Intrauterine Adhesions: Asherman's Syndrome
Authors
INTRODUCTION
Amenorrhea associated with intrauterine adhesions was first described in 1894 by H. Fritsch in a patient after postpartum curettage.1 Subsequently, in 1948 and 1950 J.G. Asherman published two reports2,3 on the frequency and the etiology of intrauterine adhesions and the eponym Asherman's syndrome has been used ever since. Many case series have appeared in the literature describing diagnostic, therapeutic, and adjunctive methods to address intrauterine adhesions. However, no randomized control trials have been conducted to assess or compare the efficacy of any of these techniques.
PREVALENCE AND SYMPTOMATOLOGY
Intrauterine adhesions, also known as synechiae, are found in 1.5% in women who undergo hysterosalpingography.4 Patients with intrauterine adhesions usually present with infertility, menstrual cycle disorders, repeated pregnancy losses, or abnormal adherence of the placenta.5,6
Among women with intrauterine adhesions, the most common symptom is infertility, affecting approximately 43%.5,7 Menstrual cycle disorders, including amenorrhea, are also a common symptom, even though the term Asherman's syndrome is technically synonymous with secondary amenorrhea.5,7 Repeated pregnancy losses are observed in 14% of patients with intrauterine adhesions. Disorders of placentation, including placenta accreta and previa, are relatively rare (1%).5,7
ETIOLOGY
Endometrial injury resulting from trauma, infection, or inflammation can lead to the formation of intrauterine adhesions. Pregnancy is the most common predisposing factor, usually associated with trauma to the endometrium, as seen in patients undergoing curettage in the puerperium, after missed abortion, evacuation of a hydatidiform mole, or cesarean section.5,7 Postpartum curettage is most likely to cause intrauterine adhesions when performed between the second and fourth weeks postpartum.5,6 Trauma after uterine surgery, including myomectomy and metroplasty, may result in intrauterine adhesions.
Infections of the endometrium that result in severe or chronic inflammation may result in intrauterine adhesions. Severe pelvic inflammatory disease, particularly in association with an intrauterine device, is one cause. Genital tuberculosis and schistosomiasis are other rare causes of chronic endometritis and may result in complete destruction of the endometrium.5,7
DIAGNOSIS
Hysteroscopy is the gold standard of methods for diagnosis of intrauterine adhesions, against which all others must be compared. Hysterosalpingography (HSG) is a useful screening outpatient radiological procedure for diagnosis8, 9, 10 and has a 75% sensitivity, a 95% specificity, a 50% positive predictive value (PPV) and a 98% negative predictive value (NPV).8 For greatest accuracy, it is important to perform HSG without a speculum in the vagina and, if a balloon catheter is used, to deflate the balloon before ending the examination to ensure that the entire cavity has been adequately visualized. Mild to moderate intrauterine adhesions generally yield irregular filling defects in a lacunar pattern and may be identified in any region of the uterine cavity.8 When adhesions are severe, it may be impossible to visualize the endometrial cavity altogether. The fluoroscopic exposure (radiation exposure) associated with a normal HSG is approximately 63 seconds (range 17–404 seconds) when the test is normal and 100 seconds (range 28–172 seconds) when abnormal.11 Mild to moderate cramping pain is commonly associated with HSG and can be minimized by treatment with nonsteroidal anti-inflammatory agents beginning approximately 1 hour before the procedure. Pelvic infections, vagal reactions, intravasation of contrast, and iodine-induced allergic reactions are uncommon but potentially serious complications of HSG.
