Surgical Techniques for First-Trimester Abortion
Authors
INTRODUCTION
Abortion has been widely practiced since ancient times, and instruments for scraping the uterine cavity existed in Greek and Roman civilizations.1 Vacuum curettage techniques, however, are of more recent origin. In 1958, the Chinese Medical Journal published reports of abortion induced by vacuum curettage.2 Within a few years, the technique became widely practiced in Russia and Eastern Europe. By the time abortion was legalized throughout the United States in 1973, the vacuum technique had largely replaced the older method of dilation and sharp uterine curettage. This is entirely appropriate: one study that compared sharp curettage to vacuum techniques for first-trimester abortion revealed that vacuum curettage is quicker, produces less operative blood loss, and has a lower rate of perforations and a lower rate of hospitalization for postabortal infection than sharp curettage.3
Approximately 1.2 million legal abortions are performed annually in the United States in 2008.4 This number has been stable over the past several years.5, 6 As the population is increasing, the abortion rate has been declining slightly. Currently, 88% of abortions are performed at less than 13 menstrual weeks; this proportion has remained stable since the 1990s.4, 5, 7, 8, 9, 10, 11 Sixty one per cent of all abortions were performed at 8 weeks or earlier in 2006, a marked increase from 51% in 1990.4, 5, 7, 8, 11 In 2008, abortion surveillance reports published by the Centers for Disease Control and Prevention reported that 15% of abortions were first-trimester medical abortions induced with mifepristone/misoprostol, or misoprostol alone.4 Uterine aspiration is necessary for only a few of the women who undergo medical abortion.
Surgical techniques in the first trimester consist virtually exclusively of vacuum or suction techniques. The term “vacuum curettage” is used interchangeably with “uterine aspiration” or “vacuum aspiration”; all refer to evacuation of the uterus by suction, regardless of the source of the suction. Manual vacuum aspiration is the term commonly applied to uterine evacuation using a hand-held syringe as the source of the vacuum. "Menstrual regulation" refers to surgical or medical treatment to "bring on" a late menstrual period without first doing a pregnancy test, and is an important means for providing safe services in countries that allow menstrual regulation, but do not allow legal abortion.
In countries where abortion is legal it usually very safe,12, 13, 14, 15, 16 in contrast to countries where abortion is restricted and large numbers are performed under unsafe conditions.17 In the United States, the overall mortality rate was 1.1/100,000 legal induced abortions for the years 1972–1997 when 30,975,129 abortions were performed.16 Mortality is primarily determined by gestational age, increasing from 0.1/100,000 for abortions performed at less than 8 weeks, to 3.3/100,000 at 18 weeks, but does not equal the overall maternal mortality rate of 8/100,000 until 22 weeks.16 More recently, the overall mortality rate for abortions in the United States was 0.6/100,000.18
INSTRUMENTS FOR VACUUM CURETTAGE
Vacuum for uterine aspiration can be produced with either an electric pump or a hand-held syringe (manual vacuum). Electric vacuum is used for most abortions in the United States, but manual vacuum is used for an increasing proportion. A number of electrically powered uterine aspirators are sold in the United States. There should be two vacuum bottles in series and a third bottle or trap with a one-way valve to protect the pump from any overflow of fluid. The system should be simple to take apart and clean. The uterine aspirator manufactured by the Berkeley Medevices (Table 1) is in widespread use. These pumps are all compatible with clear plastic hoses and handles that accept the standard-sized curettes.
Table 1. Some United States suppliers of instruments for first-trimester pregnancy termination
Berkeley Medevices Inc.
http://berkeleymedevices.com
Cheshire Medical Specialties, Inc.
Cooper Surgical
www.coopersurgical.com
Gynex
www.gynex.com
IPAS (formerly International Pregnancy Assistance Services)
www.ipas.org
MedGyn
www.medgyn.com
Thomas Medical
www.thomasmedical.com
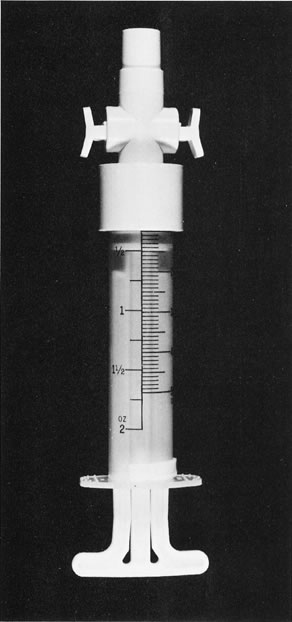
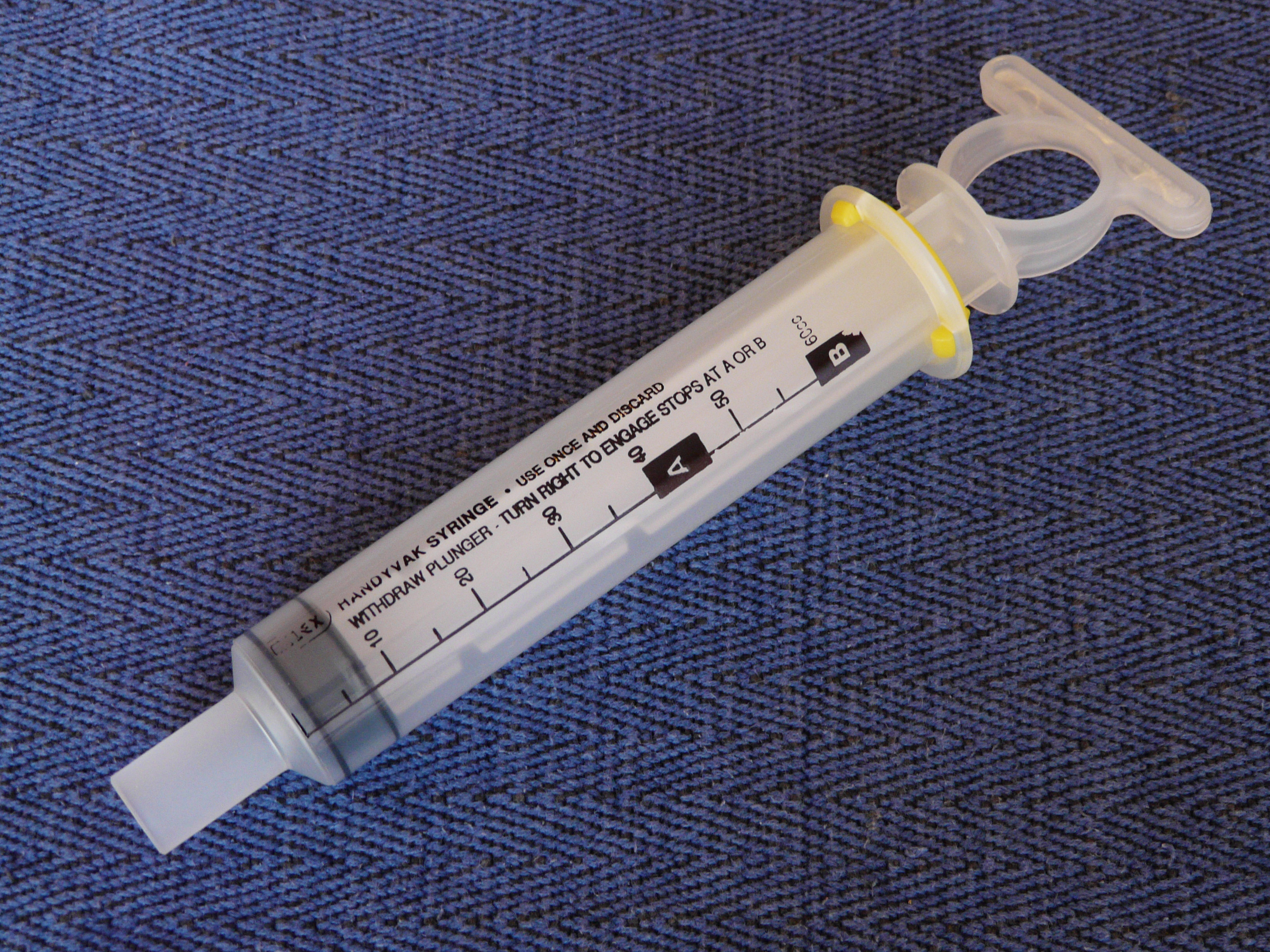
The modified 50 cc plastic syringe originally developed by Karman for early first-trimester procedures has been further modified to have 60 cc capacity and to accept vacuum cannulas with either a 6 or 12 mm base. There are three manual vacuum aspirators available in the US. One is the Ipas Single Valve aspirator (Fig. 1) that accommodates cannula from 4 to 6 mm and is meant for early abortions, endometrial biopsy, or management of dysfunctional uterine bleeding. The other two are the Ipas MVA Plus (Fig. 2) and the Milex Handyvak Locking syringe (Fig. 3). Both accept cannulas with a 12 mm base. The Ipas MVA Plus will accept 14 and 16 mm cannulas with a 12 mm base. Both are adequate for evacuation of the pregnant uterus throughout the first trimester19 and even into the midtrimester.20 The Ipas Single Valve syringe can be reused after high level decontamination in liquids. The Milex Handyvak syringe is intended for single use only. The Ipas MVA Plus can be disassembled and steam sterilized in an autoclave. Both Ipas devices have a valve which allows the plunger to be pulled out to evacuate the syringe before inserting the cannula in the uterus (Fig. 2). The Milex Handyvak has no valve and requires more strength on the part of the operator who must connect the cannula to the syringe, insert it through the cervix and then pull out the plunger. The Ipas syringes are in worldwide use, allowing safe vacuum curettage abortions at very low cost where electric power is unavailable or unreliable. Suppliers of these instruments are listed in Table 1.
