Pregnancy in Adolescence
Authors
INTRODUCTION
The birth rate for teenagers 15–19 years is rising for the first time since 1991. The adolescent birth rate had been dropping steadily since a high of 61.8 births per 1,000 in 1991 to a low of 40.5 births per 1,000 in 2005. But between 2005 and 2006 there was a 3% increase in births to adolescents. According to data from the National Vital Statistics Reports, 435,427 births occurred to mothers aged 15–19 in 2006, correlating to a birth rate of 41.9 live births per 1,000 women in this age group.1 Thus, adolescent pregnancy continues to have major medical, social, and economic impact in the United States, with an adolescent birth rate ranking the highest of developed countries.2 Overall, 47.8% of high school students reported having ever engaged in sexual intercourse, with 7.1% stating that their age at first intercourse occurred before the age of 13, according to 2007 data from the CDC.3
Recent research has shown that adolescent pregnancy is not simply the result of a girl's failure to obtain and use contraception, but is instead inexorably linked to many social, cultural, educational, and economic factors influencing adolescent risk-taking behaviors. The negative medical and social consequences of adolescent pregnancy are considerable, and programs to reduce the incidence and ramifications of adolescent pregnancy must be multidimensional in their approach to adolescent pregnancy prevention.
DEMOGRAPHICS OF ADOLESCENT PREGNANCY
Sexual Activity
American teenagers become sexually active at the same age and have similar numbers of partners as teenagers in other industrialized countries.4 However, American teenagers' use of contraception is among the lowest in the world when compared with nations of similar economic development. The result is a teenage pregnancy rate that is twice as high as rates in Canada, England, or France and seven times as high as the teenage pregnancy rate in the Netherlands.4
Although the percentage of young adolescents (younger than age 15) having intercourse is smaller than the percent of older adolescents having sex, the medical risks related to a subsequent pregnancy are greater for younger teens. Young adolescents who are sexually active are more likely to have been abused, more likely to report multiple sex partners, and face greater obstetrical risks during pregnancy. In 2001, almost 7% of students reported engaging in sexual intercourse before age 13.5 Demographic risk factors for very early sexual activity (younger than age 13) include living in a rural area, having parents who receive welfare, being black, living in the south, and having partners who are significantly older.5, 6 Unfortunately, initiation of sexual activity is not a choice for many of these girls, because they are often victims of sexual abuse or coercion. Sixteen percent of young women who initiated sexual activity before age 16 report having engaged in sex involuntarily.7 Many young teens have partners who are significantly older; of females who engaged in voluntary sexual intercourse before age 16, 13% report that their first partner was older than age 20.7
Pregnancy Rates
In the United States, approximately 1 million teenagers become pregnant each year, and the estimates of pregnancies include the sum of live births, induced abortions, and spontaneous losses.8 Because of the various outcomes of pregnancies, precise pregnancy rates are difficult to determine; in addition, reports of national data reporting are delayed because of the time required to analyze large data sets.
The demographics of adolescent pregnancy have changed dramatically in the past 25 years. In 1970, only 30% of all teen births were to unmarried teenagers. In 2001, out-of-wedlock teen births accounted for 96% of births to teens younger than age 15 years and 79% of births to girls aged 15 to 19.9
Pregnancy Outcome: Abortion and Adoption Rates
Younger teens are more likely to choose abortion than older teens; 49% of pregnancies in girls aged 10–14 ended in abortion. Thirty five percent of teenagers 15–19 years old had elective abortions, with 65% of them continuing their pregnancy. The abortion rate for both groups has shown a significant decrease since 1985 when 62% of girls 10–14 years old, and 46% of girls aged 15–19 had elective abortions.10 The exact reasons for the decrease in abortion rates is not known, but likely reflects changes in many social, political, and cultural influences. More than 90% of adolescents who gave birth chose to raise the infants themselves, with only 8% of unmarried adolescents choosing to place their infants for adoption.11
Pregnancy Outcome: Adolescent Birth Rates
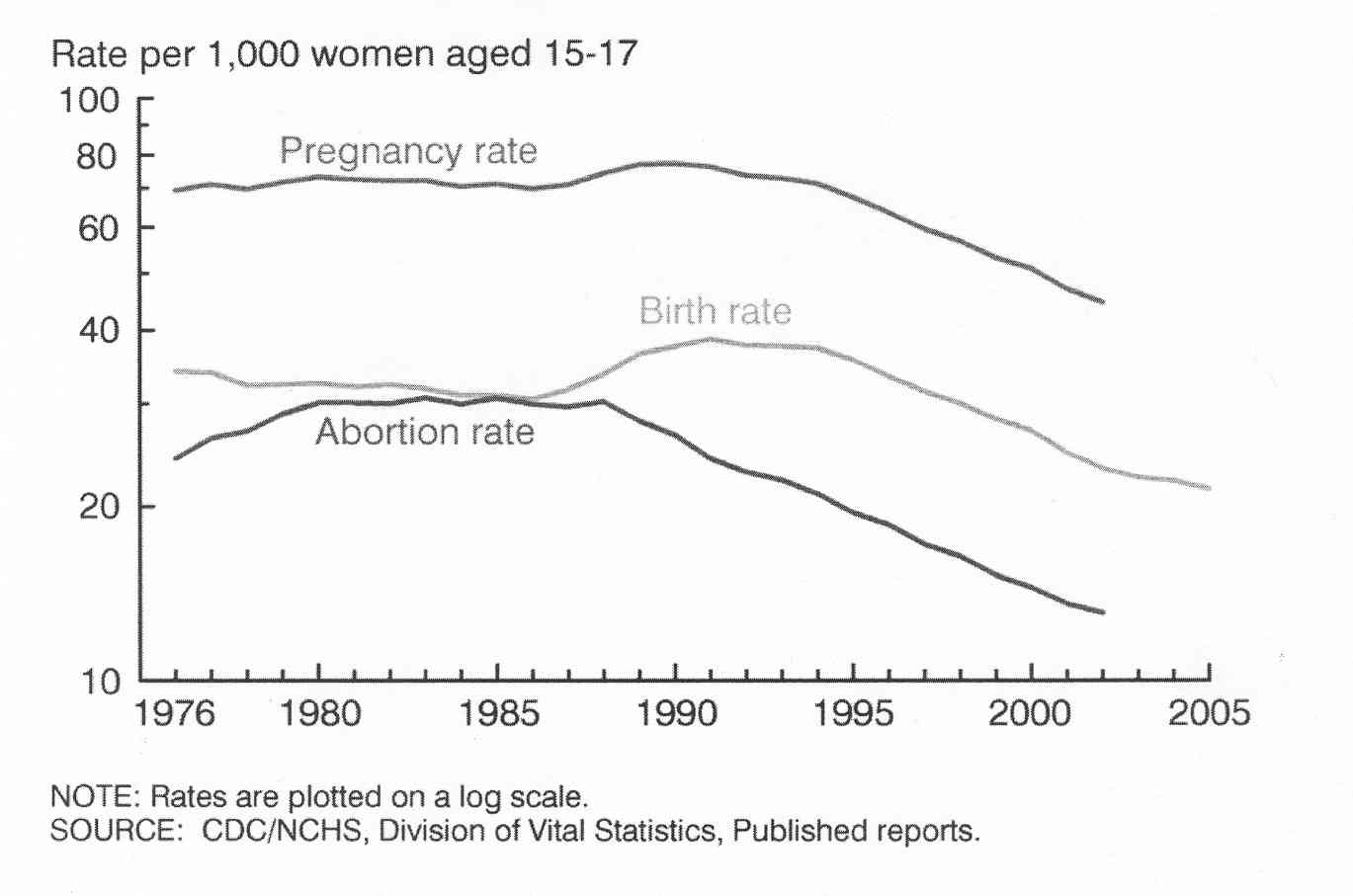
The United States continues to have one of the highest adolescent birth rates of all developed countries (Fig. 1). The following graphs show a steady decline in the pregnancy rate, birth rate, and abortion rate from an all time high in 1991 to a low noted in 2005. Rates are different for teenagers aged 15–17 and those slightly older teens aged 18–19 (Fig. 2).
Fig. 1. Adolescent birth rate in developed countries. (Singh S, Darroch J: Adolescent pregnancy and childbearing: levels and trends in developed countries. Fam Plan Perspect 32:14–23, 2000.)
{kind=link}
Fig. 2.
