Ovarian Hyperstimulation Syndrome Prevention
Authors
INTRODUCTION
Ovarian hyperstimulation syndrome (OHSS) is the price we occasionally pay for our attempt to override nature’s delicate balances that were created to ensure a single oocyte ovulation in the human. Spontaneous OHSS does occur;1, 2 however, it is rare. While natural cycle-based assisted reproductive technologies (ART) were responsible for the birth of the first in vitro fertilization (IVF) baby3 this method was abandoned because of its inherent low efficiency. Instead, gonadotropins have been used for decades in order to increase the yield of fertilizable oocytes. Typically, in these cycles, human chorionic gonadotropin (hCG) is used as a surrogate for luteinizing hormone (LH) for the purpose of oocyte maturation and induction of ovulation. Given its significantly longer half-life (>24 h versus 60 min for LH4, 5), hCG administration results in a prolonged luteotrophic effect, characterized by the development of multiple corpura lutea (CL) and supraphysiological levels of estradiol and progesterone. This sustained luteotrophic effect may result in the development of OHSS, still the most frequent and severe complication of ovarian stimulation treatments. OHSS cannot develop without functioning CL. The aim of this chapter is to review the available methods used for OHSS prevention, and to focus on the one approach that totally prevents this iatrogenic complication.
Incidence
The incidence of OHSS peaked during the 1990s as IVF practitioners aimed at getting a large number of oocytes.6 It was estimated that the incidence of severe OHSS was 0.2–1.0% of all ART cycles,7 and the associated mortality rate was estimated at 1:45,000–1:50,000 infertile women receiving gonadotropins.8
The introduction of gonadotropin releasing hormone (GnRH) antagonists in the late 1990s generated hopes that their use would be associated with a lower incidence of OHSS.9 However, subsequent large studies failed to verify that trend. Papanikolaou et al.10 summarized their experience in a prospective cohort study of women undergoing IVF treatment with a GnRH antagonist protocol over a 2-year period. A total of 1801 patients were included in that study, and underwent 2524 cycles. Fifty-three patients were hospitalized because of OHSS (2.1%). The researchers concluded that ‘clinically significant OHSS still remains a limitation of multifollicular ovarian stimulation for IVF even with the use of GnRH antagonist protocols’. Therefore, ‘there is more than ever an urgent need for alternative final oocyte maturation-triggering medication’. This alternative is available, as detailed below and completely eliminates OHSS.
Further insight into the incidence of OHSS following GnRH antagonist protocol and hCG as ovulation trigger can also be gained from a very large (1506 treated patients) prospective randomized study on the use of long-acting rFSH (corifollitropin-α).11 In an effort to minimize OHSS incidence the researchers took the following steps:
- Patients who had a history of ovarian hyperresponse (more than 30 follicles ≥11 mm) or OHSS, polycystic ovary syndrome (PCOS) or a basal antral follicle count (AFC) of more than 20 on ultrasound (<11 mm, both ovaries combined) were excluded from participation.
- If, in the opinion of the investigator, the high ovarian response was too high, a lower dose of hCG (5000 IU) could be used, instead of the routine 10,000 IU dose.
- Whenever deemed necessary by the investigator, rFSH administration could be withheld for a maximum of 3 days (coasting).
- If, in the opinion of the investigator, the high ovarian response was too high, the cycle could be canceled at any time.
- In case of a risk for OHSS, defined as more than 30 follicles of ≥11 mm on ultrasound, hCG was always to be withheld and the treatment cycle canceled as per protocol.
The result of all these safety measures was disappointing. A total of 53 patients in the corifollitropin-α-treated group (7.0%) and 47 patients in the rFSH-treated group (6.3%) developed OHSS in this trial. The incidence of (moderate/severe) OHSS was 4.1% (31/755) and 2.7% (20/750) for the corifollitropin-α and rFSH groups, respectively. In addition, pelvic pain or pelvic discomfort was reported by 23% of the patients. GnRH antagonist-based protocol did not significantly change OHSS incidence.
Grave predictions
Given the high incidence of OHSS, researchers in the late 1990s and early 2000s developed the notion that OHSS cannot be prevented. Abramov et al.12 posed the question if this is the price we have to pay since ’various prophylactic methods, e.g. i.v. albumin or coasting do not appear to reliably prevent OHSS in all cases’. Forman13 added that ‘severe OHSS will remain a complication of IVF cycles despite all attempts at prevention’. Finally, Egbase14 claimed that: ‘These are the cases in which severe OHSS is probably not preventable with current strategies except cancellation of the cycle. None of the strategies currently employed to avert severe OHSS when excessive multiple follicular growth is encountered in the course of controlled ovarian stimulation completely prevents the condition’.
These researchers chose to ignore the one approach that completely prevents OHSS, although it was described as early as 1988, as is shown herein.
PREVENTIVE STRATEGIES
In most cases OHSS risk can be prevented before ovarian stimulation is started. For example, young, thin, amenorrheic patients are at increased risk, therefore low dose gonadotropin must be used in these women. Similarly, young menstruating patients with high antral follicular count (AFC) must be approached in the same manner. However, we commonly encounter high responding patients during stimulation, for whom we must employ preventive strategies. The safest way to prevent OHSS is to abort the cycle, e.g. stop ovarian stimulation and let all growing follicles undergo demise by atresia. As mentioned above, a prerequisite for OHSS development is ovulation and CL formation. Ovarian stimulation per se does not cause OHSS, unless it is followed by ovulation. In ART cycles the ovulatory agent most commonly used is hCG, therefore, withholding it prevents OHSS. Of course, it also cancels the cycle, with all the emotional, economic and medical implications involved. Therefore, a good preventive strategy must ensure that oocyte retrieval takes place, and that it leaves the patient with a fair chance to achieve safe, OHSS-free pregnancy.