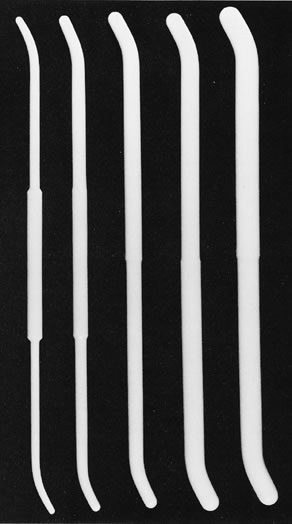
When vacuum curettage was introduced, glass or, later, metal curettes were used. Neither is satisfactory, and both were supplanted by plastic cannulas. At present, there are two main types of plastic cannulas: the flexible opaque cannula of the Karman design, ranging from 4 to 12 mm in external diameter, and the clear semirigid cannula, ranging in size from 6 to 16 mm (Fig. 4). The smaller flexible cannulas are advantageous for performing early first-trimester abortion, often without cervical dilation. However, the larger flexible cannulas have a thick wall and therefore a relatively small internal diameter relative to their external diameter. The use of flexible cannulas throughout the first trimester has been advocated.21, 22 However, apparently most operators in the US prefer the rigid vacuum cannula. With the clear cannula, the operator can see amniotic fluid and fetal tissue as it is aspirated, an important indication that the curette has been properly placed in the uterine cavity.
A typical set of instruments for first-trimester abortion is displayed in Fig. 5, and an expanded list of equipment has been tabulated by Williamson.23 These instruments are readily contained in autoclavable paper or a steel pan, allowing steam sterilization in small autoclaves. For early first-trimester procedures, whether electric or manual, fewer instruments are necessary: dilators up to #23 Pratt are usually sufficient, and curettes and sponge forceps are not usually used. The speculum deserves special attention. The weighted speculum of the Auvard type is very convenient when the patient is anesthetized because it allows the operator to pull the cervix toward the introitus, facilitating introduction of instruments through the cervical canal. The weighted speculum is usually not tolerable to patients unless they are anesthetized. The standard-length bivalved speculum (Graves) holds the uterus and cervix away from the operator. A compromise for local anesthesia abortion is offered by the Moore modification of the standard bivalved speculum. The blades of the Moore (also called Moore-Graves) speculum are about an inch shorter than the Graves.
Several different instruments have been used to provide stabilization and countertraction on the cervix. Many operators use a short, square-jaw single-tooth tenaculum. The tenaculum is placed vertically with one branch inside the cervical canal so that a solid bite of cervical tissue is taken. This tenaculum placement produces a single clean puncture of the cervix that rarely tears; transverse placement may result in circumferential tears. Alternative cervical stabilizers include a long Allis clamp or Bierer tenaculum; their multitoothed design is unlikely to produce a cervical laceration. If dilation has occurred before the abortion, a ring forceps can be used.
For middle-first-trimester and late-first-trimester abortions some operators use a sharp curette to check the uterine wall though this has not been proven necessary. Number 1, 2, and 3 Sims sharp, malleable uterine curettes are appropriate for most first-trimester procedures. For very early procedures (less than 6–7 weeks) sharp curettage is not usually done, and even a No. 1 Sims will not pass the cervix. If curettage is desired, a No. 0 or 00 curette may pass the cervix. In addition, it is useful to have a small ovum forceps available, such as a Moore forceps or the Randall kidney stone forceps. Either of these small instruments can be used with 8- or 9-week procedures. A ring sponge forceps, such as a Foerster forceps, can be used with later first-trimester abortions.
DILATION OF THE CERVIX
Most women need some form of cervical dilation for abortion; the exceptions are some women who have very early pregnancies (less than 6 weeks) or who already have cervical dilation from spontaneous abortion. Mechanical dilation is currently the most frequently used method of dilating the cervix; other methods are osmotic dilators and use of medications such as misoprostol. Hegar dilators were the standard instruments for cervical dilation many years ago. These are blunt-ended instruments that increase by 1 mm between dilators. Tapered dilators, such as Pratt dilators, require less force during insertion than blunt dilators and have replaced Hegar dilators in the US. A case series of abortions performed with Hegar dilators had more cervical lacerations and uterine perforations than a more recent series in which Pratt dilators were used.3 Thus, tapered dilators such as the Pratt (see Fig. 5), the Hawkin-Ambler, or the Hanks, are strongly recommended. Denniston's plastic dilators of the Pratt design offer a low-cost alternative for dilation (Fig. 6); this dilator is preferred by some operators because it is lightweight. Half-size Hegar dilators, which increase by only 0.5 mm between dilators, also appear acceptable. Bozorgi's24 series of abortions performed with half-sized Hegars yielded one of the lowest rates of uterine perforation at first-trimester abortion yet reported (2 per 10,000 cases). In a series of 170,000 consecutive abortions at gestational ages through 13 menstrual weeks with dilation by Pratt dilators, the reported rate of perforation was 1 in 10,625 cases.14
Alternatives to mechanical dilation
The alternatives to mechanical dilation include osmotic and pharmaceutical dilation.
OSMOTIC DILATION
Osmotic dilation compares favorably to mechanical dilation in the second half of the first trimester.25, 26 There are three types of osmotic dilators: laminaria tents, synthetic tents (Dilapan-S™), and the magnesium sulfate sponge (Lamicel™). Lamicel is no longer available in the US. Suppliers are listed in Table 1. Laminaria are the stem of a seaweed. The laminaria take up moisture after insertion into the cervical canal and swell, producing gradual dilation (Fig. 7). Laminaria japonicum are used almost exclusively in the US; L. digitata, which may become too soft during dilatation, are seldom used in the US, although they are used in other countries. Dilapan-Ss are made of polyacrilonitrile, and swell more rapidly than laminaria.27, 28
Osmotic dilators are purchased individually wrapped and presterilized. They can be placed as little as 6 hours before the abortion;29 however, dilation will be greater if they are allowed to remain in place overnight. The technique of insertion is as follows. The cervix is grasped with a tenaculum, and the cervix is washed with an antiseptic such as povidone-iodine. A paracervical block may be used. The package is opened and the dilator grasped by the end with the string, using a sterile forceps. The dilator should be inserted into the cervical canal until the tip is just above the internal os. The operator generally can tell by the sensation that the dilator has passed this point. About 3 mm of the outer end of the dilator should protrude beyond the exocervix in most cases. A second small laminaria should be inserted alongside the first to allow for easy removal of the devices (Fig. 8). This is especially important with Dilapan-S, as a single Dilapan may be difficult to remove. Some operators place a sponge (4 × 4 cm sponge) in the vagina with the intent of holding the dilators in place. Overnight, laminaria will approximately double in diameter and Dilapan swells still more. Lamicel increases in diameter approximately 1.5-fold over 2–4 hours. It is more suitable for same-day use but does not provide the amount of dilation that laminaria or Dilapan-S tents do.27
PHARMACEUTICAL CERVICAL DILATION
Currently, misoprostol (Cytotec) is the only prostaglandin analog used with frequency for cervical dilation in the US. Earlier use of prostaglandin E2 (Prostin E2) and a 15-methyl analog of prostaglandin F2a, carboprost tromethamine (Hemabate) were associated with considerable pain and for some patients vomiting and diarrhea.30
Misoprostol is approved by the Food and Drug Administration for prevention and treatment of gastric ulcers but has been used extensively for abortion, either alone or in combination with mifepristone or methotrexate. Administered by vaginal, oral, buccal or sublingual routes, it results in uterine contractions and softening and dilation of the cervix. It is inexpensive, stable at room temperature and available in many countries. Misoprostol is more effective at producing dilation than intramuscular 15-methyl prostaglandin F2a,31 vaginal gemeprost32, 33 or placebo.34 A vaginal dose of 400 μg of misoprostol is more effective than 200 μg,35 and all doses are more effective when used at least 3 hours before the abortion.36 A small study found sublingual misoprostol more effective than the oral or vaginal routes.37 With misoprostol administered at least 3 hours prior to surgery, mechanical dilation is often avoided completely, and if dilation is needed it is technically easy because the cervix is softened. A trial comparing laminaria and misoprostol found similar amounts of dilation after use, but women using laminaria reported more pain.38
Mifepristone given 48 hours before second trimester abortion produced more dilatation than misoprostol alone.39, 40 Mifepristone might be considered for cervical preparation before first-trimester abortion, although in the US this would add considerable expense.
ANALGESICS AND ANESTHETICS
In the US, most surgical abortion procedures are performed with paracervical block with or without sedation. A smaller number of procedures are performed with general anesthesia. Most patients will experience some discomfort during abortion, although the amount reported ranges from none at all to severe.41 Young women and women who are more fearful or anxious before the procedure appear to experience more pain than older women and those who are less fearful.42, 43 Women who have given birth experience less pain than nulliparous women.44
Nonsteroidal anti-inflammatory drugs, such as naproxen 550 mg, are commonly used before abortion to reduce pain during and after the procedure.45 Use of intravenous sedatives and narcotics will add to the patient's comfort, but this adds some risk24 and may not relieve distress as much as expected.41 Pain scores are modestly improved, but patient satisfaction scores range from minimally improved to significantly increased.46 A commonly used regimen for intravenous sedation is 2 mg of midazolam combined with 50–100 µg of fentanyl. Analgesic effect is improved by waiting 5 minutes after infusion of the drugs before beginning the surgical procedure. General anesthesia increases the cost of abortion and increases the risk for major injury such as uterine perforation, cervical trauma, intra-abdominal hemorrhage, and the need for blood transfusion.47, 48 Anesthesia complications accounted for 16% of US abortion deaths in 1988–1997.16 Local anesthesia has fewer major complications, and the spectrum of complications is different. Fever, presumably due to endometritis, and convulsions from the local anesthetic, are more frequently reported with local anesthesia.12 Several authors have recommended that paracervical block be used and that general anesthesia be avoided.13, 47, 48
When sedation is used, a common combination of medications is midazolam 2 mg and fentanyl 50–75 μg by slow intravenous injection. Alternatives to the sedative midazolam include diazepam; alternative narcotics are meperidine and alfentanil. All of these agents are respiratory depressants and can cause respiratory arrest if given too rapidly, in too large a dose, or even in low doses in very susceptible individuals. A pulse oximeter is recommended to monitor the patient's oxygen saturation if either a narcotic or sedative is used; when both are used together, a pulse oximeter should be used until recovery from the intravenous analgesia. The narcotic antagonist naloxone and the sedative antagonist flumazenil should be readily available and used if there is any question of respiratory depression.
