Ferin, M, Glob. libr. women's med.,
(ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10283
November 2008
Multifetal Pregnancy Reduction
Authors
INTRODUCTION
Incredibly, it is now more than three decades since Louise Brown’s birth, the first IVF baby. Millions of babies have been born benefiting from infertility therapies including more than 2,000,000 IVF babies. These incredible success stories, however, have had corresponding serious side effects. The twin pregnancy rate, commonly quoted for decades to be 1 in 90, has more than doubled in the United States to more than 1 in 30,1 and approximately 65% of all twins in the United States are secondary to infertility treatments. Some IVF programs create as many multiples as singletons. In fact nearly one half of all IVF babies are part of multiples suggesting that nearly a third of all pregnancies are multiples (Table 1).2 Furthermore, monozygotic twinning, per se, and as part of higher order multiples has continued to rise with its associated dramatically increased risks of anomalies, loss, and prematurity.3, 4 Multiple pregnancy rates have continued to rise, and the incidence of prematurity and related sequelae closely correlate with fetal number (Figure 1) (Tables 2 and 3).1 With increasing public, professional, and legal attention, some of the very high order multiples have diminished, particularly secondary to lower transfer numbers of embryos in IVF.5, 6, 7, 8 There are some suggestions that the incidence of quadruplets and higher multiples is slowly diminishing, but the incidence is still very high.9
Table 1. Twins and triplets from assisted reproductive technologies: 2005 SART data
| Age | |||||
| <35 | 35–37 | 38–40 | 41–43 | 43–44 | |
| Number of cycles | 37,223 | 20,570 | 17,805 | 8,337 | 4,680 |
| Average number transferred | 2.4 | 2.6 | 3.0 | 3.3 | 3.3 |
| %Twins | 33.0 | 27.2 | 21.7 | 13.1 | 7.6 |
| %Triplets | 4.3 | 5.0 | 4.4 | 2.5 | 1.8 |
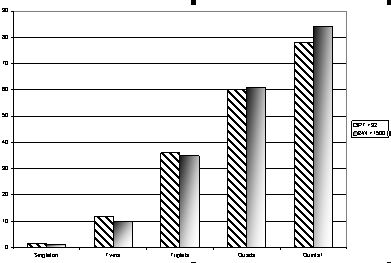 Fig. 1. Prematurity risks as a function of fetal number. Diagonally hatched bars, preterm birth <32 weeks; shaded bars, birth weight <1500 g. (2002 United States Centers for Disease Control data.)
Fig. 1. Prematurity risks as a function of fetal number. Diagonally hatched bars, preterm birth <32 weeks; shaded bars, birth weight <1500 g. (2002 United States Centers for Disease Control data.)
Table 2. Multiple births in the United States
| Year | Twins | Triplets | Quadruplets | Quintuplets and Higher Multiples |
| 2005 | 133,122 | 6,208 | 418 | 68 |
| 2004 | 132,219 | 6,750 | 439 | 86 |
| 2003 | 128,615 | 7,110 | 468 | 85 |
| 2002 | 125,134 | 6,898 | 434 | 69 |
| 2001 | 121,246 | 6,885 | 501 | 85 |
| 2000 | 118,916 | 6,742 | 506 | 77 |
| 1999 | 114,307 | 6,742 | 512 | 67 |
| 1998 | 110,670 | 6,919 | 627 | 79 |
| 1997 | 104,137 | 6,148 | 510 | 79 |
| 1996 | 100,750 | 5,298 | 560 | 81 |
| 1995 | 96,736 | 4,551 | 365 | 57 |
| 1993 | 96,445 | 3,834 | 277 | 57 |
| 1991 | 94,779 | 3,121 | 203 | 22 |
| 1989 | 90,118 | 2,529 | 229 | 40 |
| %Change from 1989 to 2005 | 47.7% | 145.5% | 82.56% | 70% |
Data taken from National Vital Statistics Report, Volume 56: 242, 2007.
Table 3. Ratio of observed to expected multiple
| Birth | Observed | Expected | Ratio |
| Twins | 133,122 | 45,981 | 2.80:1 |
| Triplets | 6,208 | 510 | 12.2:1 |
| Quadruplets | 418 | 6 | 69.7:1 |
| Quintuplets and higher multiples | 68 | 0.06 | 1133.3:1 |
The total number of births in 2005 was 4,138,349.