Coasting
This term is used by marine vessels near their destination when they move without further use of propelling power. In ovarian stimulation the propelling powers are gonadotropins, hence, coasting means stopping gonadotropin injections in OHSS high-risk patients, until serum estradiol falls into an acceptable range (typically less than 11,000 pmol/l). Coasting is popular in long GnRH agonist-based cycles, because there are no other options other than cycle cancellation. Being deprived of gonadotropins, some oocytes undergo atresia; therefore, it is not recommended to coast for more than 3–4 days.15
Although frequently used, the efficacy of coasting in OHSS prevention is not well established. In 2002, a Cochrane review concluded that there was a lack of randomized controlled trials where coasting was compared with no coasting or other interventions. Therefore, there is insufficient evidence to determine whether coasting is an effective strategy for preventing OHSS.16
Intravenous albumin
This strategy employs intravenous albumin around the time of oocyte retrieval. The dose and timing of administration of albumin varies between trials. While Shoham et al.17 used 50 g albumin 2 h before oocyte retrieval, Shalev et al.18 used 20 g albumin just after oocyte retrieval, and Isik et al.19 used 10 g albumin 2 h before oocyte retrieval. Gokmen et al.20 used 10 g albumin immediately after oocyte retrieval and Ben-Chetrit et al.21 used 50 g albumin 1 h before oocyte retrieval. The story of albumin as a preventive strategy leaves nothing to be proud of in view of the plasticity with which seemingly ‘rigid’ meta-analysis led to erroneous conclusions. Preliminary enthusiasm,17, 19 while ignoring negative reports,22, 23 led to hasty formal meta-analysis of only five trials with a total of 378 patients.24
Not surprisingly, two independent meta-analyses, with more than 1000 patients in each, reached the conclusion that intravenous albumin administration in high-risk patients does not appear to reduce the occurrence of severe OHSS.25, 26
This unfortunate sequence of events illustrates the potential inborn bias in too hasty use of ‘evidence based medicine’, i.e. meta-analysis before sufficient data are accumulated. Unfortunately, this is not an isolated case. Nevertheless, based on current knowledge, there is no room for intravenous albumin in the context of OHSS prevention.
‘Freeze all’
This technique refers to triggering ovulation with hCG while cryopreserving all zygotes or embryos, so pregnancy cannot occur. Obviously, the severe late onset, pregnancy-associated OHSS is prevented; however, early OHSS can still occur. A formal meta-analysis concluded that there is insufficient evidence to support routine cryopreservation.27
Importantly, we must remember that early OHSS can be a severe disease.28
Dopamine agonists
The pathophysiological hallmark of OHSS is increased vascular permeability. Following hCG administration in a rat model, vascular endothelial growth factor (VEGF) and VEGF receptor 2 (VEGFR-2) expression increased significantly.29
Since the dopamine agonist cabergoline can reverse VEGFR-2-dependent increased vascular permeability,29 its use in the context of OHSS prevention was tested in humans (egg donors). It was found that cabergoline (0.5 mg daily, from the day of hCG trigger, for 8 days) can significantly reduce the incidence of moderate OHSS, as well as pelvic fluid accumulation and hemoconcentration, when compared with placebo in oocyte donors at risk of OHSS.30
Another non-ergot derived dopamine agonist, quinagolide, was tested in routine IVF patients.31 While quinagolide appeared to prevent moderate/severe early OHSS, it was associated with poor tolerability (mostly vomiting, nausea, dizziness and somnolence).
A systematic review and meta-analysis of randomized trials comparing the prophylactic effect of cabergoline versus no treatment in IVF/intracytoplasmic sperm injection (ICSI) cycles showed that there was evidence of a statistically significant reduction in the incidence of OHSS in the cabergoline group, but there was no statistically significant evidence of a reduction in severe OHSS.32
Reducing hCG dose
As mentioned above, the culprit of OHSS is the use of hCG as an ovulatory agent. Therefore, it could be logical to reduce its dose as much as possible as a preventive measure. However, clinical data do not support this notion.33
Apparently, even the lowest dose of hCG (3300 IU) did not curb OHSS incidence or severity. The lowest effective hCG dose for ovulation induction is not known, and it probably depends on numerous variables, mostly the patient weight. A positive correlation was found between serum hCG concentration on the day after hCG administration and OHSS incidence34 implying that ovulatory hCG dose must be as low as possible, yet, this cannot be taken as a global preventive strategy.
Recombinant LH instead of hCG
The most natural compound with which to trigger final oocyte maturation and with an expected low incidence of OHSS would have been LH. Thus, when recombinant LH (rLH) was introduced, a clinical trial was performed to explore the efficacy of rLH to trigger ovulation in a long GnRH agonist (GnRHa) downregulation protocol.35 Doses ranging between 5000 IU and 30,000 IU, as well as a dual administration of 15,000 IU followed by 10,000 IU 3 days later, were explored. However, apart from the significant increase in cost of treatment, a low implantation rate was seen after only one bolus of rLH to trigger ovulation; moreover, a disappointingly high OHSS rate (12%) was reported. Therefore, the option of rLH as trigger is not available at this time (early 2011).