Paracervical block has been demonstrated to be superior to sham injection.49 The choice of local anesthetic is important. The major hazard of paracervical block is intravascular injection or too-rapid absorption of the agent, with resultant systemic toxicity.50 The amide local anesthetics, such as lidocaine hydrochloride, are metabolized slowly in the liver after systemic absorption. The ester local anesthetics, such as chloroprocaine, are hydrolyzed rapidly by plasma pseudocholinesterase and are less likely to cause toxicity and convulsions.48 Despite the advantage of decreased toxicity, chloroprocaine is not widely used because of its increased cost compared with lidocaine. None of the local anesthetics have been shown to be superior in terms of pain relief to the other agents.51
To avoid toxicity, the dose of lidocaine should not exceed 2 mg/lb of body weight,50 or a total of 200 mg (20 ml of 1% lidocaine solution). Many practitioners use 10 ml of 1% lidocaine (100 mg), or 20 ml of 0.5% lidocaine (100 mg). Twenty milliliters of 1% lidocaine provided the same relief as 20 ml of 0.5% lidocaine; therefore, it is reasonable to use 100 mg total by using a dilute solution. A 100 mg bolus of lidocaine is commonly used in other situations; it causes toxicity infrequently.
Other agents may be added to the local anesthetic. Vasopressin (2–4 units) will decrease bleeding in second-trimester procedures,52, 53 and although published data about efficacy in first-trimester procedures are lacking, it appears to be widely used in first-trimester abortions as well. Adding oxytocin to paracervical block did not improve blood loss or pain during first trimester abortion.54 Atropine (0.5 mg) can be mixed with the local anesthetic to reduce vagal effects and prevent syncope and nausea. Finally, sodium bicarbonate 8.4% can be added to the mixture in a 1:10 dilution (1 cc of bicarbonate to 10 ml of anesthetic) to buffer the solution and decrease the burning experienced by some women on injection. Solutions containing epinephrine should not be used because they can result in anxiety and carry a risk of cardiac arrhythmia. Glick55 described an anesthetic mixture of vasopressin and bicarbonate added routinely to 1% or 0.5% lidocaine, with atropine added as well if desired.
There are several techniques of paracervical block. A two-point injection is not sufficient for most women, and injection of large amounts of solution at each point increases the chance of intravascular injection. Intravascular injection can occur even with aspiration before injection; use of multiple injection sites with small volumes at each site decreases the volume that can be forced into a vessel. A simple four-point block is commonly used, with injections at 12, 3, 6, and 9 o'clock; an alternative is a five-point block at 12, 3, 5, 7, and 9 o'clock. Several authors describe a deep injection technique; Wiebe56 has shown in a comparative study that the deep injection technique provides better analgesia than superficially administered paracervical anesthesia. The Glick55 technique of deep injection has several steps. First, the cervix is infiltrated superficially with 2–3 ml at 12 o'clock and the needle is advanced through the anesthetized area for approximately 3 cm to reach the junction of the cervix and lower uterine segment, where an additional 2 cc is injected. This allows placement of the tenaculum without pain. The procedure is repeated at 4 and 8 o'clock, injecting 2–3 cc superficially and then advancing the needle 3 cm to infiltrate the lower uterine segment on each side with 4–5 cc. If after dilation is begun the block seems less effective on one side, an additional deep injection of 5–6 cc can be given on that side.
Other non-pharmacologic methods of pain control have been investigated, with mixed results. Hypnosis was compared to "standard care" which included instruction for relaxation and deep breathing and resulted in higher satisfaction scores than standard treatment.57 However, the addition of music to ibuprofen and paracervical block seemed to increase pain scores.58
PREOPERATIVE ASSESSMENT
Introduction to the patient
When providing abortion care, considerable skill in interpersonal relationships is necessary for all staff involved in the woman's care. Many women undergoing abortion are apprehensive, frightened, or guilty, and some pregnancies have resulted from abuse, coercion, or assault. If the physician's behavior is abrupt and cold and he or she appears angry or rushed, it will be harder for the woman to relax, and the abortion procedure will be made more difficult. The woman should receive emotional support and a feeling of calm, sympathetic interest. The woman should never be pressured to proceed with the abortion if she is not ready. If she is uncertain, distressed, or withdrawn, she needs additional counseling and support before the abortion begins. On occasion, women decide not to proceed with the abortion at the last moment, and that decision must be supported by the staff.
Size–date discrepancy
When the clinical estimate of gestational age disagrees with the period of amenorrhea, the clinician must account for the discrepancy before proceeding. Uterine size larger than dates may results from many situations, including a more advanced gestation in a normal uterus, a multiple gestation, a uterine anomaly, uterine fibroids, a molar pregnancy, or an ovarian tumor. If the operator is confident that the most likely explanation is a more advanced gestation, but one within his or her range of expertise, he or she could proceed with a standard dilation and vacuum curettage abortion. However, if the uterine mass is asymmetric or the uterine volume is apparently more than a month larger than dates, a diagnostic ultrasound is strongly advised. A small gestation in combination with a large uterine mass may be a risk for perforation at attempted abortion. Uterine size that is considerably smaller than the duration of amenorrhea should also create concern. The patient may have a less advanced pregnancy, may not be pregnant, may have a nonviable pregnancy, or may have an ectopic pregnancy. When the uterine size is expected to be larger than it actually is, instruments may be inserted too deeply.
Many clinicians perform routine ultrasound examination before abortion. However, universal ultrasound use has not been shown to be superior to selected ultrasound use in the first trimester in terms of complication rates.
Abnormal pregnancy
With the frequent use of preabortion ultrasound, findings of abnormal pregnancy are not uncommon. The suction aspiration is technically the same whether the pregnancy is viable or not. Although the procedure is the same, the woman may feel differently about terminating an abnormal pregnancy and may in fact be relieved that she is having an “indicated” rather than an “elective” procedure. She has other treatment options, such as expectant or medical management. There may be financial ramifications if termination of a nonviable pregnancy is reimbursed by insurance while elective abortion is not. Therefore, informing the woman of the abnormal pregnancy has several benefits.
Fetal abnormalities may be identified by ultrasound examination. This situation may be more complex. The woman who had initially requested an induced abortion and is presented with information obtained accidentally may feel worried and uncertain. She may request further testing or information and should be referred for additional counseling if desired. Multiple pregnancy is another complex situation. If the woman requested an elective abortion but had an ultrasound showing a multiple gestation, it is unclear whether the information is useful. The possible anxiety at a stressful time must be balanced against the desire to provide as much information as possible.
The ultrasound finding of multiple cystic structures may indicate a molar pregnancy, but can also be seen in hydropic degeneration of an abnormal pregnancy. Very early or small molar pregnancies may be missed. Therefore, not all molar pregnancies are diagnosed correctly before the abortion, and some women without trophoblastic disease may be told of the possibility of a mole. The finding of a molar pregnancy of first-trimester size is not a contraindication to evacuation in an outpatient setting. The technique of evacuation is the same. In the series by Yuen and Callegari,59 there were no complications among women who had molar evacuation on an abortion unit. When trophoblastic disease is a possibility, a baseline human chorionic gonadotropin level should be obtained. Thereafter, appropriate follow-up is determined by the diagnosis.
Prophylactic antibiotics
Antibiotics are used widely with first-trimester abortions in the US. The incidence of infectious complications of legal first-trimester abortion is low, ranging from 0.5 to 3% in many reports,12, 13, 14, 60 although the rates are higher in others.61, 62, 63, 64, 65 Antibiotics were not used routinely in the large New York City series by Hakim-Elahi and colleagues,14 but reported serious infections were rare. A different perspective is that many of the postabortion complications that do occur are caused by infection. A meta-analysis by Sawaya and coworkers66 concluded that the routine use of prophylactic antibiotics could prevent half of the cases of postabortion endometritis.
The first compelling demonstration in favor of prophylactic antibiotics was the study by Hodgson and associates.61 They used oral tetracycline (1.5 g) given 2–3 hours before the abortion and then 0.5 g four times a day for 4 days. Four successive groups of 1000 patients each were either not treated or were treated with tetracycline. Major and minor complications were significantly reduced among the 2000 patients who received the antibiotics.
Subsequently, a randomized study found a significant benefit of tetracycline for patients already colonized with chlamydia, but chlamydia-negative patients benefited as well.62 Untreated chlamydia and gonorrhea increase the rate of postabortion infection; treatment either before or at the time of abortion reduces the incidence of postabortion infection.63 Erythromycin was also effective.64
Other studies have found a benefit from a single perioperative dose of doxycycline.65, 67 Bacterial vaginosis is also associated with an increase in postabortion infections, and treatment at the time of abortion decreases the rate of infection by 75%.68 Metronidazole has also been used for routine prophylaxis for abortion patients and is associated with a decrease in the incidence of infection.69 The incidence of endometritis and the value of prophylactic antibiotics have not been established in very early surgical abortion. In a series of 2399 women undergoing surgical abortion before 6 weeks, no postabortion infections were observed.70 The American College of Obstetricians and Gynecologists recommends giving 100 mg doxycycline preoperatively and 200 mg postoperatively.71 Many clinicians give only the post-procedure dose, as doxycycline given on an empty stomach before procedure may results in vomiting.