Some reports by perinatologists are overly, and we believe inappropriately, optimistic because these physicians don’t start “counting” until they begin to see patients in the second trimester, at which time many losses have already occurred.10, 11 Many other articles have addressed these issues and are not repeated here.11, 12
Despite the increased reliance of assisted reproductive technologies (ART) in infertility treatments, the proportion of cases significantly hyperstimulated and resulting in quintuplets or more has dramatically decreased to less than 5% of all cases seen by us.13 Regardless, the 2004 report of the Society of Assisted Reproductive Technologies (SART) suggested that, of all pregnancies achieved by ART, in the United States 60.3% are singletons, 28.6% twins, 4.9% triplets or higher, and 6.2% were unknown.14 CDC data from 2005 show that the proportion of multiples that are twins, as opposed to higher numbers has increased slightly reflecting more of an increase in the number of twins rather than a fall in triplets and higher order multiples with 2003–2005 showing a decrease but being too short a time frame to be certain of a real trend.1
Such data continue to reinforce the significant role of vigilance in the monitoring of infertility therapies. We have experienced that the vast majority of multifetal cases occur to physicians with the best of equipment and with the best of intentions who have an unfortunate and reasonably unpredictable or unpreventable mal-occurrence. Despite this, clearly some cases might have been prevented if increased vigilance had been used.15, 16
DEMOGRAPHICS
Over the past decade, the pattern of patients seeking multifetal pregnancy reduction (MFPR) has evolved considerably.14, 16 With the rapid expansion of availability of donor eggs, the number of “older women” seeking MFPR has increased dramatically. In our experience over 10% of all patients we see seeking MFPR are over 40 years of age, and nearly half of them are using donor eggs.13, 17, 18 As a consequence of the shift to older patients, many of whom already have previous relationships and children, there is an increased desire by these patients to have only one further child. The number of experienced centers willing to do two-to-one reductions is still very limited, but we believe it can be justified in the appropriate circumstances.15, 17
For patients who are “older” particularly using their own eggs, genetic counseling and diagnosis has become an integral part of our process. By 2003, more than 50% of patients in the United States having ART cycles were over 35, and the proportion continues to rise (Table 4).1, 11, 12, 14 In the 1980s and early 1990s, the most common approach was to offer amniocentesis at 16–17 weeks on the remaining twins. However, a 1995 paper suggested an 11% loss rate in these cases, which caused considerable concern.19 Fortunately, the issue was settled by a much larger collaborative series in 1998 that showed that loss rates were no higher than comparable controls of MFPR patients who did not have amniocentesis.20 The collaborative data show a loss rate of 5%, which was certainly no higher than in the group of patients postMFPR who did not have genetic studies.
Table 4. Maternal age and ART (SART data 2003)
| All cases | 122,872 |
| Fresh, nondonor | 91,032 |
| <35 | 39,852 |
| 35–37 | 20,056 |
| 38–40 | 18,600 |
| 41–42 | 8,185 |
| >42 | 4,279 |
Since the centers with the most MFPR experience were also the ones that had the same accomplishments with chorionic villus sampling (CVS), combinations of the procedures were very logical.21 Over the years, we have increased the percentage of patients who have CVS prior to MFPR to nearly 80% of our patients. We perform a CVS usually on one more than the intended stopping number, and performed a fluorescent in situ hybridization (FISH) analysis with probes for chromosomes 13, 18, 21, X, and Y.13 Whereas about 30% of overall anomalies seen on karyotype would not be detectable by FISH with these probes,21, 22, 23 the absolute risk of a remaining undetected, clinically relevant anomaly is very small. Given both a normal FISH and a normal ultrasound including nuchal translucency,24 the residual risk is only about 1/400 to 1/500.13, 24 In fact, we have recently articulated that when there is a discrepancy between the FISH and karyotype, that the FISH is actually more likely than the karyotype to reflect the actual fetal status.25 We believe that such a risk is lower than the increased risk from the 2 week wait necessary to get the full karyotype. We have now commonly extended this approach to all patients who are appropriate candidates for prenatal diagnosis regardless of the fetal number (Figure 2). With data now suggesting increased risks of chromosomal and other anomalies in patients conceiving by IVF and especially with intracytoplasmic sperm injection (ICSI), the utilization of prenatal diagnosis will likely increase even further.26, 27, 28
{kind=link}
CLINICAL USES
MFPR is a clinical procedure developed in the 1980s when a small number of clinicians in both the United States and Europe attempted to reduce the usual and high, adverse sequelae of multifetal pregnancies by selectively terminating or reducing the number of fetuses to a more manageable number. The first European report by Dumez,29 and the first American report by Evans et al.,30 followed by a further report by Berkowitz et al.,31 and later Wapner et al.32 described a surgical approach to improve the outcome in such cases. Today virtually all experienced operators perform the procedure inserting needles transabdominally under ultrasound guidance, although some unpublished data have suggested that some centers continue to use 6–8 week transvaginal reduction procedures despite considerably higher loss rates.
