Adenomyosis
Authors
INTRODUCTION
Adenomyosis is a relatively common, although somewhat neglected, disorder of the female reproductive tract. Clinically, it is associated with heavy and painful periods, especially towards the end of the reproductive years; unfortunately these symptoms are shared with a number of other conditions and, until recently, an exact diagnosis could only be made at surgery and, in milder cases, it was exclusively based on the histological examination of the hysterectomy specimen. In this event, diagnosis of adenomyosis is made upon detection of endometrial glands and stroma within the myometrium, some distance away from the endo–myometrial junction. There are also smooth muscle changes associated with the main finding, although they are less obvious and difficult to quantify on routine histological examination.
It is noteworthy that the presence of epithelial and glandular structures within the peritoneal cavity and in the context of uterine leiomyomas has been known for at least 150 years. For decades, however, the vast majority of pathologists were at a loss as to the origin of these glandular entities and theories abounded as to their histogenesis. In spite of great uncertainty over their origin, all so-called "mucosal invasions" were considered as one entity and, until 1921, this new pathological entity – comprising what we would identify today as endometriosis and adenomyosis – was named "adenomyoma". Therefore, the early history of adenomyosis is interwoven with the early history of endometriosis.
Today, the term adenomyoma has a more restricted meaning, referring to a well-defined and circumscribed lesion localized in the myometrium, or sometimes protruding into the uterine cavity as a polypoid adenomyoma. Adenomyosis, however, may present itself in various disguises, ranging from simple thickening of the endo–myometrial junction to nodular or diffuse lesions involving the entire uterine wall.
Over the years, several articles have appeared describing the path that led first to the identification of adenomyoma and, later, to the separation of adenomyosis from endometriosis.1, 2, 3, 4, 5, 6 Investigating this process is not a purely academic exercise; on the contrary, it may help in identifying the natural history of adenomyosis, since today it is often impossible to observe the unquenched progression of the disease. Going back to the days when little if anything could be done to improve the situation can definitely help in understanding how this pathological condition may progress.
HISTORICAL PERSPECTIVE
The claim to have been the first to describe an adenomyoma was made by Iwanoff who, illustrating his case in 1898, reported that he had already published a paper in Russian with a microscopic evaluation of the glands found in a cystic myoma. In his view, these glands “were derived from the serosal epithelium”.7 Iwanoff, however, failed to provide a reference for his earlier paper and a search of the literature indicates that the first pathologist to have described a case of what was later named adenomyoma was Carl von Rokitansky in 1860, who found endometrial glands in the myometrium and designated this finding as “cystosarcoma adenoids uterinum”,8 obviously believing that the condition was malignant.
In 1999, Knapp,2 a medical historian, challenged the view that von Rokitansky was the first to describe an adenomyoma, claiming instead that the first, highly detailed description of the organic damage and constitutional symptoms currently identified as adenomyosis and endometriosis was produced in 1690 by the German physician, Daniel Schrön, in his thesis Disputatio Inauguralis Medica de Ulceribus Uteri.9 Knapp reported that several other late 17th and 18th century theses described cases of what we would today call endometriosis or adenomyosis. However, a careful reading of some of the original manuscripts from this period indicates that these alleged early descriptions evidenced signs of inflammation such as pus, uterine wounds or erosions that were linked to manipulation, abortion or a syphilitic lesion. The symptoms described were those of an infection and included pain, insomnia, fever, vaginal lesions, dysuria, purulent urine (if the lesion involved the bladder) or purulent stool (if the lesion involved the intestines). Sadly, Knapp passed away a few months after publication of his manuscript and a letter to the Editor of Fertility and Sterility questioning the findings remained without response.10
During the second half of the 19th century, a major controversy arose over the nature and origin of the lesions first described by von Rokitansky. The majority of researchers of the time favored the hypothesis proposed by von Recklinghausen11 that adenomyomas were the result of displacement of Wolffian or mesonephric vestiges. Von Recklinghausen distinguished two entirely separate entities: extra- and intrauterine adenomyomas, with only cases arising within the uterine wall possessing glands deriving from the uterine mucosa.
In 1903, Meyer presented his theory of the pathogenesis of adenomyomas. In his view, the condition is an example of “epithelial invasion of inflammatory infiltrated tissue”,12 that can occur in both dystopic (embryonic) and orthotopic (mature) epithelium. Among the founders of the “dystopic” theory was Orloff,13 who in 1895, describing “glandular spaces under the serosa covering uterine myomata”, considered them as arising from “embryonic cells”.
The first systematic description of what is today known as adenomyosis was made by an often forgotten pioneer, Thomas Stephen Cullen, an American gynecologist who made his first observations during the years 1893–1896.14 During this period he examined 1283 cases of myomas and found 73 adenomyomas, distinguished into interstitial, subperitoneal, and submucous. A decade later he published a detailed analysis of the presence of heterotopic epithelial cells, stroma, and glands15 within the myometrium in myomas. In his view, “In cases of adenomyoma of the uterus we usually find a diffuse myomatous thickening of the uterine muscle. This thickening may be confined to the inner layers of the anterior, posterior, or lateral walls, but in other cases the myomatous tissue completely encircles the uterine cavity. This diffuse myomatous tissue contains large or small chinks, and into these the normal uterine mucosa flows. If the chinks are small, there is only room for isolated glands, but where the spaces are goodly in size, large masses of mucosa flow into and fill them. We accordingly have a diffuse myomatous growth with normal mucosa flowing in all directions through it. The mucosa lining the uterine cavity is perfectly normal.” A notable feature of his description of uterine mucosa in the myometrium is that “sometimes its direct connection with the mucosa of the uterine cavity can be traced”.
Cullen,16 dedicated an entire book to adenomyomas of the uterus and provided the first ever classification of the condition. He distinguished three types:
1. Adenomyomas in which the uterus preserves a relatively normal contour;
2. Subperitoneal or intraligamentary adenomyomas;
3. Submucous adenomyomas.
He clearly described the effects of adenomyosis on the myometrium: “I found a uniformly enlarged uterus about four times the natural size. On opening it I found that the increase in size was due to a diffuse thickening of the anterior wall. Professor William H. Welch, when consulted, said that the condition was evidently a most unusual one and suggested that sections be made from the entire thickness of the uterine wall. Examination of these sections showed that the increase in thickness was due to the presence of a diffuse myomatous tumor occupying the inner portion of the uterine wall, and that the uterine mucosa was at many points flowing into the diffuse myomatous tissue.”
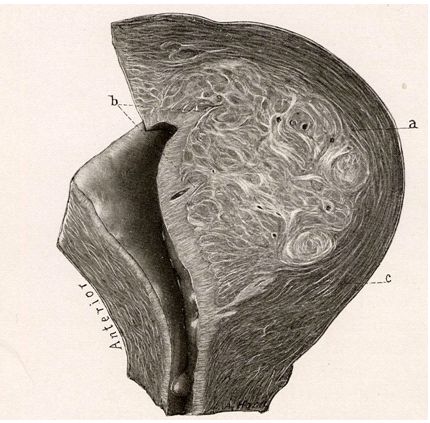
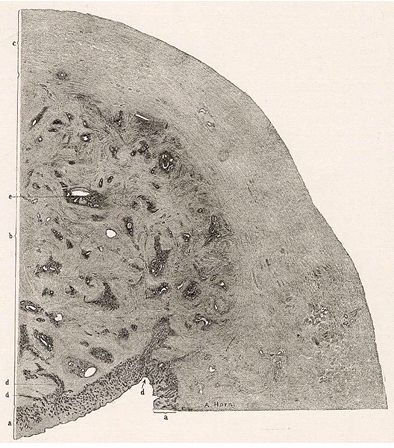
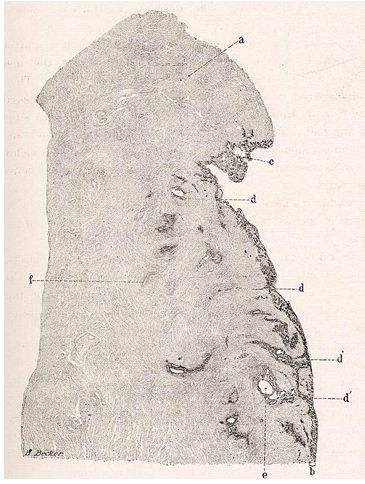
Although in the vast majority of cases, specimens he observed consisted of myomatous tissue clearly infiltrated by uterine mucosa (see Figs. 1–3), occasionally there were cases in which no visible myoma could be found (Fig. 4).
{kind=link}
Fig. 1. Drawing of a surgical specimen showing a large myoma with small lacunar spaces of infiltrated endometrium. (a) Myometrium surrounding the myoma; (b) areas where the endometrium is infiltrating the myoma; (c) a lacunar space well inside the myoma. (Cullen TS: Adenomyoma of the Uterus. Philadelphia & London, W.B. Saunders, 1908.)
{kind=link}
Fig. 2. Drawing of a surgical specimen showing the presence throughout the myometrium of endometrial glands. (a) Endometrium; (b) adenomyoma; (c) outer myometrium; (d) areas where the endometrium infiltrates the myometrium; (e) lacunar spaces within the myometrium. (Cullen TS: Adenomyoma of the Uterus. Philadelphia & London, W.B. Saunders, 1908.)
{kind=link}
Fig. 3. Drawing of a surgical specimen showing a more limited infiltration of endometrium into the myometrium. (a) Myometrium; (b) endometrium; (c) area of endometrial hyperplasia; (d) areas of endometrial infiltration; (d`) additional areas of endometriual infiltration; (e) lacunar space within the myometrium; (f) area of neoangiogenesis. (Cullen TS: Adenomyoma of the Uterus. Philadelphia & London, W.B. Saunders, 1908.)
{kind=link}
DEFINITION
In 1918, C. Lockyer, a British professor,17 wrote a comprehensive book in which he provided the following definition of adenomyomas: “the term ‘adenomyoma’ implies a new formation composed of gland-elements, hyperplastic cellular connective tissue, and smooth muscle.” There is a major difference between the definition given by Cullen, who clearly referred to adenomyosis only, and that of Lockyer, who considered adenomyomas part of a process (endometriosis!) involving a number of abdominal organs and stated: “so far as the adenomatous elements are concerned, the same type of tumour-formation can be found also in the digestive tract (bowel and stomach), and some observers claim that analogous conditions can exist in the gall-bladder, in the kidney, and elsewhere.”
Lockyer was among those who initially resisted the idea that the “islets” of epithelial tissue observed in various abdominal organs were endometrial in nature, although at the end of a long controversy – as Lockyer expressed it – there was a “gradual ascendancy of Cullen’s mucosal theory”. Among the early supporters of Cullen’s views was von Franqué18 who believed that epithelial growths found in a number of abdominal organs derived from the “mature mucous membrane of the uterus” that, somehow, had become capable of “infiltrating” other organs as a consequence of a process of inflammation.
In 1925, 2 years before Sampson19 created the word “endometriosis” to describe the presence of islets of uterine mucosa in the peritoneal cavity, Frankl20 created a name for the mucosal invasion of the myometrium and clearly described its anatomical picture. He called it “adenomyosis uteri” and explained “I have chosen the name of adenomyosis, which does not suggest any inflammatory genesis as do terms like adenometritis, adenomyositis, adenomyometritis, still employed. My own conception has been verified by the observations of various authors, among whom are Lahxn, Meyer, Schwarz, Schiller, and also supported by my more recent thirteen additional cases. We were never able to find any trace of an inflammatory infiltration, either in the musculature or in the mucosa of this region. In the histories of these patients, we did not find a single symptom suggesting a preceding puerperal or gonorrheal infection.”