Historically, prophylactic antibiotics were given with the intent of preventing bacterial endocarditis. In 1997, the American Heart Association revised guidelines for the prevention of bacterial endocarditis.72 They classified abortion as a procedure with a low risk of bacteremia and did not recommend antibiotic prophylaxis for women undergoing abortion. The recommendation is the same whether the woman is at high risk for endocarditis (e.g. prosthetic valve, right-to-left shunt) or at medium risk (e.g. mitral valve prolapse with regurgitation, aortic stenosis).
TECHNIQUE
Surgical abortion technique in the first trimester
Obviously, there are many technical variations on the actual surgical procedure. The reader is referred to several texts for similar but slightly differing approaches.73, 74, 75, 76, 77 One approach is as follows. A sterile speculum is inserted into the vagina to expose the cervix, and the cervix is washed or sprayed with antiseptic solution, such as povidone-iodine. A sterile field drape at the perineum or on an adjacent stand is sufficient. Shaving and washing of the perineum are not necessary; neither are a full sterile drape set and surgical caps and gowns. The operator should use appropriate eye protection and personal protection that would be used for other office procedures. The operator must use sterile instruments and sterile gloves and take care never to touch that part of the instrument that will enter the uterus. This has been labeled the “no-touch” technique, as opposed to the full sterile technique routinely followed in hospital operating rooms.
With the cervix visualized, local anesthetic is injected at 12 o'clock as previously described. A single-tooth tenaculum is then placed on the cervix at 12 o'clock in a vertical position with one branch up the endocervical canal, unless the shape of the cervix indicates a horizontal placement. If a Beirer or Allis clamp is used, it is usually placed on the anterior lip, but any tenaculum can be placed on the posterior lip if that provides better stabilization. The paracervical block is then completed.
For osmotic dilator removal, the speculum is inserted just far enough to visualize sponges, if any, and these are removed with forceps. The end of the dilator is then grasped and gently pulled and the dilator slides out. Any other dilators are similarly removed. Occasionally, the dilators are hard to remove. In such cases, it is best to grasp one dilator and pull gently and slowly; pulling on the string will result in breaking the string. With gentle continuous traction, the dilator will usually come out. If this does not work, it is preferable to let a few more hours go by, or wait overnight. An alternative is to use misoprostol for several hours. The cervix will soften and dilate still more during this time, and at this point the dilator will be removable.
Safe dilation depends on the operator's proper determination of the direction of the endocervical canal. Failure to appreciate that the uterus is retroverted may result in an anterior perforation. Whether or not the depth of the uterine cavity needs to be measured with a uterine sound is controversial. Most operators do not use a sound for fear of perforation and a feeling that little information is gained. Up to one quarter of perforations are associated with use of a sound.78 Mechanical dilation, if needed, is accomplished using tapered dilators such as Pratt or Denniston. The operator must take care to insert the dilators slowly and gently; this is both safer and less painful. If resistance is experienced, the operator should return to the previous dilator, reinsert it, and allow it to remain in place for a minute or so before attempting to insert the next large dilator.
The work of several investigators appears to show that there is an upper limit beyond which the cervix may not be forcibly dilated without disruption of cervical fibers, which might produce permanent injury and risk of premature birth in subsequent pregnancy.79 In the study by Johnstone and colleagues,80 when the cervix was forcibly dilated beyond 11 mm or so, the cervical canal was found to remain abnormally larger at calibration 6 weeks after abortion. Dilation should be just sufficient to allow gentle insertion of a suitably sized vacuum cannula. For pregnancies at 6–7 weeks from last menses, an appropriate combination is a 6 mm Karman or semirigid cannula and minimal dilation. The diameter of the cannula should generally be 1–2 mm smaller than the operator's estimate of the gestational age in menstrual weeks, although some operators prefer to use a cannula size equal to the number of weeks. Thus, for a 9-week pregnancy, the surgeon might use an 8 mm cannula, and for a 12 week gestation, a 10 mm cannula. Bozorgi24 used no cannula larger than 10 mm in his large series of first-trimester abortions and yet achieved a very low incidence of retained tissue, postabortion infection, and bleeding. For a given gestational age, evacuation can be accomplished more quickly with a larger cannula, but more dilation will be needed. In each case the operator makes a judgment based on ease of cervical dilation. If dilation is becoming difficult, it may be better to use a smaller vacuum cannula and take longer to empty the uterus but avoid traumatizing the cervix.
Having achieved dilation of the cervix, the operator inserts the vacuum cannula and establishes vacuum. Uterine evacuation is done with 60–80 mm Hg of negative pressure for an electric pump, or full vacuum for a 60 cc manual syringe. The cannula is gently rotated several times. This motion will start amniotic fluid and tissue flowing out through the cannula. Some operators use a rotating motion exclusively, while others use an in-and-out motion while continuing to rotate the cannula. On the outstroke, the cannula tip is pulled back to the region just above the internal os, but not through it. Typically an electric suction procedure will take two or three cannula introductions. Regardless of the technique, the cannula should not be rotated in the cervix.
The operator can feel that vacuum aspiration is completed by the gritty feeling of the cannula scraping over the uterine lining and by the increased resistance to moving the cannula. The placental site can sometimes be felt as a softer, smoother area. A sharp metal curette can confirm that the cavity is empty. There is no need to perform a complete sharp curettage. The sharp curette is used as one might use a finger to explore the cavity. Use of sharp curettage may slightly increase the blood loss from the procedure, and this step is controversial. Some operators check the uterus with a curette routinely;14, 74 others do not. A last step, also optional, is to reinsert the vacuum cannula and re-establish the vacuum for a brief interval. Care must be taken with reinsertion of the cannula because the internal os will have constricted somewhat and the direction of the uterine cavity with respect to the cervical cannula may have changed as the now-empty uterus contracts. This repeat suction may remove a few more fragments of tissue and may induce the uterus to contract further.
Women who are Rhesus-negative can be given Rh immune globulin immediately; some operators inject it into the cervix at the end of the procedure, because the cervix is anesthetized and the injection is not felt.
Surgical backup for medical abortion
Women undergoing medical abortion may have a surgical procedure for one of several reasons: the medical agent may fail to interrupt the pregnancy, the woman may decide that she does not wish to wait for completion of the medical process, or she may have an incomplete abortion or prolonged or unacceptable bleeding. Aspiration procedures in these circumstances are usually very easy. The pregnancies are usually less than 7–9 weeks, and the cervix is usually dilated. Mechanical dilation is usually not necessary, and manual vacuum aspiration is readily accomplished.
Tissue examination
This last step in a surgical abortion procedure is examination of the aspirated tissue.81 The tissue examination must be performed before the woman leaves the office or facility so that if the tissue is not adequate, the woman can be re-evaluated and treated appropriately. Laboratory results received later may be too late for optimal care of the woman.
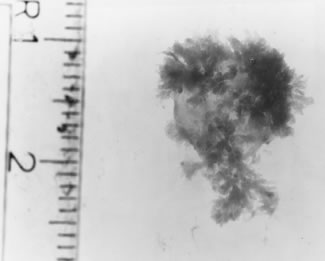
Examining the tissue is much easier if the blood and clots are removed. For electric suction systems, tap water or saline is aspirated through the suction tube. This will rinse the specimen and also remove pieces of tissue from the tubing into the collection bottle. Stockinette collection bags or tissue traps make the specimen more difficult to collect entirely for viewing and may trap key pieces of tissue in the mesh. The contents of the collection bottle or syringe should be emptied into a strainer for further rinsing. After rinsing, the specimen can be placed into a glass flat-bottom pan with backlighting. Tap water or saline is added to float the specimen. Chorionic villi, embryonic membranes (“gestational sac”), and fetal parts are distinguishable from decidua. The rinsed trophoblastic tissue will be white when compared with decidua and will appear like a fluffy ball with a filmy elastic membrane (Fig. 9). This is evident when the specimen is illuminated from beneath and is often difficult to see without backlighting.
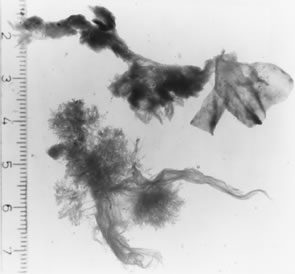
A positive identification of the early conceptus requires identification of chorionic villi attached to membranes, as seen in Fig. 10. Visualizing a few villi does not guarantee an intrauterine pregnancy; a few villi can be present with a tubal pregnancy. Visualizing gestational sac and villi can be possible as early as 4 weeks after the last menstrual period,69 but is more reliably seen 5 weeks after the last menstrual period. Small specimens are best seen when they have had a minimum of manipulation; tissue traps, long suction tubing, and small-cannula apertures are all thought to fragment the tiny specimen. Manual vacuum aspiration results in easier identification of pregnancies under 6 weeks, but it is important to use an adequately sized cannula (6 mm or larger for most pregnancies).70 At 9 menstrual weeks and beyond, definite fetal parts should be seen (Fig. 11). The size can be estimated from gross appearance, or from the foot lengths listed in Table 2.