RESULTS
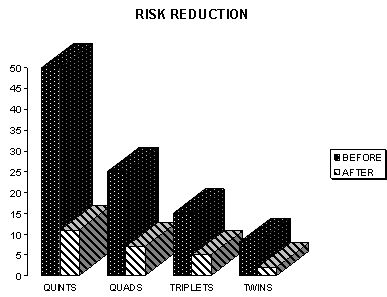
Several centers with the world’s largest experience have collaborated to increase the power of their data. In 1993 the first collaborative report showed a 16% pregnancy loss rate through 24 completed weeks.33 Such numbers actually represented a major improvement for higher order multiple pregnancies. Further collaborative papers have shown continued dramatic improvements in the overall outcomes of such pregnancies (Table 2).13, 15 The 2001 collaborative data demonstrated that the outcome of triplets reduced to twins, and quadruplets reduced to twins now perform essentially as if they started as twins.15 Even with the tremendous advances in neonatal care for premature babies, the 95% take home baby rate for those who start with triplets and the 92% take home baby rate for those who start with quadruplets clearly represent dramatic improvements over natural statistics. Not only has the pregnancy loss rate been substantially lowered, but so has the rate of very dangerous early prematurity. Both continue to be correlated with the starting number. Data from the past few years show that the improvements are, not surprisingly, greatest from the higher starting numbers (Figure 3).13, 34
{kind=link}
The lowest pregnancy loss rates are for those cases reduced to twins with increasing losses for singletons followed by triplets. The differences between leaving twins versus singletons has narrowed as an increasing percentage of cases have been triplets to twins or a singleton or twins to a singleton.34 The rate of early premature delivery has been, not surprisingly, highest with triplets followed by twins and lowest with singletons. Mean gestational age at delivery was also lower for higher order cases. Birth weights following MFPR decreased with starting and finishing numbers reflecting increasing prematurity.35
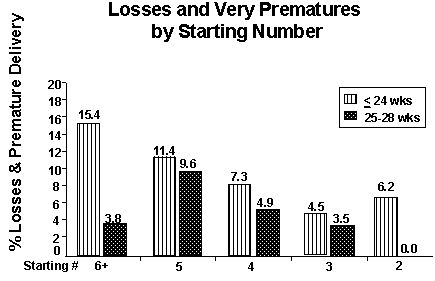
While there are still some arguments, particularly from conservative commentators, our experiences suggest that triplets reduced to twins do much better in terms of loss and prematurity than do unreduced triplets. We believe that if a patient’s primary goal is to maximize the chances of surviving children, that reduction of triplets to twins or a singleton achieves the best live born results. The trade off is between morbidity and mortality. More recent analyses suggest that while mortality is lowest with twins, morbidity is lowest with remaining singletons. Recent data have also suggested that adverse perinatal outcomes are more common in IVF patients even in singletons.36, 37 Numerous papers argued over the past several years whether triplets have better outcomes “reduced” or not. Yaron et al.38 compared triplets to twins data to unreduced triplets with two large cohorts of twins. The data show substantial improvement of reduced twins as compared to triplets. The data from the most recent collaborative series suggest that pregnancy outcomes for cases starting at triplets or even quadruplets reduced to twins do fundamentally as well as starting as twins. Antsaklis et al. showed a reduction of losses from 15.41% to 4.76% for twins and diminishment of low birth weight from 28% to 11%.39 These data therefore support some cautious aggressiveness in infertility treatments to achieve pregnancy in difficult clinical situations. However, when higher numbers occur, good outcomes clearly diminish. Luke et al. have suggested that in twin pregnancies with assisted reproduction fetal reduction increased the risks for birth at <30 weeks, very low birth weight, and slowed midgestational growth.40 This analysis, however, ignores that starting conditions, i.e., as compared to keeping the quadruplets, how did they do? Kozinsky et al. showed that the perinatal outcomes of singleton and twin pregnancies following ARTs were comparable to spontaneously conceived, matched pregnancies.41 McDonald et al. have recently shown in a meta-analysis that twins from IVF even when matched to spontaneously conceived twins had somewhat higher risks for preterm birth but no significant differences in perinatal deatlhs, congenital malformations or low birth weight.42 A 2001 paper suggested that reduced triplets did worse than continuing ones.43 However, analysis of that series showed a loss rate following MFPR twice that seen in our collaborative series15 and poorer outcomes in every other category for the remaining triplets. Several other recent papers have likewise shown higher risks for “unreduced” triplets than for reduced cases.44, 45, 46, 47 It is clear that one must use extreme caution in choosing comparison groups. Blickstein has reported that triplets do worse than reduced twins in every perinatal category in his large database.48
An ever increasing situation involves the inclusion of a monozygotic (MZ) pair of twins in a higher order multiple.49 Our experience suggests that provided the “singleton” seems healthy, that the best outcomes are achieved by reduction of the MZ twins. Obviously, if the singleton is not healthy, then keeping the twins is the next choice. Pregnancy loss is not the only deleterious outcome. Very early preterm delivery correlates with the starting number. However, it has not been well appreciated that about 20% of babies born at less than 750 g develop cerebral palsy.50 In Western Australia, Petterson et al. showed that the rate of cerebral palsy was 4.6 times higher for twins than singletons per live birth, but 8.3 times higher when calculated per pregnancy.51 Pharoah and Cooke calculated cerebal palsy rates per 1000 first year survivors at 2.3 for singletons, 12.6 for twins, and 44.8 for triplets.52 In a small series in a report of a questionnaire Dimitiriou et al. showed no differences between triplets and twins, but there was insufficient power to reach such conclusions.53