Frankl was the first to clearly distinguish between adenomyosis and adenomyoma: “In an adenomyoma the glands originate independently within the myoma as an autochthonous growth, while in adenomyosis, even when localized, the direct connection of the endometrium with the islands of mucosa located in the musculature can be established in serial sections. In the majority of cases of genuine adenomyoma, which are extremely rare, the glands are not accompanied by stroma.”
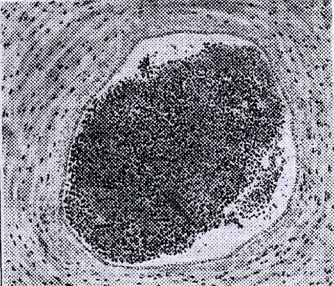
He also described similarities, but also differences between adenomyosis and endometriosis: “The entire material from thirty cases shows in twelve instances the presence of myomas, mostly of very small size, a fact which should not be overlooked. Eleven times we found the mucosa in a hyperplastic condition. The coincidence of small myomas is not so striking inasmuch as they are quite common in general, but the presence of a hyperplastic mucosa eleven times is noteworthy. The penetration of a hyperplastic mucosa into the myometrium can be readily understood if we assume for it a more marked tendency toward proliferation … An observation made only once should be mentioned, namely, the presence of blood in the glands within the myometrium. This finding was made in a woman of fifty years, who still was menstruating regularly. The last menstruation had occurred three weeks previous to operation. In a few glands, which were dilated cystically, we found only slightly changed blood. This observation reminds one of menstruating uterine mucosa on the surface of the ovary, first described by Sampson. By the courtesy of Sampson I had an opportunity of studying the original slides and I confirm that both in his and in my case, misplaced uterine glands were seen filled with blood, undoubtedly menstrual blood.”
{kind=link}
Fig. 5. Microscopic appearance of an endometrial focus in a patient with adenomyosis, at the time of menstruation. (This figure was published in Frankl O: Adenomyosis uteri. Am J Obstet Gynecol 10:680, 1925. Copyright Elsevier 1925, reproduced with permission.)
Figure 5 shows the case mentioned by Frankl about which he wrote: “The illustration will easily convince the reader of the close similarity between my picture and the one shown by Sampson.”
The current definition of adenomyosis was finally provided in 1972 by Bird21 who stated: “Adenomyosis may be defined as the benign invasion of endometrium into the myometrium, producing a diffusely enlarged uterus which microscopically exhibits ectopic non-neoplastic, endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium.” Today, the term adenomyosis should be restricted to the presence of glandular and stromal extensions of more than 2.5 mm below the endo–myometrial junction on low-power field.22
INCIDENCE
Whereas the incidence of endometriosis is estimated at between 6% and 10% of all women, and at 35–50% of women with pelvic pain and infertility,23 the incidence of adenomyosis is still under discussion because different imaging criteria are used. Kunz et al.24 found a prevalence of adenomyosis of 70% in women with endometriosis, compared to 9% in healthy controls. This contrasts with a previous study by Bazot et al.25 in which only 27% of women with pelvic endometriosis had adenomyosis on preoperative magnetic resonance imaging (MRI). Using this technique, De Souza et al.26 detected discrete and diffuse patterns of adenomyosis in 54% of young women with infertility and dysmenorrhea or menorrhagia.
DIAGNOSIS
In spite of early claims that a clinical identification of women suffering from adenomyosis was not only possible but even easy, for almost a century the diagnosis of adenomyoma and later of adenomyosis has been exclusively retrospective and based upon the opening of the uterine specimen after hysterectomy and a histological evaluation of its myometrium.
Over the past quarter of a century, however, new, modern diagnostic tools have substantially modified this reality, making a preoperative diagnosis, not only feasible, but also highly accurate.
Clinical diagnosis
Cullen27 provided a detailed clinical picture of what – as already mentioned – at the time were labeled adenomyomas, identifying two main symptoms: “lengthened menstrual periods” that – as the disease progresses – “may be replaced by a continuous hemorrhagic discharge”; and “a great deal of pain”. Contrary to Cullen’s assertion, today a clinical diagnosis of adenomyosis is considered practically impossible. Studying all cases admitted during 1 year for hysterectomy for any indication, Cocuzzi et al.28 found, over a total of 528 cases, an incidence of histologically certified adenomyosis of 11.2%. Out of these 59 patients, only in one woman did the clinical, surgical, and microscopical diagnosis coincide.
It is fair to say that Cullen admitted difficulties in arriving at a preoperative diagnosis. He wrote: “in the early years of our investigations we also failed to detect it clinically, but in the early and fairly advanced stages of the process so definite are the symptoms that the hospital assistant now frequently comes and says that a given case has all the signs of an adenomyoma and that he feels sure that this is the cause of the bleeding.”16
In a recently published study of a subset of the American Study of Women’s Health Across the Nation who had Hysterectomies, investigators tried to identify, in women undergoing the menopausal transition, possible symptoms specific for adenomyosis.29 Adenomyosis was found in 48% of 137 patients and in these women frequency of symptoms was similar to in those with and without evidence of adenomyosis. The same prevalence of fibroids was seen in the presence or absence of adenomyosis (37% versus 43%), endometriosis (3% versus 5%), abnormal bleeding (27% versus 33%), or chronic pelvic pain (12% versus 17%), respectively. They concluded that adenomyosis is an incidental finding, not the source of the symptomatology.
Parazzini et al.30 conducted a cross-sectional study on the frequency and risk factors for adenomyosis in women who underwent hysterectomy for benign gynecological conditions. A total of 820 women entered the study. Adenomyosis was identified in 231 women (28.2%, 95% confidence interval (CI) 24.6–32.5). The frequency of adenomyosis was similar in women with indication for surgery “fibroids/ menorrhagia” (143 cases, 28.5%), or “genital prolapse” (69 cases, 28.2%). The rate ratio (RR) of adenomyosis was 1.9 (95% CI 1.2–2.8) in women reporting one or more induced abortions, in comparison with those reporting no induced surgical abortion. Women with adenomyosis more frequently reported dysmenorrhea and chronic pelvic pain, but not dyspareunia. It seems therefore that adenomyosis is common in women who undergo hysterectomy and that it is more frequent among women reporting induced abortions, dysmenorrhea, and chronic pelvic pain.
To elucidate the clinical profile of adenomyosis in comparison with uterine leiomyomas, Taran et al.31 performed a retrospective case–control study involving 76 women undergoing hysterectomy with adenomyosis and 152 women with uterine leiomyomas but no adenomyosis. Comparing women undergoing hysterectomy for benign conditions with the sole pathologic finding of adenomyosis to women with leiomyomas alone, they found that adenomyosis was independently associated with younger age (41.1 years vs. 44.3 years), history of depression (57.1% vs. 24.7%), dysmenorrhea (65.7% vs. 42.3%), and pelvic pain (52.9% vs. 21.1%) in a multivariable unconditional logistic regression analysis compared with women with leiomyomas. Furthermore, in a second multivariate model analyzing all subjects with uteri weighing more than 150 g, women with adenomyosis were more likely to have a history of depression (52.6% vs. 22.2%) and endometriosis (26.3% vs. 2.8%) compared with women with leiomyomas. The authors concluded that women undergoing hysterectomy with a histological diagnosis of adenomyosis have a distinct symptomatology and medical history compared with women with leiomyomas and that better understanding of this disease is required to improve diagnosis and management.
Histology and hysteroscopy
As already stressed, adenomyosis has been an elusive diagnosis until recently due to the need for a histological confirmation on the hysterectomy specimen, which is based on the presence of endometrial glands and stroma within the myometrium, at some distance from the endo–myometrial junctional zone (see sections on Magnetic resonance imaging and The junctional zone and adenomyosis). While a myometrial needle biopsy may be highly specific for the diagnosis of adenomyosis, its sensitivity is too low to be useful in clinically suspected cases.32
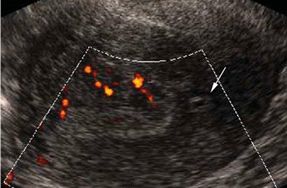
Diagnostic hysteroscopy does not provide pathognomonic signs for adenomyosis, although the presence of an irregular endometrium with endometrial defects, altered vascularization, and cystic hemorrhagic lesions can be possibly associated with the entity. In addition to the direct visualization of the uterine cavity, the hysteroscopic approach offers the possibility of obtaining endometrial/myometrial biopsies under visual control. For this reason, Molinas and Campo33 suggested that the combination of transvaginal sonography, fluid hysteroscopy, and contrast sonography can be a powerful tool for detecting endometrial and myometrial abnormalities in association with adenomyosis (Fig. 6).
{kind=link}
Transvaginal sonography
The advent of transvaginal sonography (TVS) in the 1980s substantially improved the ability to diagnose adenomyosis preoperatively. A Medline search of papers published in English showed that TVS is highly observer-dependent, but in the hands of experienced investigators has an adequate diagnostic accuracy in clinically suspected cases, but not in unselected premenopausal women with myomas.34
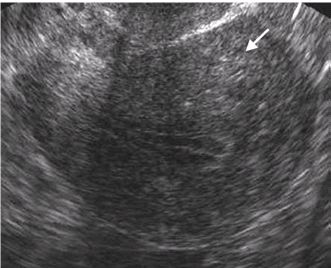
The most commonly observed TVS images characteristic of adenomyosis are those showing heterogeneous and hypoechogenic, poorly described areas in the myometrium. These areas may appear with or without anechoic lacunae or cysts of varying size, and the echo texture of the myometrium may be increased (Figs. 7–9).
{kind=link}
{kind=link}
Fig. 8. Sagittal transvaginal sonogram showing an enlarged retroflexed uterus with a heterogeneous myometrial echo texture (arrow). The shadowing over the lower uterus is an artifact related to vaginal air. (Reproduced with permission from Chopra S, Lev-Toaff AS, Ors F, Bergin, D. Adenomyosis: common and uncommon manifestations on sonography and magnetic resonance imaging. J Ultrasound Med 2006; 25:617–27. Courtesy of the American Institute of Ultrasound in Medicine.)
Fig. 9. Comparison between images obtained in a 48-year-old woman with a history of menorrhagia and the presence of myometrial cysts. (Reproduced with permission from Chopra S, Lev-Toaff AS, Ors F, Bergin D. Adenomyosis: common and uncommon manifestations on sonography and magnetic resonance imaging. J Ultrasound Med 2006;25:617–27. Courtesy of the American Institute of Ultrasound in Medicine.)
{kind=link}
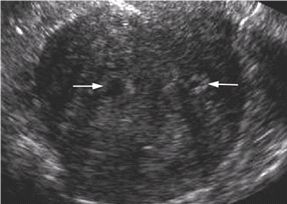
Fig. 9. (A) Sagittal transvaginal sonogram showing a heterogeneous echo texture with two large myometrial cysts (arrows) involving the anterior and posterior uterine walls. Note that the anterior myometrium is much thicker than the posterior myometrium.
{kind=link}
{kind=link}
Moreover, there may be linear striations radiating out from the endometrium into the myometrium, and an indistinct endo–myometrial junction with a pseudo-widening of the endometrium. The hypoechogenicity may be caused by the muscular hypertrophy, while the increased echogenicity, the cyst, the linear striations, and indistinct endo–myometrial junction may be caused by ectopic endometrial tissue. Although these features are commonly imaged in women with adenomyosis, there is no general agreement on which diagnostic criteria have the highest diagnostic accuracy.