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 2. Correlation between menstrual age and fetal foot length
Menstrual age (weeks) | Mean fetal foot length (mm) |
8.5 | 4.2 |
9 | 4.6 |
10 | 5.5 |
11 | 6.9 |
12 | 9.1 |
13 | 11.4 |
14 | 14 |
15 | 16.8 |
16 | 19.9 |
17 | 23 |
18 | 26.8 |
19 | 30.7 |
20 | 33.3 |
21 | 35.2 |
22 | 39.5 |
23 | 42.2 |
24 | 45.2 |
(Streeter GL: Weight, sitting height, head size, foot length, and menstrual age of the human embryo. Contrib Embryol 11:157, 1920.)
Even when obvious gestational tissue has been aspirated, it is important that the appearance of the tissue correspond to the operator's preoperative assessment of gestational age, whether the estimate was based on pelvic or ultrasound examination. For example, if the woman was thought to be 10 weeks pregnant but only a small amount of trophoblastic tissue was aspirated, the patient may indeed have been only 5–6 weeks pregnant. However, there may still be a 10 week gestation in the uterus; in effect, a chorionic villus sampling was done, and the pregnancy may continue. When abortion is performed at the end of the first trimester, the surgeon must verify that all fetal parts have been removed. The fetal cranium or other large part can be retained in the uterus to cause later bleeding and infection unless care is taken to ascertain that all fetal parts are present in the specimen.
While it is necessary that aspirated tissue be examined on site immediately after abortion, routine examination of all aborted tissue by a pathologist adds expense with no benefit.82 The operator (or his or her staff) has already identified the presence of villi and membranes as well as fetal parts when present. Identification of other findings of relevance to the woman is unlikely, but some states and hospitals have statutes requiring tissue examination in a pathology laboratory. There are several circumstances where independent pathologic examination is highly recommended: the absence of villi, the presence of a fetal anomaly, and the presence or suspicion of a molar pregnancy.
Women with a known or suspected abnormality of the pregnancy may request genetic analysis of the conceptus. The technique of tissue collection varies from site to site, and the cytogenetics laboratory should be consulted. Typically, the tissue should be collected in as sterile a manner as possible because bacterial contamination may prevent cell growth. Chorionic villus sampling before the abortion may be a better method of obtaining uncontaminated cells.83 For most situations, the sample can be floated in sterile saline, and a sample of villi removed and placed into a transport media tube. If there are recognizable fetal parts, a fetal skin sample should also be sent.
Evaluation when the tissue specimen does not show villi
When chorionic villi are not seen, there are several options. The specimen can be examined under a dissecting microscope. A trained observer can readily distinguish normal chorionic villi from decidua, but the blunted avascular and edematous villi of a nonviable abortion may present some difficulties. Identification of villi makes ectopic gestation much less likely, but to be certain, demonstration of the gestational sac is necessary. In hospital settings, a frozen-section examination of the aspirated tissue may be helpful in identifying villi and sac membranes. A fixed specimen may take 1–2 days. The absence of villi is consistent with several diagnoses. These include the possibility that the woman was not pregnant (a false-positive pregnancy test), unrecognized spontaneous abortion (more likely with very early abortions), failed abortion with either a normal uterus or a uterine anomaly, and ectopic pregnancy. If chorionic villi are not identified, the patient must be considered at risk for ectopic pregnancy and appropriate procedures must be implemented.
There are several diagnostic steps. The first step is a re-examination of the woman, palpating for adnexal tenderness or a mass. The second step is a vaginal probe or abdominal ultrasound examination to determine whether the pregnancy is still in the uterus. A vaginal ultrasound should be able to visualize almost all pregnancies over five menstrual weeks. Under five weeks, it may be impossible to demonstrate the intrauterine gestational sac.84 In the absence of a gestational sac on ultrasound, the third step would be a quantitative assay for human chorionic gonadotropin (hCG), which can provide an assessment of the risk of ectopic pregnancy. Depending on the resolution of the ultrasound equipment and the operator's skill, women with an hCG level of more than 1500–2000 mIU/mL should have a gestational sac visible on vaginal ultrasound examination if they have a normal intrauterine pregnancy. An hCG level less than 1500–2000 mlU/mL may be consistent with either an intrauterine pregnancy or an ectopic pregnancy. However, suction curettage may have already removed a small abnormal pregnancy or a very early normal pregnancy. If the pregnancy has been removed, the hCG level should drop by 50% within 2 days. The woman judged to be at low risk for ectopic pregnancy can be followed as an outpatient. At the follow-up examination 2–3 days later, if she is asymptomatic and the hCG level is falling appropriately, the diagnosis of completed abortion can be made.
Women are at high risk of ectopic pregnancy if they have pelvic pain, a palpable adnexal mass, an adnexal mass suspicious for ectopic pregnancy on ultrasound, or an hCG level higher than 2000 mlU/ml and the absence of a gestational sac on ultrasound prior to curettage. They should be assessed and treated accordingly.
PROBLEMS AND COMPLICATIONS
Difficult dilation
With early pregnancies, especially in the young nulliparous woman, the cervical canal may be quite narrow, tortuous, and resistant to dilation. The exocervix may be small, with little space for the tenaculum or stabilizer to be applied. Flexible cannulas of the Karman design may be advantageous; sometimes the 4 mm cannula can be inserted as a flexible sound, and this can be followed with a 5 mm and then a 6 mm cannula to evacuate the uterus. Rigid instruments are avoided altogether with this approach. However, on occasion a curved rigid cannula may pass more easily through the cervical canal. If the pregnancy is beyond 8 menstrual weeks, the 6 mm cannula may not consistently evacuate all of the gestational tissue. Therefore, the operator could use rigid dilators after first probing the cervical canal with the smaller cannula. Another option is to insert a laminaria tent and perform the abortion the next day. Misoprostol would produce cervical softening and dilation within 3 hours.85 Mifepristone, use 24 hours or more before abortion, will also results in softening and dilation.86 A less desirable option is to delay the abortion a week to await greater cervical softening.
Vasovagal reaction
In some women, manipulation of the cervix induces a marked vagal response with bradycardia, hypotension, and possibly syncope. If the patient loses consciousness, a tonic–clonic movement may be seen that can be confused with a convulsion. This syndrome has been seen with insertion of intrauterine contraceptive devices and may also be seen with venipuncture and other procedures in susceptible men as well as women. When it occurs during cervical dilation, vasovagal reaction must be distinguished from local anesthetic toxicity. With a vasovagal response the pulse is initially quite slow but rapidly returns to normal as the patient regains consciousness, a very different picture from the loss of consciousness, convulsions, and cardiovascular collapse of local anesthetic toxicity. If the patient begins to lose consciousness during cervical manipulation, the surgeon should immediately stop the painful stimulus, give atropine 0.4–1.0 mg intravenously or subcutaneously, turn the patient to a more comfortable position, and then monitor vital signs while the patient recovers. When the patient has fully recovered, the abortion procedure may be safely resumed.
Inability to evacuate the pregnancy and failed abortion
Failed abortion is a continuing pregnancy, whether recognized immediately or on another day. Before attempting a second procedure, the operator should consider the possibility of a uterine anomaly, multiple gestation, ectopic pregnancy, or gestation larger than expected.70, 81, 87, 88, 89 Usually a repeat ultrasound is indicated.
In a very retroverted or very anteverted uterus the pregnancy may be difficult to reach with the usual instruments. If the pregnancy is located at the fundus, the posterior wall of a retroverted uterus, or the anterior wall of an anteverted uterus, it may not be reached by the minimal curve of the cannula. Using a shorter speculum and straightening the cervix is helpful, as is ultrasound guidance. The flexible vacurettes are longer than rigid ones and may more readily follow the curve of the uterine wall to reach the gestation. A polyp forceps or curette bent into an appropriate curve may loosen the pregnancy, and suction can then remove the remainder. Contracting the uterus with a prostaglandin or oxytocic may straighten the axis of the uterus. Intraoperative ultrasound to ensue complete removal may be helpful.
When the uterus is distorted by fibroids, septa, or other anomalies, the pregnancy may be difficult to feel or to reach with any instrument. Ultrasound guidance is essential in this situation. If the uterine cavity is elongated, a flexible cannula, which is longer than a rigid cannula, may reach the pregnancy as noted above.
Pregnancy more advanced than anticipated
When a more advanced gestation is encountered, the outcome depends on several circumstances: the point in the procedure at which discovery of the more advanced gestation occurs, the operator's skill and experience, the available instruments, and staff support. If the advanced gestational age is diagnosed because the cannula is inserted to its full length and the fetal membranes remain intact, it is best to stop the procedure and reconsider. The use of ultrasound in borderline situations is strongly recommended. Where the procedure is already begun, the membranes are ruptured, and the tissue is partly removed, the decision is more difficult. An operator skilled in first-trimester abortion should be able to complete a 13–15 week abortion using the 12 mm vacuum cannula and standard ring forceps (Foerster) under local anesthesia in a freestanding clinic. Halting for 3–4 hours to treat the patient with buccal or sublingual misoprostol 400 µg will make the procedure easier and probably safer. If the error in sizing is not appreciated until some fetal parts have been extracted, measurement of the fetal foot will reveal the true gestational age (Table 2).
Management of gestations beyond 15 weeks varies depending on the availability of proper instruments and a surgeon skilled with more advanced procedures. Surgical abortion in the middle trimester, intentionally performed by experienced operators after cervical preparation with laminaria or misoprostol, has been shown to be a safe procedure.20 However, gestational age beyond 12 weeks is a predictor of uterine perforation, excessive blood loss, and incomplete abortion.12, 13 The difference may be in preparation: a procedure with adequate dilation, instrumentation, and operator experience may have a better outcome than aborting a midtrimester pregnancy by accident. If no one experienced in later procedures is available, transfer of the patient to a hospital or other facility, for either prostaglandin induction or cervical dilation and uterine evacuation is indicated.
