Pathology of Endometrial Carcinoma
Authors
INTRODUCTION
Endometrial carcinoma has become the most common invasive malignancy of the female genital tract in the United States.1,2,3 The incidence is much lower in Asia, Africa, and South America. The higher incidence in the United States is accounted for in part by the widespread use of unopposed exogenous estrogen for postmenopausal women until the 1970s. Extended longevity resulting in a higher median age for women may also be a factor.2 However, the steady increase in incidence cannot be accounted for by these conditions alone, suggesting that a lowering of the threshold for the diagnosis of endometrial carcinoma may also be a contributing factor.4
Well-documented conditions known to be associated with an increased risk of endometrial carcinoma include obesity, nulliparity, early menarche, and late menopause. Obesity appears to pose the greatest risk, especially patients 50 or more pounds over their ideal body weight.5,6 Aromatization of androstenedione to estrone, which occurs in peripheral fat, appears to be the source of the increased circulating levels of estrogen in obese patients.7 Diabetes mellitus,8 hypertension, family history, a high-fat diet,9 and previous radiation have all been implicated in the increased incidence of endometrial carcinoma.10 Interestingly, a decreased rate of occurrence is seen in cigarette smokers; this has been explained by endometrial atrophy.11 However, smoking in conjunction with the use of exogenous estrogen significantly multiplies the risk of developing endometrial carcinoma, especially in thin women.12,13
The median age for diagnosis of endometrial carcinoma is about 60 years. Abnormal bleeding is the most common presenting symptom, but a few patients are asymptomatic.10,14 Because there is no adequate screening test for endometrial cancer, it is common practice to sample the endometrium of postmenopausal women who experience abnormal bleeding. The Pap smear, although adequate for screening for cervical intraepithelial neoplasia and carcinoma, has an unacceptably high false-negative rate for detecting endometrial cancer.
Endometrial carcinomas with associated hyperplasia tend to be well differentiated and have lesser degrees of myometrial invasion than lesions without such an association.15,16,17 Exogenous estrogen users have better-differentiated tumors than women who do not use estrogen. More aggressive variants of endometrial carcinoma, such as serous and clear cell carcinoma, are usually not associated with or preceded by hyperplasia.
These data suggest that two classifications of endometrial carcinoma exist.10,14,15,18,19 One group, accounting for 65% of cases,10,19 is found in association with a high estrogen state, either endogenous or exogenous, and occurs in perimenopausal white women. This is usually a low-grade carcinoma of favorable prognosis, often accompanied by or preceded by hyperplasia, and has minimal myometrial invasion. Cessation of the hormonal stimulus may result in regression of these low-grade lesions. The second type has no known predisposing conditions10,19,20 or any association with exogenous estrogen use or endometrial hyperplasia. These lesions are usually high-grade, aggressive neoplasms occurring in postmenopausal women, often disproportionately of Asian or African-American descent.10,14,20,21,22
GROSS FINDINGS
Endometrial carcinoma most frequently arises in the corpus proper, but it may also originate in the lower uterine segment. There are no distinctive gross appearances to differentiate individual subtypes (cell type). In low-volume disease, it is common to find no evidence of residual disease after diagnostic endometrial curettage.23 Localized disease manifests as round, polypoid expansile masses that are friable and often hemorrhagic. Diffuse involvement of the endometrium may show an indurated-appearing surface without a visible exophytic component. Necrosis and hemorrhage may be seen. Foci of myometrial invasion generally appear grossly as well-demarcated gray-white areas that are lighter in color than the surrounding uninvolved myometrium. Extension from the surface lesion is commonly demonstrated.
Intraoperative pathology consultation may be obtained to determine the depth of gross myometrial invasion or cervical extension. With the revised International Federation of Gynecology and Obstetrics (FIGO) staging system,22 this important information may affect the remaining course of the surgical procedure. Ideally, the pathologist should measure both the width of the myometrium and the depth of the tumor invasion.
GENERAL HISTOPATHOLOGIC FEATURES
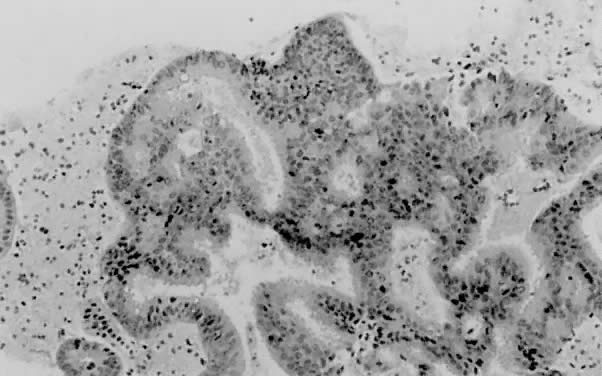
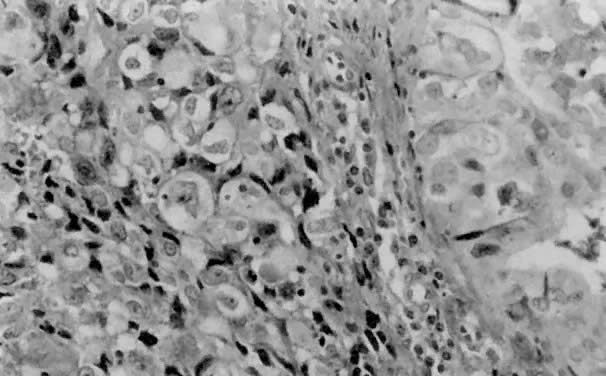
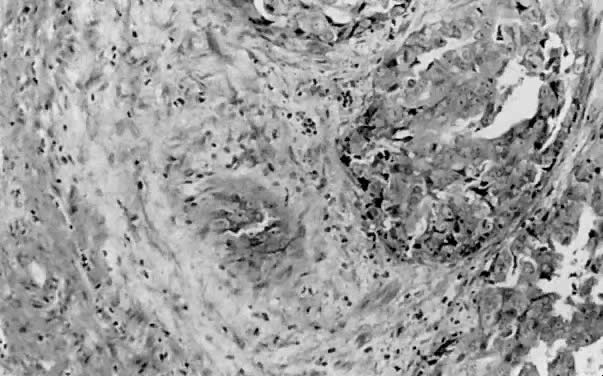
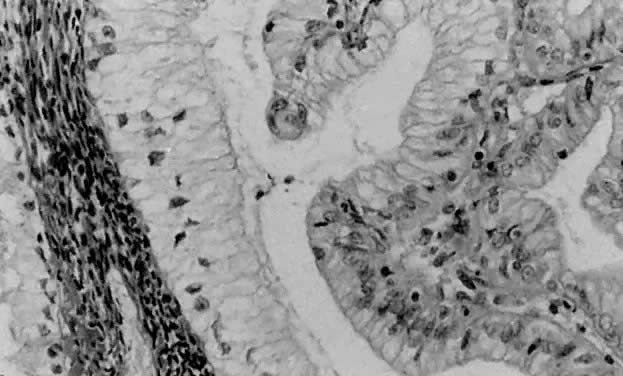
Endometrial carcinoma is divided into numerous histologic categories based on cell type (Table 1). The most common cell type, endometrioid, accounts for 75% to 80% of cases.24,25,26 Due to its common occurrence, this variant is also known as typical endometrial adenocarcinoma. In well-differentiated forms, endometrioid adenocarcinoma produces small, round back-to-back glands without intervening stroma (Fig. 1). Varying degrees of glandular complexity are demonstrated by luminal infolding, budding, papillae (with or without psammoma bodies),27,28 and cribriforming. In grade 1 lesions, nuclei of the lining epithelial cells are uniform and oval to cylindrical, with minimal atypia and small discrete nucleoli. The cellular axes are perpendicular to the basement membrane, and stratification may or may not be present. Typically, high-grade tumors (with significant solid components) display an increased amount of nuclear atypia, as demonstrated by pleomorphism, irregular chromatin clumping, and prominent nucleoli (Fig. 2). If a greater degree of nuclear atypia exists that is not parallel to the architectural grade, it is appropriate to increase the overall tumor grade by one. The degree of tumor necrosis is usually mild to moderate. A marked amount of necrosis is unusual, even in high-grade endometrioid adenocarcinoma. Stroma adjacent to the invasive adenocarcinoma exhibits a desmoplastic reaction (Fig. 3), often with an accompanying lymphocytic infiltrate. Stromal foam cells generally are identified in well-differentiated tumors, especially those associated with hyperplasia.29
