Endometrial Ablation
Authors
INTRODUCTION
Endometrial ablation has been classically used for treatment of proven menorrhagia. However, a recent ACOG Practice Bulletin has added patient-perceived heavy menstrual bleeding as an added indication.1 Although endometrial ablation is a relatively safe procedure, it is nevertheless not without risk and should be reserved for patients who fail or do not tolerate medical therapy. This procedure has been studied primarily in patients with dysfunctional uterine bleeding. Although some surgeons have used endometrial ablation to treat postmenopausal bleeding resulting from hormone replacement, this approach remains controversial because of the fear of missed endometrial carcinoma. Dysmenorrhea primarily associated with the passage of clots from excessive bleeding can also be treated effectively by endometrial ablation. Other types of pelvic pain and dyspareunia do not usually respond to endometrial ablation.
The size of the endometrial cavity significantly affects the success rate. A uterus larger than 12 gestational weeks or a cavity bigger than 12 cm has been shown to reduce success.2, 3 However, patients with small intramural fibroids that do not result in enlargement of the endometrial cavity may be reasonable candidates for ablation. Likewise, the presence of pedunculated serosal fibroids that do not impinge on, or affect the size of, the endometrial cavity probably does not adversely affect the success of endometrial ablation. Since resectoscopic methods allow treatment of an irregular or enlarged cavity, these methods may be more successful in patients with enlarged uteri than other methods. At least one study has shown that, in experienced hands, success rates in women with uterine size greater than 12 weeks was equivalent to that of women with smaller uteri.4 Deep adenomyosis has also been associated with poor success rates after endometrial ablation.
The use of ultrasound to evaluate the presence and location of fibroids should be considered in those patients noted on pelvic examination to have an enlarged uteri. Even in women with apparently normal sized uterus, consideration should be given to assessing the uterine cavity by some reliable means in all patients before endometrial ablation. This may be accomplished with ultrasound, sonohysterogram or by office hysteroscopy.
Malignant or premalignant disease of the uterus must be ruled out before endometrial ablation. This may be accomplished by office endometrial biopsy or by hysteroscopically directed biopsy. The presence of endometrial hyperplasia at the time of ablation has been associated with the subsequent development of endometrial carcinoma.5 Thus, endometrial hyperplasia is considered a contraindication to endometrial ablation. Cervical cytology should be performed to screen for cervical disease in all patients who do not have recent Papanicolaou (Pap) smears. Patients with abnormal smears should be appropriately evaluated with colposcopy before endometrial ablation.
PATIENT PREPARATION
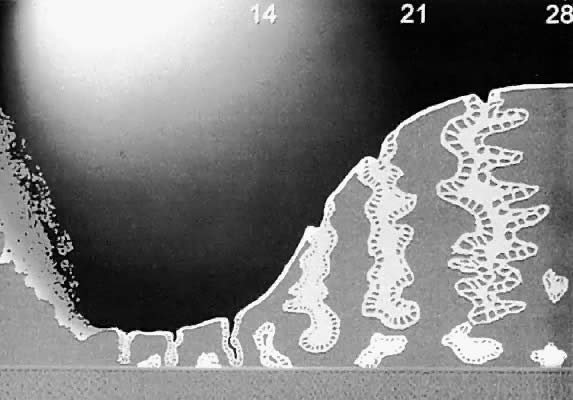
The endometrium varies in thickness from 1 mm immediately postmenstrual to more that 10 mm in the late secretory phase (Fig. 1). The Nd:YAG laser, rollerball, thermal balloon, and most other methods discussed subsequently will coagulate endometrial tissue to a depth of 3–6 mm. It is generally accepted that endometrium of less than 4 mm thickness will be effectively destroyed by all modalities used to perform endometrial ablation. Therefore, the endometrium should be prepared so that it is no thicker than 4 mm. An additional benefit to a thin atrophic endometrium is a reduction in the amount of debris produced during hysteroscopic procedures with an associated overall improvement in visibility during the procedure. An exception to this requirement may be the NovaSure device, which appears to vaporize and remove tissue and endometrial thinning may not be required. Likewise, hysteroscopic techniques which use actual tissue resection may be not as dependent on endometrial preparation.