Bleeding during and after abortion
Most women have minimal bleeding during first trimester abortion, and bleeding in excess of 100 ml is uncommon with abortion under paracervical block.3, 12 Uterine atony is the most likely cause of heavy and prolonged bleeding.90 Intracervical or intravenous ergonovine (0.2 mg) or oxytocin (10–20 units) should be used to contract the uterus. An alternative is buccal or oral misoprostol, 400 μg; doses as high as 1000 μg have been used rectally for postpartum atony.90 Prostaglandin F (Hemabate) can be given intramuscularly or into the uterus. In the absence of an obvious cervical or uterine injury, the operator should complete the abortion, evacuating the uterus rapidly but gently. The uterus is then massaged between two hands. The aspirated tissue is examined to confirm gestational age and to confirm that all fetal parts have been removed. If the bleeding does not stop, the cervix should be rechecked for a laceration or for bleeding from the tenaculum site. Next, the uterus is gently explored with a sharp curette, preferably under ultrasound guidance, checking for uterine shape and size, retained tissue, and uterine wall irregularities or defects. Repeat suction may remove clots and retained tissue and allow the uterus to contract. If bleeding persists after the uterus has been emptied, the next maneuver is tamponade: inserting a Foley urinary catheter with a 30 cc balloon then inflating the balloon to 60 ml.91, 92 If bleeding persists despite the tamponade, cervical or uterine laceration or disseminated intravascular coagulopathy are to be expected and the patient should be stabilized with intravenous fluids and transferred to hospital.
Bleeding in the postabortion period may indicate a hematometra or postabortal syndrome; this can occur immediately or up to several days later. Hematometra is a variant of uterine atony in which the uterus is distended with clots that are not expelled; the distention makes it difficult for the uterus to contract effectively, and may result in severe cramping.93 Treatment is repeat uterine evacuation and uterotonic drugs.
More serious causes of bleeding include uterine injury, placenta accreta/increta, arteriovenous malformation, and coagulopathy. These situations are rare but may not respond to uterine contraction. Treatments include reversal of coagulopathy if possible; coagulopathy may start to resolve when uterine atony or incomplete abortion is treated and the uterus can contract. Other treatments include pelvic artery embolization, open ligation of bleeding points, and hysterectomy as a last resort. The rate of hysterectomy for abortion-related hemorrhage, including second-trimester procedures, is 1 in 10,000;94 rates in first-trimester procedures would be expected to be lower than second-trimester procedures.
Suspected perforation
Uterine perforation during the performance of abortion is a potentially serious complication that can result in hemorrhage or visceral injury. Reported rates of perforation range from fewer than 1 to 3 per thousand abortions14, 60, 95, 96, 97, 98, 99, 100, 101, 102 and become more frequent with increasing gestational age.95 However, Kaali and associates99 reported a rate of 15 per thousand in a setting where laparoscopic sterilization was performed immediately after abortion; they concluded that perforations are frequently unrecognized and frequently benign. Many perforations are thought to occur during sounding or dilation because the most common site of perforations is the junction of the cervix and the lower uterine segment.99 Lateral perforation at this location may be particularly hazardous for the patient in that branches of the uterine artery can be lacerated with resultant hemorrhage,99 whereas midline perforations may be benign unless other organs are injured.
Perforation can be suspected when no tissue is obtained, when instruments are inserted deeper than expected, when ultrasound shows instruments outside the uterus, when hemorrhage occurs, or when obviously maternal tissues such as omentum are obtained. Treatment of perforation depends on the expected location, the woman's vital signs and condition, and whether the abortion is complete. Some authors have reported rates of operative evaluation and treatment as high as 80–100%;95, 96, 103 other authors do not advocate routine laparoscopy or even hospitalization.98, 100 When the uterus is already empty before a perforation is first suspected and the perforation is thought to be midline, then bleeding is unlikely and hospitalization may not be necessary. The woman can be observed for several hours. If the pain and bleeding continue to be minimal, repeated pelvic examinations are negative, and vital signs and repeat hematocrit are stable, then the patient may be given the telephone contact information, scheduled for a repeat examination the next day, and allowed to go home in the company of a responsible adult. Under any other circumstance, she should be admitted to a hospital for observation and possible laparoscopy. If the abortion is not complete at the time perforation is suspected, it should be completed with the aid of ultrasound or laparoscopy.
Incomplete abortion
Incomplete abortion may occur in 0.5–2% of surgical abortions;60 the rate depends on the operator's skill, the gestational age, and the criteria used to make the diagnosis. Although incomplete procedures were thought to be more common after abortion performed before 8 weeks, more recent reports do not support this concept.81 Typically the woman returns several days after the abortion with increased bleeding and cramping. On examination she may have an enlarged uterus or tissue visible in the cervical os, but often examination is unrevealing. Serum hCG levels are not often helpful; they are invariably positive, and a steep decline does not rule out an incomplete abortion. Ultrasound is generally not helpful: blood and debris are present in the uterus, and the amount of retained tissue may be small.
Treatment of incomplete abortion may be pharmacologic: uterotonic drugs such as methylergonovine (Methergine) or misoprostol may contract the uterus and expel the residual tissue. This method is appropriate when the amount of retained tissue is small, if the diagnosis is uncertain between incomplete abortion and retained blood clots, and if there is no sign of infection. If this route is chosen, the woman should be contacted within a few days to make sure that her symptoms have resolved.
If the uterus is tender, infection is a possibility, the amount of retained tissue is large, or the woman cannot return for follow-up, then repeat suction should be done. Repeat suction is usually easy because the cervix is dilated, and a cannula smaller than that used for the original procedure is adequate. If infection is possible, then antibiotics should definitely be used, and some operators prefer to use antibiotics after a repeat curettage for any reason.
Endometritis
Rates of postabortion endometritis of women undergoing first-trimester surgical abortion range from fewer than 0.5% to 5%;12, 13, 14, 60, 61, 62, 63, 64, 65, 67, 68, 69, 66 the incidence depends on the patient population, the incidence of other genital infections, and characteristics of the abortion, such as the use of general anesthesia. Typically the woman returns 3 or 4 days after the procedure with increased cramping and bleeding, sometimes accompanied by fever or nausea. Such symptoms 1 or 2 days after abortion may be due to β-hemolytic streptococci. On examination, the uterus is tender and usually slightly enlarged. Because of the normal or increased bleeding, cervical discharge usually cannot be evaluated. Endometritis should be treated immediately to avoid progression of infection, but if it is treated early, outpatient treatment should be sufficient. Early-onset endometritis (1 or 2 days) should be treated with an antibiotic effective against β-hemolytic streptococci, such as ampicillin. Other untreated infections, such as chlamydia or bacterial vaginosis, should be considered in the treatment plan. There are limited data about treatment of post-abortal endometritis; many people use the CDC guidelines for treatment of pelvic inflammatory disease.104 When oral treatment is preferred, other options are the combination of oral metronidazole and doxycycline or of metronidazole and ofloxacin.
If the woman has an incomplete abortion with endometritis, then repeat aspiration is necessary, preferably after the first dose of antibiotics has been given. In an outpatient setting, intramuscular ceftriaxone is often available and provides antibiotic coverage for the aspiration; oral antibiotics can be started afterward. Repeat aspiration of all women with endometritis appears to be a common practice; the utility of this approach has not been shown, however, and excessive curettage in the face of infection has the potential for endometrial damage.
Amenorrhea and cervical agglutination
Cervical agglutination occurs when the endocervical mucosa heals with obstruction of the cervical canal, resulting in amenorrhea and possibly cyclic cramping.105 This may be associated with vigorous suctioning of the lower uterine segment and cervix. It is distinguished from cervical stenosis, such as occasionally follows cone biopsy, in that with cervical agglutination damage to the underlying stroma is unlikely. Cervical agglutination is easily treated by passing a small sound through the cervical canal. This rarely needs repetition.
POSTABORTAL CONTRACEPTION
Abortion care should always include contraceptive counseling and services. Separating the services and expecting the patients to make another visit, probably to a different clinic, often results in no contraception being provided and recurrence of unwanted pregnancy. The pre-procedure patient information session can educate the patient about contraceptive options. Most abortion patients accept immediate postabortal contraception. Many receive intrauterine devices inserted right after the abortion, 106 immediate placement of a subdermal rod, intramuscular depomedroxyprogesterone acetate, or are supplied with hormonal contraceptive pills, patches or the vaginal ring. There is evidence that women using an intrauterine device placed immediately after abortion are less likely to have a repeat abortion.107
FOLLOW-UP
In the past all patients were scheduled for a follow up visit 1–2 weeks after abortion. Many do not keep the appointments. A review by Grossman and colleagues pointed out that severe complications usually must be dealt with sooner than these routine visits, that the inconvenience and cost to the patients of travel, lost wages and child-care expenses are not inconsequental.108 They advocated simple instructions and advice about detecting complications and telephone contact as sufficient for most patients. Twenty four hour a day emergency services are essential for the small number of women who do develop complications.