GnRH AGONIST TRIGGER
The notion that GnRHa trigger eliminates OHSS in high-risk patients was first introduced by Itskovitz et al.36 GnRHa elicits pituitary secretion of gonadotropins, which can be used for triggering oocyte maturation and ovulation, if given at the right time of the cycle. Numerous compounds, administered in different regimens, have been successfully used for this purpose. It appears that a single administration of a GnRHa in a dose of 200–500 µg effectively and reliably triggers the required gonadotropin surge.37, 38
The pituitary and ovarian responses to midcycle GnRHa injections in stimulated cycles have been described previously.39 The injection of GnRHa results in an acute release of LH and FSH. Serum LH and FSH levels rise for 4 and 12 hours, respectively, and are elevated for 24–36 h. The amplitude of the surge is similar to that seen in the normal menstrual cycle, but by contrast with the natural cycle, the surge consists of only two phases: a short ascending limb (>4 hours) and a long descending limb (>20 hours). This has no bearing on the ovarian hormone secretion pattern, which is qualitatively similar to the pattern observed in a natural cycle. The LH surge is associated with a rapid rise of progesterone and the attainment of peak estradiol levels during the first 12 hours after GnRHa administration. This is followed by a transient suppression of progesterone biosynthesis and a gradual decline in estradiol levels during the 24 hours preceding follicle aspiration. After oocyte retrieval, a second rapid rise in progesterone and continuous fall in estradiol are observed, reflecting normal transitions from follicular to luteal phase in ovarian steroidogenesis.
Whereas the endogenous LH surge triggered by GnRHa is associated with an apparently normal early follicular–luteal shift in ovarian steroidogenesis, serum levels of estradiol and progesterone during the luteal phase are lower compared with those achieved after hCG administration. This may be related to the longer duration of plasma hCG activity compared with the shorter GnRHa-induced LH elevation. Since normal function of the corpus luteum depends on pituitary pulsatile LH secretion,40 it is possible, therefore, that the presumed down-regulation of pituitary GnRH receptors after a midcycle injection of GnRHa results in reduced LH support for the developing corpura lutea, reduced steroidogenesis, and early, quick and robust luteolysis.
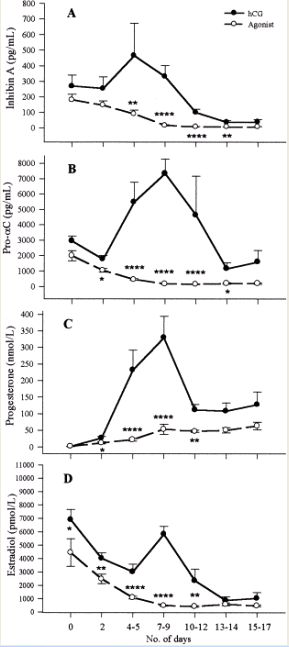
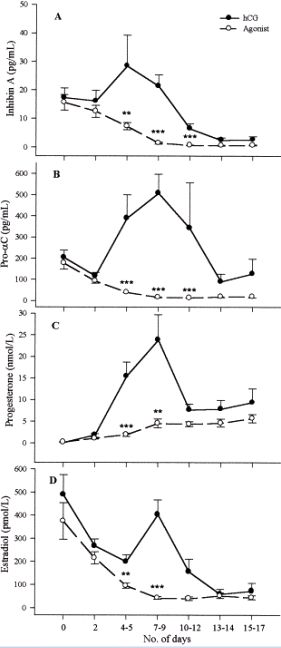
To document luteolysis, a small randomized controlled study was conducted comparing normally responding patients who were triggered with either GnRHa or hCG. Since the corpus luteum is recognized as the major source of inhibin A and pro-αC production during the luteal phase and early pregnancy,41, 42, 43 these two peptides were measured to reflect corpura lutea activity. The results show, unequivocally, that GnRHa causes quick luteolysis (Figs. 1 and 2).44
{kind=link}
{kind=link}
Importantly, if pregnancy is achieved, the endogenous hCG production does not rescue the corpura lutea. This issue is crucial for OHSS prevention, since late-onset pregnancy-associated OHSS is the more severe and protracted form. In summary, the lower levels of steroidal and nonsteroidal hormones, which are secreted by corpura lutea, are closer to the physiological range in patients triggered with GnRH agonist (in comparison with the hCG-treated patients) and may explain, at least in part, the mechanism of OHSS prevention.45 Based on these considerations, it is important to consider patient-specific luteal support. Primarily, ovarian response dictates a clinical approach to luteal support, but also patient comfort is a consideration.
The most important benefit emerging from the use of GnRHa, rather than hCG, for ovulation induction is the ability of this regimen to completely eliminate the threat of clinically significant OHSS. It should be emphasized that the clinical findings attributable to mild OHSS46 (e.g. ovarian enlargement, abdominal discomfort, and excessive steroid production) are an integral part of most cases of ovulation induction in IVF and are not clinically relevant. Effective ovulation is triggered with no risk of OHSS even in patients with extremely high estradiol levels during the late follicular phase.
Previous reports described cases in which OHSS developed despite the use of GnRHa to induce ovulation. Three cases of mild to moderate OHSS after nasal GnRHa trigger were reported by van der Meer et al.47 Gerris et al.48 have also reported OHSS following this approach; however, they used native GnRH (and not GnRHa), resulting in successful ovulation triggering but without the critical gonadotropin suppression, which is the key element in preventing OHSS. Shoham et al.49 reported a personal communication of two OHSS cases. Another group has presented its large and impressive experience with this strategy.50 Of 708 PCO, high responder IVF patients (mean estradiol on the day of ovulation triggering 7817 pg/ml), ovulation was effectively triggered with GnRHa in 682 (96%). One patient (0.1%) developed severe OHSS after being treated with hCG-based luteal support, probably in error, because the protocol dictated progesterone-only luteal support. In 18 patients the GnRHa-induced LH surge was judged as ‘inadequate’, hCG was used, resulting in 11 cases (61%) of severe OHSS. This last figure may reflect the large number of severe OHSS cases in this series that were prevented by this strategy. Kovachev described one case of OHSS in 29 PCO patients.51 Similarly, Dong et al. described one case of OHSS in 14 PCO patients.52
However, an overwhelming body of evidence clearly shows (as summarized in Table 1) that OHSS does not occur following GnRHa trigger.
