |
15.0 | 18.1 | 29.5 | 32.2 |
15.5 | 18.4 | 30.0 | 32.8 |
16.0 | 18.8 | 30.5 | 33.5 |
16.5 | 19.2 | 31.0 | 34.2 |
17.0 | 19.6 | 31.5 | 34.9 |
17.5 | 20.0 | 32.0 | 35.5 |
18.0 | 20.4 | 32.5 | 36.3 |
18.5 | 20.8 | 33.0 | 37.0 |
19.0 | 21.2 | 33.5 | 37.7 |
19.5 | 21.6 | 34.0 | 38.5 |
20.0 | 22.1 | 34.5 | 39.2 |
20.5 | 22.5 | 35.0 | 40.0 |
21.0 | 23.0 | 35.5 | 40.8 |
21.5 | 23.4 | 36.0 | 41.6 |
22.0 | 23.9 |
|
|
(Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal head circumference: Relation to menstrual age.AJR 138:649, 1982.Reprinted with permission of Williams & Wilkins, Baltimore.)
The accuracy of gestational age estimation by HC measurement is comparable with that of BPD measurement.30 However, in fetuses with abnormal head shape, either brachycephaly or dolicocephaly, HC may be a more accurate predictor of fetal age than BPD.30,65
ABDOMINAL CIRCUMFERENCE.
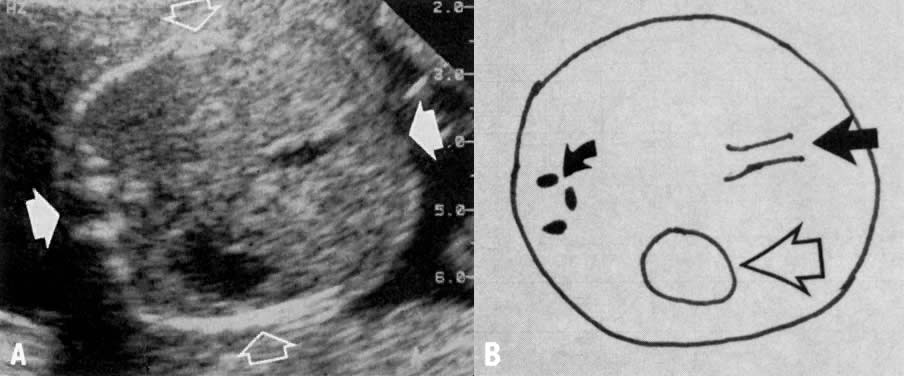
Measurement of the fetal abdominal circumference (AC) is obtained in the transaxial view of the fetal abdomen. The AC is measured at the level of the fetal liver, using the umbilical portion of the left portal vein as a landmark (Fig. 4). The fetal stomach is at the same level, which is slightly caudad to the fetal heart and cephalad to the kidneys. The AC measurement is taken from the outermost aspects of the fetal soft tissues. Measurement of the AC is performed in the same manner as that of the HC, that is, by (1) tracing the outer perimeter of the AC by the trackball on the ultrasonic equipment or by digitizer or (2) the same equation as for HC using transverse and anteroposterior diameters of the fetal abdomen. The AC may be used to estimate gestational age (Table 6) but is less accurate than head measurements (BPD or HC).33 Similar to head measurements, the accuracy of AC in estimating gestational age is greatest in the second trimester, with decreasing accuracy near term. Biologic variation and technical factors may contribute to the inaccuracy of AC measurements in a manner similar to that previously described for bi-parietal diameters. Of particular note, the abdominal circumference is the growth parameter most commonly affected in pregnancies complicated by abnormal fetal growth patterns.33 A macrosomic fetus will have increased AC relative to gestational age, and an asymmetrically growth-retarded fetus will have diminished AC measurements. Variation in AC measurements in macrosomic and growth-retarded fetuses is due to differences in liver size and width of subcutaneous tissue in these two types of abnormal growth patterns. Thus, estimation of gestational age by AC will lead to inaccuracies in fetuses displaying either of these growth patterns. However, the HC/AC ratio may be useful as a predictor of head-to-abdomen symmetry or asymmetry in order to identify the type of abnormal growth (Table 7).66
TABLE 6. Abdominal Circumference Measurements Relative to Gestational Age
Abdominal | Menstrual | Abdominal | Menstrual |
Circumference | Age | Circumference | Age |
(cm) | (weeks) | (cm) | (weeks) |
10.0 | 15.6 | 23.5 | 27.7 |
10.5 | 16.1 | 24.0 | 28.2 |
11.0 | 16.5 | 24.5 | 28.7 |
11.5 | 16.9 | 25.0 | 29.2 |
12.0 | 17.3 | 25.5 | 29.7 |
12.5 | 17.8 | 26.0 | 30.1 |
13.0 | 18.2 | 26.5 | 30.6 |
13.5 | 18.6 | 27.0 | 31.1 |
14.0 | 19.1 | 27.5 | 31.6 |
14.5 | 19.5 | 28.0 | 32.1 |
15.0 | 20.0 | 28.5 | 32.6 |
15.5 | 20.4 | 29.0 | 33.1 |
16.0 | 20.8 | 29.5 | 33.6 |
16.5 | 21.3 | 30.0 | 34.1 |
17.0 | 21.7 | 30.5 | 34.6 |
17.5 | 22.2 | 31.0 | 35.1 |
18.0 | 22.6 | 31.5 | 35.6 |
18.5 | 23.1 | 32.0 | 36.1 |
19.0 | 23.6 | 32.5 | 36.6 |
19.5 | 24.0 | 33.0 | 37.1 |
20.0 | 24.5 | 33.5 | 37.6 |
20.5 | 24.9 | 34.0 | 38.1 |
21.0 | 25.4 | 34.5 | 38.7 |
21.5 | 25.9 | 35.0 | 39.2 |
22.0 | 26.3 | 35.5 | 39.7 |
22.5 | 26.8 | 36.0 | 40.2 |
23.0 | 27.3 | 36.5 | 40.8 |
(Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal abdominal circumference as a predictor of menstrual age. AJR 139:367, 1982. Reprinted with permission of Williams & Wilkins, Baltimore.)