{kind=link}
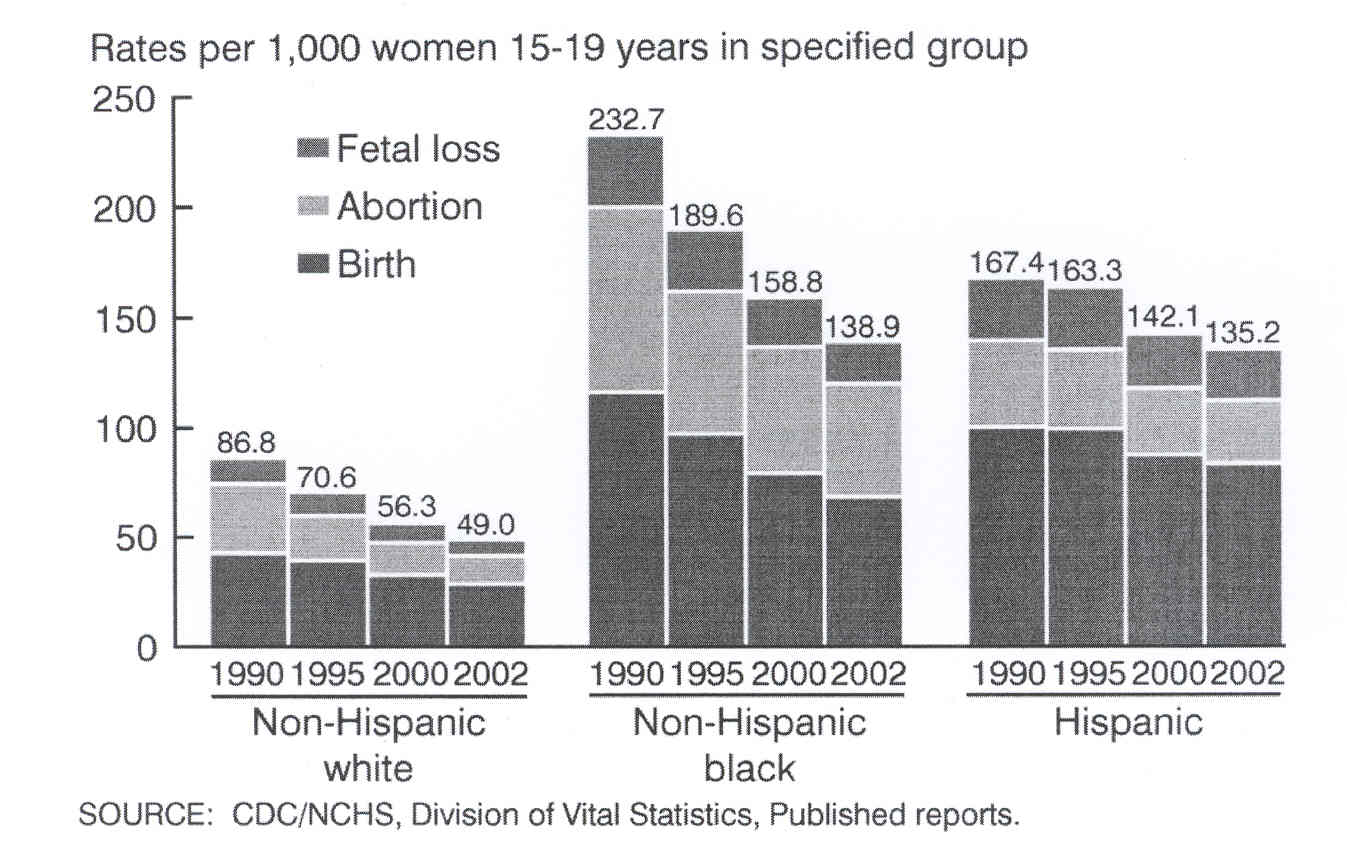
These graphs reveal a steady decline in the pregnancy, abortion and birth rates for adolescents, with more dramatic drops in teens aged 15–17 compared with their slightly older counterparts in the 18–19 year old age group. Most recent data reveal a slight rise in the birth rate between 2005 and 2006 but this is not represented in this graph.12 Pregnancy, birth and abortion and fetal loss rates vary by race, with non-Hispanic blacks having the highest rates, followed closely by Hispanic adolescents, and with non-Hispanic whites having the lowest rates (Fig. 3).
{kind=link}
Fig. 3.
Despite steady declines in adolescent pregnancy, adolescents in the United States continue to have much higher birth rates than those in other developed countries. The adolescent birth rate in several developed countries is depicted in Fig. 1.
REASONS ADOLESCENTS BECOME PREGNANT
It is well-documented that there are many negative consequences of adolescent childbearing, including lower educational attainment, poverty, limited career opportunities, lack of access to prenatal care, low birth weight/preterm delivery, family conflict, and depression.13 For years it has been assumed by the medical community that individual adolescents did not desire pregnancy, and that it was accidental when it did occur. Based on these assumptions, prevention programs focused efforts toward provision of contraception, anticipating that if adolescents did not desire pregnancy they would be motivated to use contraception. Many of these programs have had minimal impact, and this may be because at least some adolescents do not perceive pregnancy as an unwanted situation. New research is showing that many teens have mixed feelings about the possibility of pregnancy.14, 15 One must assess adolescent perceptions about adolescent pregnancy with a special focus on the role of ambivalence toward adolescent childbearing and the social factors influencing adolescents' feelings and choices.
Some adolescents do not use contraception because they are not motivated to prevent pregnancy; they either “want to become pregnant” or “do not care” if they become pregnant.13 Of pregnant teens in a racially and ethnically diverse sample, 17.5% stated that they wanted to get pregnant.16 A study of 584 girls in a urban high school in Los Angeles found that girls who perceived positive consequences associated with adolescent pregnancy were more likely to be Latina, non-United States natives, have low expected educational attainment, had low parental monitoring, had good communication with parents, and wished to have many children.13
Other girls desire pregnancy or are ambivalent about pregnancy if they think their male partner wants them to become pregnant.17 A study of 13–18 year olds in Minnesota documented the range of positive, negative, and ambivalent feelings girls have toward pregnancy and showed that perceived partner desire for pregnancy, limited future expectations, and lack of school engagement were significantly associated with positive pregnancy feelings.17 Interestingly, those who most wanted to avoid pregnancy were more likely to be using hormonal methods of birth control, and those who wanted or were ambivalent about pregnancy were more likely to use condoms or no method at all.
Parents have strong influence with regard to adolescent pregnancy. It is well-known that lack of parental involvement and lack of parental monitoring of adolescent activities are risk factors for adolescent pregnancy. A prospective study of minority adolescents showed that those who had low parental monitoring were 2.5-times more likely to become pregnant and have a documented pregnancy test at 6 month follow-up.18 Adolescents are less likely to initiate sexual activity and less likely to become pregnant if they perceive that their mothers disapprove of them having sexual intercourse, and if they were satisfied with their relationship with their mothers.19
Other factors contributing to adolescent pregnancy include developmentally normal factors such as the inability to think abstractly and plan ahead, adolescent feelings of invulnerability, and societal attitudes about sexuality that ascribe less blame to sexual activity when it occurs spontaneously without planning than when contraception and sexual activity are planned.
GIRLS AT GREATEST RISK FOR PREGNANCY
Adolescents who are having unprotected sexual intercourse or who are not using effective contraception are obviously at high risk for becoming pregnant. Much research and study has focused on identifying biological, psychological, and social characteristics of girls who are most likely to be at risk for adolescent pregnancy. Some of those risk factors and associations are listed (Table 1).
Table 1. Maternal characteristics associated with inconsistent contraceptive use and conception during adolescence16
| Sociodemographic |
| Young age |
| Non-white race and Hispanic ethnicity |
| Poverty and socioeconomic deprivation |
| Not living with parents: living alone, with friends, with boyfriends, or relatives other than parents |
| Being married |
| Being parous |
| Psychosocial characteristics |
| Dropping out of school |
| Inadequate family support |
| Depression |
| Longstanding romantic relationship |
| Older boyfriend |
| Substance use |
(Stevens-Simon C, Kelly L, Singer D, et al: Why pregnant adolescents say they did not use contraceptives prior to conception. J Adolesc Health 19(1):48–53; discussion 54–45, 1996.)
FATHERS
Much emphasis is placed on the demographic characteristics and behaviors of adolescent girls who become pregnant, but it is also important to understand who fathers these pregnancies. In one study, 12% of sexually active male high school students report having been involved in a pregnancy.20 However, not all boys involved in a pregnancy become fathers, because almost half of these pregnancies will end in either elective abortion or miscarriage. According to national surveys the prevalence of teen fatherhood ranges from 2–7%, with higher rates among inner city and minority youth.21 Male students involved in a pregnancy were found in one study to have the following characteristics: more likely to have been a victim of forced sexual contact, more likely to carry a weapon, carrying a weapon on school property, more likely to smoke more cigarettes, to have had more sexual partners in the previous 3 months, and less likely to use a condom at last intercourse20 (Fig. 4). Other characteristics of males who were involved in a pregnancy have included a greater likelihood of smoking tobacco, using alcohol and other drugs, being a member of a gang, and believing that “getting a girl pregnant proves that you are a man.”22 Certain childhood exposures are known to be associated with involvement in a teen pregnancy. Both boys and girls who have been abused have a greater number of lifetime sexual partners, earlier ages at first intercourse, and are more likely to be involved in an adolescent pregnancy.23 Male adolescent delinquents are more likely than nondelinquents to be involved in teen pregnancy.21 Adolescent fathers may be ill-equipped to parent effectively because of immaturity and lack of financial resources.21
Fig. 4. Characteristics of sexually active male students in Massachusetts. |
Adult men, aged 20 years and older, father more than one quarter of all pregnancies to adolescent girls.24 Adult fathers are responsible for 26.7% of births to adolescents younger than age 15, and, on average, are 8.8 years older than the young mothers, according to a large retrospective analysis of more than 12,000 very young mothers in California.24 These statistics raise the question of how many of these situations represented forced or coerced intercourse. The younger a sexually experienced adolescent is, the more likely she is to have experienced involuntary sex.21
CONTRACEPTION
Although an increasing percentage of adolescents are using condoms, the use of oral contraceptive pills is decreasing, thus placing many at higher risk for adolescent pregnancy. In a 2001 high school survey of sexually active teenagers, 58% reported using a condom at last intercourse, an increase from 46.2% in 1991; black adolescents were most likely to report condom use.