{kind=link}
Several methods are available to produce a thin endometrium. The procedure can be performed during the immediate postmenstrual phase when the endometrium is at its thinnest. However, most surgeons prefer methods that are more likely to reliably produce an adequate thinning. A suction or mechanical curettage can be performed immediately before the endometrial ablation. Although cost-effective, this technique may produce uneven thinning. As a result, most surgeons prefer to use some form of exogenous hormones to thin the endometrium. In addition to thinning the endometrium, many hormonal methods also reduce the vascularity of the uterus and may reduce the size of the endometrial cavity.
The two most commonly used agents for endometrial preparation are danazol and gonadotropin-releasing hormone (GnRH) agonists. Danazol 800 mg given in divided doses for 4–12 weeks has been shown to produce satisfactory endometrial thinning.6 Similarly, a single injection of a depot form of GnRH agonist is sufficient to produce an atrophic endometrium within 1 month. A repeat injection 1 month later produces an even thinner endometrium but at a substantial cost for the added thinning obtained. Progestin therapy is also widely used for endometrial preparation but is thought by some to be ineffective.7
SUCCESS RATES
Success rates among the various methods of endometrial ablation are difficult to directly compare because of differences in patient selection and endometrial preparation. Definition of success also varies among different authors, with some publications reporting patient satisfaction while others reporting amenorrhea, eumenorrhea, hypomenorrhea, and failure. Currently, no one method appears to have an obvious advantage over the others. As a rough guide, short-term amenorrhea can be expected in roughly 40–50% of patients after endometrial ablation.8, 9 Eumenorrhea and hypomenorrhea occur in slightly less than 20% of patients and failure occurs in approximately 10%. Amenorrhea rates tend to decrease with length of follow-up.
Data presented to the FDA during trials of the global ablation devices showed amenorrhea rates ranging from 13.2% for the thermal balloon to a high of 55.5% for the Microwave Endometrial Ablation System.1 Baggish and coworkers, in a review of multiple series using laser ablation, rollerball ablation, and endometrial resection, found results were considered to be excellent to good in 86–94% of patients.10 Likewise, data from the FDA pivotal trials of the global ablation devices showed satisfaction rates of 86–96%.1
METHODS OF ENDOMETRIAL ABLATION
Hysteroscopic Methods
Although the mechanics of the hysteroscopic methods of endometrial ablation are discussed in this chapter, the mechanics of operative hysteroscopy are not. The reader is referred to other chapters for discussion of general hysteroscopic principles, distention media, and technique.
LASER ENDOMETRIAL ABLATION.
The Nd: YAG laser emits an invisible beam of light with a wavelength of 1064 nm. The Nd:YAG laser has three properties that make it well-suited to endometrial ablation: (1) it penetrates the endometrium to a depth of 5–6 mm, (2) it passes unabsorbed through clear liquids, and (3) it can be directed through flexible quartz fibers.
Quartz fibers of different diameters from 600 to 1200 μm have been developed for use with the Nd:YAG laser. The tissue effect with these fibers is related to the power density produced. Wider fibers have lower power densities and require a longer contact time to produce the same effect achieved with a smaller fiber at any given power. Generally, 6000-μm fibers are recommended for endometrial ablation. The flexible quartz fibers used for endometrial ablation are surrounded by a protective plastic coat. When laser energy is directed through these “bare fibers,” it penetrates the surface of the endometrium and exerts a maximal thermocoagulation in the superficial myometrium. Thus, a deep thermocoagulation is achieved (Fig. 2). This is ideal for endometrial ablation but not well suited for other applications such as intra-abdominal applications. Consequently, shaped “sapphire” ceramic tips that can focus the laser energy in various configurations, depending on the shape of the tip, have been developed to fit onto these bare quartz fibers. Although these tips reduce the depth of tissue destruction and increase the range of applications in which the Nd:YAG laser can be used, they should not be used for endometrial ablation. In endometrial ablation, deep tissue destruction is desirable to destroy the basalis layer. Any reduction in the depth of destruction potentially reduces the effectiveness of the procedure.