Recently Meredith et al.35 analyzed relevant reports published between 1966 and 2007 for the diagnostic accuracy of TVS in women having hysterectomy. TVS predicted adenomyosis with a likelihood ratio of 4.67 (95% CI 3.13–6.17). The overall prevalence of adenomyosis was 27.9% (95% CI 25.5–30.3), whereas its probability with an abnormal TVS was 66.2% (95% CI 61.6–70.6). The probability of adenomyosis with a normal TVS was 9.1% (95% CI 7.3–11.1). In conclusion, if adenomyosis is clinically suspected, TVS should be favored as the primary diagnostic tool, although substantial experience and specific training is required to make sonography a useful diagnostic tool.
Magnetic resonance imaging
The development of magnetic resonance imaging (MRI), a high-resolution imaging technique, heralded a real turning point in the appreciation of the true features of adenomyosis. In particular, T2-weighted MR images of the uterus, have identified a specific area of the inner myometrium, named the “endo–myometrial junctional zone” (JZ) (see section on The junctional zone and adenomyosis, below), that can be clearly distinguished from the endometrium and outer myometrium36 and an irregular thickening of this zone is now recognized as the hallmark of adenomyosis. It must be underlined that JZ abnormalities detected by imaging techniques primarily reflect changes in smooth muscle organization.
It is important to stress that the cardinal diagnostic feature of adenomyosis based on histology, namely the presence of ectopic endometrial glands (the “adeno” component) differs from that of imaging techniques, based on observed differences in the organization of smooth muscle (the “myosis” component).
The relative contribution of both components of adenomyosis can vary considerably and can account for discrepancies between the histological and imaging diagnoses of the disease. Based on imaging, it is now clear that adenomyosis is not confined to older women but can be detected in young symptomatic patients.26, 37, 38
With improvements in imaging modalities it has now become feasible to establish a diagnosis of adenomyosis without hysterectomy, to exclude additional pathology, and to institute conservative symptomatic treatment and monitoring. However, the new imaging techniques have described patterns of additional abnormalities which have been linked to adenomyosis (see section on The endo–myometrial junctional zone, below).
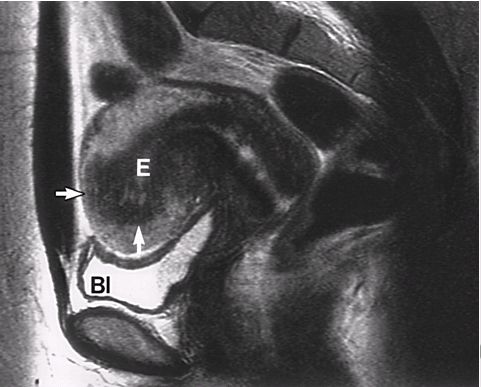
Adenomyosis may present itself with varying degrees of severity, ranging from simple JZ thickening to more diffuse and nodular lesions involving the entire uterine wall. Finally, it can take the form of an adenomyoma, a focal thickening or a nodular structure at the JZ or within the myometrium, with low signal intensity on T2-weighted MR images (Figs. 10–13).
{kind=link}
Fig. 10. MR image of asymmetrical adenomyosis. (This figure was published in Tamai K, Koyama T, Umeoka S, et al: Spectrum of MR features in adenomyosis Best Pract Res Clin Obstet Gynecol 20: 583, 2006. Copyright Elsevier 2006, reproduced with permission.)
{kind=link}
Fig. 11. MR image of focal thickening of the junctional zone. (Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation (Review). Radiographics 1999 Oct;19 Spec No:S147-60, reproduced with permission.)
{kind=link}
Fig. 13. MR image showing the contemporary presence of adenomyosis and of an endometrioma. (This figure was published in Tamai K, Koyama T, Umeoka S, et al: Spectrum of MR features in adenomyosis Best Pract Res Clin Obstet Gynecol 20: 583, 2006. Copyright Elsevier 2006, reproduced with permission.)
{kind=link}
PATHOGENESIS
As already mentioned, Kelly and Cullen15 were the first to show that – at least in some cases – a direct connection could be established between the “large or small chinks” into which normal uterine mucosa flow inside a diffuse myomatous tissue and the mucosa lining the uterine cavity. Their theory of an invasion of the myometrium by the eutopic endometrium remains valid and much of the work carried out over the past 2–3 decades deals with the identification of mechanisms through which such an invasion can take place.
This work yielded one notable result, that of bringing back the old theory of von Franqué,18 that epithelial invasion of abdominal organs was the result of a newly found ability by the mature endometrium to, in selected cases, somehow become capable of “infiltrating” other organs; von Franqué believed that this new-found ability was the consequence of an inflammatory process, whereas today inflammation is believed to be secondary to the invasion. It also created the basis for again considering adenomyosis and endometriosis as two sides of the same coin.
Adenomyosis and endometriosis
The relationship between the two endometrial disorders adenomyosis and endometriosis seems to have gone in a full circle. As already explained, at the beginning of the 20th century only one pathological definition (adenomyoma) was utilized to describe the presence of heterotopic epithelial cells, stroma, and glands. Then came Sampson,19, 39 and endometriosis was born. From there on, the two entities remained separated, although a link persisted since, at times, one was called endometriosis “interna” and the other endometriosis “externa”. Towards the end of the 20th century, with the identification and characterization of the JZ of the myometrium, connections between them began to re-appear. In 1995, Salamanca and Beltran40 in a study of inner myometrial contractility in women with endometriosis found a predominantly retrograde pattern of subendometrial contractions during menstruation. After this, Kunz et al.24 using MR established a significant correlation between increased JZ thickness and peritoneal endometriosis. As already mentioned, they calculated a prevalence of diffuse and focal adenomyosis in 79% of all patients with endometriosis; this reached 90% in women younger than 36 years, contrasting with a prevalence of 28% in their “total control” group (women without endometriosis) and only 9% in their “healthy control” group.
These data support the hypothesis that JZ hyperplasia precedes adenomyosis and endometriosis.41 This, however, does not explain why in some women JZ hyperplasia may develop at a young age. Now, the final link seems to have been found in a common predisposing factor: an alteration of the angiogenesis spiral arterioles (see the section on The role of uterine neoangiogenesis, below).
The endo–myometrial junctional zone
As already mentioned, modern imaging techniques, both TVS and MRI, have made possible for the first time a careful evaluation of the inner myometrial layers underlying the endometrium; these appear to be a distinct anatomical structure, despite the lack of histological distinction on light optic microscopy. Like the endometrium, the JZ is of müllerian origin, while the outer myometrium is of non-müllerian, mesenchymal origin.42 Furthermore, the JZ but not outer myometrium, undergoes cycle-dependent changes in response to the rise and fall of ovarian steroid hormones (Table 1).
Table 1. Similarities between junctional zone myometrium and endometrium
| Ontogeny |
| Both of müllerian origin |
| Function |
| Express similar sex steroid hormone receptors |
| Show maximum growth between day 8 and 16 of cycle |
| Both are involved in implantation and deep placentation |
Over the years a different terminology has been applied to descriptions of the JZ myometrium and these are summarized in Table 2.
Table 2. Terminology of junctional zone myometrium
| Stratum basale |
| Inner myometrium |
| Junctional zone myometrium |
| Endometrio–myometrial interface |
| Transitional zone |
| Endo–myometrial junctional zone |
| Subendometrial myometrium |
A normal JZ myometrium is commonly described as being regular in appearance on ultrasound or MRI and measuring 5 mm or less in thickness.43, 44 In adenomyosis, diffuse or focal thickening of the low-signal intensity JZ corresponds to smooth muscle hyperplasia or "myosis" and the bright foci on T2-weighted images represent embedded ectopic endometrial tissue and cystic dilated glands.22, 45
The presence of cyclical changes in the thickness of the JZ myometrium mimicking those in the endometrium, is still debated. On the one hand, Wiczyk et al. have observed growth, with a maximum between days 8 and 16 of the menstrual cycle;46 on the other, Hauth et al.44 could not detect any significant difference in thickness between the follicular and luteal phase.
Irrespective of whether there are variations in thickness during the menstrual cycle, Noe et al.42 found that the subendometrial myometrium (the so-called “stratum subvasculare”) with a predominantly circular arrangement of muscular fibers, exhibits a cyclic pattern of expression of estrogen and progesterone receptors (ER and PR) that parallels that of the endometrium, whereas the outer portion of the uterine wall, composed of the so-called “stratum vasculare” and “stratum supravasculare” (representing the bulk of the uterine musculature) does not exhibit a cyclic pattern of ER and PR expression. This phenomenon is explained by the different ontogenesis and phylogenesis of the two compartments: the outer myometrium is of non-paramesonephric origin with functions confined to parturition, while the inner myometrial layer together with the glandular epithelium and the stroma of the endometrium are of paramesonephric origin with various functions during the cycle in addition to those during pregnancy and parturition. Several other dissimilarities exist between the JZ of the myometrium and the outer myometrium: in postmenopausal women, both in those with and without adenomyosis and in those taking oral contraceptives or gonadotropin-releasing hormone (GnRH) analogues, suppression of ovarian activity decreases the zone’s thickness. In contrast to this, hormone replacement therapy may cause the reappearance of the typical zone’s anatomy.47 Finally, the use of the non-steroidal anti-estrogen tamoxifen for breast cancer treatment is known to increase the incidence of adenomyosis in postmenopausal women.48
In normally menstruating women, uterine peristaltic activity, measured by variations in myometrial contractility waves, indicates that it originates exclusively from the JZ, while the outer myometrium remains quiescent;49, 50 in addition, uterine peristalsis is primarily hormone dependent, on both estrogen and progesterone51 and its activity is likely to play a role in sperm transport, as well as in the nidation process.42
In conclusion, to date there is ample evidence that the “zonal–endometrial” complex plays an important role in uterine receptivity and in the nidation and placentation processes, to the point that studying the relative signal intensity of uterine layers is a good predictor of uterine receptivity and therefore of the outcome of assisted conception.52
The thickness of the JZ myometrium physiologically increases with age; in normal women it grows from 0.5 to 0.8 cm, whereas in those with adenomyosis or fibroids it grows from 0.5 to 1.1 cm.44 Thus, it is obvious that widening of the JZ is per se not primarily caused by adenomyosis, but rather by physiological hyperplasia.
The junctional zone and adenomyosis
When studying the JZ myometrium in women with adenomyosis, several important facts have been discovered. First, adenomyosis is characterized by a homogeneous thickening of the myometrium and this feature has become the standard parameter for the diagnosis of even mild forms of the condition.45 While a normal JZ is described as having a thickness (on T2-weighed MR images) of between 5 and 12 mm, the presence of a JZ measuring more than 12 mm in thickness, with hemorrhagic high-signal myometrial spots, is highly predictive of histological adenomyosis.22
This thickening of the JZ myometrium on MRI is thought to be the consequence of inordinate inner myocyte proliferation and/or increased angiogenesis and the suggestion has been made that the disruption of JZ architecture precedes and predisposes for the subsequent development of adenomyosis. This assumption is supported by the observation that, while adenomyosis is regarded as a condition typical of older, multiparous women, irregular JZ thickening is not an uncommon finding in young, symptomatic women.38
The thickening or abnormality of the endo–myometrial JZ has been repeatedly documented and has become the “gold standard” for posing a diagnosis of “adenomyosis”; it has also been linked to infertility.
Recently, however, Tocci et al.53 proposed that the “subendometrial myometrium unit” disruption be considered as a new entity (distinguished from adenomyosis), the diagnosis of which is feasible and straightforward on imaging and expressed mainly by pathological thickening or abnormality of the subendometrial myometrium. The influence of the abnormal thickening or disruption on human fertility and outcome of assisted reproduction techniques suggests that this new entity is epidemiologically different from adenomyosis.