TABLE 7. Head Circumference to Abdominal Circumference Ratios Relative to Gestational Age
Gestational Age | HC/AC Ratio | ||
(weeks) | 5th percentile | Mean | 95th percentile |
13–14 | 1.14 | 1.23 | 1.31 |
15–16 | 1.05 | 1.22 | 1.39 |
17–18 | 1.07 | 1.18 | 1.29 |
19–20 | 1.09 | 1.18 | 1.26 |
21–22 | 1.06 | 1.15 | 1.25 |
23–24 | 1.05 | 1.13 | 1.21 |
25–26 | 1.04 | 1.13 | 1.22 |
27–28 | 1.05 | 1.13 | 1.22 |
29–30 | 0.99 | 1.10 | 1.21 |
31–32 | 0.96 | 1.07 | 1.17 |
33–34 | 0.96 | 1.04 | 1.11 |
35–36 | 0.93 | 1.02 | 1.11 |
37–38 | 0.92 | 0.98 | 1.05 |
39–40 | 0.87 | 0.97 | 1.06 |
41–42 | 0.93 | 0.96 | 1.00 |
(Campbell S, Thoms A: Ultrasound measurement of the fetal head to abdomen circumference ratio in the assessment of growth retardation. Br J Obstet Gynaecol 84:165, 1977. Reprinted with permission of Blackwell Scientific Publications, Oxford, England.)
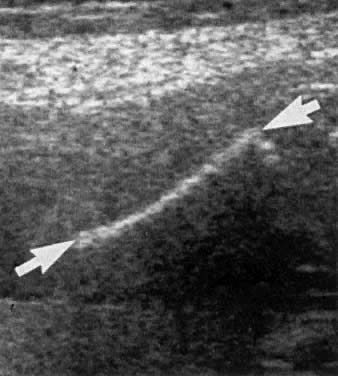
FEMUR LENGTH.
All the fetal long bones can be adequately examined and measured by ultrasound; however, the femur is the largest of the long bones, least moveable, and easiest to image. The femur may be adequately visualized from 14 weeks' gestation until delivery.38,39,40,67,68,69,70,71,72,73,74 It is measured along the long axis of the bone; a straight measurement of the osseous portion is taken from one end to the other, disregarding bone curvature (Fig. 5). The femoral neck and both proximal and distal epiphyseal cartilages are excluded from the measurement. Femur length (FL) measurements may be used to accurately predict gestational age between 14 weeks' gestation and term (Table 8).39 Most observers consider the accuracy of the FL and BPD measurements to be similar in the third trimester. Although there is controversy regarding the accuracy of the FL prior to 26 weeks' gestation,38,39 the accuracy of gestational age prediction based on FL is greatest in the second trimester and least near term.
TABLE 8. Femur Length Measurements Relative to Gestational Age
Femur | Menstrual | Femur | Menstrual |
Length | Age | Length | Age |
(cm) | (weeks) | (cm) | (weeks) |
1.0 | 12.8 | 4.5 | 24.5 |
1.1 | 13.1 | 4.6 | 24.9 |
1.2 | 13.4 | 4.7 | 25.3 |
1.3 | 13.6 | 4.8 | 25.7 |
1.4 | 13.9 | 4.9 | 26.1 |
1.5 | 14.2 | 5.0 | 26.5 |
1.6 | 14.5 | 5.1 | 27.0 |
1.7 | 14.8 | 5.2 | 27.4 |
1.8 | 15.1 | 5.3 | 27.8 |
1.9 | 15.4 | 5.4 | 28.2 |
2.0 | 15.7 | 5.5 | 28.7 |
2.1 | 16.0 | 5.6 | 29.1 |
2.2 | 16.3 | 5.7 | 29.6 |
2.3 | 16.6 | 5.8 | 30.0 |
2.4 | 16.9 | 5.9 | 30.5 |
2.5 | 17.2 | 6.0 | 30.9 |
2.6 | 17.6 | 6.1 | 31.4 |
2.7 | 17.9 | 6.2 | 31.9 |
2.8 | 18.2 | 6.3 | 32.3 |
2.9 | 18.6 | 6.4 | 32.8 |
3.0 | 18.9 | 6.5 | 33.3 |
3.1 | 19.2 | 6.6 | 33.8 |
3.2 | 19.6 | 6.7 | 34.2 |
3.3 | 19.9 | 6.8 | 34.7 |
3.4 | 20.3 | 6.9 | 35.2 |
3.5 | 20.7 | 7.0 | 35.7 |
3.6 | 21.0 | 7.1 | 36.2 |
3.7 | 21.4 | 7.2 | 36.7 |
3.8 | 21.8 | 7.3 | 37.2 |
3.9 | 22.1 | 7.4 | 37.7 |
4.0 | 22.5 | 7.5 | 38.3 |
4.1 | 22.9 | 7.6 | 38.8 |
4.2 | 23.3 | 7.7 | 39.3 |
4.3 | 23.7 | 7.8 | 39.8 |
4.4 | 24.1 | 7.9 | 40.4 |
(Hadlock FP, Harrist RB, Deter RL, Park SK; Fetal femur length as a predictor of menstrual age. AJR 138:875, 1982. Reprinted with permission of Williams & Wilkins, Baltimore.)
