Leiomyomas of the Uterus
Authors
INTRODUCTION
Leiomyomas of the uterus are one of the most common pathologic abnormalities of the female genital tract. Their occurrence increases with age, and they are found in 20–50% of women older than 30 years. Although found elsewhere in the body, leiomyomas most frequently occur in the myometrium. Uterine leiomyomas are commonly referred to as myomas, fibromyomas, or “fibroids” because of their firm, fibrous character and high content of collagen.
Leiomyomas of the uterus are the most common indication for hysterectomy in the United States. Approximately 175,000 hysterectomies are performed annually for leiomyomas. Uterine leiomyomas result in masses associated with a variety of gynecologic problems, the most prominent of which are the asymptomatic pelvic mass or abnormal vaginal bleeding.
The last two decades have seen rapid advancements in the diagnosis and treatment of uterine leiomyomas. The introduction of pelvic ultrasonography sonohysterography, hysteroscopy, and magnetic resonance imaging (MRI) have made it possible to detect small myomas not clinically suspected as a cause of abnormal bleeding. It is also possible to make a definitive diagnosis of a pelvic mass as a uterine myoma short of performing laparotomy or laparoscopy. Understanding the relation of sex steroid hormones and uterine leiomyomas has provided the foundation for using gonadatropin-releasing agonists (GnRH), which have facilitated treatment of leiomyomas by hysteroscopy, laparoscopy, and the liberal use of vaginal hysterectomy. With the introduction of the antiprogesterone RU486 and other drugs that can be used in lieu of surgery, the 21st century will be marked by dramatically new treatments of leiomyomas of the uterus.
DEFINITION AND DESCRIPTION
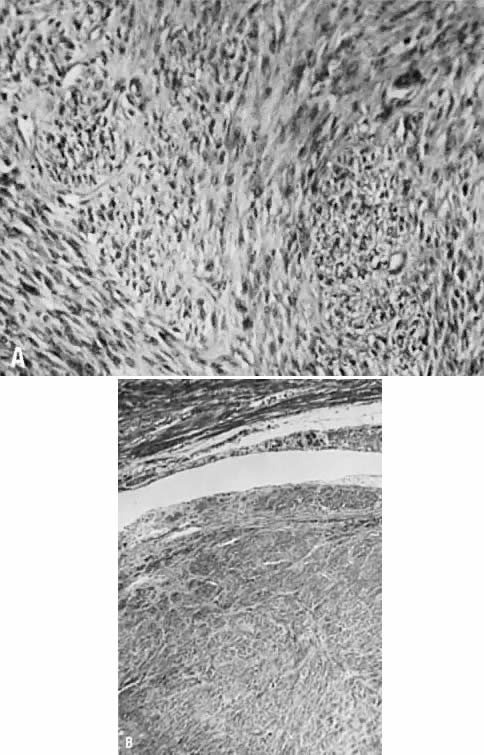
Uterine leiomyomas are usually spherical masses of tissue that can vary from a few millimeters to many centimeters in diameter. They may grow large enough to obstruct the ureters, compress the great vessels, or compromise of pulmonary ventilation. On dissection, myomas appear to have a capsule. The cells on the edge of the tumor seem to become flattened in the concentric pattern, leading to the clinical impression of a capsule, although there is no distinct fibrous tissue capsule microscopically (Fig. 1). Nevertheless, the pseudocapsule layer is the preferential plane of dissection to peel out the main mass of the myoma from the surrounding, more normal myometrium. The blood supply enters at the periphery of the tumor and the core is relatively avascular, which is the probable reason for the various forms of degeneration and necrosis that are seen in the center of some myomas.