Table 1. Summary of published studies (2006–2010) comparing human chorionic gonadotropin (hCG) and gonadotropin releasing hormone agonist (GnRHa) trigger
OHSS | n | Ovulation trigger | Oocyte source | Trial type | Reference | |
| % | n | |||||
0 31 | 0/13 4/13 | 15 13 | *GnRHa †hCG | Own | RCT, high risk | Babayof et al., 200653 |
0 31 | 0/33 10/32 | 33 32 | GnRHa hCG | Own | RCT, high risk | Engamnn et al., 200854 |
0 17 | 0/30 5/30 | 30 30 | GnRHa hCG | Donors | RCT | Acevedo et al., 200655 |
0 1.3 | 0/1046 13/1031 | 1046 1031 | GnRHa hCG | Donors | Retrospective | Bodri et al., 2009 |
0 | 0/40
| 40 | GnRHa | Own | Observational, high risk | Griesinger et al., 2010 |
0 2 | 0/152 3/150 | 152 150 | GnRHa hCG | Own | RCT | Humaidan et al., 200961 |
0 4 | 0/23 1/23 | 23 23 | GnRHa hCG | Own | Retrospective, case-controlled, high risk | Engmann et al., 2006 |
0 | 0/42
| 42 | GnRHa hCG – canceled | Own | Retrospective case-control, high risk | Manzanares et al., 2009 |
0 6 | 0/254 10/175 | 254 175 | GnRHa hCG | Donors | Retrospective | Hernandez et al., 2009 |
0 7 | 0/82 5/69 | 82 69 | GnRHa hCG | Own | Retrospective, high risk | Orvieto et al., 2006 |
0 1 | 0/32 1/42 | 32 42 | GnRHa hCG | Donors | Retrospective, high risk: agonist arm only | Shapiro et al., 2007 |
0 7 | 0/44 3/44 | 44 44 | GnRHa hCG | Donors | RCT | Sismanoglu et al., 2009 |
8 | 1/12 | 12 | GnRH, luteal rescue with hCG 1500 IU | Own | Observational, high risk | Humaidan et al., 2009 |
0 8 | 0/106 9/106 | 106 106 | GnRHa hCG | Donors | RCT | Galindo et al., 2009 |
0 16 | 0/50 08/50 | 50 50 | GnRHa hCG | Donors | RCT | Melo et al., 2009 |
0 15 | 0/45 5/33 | 45 33 | GnRHa hCG | Own | RCT, high risk | Shahrokh et al., 2010 |
*2005 patients, no cases OHSS (0%)
†1810 patients, 92 cases OHSS (5.1%)
RCT, randomized controlled trial
A practical major limitation of GnRHa trigger is that it cannot be effective in women with a low pituitary gonadotropin reserve. Therefore, it is not applicable in IVF stimulation cycles during which pituitary downregulation with a GnRHa is used (‘long protocol’). This protocol renders the pituitary unresponsive for induction of an endogenous LH surge. Because GnRHa-based protocols were used routinely by most IVF programs until the year 2000, GnRHa-induced ovulation for OHSS prevention has not gained much popularity. The introduction of GnRH antagonists in controlled ovarian hyperstimulation protocols has opened new opportunities for novel stimulation protocols.
The tremendous strength of the proposed approach is also its weakness in terms of evidence-based medicine. Two groups performed randomized controlled studies with patients at high risk of OHSS.53, 54 A third group55 used the donor–recipient model to elucidate the role of agonist trigger in terms of OHSS incidence and pregnancy rate, while neutralizing the ‘endometrial factor’. The main conclusion emerging from all three studies is clear: agonist trigger prevents OHSS. In fact, none of the patients allocated to the GnRHa trigger arm in all three studies developed OHSS.
The question of pregnancy rate post agonist trigger
A meta-analysis in 2006 summarized the results of three randomized controlled trials comprising a total of 275 patients.56 Although the occurrence of OHSS was significantly reduced when GnRHa was used to trigger final oocyte maturation, the pooled data from all the randomized studies also showed a significant reduction in the clinical pregnancy rate (7.9% in the GnRHa group versus 30.14% in the hCG group, p = 0.02). The negative impact was ascribed to a luteal phase deficiency (reduced endogenous progesterone production and low endogenous LH secretion around the time of implantation) and not to a poor oocyte quality, which was supported by good birth rates in frozen–thawed embryo replacement cycles in which the embryos derived from GnRHa triggered cycles.57
In the initial studies included in the above meta-analysis, the luteal support was a standard support with vaginal progesterone and oral estradiol. Interestingly, the initial serum hCG levels, indicative of implantation, were comparable between GnRHa and hCG triggering;58, 59 however, during the following weeks a high early pregnancy loss was seen in the GnRHa group. Therefore, it was speculated that the conventional luteal progesterone support, although supplemented with estradiol, was insufficient, indicating the need for a more intense luteal steroid treatment or supplementation with LH activity. Sufficient luteal LH activity can be secured with hCG administration. Indeed, a number of trials were conducted in IVF/ICSI patients, using GnRHa to trigger final oocyte maturation in GnRH antagonist co-treated cycles, supplementing patients with one bolus of 1500 IU hCG on the day of ovum pick-up (OPU) in addition to a standard luteal phase support with vaginal progesterone and oral estradiol.60, 61, 62
The small supplementary bolus of hCG clearly rescued the luteal phase after GnRHa triggering, resulting in a normal reproductive outcome. Thus, in the latest study (the largest randomized trial to date) including a total of 302 IVF/ICSI cycles – a not significant difference in delivery rate was seen between GnRHa triggering supplemented with a bolus of 1500 IU hCG after OPU and 10,000 IU hCG. Interestingly, no OHSS case was seen in the GnRHa group versus 2% in the 10,000 IU hCG group, despite the fact that more than one-third of patients in each group had 14 follicles or more that were more than or equal to 11 mm on the day of triggering.