{kind=link}
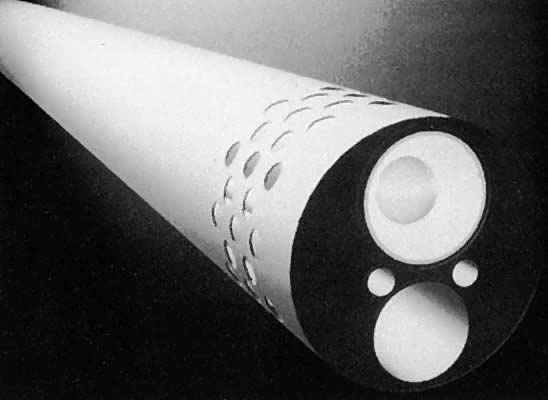
Sapphire tips by the nature of their design are subjected to very high temperatures and must be cooled by a secondary cooling system to prevent overheating. One method of cooling involves directing carbon dioxide (CO2) gas under pressure through a coaxial channel (Fig. 3). The gas exits through a small opening near the base of the sapphire tip to cool it. The combined effect of a large volume of gas under pressure instilled into the closed uterine cavity may produce a gas embolus. Several deaths from this effect have been reported.11 Therefore, the use of gas-cooled tips in the uterine cavity is absolutely contraindicated.
{kind=link}
The use of a bare quartz fiber can be used in two different ways to perform endometrial ablation. These two methods are the contact, or dragging, method and the noncontact, or blanching, method.
The contact method was the original method used by Goldrath and associates to perform the first laser endometrial ablation.12 This method involves “dragging” the bare fiber across the endometrial surface. In this technique, the fiber is kept in constant contact with the endometrial surface. The principal advantages of the dragging technique is that it is very easy to differentiate the treated areas from the untreated areas and the technique can be easily used for all areas of the uterine cavity.
In the noncontact, or blanching technique, the quartz fiber is held at right angles to, and a short distance above, the endometrial surface. This method is believed by its supporters to be less likely to interrupt underlying blood vessels, thus reducing the risk of fluid intravasation. The primary disadvantage is the difficulty in getting the fiber at the correct angle over the endometrial surface. There is also occasional difficulty in differentiating photocoagulated tissue from the pale suppressed endometrium.
Because the light produced by the Nd:YAG laser is invisible to the human eye, a helium neon (HeNe) laser is used to illuminate the distal 5 mm of the tip. Thus, the tip glows red not because it is hot but because of the light produced by the HeNe laser.
Technique of Laser Endometrial Ablation. The contact, or dragging, technique is more commonly used than the noncontact method, and a description of it follows. However, the basic principles of the technique still apply to the noncontact method.
After placement of the hysteroscope, the laser is activated at a power of 50–80 W. A power of 50 W is probably the lowest power setting that will provide adequate endometrial ablation. Higher powers are inherently more dangerous but also permit shorter treatment times and reduce the potential for fluid absorption. Powers up to 80 W are recommended by some authors.
Although several different variations in technique are available, most laser procedures start at the tubal ostium area. A series of circular parallel furrows are performed until the ostium is completely ablated. The procedure is repeated on the opposite side (Fig. 4). Then the anterior wall, the lateral walls, and finally the posterior wall are ablated.
The laser is only activated as the fiber is being pulled toward the surgeon and never as the fiber is being pushed back toward the fundus. This is a safety measure because the fiber is more likely to perforate the uterus while being advanced. If a perforation should occur while the laser is activated, serious damage can occur. The laser also should not be activated unless the glowing red tip can be seen, ensuring that the tip is within the endometrial cavity and not outside the uterus. The laser should also be fired only when the fiber is moving. Otherwise, the depth of destruction will be much greater than desired.
ELECTROSURGICAL ENDOMETRIAL ABLATION.
The development of electrosurgical methods of endometrial ablation has resulted in a decline in the use of the laser ablation techniques. Many physicians find electrosurgical methods to be easier and to require less operator skill; also the is equipment cheaper to acquire and maintain.
With laser ablation methods, the procedure is generally more prolonged, lasting 30–40 minutes compared with 20–30 minutes with electrosurgery when performed by an experienced operator. The overall reported cure rate with electrosurgical methods is slightly less than that reported with laser but the difference does not appear to be clinically significant. Unlike laser energy, electricity is conducted by electrolyte-containing fluids. Thus, nonelectrolyte fluids must be used when working with unipolar electrosurgical systems. Use of these fluids increases the likelihood of fluid overload and hyponatremia.