{kind=link}
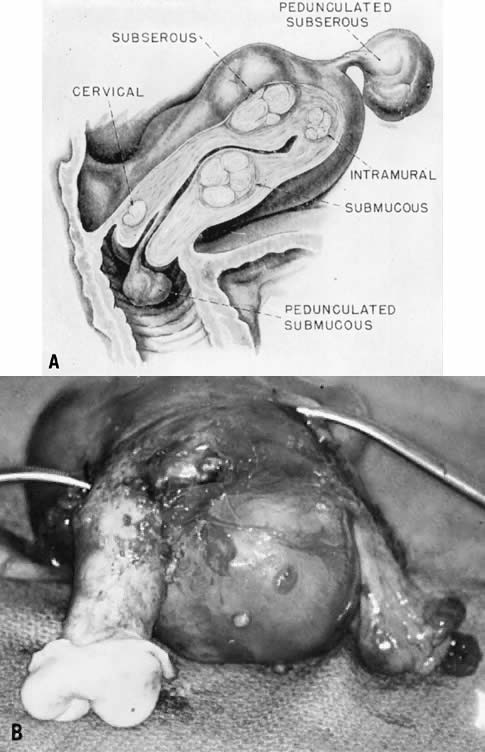
The location of leiomyomas is variable. Most commonly, they are intramural and are identified by an irregular enlargement of the uterine corpus (Fig. 2). The tumors may enlarge from the surface of the uterus late or early in their course and become subserous. Alternatively, they can protrude into and distort the endometrial cavity.
{kind=link}
The submucous fibroid penetrates the endometrial cavity and enlarges to stretch the mucosa over the tumor to the point that the submucosa is absent and ulceration of the overlying mucosal layer may occur. Blood vessels can often be seen coursing on the surface at hysteroscopy. Although not all submucous fibroids cause clinical bleeding or interfere with conception and normal pregnancy, they are statistically associated with significant symptomatic disturbances of this type, producing menorrhagia, anemia, pelvic cramping, infection, infertility, and abortion. Less frequently, a myoma may grow from a subserous location into the peritoneal folds of the broad ligaments, forming an intraligamentous fibroid. These masses and the pedunculated subserous variety can appear clinically to be adnexal in location and be confused clinically with an ovarian tumor. Modern diagnostic techniques can usually distinguish such masses from ovarian masses. Another important clinical significance of the intraligamentous myoma is that it lies near the ureter and may have variant blood supply from the uterine artery and veins. Surgical removal during myomectomy or hysterectomy must be done with ureter and blood supply in mind.
The leiomyoma typically enlarges with time until menopause. The pace of enlargement is variable and unpredictable. A variety of degenerative changes can be seen. Clinical degeneration is most commonly seen during pregnancy and causes pain. Pathologic degeneration can be seen at the time of hysterectomy or myomectomy and is most typically hyaline degeneration. Calcium deposition or myxomatous jelly material may sometimes characterize the degeneration. Malignant degeneration is uncommon, occurring in about 1 of 200 cases. There is some question about whether the sarcomas seen in fibroids carry the same risk of dissemination as those arising de novo in the myometrium. VanDinh and Woodruff1 suggested that sarcomas in fibroids are less likely to produce metastases and death. The report that 50% of uterine sarcomas arise in normal uteri suggests that myomas are not precursor lesions, because some 40% of women have fibroids.
ETIOLOGY
The cause of uterine leiomyomas remain unknown. A leiomyoma arises from a single neoplastic cell within the smooth muscle of the myometrium. Multiple myomas in the same uterus develop de novo rather than through a metastatic mechanism. The factors responsible for the initial neoplastic transformation of the myometrium to leiomyoma have yet to be elucidated. Neoplastic transformation probably involves somatic mutations of normal myometrial cells and the complex interaction of sex steroids and local growth factors.
Somatic mutations such as translocations, duplications, and deletions have been identified in almost one half of the leiomyoma studied by cytogenic analysis.2 The most frequent cytogenic changes involve chromosome bands 12q14–15 and 7q22. The somatic mutations may be the basis for the differential responsiveness of individual myomas to a variety of growth promoting agents.
The sex steroids, estrogen and progesterone, are believed to be important in leiomyoma enlargement. The tendency of uterine leiomyoma to grow during the reproductive years and regress postmenopausally strongly suggests that sex steroid hormones are implicated in the pathophysiology of the disease.3 Assay for estrogen and estrogen receptors in myomas show the concentration to be about ten times the concentration in normal myometrium.
It is believed that sex steroids promote development of leiomyomas by stimulating inappropriate expression of growth factors. Estrogen and progesterone act as physiologic regulators of gene expression by activating nuclear receptors that are themselves transcription factors. In this way estrogen and progesterone play a key role in regulating genes that direct cell growth. Some studies have shown that both steroids are important in leiomyoma growth, but it is progesterone that influences the proliferation of leiomyoma more than estrogen. Clinical evidence of the importance of sex steroids in leiomyoma growth can be seen with the shrinkage of leiomyoma during menopause and after GnRH administration in hypoestrogenic and hypoprogesterone states.