TABLE 1. Histopathologic Subtypes of Endometrial Carcinoma
- Endometrioid adenocarcinoma
Villoglandular (papillary)
Secretory
Ciliated cell
Adenocarcinoma with squamous differentiation - Mucinous carcinoma
- Serous carcinoma
- Clear cell carcinoma
- Squamous cell carcinoma
- Undifferentiated carcinoma
- Mixed carcinoma
- Metastatic carcinoma
{kind=link}
{kind=link}
{kind=link}
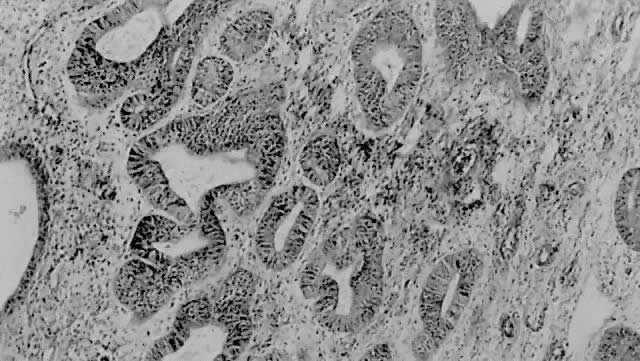
Recognizing discrete differences between complex hyperplasia with atypia (Fig. 4) and a well-differentiated carcinoma is often problematic. Investigators have shown that endometrial stromal invasion is the most helpful criterion for distinguishing between these two entities and is a reliable predictor of malignant behavior.4,23 Stromal invasion has been defined as:
{kind=link}
- Desmoplastic or fibroblastic stromal response that results in an abnormal and haphazard arrangement of glands
- Confluence or crowding of glands without intervening stroma, sometimes demonstrating cribriforming or bridging
- Complex, extensive papillary structures
- Replacement of stroma with squamous epithelium that expands the glandular elements.23
The first pattern is the most common. To be clinically significant, the less common patterns must be present in a focus greater than half of a low-power field (2.1 mm in diameter). Unfortunately, this requirement is difficult to fulfill, because the fragmented material obtained in an endometrial biopsy often fills less than half of a low-power field.30 Many grade 1 adenocarcinomas of the endometrium have little or no cytologic atypia; however, atypical hyperplasia may have severe nuclear aberrancy, thus rendering individual nuclear characteristics noncontributory in the distinction between hyperplasia and carcinoma.
Due to poor reproducibility, adenocarcinoma in situ is not accepted terminology in the current International Society of Gynecologic Pathologists (ISGYP) classification.4 Recently, however, a few authors have questioned this and argue for reconsideration of this concept, referring to entities such as adenocarcinoma in situ31 and endometrial intraepithelial carcinoma.32
HISTOPATHOLOGIC GRADING
In 1988, ISGYP and FIGO approved a revised grading scheme in response to preliminary findings of the Gynecology Oncology Group's (GOG) Protocol 33. Previous classifications lacked clear guidelines and resulted in poor reproducibility. This newer method of grading is predominantly based on architecture (Table 2). Adenocarcinomas having 5% or less nonsquamous or nonmorular solid growth are designated as grade 1, those with 6% to 50% solid growth as grade 2, and those with more than 50% solid growth as grade 3.
TABLE 2. Histopathologic Grading of Endometrial Carcinoma According to the 1988 FIGO Classification
Grade 1: Less than 5% of solid areas
Grade 2: 6–50% solid areas
Grade 3: More than 50% solid areas
Notable nuclear atypia, inappropriate for the architectural grade, raises the grade of a grade 1 or 2 tumor by one grade.
In serous, clear cell and squamous cell carcinoma, nuclear grade takes precedence.
In adenocarcinoma with squamous differentiation, the nuclear grade of the glandular component determines the histologic grade.
(Adapted from FIGO stages—1988 revision. Gynecol Oncol 35:125, 1989)
Unlike the 1971 FIGO grading, the revised system recognizes that occasional lesions have more nuclear atypia than is appropriate for the architectural grade. Significant nuclear atypia is defined as hyperchromasia, pleomorphism, irregular chromatin clumping, parachromatin clearing imparting a vesicular appearance, and loss of cellular polarity. If the nuclear grade is incongruent with the architectural grade, then the grade is increased by one (for grade 1 and 2 lesions). Nuclear grading takes precedence over architectural grading in serous, clear cell, squamous, and undifferentiated carcinomas, which are considered grade 3 lesions.
Overall, the current classification scheme results in very good reproducibility and correlates well with prognosis. The 5-year survival rate for grade 1 tumors is 89%. Grade 2 and 3 adenocarcinomas of the endometrium have a 5-year survival rate of 73% and 61%, respectively.3,33
VARIANTS OF TYPICAL ENDOMETRIAL (ENDOMETRIOID) ADENOCARCINOMA
Variants of endometrioid adenocarcinoma include villoglandular, secretory, ciliated cell, and adenocarcinoma with squamous differentiation. Overall, the epidemiologic characteristics of the subtypes are similar to those of typical endometrioid carcinoma; the few exceptions are mentioned with each section. Because it is not unusual to observe these patterns in association with the usual form of endometrioid cell type, most of the lesion must consist of the histologic features of the subtype for it to be considered a distinct entity.
Villoglandular (Papillary) Adenocarcinoma
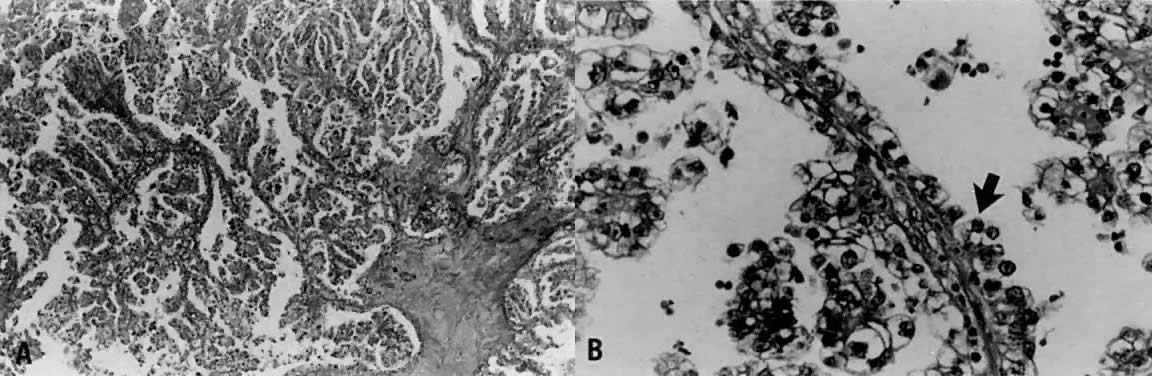
Villoglandular carcinoma is characterized by a papillary architecture with delicate fibrovascular stalks lined by cuboidal to columnar cells with minimal cellular stratification and mild nuclear pleomorphism (Fig. 5). Nucleoli are indistinct. It is important to distinguish this well-differentiated papillary variant of endometrial carcinoma from serous carcinoma, which is often papillary but displays grade 3 nuclear atypia with vesicular nuclei, prominent nucleoli, and necrosis.21,29 Serous carcinoma often forms papillary tufts, small clusters of cells that are detached from the papillary fronds. Psammoma bodies may be observed in either tumor type27 and are therefore not reliable distinguishing features. Villoglandular carcinoma only superficially invades the myometrium, being diagnosed at an early stage and thereby having a better prognosis than typical endometrioid carcinoma. To avoid confusion with papillary serous carcinoma, some authors refer to this entity as endometrioid adenocarcinoma with papillary architecture.