In the 2001 collaborative report the subset of patients who reduced from two to one (not for fetal anomalies) included 154 patients. These data suggested a loss rate comparable to three to two, but, in about one third of the two to one cases, there was a medical indication for the procedure, e.g., maternal cardiac disease or prior twin pregnancy with severe prematurity, or uterine abnormality.15 In recent years, however, the demographics have been changing and the vast majority of such cases are from women in their 40s, or even 50s, some of whom are using donor eggs and who, more for social than medical reasons, only want a singleton pregnancy.21, 43, 44, 45 New data suggest that twins reduced to a singleton do better than remaining as twins.17, 34 Consistent with the above, more women are desiring to reduce to a singleton. In a recent series of triplets, we found the average age of outpatients reducing to twins to be 37 years and to a singleton 41 years.17 While the reduction in pregnancy loss risk for three to one is not as much as three to two (15% to 7% and 15% to 5%, respectively), the gestational age at delivery for the resulting singleton is higher, and the incidence of birth weights <1500 g is 10 higher for twins than singletons.1 These data have made counseling of such patients far more complex than in the past (Figure 4). Not surprisingly there are often differences between members of the couple as to the desirability of twins or a singleton.54 There are also profound public health implications regarding these decisions, as 2000 United States data showed that of $10.2 billion spent per year on initial newborn care, 57% of the money was spent on the 9% of babies born at <37 weeks.55, 56, 57 In 2003, more than $10 billion was spent on the 12.3% born preterm.56 The Institute of Medicine in 2006 reported that preterm births cost the United States approximately $26 billion per year.57 Data are now also emerging that there is considerably higher neurologic and developmental disability in 6 year olds who survived birth at 26 weeks or less. The rates of severe, moderate, and mild disabilty were 22%, 24%, and 34%, respectively. Significant cerebral palsy was present in 12%.58 Hack et al. also have now shown that in babies born at less than 1000 g, the rate of cerebral palsy was 14% as opposed to 0% for controls. Asthma, poor vision, IQ <85, and poor motor skills were all also substantially higher.59
{kind=link}
As a results of all of the above and the changing demographics as to which women are having infertility and desiring reductions, we believe that reduction of twins to a singleton is likely to become more common over the next several years. Some programs now have as many as one third of all reduction patients going to a singleton.34 In our own personal experience the proportion is between 10 and 15%.13, 17
SOCIETAL ISSUES
While MFPR has become a completely integral part of infertility therapies, it will always be controversial because of widely divergent religious and other moral positions. For all but the most conservative of phyisicans and ethicists, the debate over the desirability of reducing triplets to improve outcomes is long since over. A serious debate will emerge over whether it will be appropriate to offer MFPR routinely for twins, even natural ones for whom the outcome has commonly been considered “good enough”.17 Our data suggest that reduction of twins to a singleton actually improves the outcome of the remaining fetus.17 No consensus on appropriateness of routine two-to-one reductions, however, is ever likely to emerge. We do, however, expect the proportion of patients reducing to a singleton to steadily increase over the next several years.
Over the years, much has been written on the subject of MFPR. Opinions, in our experience, have never followed the classic “pro-choice/pro-life” dichotomy.13, 15, 18 Opinions will always vary substantially from outraged condemnation to complete acceptance. No short paragraph could do justice to the subject other than to state that most proponents do not believe this is a frivolous procedure, but see it in terms of the principle of proportionality, i.e., therapy to achieve the most good for the least harm.60, 61, 62 What we do in this section is review a few studies that have immediate implications for MFPR clinics and ART clinics by virtue of giving some insight into how patients frame the decisions they are making and structure their social environments so as to reduce the risk of hostility in reaction to these choices.
How patients “hear” and internalize data and make decisions with respect to reduction have been fascinating to us over the years. Much of the literature on medical decision making has emphasized a rational choice model that puts hard data regarding relative risks center stage and treats emotions, feelings, and values as complications that should be considered only as a second stage analysis.63, 64 Even in the literature that talks about genuine alternative models of decision making (systematic versus heuristic, for example), a central assumption is that there are individual differences in style that can be identified through what people say.65, 66
We have approached this problem from a different direction, arguing that where controversial, high-anxiety decisions are concerned, patients treat these decisions as an ongoing part of the social reality that they are creating to live in and raise a family.67 This reality-construction process is proactive, with couples aware of the potential consequences of sharing with others what they are going through. In a recent study of sharing strategies among MFPR patients, we discovered four sharing strategies that varied in how selectively information regarding their situation and choices was shared.68 Strategies for sharing ranged in terms of selectivity from a defended-relationship approach in which only the partner and patient knew about the problems the patient was facing and the decision to reduce, through a qualified family and friends strategy in which information is shared only with those who appear to be trustworthy in terms of their reactions. Two less selective strategies also emerged from our analysis. In the first, both sets of parents are privy to what the couple is going through, and, finally, there is an extended, open network strategy of family, friends, and colleagues being in the loop.