Biologic variation may lead to inaccuracies of FL measurements in a manner similar to that of the other fetal growth parameters. In addition, several technical factors are potential sources of error in the measurement of the femur.67,70,72 Sector ultrasound imaging may lead to overestimation of FL, particularly when the femur is in the far field or lateral margins of the image. Linear-array ultrasound imaging provides more accurate measurements of FL. In addition, FL measurements obtained in the axial plane (parallel to the ultrasonic beam) have less mean absolute error than those obtained in the lateral plane, perpendicular to the ultrasonic beam (1.7 mm vs. 3.7 mm, respectively).74 Tangential section of the femur, failing to visualize the entire length of the shaft, leads to underestimation of FL and, therefore, of gestational age. Artifactual bowing of the femur may also occur on ultrasound imaging and lead to a shortened FL measurement. The distal femoral epiphysis becomes echogenic in the third trimester and is separated from the distal end of the diaphysis, the osseous portion of the shaft. Inclusion of the distal epiphysis will falsely overestimate FL.67,68
Gestational age assessment by FL is particularly useful when head measurement is difficult to obtain due to fetal position. The femur length may also be compared with the biparietal diameter (FL/BPD) as an age-independent ratio.73 The FL/BPD ratio (normal values
ASSESSMENT OF GESTATIONAL AGE
A single parameter (CRL, BPD, HC, AC, or FL) may be used to assess gestational age. The accuracy of a single parameter is dependent on the gestational age at the time of ultrasound examination (Table 9). Several methods have been employed to improve the accuracy of gestational age assessment compared with the use of a single parameter. Two of these methods, growth-adjusted sonographic age79 and averaging multiple parameters80,81 are discussed. Several principles are important to remember when assessing gestational age by ultrasound:
TABLE 9.Ultrasound Predictors of Gestational Age
| Estimated Range for |
Parameter* | 95% of Cases |
Gestational sac mean diameter | ± week |
Crown-rump length | ± 5–7 days |
BPD, 12–26 weeks | ± 10–11 days |
HC, 12–26 weeks | ± 10–14 days |
AC, 12–26 weeks | ± 10–14 days |
FL, 12–26 weeks | ± 10–20 days |
BPD, 27–42 weeks | ± 2–3 weeks |
HC, 27–42 weeks | ± 2–3 weeks |
AC, 27–42 weeks | ± 2–3 weeks |
FL, 27–42 weeks | ± 2–3 weeks |
* See text for abbreviations.
- When menstrual dates fall within the confidence limits of the ultrasound assessment, the role of ultrasound is to confirm menstrual dates.
- When menstrual dates fall outside the confidence limits of ultrasound assessment, assignment of dates should be based on ultrasound assessment of gestational age.
- When menstrual dates are unknown, assignment of dates should be based on ultrasound assessment of gestational age.
Growth-Adjusted Sonographic Age
Gestational age estimation using a single biparietal diameter is accurate within a margin of ±10 to 11 days in the second trimester. Gestational age can be more accurately predicted by obtaining paired BPD measurements (the first from 20 to 26 weeks' gestation and the second from 31 to 33 weeks' gestation) and assigning gestational age by a method developed by Sabbagha and co-workers79 known as growth-adjusted sonographic age (GASA).