With the use of endometrial resection, the risk of uterine perforation is increased over that of rollerball techniques. Furthermore, resection of the superficial portion of myometrium increases the likelihood of bleeding and exposes the venous sinuses. These open sinuses increase the absorption of the irrigation fluid and increase the possibility of hyponatremia. With rollerball coagulation, vessels are coagulated rather than opened, thus decreasing fluid absorption and bleeding compared with resection methods.
Although endometrial resection can resect small submucous fibroids, there is an increased risk of uterine perforation with resection methods. One theoretical benefit with endometrial resection is that pieces of the endometrium are available for examination by the pathologist. With coagulation methods, no material is available for review. However, with appropriate evaluation of patients before ablation procedures, along with the possibility of target biopsy at the time of the procedure, the likelihood of missed carcinoma is quite rare.
Procedure for Rollerball Ablation.
Generally, the electrosurgical generator is set at 60–100 W. Although we generally use pure cutting current, many authors use some form of blended current during ablation. Whatever the current modulation, the lower wattage should be chosen initially and then increased depending on the tissue effect observed. With the commonly used 3-mm ball and a drag speed of 1 cm/second, the crater produced is approximately 1 mm in depth with thermal damage extending for 1–2 mm more. Slower drag speeds or higher wattage are associated with greater tissue penetration. The use of a rollerbar instead of the 3-mm ball allows a greater surface to be covered in a smaller amount of time but results in a lower current density and significantly less tissue penetration than with the rollerball, if all other factors are kept equal.
As with other techniques, as a safety measure, the electrode should be activated only when it is being withdrawn toward the operator. Most surgeons prefer to begin coagulation with the anterior wall because accumulation of bubbles and debris in this area over time makes coagulation later more difficult. However, some surgeons coagulate the tubal ostia initially, with the belief that this decreases fluid loss through the fallopian tubes and, subsequently, the lateral walls and finally the posterior walls (Fig. 4). As the ablation is carried downward, care should be exercised not to treat the cervical canal itself because this could result in sealing off of the endometrial cavity with subsequent development of a hematometrium or pyometrium.
{kind=link}
Endometrial Resection.
The technique for endometrial ablation is essentially the same as that for rollerball coagulation as noted previously (Fig. 5). Because the risk of perforation is higher with this technique, special care should be taken in the thinner area around the tubal ostia.
{kind=link}
Most surgeons prefer an 8-mm diameter loop for endometrial ablation by resection. With this loop, 4 mm of tissue are resected with each pass. However, some surgeons prefer a 4-mm diameter loop because it is easier to place in restricted areas such as the ostia and because the risk of perforation is less. For this reason, this diameter loop is frequently chosen by those just learning the technique and for teaching purposes. Disadvantages to this size loop include that the loop is more easily damaged and requires more passes to obtain adequate tissue destruction.
Global Endometrial Ablation Systems
THERMAL BALLOON.
The first global endometrial ablation system granted Food and Drug Administration (FDA) approval in the United States in December 1997 was the ThermaChoice intrauterine hot water balloon (Gynecare, Inc, a division of Ethicon, Inc, Somerville, NJ). This device uses an intrauterine balloon to deliver destructive heat to the endometrial layer to destroy the blood supply (Fig. 6). Placement of the device requires cervical dilatation to 5 cm. The device is approved for use with uterine cavities up to 4–10 cm in lenght. The ThermaChoice procedure uses a water-filled balloon that conforms to the shape of the uterus. Once activated, the water is heated by a heating element to a temperature of approximately 87°C, or 187°F. The system is composed of a balloon connected to a catheter that is connected into a central control unit. The balloon is manually inflated with 5% dextrose in water (D5W) to a pressure of 160–170 mmHg. Inability to obtain suitable initial pressure may indicate a uterine perforation or a uterine cavity too large for the balloon. A heating element inside the balloon then heats the solution. In the ThermaChoice II system, a fluid mixing impeller distributes the heat more evenly. The heating interval is set at 8 minutes. If the pressure or temperature deviates outside prescribed parameters, the system automatically shuts down. If a uterine perforation occurs, the pressure decreases and deactivates the system. At the completion of the procedure, the balloon is deflated and removed.