Another way of adding LH activity to the LH insufficient luteal phase after GnRHa triggering could theoretically be repeated doses of recombinant LH (rLH). The advantage of rLH over hCG is its significantly shorter half-life, which could further reduce the risk of OHSS. To explore this concept, a pilot study was performed by Papanikolaou et al.63 Ovarian stimulation was performed using a fixed dose of 187.5 IU FSH starting on cycle day 2 in a fixed stimulation day 6 GnRH antagonist protocol in a total of 35 IVF/ICSI patients. Ovulation triggering was performed with 0.2 mg triptorelin. Six alternate doses of 300 IU rLH were administered starting on the day of OPU and repeated on days OPU + 2, OPU + 4, OPU + 6, OPU + 8 and OPU + 10 – in addition to vaginally administered micronized progesterone (600 mg daily). The control group (n = 17), consisted of patients undergoing the same stimulation protocol, having hCG to trigger ovulation. A comparable number of oocytes (13.8 versus 11.7) and embryos (8.3 versus 7.9) were seen in the GnRHa and hCG groups, respectively. All patients underwent elective single blastocyst transfer, resulting in a nonsignificant difference in delivery rate in the rLH group versus the hCG group (22.20% (n = 4/18) vs. 23.5% (n = 4/17), respectively, p = 0.91). No OHSS case was recorded in either group, but a larger sample size is necessary to draw conclusions regarding the efficacy and dose of rLH for luteal support after GnRHa triggering.
As the ideal type of luteal phase support after GnRHa has not yet been clearly defined, another point of action could be intensive luteal phase support along with close monitoring of serum steroid levels after GnRHa triggering. This concept was evaluated by Engmann et al.54 in a randomized controlled trail including a total of 59 OHSS high-risk patients, randomized to either dual pituitary suppression (OCP overlapping with GnRHa) followed by triggering of final oocyte maturation with hCG in a dose ranging from 3300 IU to 10,000 IU depending on follicular response and serum estradiol levels (hCG group; 32 patients), or a GnRH antagonist protocol followed by final oocyte maturation with a bolus of GnRHa (leuprolide acetate, 1 mg) (GnRHa group; 33 patients). The luteal phase supplementation consisted of 50 mg of IM progesterone daily starting the day after oocyte retrieval until approximately 10 weeks of gestation. Additionally, the patients received three 0.1 mg estradiol transdermal patches every other day, commencing the day after oocyte retrieval. This protocol resulted in an ongoing pregnancy rate after GnRHa triggering of 53% and no OHSS in the GnRHa group, versus 34% OHSS in the control group (10/29): five mild, four moderate and one severe case.
In summary, to secure a good clinical pregnancy rate post agonist trigger, luteal support must be patient-tailored. In OHSS high risk situations intensive estradiol and progesterone support will eliminate any threat of OHSS and will yield a good pregnancy rate. In normal responders, with no risk of OHSS, two boluses of hCG 1500 IU, one on the day of OPU and another 4–5 days later will supply enough luteal LH activity. In fact, it seems that luteal dual hCG administration may give enough luteal LH activity so that any additional estradiol and progesterone supplementation will be redundant. This ‘patient friendly’ luteal support will have a great advantage for those patients who become pregnant.
Agenda-driven meta-analysis?
Meta-analyses, especially those published as Cochrane Reviews, are internationally recognized as the highest standard in evidence-based health care as formulated on their website. A Cochrane analysis is supposed to conduct systematic reviews of primary research in human health care and health policy. However, one might ask at which level of clinical development a Cochrane Review should be performed. Clearly, the development of new strategies demands many clinical trials; trials which obviously are ‘on their way’ towards the optimal protocol. Thus, the results of previous trials serve as a basis for subsequent trials.
An example of the prevailing meta-analytical impatience is Youssef et al.64 comparing GnRHa versus hCG for triggering of final oocyte maturation. The review concludes: ‘We recommend that GnRH agonists as a final oocyte maturation trigger in fresh autologous cycles should not be routinely used due to the associated significantly lower live birth rate, ongoing pregnancy rate (pregnancy beyond 12 weeks) and higher early miscarriage (less than 12 weeks)’. Furthermore, in the conclusion in ‘Implications for research’, it states: ‘In view of the poor reproductive outcomes following oocyte triggering with GnRH agonist we believe there is no indication for further research with GnRH agonists for oocyte triggering in ART in fresh autologous cycles’.
As clearly demonstrated in this chapter, GnRHa triggering induces a luteal phase insufficiency, against which the standard luteal phase support currently used in IVF is not enough. Corrective measures to secure the reproductive outcome are listed above, and are a direct product of fruitful research in the area, against the recommendation of the above mentioned review.