Growth factors such as insulin-like growth factor (IGF), epidermal growth factor (EGF), and platelet-derived growth factors (PDGF) are known mitogens. Only elevated expression of EGF has been associated with increased mitotic activity in leiomyomas. The expression of these growth factors is higher in uterine leiomyomas than normal myometrium. The levels of few of these growth factors or their receptors are elevated during the progesterone-dominated luteal phase of the menstrual cycle, when mitotic activities of leiomyomas can be elevated. Progesterone-regulated EGF is the only characterized growth factor with elevated expression during the luteal phase, when leiomyoma mitotic activity is elevated. Leiomyomas have been shown to contain EGF receptors that are responsive to their own production of EGF. It is therefore reasonable to conclude that EGF may contribute to the increased mitotic activity of leiomyomas observed during the luteal phase. It may act in synergism with other hormones, such as insulin or PDGF.4
RISK FACTORS
Known risk factors for leiomyomas are black race, positive family history, nulliparity, and obesity. Uterine leiomyomas are thought to have an incidence in black women threefold that of white women. Black women also have a two to three times greater risks of undergoing a hysterectomy for fibroids than white women. Vikhlyaeva and colleagues reported a familial predisposition for uterine leiomyomas. They showed that the fibroids were 2.2 times more frequent in first-degree relatives within families in which there were two or more family members with fibroids.5
There is an association between nulliparity and the incidence of fibroids. The relative risk of fibroids decreases with an increasing number of term pregnancies. A woman with five term pregnancies has a 25% reduction in a risk for leiomyoma compared with a nulliparous woman.6
Women weighing 70 kg or more have an almost threefold risk of developing fibroids compared with women weighing less than 50 kg. Obesity increases the risk of developing fibroids by 21% for each 10-kg weight gain.
Smoking, oral contraception use, and the use of depot medroxyprogesterone acetate, a progesterone derivative, have all been associated with protecting against the growth of leiomyoma.
SIGNS AND SYMPTOMS
Although uterine myomas are common, most are asymptomatic and require no treatment. Predominantly intramural or subserous, they are typically found in the highly screened U.S. population as unsuspected pelvic masses at the time of an annual examination and Pap smear.
The patients are usually between 30 and 50 years old. In the past, indications for intervention for asymptomatic uterine leiomyomas included uterine size, inaccessible ovaries, facilitation of estrogen replacement, and a rapid change in uterine size. A review of the literature does not support surgical intervention for uterine leiomyomas based on size alone. According to Mayer and Shipilov, normal ovaries that are not identified by ultrasonography can be differentiated from uterine leiomyomas on MRI, allowing exclusion of ovarian tumors.7 The addition of hormone replacement therapy in standard doses does not appear to provide sufficient amounts of estrogen or progesterone to cause uterine growth. Even the age-old accepted theory of a “rapidly enlarging uterus” has been challenged as an indication for intervention for the asymptomatic leiomyoma. Parker and coworkers reviewed the medical records of 1332 women admitted between 1988 and 1992 for surgical management of uterine leiomyomas. They found no correlation between rapid uterine growth and uterine sarcoma.8
Common symptoms associated with leiomyomas are menorrhagia, pelvic pressure or pain, and reproductive symptoms. The most common symptom associated with leiomyomas is menorrhagia. The cause of leiomyoma-associated menorrhagia is unknown. Ulceration of a submucous myoma and compression of venous plexus or adjacent myometrium and endometrium by intramural myoma have been postulated.9 Rarely, fibroids may present as a result of pressure on neighboring organs, such as urinary frequency or urinary obstruction secondary to urethral obstruction. Rectal symptoms also are rare, but blockage or irritation of the rectum and rectal sigmoid can occur. Acute pain associated with a low-grade fever and uterine tenderness may be observed with degeneration of leiomyomas or with torsion or a pedunculated subserous myoma.
The major clinical issues involved with leiomyomas of the uterus include the differential diagnosis, management of the asymptomatic pelvic mass, and appraisal of the role of the fibroid in various clinical problems such as abnormal bleeding, pain, infertility, and pregnancy. A review of current approaches to the differential diagnosis and treatment options for leiomyomas is appropriate.