No sharing strategy is completely free of the risk of encountering hostility. Even so, the odds of encountering hostility are significantly greater with the more open, less selective strategies. MFPR and ART clinics will vary in terms of the cultural style they have for handling patient anxiety and stress, but these results suggest that some way should be found to sensitize couples to the fact that selectively sharing what they are going through is an effective technique for at least neutralizing some of the hostility that they are at risk of confronting from family, friends, and others. To the extent that anxiety and stress have implications for clinic success rates, such results regarding sharing strategies become doubly important.
The realities people construct – composed of supportive people and institutions together with complexes of supportive values, norms, and attitudes – are the source of frames that the patients use to view the data.60, 61, 62 The decisions they make and how they justify those decisions may help resolve incompatible elements in the realities in which they find themselves enmeshed. It may often happen, for example, that parents who have gone through reduction to two or one live in families and/or work in communities where having engaged in reduction would be considered as something shameful. The less control they have over the selection of family, friends, and workplaces, given the prospect of such stigma, the more likely they are to simply present their pregnancies to these publics as if their pregnancies had always involved twins or singleton. Where they have more control over the situation – as typically happens with friends versus family – they may be more likely to selectively share their experiences. The social realities in which people live, however, involve more than people. They also involve values, norms, and attitudes.69 The one thing all MFPR patients have in common is a very strong desire to have a family (Table 5). But there does not appear to be a single set of supportive institutions, people, and norms that is conducive to going through the pain, stress, and resource expenditure of IVF. Rather, there are three alternative resolutions. The first of these, a rational medical frame, looks superficially like what one would expect from the rational analysis model. But the commitment to factual analysis comes typically from patients’ having selected themselves into the hard sciences, medicine, dentistry, engineering or the law – disciplines in which an appreciation of and trust in “facts“ form a fundamental part of their disciplinary identity. Such women will want to see the numbers regarding the relative risk associated with different reduction choices and will want to engage in a rigorous discussion of the data and their implications even if it is relatively painful to do so. And they will be likely to choose a final number for reduction that maximizes the chances of a “take-home” baby.
The lens of scientific objectivity is not the only frame through which women who have gone through IVF in order to have a child will examine these data (Table 5). For those who have immersed themselves in a social reality that has a strong emphasis on norms against abortion and/or reduction – such that they themselves have such normative beliefs and are heavily involved in religious institutions which reinforce similar beliefs – a detached examination of the “facts” is simply not possible. These “facts” hold no special moral authority and need not be trusted in and of themselves. Their beliefs and those of the individuals and social institutions in which they have selected themselves have a moral authority as well. The balance that such women will likely seek is one that reduces their relative risk to acceptable limits. So, unless the consequences are dire, they will not reduce at all or choose to reduce only to three. We labeled such a resolution a conceptional frame because believing that life begins at conception seems to be a central tenet.
Table 5. Frame comparisons
| Medical Frame | Conceptional Frame | Lifestyle Frame |
| Intensity of commitment to having children | High | High | High |
| Intensity of training in medicine, dentistry, hard sciences, and the law | High | Low | Modest |
| Intensity of commitment to belief that life begins at conception | Modest | High | Modest |
| Intensity of commitment to career | High | Low | High |
| Source of moral authority for resolution | Relative survivability of fetuses | Minimization of damage to moral beliefs though a “barely sufficient” reduction | Having a “normal” life in a culture that values both careers and family for women |
Finally, there are those for whom the demands of career and/or existing children constitute powerful elements in their constructed realities. For such women – and this includes many of the older patients we encountered – the essential balance that they seek is a more secular one, a lifestyle frame, one that emphasizes creating a family situation in which having a family can be balanced with working – though the commitment to working is less than the intense career commitment seen among medical frame patients. Such women will more than likely choose reduction to two or even one embryo, depending on the number of other children they have and the level of resources that the family has.
Clinicians and their counseling staff need to be aware that for women who have selected themselves into and/or been trained to accept the legitimacy of rigorously determined statistics regarding relative risk (a medical frame) reduction choices can be straightforward – or at least they can appear to be relatively straightforward. This is usually not the case, however, for women who must forge a resolution amongst potentially incompatible elements, as for women who are struggling to reconcile the potentially oppositional elements of religious beliefs and involvement with risks associated with higher-level pregnancies (conceptional frame), or those who are struggling to reconcile the potentially conflicting identities of home and work (lifestyle frame).
Clinics have different styles of dealing with the multi-sourced anxieties with which patients walk through the door. The results that we have presented suggest that there is no “one size fits all” way of counseling and supporting patients. We expect, however, that successful clinics will have developed ways of understanding better where patients are coming from and what types of information and support will help them the most.
SUMMARY
Over the last two decades MFPR has become a well-established and integral part of infertility therapy and the attempts to deal with sequelae of aggressive infertility management. In the mid-1980s, the risks and benefits of the procedure could only be guessed.20, 23, 38, 39 We now have very clear and precise data on the risks and benefits as well as an understanding that the risks increase substantially with the starting and finishing number of fetuses in multifetal pregnancies. The collaborative loss rate numbers, i.e., 4.5% for triplets, 8% for quadruplets, 11% for quintuplets, and 15% for sextuplets or more seem reasonable ones to present to patients for the procedure performed by an experienced operator. Our own experience and anecdotal reports from other groups suggest that less experienced operators have worse outcomes.