REFERENCES
Devereux G: A Study of Abortion in Primitive Societies, rev ed. New York, International Universities Press, 1976:27 |
|
Van der Vlugt T, Piotrow PT: Menstrual regulation. Popul Rep (F), No. 3, June 1973 |
|
Novak F, Andolsek L: Comparison of the medical effects of induced abortion by two methods, curettage and vacuum aspiration. The Ljubljana Abortion Study, 1971-1973. National Institutes for Health, Center for Population Research, 1974:41 |
|
Jones RK, Kooistra K: Abortion incidence and access to services in the United States, 2008. Perspect Sex Reprod Health. 2011 Mar;43(1):41-50. doi: 10.1363/4304111. Epub 2011 |
|
Koonin LM, Strauss LT, Chrisman CE, Parker WY: Abortion surveillance—United States, 1997. MMWR 49: 1, 2000 |
|
Jones, RK, et al. Abortion in the United States: incidence and access to services, 2005. Perspectives on Sexual and Reproductive Health, 2008;40(1):6-16. |
|
Koonin LM, Smith JC, Ramick M, Strauss LT: Abortion surveillance—United States, 1995. MMWR 47: 31, 1998 |
|
Koonin LM, Smith JC, Ramick M et al: Abortion surveillance—United States, 1993 and 1994. MMWR 46: 37, 1997 |
|
Koonin LM, Smith JC, Ramick M, Green CA: Abortion surveillance—United States, 1992. MMWR 45: 1, 1996 |
|
Koonin LM, Smith JC, Ramick M: Abortion surveillance—United States, 1990. MMWR 42: 29, 1993 |
|
Strauss, LT, Gamble SR, Parker WY,Cook DA, Zane SB, Hamdan S; Centers for Disease Control and Prevention, Abortion Surveillance-United States, 2004. Surveillance Summaries, Nov. 23, 2007, MMWR 2007;56(No. SS-9) |
|
Tietze C, Lewit S: Joint Program for the Study of Abortion (JPSA): Early medical complications of legal abortion. Stud Fam Plann 3: 97, 1972 |
|
Grimes DA, Cates W: Complications from legally-induced abortion: A review. Obstet Gynecol Surv 34: 177, 1979 |
|
Hakim-Elahi E, Tovell HMM, Burnhill MS: Complications of first-trimester abortion: A report of 170,000 cases. Obstet Gynecol 76: 129, 1990 |
|
Lawson HW, Frye A, Atrash HK et al: Abortion mortality: United States, 1972 through 1987. Am J Obstet Gynecol 171: 1365, 1994 |
|
Bartlett L, Berg CJ, Shulman HB, Zane SB, Green CA, Whitehead S, Atrash HK. Risk factors for legal induced abortion-related mortality in the Unites States. Obstet Gynecol 2004;103:729-37. |
|
WHO. Unsafe abortion: Global and regional estimates of incidence of unsafe abortion and associated mortality in 2000, 4th Edition. Geneva, WHO, 2004 |
|
Raymond EG, Grimes DA: The comparative safety of legal induced abortion and childbirth in the UnitedStates. Obstet Gynecol. 2012 Feb;119(2 Pt 1):215-9. |
|
Goldberg AB, Dean G, Kang MS, Youssoff S, Darney PD. Manual versus electric vacuum aspiration for early first trimester abortion: a controlled study of complication rates. Obstet. Gynecol. 2004;103:101-7. |
|
Castleman LD, Oanh KT, Hyman AG et al: Introduction of the dilation and evacuation procedure for second-trimesterabortion in Vietnam using manual vacuum aspiration and buccal misoprostol. Contraception. 2006 Sep;74(3):272-6. Epub 2006 May 30. |
|
Stim EM: Soft curettage for first-trimester pregnancy termination: A single-institution experience. In Zatuchni GI, Sciarra JJ, Speidel JJ (eds):Pregnancy Termination: Procedures, Safety, and New Developments. Hagerstown, MD, Harper & Row, 1979:112 |
|
World Health Organization Task Force of Sequelae of Abortion, Special Programme of Research, Development and Research Training in Human Reproduction: Comparison of rigid and flexible cannulae for early abortion without cervical dilation. Studies Fam Plann 15:79, 1984 |
|
Williamson D: Resources for abortion providers. In Paul M, Lichtenberg ES, Borgatta L, Grimes D, Stubblefield P (eds): A Clinician's Guide to Medical and Surgical Abortion. New York, Churchill-Livingstone, 1999:286 |
|
Bozorgi N: Statistical analysis of first-trimester pregnancy termination in an ambulatory surgical center. Am J Obstet Gynecol 127: 763, 1977 |
|
Gold J, Schulz KF, Cates W Jr, Tyler CW: The safety of laminaria and rigid dilators for cervical dilation before suction curettage for first-trimester abortion: A comparative analysis. In Naftolin G, Stubblefield PG (eds): Dilation of the Uterine Cervix: Connective Tissue Biology and Clinical Management, p 363. New York, Raven Press, 1980 |
|
Schulz KF, Grimes, DA, Cates W: Measures to prevent cervical injury during suction curettage abortion. Lancet 1: 1182, 1983 |
|
Fox MC, Hayes JL: Cervical preparation for second-trimester surgical abortion prior to 20 weeks ofgestation. Contraception. 2007 Dec;76(6):486-95. Epub 2007 Nov 9. |
|
Allen RH, Goldberg AB: Cervical dilation before first-trimester surgical abortion (<14 weeks'gestation). SFP Guideline 20071. Contraception. 2007 Aug;76(2):139-56. Epub 2007 Jul 10. |
|
Kline SB, Meng H, Munsick RA: Cervical dilation from laminaria tents and synthetic osmotic dilators used for 6 hours before abortion. Obstet Gynecol 86: 931, 1995 |
|
Kirton KT: Use of prostaglandins in dilation of the cervix. In Naftolin F, Stubblefield PG (eds): Dilation of the Uterine Cervix: Connective Tissue Biology and Clinical Management, p 355. New York, Raven Press, 1980 |
|
Vimala N, Mittal S, Dadhwal V: Cervical priming with sublingual misoprostol vs. 15-methyl-prostaglandin F2alphaprior to surgical abortion. Int J Gynaecol Obstet. 2005 Feb;88(2):134-7. Epub 2004 Dec 8. |
|
Ngai SW, Yeung KC, Lao T, Ho PC: Oral misoprostol versus vaginal gemeprost for cervical dilation before vacuum aspiration in women in the sixth to twelfth week of gestation. Contraception 51: 347, 1995 |
|
Celentano C, Prefumo F, Di Andrea O et al: Oral misoprostol vs. vaginal gemeprost prior to surgical termination of pregnancyin nulliparae. Acta Obstet Gynecol Scand. 2004 Aug;83(8):764-8. |
|
Bugalho A, Bique C, Almeida L, Bergstrom S: Application of vaginal misoprostol before cervical dilation to facilitate first-trimester pregnancy interruption. Obstet Gynecol 83: 729, 1994 |
|
Ngai SW, Chan YM, Tang OS, Ho PC: The use of misoprostol for pre-operative cervical dilation before vacuum aspiration: A randomized trial. Hum Reprod 14: 2139, 1999 |
|
Singh K, Fong YF, Prasad RN, Dong F: Evacuation interval after vaginal misoprostol for preabortion cervical priming: A randomized trial. Obstet Gynecol 83: 431, 1994 |
|
Saxena P, Sarda N, Salhan S et al: A randomised comparison between sublingual, oral and vaginal route of misoprostollocal anaesthesia. Aust N Z J Obstet Gynaecol. 2008 Feb;48(1):101-6. |
|
MacIsaac L, Grossman D, Balistreri E, Darney PD: A randomized controlled trial of laminaria, oral misoprostol, and vaginal misoprostol before abortion. Obstet Gynecol 93: 766, 1999 |
|
LeFebre Y, Proulx L, Elie R et al: The effects of RU38486 on cervical ripening. Am J Obstet Gynecol 162: 61, 1990 |
|
Carbonell JL, Gallego FG, Llorente MP et al: Vaginal vs. sublingual misoprostol with mifepristone for cervical priming intrial. Contraception. 2007 Mar;75(3):230-7. Epub 2007 Jan 16. |
|
Smith GM, Stubblefield PG, Churchirillo L, McCarthy MJ: Pain of first-trimester abortion: Its quantifications and relations with other variables. Am J Obstet Gynecol 133: 489, 1979 |
|
Belanger E, Melzack R, Lauzon P: Pain of first-trimester abortion: A study of psychosocial and medical predictors. Pain 36: 339, 1989 |
|
Stubblefield PG: Control of pain for women undergoing abortion. Int J Gynaecol Obstet Suppl 3: 131, 1989 |
|
Borgatta L, Nickinovich D: Pain during early abortion. J Reprod Health 42: 287, 1997 |
|
Suprato K, Reed S. Naproxen sodium for pain relief in first-trimester abortion. Am J Obstet Gynecol 1984;150:1000-1. |
|
Keder LM: Best practices in surgical abortion. Am J Obstet Gynecol. 2003 Aug;189(2):418-22. |
|
Grimes DA, Schulz KF, Cates W Jr, Tyler CW: Local versus general anesthesia: Which is safer for performing suction curettage abortions? Am J Obstet Gynecol 135: 1030, 1979 |
|
Peterson HB, Grimes DA, Cates W Jr et al: Comparative risk of death from induced abortion at 12 weeks or less gestation performed with local versus general anesthesia. Am J Obstet Gynecol 41: 763, 1981 |
|
Renner RM, Nichols MD, Jensen JT et al: Paracervical block for pain control in first-trimester surgical abortion: arandomized controlled trial. Obstet Gynecol. 2012 May;119(5):1030-7. |
|
Grimes DA, Cates WJ: Deaths from paracervical anesthesia used for first-trimester abortion, 1972-1975. N Engl J Med 295: 1397, 1976 |
|
Nichols M, Halvorson-Boyd G, Goldstein R, Gevirtz C, Healow D. Pain management. In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinen MD (eds): Management of unintended and abnormal pregnancy: comprehensive abortion care. Wiley-Blackwell, Hoboken, New Jersey, 2009:90-110.. |
|