Birth control pill use is decreasing, with only 18.2% of students in traditional high schools (and only 14.1% of students in alternative high schools) reporting using birth control pills at last intercourse in 2001, a decrease from 20.8% one decade earlier.5 Birth control pill use varied by race, and white students (23.4%) were significantly more likely than Hispanic (9.6%) and black (7.9%) students to report birth control pill use.5 Figure 5 shows the trend of increasing oral contraceptive use and decreasing condom use with advancing grade.5 It has been suggested, however, that the use of longer-acting hormonal birth control methods are one reason that the adolescent pregnancy rates in the United States are decreasing.25 Table 2 shows sexual habits among adolescents by gender and race.
Fig. 5. Percent of sexually active students using condoms or birth control pills by grade. |
Table 2. Sexual Habits of Adolescents in 2001
| Ever had sex (%) | Condom | Pill | ≥4 partners (%) | Sex before age 13 | |
| Black male | 68.8 | 72.7 | 07.8 | 38.7 | 25.7 |
| Black female | 53.4 | 60.7 | 07.8 | 15.6 | 07.6 |
| White male | 45.1 | 63.8 | 19.3 | 12.8 | 06.2 |
| White female | 41.3 | 51.0 | 26.7 | 11.1 | 03.3 |
| Hispanic male | 53.0 | 59.1 | 08.7 | 20.6 | 11.4 |
| Hispanic female | 44.0 | 47.6 | 10.4 | 09.5 | 04.1 |
(Data from Grunbaum JA, Kann L, Kinchen SA, et al: Youth risk behavior surveillance—United States, 2001. MMWR Surveill Summ 51(4):1–62, 2002.)
Unfortunately, adolescents delay seeking medical contraceptive services by approximately 17 months after the onset of sexual activity.26 Adolescent girls are fertile; 50% of adolescents become pregnant within the first 6 months of sexual activity, well before the typical onset of medical contraceptive use.27 Unfortunately, younger adolescents are less likely to use effective contraception (hormonal methods) than older adolescents.
Compliance and correct daily use of medication is poor, even for adults with chronic and severe medical conditions;28 adolescents are particularly at risk for poor compliance with oral contraceptives. Typical failure rates of oral contraceptives among adolescents are between 9% and 18%.28 Continuation rates for adolescents' oral contraceptive use at the end of a year are low; more than one quarter of those who stop using the pills become pregnant in the next year. Logically, it is somewhat surprising that so many adolescents stop using oral contraceptives, given their multiple noncontraceptive benefits including decreased acne, predictable cycles, and less dysmenorrhea, among others. We know that those sexually active girls who use effective contraception are different from those who do not. They are typically older, are in more stable relationships, have higher academic achievement, and higher educational goals than teens who do not use contraception.11 These data suggest that for prevention programs to be successful, knowledge of sexuality and contraception must be taught before the high school years. Teens must actively desire to prevent conception, and positive alternatives to pregnancy need to be stressed to help motivate adolescents to avoid pregnancy. Helping adolescents postpone sexual involvement until they are developmentally capable of effectively using contraception will also result in lower pregnancy rates.
New dosing regimens and contraceptive delivery systems have become available, which may have a positive impact on compliance. The Quick Start method of beginning oral contraceptive pills has been studied in adolescents and has shown that instructing adolescents to start their pill pack the same day as their visit, regardless of where they are in the menstrual cycle, enhanced compliance at 3 months compared with beginning the pills with the onset of the next menstrual period.28 Long-acting drug delivery systems include the levonorgestrel intrauterine contraceptive system (Mirena IUS,) depot medroxyprogesterone acetate (Depo Provera) and Implanon, a 3 year progestin only rod system. Other recent advances in contraceptive hormone delivery systems which appeal to teens include birth control patches, and the vaginal ring. Patches may seem particularly appealing, especially to young teens, and data may ultimately show enhanced compliance in adolescents. Emergency contraception has become widely available, but its specific impact on adolescent pregnancy rates is not well known.
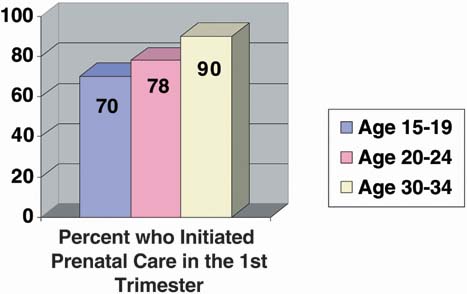
IMPACT OF PRENATAL CARE
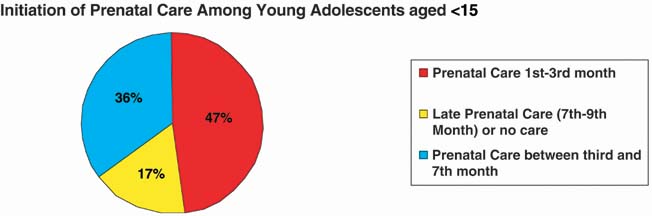
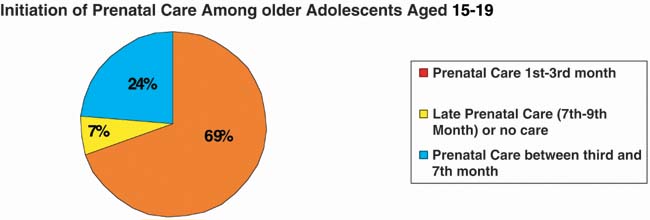
Younger pregnant adolescents are less likely to access prenatal care than older adolescents, and all adolescents are less likely to seek timely prenatal care than adults9 (Figs. 6, 7, 8). In 2001, only 48% of young adolescents (younger than age 15) began prenatal care in the first trimester, compared with 70% of girls aged 15–19. In this same year, 16.8% young adolescents had no prenatal care or entered the prenatal care system in the seventh to ninth month of their pregnancies, compared with 7% of older adolescents.9 The reasons for this are complex, including denial of the possibility of pregnancy, lack of familiarity with the health care system, fear of informing parents, fear of the pregnancy itself, adolescents' lack of awareness of both normal menstrual cyclicity and their own dates of menses, and embarrassment.29 While the available data conflict on what form of prenatal care is best for the adolescent patient, there is a clear indication that early prenatal care optimizes the outcome of adolescent pregnancies.30
{kind=link}
{kind=link}
{kind=link}
Medical risks known to be associated with teen pregnancy include higher rates of pregnancy induced hypertension (preeclampsia and eclampsia), low-birth-weight (LBW) infants, and higher rates of neonatal or infant death.31 Socioeconomic and behavioral factors are primarily responsible for the poor pregnancy and neonatal outcome associated with adolescent pregnancy. The exception to this low risk is the very young adolescent, for whom pregnancy-induced hypertension and nutritional status may be the primary reasons for poor pregnancy outcome.32 Other than preterm delivery secondary to pregnancy-induced hypertension, two of the most consistent factors associated with the occurrence of LBW infants and preterm delivery in the adolescent patient are poor prepregnancy nutritional status (as evidenced by a low body mass index) and lack of, or late onset of, prenatal care.32 An understanding of the factors that predispose adolescents to poor pregnancy and neonatal outcomes is essential for effective prevention strategies.
Adolescents have different needs from adult gravidas. The typical adolescent is not independent, either socially or financially. The care of the pregnant teen encompasses concerns regarding continued education, social support from family and the peer group, and the adolescent's ability to be able to provide emotional and financial support for the infant. All too frequently, teenage pregnancy is a marker for poverty, low socioeconomic status, low educational achievement, lack of goals for the future, and the developmentally normal need and desire of adolescents to express autonomy and individualism. While the prenatal care team must provide adequate medical care, nutrition counseling, and access to social support systems (such as the nutritional information and assistance offered by the Women, Infants, and Children [WIC] Program in the USA), the greatest challenge to the team is usually found in getting the adolescent to seek prenatal care. Once prenatal care has been initiated, the challenge is to provide a network of psychological and social support to help the adolescent avoid many of the adverse sequelae associated with teenage pregnancy. This is increasingly a challenge in today's medical climate in which comprehensive services with the availability of clinician, social workers, dietitians, and educational specialists are felt not to represent cost-effective care, as the improved outcomes resulting from these comprehensive services are difficult to measure and document.
PRENATAL CARE OPTIONS
In the United States, the health care delivery system has undergone rapid and significant change in the past two decades. Private offices and public clinics (often run by university hospitals) were once the mainstay of care options for teens, but large health maintenance offices (HMOs) now provide prenatal care to many of the nation's adolescents.33 In the past, most university-based programs include a team of health care workers to meet the special nutritional, social, psychological, and medical needs of the teenager. Studies attempting to show a difference in pregnancy outcome between adolescents receiving prenatal care in a traditional adult-focused university-based clinic setting versus a special teen pregnancy clinic have failed to show significant differences in the medical outcomes of these pregnancies.29, 34 However, the outcomes measured may not be sufficiently sensitive enough to show a difference for small numbers of patients.