Pregnancy loss is not the only poor outcome. The other main issue with which to be concerned is very early preterm delivery and the profound consequences to such infants. Here again there is an increasing rate of poor outcomes correlated with the starting number. The finishing numbers are also critical, with twins having the best viable pregnancy outcomes for cases starting with three or more. Triplets and singletons do not do as well. However, an emerging appreciation that singletons have prematurity rates less than those of twins is making the counseling far more complex. We continue to hope, however, that MFPR will become obsolete as better control of ovulation agents and ART make multifetal pregnancies uncommon.
REFERENCES
Martin JA, Hamilton BE, Sutton PD, et al. Births: Final Data for 2005. National Vital Statistics Reports vol 56#6. National Center for Health Statistics, Hyattville, MD, 2007. |
|
Society of Assisted reproductive technologies website: Clinic Summary Report for 2005: https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?ClinicPKID=0 |
|
Blickstein I: Estimation of iatrogenic monozygotic twinning following assisted reproduction: Pitfalls and caveats. Am J Obstet Gynecol 2005; 192:365-8 |
|
Toledo MG: Is there increased monozygotic twinning after assisted reproductive technology? Aust NZ Obstet Gynecol 2005; 45:360-4 |
|
Shinwell ES, Blickstein I: The risks for very low birth weight infants from multiple pregnancies. Clin Perinatol 2007; 34:587-97 |
|
Corbellini G: Scientists, bioethics, and democracy: the Italian case and its meanings. J Med Ethics 2007;33:349-52 |
|
La Sala GB, Villani MT, Nicoli A, et al: The effect of legislation on outcomes of assisted reproductive technology: lesions from the 2004 Italian law: Fertil Steril 2008;89:854-859 |
|
Blickstein I: Litigation in multiple pregnancy and birth. Clin Perinatol 2007; 34:319-27 |
|
Blickstein I, Keith LG: The decreased rates of triplet births: temporal trends and biologic speculations. Am J Obstet Gynecol 2005; 193:327-31 |
|
Evans MI, Ayoub MA, Shalhoub AG, Feldman B, Yaron Y. Spontaneous abortions in couples declining multifetal pregnancy reduction. Fetal Diagn Ther 2002;(17):343- 346. |
|
Keith LG & Blickstein I (eds) Triplet Pregnancies Parthenon Press, London 2002 |
|
Luke B, Brown MB, Nugent C, Gonzalez-Quintero VH, Witter FR, and Newman RB. Risks factors for adverse outcomes in spontaneous versus assisted conception twin pregnancies. Fertil Steril. 2004;81(2):315-9. |
|
Evans MI, Ciorica D, Britt DW, Fletcher JC: Reduction in Multiple Pregnancies in Evans MI, Johnson MP, Yaron Y, Drugan A: (eds). Prenatal Diagnosis: Genetics, Reproductive Risks, Testing, and Management. McGraw Hill Publishing Co., New York. 2006 pp561-570 |
|
2004 Assisted Reproductive Technology Success Rates: National Summary and Fertility Clinic Reports. Centers for Disease Control: January 2007, US Gov’t Printing Office |
|
Evans MI, Berkowitz R, Wapner R, Carpenter R, Goldberg J, Ayoub MA, Horenstein J, Dommergues M, Brambati B, Nicolaides K, Holzgreve W, Timor-Tritsch IE. Multifetal pregnancy reduction (MFPR): Improved outcomes with increased experience. Am J Obstet Gynecol 2001;184:97-103. |
|
Adashi EY, Barri PN, Berkowitz R, et al: Infertility therapy-Assisted Multiple Pregnancies (births): An on-going epidemic. Reprod Med OnLine. 2003; (7):515-542. |
|
Evans MI, Kaufman M, Urban AJ, Britt DW, Fletcher JC: Fetal Reduction from Twins to a Singleton: A Reasonable Consideration. Obstet Gynecol 2004;104:102-109. |
|
Evans MI, Littman L, St Louis L, LeBlanc L, Addis J, Johnson MP, Moghissi KS. Evolving patterns of iatrogenic multifetal pregnancy generation: implications for aggressiveness of infertility treatments. Am J Obstet Gynecol 1995;(172):1750-1753. |
|
Tabsh KM, Theroux NL. Genetic amniocentesis following multifetal pregnancy reduction twins: Assessing the risk. Prenat Diagn 1995;(15):221-223. |
|
McLean LK, Evans MI, Carpenter RJ, Johnson MP, Goldberg JD. Genetic amniocentesis (AMN) following multifetal pregnancy reduction (MFPR) does not increase the risk of pregnancy loss. Prenat Diagn 1998;(18):186-188. |
|
Brambati B, Tului L, Baldi M, Guercilena S. Genetic analysis prior to selective termination in multiple pregnancy: Technical aspects and clinical outcome. Hum Reprod 1995;10:818-825. |
|