{kind=link}
Secretory Carcinoma
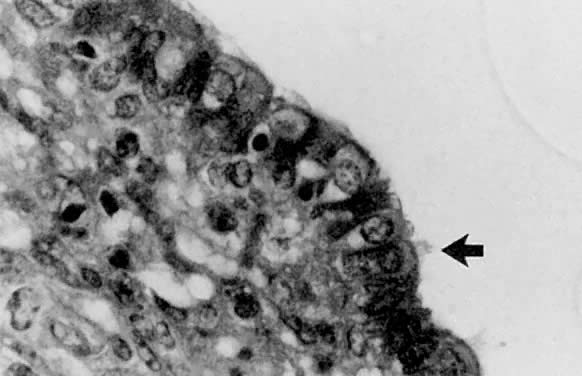
Less than 1% of endometrial adenocarcinomas are classified as secretory carcinomas.20 The well-differentiated glands of this variant appear histologically similar to secretory phase endometrium (postovulatory days 3 to 6), with abundantly vacuolated columnar cytoplasm, either subnuclear or supranuclear20,30,31,32,33,34,35 (Fig. 6). Cellular atypia is minimal. Squamous and tubal metaplasia frequently accompany this cell type.20 The adjacent nonmalignant endometrium typically shows changes consistent with prolonged or unopposed estrogen effect (e.g., hyperplasia, stromal breakdown, and thrombosis of vessels). The excellent prognosis seen in these patients is due to the fact that most have surgical stage I disease, and invariably the neoplasm is of low grade both architecturally and cytologically. Distinction from clear cell carcinoma is important due to the marked differences in prognosis. Although both types have intracytoplasmic glycogen, secretory carcinoma does not demonstrate papillary or cystic architecture, nor does it show grade 3 nuclear atypia or the hobnail pattern commonly seen in clear cell carcinoma. Separation of secretory carcinoma from secretory changes in atypical hyperplasia is based on the presence of stromal invasion and back-to-back glands found in carcinoma.
{kind=link}
Ciliated Cell Carcinoma
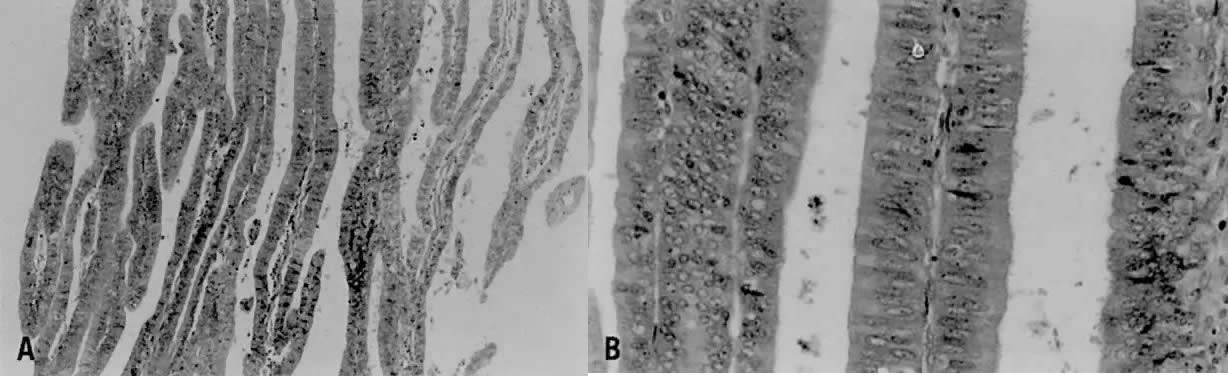
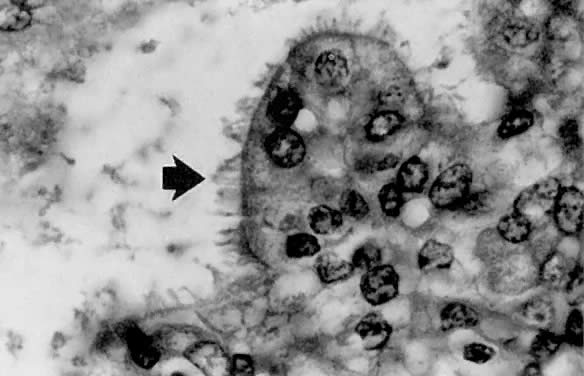
The ciliated cell variant of endometrial carcinoma is exceedingly rare, with only a few reported cases in the literature. Although most endometrial lesions with ciliated cells represent metaplasia, it is important to be cognizant of this subtype, which meets the architectural criteria for carcinoma, usually in the form of cribriforming. Ciliated cell carcinoma is well differentiated and consists of glands lined predominately by ciliated cells with abundant eosinophilic cytoplasm (Fig. 7). There is usually minimal nuclear atypia, with mildly irregular nuclear contours and prominent nucleoli. Association with exogenous estrogen use is typical,36 correlating with the observation that normal endometrium forms cilia with estrogen stimulation. Thus far, no reports of recurrence or death due to disease have been described.
{kind=link}
Endometrioid Adenocarcinoma With Squamous Differentiation
Squamous differentiation in endometrial carcinoma (Fig. 8) is a frequent finding, noted in about 25% of cases.37,38,39,40,41 To be classified as such, 5% or greater of the carcinoma must exhibit one or more of the following patterns: keratin pearl formation, defined intercellular bridges, or morules consisting of ovoid or spindled (glassy) cells.8,37 Although the occurrence of squamous differentiation in endometrial carcinoma is well accepted, its significance has proven to be quite controversial. Until recently, most have divided endometrial carcinomas with squamous differentiation into two categories. Adenoacanthoma38,39,40 was a term previously used to describe lesions that had a benign squamous component accompanying the invasive adenocarcinoma. Adenosquamous carcinoma was reserved for adenocarcinomas that also had obvious malignant squamous features. Silverberg38 defined criteria for distinguishing between adenoacanthoma and adenocarcinoma, proposing that the presence of malignant squamous elements imparts a worse prognosis. However, the current terminology used by the GOG is adenocarcinoma with squamous differentiation, making no distinction as to the degree of differentiation of the squamous component.