The social and economic disadvantages of teen pregnancy are well-established, and evidence suggests that while special teen pregnancy clinics may not have a statistically significant difference in medical outcomes, significant impacts on social outcomes may occur. The teaching and support system specially geared toward the adolescent patient may have a positive impact on future pregnancy rates, completion of high school, economic achievement, and neonatal and childhood outcomes. Many experts on adolescent pregnancy feel that the adolescent patient (regardless of socioeconomic status) is best served in a specialized clinic setting where support from nutritionists, social workers, and prenatal educators is readily available. A team approach with awareness of the social, psychological, and biological developmental issues of adolescence is also a critical component of the care that is provided in these specialized clinics. These factors are not as easily reproducible in the average private physician's office, and specialized clinic settings are essential. There is some hope that HMOs are beginning to understand the potential value of adolescent centered pregnancy care, as evidenced by a major initiative at a Massachusetts staff model HMO, which is geared toward adolescent-friendly care with regard to confidentiality, contraceptive counseling, infection screening, and provision of postpartum birth control.35
Despite recent efforts by some, most HMOs still fall short of the comprehensive care provided by most university based clinics. For example, a study in Washington State scrutinized the provision of care provided to adolescents in both Medicaid HMO plans and the care provided in traditional nonprofit staff-model plans, and found that only 27% of sexually active girls were tested for Chlamydia, with lower rates of testing in those who spoke English as a second language.36
OBSTETRICAL CONCERNS
In the past, it was believed that the adolescent was too biologically immature to achieve and complete a successful, uncomplicated pregnancy. The very young adolescent, defined as within 2 years of menarche, was felt to be subfertile secondary to an immature hypothalamic-pituitary-gonadal axis and the resultant anovulatory cycles. In the United States, the average age of menarche is 12.8 for white and 12.2 for black girls.37 Contrary to traditional beliefs, teenagers initiating intercourse before age 15 years are twice as likely to conceive within the first 6 months of sexual activity as older teens.38 Ten percent of teenagers younger than age 15 years become pregnant within the first month of initiating sexual activity; 50% of pregnancies occur within the first 6 months of sexual activity.38 This increased risk is believed to be secondary to the low rate of contraceptive use during the first few months of sexual activity and lack of education regarding the times of increased fertility during the menstrual cycle.
In general, older studies described the adolescent pregnancy as a high-risk pregnancy with an increased risk for the development of pregnancy induced hypertension, preterm labor and delivery, LBW infants, cephalo-pelvic disproportion, operative vaginal delivery, cesarean delivery, and increased perinatal morbidity or mortality. Recent literature has begun to dispute these beliefs. By dividing adolescents into two age groups (typically 10–14 years and 15–19 years) and by parity, a disparity in pregnancy outcomes has been noted. According to the National Vital Statistics Report in 2001, the rate of LBW infants born to teenage mothers younger than 15 years of age was 13% compared with an incidence of 9% for mothers aged 15–19 years.9 A racial disparity was also noted in the national statistics. The LBW infant rate was much higher for black adolescent mothers (14% for ages 15–19) than white adolescents (8.4% for ages 15–19).
Satin and associates reviewed 16,512 births to girls aged 11–15, 16–19, and 20 and older.39 They found that first births to adolescent mothers ages 16 to 19 years had no increase medical complications of pregnancy when compared with primigravidas older than age 20. Specifically, there was no increase in prematurity, hypertensive complications, or neonatal morbidity. In fact, the cesarean rate for the 16–19 age group was lower than the rate for the older than 20 age group (14% versus 18%, respectively).39
However, significant differences in pregnancy complications and outcomes were found in adolescents younger than 15 years. There was an increased risk of preterm delivery in teenage mothers younger than age 15. The percent of LBW infants (less than 2500 g) was also found to be significantly increased when compared with older adolescents and women older than age 20: 14% versus 10% versus 9%, respectively.39
Fraser and colleagues reviewed the outcomes of first pregnancies occurring in white middle-class mothers aged 13–24.40 Their findings confirmed the influence of socio-demographic factors on reproductive outcome. Inadequate prenatal care was associated with increased preterm delivery rates. They also found an increased risk for preterm and LBW babies in the youngest gravidas, even in those with the most favorable socioeconomic background, suggesting that adequate prenatal care and improvement in socioeconomic factors do not totally eliminate the medical risks of adolescent pregnancy in the youngest age group.40
Increased risk for adolescents, particularly young adolescents, has been demonstrated in a recently published retrospective chart review of 25,000 deliveries, which included 2930 young adolescents, 11,788 mature adolescents, and 11,830 controls older than age 2032 (Fig. 9). This study not only documented that pregnant adolescents were more likely to be black, diagnosed with a sexually transmitted disease, and reside with people other than their parents than were older pregnant women but also showed that risks for poor obstetric outcome differed by age of the adolescent. The risk of preeclampsia, eclampsia, preterm delivery, LBW, and very LBW was greater in the very young adolescent, while the mature adolescent was only at increased risk of eclampsia. All adolescents were less likely to have a cesarean section or an operative vaginal delivery than were older women. Other studies have also documented a lower cesarean section rate in adolescents.41 It is unclear why very young adolescents should have a lower cesarean rate.
Fig. 9. Risk of adverse pregnancy outcomes by age of adolescent. (Eure C, Lindsay M, Graves W: Risk of adverse pregnancy outcomes in young adolescent parturients in an inner-city hospital. Am J Obstet Gynecol 186:918–920, 2002.) |
Similar outcomes have been observed in earlier studies by Scholl and associates42 and Stevens-Simon.43 Scholl and associates reviewed pregnancy and fetal outcomes in adolescents by age and parity. The preterm birth rate for the young primigravida (within 3 years of menarche) was 21%, compared with 14.7% for the older adolescent primigravida.42 A decrease in the preterm birth rate by 21% was found for every year the pregnancy occurred beyond menarche.42
While the mature gravid patient will generally have an increase in birth weight in subsequent pregnancies, the young adolescent multipara with a previous history of a LBW infant has a 44% risk of delivering another LBW infant, compared with a 9.6% risk in the older adolescent multipara with a previous LBW infant.42 For the young multipara younger than age 15 years, the adverse outcome with the greatest frequency was that of delivering a LBW infant, not prematurity. Young multiparas had a two-fold increased risk of LBW infants compared with the multiparas older than age 16 years: 12.29% versus 8.51%.42 Poor prepregnancy nutritional state appears to be the main associated finding in the young multipara with a resultant LBW infant. Scholl and associates also noted that for multiparas younger than age 15 with a previous preterm delivery, the risk for another preterm delivery was 37%, compared with 8% for the older multipara with the same history. These data suggest that poor prepregnancy nutrition and continued maternal growth may have a substantial impact on fetal growth and length of gestation in the adolescent gravida.38 Other maternal characteristics that placed the pregnant adolescent patient at risk for a preterm delivery were conception within 3 years of menarche, a low body mass index, a past history of physical or sexual abuse, a socially deviant father of the baby, and vaginal bleeding during the first 8 weeks of gestation.43
From these studies, it appears that the adolescent patient can expect a positive obstetrical outcome. No increase in adverse obstetrical or perinatal outcome has been demonstrated in the adolescent patient older than age 15 years. Some studies suggest that the young adolescent (younger than 15 years or within 3 years of menarche) is at an increased risk for LBW infants and preterm delivery. However, this may be related to multiparity and poor prepregnancy nutrition, rather than to age alone.
Nutrition
Nutrition is one of the most important factors affecting pregnancy outcome for any woman; prepregnancy weight and poor weight gain during pregnancy are the two main factors linked with LBW infants. Teenagers, in general, have lower nutritional reserves than their adult counterparts, secondary to their own bodies' continued increased metabolic demands for growth and their poor diets. Adolescents most likely to become pregnant are often those who have inadequate nutritional status and lower socio-economic background.
The physical growth spurt may start as early as 10 years of age, with an average age of onset of 12.5 years of age. Menarche typically occurs toward the end of the linear growth spurt. While growth slows after menarche, it continues for several more years.44 The reproductive organs and other body tissues also continue to grow for several years after menarche.45 Pregnant adolescents continue to grow; however, their growth rate may be slower than nonpregnant adolescents at the same developmental age.44 Because measurements of linear bone growth are obscured because of increased lordosis during pregnancy, knee height measurements have been used in pregnant adolescents and have shown that approximately half of adolescents continue to get taller during pregnancy.46 What impact this continued growth and its metabolic demands have on pregnancy outcome is still controversial. Adolescents within 3 years of menarche tend to have lower total weight gains during pregnancy than do older women.
Obesity has reached an all time high in the United States, and excessive weight gain in adolescent pregnancy may lead to a greater risk of obesity after pregnancy. One study showed that excessive weight gain in adolescents and young adults who have normal prepregnancy body mass indices is associated with neither maternal growth nor duration of gestation, but rather with retention of postpartum weight and triceps skin-fold measures.
Age is felt to be a less important factor in gestational weight gain than prepregnancy body mass index (body mass index = weight ÷ height squared). The Institute of Medicine's recommendations for gestational weight gain in adolescents were originally published in 1990 and were reviewed in 1997. The comment was made that although new studies are necessary, no change in recommendations was required.38 Recommendations for weight gain by BMI are shown in Table 3. It is recommended that an adolescent with a low body mass index gain amounts at the upper end of the range. Early inadequate weight gain in the adolescent pregnancy may increase the risk for poor pregnancy outcome. A weight gain of less than 4.3 kg by 24 weeks has been associated with a significant increase in LBW infants.47 Late pregnancy weight gains of less than 0.4 kg/wk were found to be associated with an increased rate of preterm delivery.47, 48
Table 3. Recommended total weight gain ranges for pregnant women* by prepregnancy body mass index†
| Recommended Total Gain | ||
| Weight-for-Height Category | kg | lb |
| Low (BMI <19.8) | 12.5–18 | 28–40 |
| Normal (BMI of 19.8–26.0) | 11.5–16 | 25–35 |
| High‡(BMI>26.0–29.0) | 7–11.5 | 15–25 |
*Young adolescents and black women should strive for gains at the upper end of the recommended range. Short women (<157 cm, or 62 in) should strive for gains at the lower end of the range.
