Case 5 :
A 20 year old woman comes to the polyclinic because of increasing lower abdominal pain for 3 days. The pain began insidiously, but now she is unable to walk comfortably. She has had a few chills, but no rigor. She is nauseated and vomited once this morning, but she has held down some water and tea since then. There is no diarrhea or dysentery. She developed a mild vaginal discharge during the past week.
She states that she had one other episode like the current illness the previous year. A review of her polyclinic chart indicates that she was also treated 4 months ago for mucopurulent cervicitis. The past history is otherwise unremarkable.
She is G0P0. Her last menstrual period began 5 weeks ago and was scantier than usual; menses normally occurs at 28 day intervals. The patient has had two recent sexual contacts. She is unaware that either has had any STD.
Physical Examination
|
Case 5
(continued)
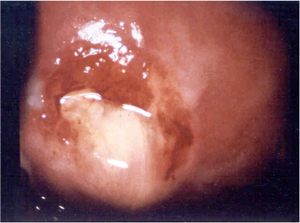
A pelvic examination is performed. There is significant pain with passage of the speculum. The cervix is reddened, and there is pus in the cervical os. A sample is taken with a swab. On digital examination, manipulation of the cervix cause exquisite pain. There is also fullness of the right adnexa, and you suspected that there is enlargement of the right Fallopian tube. A rapid pregnancy test is negative.
The cervical pus is negative for motile protozoa on a wet prep. A Gram stain is also performed and has the following appearance:
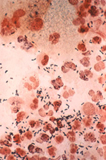
(click to enlarge photomicrograph)
Q3:
How will you treat this patient with antibiotics?
Case 5
(continued)
In addition to the prescription for medication, you advise the patient to rest for the next few days and to refrain from any sexual activity until she returns for follow-up in 1 week. You also instruct her to have her sexual contacts come to the clinic for examination and treatment and advise her to refrain from having intercourse with either of them until they complete a course of treatment. You obtain blood for an HIV serology from the patient.
The patient returns for follow-up the next week. She has taken her medication as prescribed. Her pain and discharge are resolved. She has no fever, and there is only minimal right lower quadrant tenderness on abdominal examination