{kind=link}
A study by Zaino and associates37 based on 600 women with stage 1 or 2 disease addressed this issue. They found that histologic grade and depth of myometrial invasion more accurately predicted which patients were at risk for developing nodal metastases than did designating tumors as adenoacanthoma or adenosquamous carcinoma. There was no statistically significant difference in the occurrence of lymph node metastasis between the two types. Another important finding confirmed by this study was that the differentiation of the squamous component parallels the degree of glandular differentiation in the vast majority of cases. In other words, frank malignant features present within the squamous component are observed in high-grade adenocarcinomas24,37 as determined by the glandular portion. Therefore, the observation that “adenosquamous carcinomas” had a worse prognosis was essentially correct. Although the biologic behavior of adenocarcinomas with squamous differentiation is similar to that of adenocarcinomas lacking this component, the presence of squamous elements is associated with an increased probability of survival.37,41
Mucinous Carcinoma
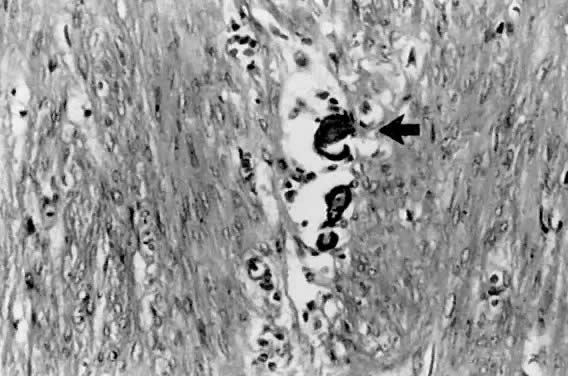
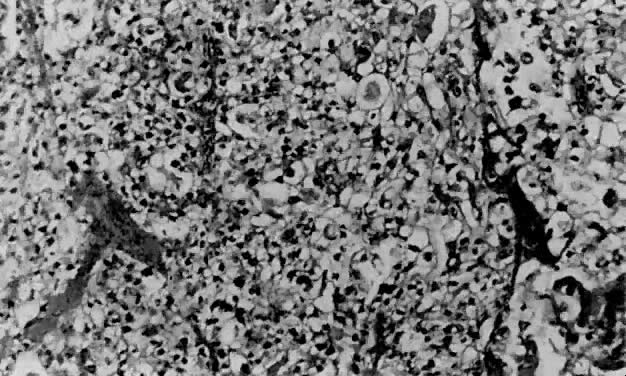
Mucinous carcinoma is typically of low grade and is the least common type of endometrial adenocarcinoma. Intracytoplasmic mucin must be present for a neoplasm to be placed in this category.8 Although polypoid lesions are more commonly identified in this type of carcinoma,42 other macroscopic features are similar to typical endometrial carcinoma. Histologically, the neoplastic glands, often forming papillary structures, are lined by mucin-secreting columnar cells resembling either endocervical (Fig. 9) or gastrointestinal epithelium. Often present are cystically dilated glands with abundant intraluminal mucin. The nuclei generally demonstrate only mild atypia, and mitoses are uncommon.
{kind=link}
On rare occasions, one encounters an endometrial lesion that appears histologically similar to microglandular hyperplasia of the cervix.43,44 This distinctive pattern consists of small glands (microcysts) lined by flattened cuboidal cells with mild nuclear atypia. Groups of polygonal cells with eosinophilic cytoplasm are present between the glands. Abundant amounts of inflammation in the form of neutrophils are present within the luminal spaces and among the epithelial cells. When this pattern is observed, it is important to exclude microglandular hyperplasia of the cervix, especially if the diagnosis is made on a curettage specimen.
AGGRESSIVE TYPES OF ENDOMETRIAL CARCINOMA
Aggressive types of endometrial carcinoma recognized by ISGYP account for less than 20% of overall cases but constitute a high proportion of nonsurvivors at 5 years.1,20,21,41 The variants include serous, clear cell, squamous, and undifferentiated carcinoma.
Serous Carcinoma
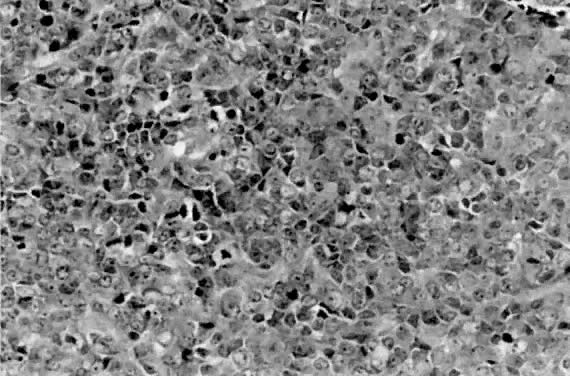
Serous carcinoma is a relatively uncommon type of endometrial carcinoma, accounting for about 5% to 10% of cases. This is an especially aggressive variant, with patients often presenting with stage II or III disease, deep myometrial invasion (40% to 50%), and frequent vascular invasion.21 The mean patient age is 70 years,45 somewhat older than for patients with endometrioid carcinoma. It occurs disproportionately in African-American women. Whereas about 53% of patients with endometrioid carcinoma have a history of exogenous estrogen use, only 21% of patients with serous carcinoma have such an association.21 Nulliparity is not a common epidemiologic factor in serous carcinoma. These tumors have a predilection for peritoneal spread, similar to primary ovarian serous adenocarcinoma.24 A papillary configuration is frequently present histologically (Fig. 10), but these lesions may grow in a solid or acinar pattern. For this reason, this variant should be referred to as serous carcinoma rather than papillary serous carcinoma. Papillae, when present, have fibrovascular cores that are lined by pleomorphic, hyperchromatic nuclei with eosinophilic macronucleoli (nuclear grade 3). Not infrequently, large, bizarre nuclei, often multinucleated, are observed. Cellular stratification and tufting or budding are frequently found (Fig. 11). The surface of the papillae are irregular and jagged, unlike the smooth surface of the villoglandular variant of endometrioid carcinoma. The solid or acinar patterns show cellular features as described above. Psammoma bodies (Fig. 12) are seen in about a third of cases. Due to the usually high nuclear grade, advanced stage of disease, deep myometrial invasion, and vascular space invasion, patients tend to have a poor prognosis, with a 25% to 35% 5-year survival rate45,46,47 and a 14% 10-year survival rate.47 Lung and liver are the most common sites of metastasis48 in advanced-stage serous carcinoma of the endometrium.
{kind=link}
{kind=link}
{kind=link}
Clear Cell Carcinoma
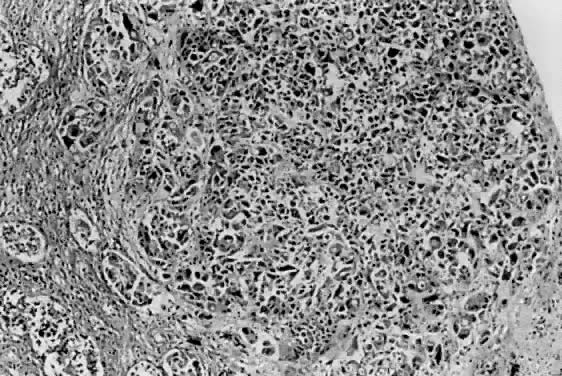
Clear cell carcinoma accounts for about 1% to 5% of endometrial carcinomas in most reports. It is associated with a poor prognosis (5-year survival rate of about 35%)20,46 and occurs almost exclusively in postmenopausal women. Although there are no distinctive macroscopic features, there are four histologic growth patterns that may aid in the diagnosis. These patterns are, in decreasing frequency, papillary (Fig. 13), tubulocystic, glandular, and solid (Fig. 14). Clear cell, hobnail, and cuboidal are the three cell types one may encounter. Most neoplasms display two or more patterns, as well as a mixture of cell types. Because of abundant glycogen accumulation, the cytoplasm of the neoplastic cells usually appears clear histologically, although it may be eosinophilic. The nuclear changes are also distinct, with irregular nuclear outlines and chromatin clumping, especially along the nuclear envelope.49 Nucleoli often are large and may be multiple. The nuclei of hobnail cells protrude into cystic spaces in the papillary variant (see Fig. 13). FIGO grading is restricted to nuclear grade in clear cell carcinoma (which is almost exclusively grade 3).22 In addition to the high nuclear grade, these patients tend to present with high-stage disease, thus contributing to their poor prognosis.