DIFFERENTIAL DIAGNOSIS
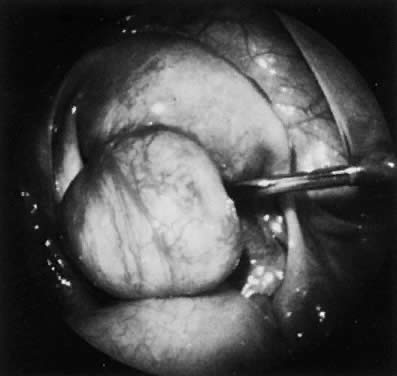
The typical problems presented by uterine leiomyomas have traditionally been evaluated by pelvic and abdominal examinations. Cantuaria and coworkers reported a strong correlation between bimanual examination and ultrasound examination with regard to determining the size of uterine myomas.10 The addition of ultrasonography (Fig. 3) and especially of magnetic resonance imaging (MRI) (Fig. 4) has increased the accuracy in the diagnosis and measurement of uterine leiomyomas. MRI often can differentiate adenomyosis from the leiomyoma. Radiologic studies are particularly important when the physical assessment is difficult, as in the case of morbid obesity, or when adnexal pathology cannot be excluded on physical examination. If there is any uncertainty about the diagnosis of uterine leiomyomas after radiologic studies, laparoscopy (Fig. 5), or laparotomy should be performed.
{kind=link}
{kind=link}
{kind=link}
The presence of associated abnormal bleeding from a myomatous uterus should always be evaluated. Anovulatory bleeding, endometrial hyperplasia, or malignancy can be diagnosed by endometrial biopsy, basal body temperatures, timed plasma progesterone levels, or hysteroscopy and curettage. More commonly, bleeding is caused by distortion of the endometrial cavity or myometrium by the myomas.
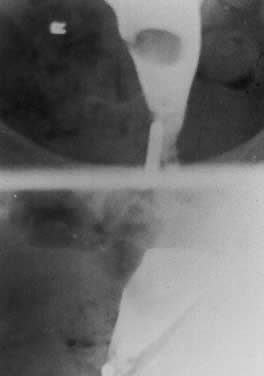
Appraisal of the endometrial cavity is best done by sonohysterography, hysterosalpingography (Fig. 6), or hysteroscopy. In patients who are bleeding heavily, the hemoglobin level should be followed, because it is easy for patients with bleeding uterine myomas to develop iron-deficiency anemia. It is also advisable to check the stool guaiac in the patient who is anemic and reports abnormal vaginal bleeding to exclude occult gastrointestinal bleeding. The combination of abnormal vaginal bleeding and uterine fibroids is so common that the examiner occasionally misses the diagnosis of occult gastrointestinal bleeding by focusing on the patient's history and not excluding other serious causes of anemia in the middle-aged woman.
{kind=link}
The overwhelming problem in the differential diagnosis of uterine fibroids is that they are so common the physician must constantly beware of the presumptive diagnosis to detect other contemporary conditions. Newer techniques have made this concern less worrisome. The gynecologist must remain wary of the obvious and explore alternative possibilities when the clinical history and physical findings are not conclusive.
COMPLICATIONS
Clinical problems associated with leiomyomas are related to pregnancy, infertility, abnormal bleeding, large masses, pain, and sarcomatous changes. Pregnancy is the most complex area in which fibroids have an impact, caused by the fact that fibroids can affect the pregnancy, and pregnancy can affect the fibroids.11 Leiomyomas in pregnancy are a relatively common occurrence, with a prevalence of 1.4–2%. Traditionally, fibroids have been thought to increase in size during pregnancy, but studies by Lev-Touff and associates showed that about 60% of myomas do not change in size during pregnancy, and in 8–19% of cases, they decrease in size. Strobelt and colleagues12 observed that myomas smaller than 5 cm in diameter could no longer be detected sonographically during pregnancy and that most myomas larger than 5 cm in diameter tended to remain stable. Most fibroids remain uncomplicated during pregnancy. Degeneration has been estimated to occur in 10% of fibroids in pregnancy, and it is characterized by abdominal pain, leukocytosis, and mild temperature elevation. Degenerating fibroids in pregnancy are usually self-limited and are best treated with bed rest and analgesia.