{kind=link}
Initial studies in women undergoing hysterectomy have indicated that the temperature of the uterine serosa remains unchanged during balloon ablation.13 These same studies also indicate that cell death could be expected up to 5 mm from the surface of the balloon. A 5-year follow-up of the FDA randomized trail with rollerball ablation showed amenorrhea rates of 10.3% with balloon and 17.5% with rollerball were obtained.14
Bipolar Radiofrequency Ablation
The NovaSure endometrial ablation system ( Cytec, Marlborough, MA) was approved by the FDA in 2001. Placement of the device requires cervical dilatation to 8 cm. The device is approved for use with uterine cavities up to 6–10 cm in length ( 4–6.5 cm from internal os). This device uses an intrauterine fan made of two layers of copper mesh. After placement in the uterine cavity, the fan is deployed ( Fig. 7). This action creates a suction to bring the endometrial walls and the mesh into close contact. The cornua to cornu width is measured by the device and this measurement, along with the endometrial cavity length, is entered into the radiofrequency generator. A cavity perforation test is performed by inflating the endometrial cavity with CO2. Intrauterine pressure must be maintained for 4 seconds for a successful test. Bipolar radiofrequency current is then used to ablate the endometrium in less than 2 minutes. The radiofrequency generator monitors the tissue impedance and automatically terminates the procedure at the desired depth of coagulation. Amenorrhea rates in the FDA pivotal trials. was 36% for Novasure and 32% for rollerball. 14
{kind=link}
BALLOONLESS HOT WATER SYSTEMS.
Several companies have developed endometrial ablation systems that use unconfined intracavitary hot water as the source of heat for endometrial ablation. In the United States, only one manufacturer (BEI Corporation) has achieved FDA approval. Approval was first obtained in 2001. This HydoTermAblator, or HTA, system uses externally heated saline at 90°C rather than an internal source of energy (Fig. 8). Unlike the previously discussed systems, the uterine cavity is irrigated with the heated solution rather than being contained within a balloon. Before heated fluid is circulated, the cavity is hysteroscopically inspected using room temperature saline at a flow rate of 300 ml/min for 2 minutes. If this priming is successful, the heating element is activated. Fluid pressure is kept below 55 mmHg. This pressure is below the opening pressure of the fallopian tubes and prevents fluid flow into the abdominal cavity. Once the fluid reached 80°C the 10-minute treatment phase begins. Fluid temperature continues to elevate to a maximum of 90°C. After the treatment cycle, the fluid is cooled to 45°C and circulated for 1 minute during the cool down phase. Preliminary studies indicate that uniform endometrial destruction to a depth of 3–4 mm in the uterine cavity and 2–3 mm in the cornual region is easily obtained.15 This irrigation is performed under constant hysteroscopic monitoring.
{kind=link}
Potential advantages include complete coverage of the endometrial cavity despite surface irregularities or uterine anomalies such as uterine septa. Other proposed advantages include low likelihood of unrecognized perforation because the procedure is performed under direct visualization and the low risk of fluid and electrolyte imbalance that can be associated with laser or electrosurgical methods. In the FDA randomized trail with rollerball ablation, amenorrhea rates of 38.5% with HTA and 34.8% with rollerball were obtained.16
CRYOSURGICAL ENDOMETRIAL ABLATION.