CONCLUSION
GnRHa trigger is the ultimate tool for complete OHSS prevention, while maintaining a more physiological trigger compared with the conventional hCG trigger. GnRH antagonist-based ovarian stimulation protocols should be considered in all OHSS high-risk patients, so GnRHa trigger can be used if needed. Luteal support must be patient tailored. In a broader perspective, GnRHa triggering is more patient friendly and offers several physiological advantages over hCG triggering in any patient, irrespective of OHSS risk.
REFERENCES
Smits G, Olatunbosun OA, Delbaere A, et al. Spontaneous ovarian hyperstimulation syndrome caused by a mutant follitropin receptor. N Engl J Med 349: 760, 2003. |
|
Baba T, Endo T, Kitajima Y, Kamiya H, Moriwaka O, Saito T. Spontaneous ovarian hyperstimulation syndrome and pituitary adenoma: incidental pregnancy triggers a catastrophic event. Fertil Steril 92:390, 2009. |
|
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 8085:366, 1978. |
|
Yen SSC, Lenera G, Little B, et al. Disappearance rate of endogenous luteinizing hormone and chorionic gonadotropin in man. J Clin Endocrinol Metab 28: 1763–7, 1968. |
|
Damewood MD, Shen W, Zacur HA, et al. Disappearance of exogenously administered human chorionic gonadotropin. Fertil Steril 52: 398-400, 1989. |
|
Abramov Y, Elchalal U, Schenker JG. Severe OHSS: An 'epidemic' of severe OHSS: a price we have to pay? Hum Reprod 14:2181, 1999. |
|
Smitz J, Camus M, Devroey P, et al. Incidence of severe ovarian hyperstimulation syndrome after GnRH agonists/HMG superovulation for in vitro fertilization. Hum Reprod 5:933–937, 1990. |
|
Brinsden PR, Wada I, Tan S, et al. Diagnosis, prevention and management of ovarian hyperstimulation syndrome. British Journal of Obstetrics and Gynaecology, 102: 767, 1995. |
|
Ragni G, Vegetti W, Riccaboni A, et al. Comparison of GnRH agonists and antagonists in assisted reproduction cycles of patients at high risk of ovarian hyperstimulation syndrome. Hum Reprod 20:2421, 1995. |
|
Papanikolaou EG, Pozzobon C, Kolibianakis EM, et al. Incidence and prediction of ovarian hyperstimulation syndrome in women undergoing gonadotropin-releasing hormone antagonist in vitro fertilization cycles. Fertil Steril 85:112, 2006. |
|
Devroey P, Boostanfar R, Koper NP, et al. A double-blind, non-inferiority RCT comparing corifollitropin alfa and recombinant FSH during the first seven days of ovarian stimulation using a GnRH antagonist protocol. Hum Reprod. 24:3063, 2009. |
|
Abramov Y, Elchalal U, Schenker JG. Severe OHSS: An 'epidemic' of severe OHSS: a price we have to pay? Hum Reprod 14:2181. 1999. |
|
Forman RG. Severe OHSS-an acceptable price? Hum Reprod 14:2687, 1999. |
|
Egbase PE. Severe OHSS: how many cases are preventable? Hum Reprod 15:8, 2000. |
|
Abdallah R, Kligman I, Davis O, Rosenwaks Z. Withholding gonadotropins until human chorionic gonadotropin administration. Semin Reprod Med. 28:486 , 2010 |
|
D'Angelo A, Amso N. "Coasting" (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome. Cochrane Database Syst Rev. 2002;(3):CD002811. |
|
Shoham Z, Weissman A, Barash A, et al. Intravenous albumin for the prevention of severe ovarian hyperstimulation syndrome in an in vitro fertilisation program: a prospective, randomised, placebo-controlled study. Fertil Steril 62, 137, 1994. |
|
Shalev E, Giladi Y, Matilsky M. and Ben-Ami M. Decreased incidence of severe ovarian hyperstimulation syndrome in high risk in-vitro fertilisation patients receiving intravenous albumin: a prospective study. Hum Reprod 10, 1373, 1995. |
|
Isik AZ, Gokmen O, Zeyneloglu HB, et al. Intravenous albumin prevents moderate-severe ovarian hyperstimulation in in-vitro fertilization patients: a prospective, randomized and controlled study. Eur J Obstet Gynecol Reprod Biol 70:179, 1996. |
|
Gokmen O, Ugur M, Ekin M, et al. Intravenous albumin versus hydroxyethyl starch for the prevention of ovarian hyperstimulation in an in-vitro fertilisation programme: a prospective randomised placebo controlled study. Eur. J. Obstet. Gynecol. Reprod. Biol. 96, 187, 2001. |
|
Ben-Chetrit, A. Eldar-Geva, T. Gal M.et al. The questionable use of albumin for the prevention of ovarian hyperstimulation syndrome in an IVF programme: a randomized placebo-controlled trial. Hum Reprod 16, 1880, 2001. |
|
Lewit N, Kol S, Ronen N, Itskovitz-Eldor J. Does intravenous administration of human albumin prevent severe ovarian hyperstimulation syndrome? Fertil Steril 66:654, 1996. |
|
Mukherjee T, Copperman AB, Sandler B, et al. Severe ovarian hyperstimulation despite prophylactic albumin at the time of oocyte retrieval for in vitro fertilization and embryo transfer. Fertil Steril 64:641, 1995 |
|
Aboulghar M, Evers JH, Al-Inany H. Intravenous albumin for preventing severe ovarian hyperstimulation syndrome: a Cochrane review. Hum Reprod 17:3027, 2002 |
|