For diagnosis of intrauterine adhesions, transvaginal ultrasonographic (TVS) examination is highly specific (95%), but also insensitive (0%), with a PPV of 50% and a NPV of 95%.8 Some have reported a significantly better sensitivity and PPV, but such results can be difficult to achieve by most ultrasonographers.8, 12 Adhesions may be best visualized with TVS in the luteal phase of the menstrual cycle and appear as an echogenic, irregular eccentric lines within the endometrium or as a focal narrowing of the endometrial thickness.8 TVS generally is not a reliable diagnostic test for identification of intrauterine adhesions,8 but may be helpful in planning hysteroscopic adhesiolysis. The presence of a well-developed endometrial stripe is highly predictive of a successful surgical and clinical outcome in women with severe Asherman's syndrome.13 In contrast, surgery in women with minimal endometrium as observed with TVS often cannot restore the uterine cavity and yields little benefit.13 The introduction of three-dimensional sonography now allows interactive visualization of the endometrial cavity, through multiplanar reformatting, and provides an improved depiction of adhesions and extent of cavity damage compared to two-dimensional ultrasound in patients with suspected Asherman's syndrome.14
Sonohysterography (SHG), involving TVS after introduction of sterile water or saline, has a diagnostic accuracy comparable to HSG for identification of intrauterine adhesions.8 SHG has a sensitivity of 75%, a specificity of 93%, a PPV of 43%, and a NPV of 98%.8 The relatively low PPV of both SHG and HSG possibly relates to artifacts produced by the inadvertent injection of air bubbles or the presence of cervical mucus.8 When observed with SHG, intrauterine adhesions usually appear as mobile, thin, echogenic bands that bridge a normally distensible endometrial cavity. Occasionally thicker, broad-based bands or complete obliteration of the endometrial cavity may be observed.15 Side effects of SHG are similar to those of HSG and include moderate (15%) to severe (8%) pain, vagal reactions (5%), and pelvic infection (1.5%).8 The procedure is generally brief in duration, requiring less than 5 minutes to perform in most cases (87%).8
Magnetic resonance imaging (MRI) has been used to detect intrauterine adhesions, but experience is limited to a few case reports in the radiological literature.16, 17 Consequently, its diagnostic accuracy is uncertain.
Hysteroscopy is the gold standard of methods for both the diagnosis and treatment of intrauterine adhesions.5, 18 Endoscopic surgery clearly reveals the location, shape, and extent of adhesions and thereby provides the means for formal classification of the extent of disease. In view of the relatively low sensitivity of both HSG and SHG, a direct hysteroscopic examination of the uterine cavity is clearly a superior method.8, 18 Standard techniques include use of a rigid 4-mm hysteroscope, inserted through a 5-mm diagnostic sheath,19 usually performed as an outpatient surgical procedure. More recently microhysteroscopes, both rigid and flexible, having an outer diameter between 2 and 3 mm, permit both diagnostic and operative procedures to be performed in the office setting.20 During hysteroscopy, the endometrial cavity may appear to be divided into several smaller chambers by central intrauterine adhesions. The adhesive bands form columns between the opposing walls of the cavity and are widest at their insertions.5 Adhesions in the cornual regions often appear as a half-drawn curtain that obscures the tubal orifice.5 Mucosal adhesions are most frequently pink, like the surrounding endometrium, and generally are easy to lyse.5 Thicker fibromuscular adhesions appear as thicker, white bands.5
PATHOLOGY
The spectrum of severity of intrauterine adhesions is broad, ranging from diffuse, thin, and filmy to thick and fibrous bands to mural adherence that effectively obliterates the entire endometrial cavity. Adhesions may arise from the endometrium, the myometrium or from connective tissue.5 Endometrial synechiae generally are filmy and easily lysed. Myometrial adhesions are the most common variety and appear thicker with a thin layer of overlying endometrium and glandular ostia on the surface.5 Fibrous connective tissue adhesions are dense, have no overlying endometrium, and have the worst prognosis because the basalis layer of the endometrium, from which new grown arises, is altogether absent.5
CLASSIFICATION
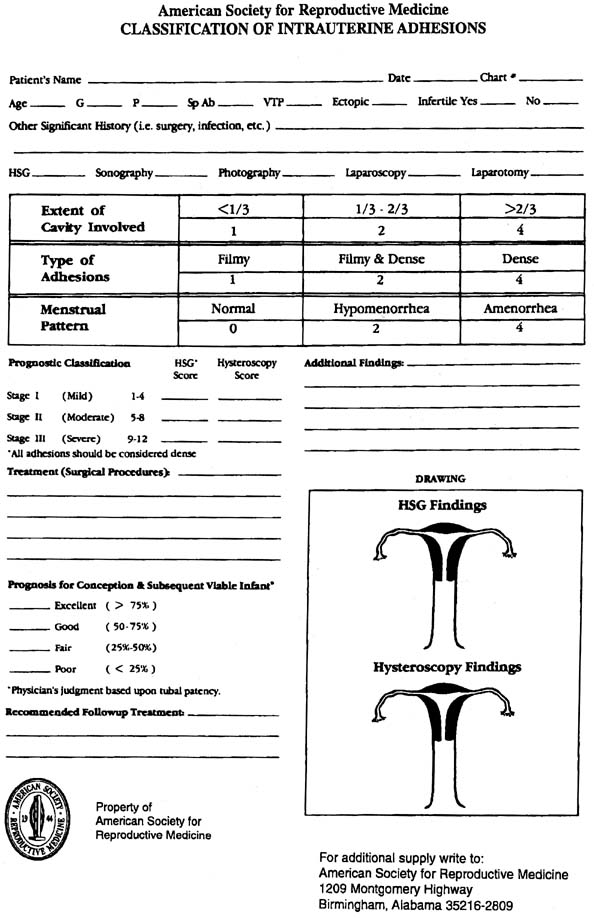
Many systems for the classification of intrauterine adhesions have been proposed,21, 22, 23, 24, 25, 26, 27 but all such schemes are based on hysteroscopic findings at the time of their definitive diagnosis and treatment. The American Society for Reproductive Medicine classification correlates the menstrual pattern with the severity of adhesive disease (type of adhesions and extent of the cavity involved) as demonstrated by HSG and hysteroscopy (Fig. 1).21 Unfortunately, well-designed prospective studies have not been conducted to accurately determine the prognostic value of this or any other classification system.