Evans MI, Henry GP, Miller WA, et al. International, Collaborative Assessment of 146,000 Prenatal Karyotypes: Expected Limitations if only Chromosome-Specific Probes and Fluorescent In Situ Hybridization were used. Hum Reprod 1999;14:1213-16. |
|
Homer J, Bhatt S., Huang B and Thangavelu M: Residual risk for cytogenetic abnormalities after prenatal diagnosis by interphase fluorescence in situ hybridizatio (FISH). Prenatal Diagn 2003;23:556-571. |
|
Greene RA, Wapner J, Evans MI: Amniocentesis and choironic villus sampling in triplet pregnancy In, Keith LG, Blickstein I, Oleszcuk JJ (eds.) Triplet Pregnancy. Parthenon Publishing Group, London, New York , pp 73-84. |
|
Evans M, Andriole S, Pergament E: Changing the paradigm: both FISH and karyotype should be routine for prenatal diagnosis. Am J Obstet Gynecol 2006; 197:S167 |
|
Pinborg A, Loft A, Schmidt L, Andersen AN. Morbidity in a Danish national cohort of 472 IVF/ICSI twins, 1132 non-IVF/ICSI twins and 634 IVF/ICSI singletons: health-related and social implications for the children and their families. Hum Reprod. 2003;18(6):1234-43. |
|
Retzloff MG, Hornstein MD. Is intracytoplasmic sperm injection safe? Fertil Steril 2003; 80(4):851-9. |
|
Kurinczuk JJ. Safety issues in assisted reproduction technology. From theory to reality—just what are the data telling us about ICSI offspring health and future fertility and should we be concerned? Hum Reprod 2003;18(5);925-31. |
|
Dumez Y, Oury JF. Method for first trimester selective abortion in multiple pregnancy. Contrib Gynecol Obstet 1986; (15):50. |
|
Evans MI, Fletcher JC, Zador IE, Newton BW, Struyk CK, Quigg MH. Selective first trimester termination in octuplet and quadruplet pregnancies: clinical and ethical issues. Obstet Gynecol 1988;(71):289-296. |
|
Berkowitz RL, Lynch L, Chitkara U, et al: Selective reduction of multiple pregnancies in the first trimester. N Engl J Med. 1988; 318:1043. |
|
Wapner RJ, Davis GH, Johnson A. Selective reduction of multifetal pregnancies. Lancet 1990;(335):90-3. |
|
Evans MI, Dommergues M, Wapner RJ, Lynch L, Dumez Y, Goldberg JD, Zador IE, Nicolaides KH, Johnson MP, Golbus MS, Boulot P, Berkowitz RL. Efficacy of transabdominal multifetal pregnancy reduction: collaborative experience among the world's largest centers. Obstet Gynecol 1993;82:61-67. |
|
Stone J, Belogolovkin V, Matho A, et al: Evolving trends in 200 cases of multifetal pregnancy reduction: a single center experience. Am J Obstet Gynecol 2007; 394.e1-4 |
|
Torok O, Lapinski R, Salafia CM, Bernasko J, Berkowitz RL: Multifetal pregnancy reduction is not associated with an increased risk of intrauterine growth restriction, except for very high order multiples. Am J Obstet Gynecol 1998;(179):221-5. |
|
Jackson RA, Gibson KA, Wu YU et al: Perinatal outcomes in singletons following in vitro fertilization: a meta analysis. Obstet Gynecol 2004; 103: 551-63 |
|
Schieve LA, Ferre C, Peterson HB, et al: Perinatal outcome among singleton infants conceived through assisted reproductive technology in the United States Obstet Gynecol 2004; 103: 1144-53 |
|
Yaron Y, Bryant-Greenwood PK, Dave N, et al: Multifetal pregnancy reduction (MFPR) of triplets to twins: Comparison with non-reduced triplets and twins. Am J Obstet Gynecol 1999;(180):1268-71. |
|
Antsaklis A, Souka AP, Daskalakis G, et al: Embryo reduction versus expectant management in triplet pregnancies. J Matern Fetal Neonatal Med 2004; 16: 219-22 |
|
Luke B, Brown MD, Nugent C, et al: Risk factors for adverse outcomes in spontaneous versus assisted conception in twin pregnancies. Fertil Steril 2004: 81 315-9 |
|
Kozinsky Z, Zadori J, Ovros H, et al: Obstetric and neonatal risk of pregnancies after assisted reproductive technology: a matched control study Acta Obstet Gynecol Scand 2003; 82:850-6 |
|
McDonald S, Murphy K, BeyeneJ, et al Perinatal outcomes of in vitro fertilization twins: A systematic review and meta analysis. Am J. Obstet Gynecol 2005; 193:141-52. |
|
Leondires MP, Ernst SD, Miller BT, et al. Triplets: outcomes of expectant management versus multifetal reduction for 127 pregnancies. Am J Obstet Gynecol 1999;72:257-60. |
|
Lipitz S, Shulman A, Achiron R, et al. A comparative study of multifetal pregnancy reduction from triplets to twins in the first versus early second trimesters after detailed fetal screening. Ultrasound Obstet Gynecol 2001;(18):35-8. |