Venetis CA, Kolibianakis EM, Toulis KA, et al. Intravenous albumin administration for the prevention of severe ovarian hyperstimulation syndrome: a systematic review and metaanalysis. Fertil Steril 95:188, 2011 |
|
Jee BC, Suh CS, Kim YB. Administration of intravenous albumin around the time of oocyte retrieval reduces pregnancy rate without preventing ovarian hyperstimulation syndrome: a systematic review and meta-analysis. Gynecol Obstet Invest. 70:47, 2010 |
|
D'Angelo A, Amso N. Embryo freezing for preventing ovarian hyperstimulation syndrome. Cochrane Database Syst Rev. 18:CD002806, 2007. |
|
Tang T, Balen AH. A woman with polycystic ovary syndrome treated for infertility by in vitro fertilization. Nat Rev Endocrinol. 5:462, 2009 |
|
Gomez R, Gonzalez-Izquierdo M, Zimmermann RC, et al. Low-dose dopamine agonist administration blocks vascular endothelial growth factor (VEGF)-mediated vascular hyperpermeability without altering VEGF receptor 2-dependent luteal angiogenesis in a rat ovarian hyperstimulation model. Endocrinology 147:5400-5411, 2006 |
|
Alvarez C, Martí-Bonmatí L, Novella-Maestre E, et al. Dopamine agonist cabergoline reduces hemoconcentration and ascites in hyperstimulated women undergoing assisted reproduction. J Clin Endocrinol Metab 92:2931-2937, 2007 |
|
Busso C, Fernández-Sánchez M, García-Velasco JA, et al. The non-ergot derived dopamine agonist quinagolide in prevention of early ovarian hyperstimulation syndrome in IVF patients: a randomized, double-blind, placebo-controlled trial. Hum Reprod 25:995-1004, 2010 |
|
Youssef MA, van Wely M, Hassan MA, et al. Can dopamine agonists reduce the incidence and severity of OHSS in IVF/ICSI treatment cycles? A systematic review and meta-analysis. Hum Reprod Update. 16:459-66, 2010. 20354100 |
|
Schmidt DW, Maier DB, Nulsen JC, Benadiva CA. Reducing the dose of human chorionic gonadotropin in high responders does not affect the outcomes of in vitro fertilization. Fertil Steril 82:841-6, 2004. |
|
Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Ross R, Morris S. Effects of the ovulatory serum concentration of human chorionic gonadotropin on the incidence of ovarian hyperstimulation syndrome and success rates for in vitro fertilization. Fertil Steril 84:93-8, 2005 16009163 |
|
European Recombinant LH Study Group. Human recombinant luteinizing hormone is as effective as, but safer than, urinary human chorionic gonadotropin in inducing final follicular maturation and ovulation in in vitro fertilization procedures: results of a multicenter double-blind study. The Journal of clinical endocrinology and metabolism 86:2607-18, 2001. |
|
Itskovitz J, Boldes R, Barlev A, Erlik Y, Kahana L, Brandes JM. The induction of LH surge and oocyte maturation by GnRH analogue (Buserelin) in women undergoing ovarian stimulation for in vitro fertilization. Gynecol Endocrinol 2 (supplement 1), 165, 1988. |
|
Segal S, Casper RF. Gonadotropin-releasing hormone agonist versus human chorionic gonadotropin for triggering follicular maturation in in vitro fertilization. Fertil Steril 57:1254–1258, 1992. |
|
Lewit N, Kol S, Manor D, Itskovitz-Eldor J. Comparison of gonodotrophin-releasing hormones analogs and human chorionie gonadotrophin for the induction of ovulation and prevention of ovarian hyperstimulation syndrome: a casecontrol study. Hum Reprod 11:1399–1402, 1996. |
|
Itskovitz J, Boldes R, Levron J, Erlik Y, Kahana L, Brandes JM. Induction of preovulatory luteinizing hormone surge and prevention of ovarian hyperstimulation syndrome by gonadotropin-releasing hormone agonist. Fertil Steril 56:213–220, 1991. |
|
Mais V, Kazer RR, Cetel NS, Rivier J, Vale W, Yen SS. The dependency of folliculogenesis and corpus luteum function on pulsatile gonadotropin secretion in cycling women using a gonadotropin-releasing hormone antagonist as a probe. J Clin Endocrinol Metab 62:1250–1255, 1986. |
|
Lockwood GM, Ledger WL, Barlow DH, Groome NP, Muttkrishna S. Identication of the source of inhibins at the time of conception provides a diagnostic role for them in very early pregnancy. Am J Reprod Immunol 40:303–8, 1998 |
|
Yamoto M, Minami S, Nakano R. Immunohistochemical localization of inhibin subunits in human corpora lutea during menstrual cycle and pregnancy. J Clin Endocrinol Metab 73:470–7, 1991. |
|
Treetampinich C, O’Connor AE, MacLachlan V, Groome NP, Kretser DM. Maternal serum inhibin A concentrations in early pregnancy after IVF and embryo transfer reect the corpus luteum contribution and pregnancy outcome. Hum Reprod 15:2028–32, 2000. |
|
Nevo O, Eldar-Geva T, Kol S, Itskovitz-Eldor J. Lower levels of inhibin A and Pro-alphaC during the luteal phase after triggering oocyte maturation with a gonadotropin-releasing hormone agonist versus human chorionic gonadotropin. Fertil Steril 79:1123-8, 2003. |
|
Kol S. Luteolysis induced by a gonadotropin-releasing hormone agonist is the key to prevention of ovarian hyperstimulation syndrome. Fertil Steril 81:1-5. 2004. |