{kind=link}
{kind=link}
Squamous Cell Carcinoma
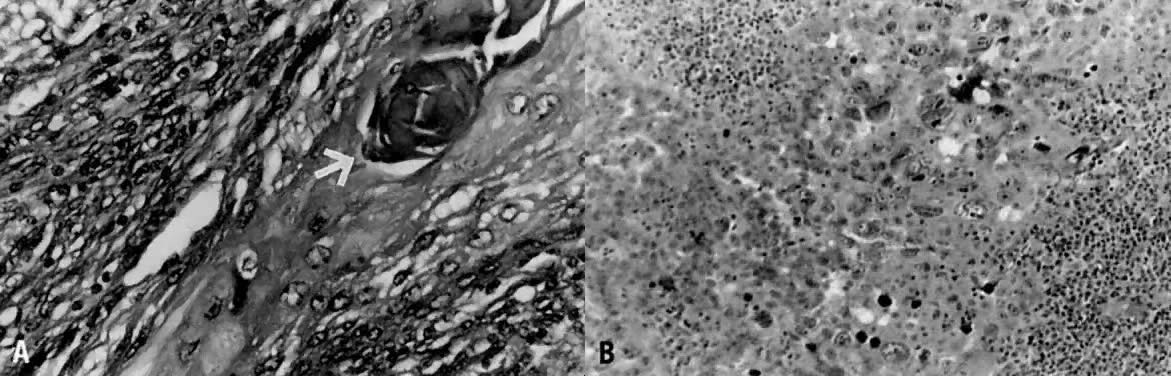
About 30 cases of primary squamous cell carcinoma (SCC) of the endometrium have been described.50,51,52 Tumors classified as pure SCC must fail to show involvement of the cervix. By convention, SCC involving both the cervix and the endometrium is considered a cervical primary. An additional requirement for categorization of pure SCC of the endometrium is an absence of adenocarcinoma of the endometrium. If present, the squamous component is then considered extensive squamous differentiation within an endometrial carcinoma. Varying degrees of differentiation of the SCC can be seen. Identifying features of SCC include intercellular bridges and keratinization (Fig. 15). Primary SCC of the endometrium is associated with a grim prognosis,50 with deep myometrial invasion and extrauterine extension common. Five-year survival is about 36%.
{kind=link}
Verrucous carcinoma of the endometrium has also been described.51,53 Criteria for classification are similar to those of pure SCC. These lesions are exophytic and microscopically consist of papillary projections lacking fibrovascular cores. The deep margin has a pushing broad-based front. Superficial myometrial invasion may be observed. Similar to verrucous carcinomas in other locations, it usually has a good prognosis.
Undifferentiated Carcinoma
Tumors lacking definitive glandular or squamous differentiation are termed undifferentiated carcinomas. This group is often divided into large and small cell categories.54 Small cell carcinomas range histologically from diffuse sheets of poorly differentiated cells (Fig. 16), similar to small cell carcinomas of other locations, to patterns simulating carcinoid tumors.55 Reactivity with neuroendocrine antibodies is not uncommon in the small cell group.54,56 Also described in the literature are undifferentiated carcinomas with multinucleated giant cells,57 occasionally resembling osteoclast-like giant cells. The prognosis is comparable to a grade 3 endometrial carcinoma, regardless of small or large cell morphology.
{kind=link}
MIXED CARCINOMA
Mixed carcinomas of the endometrium, by definition, contain more than one cell type. The second cell type must account for at least 10% of the tumor volume. The prognosis is most likely related to the highest-grade component; however, long-term studies have not been performed to confirm the behavior of these lesions.
METAPLASIA
Numerous types of metaplasias, defined as replacement of endometrial glandular epithelium by epithelium not normally found in the endometrium, are recognized. These include tubal (Fig. 17), squamous, mucinous, ciliated cell, eosinophilic, surface syncytial, papillary (Fig. 18), and clear cell.58,59 Metaplasias often occur in women receiving exogenous estrogens.58,60 The importance of recognizing metaplasias lies not only in differentiating this group of benign epithelial changes from carcinoma but also in appreciating that they often accompany carcinoma58,60 and hyperplasia.
{kind=link}
{kind=link}
MYOMETRIAL INVASION
Depth of myometrial invasion has proven to be an independent predictor of outcome in early-stage endometrial carcinoma.61,62,63,64,65 Increasing depth of myometrial invasion is associated with a greater probability of nodal metastasis and death from tumor,2,3,37,38,64,66 even when adjusted for histologic grade and subtype. It is common practice in the United States to report depth of myometrial invasion by thirds (inner third, middle third, and outer third of myometrial thickness), even though FIGO divides depth of invasion into halves. Ideally, the total width of the myometrium should be measured and reported in addition to the measurement of the thickness of tumor invasion. With these two measurements, the clinician can proceed with the division of his or her choice.
Determining the depth of myometrial invasion by endometrial carcinoma may be complicated when foci of adenomyosis are involved. Adenocarcinoma present in adenomyosis does not represent true myometrial invasion and does not correlate with a worse prognosis.61 Recognizing well-demarcated rounded areas deep within the myometrium with associated benign endometrial glands or stroma and without extension to the neoplasm involving the surface is important in separating adenomyosis from invasive carcinoma. Adenocarcinoma arising within a focus of adenomyosis without synchronous surface involvement is rare.62,63 Not infrequently, adenocarcinomas arise in hyperplastic endometrial polyps. If limited to the polyp without stalk invasion, the prognosis is excellent.
CERVICAL EXTENSION
Involvement of the cervix has adverse effects on prognosis. One study compared women treated with radiotherapy, hysterectomy, and bilateral salpingo-oophorectomy who had gross cervical disease with women who received identical therapy but lacked apparent involvement of the cervix.67 The authors found that women without gross cervical extension had a median survival time three times that of women with cervical involvement. Deep myometrial invasion often coexists with cervical involvement by endometrial adenocarcinoma.68
VASCULAR SPACE INVASION
Because vascular invasion is an important predictor of recurrence,69,70,71,72 its presence should always be stated in the pathology report. The incidence of vascular space invasion is higher in serous and clear cell types, but it may be present in any cell type. When observed, the risk of metastasis to pelvic and para-aortic lymph nodes increases significantly.25,71 Vascular space invasion, in conjunction with depth of myometrial invasion, appears to be a good predictor of survival in stage I endometrioid endometrial adenocarcinoma.25,26 In one report, the survival rate for patients whose tumor showed both deep myometrial invasion and vascular space invasion was 35%, compared to 95% in those lacking these two features.25
SYNCHRONOUS ENDOMETRIAL AND OVARIAN CARCINOMAS
Not uncommonly, one encounters simultaneously occurring endometrial and ovarian tumors, usually of endometrioid cell type. Although it may be diagnostically challenging to discern if these represent an endometrial carcinoma metastatic to the ovary, an ovarian carcinoma metastatic to the endometrium, or true synchronous tumors, there are significant implications in regard to therapy and prognosis. Synchronous lesions are favored when the endometrial carcinoma is minimally invasive and small.73 An endometrial primary with metastasis to the ovary is most likely when the ovarian tumors are multiple and less than 5 cm in greatest dimension, and when deep myometrial invasion and vascular invasion are present. Although metastasis to the ovary from an endometrial primary occurs with some frequency, ovarian neoplasms only rarely metastasize to the endometrium.74 A recent investigation of loss of heterozygosity, examined through the polymerase chain reaction technique, suggested that a higher rate of loss of heterozygosity was detected in patients with synchronous lesions than in patients with single tumors.75,76,77,78 Obviously, additional studies are necessary to confirm this information, but the findings are intriguing and an example of how molecular diagnostics may provide useful information.