|
Angel JL, Kalter CS, Morales WJ, et al. Aggressive perinatal care for high-order multiple gestations: Does good perinatal outcome justify aggressive assisted reproductive techniques? Am J Obstet Gynecol 1999;(181):253-9. |
|
Sepulveda W, Munoz H, Alcalde JL. Conjoined twins in a triplet pregnancy: early prenatal diagnosis with three-dimensional ultrasound and review of the literature. Ultrasound Obstet Gynecol 2003;22(2):199-204. |
|
Francois K, SEARS C, Wilson R, Elliot J. Twelve year experience of triplet pregnancies at a single institution. Am J Obstet Gynecol 2001;(185):S112. |
|
Blickstein I: How and why are triplets disadvantaged compared to twins. Best Pract Res Clin Obstet Gynecol 2004;18:631-44 |
|
Yakin K, Kahraman S, Comert S. Three blastocyst stage embryo transfer resulting in a quintuplet pregnancy. Hum Reprod 2001;16(4):782-4. |
|
Neonatal Encephalopathy and Cerebral Palsy: defining the pathogensis and pathophysiology. Task Force of American College of Obstetricians and Gynecologists, ACOG Washington DC, 2003. |
|
Petterson B, Nelson K, Watson L et al. Twins, triplets, and cerebral palsy in births in Western Australia in the 1980s. BMJ 1993;307: 1239-1243. |
|
Pharoah PO, Cooke T. Cerebral Palsy and Multiple Births. Arch Dis Childhood Fetal Neonatal edn 1996;(75), F174-177. |
|
Dimitriou G, Pharoah PO, Nicolaides KH, et el: Cerebral Palsy in triplet pregnancies with and without iatrogenic reduction. Eur J Pediatr 2004; 163:449-51 |
|
Kalra SK, Milad MP, Klock SC, Crobman WA: Infertility patients and their partners: differences in the desire for twin gestations. Obstet Gynecol 2003;102:152-155. |
|
St. John EB, Nelson KG, Oliver SP, Bishno, RR, Goldenberg RL. Cost of Neonatal care according to gestational age at birth and survival status. Am J Obstet Gynecol 2000;(182):170-175. |
|
Cuevas KD, Silver DR, Brooten D, et al: The cost of prematurity: Hospital charges at birth and frequency of rehospitalizations and acute care visits over the first year of life: a comparison by gestational age and birth weight. Am J Nurs 2005; 105:56-64. |
|
Preterm Birth: causes, consequences, and prevention. Committee on Understanding Premature Birth and Assuring Healthy Outcomes Board on Health Science Policy. Institute of Medicine. National Academic Press Washington, DC 2006 |
|
Marlow N, Wolke D, Bracewell MA, et al: Neurologic and developmental disability at six years of age after extremely preterm birth. N Engl J Med 2005; 352:9-19. |
|
Hack M, Taylor HG, Drotar D, et al: Chronic conditions, functional limitations, and special health care needs of school-aged children born with extremely low birth weights in the 1990’s. JAMA 2005;294:318-325 |
|
Britt DW, Risinger ST, Mans M, Evans MI. Devastation and relief: conflicting meanings in discovering fetal anomalies. Ultrasound Obstet Gynecol 2002;20:1-5. |
|
Britt DW, Risinger ST, Mans M, Evans MI. Anxiety among women who have undergone fertility therapy and who are considering MFPR: Trends and Scenarios. J Matern Fetal Neonat Med 2003;13:271-8. |
|
Britt DW, Evans WJ, Mehta SS, and Evans MI. Framing the decision: Determinants of how women considering MFPR as a pregnancy-management strategy frame their moral dilemma. Fetal Diagn Ther 2004;(19):232-240. |
|
Redelmeier, DA, Rozin, P, Kahneman, D. Understanding patients’ decisions: cognitive and emotional perspectives. JAMA 1993; 270: 72-76. |
|
Chapman, GB, and Elstein, AS. (2000) Cognitive processes and biases in medical decision making. In Chapman, GB, and Sonnenberg, FA (Eds.). Decision Making in Health Care: Theory, Psychology and Applications. Cambridge University Press: New York. Pp. 183-210. |
|
Steginga SK, Occhipinti S. The application of the heuristic-systematic processing model to treatment decision making about prostate cancer. Med Decis Making 2004;24:573-83 |
|
Hamm RM. Theory about heuristic strategies based on verbal protocol analysis: The emperor needs a shave. Med Decis Making 2004;24:681-686 |
|
Britt DW, Campbell EQ. Assessing the Linkage of Norms, Environments and Deviance. Social Forces, 1977;(December):532-549. |
|
Britt DW, Evans MI: Information sharing among MFPR patients. Fertil Steril 2007;87:490-95 |
|
Britt DW, Evans MI: “Sometimes doing the right thing sucks”: Frame combinations and MFPR decision difficulty. Social Science Med 2007:65:2342-2356. |