†BMI is calculated using metric units.
‡The recommended target weight gain for obese women >29.0) is at least 6.0 kg (15 lb).
(Nutrition During Pregnancy. © 1990, National Academy Press.)
The nutritional requirements for pregnant teenagers are not fully understood. Typically, the requirements for pregnant adults are added to the nutritional requirements for nonpregnant adolescents to provide an estimate for the pregnant adolescent's daily nutritional needs. Because of the very young adolescent's continued growth demands, the daily nutritional requirements are usually placed at the upper limit of the range. The average energy cost for a full-term pregnancy is estimated at 300 kcal/day in a woman gaining 27.8 pounds (12.5 kg) and delivering a 7.8-pound (3.4-kg) infant. Very young adolescents are encouraged to consume an additional 200 kcal/day for a total of 500 kcal/day.49
Twenty-five percent of all pregnant teenagers have diets deficient in calcium, protein, vitamins, and iron.48 The 2001 Youth Risk Behavior Survey indicated that 84% of high school students drink fewer than three glasses of milk per day,5 which is less than the daily recommended intake of calcium for pregnant adolescents (1,300 mg.)46 Most prenatal vitamin preparations provide only 300 mg of calcium. Protein should provide 15% of the total energy needs. The additional amount of protein needed during pregnancy is based on the amount of protein deposited in new tissues, plus the efficiency of conversion of dietary protein to tissue protein. Protein needs follow the pattern of fetal growth needs, increasing in the late gestation. Currently, it is recommended that pregnant adolescents maintain a daily protein intake of 60 g per day.48 This is usually met by increasing the amount of whole grains, milk, and meat from prepregnancy diet.
Adequate intake of vitamins and minerals is essential to a healthy pregnancy; folate and iron are particularly important. Folate supplementation both before and during pregnancy is known to decrease the risk of neural tube defects, and the recommended daily supplement is 0.4 mg of folate or a daily intake of 0.6 mg.46 Because more than 50% of pregnant women in developing countries have iron-deficient anemia, adequate iron intake before and during pregnancy is essential. Physiologic iron requirements are three-times higher in pregnancy than they are in menstruating women, and that need is most significant during the second and third trimester when requirements reach between 4–6 mg per day.50 During late pregnancy, most women have exhausted their iron stores and rely on absorption of iron from their diet or from supplements. Women who conceive during or soon after adolescence are even more likely than their adult counterparts to enter pregnancy with low or even absent iron stores.50 Iron deficiency during pregnancy is known to be associated with premature delivery, LBW and increased perinatal mortality. In addition, infants born to iron-deficient mothers have a higher prevalence of anemia in the first 6 months of life.50
Adolescents who become pregnant are often in lower socioeconomic groups, have poor baseline nutrition, and are not very knowledgeable about nutrition. One study compared pregnant women who were eligible for the Special Supplemental Nutrition Program of WIC but who were not participating in the program with those who were participating. Results showed that the longer a woman participated in WIC, the heavier her baby was likely to be at birth. In addition, those who entered prenatal care and received WIC support before 12 weeks of gestation were 25% less likely to deliver a small-for-gestation baby.46
Risk-Taking During Pregnancy
Adolescents are still maturing, emotionally and cognitively, and their immaturity often results in risk-taking behaviors that have serious consequences, especially during pregnancy. For an adolescent, social acceptance gained by smoking, for example, may be considered a benefit that outweighs the risk of poor pregnancy outcome. This is related in part to the fact that young adolescents are typically concrete in their thinking and not developmentally able to appreciate the future consequences of their current actions. Decisions about health and risky behaviors are more strongly associated with an adolescent's perception of the current benefits of certain choices (such as choosing to drink, smoke, not using seatbelts) than influenced by knowledge or understanding of the risks associated with those behaviors.51
Substance Use
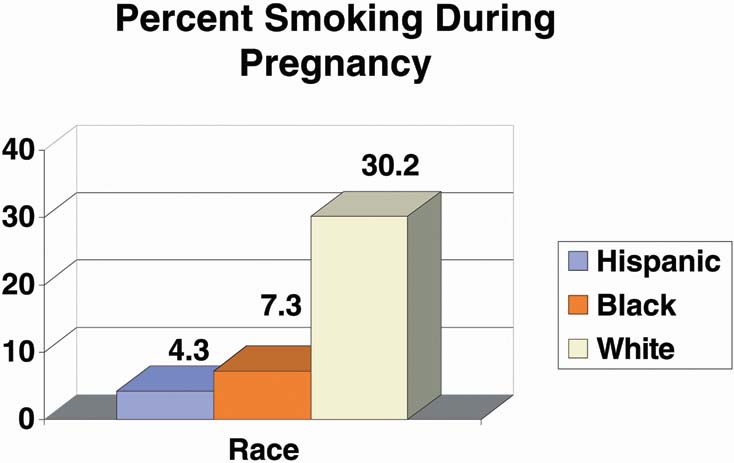
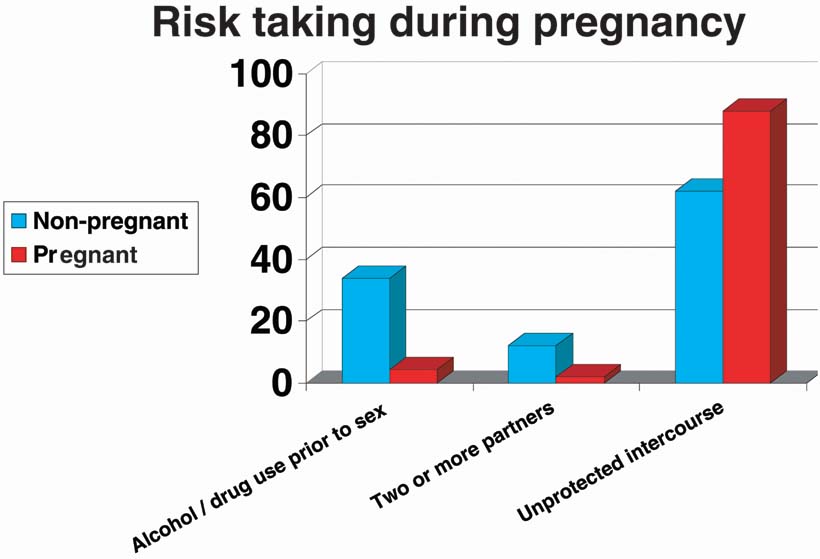
National data suggest that more than 17% of pregnant adolescents between the ages of 15 and 19 smoke cigarettes.51 Smoking varies by race, with more than 30% of non-Hispanic white girls reporting smoking during pregnancy52 (Fig. 10). Estimates of alcohol use by pregnant teens range between 17% and 54%, and a significant number of pregnant adolescents do not abstain from alcohol even after recognizing that they are pregnant, particularly if their partners use alcohol.51 Interestingly, in a 2003 study by Niccolai and associates, only 4.5% of pregnant adolescents reported using alcohol or drugs before sex, compared with 34% of matched nonpregnant controls53 (Fig. 11).
{kind=link}
{kind=link}
Sexually Transmitted Disease: Adolescents and Pregnant Adolescents
Nearly four million adolescents are infected with sexually transmitted diseases (STDs) each year, and 25% of the 12 million new sexually transmitted infections occur in the adolescent population.52 A variety of diseases exist today that can be transmitted sexually. Chlamydia trachomatis, Neisseria gonorrhea, genital herpes, hepatitis B, syphilis, HIV, the human papilloma virus (HPV), and trichomoniasis are the most common. Our knowledge of the rates of Chlamydia infection has been enhanced by three main factors: (1) Chlamydia is now a reportable infection in all 50 of the United States; (2) Chlamydia can be found with voided urine or cervical specimens; and (3) the DNA amplification tests have higher sensitivity than older tests. In 2001, the CDC reported that females aged 15–19 had the highest rates of Chlamydia infection compared with all other groups, with an infection rate of 2536.1 per 100,000 girls in the population. It is estimated that one of every 10 sexually active girls has Chlamydia.52 The prevalence of HPV infection in sexually active adolescents varies depending on the population studied but appears to be 30–50%.54, 55, 56 In 2001, 1155 new cases of HIV were reported among adolescents aged 13–19, with three-times that number reported among women aged 20–24. Because the average time between infection with HIV and the onset of AIDS symptoms is 10 years, most of the new cases of AIDS in the 20–29 age group were contracted during the teen years. More than 50% of adolescents with new diagnoses of HIV contracted it through heterosexual contact.57 This, combined with the knowledge that 10–25% of teenage girls have had more than four sex partners, makes it imperative that clinicians who see adolescents be comfortable and knowledgeable about sexually transmitted diseases to diagnose, treat, and counsel the adolescent patient regarding high-risk sexual behaviors.