METASTATIC LESIONS TO THE ENDOMETRIUM
Metastatic lesions involving the endometrium are uncommon. Direct extension from cervical or fallopian tube primaries account for the majority. Extragenital primaries are exceedingly infrequent75,77 and occur only in disseminated disease.76 The most common primary sites are breast (Fig. 19), stomach, melanoma, and colon.
{kind=link}
ANCILLARY STUDIES
Provocative studies investigating hormone receptor status and genetic alterations in endometrial carcinoma have been reported recently. In time, application of this information will be directed toward patient therapy; however, currently these ancillary studies should be limited to accumulating data rather than influencing patient care.79
Estrogen and Progesterone Receptor Status
Expression of estrogen receptors (ER) and progesterone receptors (PR) is found in most endometrial carcinomas, but in amounts lower than can be identified in normal cycling endometrium.80,81,82,83,84,85 Although neither ER nor PR expression correlates with stage, myometrial invasion, or lymph node metastasis, many recent reports suggest that expression of PR correlates with low tumor grade, low recurrence rate, and higher survival.84,86,87 Conversely, the absence of PR is associated with a worse prognosis.80 In patients with disease clinically confined to the uterus, the 5-year survival is 86% with ER-positive and PR-positive tumors and only 52% in ER-positive and PR-negative tumors.83,84 Therefore, PR status may be relevant in predicting prognosis as well as consideration of therapy with progestational agents in PR-positive tumors. High-grade tumors such as serous and clear cell carcinoma tend to be negative, with antibodies directed toward ER and PR.80,81,82 Although a number of studies have provided encouraging data, additional long-term studies are required to establish definitive predictive and therapeutic value.
HER-2/neu
HER-2/neu oncogene encodes a cell surface protein that has characteristics similar to the human growth factor receptor. Some studies have observed overexpression of this oncogene in endometrial carcinomas, correlating inversely with survival26,88 and occurring more frequently in patients with advanced stages (metastatic disease).89 Studies investigating C-myc, H-ras, N-ras, and other oncogenes have not demonstrated convincing evidence of significant overexpression in endometrial carcinoma.90,91
p53
p53 is a suppressor gene that is commonly altered in numerous types of human cancer. Mutations of p53 have been identified in endometrial carcinoma and hyperplasia. Inactivation of this suppressor gene occurs at a much more frequent rate in high-grade and high-stage endometrial cancers such as serous carcinoma than in well-differentiated carcinomas and hyperplasia.92,93,94
DNA Ploidy
Additional information does not seem to be added using DNA ploidy and nuclear morphometry. Because clinical grading and morphometry parallel one another, the estimation of grade by pathologists during the routine microscopic examination seems adequate. Aneuploidy correlates positively with deep myometrial invasion95 and metastatic disease.96 If the pathologic and surgical findings are inconclusive in regard to predicting degree of risk (such as a grade 2 lesion), then the DNA ploidy may be useful data. One study found that aneuploid grade 2 endometrial adenocarcinomas were twice as likely to metastasize as diploid grade 2 lesions.97 Most reports suggest a lower survival rate in patients with aneuploid tumors; however, results have been inconsistent, due in part to differences in methodology and preparation.98
REFERENCES
Hendrickson MR, Ross JC, Kempson RL: Toward the development of morphologic criteria for well differentiated adenocarcinoma of the endometrium. Am J Surg Pathol 7: 819– 838, 1983 |
|
Glassburn JR: Carcinoma of the endometrium. Cancer 48: 575– 581, 1981 |
|
Creasman WT, Morrow CP, Bundy BN et al: Surgical pathologic spread patterns of endometrial cancer: A Gynecologic Oncology Group study. Cancer 60: 2035– 2041, 1987 |
|
Norris HI, Tavassoli FA, Kurman RJ: Endometrial hyperplasia and carcinoma: Diagnostic considerations. Am J Surg Pathol 7: 839– 847, 1983 |
|
Gambrell RD, Bagnell CA, Greenblatt RB: Role of estrogens and progesterone in the etiology and prevention of endometrial cancer [Review]. Am J Obstet Gynecol 146: 696– 707, 1983 |
|
Davies JL, Rosenshein NB, Antunes CMF, Stolley PD: A review of the risk factors for endometrial cancer. Obstet Gynecol Surv 36: 107– 116, 1981 |
|
Schenker JG, Weinstein D, Okon E: Estradiol and testosterone levels in the peripheral and ovarian circulation in patients with endometrial cancer. Cancer 44: 1809– 1812, 1979 |
|
Sidaway MK, Silverberg SG: Endometrial carcinoma: Pathologic factors of therapeutic and prognostic significance. Pathol Ann 27: 153– 185, 1992 |
|
Gusberg SB: Current concepts in cancer: The changing nature of endometrial cancer. N Engl J Med 302: 729– 731, 1980 |
|
Smith M, McCartney J: Occult high-risk endometrial cancer. Gynecol Oncol 22: 154– 161, 1985 |
|
Baron JA, LaVecchia C, Levi F: The antiestrogenic effect of cigarette smoking in women. Am J Obstet Gynecol 162: 502– 514, 1990 |
|
Brinton LA, Hoover RN: The endometrial cancer collaborative group: Estrogen replacement therapy and endometrial cancer risk: Unresolved issues. Obstet Gynecol 81: 265– 271, 1993 |
|
Brinton LA, Barrett RJ, Berman ML et al: Cigarette smoking and the risk of endometrial cancer. Am J Epidermol 137: 281– 291, 1993 |
|
Koss LG, Scheiber K, Oberlander S et al: Detection of endometrial carcinoma and hyperplasia in asymptomatic women. Obstet Gynecol 64: 1– 11, 1984 |
|
Deligdisch L, Cohen CJ: Histologic correlates and virulence implications of endometrial carcinoma associated with adenomatous hyperplasia. Cancer 56: 1452– 1455, 1985 |
|
Beckner ME, Mori T, Silverberg SG: Endometrial carcinoma: Nontumor factors in prognosis. Int J Gynecol Pathol 4: 131– 145, 1985 |
|
Robboy SJ, Bradley R: Changing trends and prognostic features in endometrial cancer associated with exogenous estrogen therapy. Obstet Gynecol 54: 269– 277, 1979 |
|