In approximately 90% of fetuses, BPD growth from 20 to 33 weeks' gestation tends to progress within narrow percentile ranks (Table 10).21,25 BPD growth patterns can be subdivided into three types: large (
TABLE 10. Assignment of Growth-Adjusted Sonographic Age (GASA)
| First Sonar* |
| ||||
(BPD vs Fetal Age Percentile Range) | Second Sonar† (BPD Percentile Range) | |||||
| Large Fetus | Average Fetus |
| |||
| vs Small | (age accepted | Fetal Age | Average BPD | Large BPD | Small BPD |
BPD | Fetus (wk) | temporarily) | (wk) | >10 <90 | ||
2.8 | ±1 | 14 |
| |||
3.2 | ±1 | 15 | 29 | 7.0–8.1 | ||
3.5 | ±1 | 16- |
| |||
3.6 | ±1.6 | 16 | 30 | 7.3–8.4 | ||
3.7 | ±1.6 | 16+ |
| |||
3.8 | ±1.6 | 17- | 30+ | 7.4–8.5 | ||
3.9 | ±1.6 | 17 |
| |||
4.0 | ±1.6 | 17+ | 31- | 7.4–8.5 | ||
4.1 | ±1.6 | 18- |
| |||
4.2 | ±1.6 | 18 | 31 | 7.5–8.6 | ||
4.3 | ±1.6 | 18+ |
| |||
4.4 | ±1.6 | 19- | 31+ | 7.6–8.7 | ||
4.5 | ±1.6 | 19 |
| |||
4.6 | ±1.6 | 19+ | 32- | 7.6–8.7 | ||
4.7 | ±1.6 | 20- |
| |||
4.8 | ±1.6 | 20 | 32 | 7.7–8.8 | ||
4.9 | ±1.6 | 20+ |
| |||
5.0 | ±1.6 | 21- | 32+ | 7.8–8.9 | ||
5.1 | ±1.6 | 21 |
| |||
5.2 | ±1.6 | 21+ | 33- | 7.8–8.9 | ||
5.3 | ±1.6 | 22- |
| |||
5.4 | ±1.6 | 22- | 33 | 7.9–9.0 | ||
5.5 | ±1.6 | 22 |
| |||
5.6 | ±1.6 | 22+ | 33+ | 8.0–9.0 | ||
5.7 | ±1.6 | 23- |
| |||
5.8 | ±1.6 | 23 | 34- | 8.0–9.0 | ||
5.9 | ±1.6 | 23+ |
| |||
6.0 | ±1.6 | 24- | 34 | 8.1–9.1 | ||
6.1 | ±1.6 | 24 |
| |||
6.2 | ±1.6 | 24+ | 35 | 8.4–9.4 | ||
6.3 | ±1.6 | 25- |
|
|
|
|
6.4 | ±1.6 | 25 |
|
|
|
|
6.5 | ±1.6 | 25+ |
|
|
|
|
6.6 | ±1.6 | 26- |
|
|
|
|
6.7 | ±1.6 | 26 |
|
|
|
|
BPD = biparietal diameter; + = plus 1 to 3 days; - = minus 1 to 3 days.
* First sonar is done prior to 26 weeks because of small variation in fetal age of ±11 days.
† Second sonar: (1) Must be done between 30 to 33 weeks because of maximal variation in fetal BPD size in this interval and prior to onset of IURG in most cases.(2) Must be done at least 6 weeks after first BPD
(Adapted from Sabbagha RE, Hughey M, Depp R: Growth adjustment sonographic age [GASA]: A simplified method.Obstet Gynecol 51:383, 1978: and Evans CB, Motew MN, Sabbagha RE: Growth adjusted sonographic age [GASA]: Expansion of the margins delineating the fetus with average BPDs to the 10th and 90th percentiles.Obstet Gynecol (in press).Reprinted with permission of American College of Obstetricians and Gynecologists.
 90th percentile), average (between 10th and 90th percentiles), or small (
90th percentile), average (between 10th and 90th percentiles), or small ( 10th percentile) and lead to a closer assessment of fetal age.
10th percentile) and lead to a closer assessment of fetal age.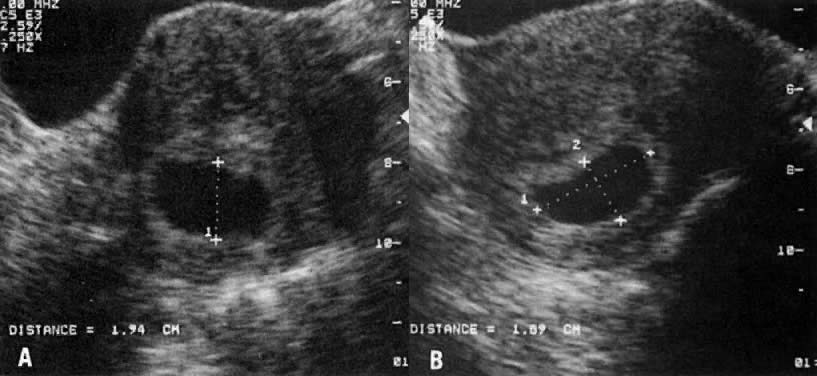{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The method of GASA has not been used when the first BPD measurement is obtained prior to 20 weeks' gestation; therefore, it is best to confine the use of GASA to pregnancies in which serial ultrasound studies are contemplated and the first measurement is obtained between 20 and 26 weeks' gestation. Smazal and associates51 evaluated the method of GASA and suggested that the accuracy was indeed ±5 days. However, in this report, the accuracy of a single BPD was also approximately ±5 days.
Multiple Fetal Growth Parameters
Hadlock and co-workers80,81 combined several measurements in an effort to increase the accuracy of gestational age assessment. The rationale for employing multiple parameters for fetal dating is that when two or more parameters predict the same end point, the probability of correctly predicting that end point is increased. The BPD, HC, AC, and FL measurements were obtained and the mean gestational ages of combinations of these parameters were averaged to obtain a mean gestational age. The use of multiple parameters improved the accuracy of gestational age assessment compared with any single parameter (Table 11).80 If the gestational age estimates derived from all of the parameters are similar, assignment of gestational age from the average of all the parameters will improve accuracy. However, if gestational age estimates of the various parameters are quite different, averaging multiple parameters will decrease the accuracy of the best predictor(s). Averaging of fetal growth parameters should be avoided when certain conditions are suspected, such as fetal macrosomia, intrauterine growth retardation (both symmetric and asymmetric), and congenital anomalies (skeletal dysplasias, hydrocephalus, and others).