Sexually transmitted infections are even more common among pregnant adolescents than nonpregnant sexually active girls, with one recent study from an inner-city clinic reporting that 19% had Chlamydia and 3.5% had gonorrhea during pregnancy.53 Pregnancy represents a risk marker for unprotected sexual activity. Chlamydia and gonorrhea rates vary dramatically by region, and it is essential to screen adolescents during pregnancy, both at initiation of care and later in gestation to evaluate for re-infection. Adolescents are much less likely to use condoms once they know they are pregnant, with 87% of pregnant adolescents reporting unprotected intercourse within the last 30 days, compared with 62% of matched nonpregnant controls.53
Although rates of HIV infection are relatively low among adolescents, those who become pregnant may be at higher risk than other teens. Pregnancy is an excellent time to screen adolescents for HIV and provide education about HIV transmission. In addition, babies who were infected at birth are now reaching reproductive age. HIV screening is recommended by the American College of Obstetrics and Gynecology (ACOG) for all pregnant women at initiation of care.
Prenatal care for adolescents is also an excellent opportunity to provide preventative care and guidance. Pregnant adolescents are at high risk for other STDs, and therefore should also be screened for Chlamydia, gonorrhea, HIV, and syphilis during pregnancy and should be encouraged to have the hepatitis B vaccine if nonimmune. Although a Pap test has been a routine part of prenatal care, current guidelines for screening recommend that screening be initiated approximately 3 years after first vaginal intercourse; thus, cervical cytology screening may not be indicated for some adolescents who are currently being screened routinely.58 Because we know adolescents are less likely to use condoms while pregnant, condom use for STD prevention should be encouraged.
Violence Before, During, and after Pregnancy
Many pregnant girls have been victims of physical or sexual abuse before pregnancy, and this strong association has been well-documented in the literature. The rate of abuse reported by adolescents has ranged from 26–31.6%.59 Adolescent girls may be especially vulnerable to abuse because of lower self-esteem and greater adherence to dependent female gender roles. A significant number of pregnant girls are abused by their male partners; others are victims of continuing physical abuse from parents or guardians. Twelve percent of adolescents of diverse ethnic background reported intimate partner violence during pregnancy, and even higher rates postpartum, according to a 2002 study60 (Fig. 12). In one study reporting prospective abuse screening, 28% percent of teens versus 23% of adult gravidas reported abuse before the pregnancy.59 Fifty percent of the patients reporting a history of abuse during the year before pregnancy would go on to experience further abuse during pregnancy, making a previous history of abuse the number one risk factor for abuse during pregnancy. The rate of abuse during pregnancy was 20.6% for teens and 14.2% for adults. While the rate of abuse was higher for teens, the intensity of abuse was greater in the adult gravidas. The association between abuse and late onset of prenatal care was demonstrated in this study. Of abused teens, 21.9% entered prenatal care in the third trimester compared with 7.5% of nonabused teens. While abuse during pregnancy was found to be a significant risk factor for delivering a LBW infant, it was a more significant associated risk factor for the adult women than for the teens. Abused teens were found to have a significantly greater risk for poor weight gain, first or second trimester bleeding, smoking, alcohol, and illicit drug use.59
Fig. 12. Intimate partner violence. (Harrykissoon S, Rickert V, Wiemann C: Prevalence and patterns of intimate partner violence among adolescent mothers during the postpartum period. Arch Pediatr Adolesc Med 156:325–330, 2002.) |
Pregnancy provides one of the few times adolescents may be motivated to seek health care. Clinicians thus have a unique opportunity to offer intervention and assistance to the abused adolescent patient, perhaps breaking the cycle of abuse and preventing the escalating intensity of abuse that occurs for one out of five adolescents as they become adults.59
IMPACT OF ADOLESCENT PREGNANCY ON EDUCATIONAL ATTAINMENT
Adolescent pregnancy is known to adversely affect the educational, occupational, and marital status achieved by these young women. Educational attainment among pregnant adolescents varies by region and is likely affected by socio-demographic characteristics. A recent study of pregnant adolescents from a racially mixed sample in Baltimore reported that 70% were enrolled in school or had already graduated, and 79% perceived finishing high school as very important.61 Unfortunately, there is a discrepancy between the number of childbearing adolescents who say they want to continue their education and those who actually do so.61 Ultimately, only 50% of adolescent mothers complete high school, compared with 97% of women who delay childbearing until their 20s.62 The resulting loss of education results in poorer achievement in the job market, resulting in a socioeconomic disadvantage for these young women and their children, which can lead to inadequate nutrition, medical care, and poverty. Adolescent mothers who fail to complete high school within 5 years after birth of their first child have twice the risk of welfare dependence two decades later.63 Frequently, educational failure and withdrawal from school antedate adolescent pregnancy and may be seen as a marker for poorer educational achievement after pregnancy. Academic achievement and future aspirations before pregnancy are among the best predictors of adolescent gravidas' completion of high school after delivery.27
THE ADOLESCENT MULTIPARA
Adolescent mothers are at extremely high risk for repeated pregnancy while still in adolescence. Because the adolescent multipara is at increased risk for delivering a LBW infant compared with her adult counterpart, and because many adolescent mothers are already economically disadvantaged or have social stress, it is essential to target these girls for pregnancy prevention. Age at first birth, shorter pregnancy intervals, unmarried status, and cultural factors influence risk of subsequent pregnancy. One study showed that without intervention, 25% of adolescents mothers will become pregnant again during the first, and 40% during the second, postpartum year.63 In one study, 67% percent of these multiparas did not finish high school.30 The researchers found that adolescents having a second or higher-order pregnancy sought prenatal care later, had fewer prenatal visits, had poorer compliance with postpartum care, and were at higher risk for dropping out of the educational system. Of teens not using contraception consistently during the postpartum period, side effects, plans to abstain from sexual intercourse, and a lack of motivation to postpone additional childbearing were noted as the reasons they did not use contraception consistently.64 These data are a reminder that aggressive intervention is needed during the first teen pregnancy to reduce second and subsequent pregnancies.
NEONATAL AND CHILDHOOD SEQUELAE
Infants born to mothers younger than age 16 are nearly three times as likely to die within the first 28 days of life as are infants born to older mothers, and are twice as likely to die in the postneonatal period.27 The increased risk of neonatal and postneonatal death was thought to be secondary to LBW and prematurity, but a recent study examined the risk of death for infants born healthy and full term to adolescent mothers. In the postneonatal period, the mortality rate was doubled for infants born to mothers aged 18–20, was 2.5 times greater for infants of mothers aged 16–17, and tripled for mothers younger than age 15, when compared with women aged 23–29.65 Sudden infant death syndrome (SIDS) is more common in infants of adolescent mothers.65 Environmental factors such as poverty, poor health habits (such as smoking), inappropriate childrearing practices, and lack of knowledge regarding child development and supervision appear to be associated factors.
Children of adolescent mothers also appear to exhibit more behavioral problems, score lower on intellectual tests, and more often have to repeat grades than children of similar socioeconomic status born to older mothers.63 One important factor may be that young mothers themselves are more likely to score below the mean on cognitive ability tests and are often, for socioeconomic reasons, less able to provide intellectual stimuli to their young children.66 Adult offspring of adolescent mothers are more likely to become school dropouts, unemployed, adolescent parents, and violent offenders, according to a recent 20-year longitudinal study.67
NEW SOURCES OF INFORMATION FOR ADOLESCENTS
In the past, adolescents relied on parents, friends, books, and school-based sexual education for information regarding, sex, contraception, sexually transmitted infections, and pregnancy. Today, adolescents have additional sources of information via the World Wide Web. Adolescents of all socioeconomic groups can, and do, access the Internet. A web browsers search on the topic teen pregnancy will link an adolescent with web sites from a variety of sources, with a multitude of messages. Some sites are misleading and offer an online pregnancy test, while others offer expert advice from adolescent parents. Many sites are against the choice of abortion and encourage viewers to continue pregnancy. Although the messages and information available to adolescents is variable, many sites do offer valid and valuable information regarding nutrition, birth control, the risks of smoking during pregnancy, prenatal care options, parenting, and more. How well adolescents will filter the information on the Internet and how well they can differentiate the high-quality sites from those with misleading messages is unknown. Clinicians may be able to encourage adolescents to access accurate information by providing specific web addresses to medically accurate sites for teens, or by providing their own web sites tailored to local needs and concerns.
SOCIOECONOMIC IMPACT OF ADOLESCENT PREGNANCY
Teenage mothers are much less likely to finish high school than mothers delaying childbearing until their 20s.11 They are also less educated than older mothers, and thus are less likely to be employed.11 They are more likely to live in poverty, receive public assistance, and have long periods of welfare dependency.52 The daughters of adolescent mothers are 83% more likely to become adolescent parents;68 the sisters of adolescent mothers are more likely to become adolescent mothers; and the sons of adolescent mothers are more likely to be incarcerated.52 Children of young adolescent mothers are at increased risk of abandonment, abuse, and neglect.69
The medical and social ramifications of adolescent pregnancy create an economic burden on parents and society. The Robin Hood Foundation published a report in 1996 outlining the economic and social impact of teen pregnancy in which they reported that adolescent childbearing itself costs taxpayers approximately $6.9 billion per year. In addition, public-assistance benefits, welfare, and food stamps add an additional $2.2 billion per year, and related medical expenses cost $1.5 billion. Taxpayers would save $13–19 billion per year annually if adolescent childbearing were to be delayed by 2–4 years.70 An adolescent advocacy group, Advocates for Youth, reports that the economic impact of adolescent childbearing is even greater than has been noted and should include estimates of expenses incurred by adult females who were teenagers when they had their first child. They estimate that the federal government spent $38 billion in 1996 in services and support for those families which began with a birth to a teen, but spent only $138.1 million on prevention programs.71
PREGNANCY PREVENTION
Because of the negative impact of early sexual involvement and adolescent pregnancy, schools, religious groups, youth organizations, and health care professionals in the United States have developed programs to decrease the incidence of adolescent pregnancy.72 Although a variety of strategies has been developed by many different agencies with the goals of decreasing STDs, early intercourse, and the number of adolescents who become pregnant, few have been rigorously studied to assess effectiveness.68 Many programs have never been evaluated for effectiveness, or have not been studied with high academic standards because of limitations on funding, small numbers of subjects, or poor study design. Others have been fairly well studied and seem to be beneficial, or show no change in adolescent pregnancy rates. Evaluation of pregnancy prevention programs is difficult because typically, the number of subjects is relatively small, programs use a wide a wide variety of approaches to prevention, and programs seemingly effective for one population may reflect socio-demographic variation of risk and thus may not be applicable to other populations.