Kurman RJ, Kaminski PR, Norris HJ: The behavior of endometrial hyperplasia: A long-term study of “untreated” hyperplasia in 170 patients. Cancer 56: 403– 412, 1985 |
|
Bokman JV: Two pathogenetic types of endometrial carcinoma. Gynecol Oncol 15: 10– 17, 1983 |
|
Christopherson WM, Alberhasky RC, Connelly PJ: Carcinoma of the endometrium: I. A clinicopathologic study of clear cell carcinoma and secretory carcinoma. Cancer 49: 1511– 1523, 1982 |
|
Hendrickson M, Ross J, Eifel P et al: Uterine papillary serous carcinoma: A highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol 6: 93– 108, 1982 |
|
FIGO stages—1988 revision. Gynecol Oncol 35:125–126, 1989 |
|
Kurman RJ, Norris HJ: Evaluation of criteria for distinguishing atypical endometrial hyperplasia from well-differentiated carcinoma. Cancer 49: 2547– 2559, 1982 |
|
Fanning J, Evans MC, Peters AJ et al: Endometrial adenocarcinoma histologic subtypes: Clinical and pathologic profiles. Gynecol Oncol 32: 288– 291, 1989 |
|
Ambros RA, Kurman RJ: Combined assessment of vascular and myometrial invasion as a model to predict prognosis in stage I endometrial adenocarcinoma of the uterine corpus. Cancer 9: 1424– 1430, 1992 |
|
Hernandez E: Pathological findings and prognosis from uterine malignancy. Curr Opinion Obstet Gynecol 5: 480– 485, 1993 |
|
Parkash V, Carcangui ML: Endometrioid endometrial adenocarcinoma with psammoma bodies. Am J Surg Pathol 21: 399– 406, 1997 |
|
Factor SM: Papillary adenocarcinoma of the endometrium with psammoma bodies. Arch Pathol 98: 201– 205, 1974 |
|
Chen J, Trost DC, Wilkinson EG: Endometrial papillary adenocarcinomas: Two clinicopathologic types. Int J Gynecol Pathol 4: 279, 1985 |
|
Dawagne MP, Silverberg SG: Foam cells in endometrial carcinoma: A clinicopathologic study. Gynecol Oncol 13: 67– 75, 1982 |
|
Silverberg SG: Hyperplasia and carcinoma of the endometrium: Differential diagnosis and other relationships. International Society of Gynecological Pathologists Conference, USCAP Meeting, New Orleans, 1993 |
|
Spiegel GW: Endometrial carcinoma in situ in postmenopausal women. Am J Surg Pathol 19: 417– 432, 1995 |
|
Ambros RA, Sherman ME, Zahn CM et al: Endometrial intraepithelial carcinoma: A distinctive lesion specifically associated with tumors displaying serous differentiation. Hum Pathol 26: 417– 432, 1996 |
|
Nielsen AK, Thomsen HK, Nyholm HC: Evaluation of the reproducibility of the revised 1988 International Federation of Gynecology and Obstetrics grading system of endometrial cancers with special emphasis on nuclear grading. Cancer 68: 2303– 2309, 1991 |
|
Tobon H, Watkins GJ: Secretory adenocarcinoma of the endometrium. Int J Gynecol Pathol 4: 328– 335, 1985 |
|
Hendrickson MR, Kempson R: Ciliated carcinoma: A variant of endometrial carcinoma: A report of 10 cases. Int J Gynecol Pathol 2: 1– 12, 1983 |
|
Zaino RJ, Kurman R, Herbold D et al: The significance of squamous differentiation in endometrial carcinoma: Data from a Gynecologic Oncology Group study. Cancer 68: 2293– 2302, 1991 |
|
Silverberg SG: New aspects of endometrial carcinoma. Clin Obstet Gynecol 11: 189– 208, 1984 |
|
Crum CP, Richart RM, Fenoglio CM: Adenoacanthosis of the endometrium: A clinicopathologic study of premenopausal women. Am J Surg Pathol 5: 15– 20, 1981 |
|
Silverberg SG: Significance of squamous elements in carcinoma of the endometrium: A review. Prog Surg Pathol 4: 115– 136, 1981 |
|
Connelly PJ, Alberhasky RC, Christopherson WM: Carcinoma of the endometrium III: Analysis of 865 cases of adenocarcinoma and adenoacanthoma. Obstet Gynecol 59: 569– 574, 1982 |
|
Melham MF, Tobon H: Mucinous adenocarcinoma of the endometrium. A clinicopathologic review of 18 cases. Int J Gynecol Pathol 6: 347– 355, 1987 |
|
Young RH, Scully RE: Uterine carcinomas simulating microglandular hyperplasia. Am J Surg Pathol 16: 1092– 1097, 1992 |
|
Zaloudek C, Hayashi GM, Ryan IP et al: Microglandular adenocarcinoma of the endometrium: A form of mucinous adenocarcinoma that may be confused with microglandular hyperplasia of the cervix. Int J Gynecol Pathol 16: 52– 59, 1997 |
|
Jeffrey JF, Krepart GV, Lotocki RJ: Papillary serous adenocarcinoma of the endometrium. Obstet Gynecol 67: 670– 674, 1986 |
|
Christopherson WM, Alberhasky RC, Connelly PJ: Carcinoma of the endometrium: II. Papillary adenocarcinoma: A clinical pathological study of 46 cases. Am J Clin Pathol 77: 534– 540, 1982 |
|
Abeler VM, Kjorstad KE: Serous papillary carcinoma of the endometrium: A histopathological study of 22 cases. Gynecol Oncol 39: 266– 271, 1990 |
|
Gallion HH, Van Nagell JR, Powell DF et al: Stage I serous papillary carcinoma of the endometrium. Cancer 63: 2224– 2228, 1989 |
|
Kanbour-Shakir A, Tobon H: Primary clear cell carcinoma of the endometrium: A clinicopathologic study of 20 cases. Int J Gynecol Pathol 10: 67– 78, 1991 |
|
Simon A, Kopolvic J, Beyth Y: Primary squamous cell carcinoma of the endometrium. Gynecol Oncol 31: 454– 461, 1988 |
|
Hussain SF: Verrucous carcinoma of the endometrium: A case report. APMIS 96: 1075– 1078, 1988 |
|
Pritzker J, Anselmo MT, Veridiano NP, Tancer ML: Squamous cell carcinoma of the endometrium: A case report. J Reprod Med 37: 194– 198, 1992 |
|
Ryder DE: Verrucous carcinoma of the endometrium: A unique neoplasm with long survival. Obstet Gynecol 59: 78S– 80S, 1982 |
|
Abeler VM, Kjorstad KE, Nesland JM: Undifferentiated carcinoma of the endometrium. Cancer 68: 98– 105, 1991 |
|
Huntsman DG, Clement PB, Gilks CB, Scully RE: Small cell carcinoma of the endometrium: A clinicopathologic study of 16 cases. Am J Surg Pathol 18: 364, 1994 |
|
van Hoeven KH, Hudock JA, Woodruff JM, Suhrland MJ: Small cell neuroendocrine carcinoma of the endometrium. Int J Gynecol Pathol 14: 21, 1995 |
|
Jones MA, Young RH, Scully RE: Endometrial adenocarcinoma with a component of giant cell carcinoma. Int J Gynecol Pathol 10: 260– 270, 1991 |
|
Hendickson MR, Kempson RL: Endometrial epithelial metaplasias: Proliferations frequently misdiagnosed as adenocarcinoma. Am J Surg Pathol 4: 525– 542, 1980 |
|
Winkler BA, Alvarez S, Richart RM et al: Pitfalls in the diagnosis of endometrial neoplasia. Obstet Gynecol 64: 185– 194, 1984 |
|