TABLE 11. Accuracy of Gestational Age Assessment by Multiple Fetal Growth Parameter
| Subgroup Variability (±2 SD) in Weeks | ||||
Fetal | 12–18 Weeks | 18–24 Weeks | 24–30 Weeks | 30–36 Weeks | 36–42 Weeks |
Parameters | (N = 43) | (N = 69) | (N = 76) | (N = 95) | (N = 78) |
BPD | ±1.19 | ±1.73 | ±2.18 | ±3.08 | ±3.20 |
HC | ±1.19 | ±1.48 | ±2.06 | ±2.98 | ±2.70 |
AC | ±1.66 | ±2.06 | ±2.18 | ±2.96 | ±3.04 |
FL | ±1.38 | ±1.80 | ±2.08 | ±2.96 | ±3.12 |
BPD, AC | ±1.26 | ±1.68 | ±1.92 | ±2.60 | ±2.88 |
BPD, AC | ±1.08 | ±1.49 | ±1.99 | ±2.86 | ±2.64 |
BPD, FL | ±1.12 | ±1.46 | ±1.84 | ±2.60 | ±2.62 |
HC, AC | ±1.20 | ±1.52 | ±1.98 | ±2.68 | ±2.52 |
HC, FL | ±1.08 | ±1.34 | ±1.86 | ±2.52 | ±2.28 |
AC, FL | ±1.32 | ±1.64 | ±1.88 | ±2.66 | ±2.60 |
BPD, AC, FL | ±1.20 | ±1.52 | ±1.82 | ±2.50 | ±2.52 |
BPD, HC, FL | ±1.04 | ±1.35 | ±1.81 | ±2.52 | ±2.34 |
HC, AC, FL | ±1.14 | ±1.46 | ±1.86 | ±2.52 | ±2.34 |
HC, AC, BPD | ±1.21 | ±1.58 | ±1.94 | ±2.60 | ±2.52 |
BPD, HC, AC, FL | ±1.08 | ±1.40 | ±1.80 | ±2.44 | ±2.30 |
(Hadlock FP, Deter RL, Harrist RB, Park SK: Estimating fetal age: Computer-assisted analysis of multiple fetal growth parameters. Radiology 152:497, 1984. Reprinted with permission of Radiological Society of North America, Oak Brook, IL.)
Multiple Gestations
The detection of multiple gestations is important since multiple gestations are at greater risk for many complications, particularly fetal growth retardation. Fetal biometric data are available for twin gestations81,82,83,84,85; however, triplet and quadruplet pregnancies have not been adequately studied owing to their infrequent occurrence.
In general, ultrasound-derived fetal dating tables obtained for singleton pregnancies can be used accurately for twin pregnancies until approximately 30 weeks' gestation.82,83,84,85,86 During the last 10 weeks of pregnancy there is a decrease in the growth rate for twin fetuses compared with singleton fetuses. Grumbach and co-workers86 have suggested that the femur continues to grow normally throughout pregnancy in twin gestations, while the head (BPD and HC) and abdominal (AC) growth rates decrease in the last 10 weeks of pregnancy. Although further studies are required to confirm these findings, this study suggests that FL measurement may be a more reliable parameter to use for gestational age assessment in twin gestations during the third trimester. Gestational age estimations in twin pregnancies prior to 30 weeks' gestation should be performed in a similar manner to that for singleton pregnancies.
SUMMARY
A simple, but uniform approach to the evaluation of gestational age should be performed in all fetuses. The ultrasound assessment of fetal age is based on the earliest ultrasound study, provided the measurement is technically adequate. Early in gestation fetal measurements have the least variability and, therefore, are most likely to predict fetal age. In the first trimester, the CRL measurement is used to estimate gestational age, whereas in the second and third trimesters fetal head (BPD and HC), body (AC), and extremity (FL) measurements are used to assess gestational age. The following guidelines are recommended for the assessment of gestational age:
- Crown-rump length measurement is used to establish fetal age in pregnancies with unknown menstrual dates or in pregnancies with discrepancy between menstrual dates and crown-rump length measurement of greater than ±7 days. If CRL and menstrual dates are within the normal range of error of the measurement (±7 days), the menstrual dates are used to establish fetal age.
- In the second trimester, menstrual dates are used if the mean gestational age predicted by (a) a single parameter (BPD, HC, or FL) or (b) multiple parameters (BPD or HC and FL ± AC) is within the range of error of these measurements. If menstrual dates are unknown, or the difference between menstrual dates and the mean gestational age predicted by single or multiple parameters is greater than the range of error of these measurements, fetal age should be established using the best ultrasound predictors (either single or multiple parameters) or GASA method.
- In the third trimester, gestational age assessment is particularly problematic. Menstrual dates should be used to establish fetal age if the mean gestational age predicted by multiple parameters is within the range of error of these measurements (±2–3 weeks). In the pregnancy with unknown menstrual dates or a discrepancy between menstrual dates and mean gestational age predicted by multiple parameters of more than 3 weeks, fetal age should be estimated by the multiple parameters method. However, the potential error of this method in the third trimester of pregnancy may not be acceptable. Obstetric management must appreciate this potential for error. For example, a patient presenting in spontaneous labor at 33 ± 3 weeks' gestation should be managed as if the pregnancy may be as little as 30 weeks' gestation, rather than as advanced at 36 weeks' gestation. Similarly, the patient presenting for prenatal care at 39 ± 3 weeks' gestation, should be managed for the potential of postdates pregnancy.