The fibroid-related pregnancy complications are spontaneous abortion, preterm labor, preterm rupture of membranes, placental abruption, fetal growth restriction, and postpartum hemorrhage. The most hazardous complication is an incomplete abortion in a fibroid uterus, which then becomes an infected abortion. If the uterine cavity is markedly enlarged or distorted, it can be challenging and even dangerous to curette the uterus. Hemorrhage caused by partially separated but inaccessible placental tissue is a major problem. Placentitis and the failure of the uterus to contract firmly are potential problems.
When myomatous uteri during pregnancy were compared with matched controls, there was an increased rate of preterm labor and preterm delivery for the patients with myomatous uteri. The average weights of the newborns in the two groups were not statistically different.13 Rice and coworkers reported that premature labor was not significantly increased for patients with myomas smaller than 3 cm, but a myoma greater than 5 cm in diameter was associated with a 28% increased incidence of preterm labor.14
Cesarean section is more common in women with fibroids. This may be caused by obstructed labor or physician anxiety. A factor that predicts the need for cesarean section is a lower uterine segment myoma larger than 5 cm.15 The risk of cesarean hysterectomy in women with fibroids is significantly increased because of excessive hemorrhage.
The association between infertility and uterine leiomyomas remains controversial. Uterine myomas, especially the submucous type, are associated with an increased risk of spontaneous abortion and recurrent abortions. Uterine fibroids occur in apparently normal fertile and infertile women, however; approximately 43% of pregnant women with fibroids have a history of infertility before pregnancy. Impaired gamete transport, distortion of the endometrial cavity, impairment of blood supply to the endometrium, and atrophy and ulceration may be responsible for reduced implantation in patients with these tumors.
Farhi and colleagues16 concluded that implantation rates and pregnancy outcomes are impaired in women with uterine leiomyomas only when they cause deformities of the uterine cavity. In examining the implantation rates of women undergoing assisted reproduction, Eldar-Geva found that implantation rates were lower for women with intramural and submucous fibroids, even if no deformity of the uterine cavity existed.17 The investigators speculate that the presence of intramural or submucous fibroids can cause endometrial changes or changes in vascularization through secretion of growth or angiogenic factors, through impairment of normal secretion of these factors, through changes in the surrounding myometrial contractility, or through mechanical pressure. The presence of subserosal myomas had no affect on implantation rates.
TREATMENT
The problems associated with bleeding myomas are related primarily to anemia, but the myomas can also create difficulties in maintaining an acceptable lifestyle because of the problems of pelvic discomfort. The submucous myoma particularly can be the cause of major hemorrhage and produce emergency situations. Intramural fibroids and a distorted endometrial cavity can produce a similar picture and force intervention.
The clinical problems produced by the mass of the myomatous uterus usually are not observed until the mass rises out of the pelvis. In nonpregnant states, the mass may cause ureteral obstruction, bladder and rectal pressure, pelvic pain, and if the mass extends to the umbilicus or above, diaphragmatic pressure. Rarely, when the pedunculated subserous myomas twist and causes acute or chronic symptoms or marked abdominal protuberance, surgical intervention is warranted.
Benign degeneration of the myoma is usually caused by avascular necrosis. It is principally seen during pregnancy, when it should be treated symptomatically. Malignant degeneration results in sarcoma, which occurs in 0% to 5% of cases. Sarcomas arising de novo in normal uteri usually tend to be more aggressive. Changes in size, especially those associated with vaginal bleeding a postmenopausal woman, are signs of possible malignant degeneration.
Major advances in the treatment of symptomatic fibroids have created treatment options. The principal treatments for uterine myomas are control of the symptoms after a benign diagnosis is established. The options for treatment of symptomatic fibroids are medical management and surgery.
Medical Management
The management of symptomatic uterine myomas has traditionally involved surgery. However, the introduction of GnRH agonists in the 1980s offered temporary relief to women with myomas who do not desire surgery and are approaching menopause.18
The use of a GnRH agonist produces a hypoestrogenic state, which leads to a median reduction in uterine volume of approximately 50%. The maximal effect is seen after 12 weeks of therapy, with no further reduction in uterine size observed between 12 and 24 weeks of therapy. Unfortunately, rapid regrowth of myomas after therapy and side effects related to the hypoestrogenic state such as bone loss and hot flashes have limited the usefulness of the GnRH agonists.