{kind=link}
TREATMENT
Hysteroscopic adhesiolysis is the treatment of choice for the management of intrauterine adhesions. When the adhesions are thin and filmy in nature, blunt dissection with the leading edge of the hysteroscope often is sufficient to achieve their lysis. Thicker adhesions must be divided with scissors, electrosurgical instruments, or with a fiberoptic laser. No one method appears to offer a distinct advantage over others.5 Adhesiolysis is usually performed as an outpatient procedure under general or epidural anesthesia. Office-based operative hysteroscopy using modern 3-mm multichannel instruments under local anesthesia is also possible, but proper patient selection is essential to success and to minimize operative complications.20, 28
Restoration of normal anatomy (93%) and endometrial function (95%) generally can be achieved with hysteroscopic surgery.29 The likelihood of success relates to the appearance of the endometrium as observed with preoperative TVS and on the extent and character of the adhesions.13, 30
In severe cases in which the uterine cavity has been obliterated or is very narrow and fibrotic, a number of adjuvant methods have been described that may improve results and minimize the risk of uterine perforation.31, 32, 33, 34, 35, 36 Operative hysteroscopy can be performed under the control of simultaneous abdominal ultrasound32 or laparoscopy in efforts to better define the correct plane for dissection.. Recently, use of a specially designed laparoscopic ultrasound probe, introduced through a 10-mm abdominal port, has been described to achieve the same purpose.34 Alternatively, pressure lavage with normal saline under ultrasound guidance may be used to effectively hydrodissect intrauterine adhesions that are not particularly dense or extensive.35 Effective lysis of intrauterine adhesions can also be accomplished with scissors or a balloon catheter under fluoroscopic control and local or intravenous anesthesia.36
Various adjuvant therapies designed to improve outcomes after intrauterine adhesiolysis have been described. However, such descriptions are largely limited to case series and few randomized controlled trials (RCT) have been conducted to assess their efficacy.
Vaginal misoprostol 200-mg has been advocated to soften the cervix before operative hysteroscopy and one recent RCT indicates that such treatment can eliminate the need for mechanical dilation and thereby reduce the risk of operative complications.37
To prevent recurrence of intrauterine adhesions after effective lysis, an 8-French pediatric Foley catheter with a 3-mL balloon can be inserted into the uterus and left in place for 7–10 days after surgery.7, 38, 39, 40 Insertion of an intrauterine device (IUD) immediately after adhesiolysis has been used successfully to prevent recurrence of adhesions,7 but it may not be as effective as placement of a pediatric foley,40 and has fallen from favor in the United States.
Although postoperative treatment with antibiotics for prevention of endometritis and exogenous estrogen supplementation to stimulate rapid endometrial regeneration are frequently used in efforts to improve outcomes, there is no objective evidence to demonstrate the effectiveness of these adjuvant treatments.39 Oral doxycycline 100-mg twice daily is commonly prescribed for the interval during which an intrauterine catheter is in place.38 Oral conjugated equine estrogens, 1.25–2.5 mg daily, are often prescribed for an interval of 10 38up to 30 days after surgery, in combination with oral medroxyprogesterone acetate, 10 mg daily, during the last 10 days of exogenous estrogen treatment.