|
Schenker JG, Weinstein D. Ovarian hyperstimulation syndrome: a current survey. Fertil Steril 30: 255–26, 1978. |
|
van der Meer S, Gerris J, Joostens M, Tas B. Triggering of ovulation using a gonadotrophin-releasing hormone agonist does not prevent ovarian hyperstimulation syndrome. Hum Reprod 8:1628–1631, 1993. |
|
Gerris J, De Vits A, Joostens M, Van Royen E. Triggering of ovulation in human menopausal gonadotropin-stimulated cycles: comparison between intravenous administered gonadotrophin-releasing hormone (100 and 500 micrograms), GnRH agonist (buserelin, 500 micrograms) and human chorionic gonadotrophin (10,000 IU). Hum Reprod 10:56–62, 1995. |
|
Shoham Z, Schacter M, Loumaye E, Weissman A, MacNamee M, Insler V. The luteinizing hormone surge— the nal stage in ovulation induction: modern aspects of ovulation triggering. Fertil Steril 64:237–251, 1995. |
|
Imoedemhe D, Chan R, Pacpaco E, et al. Preventing OHSS in at-risk patients: evidence from a long-term prospective study. Hum Reprod 14:102–103, 1999 [abstract from the European Society of Human Reproduction and Embryology [ESHRE] Conference, 1999] |
|
Kovachev E. Protocol with GnRH-antagonist and ovulation trigger with GnRH-agonist in risk patients--a reliable method of prophylactic of OHSS. Akush Ginekol (Sofiia). 4716-9. 2008. |
|
Dong H, Chen S, Xing F. Application of gonadotropin-releasing hormone agonist for triggering ovulation in high risk gonadotropin stimulating cycles of infertile polycystic ovary syndrome patients. Zhonghua Fu Chan Ke Za Zhi. 34:94-6, 1999. |
|
Babayof R, Margalioth EJ, HuleihelM, et al. Seruminhibin A, VEGF and TNFalpha levels after triggering oocyte maturation with GnRH agonist compared with HCG in women with polycystic ovaries undergoing IVF treatment: a prospective randomized trial. Hum Reprod 21:1260–1265, 2006. |
|
Engmann L, DiLuigi A, Schmidt D, Nulsen J, Maier D, Benadiva C. The use of gonadotropin-releasing hormone (GnRH) agonist to induce oocyte maturation after cotreatment with GnRH antagonist in high-risk patients undergoing in vitro fertilization prevents the risk of ovarian hyperstimulation syndrome: a prospective randomized controlled study. Fertil Steril 89:84–91, 2008. |
|
Acevedo B, Gomez-Palomares JL, Ricciarelli E, Hernandez ER. Triggering ovulation with gonadotropin-releasing hormone agonists does not compromise embryo implantation rates. Fertil Steril 86:1682–1687, 2006. |
|
Griesinger G, Diedrich K, Devroey P, Kolibianakis EM. GnRH agonist for triggering final oocyte maturation in the GnRH antagonist ovarian hyperstimulation protocol: a systematic review and meta-analysis. Hum Reprod Update 12: 159-168, 2006. |
|
Griesinger G, Kolibianakis EM, Papanikolaou EG, Diedrich K, Van Steirteghem A, Devroey P, Ejdrup Bredkjaer H, Humaidan P. Triggering of final oocyte maturation with gonadotropin-releasing hormone agonist or human chorionic gonadotropin. Live birth after frozen-thawed embryo replacement cycles. Fertil Steril 88: 616-621, 2007. |
|
Humaidan P, Bredkjaer HE, Bungum L, Bungum M, Grondahl ML, Westergaard L, Andersen CY. GnRH agonist (buserelin) or hCG for ovulation induction in GnRH antagonist IVF/ICSI cycles: a prospective randomized study. Hum Reprod 20:1213-1220, 2005. |
|
Kolibianakis EM, Schultze-Mosgau A, Schroer A, van Steirteghem A, Devroey P, Diedrich K, Griesinger G. A lower ongoing pregnancy rate can be expected when GnRH agonist is used for triggering final oocyte maturation instead of HCG in patients undergoing IVF with GnRH antagonists. Hum Reprod 20: 2887-2892, 2005. |
|
Humaidan P, Bungum L, Bungum M, Yding Andersen C. Rescue of corpus luteum function with peri-ovulatory HCG supplementation in IVF/ICSI GnRH antagonist cycles in which ovulation was triggered with a GnRH agonist: a pilot study. Reprod Biomed Online 13:173-178, 2006. |
|
Humaidan P. Luteal phase rescue in high-risk OHSS patients by GnRHa triggering in combination with low-dose HCG: a pilot study. Reprod Biomed Online 18: 630-634, 2009. |
|
Humaidan P, Ejdrup Bredkjaer H, Westergaard LG, Yding Andersen C. 1,500 IU human chorionic gonadotropin administered at oocyte retrieval rescues the luteal phase when gonadotropin-releasing hormone agonist is used for ovulation induction: a prospective, randomized, controlled study. Fertil Steril 93:847-854, 2010. |
|
Papanikolaou EG, Verpoest W, Fatemi H, Tarlatzis B, Devroey P, Tournaye H. A novel method of luteal supplementation with recombinant LH, when a GnRH-Agonist is used instead of HCG for ovulation triggering. A randomized prospective proof of concept study. Fertil Steril 2010. |
|
Youssef MAFM, Van der Veen F, Al-Inany HG, Griesinger G, Mochtar MH, van Wely M. Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist assisted reproductive technology cycles. Cochrane Database Syst Rev 2010, Issue 11. Art. No.: CD008046 |