Role of uterine neoangiogenesis
It is well documented that each menstrual cycle produces waves of neoangiogenesis within the endometrium, with the development of arterioles and of a capillary network. This process involves a spatially regulated process of vascular smooth cell differentiation, which is under the influence of a number of factors.54 This process constitutes the prerequisite for the remodeling of the placental bed spiral arterioles needed to ensure an adequate blood supply for the fast growing pregnant uterus, and represents a unique example of rapid angiogenesis. In this sense the uterus has a remarkable capacity of vascular regeneration, not only after each menstrual cycle, but also, and even more, after delivery. The fact that JZ spiral arteries are capable of complete involution in the puerperium and that those with atherosclerotic lesions return to normal has important implications in the field of vascular pathology and an abnormal angiogenesis is probably involved in the genesis of both adenomyosis and endometriosis.
In women with adenomyosis there is an increased expression of the vascular endothelial growth factor (VEGF), a major mediator of angiogenesis and vascular permeability, of the hypoxia-inducible factor-1alpha (HIF-1alpha), and of microvessel density especially in epithelial cells. This phenomenon has been demonstrated comparing, in the same woman, heterotopic versus normotopic endometrium.55 It seems therefore that VEGF may play a key role in the development of adenomyosis; Kang et al. investigating four VEGF polymorphic alleles found significant differences between adenomyosis patients and a control group in the allele frequencies and genotype distributions. They concluded that two alleles of VEGF genes (22578A and 21154A) could significantly decrease the risk of adenomyosis and might be potentially protective factors for its development.56
Further evidence linking adenomyosis to abnormal angiogenesis comes from a study by Tokyol et al.57 who investigated the expression of cyclo-oxygenase (COX)-2 and matrix metalloproteinase (MMP)-2 in patients with this condition. They observed that, whereas the quantity and intensity of COX-2 expression in endometrium did not vary during the menstrual cycle in normal women, in patients with adenomyosis it was higher both during the follicular and secretory phase.
In conclusion, there are today good reasons to believe that a potential link exists between abnormal uterine angiogenesis and the development of adenomyosis and endometriosis.
The endometrium in adenomyosis
Evidence is beginning to appear that eutopic endometrium in women with adenomyosis and endometriosis possesses unique characteristics.
In reviewing the role of the immune system in endometriosis, Braun and Dmowski58 stressed the fact that endometrial cells, although inherently resistant to apoptosis and immune-mediated elimination, may acquire the capacity to utilize the products of an activated immune system to establish ectopic foci of disease. If this is followed by cyclical inflammatory/immune cell stimulation, a situation may arise where the body fails to eliminate ectopic endometrial implants with a progressive immune derangement.
In another study, Taylor et al.59 have evaluated the expression in women with endometriosis of two homeobox genes (HOXA10 and HOXA11) with a role in regulating endometrial development. Comparing results obtained in 40 normally cycling controls and in 40 patients with documented endometriosis, the latter failed to show the expected mid-luteal rise in HOX gene expression, which was evident in the controls. The authors concluded that the aberrant HOX gene expression is indicative of altered development of the endometrium at the molecular level.
The menstruation-conditioning hypothesis: establishing a relationship between presence of adenomyosis and/or endometriosis and pregnancy outcome
As mentioned above, evidence is being accumulated that eutopic endometrium of patients with endometriosis and, possibly, also that of women with adenomyosis is abnormal. This abnormality may constitute a link between the two endometrial disorders. In this sense, a major obstetric syndrome may exist, characterized by a modified uterine environment around the time of nidation, with the consequence that this abnormal endometrium, its decidualized stroma and the ensuing impaired placentation, will increase the risk of preterm birth, intrauterine growth restriction, and small-for-gestational-age babies.60
Recent studies have found that women with adenomyosis61 and women with endometrosis62, 63 have a significantly increased risk of preterm delivery syndrome. It is recognized that endometriosis, especially in advanced stage, is associated with increased thickness of the JZ myometrium and often with adenomyosis,38, 64 and, conversely, that women with adenomyosis are more likely to have a history of endometriosis in comparison to those with leiomyomas.31 This would suggest that adenomyosis and endometriosis may be associated with a shallow type of defective deep placentation.
Combining this information, a hypothesis can be formulated that ovulatory menstrual cycles during early reproductive life have an angiogenic priming effect that will permit successful deep placentation also in the nullipara. This phenomenon involves full restructuring of the spiral arteries in the decidua and the JZ of the myometrium with interstitial and intravascular trophoblast invasion. Therefore, zone hyperplasia, adenomyosis, and endometriosis may be related to an aberrant angiogenesis in the myometrial JZ.65 Menstruation is widely viewed as serving no purpose other than to reinitiate the endometrial cycle in the absence of pregnancy. Yet, menstruation and pregnancy are both inflammatory conditions that cause a degree of physiological ischemia–reperfusion tissue injury, albeit much more so in pregnancy. It can be speculated that menstruation may not have been an evolutionary coincidence, but serves to protect uterine tissues from the profound hyperinflammation and oxidative stress associated with deep placentation. This process of preconditioning provides a novel paradigm for understanding how reproductive disorders impact on pregnancy outcome, while, on the other hand, in the absence of pregnancy they may cause uterine reproductive disorders.66
In the light of newly acquired knowledge, the question then arises whether spontaneous ovulatory menstrual cycles have a functional role in priming the uterine vascular microenvironment to secure the rapid spiral artery remodeling and deep placentation before a first pregnancy. In this connection, it has been well documented that the risk of pre-eclampsia is reduced for second and later pregnancies; this protective effect is achieved even if pregnancy is terminated during the first trimester. A large epidemiological study recently confirmed this fact: the protective effect of two induced abortions is similar to what is commonly seen after a first term pregnancy.67 As already mentioned, there seems to be a common predisposing factor linking adenomyosis, endometriosis, and pregnancy complications: the preconditioning of the uterus for successful deep placentation.
Cyclic endometrial decidualization and the subsequent menstrual shedding are therefore examples of the physiological preconditioning necessary to prepare the uterus for a dramatic vascular remodeling, reactive oxygen species production, and the hyperinflammation associated with deep hemochorial placentation. Indeed, decidualization in the human offers a unique example of rapid angiogenesis starting in the mid-luteal phase. Remodeling of myometrial JZ spiral arteries is a complex process and has been reviewed by Brosens et al.68 in the event of both normal and abnormal gestations. They reported that decidualized cells are a major source of angiogenic growth factors the levels of which decrease with increasing gestational age, suggesting that decidual angiogenesis may play a role in the initial spiral artery remodeling. Decidual uterine natural killer (uNK) cells are potent secretors of an array of angiogenic factors and regulate trophoblast invasion both in vitro and in vivo by production of the interleukin-8 and interferon-inducible protein-10 chemokines.69
As already mentioned, MRI found that the JZ myometrium is significantly thicker on T2-weighted imaging in patients with adenomyosis and/or endometriosis when compared with age-matched control subjects. In addition, power Doppler ultrasound studies have shown that endometriosis is associated with increased endometrial and JZ blood flow during the late secretory phase of the cycle.70 The most compelling evidence for cyclic endometrial preconditioning comes from the observation that stromal purified cells from eutopic endometrial biopsy material from patients with and without endometriosis exhibit different responses to a decidualizing stimulus, even after prolonged culture.71, 72, 73
Endometrial stem cells and their possible role in the genesis of adenomyosis and endometriosis
Recent studies have provided evidence of the existence of human endometrial stem/progenitor cells. Chan et al.74 demonstrated clonogenicity of endometrial-derived cells by generating single-cell suspensions of epithelial and stromal cells from hysterectomy samples. Schwab et al.75 showed that the frequency of clonogenic epithelial and stromal cells did not differ between phases of the menstrual cycle; also, there was no significant change in the number of clonogenic cells isolated from inactive endometrium. Because inactive endometrium contains only a basal layer, while the functional layer is absent, these data suggest that putative endometrial stem/progenitor cells reside along the endometrial–myometrial border.76
Although these data are preliminary, Sasson and Taylor have pointed out that they pose a series of questions.77 First and foremost, which cell lineages – epithelial, stromal, or myometrial – are generated by endometrial stem cells? In addition, what is the physiological role of endometrial stem cells and what are their niches in pathological processes? The question then arises whether the primary defect in the pathway leading to endometriosis and possibly also to adenomyosis lies in the stem cell, or, alternatively, is a disregulation within the niche that starts an aberrant biological process at the stem cell level.
Whereas no answer to these questions (and too many others) is expected for some times, the identification of “endometrial progenitor cells” opens up entirely novel avenues for research and may hold the key to explaining how endometriosis (and adenomyosis?) occur.
CLASSIFICATION
Current imaging techniques allow the detection of a spectrum of adenomyosis-related uterine lesions (Table 3).
Table 3. Diagnostic criteria on transvaginal sonography and magnetic resonance imaging. (After Wyczik et al. 1988;46 Dueholm et al. 2001;78 Bazot et al. 2001;79 and Hauth et al. 200744)
| Junctional zone hyperplasia |
| MRI |
| Thickness of junctional zone on T2-weighted images between 5 and 12 mm |
| Extension |
| Diffuse or focal |
| Adenomyosis |
| TVS |
| Thickening and asymmetry of the anterior and posterior myometrial walls |
| Increased echotexture of the outer myometrium |
| MRI |
| One or both of the following: |
| Junctional zone hyperplasia of 12 mm or more |
| High-signal myometrial spots |
| Extension |
| Involvement of the outer myometrium: <1/3, <2/3, >2/3 |
| Homogenous uterine enlargement: diffuse |
| Adenomyoma |
| TVS |
| Heterogeneous, indistinctly marginated areas in the myometrium |
| MRI |
| Myometrial mass with indistinct margins of primarily low signal intensity on all sequences |
| Types |
| Polypoid adenomyoma, cystic adenomyoma, junctional zone adenomyoma, outer myometrium adenomyoma |
| Extrauterine adenomyoma |
| Locations |
| Retrocervical |
| Rectovaginal |
| Fallopian tube |
| Bladder |
Junctional zone hyperplasia
The term "JZ hyperplasia" was coined to define partial or diffuse thickening of the JZ in the absence of additional signs of adenomyosis, such as high-signal intensity foci.41, 51 The rationale for this term was to indicate that inordinate proliferation of inner myometrial smooth muscle cells or "myosis" of the JZ does not necessary indicate the presence of heterotopic endometrial implants, an obligatory feature for the histological diagnosis of adenomyosis. The underlying assumption was that disruption of JZ architecture constitutes the primary event in the development of adenomyosis, a notion now supported by animal studies demonstrating that myometrial changes precede invasion of endometrial glands and stroma.80, 81 In addition, cases have been published of iatrogenic induction of adenomyosis following hysteroscopic endometrial ablation,82 or after laparoscopic myomectomy without reconstruction of the uterine wall.83
A major confounding factor is that JZ thickness increases with age. Hauth et al.44 indicated that the mean JZ width increases from 5 mm in women aged 20–30 years to 8 mm in those over 40 years. Kunz et al.38 measured the thickness of the posterior JZ myometrium by MRI and reported a gradual increase in diameter starting in the third decade of life; the process then markedly accelerates in women older than 34 years. Interestingly, the authors also found that, whereas the posterior JZ thickness was invariably greater in patients with endometriosis, the age-dependent increase paralleled that of women without endometriosis.