Use of the multiple parameters method of assessing gestational age is valid when the gestational age estimates of the various ultrasound parameters are similar. If the gestational age estimates of one or several parameters is greater than 2 weeks different than the estimates of the other parameters, either the abnormal ultrasound parameters should be excluded or a different method should be used to estimate gestational age. When the various ultrasound parameters predict different gestational ages the fetus should be further evaluated to explain these differences. For example, an abnormally small FL measurement may suggest short-limb defects, a large BPD may be secondary to hydrocephalus, and an abnormally small or large AC measurement may suggest asymmetric intrauterine growth retardation or macrosomia, respectively. As mentioned previously, the different ultrasound ratios (CI, HC/AC, and FL/BPD) may be used to identify abnormally small or large parameters. In the instance of an abnormal cephalic index, the HC should be used to estimate gestational age, rather than the BPD measurement.
In conclusion, assessment of gestational age is fundamental to obstetric care and should be a carefully thought-out process. Assessment should depend on history and physical examination, as well as ultrasound evaluation.
REFERENCES
Cowchock FS: Use of alpha-fetoprotein in prenatal diagnosis. Clin Obstet Gynecol 19: 871, 1976 |
|
Liley AW: Liquor amnii in the management of the pregnancy complicated by rhesus sensitization. Am J Obstet Gynecol 82: 1359, 1961 |
|
Queenan JT: Amniotic fluid analysis. Clin Obstet Gynecol 14: 505, 1971 |
|
Goldenberg RL, Nelson K: Iatrogenic respiratory distress syndrome. Am J Obstet Gynecol 123: 617, 1975 |
|
Hack M, Fanaroff AA, Klaus MH et al: Neonatal respiratory distress following elective delivery: A preventable disease? Am J Obstet Gynecol 126: 43, 1976 |
|
Campbell S, Warsof SL, Little D, Cooper DJ: Routine ultrasound screening for the prediction of gestational age. Obstet Gynecol 65: 613, 1985 |
|
Dewhurst CJ, Beazley JM, Campbell S: Assessment of fetal maturity and dysmaturity. Am J Obstet Gynecol 113: 141, 1972 |
|
Sabbagha RE: Ultrasound in managing the high-risk pregnancy. In Spellacy WD (ed): Management of the High-Risk Pregnancy, pp 137–167. Baltimore, University Park Press, 1976 |
|
Hertz RH, Sokol RJ, Knoke JD et al: Clinical estimation of gestational age: Rules for avoiding preterm delivery. Am J Obstet Gynecol 131: 395, 1978 |
|
Beazley JM, Underhill RA: Fallacy of the fundal height. Br Med J 4: 404, 1970 |
|
Bell ET, Loraine JA: Time of ovulation in relation to cycle length. Lancet 1: 1029, 1965 |
|
Queenan JT, O'Brien GD, Bains LM et al: Ultrasound scanning of ovaries to detect ovulation in women. Fertil Steril 34: 99, 1980 |
|
Rossavik IK, Gibbons WE: Variability of ovarian follicular growth in natural menstrual cycles. Fertil Steril 44: 195, 1985 |
|
Moghissi KS: Prediction and detection of ovulation. Fertil Steril 34: 89, 1980 |
|
Hellman LF, Kobayashi M, Fillisti L et al: Growth and development of the human fetus prior to the twentieth week of gestation. Am J Obstet Gynecol 103: 789, 1969 |
|
Jouppila PC: Length and depth of the uterus and the diameter of the gestation sac in normal gravidas during early pregnancy. Acta Obstet Gynecol Scand 50 (suppl): 29, 1971 |
|
Robinson HP, Fleming JEE: A critical evaluation of sonar “crown-rump length” measurements. Br J Obstet Gynaecol 82: 702, 1975 |
|
Drumm JE, Clinch J, MacKinzie G: The ultrasonic measurement of fetal crown-rump length as a method of assessing gestational age. Br J Obstet Gynaecol 83: 417, 1976 |
|
MacGregor SN, Tamura RK, Sabbagha RE et al: Underestimation of gestational age by conventional crown-rump length growth curves. Obstet Gynecol 70: 344, 1987 |
|
Campbell S: The prediction of fetal maturity by ultrasonic measurement of the biparietal diameter. J Obstet Gynaecol Br Commonw 76: 603, 1969 |
|
Sabbagha RE, Turner H, Rockett H et al: Sonar BPD and fetal age: Definition of the relationship. Obstet Gynecol 43: 7, 1974 |
|
Campbell S, Newman GB: Growth of the fetal biparietal diameter during normal pregnancy. J Obstet Gynaecol Br Commonw 78: 513, 1971 |
|
Sabbagha RE, Hughey M: Standardization of sonar cephalometry and gestational age. Obstet Gynecol 52: 402, 1978 |
|
Sabbagha RE, Barton FB, Barton BA: Sonar biparietal diameter: I. Analysis of percentile growth differences in two normal populations using same methodology. Am J Obstet Gynecol 126: 479, 1976 |
|