Schulz KF, Grimes DA, Christensen DD: Vasopressin reduces blood loss from second-trimester dilatation and evacuation abortion. Lancet 2: 353, 1985 |
|
Stubblefield PG: Surgical techniques of uterine evacuation in first- and second-trimester abortion. Clin Obstet Gynecol 13: 53, 1986 |
|
Nygaard IH, Valbo A, Heide HC et al: Is oxytocin given during surgical termination of first trimester pregnancyuseful? A randomized controlled trial. Acta Obstet Gynecol Scand. 2011 Feb;90(2):174-8. doi: |
|
Glick E: Surgical Abortion, pp 17–22. Reno, Nevada, West End Women's Medical Group, 1998 |
|
Weibe ER: Comparison of the efficacy of different local anesthetic techniques and techniques of local anesthesia in therapeutic abortions. Am J Obstet Gynecol 167: 131, 1992 |
|
Marc I, Rainville P, Masse B et al: Women's views regarding hypnosis for the control of surgical pain in the contextof a randomized clinical trial. J Womens Health (Larchmt). 2009 Sep;18(9):1441-7. |
|
Guerrero JM, Castano PM, Schmidt EO et al: Music as an auxiliary analgesic during first trimester surgical abortion: arandomized controlled trial.group (p=.65).Contraception. 2012, epub ahead of print. |
|
Yuen BH, Callegari: Occurrence of molar pregnancy in patients undergoing elective abortion: Comparison with other clinical presentations. Am J Obstet Gynecol 154: 273, 1986 |
|
Lichtenberg ES, Grimes DA. Surgical complications: Prevention and management. In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinen MD (eds): Management of unintended and abnormal pregnancy: comprehensive abortion care. Wiley-Blackwell, Hoboken, New Jersey, 2009:224-251. |
|
Hodgson JE, Major B, Partmann K, Quattlebaum FW: Prophylactic use of tetracycline for first-trimester abortions. Obstet Gynecol 45: 574, 1975 |
|
Levallois P, Rioux JE: Prophylactic antibiotics for suction curettage abortion: Results of a clinical controlled trial. Am J Obstet Gynecol 158: 100, 1988 |
|
Moller BR, Ahrons S, Laurin J, Mardh PA: Pelvic infection after elective abortion associated with Chlamydia trachomatis. Obstet Gynecol 59: 210, 1982 |
|
Sorensen JL, Thranov I, Hoff G et al: A double-blind randomized study of the effect of erythromycin in preventing pelvic inflammatory disease after first-trimester abortion. Br J Obstet Gynecol 99: 434, 1992 |
|
Darj E, Strain EB, Nilsson S: The prophylactic effect of doxycycline on postoperative infection rate after first-trimester abortion. Obstet Gynecol 70: 755, 1987 |
|
Sawaya GF, Grady D, Kerlikowske K, Grimes DA: Antibiotics at the time of induced abortion: The case for universal prophylaxis based on meta-analysis. Obstet Gynecol 86: 884, 1996 |
|
Brewer C: Prevention of infection after abortion with a supervised single dose of oral doxycycline. Lancet 281: 780, 1980 |
|
Larrson PG, Platz-Christensen JJ, Theijls H et al: Incidence of pelvic inflammatory disease after first-trimester legal abortion in women with bacterial vaginosis after treatment with metronidazole: A double-blind, randomized trial. Am J Obstet Gynecol 166: 100, 1992 |
|
Heisterberg L, Petersen K: Metronidazole prophylaxis in elective first trimester abortion. Obstet Gynecol 65: 371, 1985 |
|
Edwards J, Carson SA: New technologies permit safe abortion at less than six weeks' gestation and provide timely detection of ectopic pregnancy. Am J Obstet Gynecol 176: 1101, 1997 |
|
: ACOG Practice Bulletin No. 74. Antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2006 Jul;108(1):225-34. |
|
Dajani AS, Taubert KA, Wilson W et al:. Prevention of bacterial endocarditis: Recommendations by the American Heart Association. JAMA 277:1794, 1997 |
|
Glick E: Surgical Abortion, pp 2–43. Reno, Nevada, West End Women's Medical Group, 1998 |
|
Hern WM: Abortion Practice, pp 108–122. Philadelphia, JB Lippincott, 1990 |
|
Darney PD, Horbach NS, Korn AP: First-trimester elective abortion. In:Protocols for Office Gynecologic Surgery, pp 158–193. Cambridge, MA, Blackwell Science, 1996 |
|
Meckstroth K, Paul M: First trimester aspiration abortion. In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinen MD (eds): Management of unintended and abnormal pregnancy: comprehensive abortion care. Wiley-Blackwell, Hoboken, New Jersey, 2009:135-156. |
|
Castadot RG: Pregnancy termination: Techniques, risks, and complications and their management. Fertil Steril 45: 5, 1986 |
|
Chen LH, Lai SF, Lee WH, Leong NK: Uterine perforation during elective first-trimester abortions: A 13-year review. Singapore Med J 36: 63, 1995 |
|
Molin A: Risk of damage to the cervix by dilation for first-trimester induced abortion by suction aspiration. Gynecol Obstet Invest 35: 152, 1993 |
|
Johnstone FD, Beard RJ, Boyd IE, McCarthy TG: Cervical diameter after suction termination of pregnancy. Br Med J 1: 68, 1976 |
|
Fielding WL, Lee SY, Borten M, Friedman EA: Continued pregnancy after failed first-trimester abortion. Obstet Gynecol 63: 421, 1984 |
|
Paul M, Lackie E, Mitchell C et al: Is pathology examination useful after early surgical abortion? Obstet Gynecol. 2002 Apr;99(4):567-71. |
|
Johnson MP, Drugan A, Koppitch FC et al: Postmortem chorionic villus sampling is a better method for cytogenetics evaluation of early fetal loss than culture of abortus material. Am J Obstet Gynecol 163: 1505, 1990 |
|
Edwards J, Creinin MD: Surgical abortion for gestations of less than 6 weeks. Curr Probl Obstet Gynecol 20: 11, 1997 |
|
Allen RH, Goldberg AB: Cervical dilation before first-trimester surgical abortion (<14 weeks'gestation). SFP Guideline 20071. Contraception. 2007 Aug;76(2):139-56. |
|
Ashok PW, Flett GM, Templeton A: Mifepristone versus vaginally administered misoprostol for cervical priming Am J Obstet Gynecol. 2000;183:998-1002. |
|
Kaunitz AM, Rovira EZ, Grimes DA, Schulz KF: Abortions that fail. Obstet Gynecol 66: 533, 1985 |
|
Zorlu CG, Aral K, Ekici E et al: Causative factors in first trimester abortion failure. Advan Contraception 12: 63, 1996 |
|
Pennes DR, Bowerman RA, Silver TM, Smith SJ: Failed first-trimester pregnancy termination: Uterine anomaly as etiologic factor. J Clin Ultrasound 15: 165, 1987 |
|
Sands RX, Burnhill MS, Hakim-Elahi E: Postabortal uterine atony. Obstet Gynecol 43: 595, 1974 |
|
Kauff ND, Chelmow D, Kawada CY: Intractable bleeding managed with Foley catheter tamponade after dilation andevacuation. Am J Obstet Gynecol. 1995 Sep;173(3 Pt 1):957-8. |
|
De Loor JA, van Dam PA: Foley catheters for uncontrollable obstetric or gynecologic hemorrhage. Obstet Gynecol. 1996 Oct;88(4 Pt 2):737. |
|
Valle RF, Sabbagha: Management of first-trimester pregnancy termination failures. Obstet Gynecol 55: 625, 1980 |
|
O'Brien P, El-Refaey H, Gordon A et al: Rectally administered misoprostol for the treatment of postpartum hemorrhage unresponsive to oxytocin and ergometrine: A descriptive study. Obstet Gynecol 92: 212, 1998 |
|
Grimes DA, Schulz KF, Cates WJ: Prevention of uterine perforation during curettage abortion. JAMA 251: 2108, 1984 |
|
Grimes DA, Flock ML, Schulz KF et al: Hysterectomy as treatment for complications of legal abortion. Obstet Gynecol 63: 461, 1984 |
|
Ameling R, Tews L, Dudley S: Abortion training in U.S. obstetrics and gynecology residency programs, 1998. Fam Plann Perspect 32: 268, 2000 |
|
Lauerson NH, Birnbaum S: Laparoscopy as a diagnostic and therapeutic technique in uterine perforations during first-trimester abortions. Am J Obstet Gynecol 167: 522, 1974 |
|
Kaali SG, Szigetvari IA, Bartfai GS: The frequency and management of uterine perforations during first-trimester abortions. Am J Obstet Gynecol 161: 406, 1989 |
|
Berek JS, Stubblefield PG: Anatomic and clinical correlates of uterine perforation. Am J Obstet Gynecol 135: 181, 1979 |
|
Lindell G, Flam F. Management of uterine perforations in connection with legal abortions. Acta Obstet Gynecol Scand 74:373, 1995 |
|
Goldchmit R, Zalel Y, Elchalal U et al: Management of uterine perforation complicating first-trimester termination of pregnancy. Isr J Med Sci 31: 232, 1995 |
|
Mittal S, Misra SL: Uterine perforation after medical termination of pregnancy by vacuum aspiration. Int J Gynaecol Obstet 23: 45, 1985 |
|
Workowski KA, Berman S: Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010 Dec 17;59(RR-12):1-110. |
|
Hakim-Elahi E: Postabortal amenorrhea due to cervical stenosis. Obstet Gynecol 48: 723, 1976 |
|
Grimes D, Schulz K, Stanwood N: Immediate postabortal insertion of intrauterine devices. Cochrane Database Syst Rev. 2002;(3):CD001777. |
|
Roberts H, Silva M, Xu S: Post abortion contraception and its effect on repeat abortions in Auckland, NewZealand. Contraception. 2010 Sep;82(3):260-5. Epub 2010 Apr 14. |
|
Grossman D, Ellertson C, Grimes DA et al: Routine follow-up visits after first-trimester induced abortion. Obstet Gynecol. 2004 Apr;103(4):738-45. |