In view of these recent findings, JZ hyperplasia could be viewed as a sign of uterine aging without specific pathological connotations. Alternatively, JZ thickening in older women may be directly linked to age-dependent decrease in fertility or increase in dysfunctional uterine bleeding and pregnancy complications. At present, it is prudent to restrict the use of the term "JZ hyperplasia" to younger women (less than 35 years) with a thickened inner myometrium but insufficiently so to make a confident diagnosis of adenomyosis (i.e. 8 mm or more but less than 12 mm). Clearly, additional studies are warranted to determine whether JZ hyperplasia, irrespectively of age, is associated with objective signs of uterine dysfunction, such as impaired subendometrial peristalsis or increased menstrual blood loss.
Adenomyosis
In contrast to the expression "JZ hyperplasia", the term "adenomyosis" implies the presence of heterotopic endometrium. Adenomyosis can be diffuse or focal, although the term "adenomyoma" should be preferred to describe the latter. The posterior uterine wall is more frequently involved compared to the anterior and lateral sides.24 As already mentioned (see above), based on various criteria, the mean sensitivity and specificity of transvaginal ultrasound for the diagnosis of adenomyosis are 74% (95% CI 63–82%) and 87% (95% CI 81–91%), respectively.34 Ultrasound is much more operator-dependent than MRI, and additional factors, such as equipment and patient characteristics, affect its reliability. Co-existing uterine pathologies when the uterus is large or multiple myomas are found may render ultrasound diagnosis unreliable.78 In addition, it is often difficult to distinguish between focal myometrial pathologies such as adenomyoma and leiomyoma. Although ultrasound is a useful screening tool, confirmation of the diagnosis requires, where possible, MRI.
MRI offers a reliable and accurate non-invasive diagnosis of adenomyosis and, for this reason, several attempts have been made to compare MRI with histology, using a variety of diagnostic criteria and sampling techniques; the reported average sensitivity and specificity are 78% (95% CI 68–86%) and 88% (95% CI 83–92%), respectively.34, 45, 84 However, Reinhold et al.85 demonstrated that a JZ thickness measuring 12 mm or more is highly predictive of the presence of glandular and stromal lesions 2.5 mm or more below the endo–myometrial junction. In the absence of additional high-signal intensity lesions, a JZ width on T2-weighted images of 12 mm or more is increasingly accepted as an accurate diagnostic criterion for adenomyosis.22 It is advisable to perform MRI for the diagnosis of adenomyosis after menstruation, as menstrual contractions waves can mimic abnormal JZ thickening.
Adenomyoma
The term adenomyoma refers to a well-circumscribed form of adenomyosis. Different types can be distinguished:
- Focal thickening of the JZ or the presence of primarily low-signal intensity nodules in the outer myometrium or subserosa on T2-weighted MR images.25, 78
- Polypoid adenomyoma, which is characterized by a well-defined polypoid mass protruding into the uterine cavity. Approximately 50% of cases present as an isointense mass relative to the myometrium with small or large hyperintense foci on T1- or T2-weighted imaging), reflecting the fascicle of smooth muscle with islands of hemorrhagic endometrial tissue.86
- Cystic adenomyoma: a rare variation of adenomyoma caused by an extensive menstruation-like bleeding into the ectopic lesion.87, 88
- Retrocervical and rectovaginal endometriosis, which histologically is indistinguishable from uterine adenomyoma.89
It is important to bear in mind that an image with features of an adenomyoma can simulate other lesions, including leiomyoma, endometrial polyps, and adenosarcomas. For this reason, in case of doubt, the correct diagnosis may require histological confirmation.
ADENOMYOSIS AND INFERTILITY
The precise role of adenomyosis in infertility remains controversial and whether adenomyosis per se causes infertility is not known.
Having said this, the current consensus is that, for successful conception, JZ contractions at the time of implantation should be minimal. Excessive JZ contractions have been shown to reduce implantation rates in both spontaneous and stimulated cycles.90, 91 A low frequency contraction of the JZ before embryo transfer (ET) during in vitro fertilization (IVF) cycles is associated with a higher implantation rate and a higher clinical and ongoing pregnancy rate,92 while a significantly lower clinical pregnancy rate occurs if immediately after ET five or more contractions per minute are observed.93, 94
Therefore the question arises whether abnormal contractility is associated with reduced fertility. Women with endometriosis show a significant increase in JZ contractions and a disruption in the pattern of contractility in comparison to healthy controls.91, 95 Leyendecker’s group96 demonstrated that in women with endometriosis the mechanism of rapid sperm transport is compromised. The evidence for disrupted sperm transport in women with endometriosis and/or adenomyosis is quite convincing, but probably of greater importance is the increased contractility or hyperperistalsis.24, 97
TREATMENT
In a recent review, Yang et al.98 list 12 different medical or surgical techniques for the treatment of adenomyosis; by and large these modalities are identical to those utilized in case of endometriosis. At present medical therapy of adenomyosis can be attempted for symptomatic relief, especially in premenopausal women and in women who wish to become pregnant.
Surgery
HYSTERECTOMY
For more than a century hysterectomy has been both the primary diagnostic tool and therapeutic strategy for uterine adenomyosis. Vaginal hysterectomy is preferable to abdominal hysterectomy because of lower morbidity and faster recovery, although the decision to perform a hysterectomy using the abdominal or vaginal route is often based not only on the indication, but also on the familiarity and experience of the individual surgeon.
In a large comparative study of complications of vaginal hysterectomy in patients with leiomyomas and in patients with adenomyosis, Furuhashi et al.99 found that women with adenomyosis had a significantly higher risk of bladder injury, while there was no difference in blood loss and operating time when the uterine weight was taken into account. The definite reason for the increased risk of bladder injury is unknown, but it may be due to the greater difficulty in identifying the supravaginal septum and the vesicovaginal and vesicocervical planes. Most cases of failed vaginal hysterectomy for uterine adenomyosis are due to associated adhesions. The use of laparoscopic-assisted vaginal hysterectomy is likely to decrease the risk of bladder injury and the failure of vaginal hysterectomy.
CONSERVATIVE SURGERY
In terms of conservative surgical treatment of adenomyosis, a distinction must be made between the two main forms in which the condition presents itself: adenomyosis with diffuse lesions involving the entire superficial or deep myometrium; and adenomyoma, or focal adenomyosis, where lesions are localized in the anterior or posterior wall. In specific cases of both conditions conservative surgery can today be attempted, since imaging technology has allowed, in symptomatic women who want to preserve their uterus, a presumptive diagnosis of the localization of the lesions.
Superficial adenomyosis
Symptomatic, submucous or superficial adenomyosis is usually a diffuse process involving the entire circumference of the uterine wall. Ultrasound and MRI studies have shown that in diffuse adenomyosis the posterior wall is the area most frequently and severely affected.100, 101 Superficial submucous adenomyosis can be treated by transcervical endometrial coagulation or resection and, according to Loffer,102 the failure rate for endometrial ablation lies between 8 and 10%. In a study of 305 ablations, Pagedas et al.103 reported that histological examination of uteri from patients requiring hysterectomy because of an unsuccessful endometrial ablation showed an incidence of adenomyosis of around 75%. Similar results have also been reported by McCausland and McCausland:104 seven out of eight cases requiring hysterectomy were found to have adenomyosis. These authors also found that the likelihood of recurrent symptoms and especially the likelihood of hysterectomy correlated with the depth of penetration of the adenomyotic disease.
In spite of this, there is today concern that the presence of adenomyosis could be responsible for many of the failures of endometrial ablation or resection. Wortman and Daggett105 found that operative hysteroscopy is useful in women after failed endometrial ablation and resection. They published a series of 26 women in whom adenomyosis was present in 58% of the specimens and who had undergone endometrial ablation or resection and experienced failure characterized by intolerable pain, bleeding, or asymptomatic hematometra. In these women, re-operative hysteroscopic surgery gave excellent results in achieving amenorrhea and relief of pelvic pain, thereby avoiding hysterectomy in most patients. It is therefore likely that, despite previous concerns, many women with superficial submucous adenomyosis may experience great symptomatic improvement by the hysteroscopic and third-generation procedures of endometrial ablation.
In contrast to this, patients with deep endometrial penetration of more than 2.5 cm (deep adenomyosis) usually have persistent problems and should be offered hysterectomy over repeat ablation. MRI or high-resolution ultrasound may be appropriate preoperative screening tools to determine the depth of adenomyosis and to select patients for endometrial ablation.106
Deep adenomyosis
Wang et al.107 published a prospective pilot study of laparoscopic uterine artery ligation (UAE) in 20 women with symptomatic adenomyosis. The outcome of the treatment was rated as satisfactory 6 months postoperatively by 15% of patients, but 45% were dissatisfied. The poor satisfaction in this preliminary study suggests that the approach may not be effective for symptomatic adenomyosis.
Nishida et al.108 described a series of 44 cases of women with diffuse uterine adenomyosis wishing to avoid hysterectomy in whom he attempted a new conservative surgical management. The procedure involves longitudinal dissection of the uterus in the midline, excision of the lesion from the center of the anterior/posterior wall, and suturing to rejoin the right and left sides of the uterus. After this surgery, the mean visual analog scale score of dysmenorrhea decreased from 9.4 to 0.8, and anemia due to menorrhagia improved in all 44 women. Two patients became pregnant, with one interstitial pregnancy and one normal gestation. This procedure can be considered as a therapeutic option in women with symptoms of diffuse uterine adenomyosis who wish to avoid hysterectomy.
Myometrial adenomyoma
Conservative laparotomic surgery for deep uterine adenomyomas by excision may be difficult as it is extremely difficult to expose the lesion and determine the precise extent of the disease. The disease may be infiltrating an area close to the fallopian tubes, or involve major vessels, and the lesions may be very vascular. Frequently surgery is preceded by a medical treatment with a GnRH agonist. The classical technique is almost the same as that of myomectomy.
Fujishita et al.109 have published a preliminary report of the use of a transverse H incision technique to improve exposure and allow careful examination by manual palpation and serial resection of myometrium containing adenomyotic tissue. When comparing this new procedure to the classic technique the risk of endometrial perforation was reduced from 40% to 17%. Liu et al.110 reported that, of 26 patients with histologically proven adenomyoma who wanted to preserve their reproductive capacity, they were able to perform adenomyomectomy in ten, whereas only partial resection was feasible in the other 16 cases. The rates of severe dysmenorrhea and hypermenorrhea after the operation were considered significantly lower than those before, while three pregnancies and term deliveries were reported. Three patients relapsed after an average time of 50 months.
A laparoscopic excision of myometrial adenomyomas and tumor reduction has been described in patients with chronic pelvic pain, although locating the adenomyotic tissue may be difficult at laparoscopy. In a first study Phillips et al.111 used MRI to diagnose and locate adenomyomas in ten symptomatic patients and successfully used laparoscopic bipolar coagulation in seven of them; in the failed group one patient required resection, one patient required hysterectomy, and one patient refused further treatment. In a second study, Nabeshima et al.112 used hydro-ultrasonography to locate a cystic adenomyoma within the myometrium in a symptomatic patient and performed a successful resection. In a third study Morita et al. 113 located the adenomyoma by preoperative MRI and achieved successful resection in three symptomatic patients.