Sabbagha RE, Barton BA, Barton FB et al: Sonar biparietal diameter: II. Predictive of three fetal growth patterns leading to a closer assessment of gestational age and neonatal weight. Am J Obstet Gynecol 126: 485, 1976 |
|
Hughey M, Sabbagha RE: Cephalometry by real time imaging: A critical evaluation. Am J Obstct Gynecol 131: 825, 1978 |
|
Kurtz AB, Wapner RJ, Kurtz RJ et al. Analysis of biparietal diameter as an accurate indicator of gestational age. J Clin Ultrasound 8:319, 1980 |
|
Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal biparietal diameter: A critical reevaluation of the relation to menstrual age by means of realtime ultrasound. J Ultrasound Med 1: 97, 1982 |
|
Doubilet PM, Greenes RA: Improved prediction of gestational age from fetal head measurement. AJR 142: 797, 1984 |
|
Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal head circumference: Relation to menstrual age. AJR 138: 649, 1982 |
|
Campbell S, Wilken D: Ultrasonic measurement of fetal abdomen circumference in the estimation of fetal weight. Br J Obstet Gynaecol 82: 689, 1975 |
|
Tamura RK, Sabbagha RE: Percentile ranks of sonar fetal abdominal circumference measurements. Am J Obstet Gynecol 138: 475, 1980 |
|
Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal abdominal circumference as a predictor of menstrual age. AJR 139: 367, 1982 |
|
Hadlock FP, Deter RL, Harrist RB et al: A date-independent predictor of intrauterine growth retardation: Femur length/abdominal circumference ratio. AJR 141: 979, 1983 |
|
Eriksen PS, Secher NJ, Weis-Bentzon M: Normal growth of the fetal biparietal diameter and the abdominal diameter in a longitudinal study. Acta Obstet Gynecol Scand 64: 65, 1985 |
|
Queenan JF, O'Brien GD, Campbell S: Ultrasound measurement of fetal limb bones. Am J Obstet Gynecol 138: 297, 1980 |
|
O'Brien GD, Queenan JT, Campbell S: Assessment of gestational age in the second trimester by real-time ultrasound measurement of the femur length. Am J Obstet Gynecol 139: 540, 1981 |
|
Hadlock FP, Harrist RB, Deter RL, Park SK: Fetal femur length as a predictor of menstrual age. A JR 138: 875, 1982 |
|
Jeanty P, Rodesch F, Delbeke D, Dumont JE: Estimation of gestational age from measurement of fetal long bones. J Ultrasound Med 3: 75, 1984 |
|
Jeanty P. Dramaiz-Wilmer M, Dramaiz-Wilmer M, Delbeke D et al: Ultrasonic evaluation of fetal ventricular growth. Neuroradiology 21: 127, 1981 |
|
Mayden KL, Tortora M, Berkowitz RL et al: Orbital diameters: A new parameter for prenatal diagnosis and dating. Am J Obstet Gynecol 144: 289, 1982 |
|
Jeanty P, Cantraine F, Cousaert E et al: The binocular distance: A new way to estimate fetal age. J Ultrasound Med 3: 241, 1984 |
|
Goldstein I, Reece EA, Pilu et al: Cerebellar measurements with ultrasonography in the evaluation of fetal growth and development. Am J Obstet Gynecol 156: 1065, 1987 |
|
Chitkara U, Rosenberg J, Chervenak FA et al: Prenatal sonographic assessment of the fetal thorax: Normal values. Am J Obstet Gynecol 156: 1069, 1987 |
|
Reece EA, Scioscia AL, Green J et al: Embryonic trunk circumference: A new biometric parameter for estimation of gestational age. Am J Obstet Gynecol 156: 713, 1987 |
|
Goldstein I, Reece EA, Hobbins JC: Sonographic appearance of the fetal heel ossification centers and foot length measurements provide independent markers for gestational age estimation. Am J Obstet Gynecol 159: 923, 1988 |
|
Schwimer SR, Lebovic J: Transvaginal pelvic ultrasonography. J Ultrasound Med 3: 381, 1984 |
|
Robinson HP: Sonar measurement of fetal crown-rump length as means of assessing maturity of first trimester of pregnancy. Br Med J 4: 28, 1973 |
|
Drumm JE: The prediction of delivery date by ultrasonic measurement of fetal crown-rump length. Br J Obstet Gynaecol 84: 1, 1977 |
|
Yerushalmy J: Relation of birth weight, gestational age, and the rate of intrauterine growth to perinatal mortality. Clin Obstet Gynecol 13: 107, 1970 |
|
Smazal SF, Weisman LE, Hoppler KD et al: Comparative analysis of ultrasonographic methods of gestational age assessment. J Ultrasound Med 2: 147, 1983 |
|
Kopta MM, May RR, Crane JP: A comparison of the reliability of the estimated date of confinement predicted by crown-rump length and biparietal diameter. Am J Obstet Gynecol 145: 562, 1983 |
|
Lubchenco LO, Hansman C, Dressier J, Boyd E: Intrauterine growth as estimated from live-born weight data at 24–42 weeks of gestation. Pediatrics 32: 793, 1963 |
|
Brenner WE, Edelman DA, Hendricks DH: A standard of fetal growth for the United States of America. Am J Obstet Gynecol 126: 555, 1976 |
|
Williams RL, Creasy RK, Cunningham GC et al: Fetal growth and perinatal viability in California. Obstet Gynecol 59: 624, 1982 |
