Positron Emission Tomography Imaging of Gynecologic Malignancies
Authors
INTRODUCTION
Positron emission tomography (PET) imaging utilizes radiopharmaceuticals that are labeled with positron emitters. After injection of these radiopharmaceuticals, the emitted radiation from the body is registered by external detectors of the PET camera and tomographic images are reconstructed to obtain images of tracer distribution.
Positrons, the antiparticles of electrons, are emitted from radionuclides that contain excess protons. The emitted positron has a short range and readily captures an electron when it comes to rest. This reaction is called annihilation and results in formation of two 511-keV photons that travel at 180 degrees in opposite directions. In a PET camera, these are detected by two opposite detectors that record an event only if the detection occurs at precisely the same time (coincidence detection), that is when the annihilation takes place along a line between two detectors.
Because the origin of coincidence photons can be accurately localized with PET imaging, the differential attenuation of photons in the tissue can be easily mapped and corrected by using an external source of radiation. This allows accurate quantification of uptake of the radiopharmaceutical to provide a reliable measure of perfusion and metabolism in a specific organ or tumor. This can be used to distinguish between benign versus malignant lesions and also to measure response to therapy. The most commonly applied method for quantification is the standardized uptake value (SUV), which is the ratio of concentration of the radiopharmaceutical in the tumor to the average concentration in the whole body.
The most commonly used radiopharmaceutical in clinical PET imaging is a glucose analogue: 2-[18F]-fluoro-2-deoxy-d-glucose (FDG). FDG uptake is enhanced in malignant cells because of enhanced transport of glucose (increased number of glucose transporter proteins on cancer cells) and increased rate of glycolysis promoted by increased activity of glycolytic enzymes of hexokinase and phosphofructokinase. After FDG enters the cells it is phosphorylated similar to glucose but does not enter further metabolic pathways and therefore accumulates inside the cell. FDG uptake is, unfortunately, not specific for tumors and can be seen with infections and inflammation, likely because of the increased rate of glycolysis in inflammatory cells, especially in activated macrophages. The uptake of FDG in inflammations is however usually less than malignancies, that is the higher the FDG uptake (or the higher the SUV), the higher is the likelihood for malignancy in a lesion.
FDG-PET is currently routinely performed for the imaging of lung, esophageal, head and neck, colon, and breast cancers, and lymphoma and melanoma. The available literature for FDG-PET imaging in gynecologic tumors is limited and mainly includes imaging of ovarian and cervical cancers.
CERVICAL CANCER
Cervical cancer is the third most common gynecologic cancer in the United States with an annual incidence of 12,800 cases and 4600 deaths per year. The overall mortality from cervical cancer has decreased as a result of early detection of preinvasive disease with Pap smears; however, the mortality from invasive disease has not changed in 30 years. Carcinoma of the cervix is most commonly staged using the FIGO (International Federation of Gynecology and Obstetrics) classification that stages the tumors based on their size, local extension, and spread to adjacent or distant organs. These are evaluated by a combination of clinical and radiologic examinations that include biopsy, colposcopy, endocervical curretage, hysteroscopy, proctoscopy, intravenous pyelogram, chest x-ray and skeletal x-rays. Another important prognostic factor in cervical cancer, which is not included in FIGO classification, is the lymph node status. The preoperative evaluation of lymph node status has been done with lymphangiography, computed tomography (CT), or magnetic resonance imaging (MRI). The sensitivity of CT and MRI for detection of lymph node metastasis is not satisfactory (44% to 50%). Lymphangiography is not widely available and does not appear to be more accurate than CT or MRI. Therefore, surgical or laparascopic total pelvic lymphadenectomy and selective paraaortic lymphadenectomy are commonly performed in conjunction with hysterectomy to evaluate for lymph node involvement in surgical candidates. Patients with positive pelvic lymph nodes are treated with postoperative whole-pelvis external beam irradiation and intracavitary brachytherapy.