Surgery in combination with GnRH agonist therapy
A few authors have reported on successful pregnancies or live births following surgical treatment in combination with GnRH agonists for adenomyosis and infertility. One study reported a live birth after conservative surgery for severe adenomyosis following diagnosis by MRI and preoperative treatment with GnRH agonist therapy followed by resection of the localized lesion and postoperative therapy with danazol.114 In another study, Huang et al. reported a case of deep adenomyosis successfully treated by cytoreductive surgery and a subsequent 6-month course of GnRH agonist therapy.115 In a further report, Lin et al.116 utilized TVS to diagnose the presence of a posterior uterine wall adenomyoma in four symptomatic patients with infertility and enlarged uteri. After treating them preoperatively with a GnRH agonist, during 6 months all enlarged uteri decreased to normal or near-normal size. Following laparoscopic reductive surgery by adenomyomectomy, three patients conceived within four menstrual periods. Finally, Wang et al.117 reported pregnancies in three patients treated with microsurgical resection of the visible adenomyotic areas followed by treatment of GnRH agonists.
In spite of these reports, the role of the combination of cytoreductive surgery and GnRH agonist treatment in managing infertile women with adenomyosis is still far from clear. The approach seems to be attractive, but one must be aware of the surgical and obstetric risks: one of Huang’s cases was complicated by antepartum bleeding and threatened preterm labor, and in one of Lin’s cases pregnancy was terminated by emergency cesarean section at 30 weeks because of threatened rupture of the uterus. Also, it must be remembered that silent and spontaneous rupture of the uterus during labor has been reported in pregnant women with uterine adenomyosis.118, 119
UTERINE ARTERY EMBOLIZATION
Following the already mentioned pilot study of laparoscopic uterine artery ligation published by Wang et al.107 Siskin et al. 120 retrospectively evaluated the MRI appearance and clinical response of patients undergoing uterine artery embolization (UAE) for the treatment of menorrhagia due to adenomyosis. Of the 15 patients in the study, five had diffuse adenomyosis without evidence of uterine fibroids, one had focal adenomyosis without evidence of uterine fibroids, and the remaining nine had adenomyosis with one or more fibroids. At 12-month follow-up, 92.3% patients reported significant improvement in symptomatology and quality of life. Postoperative MRI revealed significant reductions in median uterine and fibroid volume and mean JZ. However, in this retrospective review the follow-up was incomplete (only 9/15 patients underwent MRI during follow-up) and 12 patients included in the study had concurrent fibroids, for which embolization is an established treatment option.
Several reports followed, mostly from the Far East, confirming that UAE is an effective therapy for adenomyosis. It is worth mentioning a South Korean study of UAE in women with adenomyosis, but no fibroids.121 The authors observed significant improvement of dysmenorrhea and menorrhagia with a decrease in uterine size in most patients. In addition, MR evaluation produced results suggestive of coagulation necrosis of adenomyosis in the majority of patients.
Another important study was conducted in South Korea122 to evaluate return of fertility; unfortunately, of the initial series of 94 patients, only six had a desire to become pregnant, five of them succeeded with one case of premature rupture of membrane.
Although the procedure seems promising, larger, prospective studies are needed to establish its safety and efficacy in women with adenomyosis.
MAGNETIC RESONANCE-GUIDED FOCUSED ULTRASOUND SURGERY
A new technology that seems to hold hope of soon developing a method for the conservative treatment of a number of benign conditions of the female reproductive tract is high intensity focused ultrasound ablation. Recently, Fukunishi et al.123 evaluated its thermal ablative effects on adenomyosis; in 20 premenopausal symptomatic women they tested its ability to improve clinical parameters; taking advantage of the similarity between adenomyosis symptoms and those of uterine myomas, they used the symptom severity score questionnaire available for evaluating the effect of magnetic resonance-guided focused ultrasound surgery (MRgFUS) on myoma and reported that most adenomyotic lesions could be satisfactorily ablated close to the serosal surface of the endometrium. At 6 months, the mean uterine volume decreased by 12.7%, symptom severity score improved significantly, and no serious complications were observed.
These preliminary observations indicate that MRgFUS represents a new, safe and effective method for the ablation of adenomyotic tissue.
Medical therapies
LEVONORGESTREL-RELEASING INTRAUTERINE SYSTEM
Long-term medical treatment of symptomatic adenomyosis has now been attempted with the well-known levonorgestrel-releasing intrauterine system (LNG-IUS), commercially known in the West as Mirena®. In a first trial published in 2008, Cho et al.124 evaluated the long-term clinical effects of the LNG-IUS in 47 patients with symptomatic adenomyosis, diagnosed through TVS. They checked the uterine volume, uterine artery blood flow, pictorial blood loss assessment chart (PBAC) scores, and the degree of dysmenorrhea before and 36 months after insertion of the device and observed a dramatic drop in pain and PBAC scores within 6 months, with the decrease remaining significant at 36 months. They also observed a decrease in uterine volume, although this effect seemed to diminish 2 years after insertion.
The following year, Sheng et al.125 evaluated, over 3 years, the efficacy of the LNG-IUS in 94 women with moderate or severe dysmenorrhea associated with adenomyosis, as diagnosed by TVS. They measured uterine volume and serum CA125 and utilized a visual analogue scale (VAS) for the analysis of the effects on dysmenorrhea. They observed a continuous and significant drop in VAS from the baseline score (p<0.001). The uterine volume decreased significantly from 113.8 ± 46.9 ml to 87.7 ± 35.8 ml (p<0.001) at 12 months and serum CA125 levels were significantly reduced from 6 months onwards (p<0.001).
In conclusion, the limited evidence available indicates that the LNG-IUS, when inserted in women with adenomyosis, is effective in relieving symptoms, improving vascularity and decreasing uterine volume. A major disadvantage of the device seems to be a frequent and unpredictable intermenstrual bleeding and spotting both during the first few months and after prolonged use.
DANAZOL-LOADED INTRAUTERINE DEVICES
A Japanese company (FD-1, Fuji Latex, Tokyo) has now developed a danazol-loaded intrauterine device (IUD) by covering the device with a silicone rubber (MDX 4-4210, produced by Dow Corning Corporation, Midland, MI, USA) containing 300–400 mg danazol. The overall shape of the device is that of a copper-T IUD, although it is much thicker in the anteroposterior diameter. Because of this characteristic, cervical dilatation may be needed for proper insertion and intrauterine placement. In a pharmacokinetic study, serum levels of danazol remained below the detection threshold and therefore none of the systemic side-effects associated with oral danazol should be expected.126 Igarashi et al.127 have tested this device in 14 women with dysmenorrhea, hypermenorrhea or infertility; they observed complete resolution of menorrhagia in 12 of them, whereas complete remission of dysmenorrhea was evident in nine patients. Only in two women did no change occur. In a subsequent, prospective, non-comparative study of 21 symptomatic women with adenomyosis, at 6 months complete relief of menstrual pain and dysmenorrhea was observed in 81% of the patients, whereas improvement of menstrual bleeding occurred in 76% of them. None of the well-known systemic side-effects of danazol became apparent during the study.126
The only disadvantages of the danazol-loaded IUD observed in this preliminary experience, has been uterine spotting and spontaneous expulsion.
Novel approaches
Treatment of adenomyosis is still far from ideal and, for this reason, a number of novel approaches are being attempted.
AROMATASE INHIBITORS
Endometriosis and adenomyosis are generally considered to be estrogen-dependent diseases. One of the most important advances in the understanding of these diseases has been the discovery that, in affected women, both eutopic and ectopic endometrium express the enzyme that converts androgens to estrogens: the “aromatase P450”,128, 129 a phenomenon that is believed to be restricted to women with proliferative reproductive tract disorders such as endometriosis, adenomyosis, and leiomyomas. In addition, estrone sulphatase has also been localized in uterine endometrium in cases of adenomyosis.130
It seems therefore that ectopic endometrium produces estrogens; this has important consequences for both medical and surgical treatment because it tends to support the view that, to minimize the risk of recurrence in severe disease, a complete excision is mandatory and the reality is that, today, whether in severe endometriosis or in uterine adenomyosis, complete excision cannot be guaranteed.
This fact provides a rationale for the use of agents capable of suppressing both ovarian (GnRH superagonists and antagonists) and local (aromatase inhibitors) estrogen biosynthesis, since these agents may significantly reduce the risk of recurrence after conservative surgery.
Proof of this has been obtained in a randomized, double-blind, placebo-controlled trial by Soysal et al.131 who found that after conservative surgery for severe endometriosis the addition of the aromatase inhibitor anastrozole to the GnRH-superagonist goserelin reduced the risk of recurrence and increased the maintenance of efficacy of the surgical treatment for at least 24 months. There is no reason to believe that the same results cannot be obtained in adenomyosis patients.
It seems therefore that a combined treatment with an aromatase inhibitor and a GnRH superagonist (or antagonist) or an oral contraceptive can be added to the armamentarium of therapeutic options for severe endometriosis and adenomyosis in premenopausal women.132
INHIBITORS OF ANGIOGENESIS
As already mentioned, evidence is accumulating that angiogenesis is altered in heterotopic uterine mucosa in case of endometriosis and adenomyosis. This discovery is opening the way for a new line of treatment. Since dopamine and its agonists, such as cabergoline (Cb2), promote endocytosis of VEGF receptor-2 (VEGFR-2) in endothelial cells, thereby preventing VEGF–VEGFR-2 binding and reducing neoangiogenesis, the group of Pellicer133 has now evaluated in an animal model the anti-angiogenic properties of Cb2 on growth of established endometriosis lesions. After treatment with Cb2 they found a significant decrease in the percentage of active endometriotic lesions and of cellular proliferation index, associated to a reduced neoangiogenesis and a significant modification of gene expression.
Another approach aimed at inhibiting angiogenesis has been studied by the group of Creatsas134 using pentoxiphylline, a phosphodiesterase inhibitor. In an animal model, they evaluated changes in morphology and in the expression of VEGF-C and of the receptor for tyrosine kinase, Flk-1 (a VEGF receptor), and observed a significant reduction in the mean volume of the endometriotic implants per animal when compared to the control group. Their conclusion was that pentoxifylline may cause suppression of endometriotic lesions by blocking angiogenesis through VEGF-C and Flk-1 expression.