|
Mantoni M, Pedersen JF: Fetal growth delay in threatened abortion: An ultrasound study. Br J Obstet Gynaecol 89: 525, 1982 |
|
Pedersen JF, Pedersen LM: Early growth retardation in diabetic pregnancy. Br Med J 1: 18, 1979 |
|
Shepard M, Filly RA: A standardized plane for biparietal diameter measurement. J Ultrasound Med 1: 145, 1982 |
|
Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal biparietal diameter: Rational choice of plane of section for sonographic measurement. AJR 138: 871, 1982 |
|
Cooperberg PL, Chow T, Kite V, Austin S: Biparietal diameter: A comparison of real time and conventional B-scan techniques. J Clin Ultrasound 4: 421, 1976 |
|
Lunt RM, Chard L: Reproducibility of measurement of fetal biparietal diameter by ultrasonic cephalometry. J Obstet Gynaecol Br Commonw 81: 682, 1974 |
|
Davison JM, Lind T, Farr V, Whittingham TA: The limitations of ultrasonic fetal cephalometry. J Obstet Gynaecol Br Commonw 80: 769, 1981 |
|
Hadlock FP, Kent WR, Loyd JL et al: An evaluation of two methods for measuring fetal head and body circumferences. J Ultrasound Med 1: 359, 1982 |
|
Hadlock FP, Deter RL, Carpenter RJ, Park SK: Estimating fetal age: Effect of head shape on BPD. AJR 137: 83, 1981 |
|
Shields JR, Medearis AL, Bear MB: Fetal head and abdominal circumferences: Ellipse calculations versus planimetry. J Clin Ultrasound 15: 237, 1987 |
|
Campbell S, Thorns A: Ultrasound measurement of the fetal head to abdomen circumference ratio in the assessment of growth retardation. Br J Obstet Gynaecol 84: 165, 1977 |
|
Goldstein RB, Filly RA, Simpson G: Pitfalls in femur length measurements. J Ultrasound Med 6: 203, 1987 |
|
Chinn DH, Bolding DB, Callen OW et al: Ultrasonographic identification of fetal lower extremity epiphyseal ossification centers. Radiology 147: 815, 1983 |
|
Wolfson RN, Peisner DB, Chik LL, Sokol RJ: Comparison of biparietal diameter and femur length in the third trimester: Effects of gestational age and variation in fetal growth. J Ultrasound Med 5: 145, 1986 |
|
Winter J, Kimme-Smith C, King W: Measurement accuracy of sonographic sector scanners. AJR 144: 645, 1985 |
|
Gamba JL, Bowie JD, Dodson WC, Hedlund LW: Accuracy of ultrasound in fetal femur length determination: Ultrasound phantom study. Invest Radiol 20: 316, 1985 |
|
Jeanty P, Beck GJ, Chervenak FA et al: A comparison of sector and linear array scanners for the measurement of the fetal femur. J Ultrasound Med 4: 525, 1985 |
|
Hohler CW, Quetel TA: Comparison of ultrasound femur length and biparietal diameter in late pregnancy. Am J Obstet Gynecol 141: 759, 1981 |
|
Abramowicz J, Jaffe R: Comparison between lateral and axial ultrasonic measurements of the fetal femur. Am J Obstet Gynecol 159: 921, 1988 |
|
Ott WJ: Fetal femur length, neonatal crown-heel length, and screening for intrauterine growth retardation. Obstet Gynecol 65: 460, 1985 |
|
Vintzileos AM, Neckles S, Campbell WA et al: Three fetal ponderal indexes in normal pregnancy. Obstet Gynecol 65: 807, 1985 |
|
Benson CB, Doubilet PM, Saltzman DH, Jones TB: FL/AC ratio: Poor predictor of intrauterine growth retardation. Invest Radiol 20: 727, 1985 |
|
Benson CB, Doubilet PM, Saltzman DH et al: Femur length/abdominal circumference ratio: Poor predictor of macrosomic fetuses in diabetic mothers. J Ultrasound Med 5: 141, 1986 |
|
Sabbagha RE, Hughey M, Depp R: Growth adjustment sonographic age (GASA): A simplified method. Obstet Gynecol 51: 383, 1978 |
|
Hadlock FP, Deter RL, Harrist RB, Park SK: Estimating fetal age: Computer-assisted analysis of multiple fetal growth parameters. Radiology 152: 497, 1984 |
|
Hadlock FP, Harrist RB, Shah YP et al: Estimating fetal age using multiple parameters: A prospective evaluation in a racially mixed population. Am J Obstet Gynecol 156: 955, 1987 |
|
Leveno KJ, Santos-Ramos R, Duenholter JH et al: Sonal cephalometry in twins: A table of biparietal diameters for normal twin fetuses and a comparison with singletons. Am J Obstet Gynecol 135: 727, 1979 |
|
Crane JF, Tomich PG, Kopta M: Ultrasound growth patterns in normal and discordant twins. Obstet Gynecol 55: 678, 1980 |
|
Leveno K J, Santos-Ramos R, Duenholter JH et al: Sonar cephalometry in twin pregnancy: Discordancy of the biparietal diameter after 28 weeks' gestation. Am J Obstet Gynecol 138: 615, 1980 |
|
Socol M, Tamura R, Sabbagha RE et al: Diminished biparietal diameter and abdominal circumference growth in normal twins. Obstet Gynecol 64: 235, 1984 |
|
Grumbach K, Coleman BG, Arger PH et al: Twin and singleton growth patterns compared using ultrasound. Radiology 158: 237, 1986 |