Despite the wide variety of programs developed, most use one of five basic approaches: (1) educational programs for children and adolescents; (2) programs to improve access to contraception; (3) programs geared toward educating parents and family members; (4) multicomponent programs; and (5) youth development programs.68 Some of these programs receive government funds and meet criteria for abstinence-only education, while others provide a more comprehensive approach and include instruction not only on abstinence but also on contraception, sexuality, sexually transmitted infection prevention, and youth development (abstinence-plus programs).73
School-based education is one of the most prevalent methods for providing sexuality education and information on pregnancy prevention. Although schools are providing information on STD prevention, HIV, abstinence, and condom use to students in lower grades than they were a decade ago, the instruction is less likely to provide information on birth control, abortion, sexual orientation, and information on how to obtain contraceptive and STD services. Abstinence-only education is gaining popularity: in 1988, abstinence-only curricula were taught by only 2% of sexuality education teachers, compared with 23% of teachers in 1999. This change likely reflects the effect of Title V of the social Security Act, which was adopted by the federal government in 1996 and which provides access to federal dollars for abstinence only programs which meet strict criteria.74, 75 (Table 4).
Table 4. Federal criteria for abstinence-only education74, 75
| Has as its exclusive purpose teaching the social, psychological, and health gains to be realized by abstaining from sexual activity |
| Teaches abstinence from sexual activity outside of marriage as the expected standard for all school-age children |
| Teaches that abstinence from sexual activity is the only certain way to avoid out-of-wedlock pregnancy, sexually transmitted diseases, and other associated health problems |
| Teaches that a mutually faithful monogamous relationship in the context of marriage is the expected standard of sexual activity |
| Teaches that sexual activity outside the context of marriage is likely to have harmful psychological and physical side effects |
| Teaches that bearing children out-of-wedlock is likely to have harmful consequences for the child, the child's parents, and society |
| Teaches young people how to reject sexual advances and how alcohol and drug use increase vulnerability to sexual advances |
| Teaches the importance of attaining self-sufficiency before engaging in sexual activity. |
Information available from: Advocates for Youth, 8 Point definition of abstinence-only education as defined by section 510(b) of Title V of the Social Security Act, P.L. 104–193 [Web Page]. Available at: http://www.advocatesforyouth.org/abstinenceonly.htm. (accessed June 2003) and Allan Guttmacher Institute: Fueled by campaign promises, drive intensifies to boost abstinence only-until-marriage programs. The Guttmacher Report on Public Policy. 3, 2000.
Although abstinence-only sexuality education has been funded by the federal government for more than 20 years,76 it has been minimally studied, and the research that has been conducted shows no scientific evidence that abstinence-only programs are effective in changing sexual behaviors.77 Programs that promote abstinence and also incorporate sexuality education and information about contraception, STDs, and preventative health care have been shown to delay the onset of sexual activity and to increase the use of contraceptives in adolescents.78
One comprehensive program, “Reducing the Risk,” is a high school level sexuality education curriculum designed to prepare teenagers to manage situations that can lead to unwanted pregnancy and uses social learning theory, social inoculation theory, and cognitive behavior theory.72, 79 Evaluation of this program showed that participants were significantly less likely to initiate sexual intercourse, more likely to use condoms and other contraceptives if they were sexually inexperienced at the onset of the program but became sexually active during the study, and more likely to communicate with parents about birth control and STD prevention than the control group. Similar results have been found for participants in the Postponing Sexual Involvement (PSI) program, a national sexuality education initiative.72 Comprehensive age-appropriate sexuality education for kindergarten through 12th grade has been endorsed by the ACOG. A statement from ACOG also endorses access to effective contraception as a foundation for effective adolescent pregnancy prevention programs.72 The American Academy of Pediatrics (AAP) has also issued the statement that “children and adolescents need accurate and comprehensive education about sexuality to practice healthy sexual behavior as adults.”80
CONCLUSION
Adolescent pregnancy continues to be a major social concern. Except for the very young adolescent, age in and of itself does not appear to be a major factor in the myriad of medical and obstetric complications previously ascribed to the teen pregnancy. The social and economic impact of teen pregnancy is great, not only for the adolescent but also for society. It is apparent from recent data that by encouraging and providing adolescents with adequate prenatal care, most will have a positive obstetric course. Greater emphasis is needed on providing adolescents with the skills to postpone sexual activity until they are able to practice responsible sexual behavior.
The problem of adolescent pregnancy needs to be addressed with a multifaceted approach. Not only do adolescents need comprehensive sexuality education that encourages them to remain abstinent and provides instruction on appropriate use of birth control but they also need ready access to affordable contraception. In addition, education regarding the negative consequences of adolescent parenthood, encouragement to practice healthy behaviors, and help finding emotional support are also essential. Through a multidimensional approach to adolescent-centered preventative health, adolescents may develop the knowledge, behaviors, and self-esteem that will allow them to be motivated to prevent pregnancy through abstinence or responsible sexual behavior.
REFERENCES
Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2006. National vital statistics reports; vol 56 no 7. Hyattsville, MD: National Center for Health Statistics. 2007. |
|
Singh S, Darroch J: Adolescent pregnancy and childbearing: levels and trends in developed countries. Fam Plan Perspect. 32:14-23, 2000 |
|
Youth Risk Behavior Surveillance - United States 2007. HTTP://apps.nccd.cdc.gov/yrbss |
|
Jones EF, Forrest JD, Goldman N et al: Teenage pregnancy in developed countries: Determinants and policy implications. Fam Plann Perspect 17:53-63, 1985 |
|
Grunbaum JA, Kann L, Kinchen SA et al: Youth risk behavior surveillance–United States, 2001. MMWR Surveill Summ 51:1-62, 2002 |
|
Blum RW, Rinehart PM: Reducing the Risk: Connections that make a difference in the lives of youth 1-40, 1998 |
|
Abma JC, Chandra A, Mosher WD et al: Fertility, family planning, and women's health: new data from the 1995 National Survey of Family Growth. Vital Health Stat 23 5/1997. 19:1-114, 1997 |
|
Ventura SJ, Mosher WD, Curtin SC et al: Trends in pregnancy rates for the United States, 1976-97: an update. Natl Vital Stati Rep 49:1-9, 2001 |
|
Maritin JA, Park MM, Sutton P: Births: Preliminary Data for 2001. Natl Vital Stat Rep 50:(10): 2002 |
|
Henshaw S: U.S. teenage pregnancy statictics: with comparative statistics for women aged 20–24. The Alan Guttmacheer Institute, 2001 |
|
McLaughlin SD: Do Adolescents Who Relinquish Their Children Fare Better or Worse Than Those Who Raise Them? Fam Plann Perspect 20:25, 1988 |
|
Recent Trends in Teenage Pregnancy in the United States, 1990-2002 by Stephanie J. Ventura, M.A.; Joyce C. Abma, Ph.D.; William D. Mosher, Ph.D., Division of Vital Statistics; and Stanley K. Henshaw, Ph.D., The Guttmacher Institute |
|
Unger J, Molina G, Teran L: Perceived consequences of teenage childbearing among adolescent girls in an urban sample. J Adolesc Health 26:205-212, 2000 |
|
Farrow A, Hull MG, Northstone K et al: Prolonged use of oral contraception before a planned pregnancy is associated with a decreased risk of delayed conception. Hum Reprod 17:2754-2761, 2002 |
|
Cowley C, Farley T: Adolescent girl's attitudes toward pregnancy. J Fam Pract 50:603, 2001 |
|
Stevens-Simon C, Kelly L, Singer D et al: Why pregnant adolescents say they did not use contraceptives prior to conception. J Adolesc Health 19:48-64, 1996 |
|
Hellerstedt W, Fee R, McNeely C et al: Pregnancy feelings among adolescents awaiting pregnancy test results. Public Health Rep 116:(S1):180-193, 2001 |
