Chapter 7
Patient Positioning
(see Video 4: Patient positioning)
Video 4 Patient positioning
Correct patient positioning is a key component of successful laparoscopic hysterectomy. Figure 3 shows a properly positioned patient prior to the start of the operation. Key elements of the proper positioning include:

Figure 3 Properly positioned patient
- Horizontal position of the patient on the table. Trendelenburg position should not be used prior to the insertion of the primary trocar. Premature induction of the Trendelenburg position changes the location of the bifurcation of the aorta into its common iliac branches. In normal circumstances with the patient supine, the bifurcation is at the level of the upper margin of the umbilicus. With Trendelenburg position, however, this location shifts caudally in relation to the umbilicus, thereby increasing the risk of aortic injury. Even a small shift is important because the primary trocar is normally directed at a 45° angle to the horizontal (Figure 4).
- Table height should be at or below the waist line of the operating surgeon in order to avoid muscular fatigue from the non-physiological position of the surgeon’s arms during the procedure.
- The patient’s knees should be widely separated in Allen type stirrups.
- Padded supports should be applied to the foot and posterior calf.
- Deep vein thrombosis (DVT) prophylaxis stockings – above knee type – should be applied before positioning the legs in stirrups.
- Sequential calf muscle compressors should be in place over DVT stockings.
- Both upper limbs are tucked on the patient’s sides with the IV line in place with extension tubing (Figure 5).
- When available, the body warmer mat should be used to prevent hypothermia and put in place before placing the patient on the table. Air from a warm blower can be directed onto the anterior surface of the chest. The patient’s eyes must be taped closed by the anesthesiologist after instillation of appropriate lubricant.
- The buttocks should be brought near the edge of the lower end of the table in order to facilitate easy maneuverability of the uterine manipulator (Figure 6).
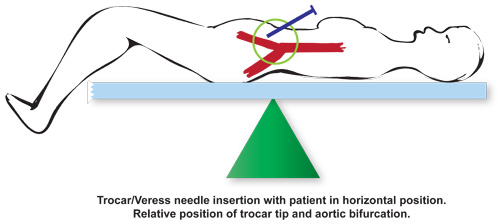
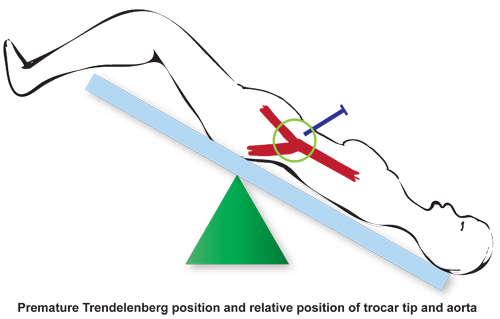
Figure 4 Diagrammatic representation of bifurcation of aorta in relation to trocar entry

Figure 5 Patient with arm at side and IV line

Figure 6 Patient with buttocks at the end of operating table