Anderson WA, Taylor PT, Fechner RE: Endometrial metaplasia associated with endometrial adenocarcinoma. Am J Obstet Gynecol 154: 597– 604, 1987 |
|
Hall JB, Young RH, Nelson JH: The prognostic significance of adenomyosis in endometrial carcinoma. Gynecol Oncol 17: 32– 40, 1984 |
|
Coleman HI, Rosenthal AH: Carcinoma developing in areas of adenomyosis. Obstet Gynecol 14: 342– 348, 1959 |
|
Hernandez E, Woodruff JD: Adenocarcinoma in adenomyosis. Am J Obstet Gynecol 138: 829– 832, 1980 |
|
Kadar N, Malfetano JH, Homesley HD: Determinants of survival of surgically staged patients with endometrial cancer histologically confined to the uterus: Implications for therapy. Obstet Gynecol 80: 655– 659, 1992 |
|
Morrow CP, Bundy BN, Kurman RJ et al: Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: A Gynecologic Oncology Group study. Gynecol Oncol 40: 55– 65, 1991 |
|
Abeler VM, Kjorstad KE, Berle E: Carcinoma of the endometrium in Norway: A histopathological and prognostic survey of a total population. Int J Gynecol Oncol 2: 9– 22, 1992 |
|
Podczaski ES, Kaminski P, Manetta A et al: Stage II endometrial carcinoma treated with external beam radiotherapy, intracavitary application of cesium and surgery. Gynecol Oncol 35: 251– 254, 1989 |
|
Trimble EWL, Jones HW: Management of stage II endometrial adenocarcinoma. Obstet Gynecol 71: 323– 326, 1988 |
|
Hanson MB, vanNagell JR, Powell DE et al: The prognostic significance of lymph-vascular space invasion in stage I endometrial carcinoma. Cancer 55: 1753, 1985 |
|
Alders JG, Abeler V, Kolstad P: Recurrent carcinoma of the endometrium. A clinical and pathological study of 379 patients. Gynecol Oncol 17: 85, 1982 |
|
Ambros RA, Kurman RJ: Identification of patients with stage I uterine endometrioid adenocarcinoma at high risk of recurrence by DNA ploidy, myometrial invasion and vascular invasion. Gynecol Oncol 45: 235– 239, 1992 |
|
Zaino RJ, Kurman RJ, Diana KL, Morrow P: Pathologic models to predict outcome for women with endometrial adenocarcinoma: The importance of the distinction of surgical stage from clinical stage. Cancer 77: 1115– 1121, 1996 |
|
Eifel P, Hendrickson M, Ross J et al: Simultaneous presentation of carcinoma involving the ovary and uterine corpus. Cancer 50: 163, 1982 |
|
Ulbright TM, Roth LM: Metastatic and independent cancers of the endometrium and ovary: A clinicopathologic study of 34 cases. Hum Pathol 16: 28– 34, 1985 |
|
Kumar NB, Hart WR: Metastasis to the uterine corpus from extragenital cancers: A clinicopathologic study of 63 cases. Cancer 50: 2163– 2169, 1982 |
|
Kumar A, Schneider V: Metastases to the uterus from extrapelvic primary tumors. Int J Gynecol Pathol 2: 134, 1983 |
|
Jordan CD, Andrews SJ, Memoli VA: Well-differentiated pulmonary neuroendocrine carcinoma metastatic to the endometrium: A case report. Mod Pathol 9 (11): 1066– 1070, 1996 |
|
Emmert-Buck MR, Chuaqui R, Zhuang Z et al: Molecular analysis of synchronous uterine and ovarian endometrioid tumors. Int J Gynecol Oncol 16: 143– 151, 1997 |
|
Sasano H, Watanabe K, Ito K et al: New concepts in the diagnosis and prognosis of endometrial carcinoma. Pathol Ann 2: 31– 49, 1994 |
|
Liao BS, Twiggs LB, Leung BS et al: Cytoplasmic estrogen and progesterone receptors as prognostic parameters in primary endometrial carcinoma. Obstet Gynecol 67: 463– 467, 1986 |
|
Soper JT, Segreti EM, Novotny DB et al: Estrogen and progesterone receptor content of endometrial carcinomas: Comparison of total tissue versus cancer component analysis. Gynecol Oncol 36: 363– 368, 1990 |
|
Yorishima M, Hirra M, Moriwaki S et al: Clear cell carcinoma of the endometrium with lipid-producing activity. Int J Gynecol Oncol 8: 286– 295, 1989 |
|
Creasman WT: Prognostic significance of hormone receptors in endometrial cancer. Cancer 71: 1467– 1470, 1993 |
|
Kleine W, Maier T, Geyer H, Pfleiderer A: Estrogen and progesterone receptors in endometrial cancer and their prognostic relevance. Gynecol Oncol 38: 59– 65, 1990 |
|
Janne O, Kauppila K, Syrjala P, Vihko R: Female sex steroid receptors in normal, hyperplastic and carcinomatous endometrium: The relationship to serum steroid hormones and gonadotropins and changes during medroxyprogesterone acetate administration. Int J Cancer 24: 545– 554, 1979 |
|
Creasman WT, Soper JT, McCarty KS Jr et al:Influence of cytoplasmic steroid receptor content on prognosis of early-stage endometrial carcinoma. Am J Obstet Gynecol 151: 922, 1985 |
|
Ehrlich CE, Young PCM, Stehman FB et al: Steroid receptors and clinical outcome in patients with adenocarcinoma of the endometrium. Am J Obstet Gynecol 158: 796– 807, 1988 |
|
Hertel DJ, Wilson TD, Keeney GL et al: HER-2/neu expression: A major prognostic factor in endometrial cancer. Gynecol Oncol 45: 179– 185, 1992 |
|
Berchuck A, Rodrigues G, Kinney RB et al: Overexpression of HER-2/neu in endometrial cancer is associated with advanced-stage disease. Am J Obstet Gynecol 164: 15– 21, 1991 |
|
Fujimoto I, Shimizu Y, Hirai Y et al: Studies on ras oncogene in endometrial carcinoma. Gynecol Oncol 48: 196– 202, 1993 |
|
Ignar-Trowbridge D, Risinger J, Dent G et al: Mutations of the Ki-ras oncogene in endometrial carcinoma. Am J Obstet Gynecol 167: 227– 232, 1992 |
|
Kohler MF, Berchuck A, Davidoff AM et al: Overexpression and mutation of p53 in endometrial carcinoma. Cancer Res 52: 1622– 1627, 1992 |
|
Bur ME, Perlman C, Edelmann L et al: p53 expression in neoplasms of the uterine corpus. Am J Clin Pathol 98: 81– 87, 1992 |
|
Taskin M, Lallas TA, Barber HRK, Shevchuk MM: bcl-2 and p53 in endometrial adenocarcinoma. Mod Pathol 10: 728– 734, 1997 |
|
Christopherson WM, Connelly PJ, Alberhasky RC: Carcinoma of the endometrium V. An analysis of prognosticators in patients with favorable subtype and stage I disease. Cancer 51: 1705– 1709, 1983 |
|
Prodratz KC, Wilson TO, Gaffey TA et al: Deoxyribonucleic acid analysis facilitates the pretreatment identification of high-risk endometrial cancer patients. Am J Obstet Gynecol 168: 1206– 1215, 1993 |
|
Symonds DA: Prognostic value of pathologic features and DNA analysis in endometrial carcinoma. Gynecol Oncol 39: 272– 276, 1990 |
|
Homesley HD, Zaino RJ: Endometrial cancer: Prognostic factors. Sem Oncol 21: 71– 88, 1994 |