After successful lysis of intrauterine adhesions, normal menstruation resumes in 78–92% of women; another 8–9% may have menses relatively light or short in duration (hypomenorrhea).41 The incidence of spontaneous abortion after lysis of intrauterine adhesions (15–43%) is generally lower than that reported before treatment (24–87%).42, 43 After hysteroscopic adhesiolysis, 69% of women achieve a successful pregnancy. The incidence of preterm delivery (2%), placenta previa (1%), stillbirth (1%), postpartum hemorrhage or retained placenta (4%) is generally low.42
Acute complications of operative hysteroscopy include uterine perforation, fluid overload, and hyponatremia, hemorrhage, infection, and death. Late-occurring complications of hysteroscopic surgery include recurrent adhesions and uterine rupture in a subsequent pregnancy.44, 45
Postoperative diagnostic tests (HSG, SHG, or hysteroscopy) should be performed after 4–6 weeks to reevaluate the endometrial cavity and determine whether recurrence of intrauterine adhesions has occurred. This is especially true in the case of repeated pregnancy losses.
For further information: www.ashermans.org
The International Asherman's Association
REFERENCES
Fritsch H: Ein Fall von Volligem Schwund der Gebarmutterhohle nach Auskratzung. Zentralbl Gynaekol 18:1337, 1894 |
|
Asherman JG: Amenorrhea traumatic (atretica). J Obstet Gynaecol Br Emp 55:23, 1948 |
|
Asherman JG: Traumatic intra-uterine adhesions. J Obstet Gynaecol Br Emp 7:892, 1950 |
|
Dmowski WP, Greenblatt RB: Asherman's syndrome and risk of placenta accreta. Obstet Gynecol 34:288-299, 1969 |
|
Al Inany H: Intrauterine adhesions. An update. Acta Obstet Gynecol Scand 80:986-993, 2001 |
|
March CM: Intrauterine adhesions. Obstet Gynecol Clin North Am 22:491-505, 1995 |
|
Schenker JG: Etiology of and therapeutic approach to synechia uteri. Eur J Obstet Gynecol Reprod Biol 65:109-113, 1996 |
|
Soares SR, Barbosa dos Reis MM, Camargos AF: Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertil Steril 73:406-411, 2000 |
|
Preutthipan S, Linasmita V: A prospective comparative study between hysterosalpingography and hysteroscopy in the detection of intrauterine pathology in patients with infertility. J. Obstet Gynaecol Res 29:33-37, 2003 |
|
Dalfo A, Ubeda B, Ubeda A, et al.: Diagnostic value of hysterosalpingography in the detection of intrauterine abnormalities: A comparison with hysteroscopy. Am J Roentgenol 183:1405-1409, 2004 |
|
Karande VC, Pratt DE, Balin MS et al: What is the radiation exposure to patients during a gynecoradiologic procedure? Fertil Steril 67:401-403, 1997 |
|
Fedele L, Bianchi S, Dorta M et al: Intrauterine adhesions: detection with transvaginal US. Radiology 199:757-759, 1996 |
|
Schlaff WD, Hurst BS: Preoperative sonographic measurement of endometrial pattern predicts outcome of surgical repair in patients with severe Asherman's syndrome. Fertil Steril 63:410-413, 1995 |
|
Sylvestre C, Child T, Tulandi T, et al.: A prospective study to evaluate the efficacy of two- and three-dimensional sonohysterography in women with intrauterine lesions. Fertil Steril 79:1222-1225, 2003 |
|
Davis PC, O'Neill MJ, Yoder IC et al: Sonohysterographic findings of endometrial and subendometrial conditions. Radiographics 22:803-816, 2002 |
|
Letterie GS, Haggerty MF: Magnetic resonance imaging of intrauterine synechiae. Gynecol Obstet Invest 37:66-68, 1994 |
|
Dykes TA, Isler RJ, McLean AC: MR imaging of Asherman syndrome: total endometrial obliteration. J Comput Assist Tomogr 15:858-860, 1991 |
|
Raziel A, Arieli S, Bukovsky I et al: Investigation of the uterine cavity in recurrent aborters. Fertil Steril 62:1080-1082, 1994 |
|
Fedele L, Vercellini P, Viezzoli T et al: Intrauterine adhesions: Current diagnostic and therapeutic trends. Acta Eur Fertil 17:31-37, 1986 |