To overcome the side effects of long-term GnRH therapy and maintain decrease in uterine size, Friedman and coworkers proposed an “add-back” regimen of estrogen and progesterone in small doses.19 Early reports with add-back therapy appear promising, but the high cost ($300.00/month) associated with GnRH agonist with estrogen and progesterone have limited this approach. The ultimate place for GnRH agonist therapy may be as a presurgical treatment before myomectomy or hysterectomy.
The GnRH agonist can cause a cessation of menses, allowing severe anemia to be corrected before surgery and avoiding preoperative blood transfusions. It also been shown to reduce operative blood lose. Preoperative GnRH also opens the possibility for converting some cases of abdominal hysterectomy into a vaginal hysterectomy through reduction in uterine mass.
Surgical Management
The key factors governing the surgical options are the patient's age, fertility status, and reliability; the impact of fibroids on surrounding organs; and attendant medical, surgical, or anesthetic risks that may complicate surgical treatment. If fertility is a consideration and the patient has major symptoms, myomectomy is the procedure of choice. Myomectomy should be preceded by a hysterosalpingogram to determine the location and patency of the fallopian tubes and to screen for submucous myomas. Extensive and aggressive myomectomy runs the risk of resulting in emergency hysterectomy. The use of uterine tourniquets and vasopressin has reduced the amount of blood loss during myomectomy. Dillon reported that, with the use of vasopressin, 72% of patients undergoing myomectomy did not need blood products.20 Other complications associated with abdominal myomectomy are pelvic adhesion and bowel obstruction. In comparing the overall morbidity associated with myomectomy with that of hysterectomy, Iverson found no difference.21
A patient undergoing myomectomy should understand that the procedure is a treatment for fibroids, not a cure. There is a 15% recurrence rate of myomas after myomectomy and a 10% reoperation rate.
Dubuisson first reported myomectomy under laparoscopic control.22 Technical innovations such as electric morsulators (Karl Stortz) and simplified suturing techniques have made this procedure more feasible. Laparoscopic myomectomy can be offered as an alternative to abdominal myomectomy in selected cases (i.e. with a single myoma smaller than 6 cm) and should only be attempted by experienced laparoscopic surgeons. It has been suggested that adequate closure of the myometrium after laparoscopic myomectomy is difficult and may account for uterine rupture during pregnancy after undergoing a laparoscopic myomectomy.
The hysteroscope has been employed to establish the diagnosis of submucous fibroids and, in selected cases, has been used successfully to perform total (Fig. 7) or subtotal (Fig. 8) submucous myomectomy (Fig. 9). Younger women with infertility, recurrent abortion, or menorrhagia have had successful pregnancies after this procedure and avoided a cesarean section.23
{kind=link}
{kind=link}
{kind=link}
Two other modalities are available for the treatment of symptomatic fibroids: myolysis and uterine artery embolization. Myolysis was described by Goldfarb in the United States, and it is performed by penetrating the fibroid (3–10 cm) at multiple sites at a 90-degree angle with the neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser or bipolar needles.24 In response to the treatment, the myoma undergoes thermal necrosis and frequently atrophies. The complication rate is not established.
Transcatheter arterial embolization has been used for postpartum hemorrhage since 1979. Ravin in Paris reported that bilateral uterine artery embolization could be used to effect a 39–70% decrease in uterine size and an 85% decrease in patient symptoms.25 Although results of uterine artery embolization for fibroids have been encouraging, serious complications have occurred, complication rates are unknown, and long-term follow-up is needed.
If fertility is not a factor, hysterectomy remains the traditional therapy. However, for those patients whose major problem is bleeding and who wish or need to avoid hysterectomy, hysteroscopic endometrial ablation of the endometrial cavity has been tried with success in a growing number of patients. Long-range follow-up has shown these methods to be effective for up to 8 years, because more than 80% of patients so treated have not required further surgery in the interval.26 New techniques of nonhysteroscopic endometrial ablation are becoming available. If the uterine cavity is of normal shape and not larger than 10 cm, Thermachoice, a thermal balloon ablation technique can be employed with equal effectiveness to that of hysteroscopic ablation, even if intramural or subserosal myomas are present.