Several studies have reported promising results for PET imaging with FDG in diagnosis of lymph node metastases from cervical cancer. Sugawara and colleagues1 studied 21 patients with cervical cancer, 7 of whom were shown to have lymph node metastases based on surgical data and clinical or imaging follow-up. Abnormal accumulation of FDG on PET images and presence of lymph nodes greater than 1 cm in paraaortic or pelvic chain on CT scans were considered as positive for malignant. The FDG-PET scan showed a sensitivity of 86% compared to 57% for CT. The SUVs of metastatic lymph nodes ranged from 2.14 to 6.81. Identification of para-aortic nodal metastasis is of special importance because in these patients the field of radiotherapy is extended to include the abdomen up to the level of T-12 vertebra. Rose amd colleages,2 in their study of 32 patients with predominantly FIGO stage IIIB disease with no evidence of para-aortic nodal disease on CT found a sensitivity of 75% (6/8) and a specificity of 92% (22/24) for identification of para-aortic nodal metastases with FDG-PET. PET correctly identified pelvic nodal metastases in all 11 patients with pelvic nodal involvement and was superior to CT, which identified pelvic nodal enlargement only in 5 patients. Reinhardt and coworkers3 compared FDG-PET and MRI in 35 patients with FIGO stage IB and II disease. All patients had pelvic lymphadenectomy and 12 patients also had dissection of para-aortic lymph nodes. Eleven patients had lymph node metastases. The criterion for malignancy was lymph node diameter of 1 cm or greater for MRI and focal uptake of FDG in pelvic and para-aortic nodes for PET imaging. The sensitivity/specificity values of PET and MRI in diagnoisis of nodal disease were 0.81/0.99 and 0.67/0.99, respectively.3
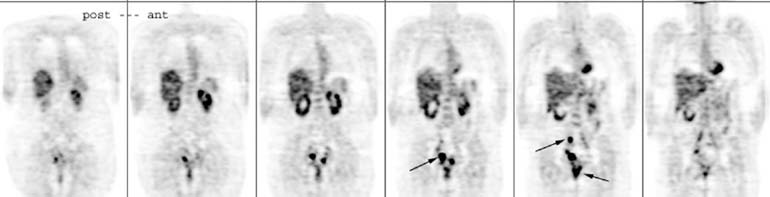
The prognostic significance of FDG uptake was addressed by Grigsby and colleagues4 in a retrospective study that included 101 patients with cervical cancer who were followed for a median period of 15.4 months after definitive irradiation and chemotherapy. Patients with negative para-aortic lymph nodes by CT had a 64% 2-year progression-free survival rate when PET was negative, but only 18% if PET showed abnormal FDG uptake. The FDG PET scan of a patient with recurrent cervical cancer is shown in Figure 1.
{kind=link}
OVARIAN CANCER
Ovarian cancer is the fifth most common cancer diagnosed in women in the United States with an annual incidence of 23,100 and 14,000 deaths per year. This high mortality rate is attributed to the presence of advanced-stage disease in 2 of 3 patients at the time of initial diagnosis. There is a great need for effective screening methods of ovarian cancer in asymptomatic patients. Surgical exploration is the gold standard investigation in primary or recurrent ovarian carcinoma. Staging laparatomy is required for histologic diagnosis, identification of tumor spread, and debulking of tumor masses prior to chemotherapy. After initial chemotherapy a second-look operation can be performed to tailor subsequent therapy.
Several studies have evaluated the accuracy of FDG-PET in the diagnosis of cancer in ovarian masses. Despite the promising results in earlier studies, recent studies have failed to show a satisfactory accuracy for PET in distinguishing benign masses from cancerous lesions. This is likely related to patient selection, which in earlier studies enrolled selected patients with a high likelihood of cancer compared to more recent studies that were conducted in patient populations with a more realistic incidence of ovarian cancer. PET shows a reasonable accuracy for advanced ovarian cancers but misses most small and borderline cancers, which are most relevant for screening since they have the highest cure potential. The sensitivity and specificity of PET in diagnosis of ovarian cancer in different series is summarized in Table 1.