|
Lindheim SR, Kavic S, Shulman SV et al: Operative hysteroscopy in the office setting. J Am Assoc Gynecol Laparosc 7:65-69, 2000 |
|
The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril 49:944-955, 1988 |
|
March CM, Israel R, March AD: Hysteroscopic management of intrauterine adhesions. Am J Obstet Gynecol 130:653-657, 1978 |
|
Valle RF, Sciarra JJ: Intrauterine adhesions: Hysteroscopic diagnosis, classification, treatment, and reproductive outcome. Am J Obstet Gynecol 158:1459-1470, 1988 |
|
Wamsteker K, De Block S: Diagnostic hysteroscopy: technique and documentation. In: Sutton C, Diamond M, (eds): Endoscopic Surgery for Gynaecologists. 263-276, London, WB Saunders, 1993 |
|
Nasr AL, Al-Inany HG, Thabet SM et al: A clinicohysteroscopic scoring system of intrauterine adhesions. Gynecol Obstet Invest 50:178-181, 2000 |
|
Hamou J, Salat-Baroux J, Siegler AM: Diagnosis and treatment of intrauterine adhesions by microhysteroscopy. Fertil Steril 39:321-326, 1983 |
|
Sugimoto O: Diagnostic and therapeutic hysteroscopy for traumatic intrauterine adhesions. Am J Obstet Gynecol 131:539-547, 1978 |
|
Perez-Medina T, Bajo JM, Martinez-Cortes L et al: Six thousand office diagnostic-operative hysteroscopies. Int J Gynaecol Obstet 71:33-38, 2000 |
|
Pace S, Stentella P, Catania R et al: Endoscopic treatment of intrauterine adhesions. Clin Exp Obstet Gynecol 30:26-28, 2003 |
|
Pistofidis GA, Dimitropoulos K, Mastrominas M: Comparison of operative and fertility outcome between groups of women with intrauterine adhesions after adhesiolysis. J Am Assoc Gynecol Laparosc 3:S40, 1996 |
|
Magos A: Hysteroscopic treatment of Asherman's syndrome. Reprod Biomed Online Suppl 3:46-51, 2002 |
|
Bellingham FR: Intrauterine adhesions: hysteroscopic lysis and adjunctive methods. Aust N Z J Obstet.Gynaecol 36:171-174, 1996 |
|
McComb P, Wagner BL: Simplified therapy for Asherman's syndrome. Fertil Steril 68:1047-1050, 1997 |
|
Bulent TM, Oktem M, Noyan V: Laparoscopic intracorporeal ultrasound guidance during hysteroscopic adhesiolysis. Eur J Obstet Gynecol Reprod Biol 108:80-84, 2003 |
|
Coccia ME, Becattini C, Bracco GL et al: Pressure lavage under ultrasound guidance: a new approach for outpatient treatment of intrauterine adhesions. Fertil Steril 75:601-606, 2001 |
|
Karande V, Levrant S, Hoxsey R et al: Lysis of intrauterine adhesions using gynecoradiologic techniques. Fertil Steril 68:658-662, 1997 |
|
Preutthipan S, Herabutya Y: Vaginal misoprostol for cervical priming before opereative hysteroscopy: a randomized controlled trialObstet Gynecol 97:640-641, 2001 |
|
Knopman J, Copperman AB: Value of 3D ultrasound in the management of suspected Asherman's syndrome. J Reprod Med 52:1016-1022, 2007 |
|
Doyle MB, Lavy G: Intrauterine synechiae and pregnancy loss. Infertil Reprod Med Clin North Am 2:91-103, 1991 |
|
Orhue AAE, Aziken ME, Igbefoh JO: A comparison of two adjunctive treatments for intrauterine adhesions following lysis. Int J Gynecol Obstet 82:49-56, 2003 |
|
Polishuk WZ, Sadovsky E, Aviad I: Clinical significance of organic hypomenorrhea. Am J Obstet Gynecol 116:1058-1064, 1973 |
|
Shaffer W: Role of uterine adhesions in the cause of multiple pregnancy losses. Clin Obstet Gynecol 29:912-924, 1986 |
|
Goldenberg M, Sivan E, Sharabi Z et al: Reproductive outcome following hysteroscopic management of intrauterine septum and adhesions. Hum. Reprod. 10:2663-2665, 1995 |
|
Cooper JM, Brady RM: Late complications of operative hysteroscopy. Obstet Gynecol Clin North Am 27:367-374, 2000 |
|
Sandridge DA, Councell RB, Thorp JM: Endometrial carcinoma arising within extensive intrauterine synechiae. Eur J Obstet Gynecol Reprod Biol 56:147-149, 1994 |