REFERENCES
Benagiano G, Brosens I: The history of endometriosis: identifying the disease. Hum Reprod 6:963, 1991 |
|
Knapp VJ: How old is endometriosis? Late 17th- and 18th-century European descriptions of the disease. Fertil Steril 72:10, 1999 |
|
Benagiano G, Brosens I: History of Adenomyosis. Best Pract Res Clin Obstet Gynaecol 20:449, 2006 |
|
Batt RE: Emergence of endometriosis in North America: A study in the History of ideas. Dissertation submitted to the Faculty of the Graduate School of the University of Buffalo, State University of New York 109, 2008 |
|
Hudelist G, Keckstein J, Wright JT: The migrating adenomyoma: past views on the etiology of adenomyosis and endometriosis. Fertil Steril 92:1536, 2009 |
|
Benagiano G, Brosens I. Who identified endometriosis? Submitted. |
|
Iwanoff N: Drusiges cystenhaltiges Uterusfibrom compliciert durch Sarcom und Carcinom. Monatsschrift für Geburtshilfe und Gynaekologie 5:295, 1898 |
|
Von Rokitansky C: Über Uterusdrüsen-Neubildung in Uterus- und Ovarial-Sarcomen. Zeitschift Gesellschaft der Aerzte in Wien 16:577, 1860 |
|
Schrön DC: Disputatio Inauguralis Medica de Ulceribus Uteri. p 32, University of Jenae, literis Krebsianis, 1690 |
|
Brosens I, Steeno O: A compass for understanding endometriosis. Fertil Steril 73: 179, 2000 |
|
Von Recklinghausen F: Die Adenomyomata und Cystadenomata der Uterus und Tubenwandung: Ihre Abkunft von Resten des Wolffischen Koerpers. Berlin, August Hirschwald Verlag, 1896 |
|
Meyer R: Eine unbekannte Art von Adenomyom des Uterus mit einer kritischen Besprechung der Urnierenhypothese v. Recklinghausens. Zeischrift für Geburtshilfe und Gynaekologie 49:464, 1903 |
|
Orloff WN: Zür Genese der Uterusmyome. Zeitschr Heilkunde 5:312, 1895 |
|
Cullen TS: Adeno-myoma Uteri diffusum benignum. Johns Hopkins Hosp Rep 6:133, 1896 |
|
Kelly HA, Cullen TS: Myomata of the uterus. Philadelphia & London, W.B. Saunders, 1909 |
|
Cullen TS: Adenomyoma of the uterus. Philadelphia & London, W.B. Saunders, 1908 |
|
Lockyer C: Fibroids and allied tumours (Myoma and Adenomyoma). London, MacMillan and Co, 1918 |
|
Von Franqué O: Salpingitis nodosa isthmica und Adenomyoma tubae. Zeitschr F Geb 42:41, 1900 |
|
19. Sampson JA: Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol 14:422, 1927 |
|
Frankl O: Adenomyosis uteri. Am J Obstet Gynecol 10:680, 1925 |
|
Bird CC, McElin TW, Manalo-Estrella P: The elusive adenomyosis of the uterus. Am J Obstet Gynecol 112:583, 1972 |
|
Reinhold C, Tafazoli F, Wang L: Imaging features of adenomyosis. Hum Reprod Update 4:337, 1998 |
|
Kuohung W, Jones GL, Vitonis AF et al: Characteristics of patients with endometriosis in the United States and the United Kingdom. Fertil Steril 78: 767, 2002 |
|
Kunz G, Beil D, Huppert P, et al: Adenomyosis in endometriosis - Prevalence and impact on fertility. Evidence from magnetic resonance imaging. Hum Reprod 20: 2309, 2005 |
|
Bazot M, Darai E, Hourani R et al: Deep pelvic endometriosis: MR imaging for diagnosis and prediction of extension of disease. Radiology 232:379, 2004 |
|
De Souza NM, Brosens JJ, Schwieso JE et al: The potential value of magnetic resonance imaging in infertility. Clin Radiol 50:75, 1995 |
|
Cullen TS: The distribution of adenomyomata containing uterine mucosa. Arch. Surg 1: 215, 1920 |
|
Cocuzzi E, Cocuzzi L, Benagiano G: Unpublished observations. |
|
Weiss G, Maseelall P, Schott LL, et al: Adenomyosis a variant not a disease? Evidence from hysterectomized menopausal women in the Study of Women’s Health Across the Nation (SWAN). Fertil Steril 91: 201, 2009 |
|
Parazzini F, Mais V, Cipriani S, et al: Determinants of adenomyosis in women who underwent hysterectomy for benign gynecological conditions: Results from a prospective multicentric study in Italy. Eur J Obstet Gynecol Reprod Biol 143: 103, 2009 |
|
Taran FA, Weaver AL, Coddington CC, Stewart EA: Characteristics indicating adenomyosis coexisting with leiomyomas: a case-control study. Hum Reprod 25(5):1177, 2010 |
|
Brosens JJ, Barker FG: The role of myometrial needle biopsies in the diagnosis of adenomyosis. Fertil and Steril 63: 1347, 1995 |
|
Molinas CR, Campo R: Office hysteroscopy and adenomyosis. Best Practice and Research: Clinical Obstetrics and Gynaecology 20: 557, 2006 |
|
Dueholm M: Transvaginal ultrasound for diagnosis of adenomyosis: a review. Best Practice and Research: Clinical Obstetrics and Gynaecology 20: 569, 2006 |
|
Meredith S, Sanchez-Ramos L, Kaunitz A: Diagnostic accuracy of transvaginal sonography for the diagnosis of adenomyosis: systematic review and metanalysis. Am J Obstet Gynecol 201:1, 2009 |
|
Hricak H, Alpers C, Crooks LE, Sheldon PE: Magnetic resonance imaging of the female pelvis: initial experience. Am J Roentgenol 141:1119, 1983 |
|
Kissler S, Zangos S, Kohl J, et al: Duration of dysmenorrhoea and extent of adenomyosis visualised by magnetic resonance imaging. Eur J Obstet Gynecol Reprod Biol 37:204, 2008 |
|
Kunz G, Herbertz M, Beil D, Huppert G, Leyendecker G: Adenomyosis as a disorder of the early and late human reproductive period. Reprod. BioMed. Online 15: 6815, 2007 |
|
Sampson JA: Perforating hemorrhagic (chocolate) cysts of the ovary. Arch. Surg 3: 245, 1921 |
|
Salamanca A, Beltran E: Subendometrial contractility in menstrual phase visualized by transvaginal sonography in patients with endometriosis. Fertil Steril 64:193, 1995 |
|
Brosens JJ, Barker FG, De Souza NM: Myometrial zonal differentiation and uterine junctional zone hyperplasia in the non-pregnant uterus. Hum Reprod Update 4: 496, 1998 |
|
Noe M, Kunz G, Herbertz M, et al: The cyclic pattern of the immunocytochemical expression of oestrogen and progesterone receptors in human myometrial and endometrial layers: characterization of the endometrial-subendometrial unit. Hum Reprod 14: 190, 1999. |
|
Mark AS, Hricak H, Heinrichs LW et al: Adenomyosis and leiomyoma: differential diagnosis with MR imaging. Radiology 163: 527, 1987 |
|
Hauth EA, Jaeger HJ, Libera H, Lange S, Forsting M: MR imaging of the uterus and cervix in healthy women: determination of normal values. Eur Radiol 17: 734, 2007 |
|
Tamai K, Togashi K, Ito T et al: MR imaging findings of adenomyosis: correlation with histopathologic features and diagnostic pitfalls. Radiographics 25: 21, 2005 |
|
Wiczyk HP, Janus CL, Richards CJ et al: Comparison of magnetic resonance imaging and ultrasound in evaluating follicular and endometrial development throughout the normal cycle. Fertil Steril 49: 969, 1988 |
|
McCarthy S, Tauber C, Gore J: Female pelvic anatomy: MR assessment of variations during the menstrual cycle and with use of oral contraceptives. Radiology 160: 119, 1986 |
|
Cohen I, Beyth Y, Tepper R et al: Adenomyosis in postmenopausal breast cancer patients treated with tamoxifen: a new entity? Gynecol Oncol 58: 86, 1995 |
|
De Vries K, Lyons EA, Ballard G, et al: Contractions of the inner third of the myometrium. Am J Obstet Gynecol 162: 679, 1990 |
|
Lyons EA, Taylor PJ, Zheng XH, et al: Characterization of subendometrial myometrial contractions throughout the menstrual cycle in normal fertile women. Fertil Steril 55: 771, 1991 |
|
Brosens JJ, De Souza NM, Barker FG: Uterine junctional zone: function and disease. Lancet 346: 558, 1995 |
|
Turnbull LW, Rice CF, Horsman A, et al: Magnetic resonance imaging and transvaginal ultrasound of the uterus prior to embryo transfer. Hum Reprod 9: 2438, 1994 |
|
Tocci A., Greco E, Ubaldi, FM: Adenomyosis and “endometrial-subendometrial myometrium unit disruption disease” are two different entities. Reprod Biomed Online 17: 285, 2008 |
|
Kohnen G, Campbell S, Jeffers MD, Cameron IT: Spatially regulated differenziation of endometrial vascular smooth muscle cells. Hum. Reprod 15: 284, 2000 |
|
Goteri G, Lucarini G, Montik N et al: Expression of Vascular Endothelial Growth Factor (VEGF), Hypoxia Inducible Factor-1alpha (HIF-1alpha), and Microvessel Density in Endometrial Tissue in Women With Adenomyosis. Int J Gynecol Pathol 28(2):157, 2009. |
|
Kang S, Zhao J, Liu Q, et al: Vascular endothelial growth factor gene polymorphisms are associated with the risk of developing adenomyosis. Environ Mol Mutagen 50(5):361,2009. |
|
Tokyol C, Aktepe F, Dilek FH, et al: Expression of Cyclo-oxygenase-2 and Matrix Metalloproteinase-2 in Adenomyosis and Endometrial Polyps and its Correlation With Angiogenesis. Int J Gynecol Pathol 28(2):148, 2009 |
|
Braun DP, Dmowski WP: Endometriosis: abnormal endometrium and dysfunctional immune response Curr Opin Obstet Gynecol 10: 365, 1998 |
|
Taylor HS, Bagot C, Kardana A, et al: HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod 14: 1328, 1999 |
|
Brosens I, Pijnenborg R, Romero R Different types of defective deep placentation in obstetrical syndromes Am J Obstet Gynecol (submitted for publication) |
|
Juang C.-M., Chou P., Yen M.-S., Twu N.-F., Horng H.-C., Hsu W.-L. Adenomyosis and risk of preterm delivery Brit J Obstet Gynaecol 114(2):165, 2007. |
|
Fernando, S., Breheny, S., Jaques, A.M., Halliday, J.L., Baker, G. Healy, D. Preterm birth, ovarian endometriomata, and assisted reproduction technologies. Fertil Steril 91:325, 2009. |
|
Stephansson O, Kieler H, Granath F, Falconer H Endometriosis, assisted reproduction technology, and risk of adverse pregnancy outcome Hum Reprod 24:2341, 2009. |
|
Landi, S., Mereu, L., Pontrelli, G., et al The Influence of adenomyosis in patients laparoscopically treated for deep endometriosis. J Minim Invasive Gynecol 2008 15 (5), pp. 566-570 |
|
Pijnenborg R, Vercruysse L, Hanssens M. The uterine spiral arteries in human pregnancy: facts and controversies. Placenta 27: 939, 2006 |
|
Brosens I, Derwig I, Brosens J, Fusi L, Benagiano G, Pijnenborg R. The enigmatic uterine junctional zone: the missing link between reproductive disorders and major obstetrical syndromes Hum Reprod 25:569, 2010. |
|
Trogstad L, Magnus P, Skjaerven R, Stoltenberg C: Previous abortions and risk of pre-eclampsia. Int J Epidemiol 37: 1333, 2008 |
|
Brosens JJ, Pijnenborg R, Brosens IA: The myometrial junctional zone spiral arteries in normal and abnormal pregnancies. Am J Obstet Gynecol 187: 1416, 2002 |
|
Hanna J, Goldman-Wohl D. Hamani Y, et al: Decidual NK cells regulate key developmental processes at the human fetal-maternal interface. Nature Med 12: 1065, 2006 |
|