TABLE 1. Sensitivity and Specificity of Position Emission Tomography for Diagnosis of Cancer in Ovarian Masses
Study | Total Number of Patients | Patients with Primary Ovarian Cancer | Number of Advanced Cancers | Number of Borderline Tumors | Overall Sensitivity/Specificity | Sensitivity for Borderline Tumors |
Grab et al.5 (2000) | 101 | 12 | 7 | 5 | 0.58/0.80 | 0.20 |
Fenchel et al.6 (1999) | 85 | 8 | 5 | 3 | 0.50/0.78 | 0.33 |
Schroeder et al.7 (1999) | 40 | 14 | 12 | 2 | 0.80/0.90 | 0.00 |
Hubner et al.8 (1993) | 51 | 15 | Not available | Not available | 0.93/0.82 | Not available |
Ovarian cancer is staged surgically. Localization of tumor deposits prior to surgery is helpful in respect to detailed planning of the operation. The most common forms of spread of ovarian cancer are peritoneal and lymphogenic. Using FDG-PET, Schroder and colleagues7 have imaged 30 patients with ovarian cancer who were staged with laparatomy. FDG-PET showed a sensitivity of 71% in diagnosis of peritoneal involvement and 73% for diagnosis of pelvic lymph node metastasis.7
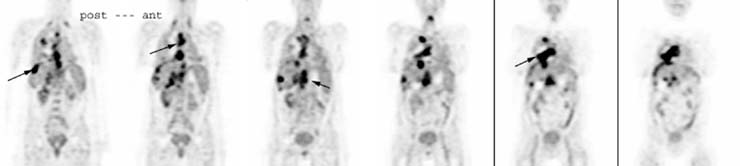
Ovarian cancer has a high recurrence rate even after primary chemotherapy in early-stage tumors. Recurrent tumors are usually sensitive to chemotherapy if they responded initially and recurrence has not occurred before 6 months after initial chemotherapy. However, a second cytoreductive surgery may prolong survival in patients with resectable tumors. Nakamoto and colleagues9 have compared PET and conventional imaging in 24 patients with suspected recurrence of ovarian cancer after initial surgery and chemoradiotherapy. The accuracy of PET imaging for recurrence was 79.2%, which was not significantly different from 73.3% obtained for conventional imaging that included CT and/or MRI. The accuracy however was significantly improved to 94.4% when PET was combined with conventional imaging. PET provided additional information in 42% of patients, which resulted in change of management in 33% of the patient group. The FDG PET scan of a patient with recurrent ovarian cancer is presented in Figure 2.
{kind=link}
In conclusion, FDG-PET imaging appears to be a new promising tool for diagnosis of recurrent and metastatic disease in ovarian and cervical cancers. It has a good accuracy for detection of pelvic and para-aortic nodal disease in cervical cancer and appears superior to conventional imaging modalities. At this time, FDG-PET cannot be recommended for screening of asymptomatic ovarian masses because of its low sensitivity for small and borderline tumors. Although FDG-PET appears to be a particularly useful tool in recurrent ovarian cancer to evaluate for metastatic disease, especially when combined with conventional imaging, it cannot exclude the presence of peritoneal and pelvic nodal disease and therefore cannot replace initial staging or second-look surgery.
REFERENCES
Sugawara Y, Eisbruch A, Kosuda S, et al: Evaluation of FDG PET in patients with cervical cancer. J Nucl Med 40:1125, 1999 |
|
Rose PG, Adler LP, Rodrigues M, et al: Positron emission tomography for evaluating para-aortic nodal metastasisin locally advanced cervical cancer before surgical staging: A surgicopatholgic study. J Clin Oncol 17:41, 1999 |
|
Reinhardt MJ, Ehritt-Braun C, Vogelgesang D, et al: Metastatic lymph nodes in patients with cervical cancer: Detection with MRimaging and FDG PET. Radiology 218:776, 2001 |
|
Grigsby PW, Siegel B, Dehdashti F: Lymph node staging by positron emission tomography in patients with carcinoma of the cervix. J Clin Oncol 19:3745, 2001 |
|
Grab D, Flock F, Stohr I, et al: Classification of asymptomatic adnexal masses by ultrasound, magneticresonance imaging, and positron emission tomography. Gynecol Oncol 77:454, 2000 |
|
Fenchel S, Kotzerke J, Stohr I, et al: Preoperative assessment of asymptomatic adnexal tumors by positronemission tomography and F 18 fluorodeoxyglucose. Nuklearmedizin 38:101, 1999 |
|
Schroder W, Zimny M, Rudlowski C, et al: The role of 18F-fluoro-deoxyglucose positron emission tomography (18F-FDG PET)in diagnosis of ovarian cancer. Int J Gynecol Cancer 9:117, 1999 |
|
Hubner KF, McDonald TW, Niethammer JG, et al: Assessment of primary and metastatic ovarian cancer by positron emissiontomography (PET) using 2-[18F]deoxyglucose (2-[18F]FDG). Gynecol Oncol 51:197, 1993 |
|
Nakamoto Y, Saga T, Ishimori T, et al: Clinical value of positron emission tomography with FDG for recurrent ovarian cancer. AJR Am J Roentgenol 176:1449, 2001 |