REFERENCES
Van Dinh T, Woodruff JD: Leiomyosarcoma of the uterus. Am J Obstet Gynecol 55: 20, 1980 |
|
Pandis N, Heim S, Bandi G: Chromosome analysis of 96 uterine leiomyoma. Cancer Genet Cytogenet 55: 11, 1991 |
|
Sener AB, Seckin NC: The effect of hormone replacement on uterine fibroids in postmenopausal women. Fertil Steril 65: 354, 1996 |
|
Yeh J, Rein M, Nowak R: Presence of messenger ribonucleic acid for epidermal growth factor (EGF) and EGF receptor demonstrable in monolayer cell cultures of myometria and leiomyomata. Fertil Steril 56: 997, 1991 |
|
Vikhlyaeva EM, Khodzhaeva ZS: Familial predisposition to uterine leiomyomas. Int J Gynecol Obstet 51: 127, 1995 |
|
Parazzini F, Negri E: Reproductive factors and risk of uterine fibroids. Epidemiology 7: 440, 1996 |
|
Mayer D, Shipilov MS et al: Ultrasonography and magnetic resonance imagining (MRI) of uterine fibroids. Obstet Gynecol Clin North Am 22: 4, 1995 |
|
Parker WH, Fu YS, Berek JS: Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol 83: 413, 1994 |
|
Farrer-Brown G, Bobbeilby JW: Venous changes in the endometrium of myomatous uteri. Obstet Gynecol 38: 743, 1971 |
|
Cantuaria G, Angioli R et al: Comparison of bimanual examination with ultrasound examination before hysterectomy for uterine leiomyoma. Obstet Gynecol 92: 109, 1998 |
|
Katz VL, Dotters DJ, Droegemuller W: Complication of uterine leiomyoma in pregnancy. Obstet Gynecol 73: 593, 1989 |
|
Lev-Toaff AS, Coleman BG, Arger PH: Leiomyoma in pregnancy: sonographic study. Radiology 164: 375, 1987 |
|
Strobelt N, Ghidini A, Cavallone W: Natural history of uterine leiomyoma in pregnancy. J Ultrasound Med 13: 399, 1994 |
|
Rice JP, Kay H, Mahoney BS: The clinical significance of uterine leiomyomas in pregnancy. Am J Obstet Gynecol 160: 1212, 1989 |
|
Strobelt N, Ghidini A, Cavallone W: Natural history of uterine leiomyoma in pregnancy. J Ultrasound Med 13: 399, 1994 |
|
Farhi J, Ashkenazi J, Feldberg D et al: Effect of uterine leiomyomata on the results of in vitro fertilization treatment. Hum Reprod 10: 2576, 1995 |
|
Eldar-Geva T, Meagher S, Healy DL et al: Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril 70: 687, 1998 |
|
Filicori M, Hall DA, Loughlin JS et al: A conservative approach to the management of uterine leiomyoma: pituitary desensitization by luteinizing hormone-releasing hormone analog. Am J Obstet Gynecol 147: 726, 1983 |
|
Freidman AJ. Treatment of leiomyomata uteri with short-term leuprolide plus estrogen-progestin hormone replacement therapy for 2 years: a pilot study. Fertil Steril 51: 526, 1989 |
|
Dillon T: Control of blood loss during gynecologic surgery. Obstet Gynecol 19: 428, 1962 |
|
Iverson R, Chelmow D: Relative morbidity of abdominal hysterectomy and myomectomy for management of uterine leiomyomas. Obstet Gynecol 88: 415, 1996 |
|
Dubuisson JB, Lecuru F, Foulot H et al: Myomectomy by laparoscopy: preliminary report of 43 cases. Fertil Steril 56: 828, 1991 |
|
Neuwirth RS: Hysteroscopic management of symptomatic submucous fibroids. Obstet Gynecol 62: 509, 1993 |
|
Goldfarb HA: Nd:YAG laser laparoscopic coagulation of symptomatic myomas. J Reprod Med 37: 636, 1992 |
|
Ravina JH, Herbreteau D, Ciraru-Vigneron N et al: Arterial embolization to treat uterine myomata. Lancet 346: 671, 1995 |
|
Derman S, Rehnstrom J, Neuwirth RS: The long-term effectiveness of hysteroscopic treatment of menorrhagia and leiomyomas Obstet Gynecol 77:591, 1991 |