|
Crosby R, Di CR, Wingood G et al: Low parental monitoring predicts subsequent pregnancy among African-American adolescent females. J Pediatr Adolesc Gynecol 15:43-46, 2002 |
|
Dittus P, Jaccard J: Adolescents' perceptions of maternal disapproval of sex: relationship to sexual outcomes. J Adolesc Health 26:268-278, 2000 |
|
Pierre N, Shrier LA, Emans SJ et al: Adolescent males involved in pregnancy: associations of forced sexual contact and risk behaviors. J Adolesc Health 23:364-369, 1998 |
|
Stouthamer-Loeber M, Wei EH: The precoursors of young fatherhood and its effect on delinquency of teenage males. J Adolesc Health 22:56-65, 1998 |
|
Resnick MD, Chambliss SA, Blum RW: Health and risk behaviors of urban males involved in a pregnancy. Fam Soc J Contemp Hum Serv 74:366-374, 1993 |
|
Anda RF, Felitti VJ, Chapman DP et al: Abused boys, battered mothers, and male involvement in teen pregnancy. Pediatrics 107:E19, 2001 |
|
Taylor DJ, Chavez GF, Adams EJ et al: Demographic characteristics in adult paternity for first births to adolescents under 15 years of age. J Adolesc Health 24:251-258, 1999 |
|
Darroch J, Singh S, Frost J: Differences in teenage pregnancy rates among five developed countries: the roles of sexual activity and contraceptive use. Fam Plann Perspect 33:244-250, 281 2001 |
|
Zabin LS: Why They Delay: A Study of Teenage Family Planning Clinic Patients. Fam.Plann.Perspec 24:205-205, 1981 |
|
McAnarney E: Adolescent pregnancy and its consequences. JAMA 262:74, 1989 |
|
Lara-Torre E, Schroeder B: Adolescent compliance and side effects with Quick Start initiation of oral contraceptive pills. Contraception 66:81-85, 2002 |
|
Jones ME: Lessons for Prevention and Intervention in Adolescent Pregnancy: A Five-year Comparison of Outcomes of Two Programs for School-Aged Pregnant Adolescents. J PediatrHealth Care 1995 |
|
Morris D, Berenson A, Lawson J et al: Comparison of adolescent pregnancy outcomes by prenatal care source. J Reprod Med 38:375-380, 1993 |
|
Cowden AJ, Funkhouser E: Adolescent pregnancy, infant mortality, and source of payment for birth: Alabama residential live births, 1991–1994. J Adolesc Health 29:37-45, 2001 |
|
Eure C, Lindsay M, Graves W: Risk of adverse pregnancy outcomes in young adolescent parturients in an inner-city hospital. Am J Obstet Gynecol 186:918-920, 2002 |
|
Fine J: Adolescent pregnancy prevention in managed care 1997 |
|
Morris D: Comparison of adolescent pregnancy outcomes by prenatal care source. J Reprod Med 38:(375): 1993 |
|
Fine J: Adolescent pregnancy prevention in managed care. Womens Health Issues 8:148-168, 1998 |
|
Lafferty W, Downey L, Holan C et al: Provision of sexual health services to adolescent enrollees in Medicaid managed care. Am J Public Health 92:1779-1783, 2002 |
|
Herman-Giddens ME, Slora EJ, Wasserman RC et al: Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 99:505-512, 1997 |
|
Forbes G: Pregnancy in the teenager: biological aspects. Birth Defects 17:85, 1981 |
|
Satin A: Maternal Youth and Pregnancy Outcomes: Middle School versus High School Age Groups Compared with Women Beyong the Teen Years. Am J Obstet Gynecol 171:184, 1994 |
|
Fraser AM: Association of young maternal age with adverse reporductive outcomes. N Engl J Med 332:1113, 1995 |
|
Lubarsky SL, Schiff E, Friedman SA et al: Obstetric characteristics among nulliparas under age 15. Obstet Gynecol 84:365-368, 1994 |
|
Scholl T: Young Maternal Age and Parity. Influences on Pregnancy. Ann Epidemiol 2:565, 1992 |
|
Stevens-Simon C: Factors Associated with Preterm Delivery Among Pregnant Adolescents. J Adolesc Health 14:340-340, 1993 |
|
Forbes GB: Human Body Composition. Growth, Aging, Nutrition and Activity. New York, Springer-Verlag, 1987 |
|
Garn SM: Are Pregnant Teenagers Still in Rapid Growth? Am J Dis Child 130:32, 1984 |
|
Lenders C, McElrath T, Scholl T: Nutrition in adolescent pregnancy. Curr Opin Pediatr 12:291-296, 2000 |
|
Hediger ML, Scholl TD, Belsky DH et al: Patterns of weight gain in adolescent pregnancy: Effects on birth weight and preterm delivery. Obstet Gynecol 74:6-12, 1989 |
|
National Research Council: Subcommittee on the Tenth Edition of the RDAs, Food and Nutrition Board, Commission on Life Sciences. Recommended Dietary Allowances. 10th ed.. Washington DC, National Academy Press, 1989 |
|
National Research Council, Food and Nutrition Board: Recommended Daily Allowances 1989 |
|
Lynch S: The potential impact of iron supplementation during adolescence on iron status in pregnancy. J Nutr 130:(2S):448S-451S, 2000 |
|
Albrecht S, Higgins L, Lebow H: Knowledge about the deleterious effects of smoking and its relationship to smoking cessation among pregnant adolescents. Adolescence 35:709-716, 2000 |
|
ACOG: Adolescent Pregnancy Facts. Women's Health Care Physicians 2003 |
|
Niccolai LM, Ethier KA, Kershaw TS et al: Pregnant Adolescents at Risk: Sexual behaviors and sexually transmitted disease prevalence. Am J Obstet Gynecol 188:(1): 2003 |
|
Fisher M, Rosenfeld WD, Burk RD: Cervicovaginal human papillomavirus infection in suburban adolescents and young adults. J Pediatr 119:821-825, 1991 |
|
Ho GY, Bierman R, Beardsley L et al: Natural history of cervicovaginal Papillomavirus infection in young women. N Engl J Med 338:423-428, 1998 |
|
Centers for Disease Control and Prevention: Division of STD/HIV Prevention 1992 Annual Report. Atlanta, Georgia, CDC1993 |
|
CDC: Center for Disease Control and Prevention. Sexually transmitted disease surveillance 2002 |
|
Saslow D, Runowicz C, Solomon D et al: American Cancer Society guideline for the early detection of cervical neoplasia and cancer. CA Cancer J Clin 52:342-362, 2002 |
|
Parker B, McFarlane J, Soeken K: Abuse during pregnancy: effects on maternal complications and birth weight in adult and teenage women. Obstet Gynecol 84:323-328, 1994 |
|
Harrykissoon S, Rickert V, Wiemann C: Prevalence and patterns of intimate partner violence among adolescent mothers during the postpartum period. Arch Pediatr Adolesc Med 156:325-330, 2002 |
|
Stevenson BA, Malton K, Teti D: School importance and dropout among pregnant adolescents. J Adolesc Health 22:376-382, 1998 |
|
Alexander C: Adolescent Pregnancy: Occurrence and Consequences. Pediatr Ann 22:85, 1993 |
|
Stevens-Simon CA: Adolescent Pregnancy. Pediatr Ann 20:322, 1991 |
|
Stevens-Simon C, Kelly L, Singer D et al: Reasons for first teen pregnancies predict the rate of subsequent teen conceptions. Pediatrics 101:E8, 1998 |
|
Phipps M, Blume J, De Monner SM: Young maternal age associated with increased risk of postneonatal death. Obstet Gynecol 100:481-486, 2002 |
|
Klerman LV: Adolescent pregnancy and parenting: Controversies of the past and lessons for the future. J Adolesc Health 14:553-561, 1993 |
|
Jaffee S, Caspi A, Moffitt T et al: Why are children born to teen mothers at risk for adverse outcomes in young adulthood? Results from a 20-year longitudinal study Dev Psychopathol 13:377-397, 2001 |
|
Miller F: Impact of adolescent pregnancy as we approach the new millennium. J Pediatr Adolesc Gynecol 13:5-8, 2000 |
|
Zelenko M, Huffman L, Lock J et al: Poor adolescent expectant mothers: can we assess their potential for child abuse? J Adolesc Health 29:271-278, 2001 |
|
Foundation TRH: Kids having kids: a Robin Hood Foundation special report on adolescent childbearing 1996 |
|
Feijoo AN: Teenage Pregnancy, The Case for Prevention. 2nd ed. Washington, DC, Advocates for Youth, 1999 |
|
ACOG: Strategies for adolescent pregnancy prevention. Committee on adolescent health care 2003 |
|
The Alan Guttmacher Institute: Trend toward abstinence-only sex ed means many U.S. teenagers are not getting vital messages about contraception. [Web Page] http://www.agi-usa.org/pubs/archives/newsrelease3205.html Accessed June 2003 |
|
Advocates ForYouth: Point definition of abstinence-only education as defined by section 510(b) of Title V of the Social Security Act, P.L. 104–193 [Web Page] http://www.advocatesforyouth.org/abstinenceonly.htm. Accessed June 2003 |
|
Advocates For Youth: The History of Federal Abstinence-Only Funding [Web Page] http://www.advocatesforyouth.org/publications/factsheet/fshistoryabonly.htm. |
|
Advocates For Youth: http://advocatesforyouth.org/rrr/history.htm. [Web Page] Accessed June 2003 |
|
Emerging answers: Research findings on programs to reduce teen pregnancy. Washington, DC, National Campaign to Prevent Teen Pregnancy 2001 |
|
Kriby D: Emerging answers: research findings on programs to reduce teen pregnancy. Washington, DC National Campaign to Prevent Teen Pregnancy. 2001 |
|
Hubbard BM, Giese ML, Rainey J: A replication study of Reducing the Risk, a theory-based sexuality curriculum for adolescents. J School Health 68:243-247, 1998 |
|
American Academy of Pediatrics: Committee on Adolescence. Sexuality Education for Children and Adolescents Pediatrics 108:498-502, 2001 |