Xavier P, Beires J, Barros H, Martinez-De-Oliveira J: Subendometrial and intraendometrial blood flow during the menstrual cycle in patients with endometriosis. Fertil Steril 84: 52, 2005 |
|
Klemmt PAB, Carver JG, Kennedy SH, et al: Stromal cells from endometriotic lesions and endometrium from women with endometriosis have reduced decidualization capacity. Fertil Steril 85: 564, 2006 |
|
Minici F, Tiberi F, Tropea A et al.: Endometriosis and human infertility: A new investigation into the role of eutopic endometrium. Hum Reprod 23: 530, 2008 |
|
Gellersen B, Brosens IA, Brosens JJ: Decidualization of the human endometrium: Mechanisms, functions, and clinical perspectives. Seminars Reprod Med 25: 445, 2007 |
|
Chan RW, Schwab KE, Gargett CE: Clonogenicity of human endometrial epithelial and stromal cells. Biol. Reprod 70: 1738, 2004 |
|
Schwab KE, Chan RW, Gargett CE: Putative stem cell activity of human endometrial epithelial and stromal cells during the menstrual cycle. Fertility Sterility 84: 1124, 2005 |
|
Sivridis E, Giatromanolaki A : New insights into the normal menstrual cycle-regulatory molecules. Histol. Histopathol 19: 511, 2004 |
|
Sasson IE, Taylor HS: Stem Cells and the Pathogenesis of Endometriosis. Annals of the New York Academy of Sciences 1127: 106, 2008 |
|
Dueholm M, Lundorf E, Hansen ES et al: Magnetic resonance imaging and transvaginal ultrasonography for the diagnosis of adenomyosis. Fertil Steril 76: 588, 2001 |
|
Bazot M, Cortez A, Darai E et al: Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Hum Reprod 2001;16:2427-33 |
|
Parrott E, Butterworth M, Green A et al: Adenomyosis--a result of disordered stromal differentiation. Am J Pathol 159 :623, 2001 |
|
Greaves P, White IN: Experimental adenomyosis. Best Pract Res Clin Obstet Gynaecol 20: 503, 2006 |
|
Yuen PM: Adenomyosis following endometrial rollerball ablation. Aust N Z J Obstet Gynaecol 35 :335, 1995 |
|
Ostrezenski A: Extensive iatrogenic adenomyosis after laparoscopic myomectomy Fertil Steril 69: 143, 1998 |
|
Tamai K, Koyama T, Umeoka S, et al: Spectrum of MR features in adenomyosis Best Prat Res Clin Obstet. Gynaecol 20: 583, 2006 |
|
Reinhold C, McCarthy S, Bret PM, et al: Diffuse adenomyosis: comparison of endovaginal US and MR imaging with histopathologic correlation. Radiology 199: 151, 1996 |
|
Kitajima K, Imanaka K, Kuwata Y et al: Magnetic resonance imaging of typical polypoid adenomyoma of the uterus in 8 patients: correlation with pathological findings. J Comput Assist Tomogr 31: 463, 2007 |
|
Takeda A, Sakai K, Mitsui T, Nakamura H: Laparoscopic management of juvenile cystic adenomyoma of the uterus: report of two cases and review of the literature J Minim Invasive Gynec 14: 370, 2007 |
|
Protopapas A, Milingos S, Markaki S, et al: Cystic Uterine Tumors Gynecol Obstet Invest 65: 275, 1980 |
|
Donnez J, Nisolle M, Casanas-Roux F et al: Rectovaginal septum, endometriosis or adenomyosis: laparoscopic management in a series of 231 patients. Hum Reprod 10: 630, 1995 |
|
Ijland MM, Evers JLH, Dunselman GAJ et al: Relation between wavelike activity and fecundability in spontaneous cycles. Fertil Steril 67: 492, 1997 |
|
Bulletti C, De Ziegler D: Uterine contractility and embryo implantation. Curr Opin Obstet Gynecol 18: 473, 2006 |
|
Fusi L, Cloke B , Brosens JJ: The uterine junctional zone. Best Practice & Res Clin Obstet Gynecol 20: 479, 2006 |
|
Fanchin R, Rhigini C, Olivennes F et al.: Uterine contractions at the time of embryo transfer alter pregnancy rate after in vitro fertilisation. Hum Reprod 13: 1968, 1998 |
|
Killick S: Ultrasound and the receptivity of the endometrium. Reprod Biomed Online 15: 63, 2007 |
|
Kido A, Togashi K, Nishino M et al.: Cine MR imaging of uterine peristalsis in patient with endometriosis. Eur Radiol 17: 1813, 2007 |
|
Leyendecker G, Kunz G, Wildt L et al.: Uterine peristalsis and dysperistalsis as dysfunction of the mechanism of rapid sperm transport in patients with endometriosis and infertility. Hum Reprod 11: 1542, 1996 |
|
Leyendecker G, Kunz G, Herbertz M et al. : Uterine peristaltic activity and the development of endometriosis.. Ann NY Acad Sci 1034: 338, 2004 |
|
Yang J-H, Ho H-N, Yang Y-S: Current diagnostic and treatment strategies for adenomyosis. Expert Rev. Obstet. Gynecol 1: 111, 2006 |
|
Furuhashi M, Miyabe Y, Katsumata Y, et al: Comparison of complications of vaginal hysterectomy in patients with leiomyomas and in patients with adenomyosis. Arch Gynecol Obstet 262: 69, 1998 |
|
Bohlman ME, Ensor RE, Sanders RC: Sonographic findings in adenomyosis of the uterus. Am J Roentgenol 148: 765, 1987 |
|
Togashi K, Nishimura K, Itoh K, et al: Adenomyosis: diagnosis with MR imaging. Radiology 166: 111, 1988 |
|
Loffer FD: Endometrial ablation and resection. Curr Opin Obstet Gynecol 7: 290, 1995 |
|
Pagedas AC, Boe IH, Perkins HE: Review of 24 cases of uterine ablation failure. J Am Assoc Gynecol Laparosc 2: 239, 1995 |
|
McCausland AM, McCausland VM: Depth of endometrial penetration in adenomyosis helps determine outcome of rollerball ablation. Am J Obstet Gynecol 174: 1786, 1996 |
|
Wortman M, Daggett A: Reoperative hysteroscopic surgery in the management of patients who fail endometrial ablation and resection. J Am Assoc Gynecol Laparosc 8: 272, 2001 |
|
McCausland V, McCausland A: The response of adenomyosis to endometrial ablation/resection. Hum Reprod Update 4: 350, 1998 |
|
Wang CJ, Yen CF, Lee CL, Soong YK: Laparoscopic uterine artery ligation for treatment of symptomatic adenomyosis. J Am Assoc Gynecol Laparosc 9: 293, 2002 |
|
Nishida M, Takano K, Arai Y, et al: Conservative surgical management for diffuse uterine adenomyosis. Fertility and Sterility Apr 28. [Epub ahead of print], 2009. |
|
Fujishita A, Masuzaki H, Khan KN, et al: Modified reduction surgery for adenomyosis. A preliminary report of the transverse H incision technique. Gynecol Obstet Invest 57: 132, 2004 |
|
Liu X, Huang H, Huang R, et al: Clinical observation of conservative surgery for adenomyosis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 20: 440, 1998 |
|
Phillips DR, Nathanson HG, Milim SJ, Haselkorn JS: Laparoscopic bipolar coagulation for the conservative treatment of adenomyomata. J Am Assoc Gynecol Laparosc 4: 19, 1996. |
|
Nabeshima H, Murakami T, Terada Y, et al: Total laparoscopic surgery of cystic adenomyoma under hydroultrasonographic monitoring. J Am Assoc Gynecol Laparosc 10: 195, 2003 |
|
Morita M, Asakawa Y, Nakakuma M, Kubo H: Laparoscopic excision of myometrial adenomyomas in patients with adenomyosis uteri and main symptoms of severe dysmenorrhea and hypermenorrhea. J Am Assoc Gynecol Laparosc 11: 86, 2004 |
|
Ozaki T, Takahashi K, Okada M, et al: Live birth after conservative surgery for severe adenomyosis following magnetic resonance imaging and gonadotropin-releasing hormone agonist therapy. Int J Fertil Womens Med 44: 260, 1999 |
|
Huang WH, Yang TS, Yuan CC: Successful pregnancy after treatment of deep adenomyosis with cytoreductive surgery and subsequent gonadotropin-releasing hormone agonist: a case report. Zhonghua Yi Xue Za Zhi (Taipei) 61: 726, 1998 |
|
Lin J, Sun C, Li R: Gonadotropin releasing hormone agonists in the treatment of adenomyosis with infertility. Zhonghua Fu Chan Ke Za Zhi 34: 214, 1999 |
|
Wang PH, Yang TS, Lee WL, et al: Treatment of infertile women with adenomyosis with a conservative microsurgical technique and a gonadotropin-releasing hormone agonist. Fertil Steril 73: 1061, 2000 |
|
Pafumi C, Farina M, Pernicone G, et al: Adenomyosis and uterus rupture during labor. Zhonghua Yi Xue Za Zhi (Taipei) 64: 244, 2001 |
|
Bensaid F, Kettani F, El Fehri S, et al: Obstetrical complications of adenomyosis. Literature review and two case reports. J Gynecol Obstet Biol Reprod (Paris) 25: 416, 1996 |
|
Siskin GP, Tublin ME, Stainken BF et al: Uterine artery embolization for the treatment of adenomyosis: clinical response and evaluation with MR imaging. Am J Roentgenol 177: 297, 2001 |
|
Kim MD, Won JW, Lee DY, Ahn CS: Uterine artery embolization for adenomyosis without fibroids. Clin Radiol 59: 520, 2004 |
|
Kim MD, Kim NK, Kim HJ, Lee MH: Pregnancy following uterine artery embolization with polyvinyl alcohol particles for patients with uterine fibroid or adenomyosis. Cardiovasc Intervent Radiol 28: 611, 2005 |
|
Fukunishi H, Funaki K, Sawada K, et al: Early Results of Magnetic Resonance–guided Focused Ultrasound Surgery of Adenomyosis: Analysis of 20 Cases. J Min Inv Gynecol 15: 571, 2008 |
|
Cho S, Nam A, Kim H, et al: Clinical effects of the levonorgestrel-releasing intrauterine device in patients with adenomyosis. Am J Obstet Gynecol 198: 373, 2008 |
|
Sheng J, Zhang WY, Zhang JP, Lu D: The LNG-IUS study on adenomyosis: a 3-year follow-up study on the efficacy and side effects of the use of levonorgestrel intrauterine system for the treatment of dysmenorrhea associated with adenomyosis. Contraception 79: 189, 2009 |
|
Shawki OA.: Danazol loaded intrauterine device (D-IUD): A novel conservative management for uterine adenomyosis. Middle East Fertil Soc J, 7(3):214, 2002. |
|
Igarashi M, Abe Y, Fukuda M, et al: Novel conservative medical therapy for uterine adenomyosis with a danazol-loaded intrauterine device. Fertil Steril 74: 412, 2000 |
|
Noble LS, Simpson ER, Johns A, Bulun SE: Aromatase expression in endometriosis. J Clin Endocrinol Metab 81: 174, 1996 |
|
Bulun SE, Fang Z, Imir G, et al: Aromatase and endometriosis. Semin Reprod Med 22: 45, 2004. |
|
Ezaki K, Motoyama H, Sasaki H: Immunohistologic localization of estrone sulfatase in uterine endometrium and adenomyosis. Obstet Gynecol 98: 815, 2001 |
|
Soysal S, Soysal ME, Ozer S, et al: The effects of post-surgical administration of goserelin plus anastrozole compared to goserelin alone in patients with severe endometriosis: a prospective randomized trial. Hum Reprod 19: 160, 2004 |
|
Amsterdam LL, Gentry W, Jobanputra S, et al: Anastrazole and oral contraceptives: a novel treatment for endometriosis. Fertil Steril 84: 300, 2005 |
|
Novella-Maestre E, Carda C, Noguera I, et al: Dopamine agonist administration causes a reduction in endometrial implants through modulation of angiogenesis in experimentally induced endometriosis. Hum Reprod 24 :1025, 2009 |
|
Vlahos NF, Gregoriou O, Deliveliotou A et al.: Effect of pentoxifylline on vascular endothelial growth factor C and flk-1 expression on endometrial implants in the rat endometriosis model. Fertil Steril 93: 1316, 2010 |