A different method from the thermal methods of endometrial ablation is taken by the manufacturers of a cryogenic probe for endometrial ablation. The Her Option system (American Medical System, MN) received FDA approval in 2001. With this system, the probe is placed and monitored under ultrasonic guidance. Cervical dilation of 5 cm with a cavity length of under 10 cm is required. The cryoprobe is cooled by pressurized proprietary gas to –100°C to –120C. The cryoablation is capable of producing profound tissue destruction, averaging 9–12 mm in depth. The as-yet unproven assumption is that this deeper ablation should be associated with higher amenorrhea rates. The initial FDA trial used two freeze cycles of 4–6 minutes. The cryoablation procedure is a 10- to 12-minute procedure. Because the freezing has a partial anesthetic effect, it may prove to be an effective office procedure performed under paracervical block. In the FDA trial, 39% of women were managed under conscious sedation and paracervical block versus 1% of the rollerball group. Amenorrhea rates of 22.2% for Her Option versus 46.5% for rollerball have been reported.14
Microwave Endometrial Ablation
In 2000, the FDA approved the MEA (Microwave Endometrial Ablation) by Microsulis Americas Inc, Boca Raton for endometrial ablation. This device uses microwave energy at 9.2 GHz to accomplish endometrial ablation. The applicator is inserted into the uterine fundus and then moved from side-to-side. Once the fundal temperature reaches 70°C, the applicator is withdrawn while continuing the side-to-side motions. D&C is not recommended. Hysteroscopy is also recommended prior to device placement. Ultrasound verification of a uterine wall thickness of over 10 mm is needed prior to the procedure. Uterine cavities up to 14 cm in length can be treated. Amenorrhea rates from the FDA pivotal trial were 55.3% for MEA and 45.8% for rollerball.14
REFERENCES
American College of Obstetrics and Gyecology. ACOG Practice Bulletin. Clinical management guidelines for Obstet Gynecol. 2007 May;109(5):1233-48 |
|
Lomano J: Endometrial ablation for the treatment of menorrhagia: A comparison of patients with normal, enlarged, and fibroid uteri. Lasers Surg Med 11: 8, 1991 |
|
Shamonki MI, Ziegler WF, Badger GJ, Sites CK: Prediction of endometrial ablation success according to perioperative findings. Am J Obstet Gynecol 182: 1005, 2000 |
|
Eskandar MA, Vilos GA, Aletebi FA et al: Hysteroscopic endometrial ablation is an effective alternative to hysterectomy in women with menorrhagia and large uteri. J Am Assoc Gynecol Laparosc. 2000 Aug;7(3):339-45 |
|
Valle RF, Baggish MS: Endometrial carcinoma after endometrial ablation: High-risk factors predicting its occurrence. Am J Obstet Gynecol 179: 569, 1998 |
|
Goldrath MH: Use of danazol in hysteroscopic surgery for menorrhagia. J Reprod Med 35: 91, 1990 |
|
Brooks PG, Serden SP, Davos I: Hormonal inhibition of the endometrium for resectoscopic endometrial ablation. Am J Obstet Gynecol 164: 1601, 1991 |
|
Baggish MS, Sze EH: Endometrial ablation: A series of 568 patients treated over an 11-year period. Am J Obstet Gynecol 174: 908, 1996 |
|
Brooks PG: A clinical comparison between hydrothermablation and rollerball ablation to treat menorrhagia: A multicenter clinical trial. Obstet Gynecol 95: S59, 2000 |
|
Baggish MS, Valle RF, Barbot J: Endometrial ablation. In Baggish MS, Barbot J, Valle RF (eds): Diagnostic and Operative Hysteroscopy. St Louis, Mosby, 1999 |
|
Baggish MS, Daniell JF: Catastrophic injury secondary to the use of coaxial gas-cooled fibers and artificial sapphire tips for intrauterine surgery: A report of five cases. Lasers Surg Med 9: 581, 1989 |
|
Goldrath MH, Fuller TA, Segal S: Laser photovaporization of endometrium for the treatment of menorrhagia. Am J Obstet Gynecol 140: 14, 1981 |
|
Singer A, Almanza R, Gutierrez A et al: Preliminary clinical experience with a thermal balloon endometrial ablation method to treat menorrhagia. Obstet Gynecol 83: 732, 1994 |
|
Zarek S, Sharp HT: Global endometrial ablation devices. Clin Obstet Gynecol. 2008 Mar;51(1):167-75 |
|
Richart RM, das Dores GB, Nicolau SM et al: Histologic studies of the effects of circulating hot saline on the uterus before hysterectomy. J Am Assoc Gynecol Laparosc 6: 269, 1999 |
|
Goldrath MH: Evaluation of HydroThermAblator and rollerball endometrial ablation for menorrhagia 3 Years after treatment. J Am Assoc Gynecol Laparosc. 2003 Nov;10(4):505-11 |